
Standardization of Strategies to Perform a Parafascicular Tubular Approach for the Resection of Brain Tumors in Eloquent Areas


 ,
,  , ,
, ,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Diagnostic Imaging
2.3. Incision, Craniotomy and Extent of Resection
2.4. Intraoperative Technical Features
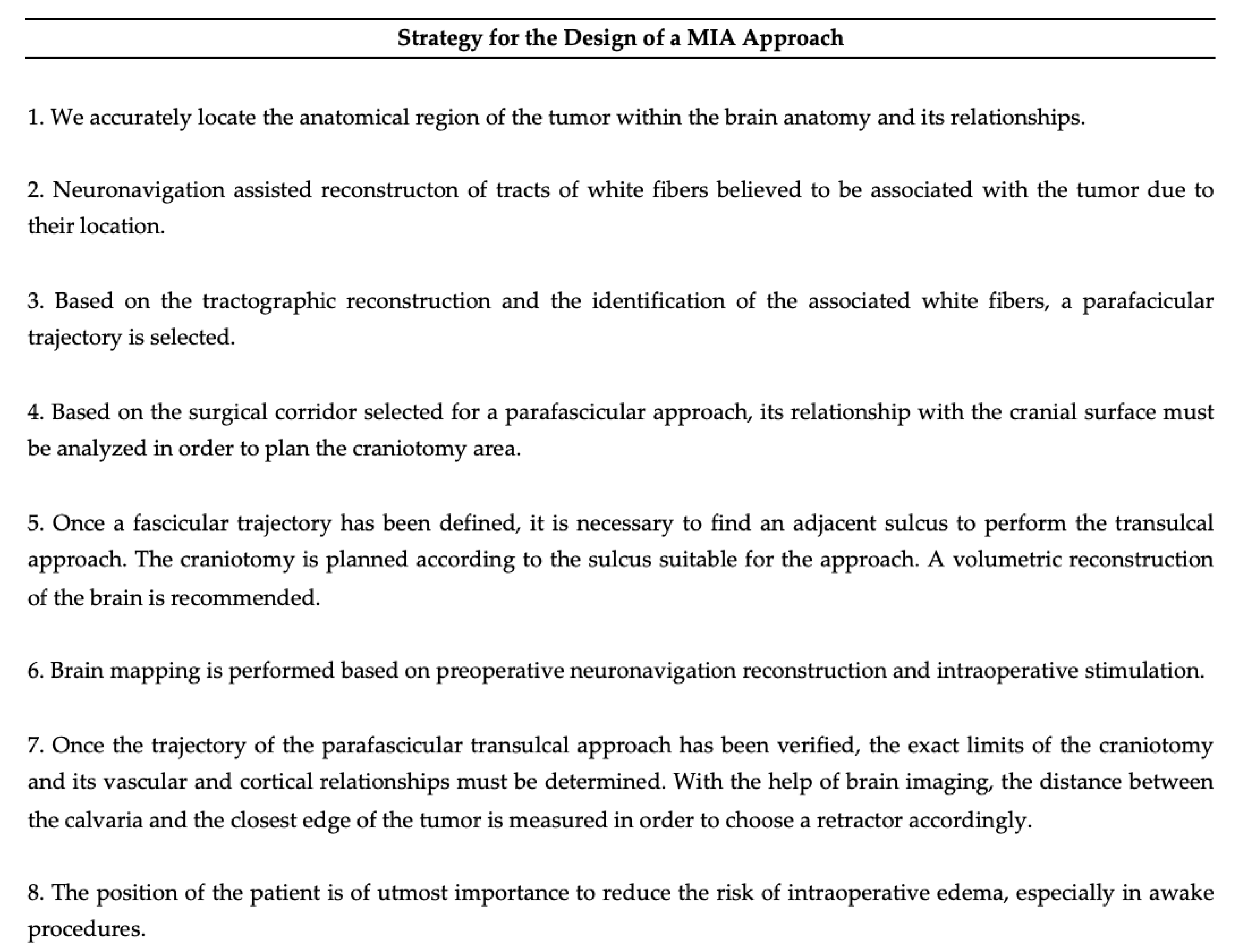
2.5. Eight Step Strategy for PTA Design
3. Results
4. Illustrative Cases
4.1. Case 1
4.2. Case 2
4.3. Surgical Nuances
5. Discussion
Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MIA | minimally invasive approach (MIA) |
| MITRs | minimally invasive tubular retractors (MITRs) |
| PTA | parafascicular transulcal approach (PTA) |
| KPS | Karnofsky Performance Scale (KPS) |
| GCS | Glasgow Coma Scale (GSC) |
| MRC | Medical Research Council (MRC) |
| LGG | low-grade glioma (LGG) |
| HGG | high-grade glioma (HGG) |
| MRI | magnetic resonance imaging (MRI) |
| DTI | diffusion tensor imaging (DTI) |
| SLF | superior longitudinal fasciculus (SLF) |
| ILF | inferior longitudinal fasciculus (ILF) |
| GCT | geniculo-calcarine fasciculus (GCT) |
| UF | uncinate fasciculus (UF) |
| CST | corticospinal tract (CST) |
| AF | arcuate fasciculus (AF) |
| AsF | anterior superior frontal (AsF) |
| nTMS | navigated trans-cranial magnetic stimulation (nTMS) |
References
- Rao, D.; Le, R.T.; Fiester, P.; Patel, J.; Rahmathulla, G. An Illustrative Review of Common Modern Craniotomies. J. Clin. Imaging Sci. 2020, 10, 81. [Google Scholar] [CrossRef]
- Teo, C. The Concept of Minimally Invasive Neurosurgery. Neurosurg. Clin. N. Am. 2010, 21, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Walker, M.L. History of Ventriculostomy. Neurosurg. Clin. N. Am. 2001, 12, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Kelly, P.J.; Goerss, S.J.; Kall, B.A. The stereotaxic retractor in computer-assisted stereotaxic microsurgery. J. Neurosurg. 1988, 69, 301–306. [Google Scholar] [CrossRef]
- Jane, J.A.; Park, T.S.; Pobereskin, L.H.; Winn, R.H.; Butler, A.B. The Supraorbital Approach: Technical Note. Neurosurgery 1982, 11, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Reisch, R.; Perneczky, A. Ten-year Experience with the Supraorbital Subfrontal Approach through an Eyebrow Skin Incision. Neurosurgery 2005, 57, 242–255. [Google Scholar] [CrossRef]
- Perneczky, A.; Reisch, R. Keyhole approaches in neurosurgery, Volume 1, Concept and surgical technique. J. Korean Neurosurg. Soc. 2009, 45, 132. [Google Scholar]
- Burkhardt, J.K.; Neidert, M.C.; Woernle, C.M.; Bozinov, O.; Bernays, R.L. Intraoperative low-field MR-guided frameless stereotactic biopsy for intracerebral lesions. Acta Neurochir. 2013, 155, 721–726. [Google Scholar] [CrossRef]
- Garrett, M.; Consiglieri, G.; Nakaji, P. Transcranial Minimally Invasive Neurosurgery for Tumors. Neurosurg. Clin. N. Am. 2010, 21, 595–605. [Google Scholar] [CrossRef]
- Larson, A.S.; Zuccarello, M.; Grande, A.W. Minimally-invasive tubular retraction ports for intracranial neurosurgery: History and future perspectives. J. Clin. Neurosci. 2021, 89, 97–102. [Google Scholar] [CrossRef]
- Sun, G.C.; Chen, X.L.; Zhao, Y.; Wang, F.; Hou, B.-k.; Wang, Y.-b.; Song, Z.-J.; Wang, D.; Xu, B.-n. Intraoperative high-field magnetic resonance imaging combined with fiber tract neu-ronavigation-guided resection of cerebral lesions involving optic radiation. Neurosurgery 2011, 69, 1070–1084. [Google Scholar] [CrossRef] [PubMed]
- Muthusami, P.; James, J.; Thomas, B.; Kapilamoorthy, T.R.; Kesavadas, C. Diffusion tensor imaging and tractography of the human language pathways: Moving into the clinical realm. J. Magn. Reson. Imaging 2014, 40, 1041–1053. [Google Scholar] [CrossRef]
- Day, J.D. Transsulcal Parafascicular Surgery Using Brain Path® for Subcortical Lesions. Neurosurgery 2017, 64, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Adawi, M.; Mosaad, N.; Teama, M. Utility of Linear Scalp Incision in Various Cranial Surgeries. Med. J. Cairo Univ. 2020, 88, 1903–1908. [Google Scholar]
- Al-Otaibi, F.; Albloushi, M.; Baeesa, S. Minicraniotomy for Standard Temporal Lobectomy: A Minimally Invasive Surgical Approach. Int. Sch. Res. Not. 2014, 2014, 532523. [Google Scholar] [CrossRef]
- Klimo, P.; Matthews, A.; Lew, S.M.; Zwienenberg-Lee, M.; Kaufman, B.A. Minicraniotomy versus bur holes for evacuation of chronic subdural collections in infants—A preliminary single-institution experience. J. Neurosurg. Pediatr. 2011, 8, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Stadie, A.T.; Kockro, R.A.; Serra, L.; Fischer, G.; Schwandt, E.; Grunert, P.; Reisch, R. Neurosurgical craniotomy localization using a virtual reality planning system versus intraoperative image-guided navigation. Int. J. Comput. Assist. Radiol. Surg. 2011, 6, 565–572. [Google Scholar] [CrossRef]
- Luo, M.; Frisken, S.F.; Narasimhan, S.; Clements, L.W.; Thompson, R.C.; Golby, A.J.; Miga, M.I. A comprehensive model-assisted brain shift correction approach in image-guided neurosurgery: A case study in brain swelling and subsequent sag after craniotomy. In Proceedings of the Medical Imaging 2019: Image-Guided Procedures, Robotic Interventions, and Modeling, San Diego, CA, USA, 17–19 February 2019; Volume 10951, pp. 15–24. [Google Scholar] [CrossRef]
- Monroy-Sosa, A.; Chakravarthi, S.S.; Epping, A.; Fukui, M.B.; Jennings, J.; Rovin, R.; Kassam, A.B. Trans-sulcal Parafascicular Surgical Corridor for Resection of Brain Tumors: The Last Frontier. In Principles of Neurooncology; Springer: Cham, Switzerland, 2021. [Google Scholar]
- Kinoshita, M.; Miyashita, K.; Tsutsui, T.; Furuta, T.; Nakada, M. Critical Neural Networks in Awake Surgery for Gliomas. Neurol. Med. Chir. 2016, 56, 674–686. [Google Scholar] [CrossRef]
- Skrap, M.; Marin, D.; Ius, T.; Fabbro, F.; Tomasino, B. Brain mapping: A novel intraoperative neuropsychological approach. J. Neurosurg. 2016, 125, 877–887. [Google Scholar] [CrossRef]
- Greenfield, J.P.; Cobb, W.S.; Tsouris, A.J.; Schwartz, T.H. Stereotactic minimally invasive tubular retractor system for deep brain lesions. Neurosurgery 2008, 63 (Suppl. 2), 334–339. [Google Scholar] [CrossRef]
- Kurozumi, K.; Otani, Y.; Ishida, J.; Hiramatsu, M.; Kameda, M.; Ichikawa, T.; Date, I. Combination of the tubular retractor and brain spatulas provides an adequate operative field in surgery for deep-seated lesions: Case series and technical note. Surg. Neurol. Int. 2018, 9, 220. [Google Scholar] [CrossRef]
- Umana, G.E.; Scalia, G.; Graziano, F.; Maugeri, R.; Alberio, N.; Barone, F.; Crea, A.; Fagone, S.; Giammalva, G.R.; Brunasso, L.; et al. Navigated Transcranial Magnetic Stimulation Motor Mapping Usefulness in the Surgical Management of Patients Affected by Brain Tumors in Eloquent Areas: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 644198. [Google Scholar] [CrossRef]
- Conti, A.; Raffa, G.; Granata, F.; Rizzo, V.; Germanò, A.; Tomasello, F. Navigated Transcranial Magnetic Stimulation for “Somatotopic” Tractography of the Corticospinal Tract. Neurosurgery 2014, 10 (Suppl. 4), 542–554. [Google Scholar] [CrossRef]
- Raffa, G.; Conti, A.; Scibilia, A.; Sindorio, C.; Quattropani, M.C.; Visocchi, M.; Germanò, A.; Tomasello, F. Functional Reconstruction of Motor and Language Pathways Based on Navigated Transcranial Magnetic Stimulation and DTI Fiber Tracking for the Preoperative Planning of Low Grade Glioma Surgery: A New Tool for Preservation and Restoration of Eloquent Networks. Acta Neurochir. 2017, 124, 251–261. [Google Scholar] [CrossRef]
- Raffa, G.; Picht, T.; Scibilia, A.; Rösler, J.; Rein, J.; Conti, A.; Ricciardo, G.; Cardali, S.M.; Vajkoczy, P.; Germanò, A. Surgical treatment of meningiomas located in the rolandic area: The role of navigated transcranial magnetic stimulation for preoperative planning, surgical strategy, and prediction of arachnoidal cleavage and motor outcome. J. Neurosurg. 2019, 133, 107–118. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Neurological Examination | % | |
|---|---|---|
| Altered Force | 41.6 | |
| Language Disturbances | ||
| Paraphasia | 12.5 | |
| Aphasia | 11.1 | |
| Anomic | 2.7 | |
| Conduction | 2.7 | |
| Global | 1.3 | |
| Broca’s | 2.7 | |
| Transcortical | 1.3 | |
| Tumor Localization | ||
| Frontal | 26.3 | |
| Parietal | 11.1 | |
| Frontoparietal | 25 | |
| Other | 37.6 | |
| Tumor Type | ||
| High Grade Gliomas | 34.7 | |
| Low Grade Gliomas | 29.2 | |
| Metastasis | 25 | |
| Other | 11.1 | |
| Resection | ||
| Total | 94.4 | |
| Sub-Total | 5.5 | |
| Partial | 0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdala-Vargas, N.J.; Umana, G.E.; Patiño-Gomez, J.G.; Ordoñez-Rubiano, E.; Cifuentes-Lobelo, H.A.; Palmisciano, P.; Ferini, G.; Viola, A.; Zagardo, V.; Casanova-Martínez, D.; et al. Standardization of Strategies to Perform a Parafascicular Tubular Approach for the Resection of Brain Tumors in Eloquent Areas. Brain Sci. 2023, 13, 498. https://doi.org/10.3390/brainsci13030498
Abdala-Vargas NJ, Umana GE, Patiño-Gomez JG, Ordoñez-Rubiano E, Cifuentes-Lobelo HA, Palmisciano P, Ferini G, Viola A, Zagardo V, Casanova-Martínez D, et al. Standardization of Strategies to Perform a Parafascicular Tubular Approach for the Resection of Brain Tumors in Eloquent Areas. Brain Sciences. 2023; 13(3):498. https://doi.org/10.3390/brainsci13030498
Chicago/Turabian StyleAbdala-Vargas, Nadin J., Giuseppe E. Umana, Javier G. Patiño-Gomez, Edgar Ordoñez-Rubiano, Hernando A. Cifuentes-Lobelo, Paolo Palmisciano, Gianluca Ferini, Anna Viola, Valentina Zagardo, Daniel Casanova-Martínez, and et al. 2023. "Standardization of Strategies to Perform a Parafascicular Tubular Approach for the Resection of Brain Tumors in Eloquent Areas" Brain Sciences 13, no. 3: 498. https://doi.org/10.3390/brainsci13030498
APA StyleAbdala-Vargas, N. J., Umana, G. E., Patiño-Gomez, J. G., Ordoñez-Rubiano, E., Cifuentes-Lobelo, H. A., Palmisciano, P., Ferini, G., Viola, A., Zagardo, V., Casanova-Martínez, D., Tomasi, O. S., Campero, A., & Baldoncini, M. (2023). Standardization of Strategies to Perform a Parafascicular Tubular Approach for the Resection of Brain Tumors in Eloquent Areas. Brain Sciences, 13(3), 498. https://doi.org/10.3390/brainsci13030498