
Does Motor Tract Integrity at 1 Month Predict Gait and Balance Outcomes at 6 Months in Stroke Patients?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Functional Assessment
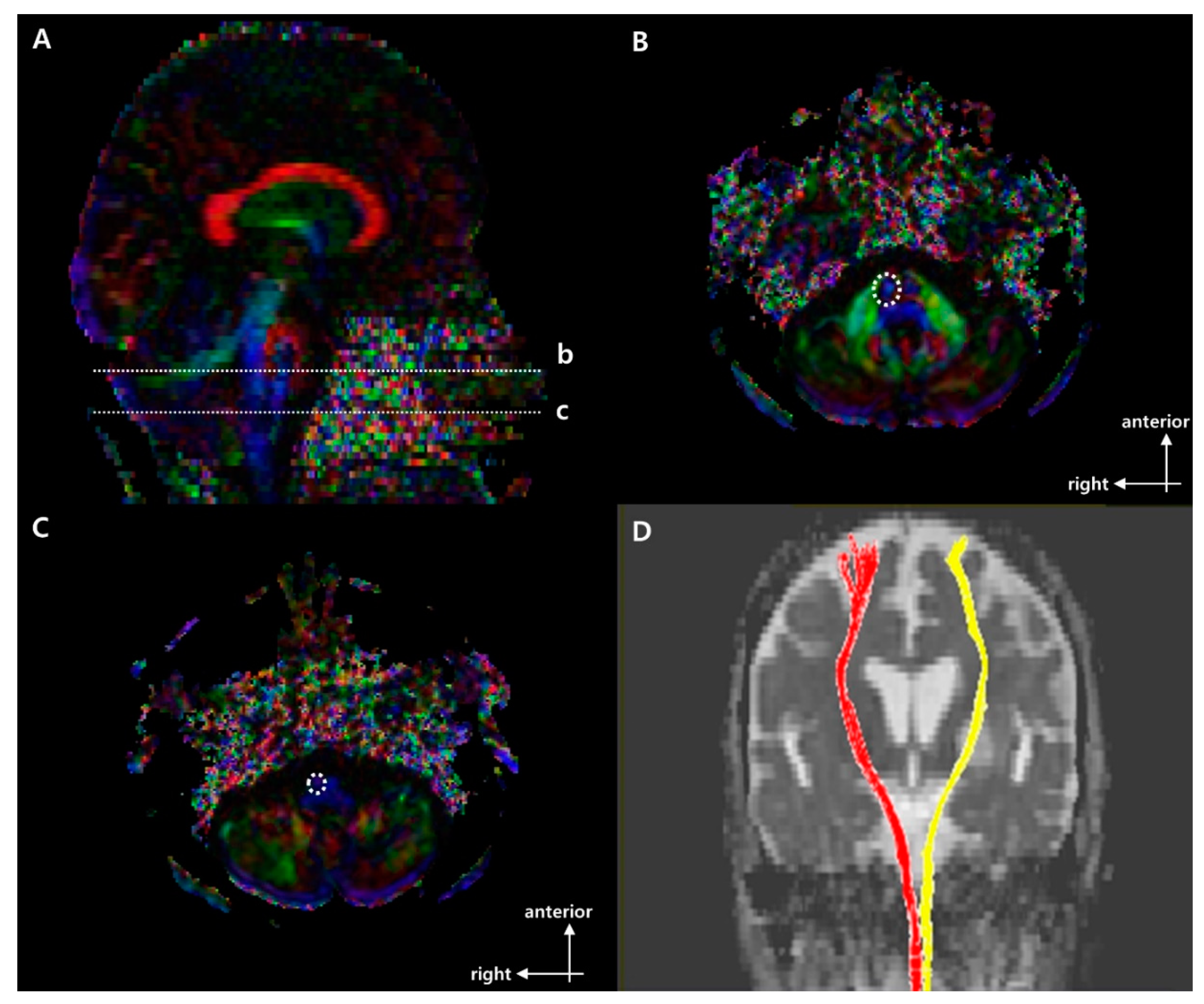
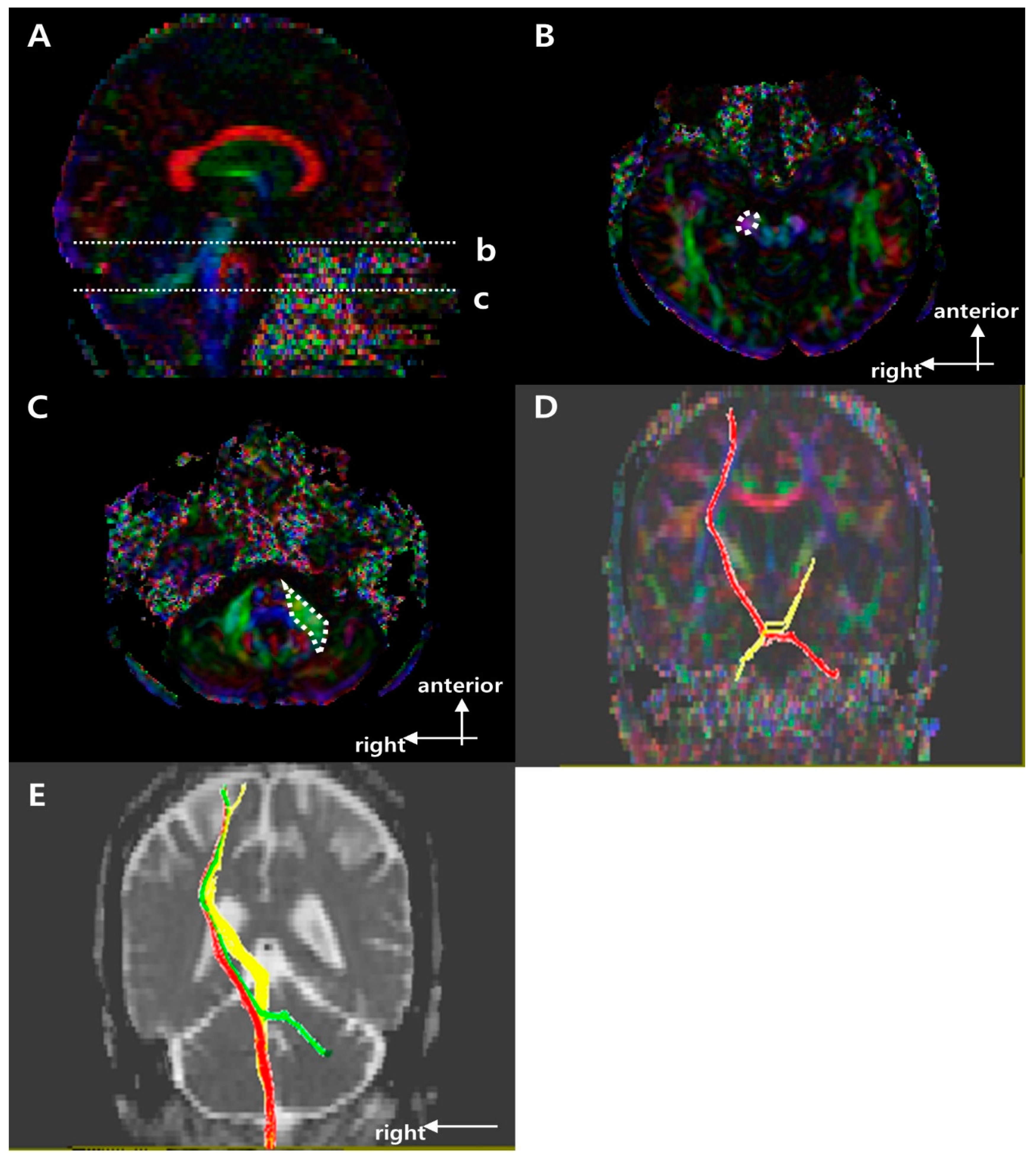
2.3. Fiber Bundle Tracking
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Takakusaki, K. Neurophysiology of gait: From the spinal cord to the frontal lobe. Mov. Disord. 2013, 28, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Alexander, L.D.; Black, S.E.; Patterson, K.K.; Gao, F.; Danells, C.J.; McIlroy, W.E. Association Between Gait Asymmetry and Brain Lesion Location in Stroke Patients. Stroke 2009, 40, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.B.; Kim, J.S.; Hong, B.Y.; Lim, S.H. Clinical recovery from stroke lesions and related outcomes. J. Clin. Neurosci. 2017, 37, 79–82. [Google Scholar] [CrossRef]
- Lee, K.B.; Kim, J.S.; Hong, B.Y.; Sul, B.; Song, S.; Sung, W.J.; Hwang, B.Y.; Lim, S.H. Brain lesions affecting gait recovery in stroke patients. Brain Behav. 2017, 7, e00868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soulard, J.; Huber, C.; Baillieul, S.; Thuriot, A.; Renard, F.; Broche, B.A.; Krainik, A.; Vuillerme, N.; Jaillard, A.; on behalf of the ISIS-HERMES Group. Motor tract integrity predicts walking recovery. Neurology 2020, 94, e583–e593. [Google Scholar] [CrossRef] [PubMed]
- Schaechter, J.D.; Fricker, Z.P.; Perdue, K.; Helmer, K.G.; Vangel, M.G.; Greve, D.N.; Makris, N. Microstructural status of ipsilesional and contralesional corticospinal tract correlates with motor skill in chronic stroke patients. Hum. Brain Mapp. 2009, 30, 3461–3474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, A.R.; Kim, D.H.; Park, S.Y.; Kyeong, S.; Kim, Y.; Lee, S.-K.; Kim, D.Y. Can the integrity of the corticospinal tract predict the long-term motor outcome in poststroke hemiplegic patients? NeuroReport 2018, 29, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Yoo, Y.J.; Kim, J.W.; Kim, J.S.; Hong, B.Y.; Lee, K.B.; Lim, S.H. Corticospinal Tract Integrity and Long-Term Hand Function Prognosis in Patients with Stroke. Front. Neurol. 2019, 10, 374. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H.; Lee, S.J. Corticoreticular Tract in the Human Brain: A Mini Review. Front. Neurol. 2019, 10, 1188. [Google Scholar] [CrossRef]
- Kim, Y.; Im, S.; Kim, S.-H.; Park, G.-Y. Laterality of cerebellar afferent and efferent pathways in a healthy right-handed population: A diffusion tensor imaging study. J. Neurosci. Res. 2019, 97, 582–596. [Google Scholar] [CrossRef]
- Jang, S.H.; Kwon, H.G. Injury of the cortico-ponto-cerebellar tract in a patient with mild traumatic brain injury. Medicine 2017, 96, e8749. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.B.; Hong, B.Y.; Kim, J.S.; Sul, B.; Yoon, S.C.; Ji, E.-K.; Son, D.B.; Hwang, B.Y.; Lim, S.H. Which brain lesions produce spasticity? An observational study on 45 stroke patients. PLoS ONE 2019, 14, e0210038. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.-T.; Lin, K.-C.; Liu, H.-L.; Chen, Y.-L.; Wu, C.-Y. Changes in structural integrity are correlated with motor and functional recovery after post-stroke rehabilitation. Restor. Neurol. Neurosci. 2015, 33, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Imura, T.; Nagasawa, Y.; Inagawa, T.; Imada, N.; Izumi, H.; Emoto, K.; Tani, I.; Yamasaki, H.; Ota, Y.; Oki, S.; et al. Prediction of motor outcomes and activities of daily living function using diffusion tensor tractography in acute hemiparetic stroke patients: A multi-time-point study. J. Phys. Ther. Sci. 2015, 27, 1383–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehrholz, J.; Wagner, K.; Rutte, K.; Meiβner, D.; Pohl, M. Predictive Validity and Responsiveness of the Functional Ambulation Category in Hemiparetic Patients After Stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1314–1319. [Google Scholar] [CrossRef]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in Stroke Rehabilitation: A Systematic Review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef]
- Jung, H.Y.; Park, B.K.; Shin, H.S.; Kang, Y.K.; Pyun, S.B.; Paik, N.J.; Kim, S.H.; Kim, T.H.; Han, T.R. Development of the Korean version of modified barthel index (k-mbi): Multi-center study for subjects with stroke. J. Korean Acad. Rehabil. Med. 2007, 31, 283–297. [Google Scholar]
- Lee, Y.; Kim, J.S.; Hong, B.Y.; Park, J.G.; Yoo, J.W.; Lee, K.B.; Kim, T.-W.; Lim, S.H. Determinant of Quality of Life in Patients with Chronic Cerebral Infarct. Brain Neurorehabilit. 2020, 13, 10–12786. [Google Scholar] [CrossRef]
- Binkofski, F.; Seitz, R.J.; Hacklander, T.; Pawelec, D.; Mau, J.; Freund, H.J. Recovery of motor functions following hemipa-retic stroke: A clinical and magnetic resonance-morphometric study. Cerebrovasc. Dis. 2011, 11, 273–281. [Google Scholar] [CrossRef]
- Jiang, H.; van Zijl, P.C.; Kim, J.; Pearlson, G.D.; Mori, S. DtiStudio: Resource program for diffusion tensor computation and fiber bundle tracking. Comput. Methods Programs Biomed. 2006, 81, 106–116. [Google Scholar] [CrossRef]
- Seo, J.; Jang, S. Different Characteristics of the Corticospinal Tract According to the Cerebral Origin: DTI Study. Am. J. Neuroradiol. 2013, 34, 1359–1363. [Google Scholar] [CrossRef] [Green Version]
- Son, S.M.; Shin, S.M. Disruption of the Corticoreticular Tract in Pediatric Patients with Trunk Instability: A Diffusion Tensor Tractography Study. Ann. Rehabil. Med. 2017, 41, 1093–1099. [Google Scholar] [CrossRef]
- Jang, S.H.; Kim, K.; Kim, S.H.; Son, S.M.; Jang, W.H.; Kwon, H.G. The relation between motor function of stroke patients and diffusion tensor imaging findings for the corticospinal tract. Neurosci. Lett. 2014, 572, 1–6. [Google Scholar] [CrossRef]
- Perennou, D.A.; Mazibrada, G.; Chauvineau, V.; Greenwood, R.; Rothwell, J.; Gresty, M.A.; Bronstein, A.M. Lateropulsion, pushing and verticality perception in hemisphere stroke: A causal relationship? Brain 2008, 131, 2401–2413. [Google Scholar] [CrossRef] [Green Version]
- Johannsen, L.; Broetz, D.; Naegele, T.; Karnath, H.-O. “Pusher syndrome” following cortical lesions that spare the thalamus. J. Neurol. 2006, 253, 455–463. [Google Scholar] [CrossRef]
- Lee, K.; Yoo, S.; Ji, E.; Hwang, W.; Yoo, Y.; Yoon, M.-J.; Hong, B.; Lim, S. Is Lateropulsion Really Related with a Specific Lesion of the Brain? Brain Sci. 2021, 11, 354. [Google Scholar] [CrossRef]
- Surgent, O.J.; Dadalko, O.I.; Pickett, K.A.; Travers, B.G. Balance and the brain: A review of structural brain correlates of postural balance and balance training in humans. Gait Posture 2019, 71, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.S.; Pomeroy, V.; Wang, J.; Schlaug, G.; Marrapu, S.T.; Geva, S.; Rowe, P.; Chandler, E.; Kerr, A.; Baron, J.; et al. Does stroke location predict walk speed response to gait rehabilitation? Hum. Brain Mapp. 2016, 37, 689–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.B.; Lim, S.H.; Kim, K.H.; Kim, K.J.; Kim, Y.R.; Chang, W.N.; Yeom, J.W.; Kim, Y.D.; Hwang, B.Y. Six-month functional recovery of stroke patients. Int. J. Rehabil. Res. 2015, 38, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Fall Risk→ | High (0 ≤ BBS ≤ 20) | Moderate (21 ≤ BBS ≤ 40) | Low (41 ≤ BBS ≤ 56) | p-Value |
|---|---|---|---|---|
| Numbers of subjects | 6 | 8 | 13 | |
| Age, years | 61.0 (56.3–66.5) | 75.5 (62.5–81.0) | 63.5 (33.5–73.8) | 0.060 |
| Gender | 0.090 | |||
| Female, n (%) | 1 (16.7) | 6 (75.0) | 4 (30.8) | |
| Male, n (%) | 5 (83.3) | 2 (25.0) | 9 (69.2) | |
| Stroke type | 0.206 | |||
| Infarction, n (%) | 5 (83.3) | 8 (100.0) | 9 (69.2) | |
| Hemorrhage, n (%) | 1 (16.7) | 0 (0.0) | 4 (30.8) | |
| Brain injury location | 0.778 | |||
| Cortex, n (%) | 0 (0.0) | 0 (0.0) | 1 (7.7) | |
| Subcortex, n (%) | 6 (100.0) | 7 (87.5) | 12 (92.3) | |
| Mixed, n (%) | 0 (0.0) | 1 (12.5) | 0 (0.0) | |
| Hemispheric lesion | 0.889 | |||
| Left, n (%) | 4 (66.7) | 4 (50.0) | 7 (53.8) | |
| Right, n (%) | 2 (33.3) | 4 (50.0) | 6 (46.2) | |
| K-MBI | 23.0 (12.0–34.8) | 63.5 (33.5–73.8) | 81.0 (77.0–84.0) | |
| Fall Risk→ | High (0 ≤ BBS ≤ 20, n = 6) | Moderate (21 ≤ BBS ≤ 40, n = 8) | Low (41 ≤ BBS ≤ 56, n = 13) | p-Value | |
|---|---|---|---|---|---|
| CST | FN | 0.043 (0.003–0.495) | 0.414 (0.362–0.677) | 0.392 (0.124–0.546) | 0.214 |
| FA | 0.644 (0.134–0.898) | 0.882 (0.846–0.964) | 0.948 (0.862–0.971) | 0.058 | |
| CRP | FN | 0.379 (0.275–0.480) | 0.280 (0.193–0.636) | 0.354 (0.211–0.483) | 0.920 |
| FA | 0.992 (0.935–1.033) | 0.959 (0.940–0.978) | 0.962 (0.934–0.977) | 0.506 | |
| CPCT | FN | 0.123 (0.018–0.443) | 0.052 (0.0–0.465) | 0.162 (0.0–0.351) | 0.960 |
| FA | 0.927 (0.230–0.983) | 0.476 (0.0–1.019) | 0.915 (0.0–0.965) | 0.878 | |
| Nonfunctional (FAC 0,1, n = 19) | Dependent (FAC 2,3, n = 6) | Independent (FAC 4,5, n = 2) | p-Value | ||
|---|---|---|---|---|---|
| CST | FN | 0.406 (0.195–0.571) | 0.335 (0.119–0.559) | 0.665 (0.389–0.942) | 0.870 |
| FA | 0.862 (0.788–0.947) | 0.962 (0.939–0.986) | 0.952 (0.950–0.954) | 0.173 | |
| CRP | FN | 0.299 (0.204–0.510) | 0.346 (0.303–0.408) | 0.348 (0.206–0.491) | 0.877 |
| FA | 0.977 (0.933–0.988) | 0.958 (0.948–0.971) | 0.924 (0.919–0.929) | 0.330 | |
| CPCT | FN | 0.118 (0.0–0.442) | 0.0 (0.0–0.259) | 0.289 (0.145–0.434) | 0.692 |
| FA | 0.952 (0.0–1.003) | 0.0 (0.0–0.713) | 0.458 (0.229–0.686) | 0.331 | |
| Nonfunctional (FAC 0,1, n = 9) | Dependent (FAC 2,3, n = 10) | Independent (FAC 4,5, n = 8) | p-Value | ||
|---|---|---|---|---|---|
| CST | FN | 0.159 (0.014–0.883) | 0.410 (0.290–0.513) | 0.403 (0.121–0.546) | 0.859 |
| FA | 0.867 (0.535–0.947) | 0.932 (0.836–0.967) | 0.905 (0.848–0.953) | 0.634 | |
| CRP | FN | 0.299 (0.269–0.485) | 0.344 (0.216–0.451) | 0.330 (0.174–0.643) | 0.998 |
| FA | 0.976 (0.922–1.008) | 0.971 (0.950–0.981) | 0.954 (0.929–0.978) | 0.703 | |
| CPCT | FN | 0.073 (0.0–0.533) | 0.0 (0.0–0.115) | 0.348 (0.121–0.615) | 0.163 |
| FA | 0.918 (0.0–0.999) | 0.0 (0.0–0.962) | 0.957 (0.686–1.015) | 0.405 | |
| CST | CRP | CPCT | ||||
|---|---|---|---|---|---|---|
| FN | FA | FN | FA | FN | FA | |
| BBS on 6 month | 0.106 | 0.329 | −0.049 | −0.138 | −0.016 | −0.078 |
| 0.497 | 0.035 | 0.751 | 0.375 | 0.924 | 0.634 | |
| FAC on 1 month | 0.004 | 0.285 | 0.033 | −0.214 | −0.116 | −0.245 |
| 0.979 | 0.074 | 0.834 | 0.181 | 0.492 | 0.146 | |
| FAC on 6 month | 0.027 | 0.121 | −0.014 | −0.104 | 0.152 | 0.091 |
| 0.859 | 0.436 | 0.929 | 0.504 | 0.351 | 0.576 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jun, S.; Hong, B.; Kim, Y.; Lim, S. Does Motor Tract Integrity at 1 Month Predict Gait and Balance Outcomes at 6 Months in Stroke Patients? Brain Sci. 2021, 11, 867. https://doi.org/10.3390/brainsci11070867
Jun S, Hong B, Kim Y, Lim S. Does Motor Tract Integrity at 1 Month Predict Gait and Balance Outcomes at 6 Months in Stroke Patients? Brain Sciences. 2021; 11(7):867. https://doi.org/10.3390/brainsci11070867
Chicago/Turabian StyleJun, SoYeon, BoYoung Hong, YoungKook Kim, and SeongHoon Lim. 2021. "Does Motor Tract Integrity at 1 Month Predict Gait and Balance Outcomes at 6 Months in Stroke Patients?" Brain Sciences 11, no. 7: 867. https://doi.org/10.3390/brainsci11070867
APA StyleJun, S., Hong, B., Kim, Y., & Lim, S. (2021). Does Motor Tract Integrity at 1 Month Predict Gait and Balance Outcomes at 6 Months in Stroke Patients? Brain Sciences, 11(7), 867. https://doi.org/10.3390/brainsci11070867