Featured Application
Roberto Cameriere and Ivan Galić equally contributed to this paper.
Abstract
This paper aims to propose a statistical model to assess pubertal growth spurt using the ratio of the anterior height projection to the posterior (Vba) of the fourth cervical vertebra body (C4) on cephalograms and to calculate the residual proportion of skeletal maturation and the time for the pubertal growth spurt to end for a given Vba. A sample of 538 cephalograms from healthy-living children aged between 5 and 15 years was analyzed. A segmented regression model was used to explain the different Vba stages relative to the pubertal growth spurt. In addition, the time to achieve skeletal maturation was evaluated for a given Vba between the beginning (Vba1) and the end (Vba2) of the pubertal growth spurt. A longitudinal sample of 25 males and 25 females was analyzed to validate the proposed method. The values of Vba corresponding to higher pubertal development rate ranged from Vba1 = 0.677 (95%CI, 0.644–0.711) to Vba2 = 0.966 (95%CI, 0.905–1.028) and from Vba1 = 0.669 (95%CI, 0.645–0.693) to Vba2 = 1.073 (95%CI, 1.044–1.101) in males and females, respectively. The validation process results showed that our model did not produce any incorrect forecasts. The proposed method estimates the beginning and the end of the pubertal growth spurt together with the residual proportion of skeletal maturation for a given Vba.
1. Introduction
Dynamics and timing of dental and skeletal maturation in growing children are fundamental in orthodontic treatment planning; they provide clinical information on how and when a patient should start using maxillary orthopedic appliances or indicate the necessity for orthognathic surgery [1,2,3]. Growth and development assessments use individual indicators or developmental stages to describe the changes that occur during life. Indicators can vary from height and weight gain, development of sexual characteristics, menarche in women, and assessment of mental maturity [4]. Since chronological age is an unreliable way to estimate pubertal growth spurt because of the high variability among individuals in its timing of initiation, duration, and amount during children’s growth, several other approaches have been used [5,6,7,8,9,10].
X-ray of the hand and wrist to assess skeletal maturity has been a standard procedure in clinical orthodontics to assess whether a person is skeletally mature or determine the possibilities of planned therapy [11]. The most straightforward approach to assessing the development of the hand and wrist is to compare the X-ray image with the available Atlas of the development of the hand and wrist [12]. According to Greulich and Pyle, the Atlas of skeletal development of the hand and wrist contains images of the hand and wrist of normal healthy children from birth to adulthood with an age interval of 3 years [13]. Hagg and Taranger [12] studied the skeletal stages of the hand and wrist to indicate a pubertal growth spurt. They concluded that specific skeletal indicators, the ulnar sesamoid of the metacarpophalangeal joint of the first finger, the epiphyses of the middle and distal phalanges of the third finger, and the distal epiphysis of the radius might indicate the onset, peak, and end of the pubertal growth spurt [12]. Bjork et al. [4], in their method for epidemiological registration of malocclusion, defined two stages of the eruption of deciduous teeth, five stages of the eruption of permanent anterior teeth, and four stages of the eruption of permanent molars. Björk and Helm [14] showed that dental stages from Bjork et al. [4], close to the timing of maximum pubertal growth in height, DS4, all canines, and premolars fully erupted, and DS M2, all second molars fully erupted, were of little value as criteria of pubertal peak comparing to ossification of the ulnar sesamoid at the metacarpophalangeal joint of the thumb or menarche. The timing of the eruption of permanent teeth is more dependent on local factors such as loss of deciduous teeth or crowding [15].
Historically, the most common method for assessment of skeletal maturation was an analysis of hand–wrist radiograph, used later by Fishman [16], who related specific skeletal maturity indicator stages to pubertal growth spurt. Furthermore, Lamparski [17] claimed that the use of the cervical vertebrae was as valid as the hand–wrist bones to assess skeletal maturation and described a new approach based on the changes in the shape of five cervical vertebrae. His study designed a series of standards of cervical vertebral maturation (CVM), separating male and female participants concerning chronological age and skeletal maturation [17]. Hassel and Farman [18] modified Lamparski’s method and proved that CVM was acceptably accurate and helpful in estimating an individual’s skeletal maturity and residual growth potential, as well as the hand–wrist method. Studies from Baccetti [1] and Franchi [19] further demonstrated that CVM method is useful as a biological indicator for both mandibular and somatic maturation.
Hassel and Farman [18] modified Lamparski’s method and demonstrated the changes in the shape of cervical vertebrae in each stage of skeletal growth, proving to be acceptably accurate and valuable for estimating skeletal maturity and residual growth potential of an individual as the hand–wrist method. Finally, Baccetti et al. [1] and Franchi et al. [19] showed that the cervical vertebral maturation method is useful as a biological indicator for both mandibular and somatic maturation. Their study was critical due to the use of longitudinal data from radiographs and because their method was based on changes in the annual increase in total mandibular length instead of comparison with hand–wrist skeletal age [1,19].
Dental age estimation methods in children can help assess the development of the dentition, whether it is accelerated or delayed, and the effect of specific therapeutic procedures in oncology patients. In addition, they can be used in research on the growth and development of twins, the effect of hormone replacement therapy, or in estimating age in persons without the possibility of identification [20,21,22,23,24,25]. In the development of permanent teeth, their exchange with milk teeth is essential, as the lower and upper molars and front incisors sprout first, and tooth sprouting takes place until 21–23 years of age [26]. In addition to age assessment based on the number of permanent teeth in the mouth, more reliable methods of dental age assessment are based on the analysis of radiographic images, and so far, several methods have been presented that mainly assess tooth development in stages. The most commonly used methods that use developed stages are Demirjian, Willems, Haavikko, and Chaillet [27,28,29,30]. If a strong association of dental development with skeletal development were to be proven, some of the values used to assess tooth development could be taken as a reference or even the first choice in diagnosing the pubertal growth spurt. Dental scans are a mandatory part of the protocol when planning orthodontic therapy so that they can assess the expected or completed pubertal growth spurt [31].
The atlas or staging systems generally used in estimating the development regularly contain a set of longitudinal figures of different ossification stages, which typically do not stand on accurate measurements with definite orientation points [32]. Cameriere et al. introduced another approach for studying dental and skeletal development for age estimation by specific lengths or area measurements of the apposition of secondary dentine in dental radiographs and the ossification of the carpal skeleton in hand and wrist radiographs [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49].
Cameriere et al. [40] and Gulsahi et al. [50] published articles where the heights of the anterior and posterior sides of the C4 vertebral body from lateral cephalograms in individuals aged 5–15 years were used to estimate the chronological age with forensic purposes. The ratio of heights or Vba has shown a correlation to chronological age and was recognized as a potential indicator for age estimation in this age range [40]. After Bayes calibration, the mean absolute errors (MAEs) were 1.34 years with standard deviation (SD) of 0.95 years and 1.01 years (SD 0.71 years), and the mean inter-quartile ranges (MIQRs) of the calibrating distribution were 2.32 years (SD, 0.25 years) and 1.72 years (SD, 0.39 years) in males and females, respectively [40]. Gulsahi et al. [50] also investigated the correlation of age and Vba on the Turkish sample, and after Bayes calibration, MAEs were 0.879 years and 0.906 years (mean interquartile ranges (MIQR.s) 1.290 and 1.435 years) in males and females, respectively.
According to published results of the usefulness of Vba in the specific age span of development when adolescent growth spurt occurs, we decided to study the values of Vba, particularly the distributions of its minimum and maximum, during adolescence.
The aims of this study were, therefore, to evaluate the ratio of the anterior height projection to the posterior (Vba) of the fourth cervical vertebra body (C4) on cephalograms and its relationship with a pubertal growth spurt and to propose a statistical model based on segmented regression to calculate the residual proportion of the skeletal maturation for a given Vba and the time for the pubertal growth spurt to end for a given Vba.
The proposed model will be validated using longitudinal data from the Michigan Growth Center supported by the American Association of Orthodontists Foundation (AAOF).
2. Materials and Methods
This cross-sectional observational study evaluated 527 lateral cephalograms previously taken for dental diagnoses and pretreatment planning. All participants were healthy individuals aged between 5 and 15 years who lived in Croatia and without a recorded history of genetic or developmental anomalies of the skeleton. The study was conducted by the ethical standards laid down by the Declaration of Helsinki [51].
The age and sex distribution for each age category of the sample are presented in Figure 1.
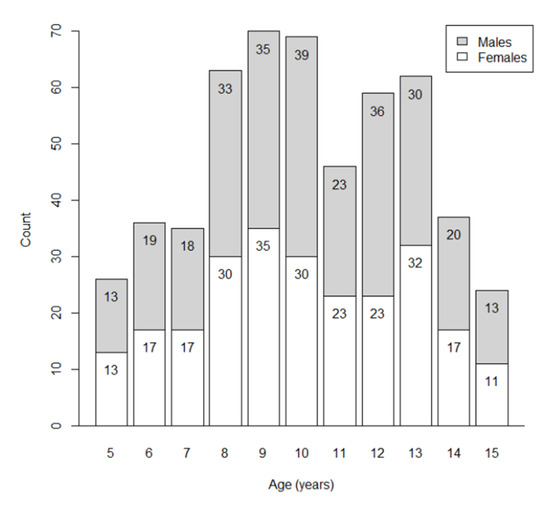
Figure 1.
Frequency distribution of the sample by sex and age cohort.
In addition, the following data were recorded for each subject: dates of birth and of the radiograph, sex, as reported on the radiograph, and ancestry as reported by either self or family. The observers were blinded to information on the subject’s sex and age.
The radiographs were processed according to the method of Cameriere et al. [40]. The ratio of the anterior height projection to the posterior (A/B = Vba), Figure 2, was used first to correlate with the different moments of the pubertal growth spurt and second, to propose a method that can quantitatively determine the beginning and the end of the pubertal growth spurt in an individual.

Figure 2.
An example of the anterior (A) and the posterior (B) sides of the fourth cervical vertebral body. The anterior side of the body is measured up to the point where the anterior side (A) curves (C1) towards the superior side (C2) of the vertebral body.
We evaluated lateral cephalograms from 50 subjects (25 males and 25 females) to validate the proposed model. The lateral cephalograms of the subjects belong to the Michigan Growth Center and include the subset of subjects with at least four radiographs. For each subject, the number of observations ranged from 4 to 6, totaling 227 radiographs.
Statistical Analysis
Thirty randomly selected lateral cephalograms were reanalyzed after two weeks to assess the intra-observer repeatability and inter-observer reliability of Vba by the same observer and a second one, respectively. The intra-class correlation coefficient (ICC) was used to evaluate intra- and inter-observer agreement [52].
According to the results in this study and reported by Cameriere et al. [40], we considered that C4 development presented as Vba increment is not constant concerning age, but it seems to follow three distinct phases with increment in the intermediate phase.
The nonlinear relationship between Vba and actual age suggests fitting data using a segmented regression model, which allows us to estimate two breakpoints, τ1 and τ2 and both regression coefficients characterize the interval of ages with higher pubertal development rate [53]. The proposed segmented regression model to fit the data is:
where βi, i = 0, … 3, are the regression coefficients, and (x)+ is equal to x if x is positive and 0 otherwise. The meanings of the regression coefficients are: β0 is the intercept of the piecewise linear curve with the vertical axis (see Figure 3), i.e., it is the mean Vba value at age = 0; β1 is the “left” slope, i.e., the growth rate when age < τ1; the sum β1 + β2 is the “central” slope, i.e., the growth rate of Vba when the individual age belongs to the interval (τ1, τ2); finally, the sum β1 + β2 + β3 is the “right” slope, namely the slope when age > τ2) and it is the growth rate of Vba when individual’s age is greater than τ2.
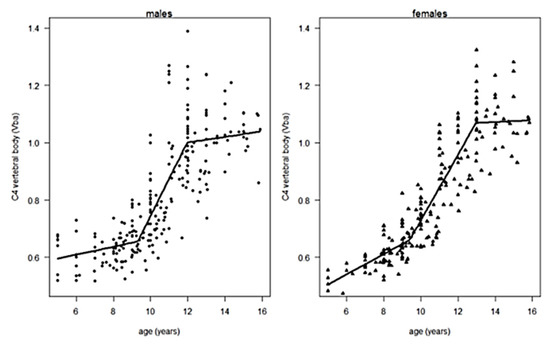
Figure 3.
The distribution of the proportions of the anterior and posterior sides of the C4 vertebral body (Vba) as the function of age for males (left) and females (right) subjects with segmented regression plots.
Fitting the model to the data, we estimated the regression coefficients and two breakpoints. Furthermore, we estimated the values of Vba corresponding to the two breakpoints, Vba1 and Vba2 (spurts), and, for a given value of Vba, the residual proportion of maturation of the C4 vertebral body, θ. Considering that Vba1 and Vba2 are the random variables normally distributed, the residual proportion of maturation, θ, is also a random variable, but it is not normally distributed. Consequently, for each value of Vba, we reported the median, the first, and the third quartile of θ.
Concerning the validation process, for the k-th subject (k = 1, … N), the gathered information can be summarized considering the set k = {(ai, Vbai), i = 1, … nk}, where ai is the age of the subject at the i-th radiograph, Vbai is the corresponding Vba value, and nk is the number of radiographs of the k-th subject.
Since our model allowed us to estimate the beginning of the pubertal spurt, τ1, and the corresponding Vba value, Vba1, we can consider η1 = min {Vbai: Vbai ≥ v}, i.e., the first radiograph of the subject with Vba value greater than Vba1, and t1, the corresponding age of the subject. Subsequently, we evaluated the residual proportion of maturation of the C4 vertebral body θk = Vba2 − η1, and Δτ, the time elapsed from η1 to Vba2.
Finally, we estimated the expected age for the end of the spurt, t2 = t1 + Δτ, for the k-th subject, the value α = min {ai: ai ≥ t2, i = 1, … nk} and η2, the corresponding Vba value obtained using equation (1): η2 = Vba(α).
If η2 belonged to the 95% CI for Vba2, the forecast of the expected end of the pubertal spurt for the k-th subject was considered correct (C). If η2 resulted in less than the lower limit of the 95% CI for Vba2, but the next observed Vba value of the subject, say η3, belonged to the 95% CI for Vba2, the forecast was considered slightly underestimated (U). If none of the above conditions was verified, the estimate was considered an incorrect forecast (I). Statistical analyses were performed with the R statistical program [54].
3. Results
There were no statistically significant intra-observer differences between paired sets of measurements on re-examined lateral cephalograms, ICC = 0.97 (95%CI, 0.95–0.98). A similar result was obtained considering the agreement between the two observers, ICC = 0.93 (95%CI, 0.89–0.96).
The parameter estimates of the segmented model used to fit the data for both males and females are listed in Table 1, with their standard errors.

Table 1.
Parameter estimates of the segmented regression model (1) were used to fit the data separately for males and females.
The segmented regression equations explained 73% and 86% of the total variance of Vba for males and females, respectively.
For males, the two breakpoints, characterizing the higher pubertal development rate, lasted for 1.71 years with a Vba increasing rate (slope of the curve) of 0.169 years−1 (se = 0.029 years−1), Figure 3. The values of Vba corresponding to the beginning and the end of the growth spurt were Vba1 = 0.676 (95%CI, 0.642–0.711) and Vba2 = 0.966 (95%CI, 0.905–1.028).
For females, the two breakpoints, characterizing the higher pubertal development rate, lasted for 3.76 years with a Vba increasing rate (slope of the curve) of 0.114 years−1 (se = 0.007 years). The values of Vba, corresponding to the beginning and end of the higher pubertal development rate, were Vba1 = 0.658 (95%CI, 0.634–0.682) and Vba2 = 1.073 (95%CI, 1.044–1.101) respectively. Table 2 reported, for some different values of Vba, the corresponding median values of θ (%) and the median of the time elapsed to the end of the pubertal spurt Δτ (years) with the first and third quartile of its distribution.
Table 2.
Median, first, and third quartile of the distribution of the residual proportion of the maturation, θ (%), and the time elapsed to the end of the pubertal spurt, Δτ (years), for the given ratio of projections of the anterior and posterior heights of the C4 vertebral body (Vba) in males and females.
The results of the validation process are synthesized in Table 3. It shows that our model did not produce any incorrect forecast. Furthermore, although the difference between males and females is not statistically significant, the number of correct forecasts in sampled males is almost twice that of females.
Table 3.
The frequency distribution of the forecasts of the expected end of the spurt periods using regression model (1) for the 50 subjects belongs to the Michigan Growth Center.
4. Discussion
In our study, we analyzed the ratio of the anterior and posterior sides of C4 (Vba), and our findings showed the variability of time and the incremental span of Vba in the circumpubertal period of life. Therefore, we hypothesized that this incremental span of Vba was a potential indicator of the beginning and the end of the pubertal growth spurt and skeletal development.
Segmental regression analysis detected specific Vba values at the beginning and the end of the pubertal growth spurt in males and females, which also determined the specific age interval of the spurt in the tested population. The spurt began at nine years and three months old in females and was ahead of males for over four months. The mean ending of the spurt was at twelve years and nine months and was delayed in males for over fourteen months. Different regression models, Bayesian approach, and response surface methodology with statistical potentials in other topics may be a potential statistical tool for fitting an assumed experimental model to data obtained under the chosen design [7,55,56,57,58,59].
One of the limitations of qualitative vertebral cervical methods is identifying the different stages or shapes. Nestman et al. [60] studied CVM reproducibility and observed poor concordance and difficulties in classifying the shapes of C3 and C4 vertebral bodies as trapezoidal, rectangular horizontal, square, or rectangular vertical. Because of those difficulties, the method’s reproducibility was tested for clinical use in determining the timing of orthodontic treatment. However, Perinetti et al. [61] reported that visual assessment of CVM appears accurate and repeatable, but stages 4 and 5 require a more careful evaluation. Furthermore, in a systematic review of the reliability of the CVM method to predict pubertal spurt, the authors concluded that although there was a good correlation between hand–wrist and CVM methods, there was a low level of evidence. Therefore, the reliability of the method remained uncertain [62].
The previous observations suggest the need for improvement of current methods by using a different approach that relies more on quantitative measurements rather than comparison based on stages. For example, when comparing Vba visually to the CVM stages, it is possible to observe that Vba values close to Vba1 correspond to a trapezoidal shape or CVMS II, while Vba values of Vba2 or close to 1.00 are more rectangular and, therefore, similar to CVM III. However, the CVM and Cervical Vertebral Maturation Stage (CVMS) methods can only show the stage of the evaluated patient.
The studies that have observed the morphological changes of the cervical vertebral bodies during growth from lateral cephalograms describe a consistent shift from a trapezoidal shape in the initial stages of maturation to a more rectangular shape related to the final stages of maturation [16,17]. Such variations in cervical vertebral body shapes suggest a relationship between the proportions of the posterior and anterior sides of the cervical bodies and the beginning and end of the pubertal growth spurt; the C4 vertebral body was chosen because it is usually clearly visible in the lateral cephalograms. Björk and Helm investigated the age at maximum height growth at puberty in Danish children to determine whether the maximal growth spurt had been reached or passed. They compared the maximum increase in height with age at ossification of the sesamoid of the thumb, and menarche, two specific stages of tooth development: all canines and premolars fully erupted, and all second molars fully erupted. They showed that the maximum growth in height was 18 ± 3.0 months and ossification of the ulnar sesamoid of the thumb 21 ± 3.0 months ahead in girls compared to boys. The gender difference in tooth development was significantly smaller, with the full eruption of the occlusal level of the canines and premolars being attained only 2 ± 5.2 months earlier in girls, while the full eruption of the second molars was earlier in girls by 6 ± 4.7 months. The ulnar sesamoid of the thumb was ossified by an average of 12 months before maximum pubertal growth in females and nine months before in males and preceded or coincided with maximum pubertal growth for both sexes.
From a clinical perspective, it would be helpful to obtain more precise information on the residual amount of growth just by calculating an easy-to-measure single variable such as Vba since this was not possible with current CVM or CVMS methods. Furthermore, our intra-observer and inter-observer reliability results show excellent concordance due to the ease of measuring precise and visible projections and calculating their proportion, making the method straightforward and practical.
The possible application of dental development analysis to assess pubertal growth spurt compared to skeletal development was compared by Bittencourt et al. [31] in a systematic review and meta-analysis. In the analyzed articles, the authors used skeletal methods according to Greulich-Pyle and Fishman and dental methods according to Nolla, Demirjian, and Moorrees [25]. Half of the research in the meta-analysis indicates a strong correlation between tooth development and skeletal development, identifying the lower canine as the tooth that correlates the most with skeletal development. However, they pragmatically concluded that it is not possible to assess pubertal growth spurt by tooth development [31].
For orthodontic clinicians, the measurements of the posterior and anterior projections of body heights from C4 vertebrae and their ratio Vba would allow them to estimate the amount of time remaining for the growth spurt to occur or to determine if it has already passed. However, similar to other growth indicators, it must be used considering the individual variations and using additional information since no method has complete diagnostic reliability in identifying the pubertal growth spurt [27,45,63].
The longitudinal sample of cephalograms taken from the Michigan Growth Center to test the method presented positive results showing no incorrect predictions. However, it suggests that future studies should verify them using a larger sample of longitudinal data with the Vba measurement and evaluate the method and its specific cut-offs of Vba with other skeletal methods on different samples to test its applicability in clinical practice.
5. Conclusions
This study analyzed the ratio of the anterior height projection to the posterior of the C4 vertebral body or Vba during childhood, where preadolescence and adolescence occurred, and proved the applicability of Vba for estimating the beginning and end of the pubertal growth spurt and in a specific population. Based on the observations, the proposed method estimated the starting cut-off value of Vba, Vba1, and the ending cut-off value, Vba2, of the higher pubertal development rate and the residual proportion of Vba of C4 maturation, θ (%), with their standard errors.
The specific results suggest that the cut-off value of Vba breakpoints and θ (%) need to be validated on other available C4 samples of different ethnic and geographical specificities.
Author Contributions
Conceptualization, R.C., I.G. and L.F.; methodology, L.F., E.N. and D.K.G.; statistics, L.F.; validation, L.A.V.P. and L.J.; writing—original draft preparation, E.N., I.G., D.J. and L.A.V.P.; writing—reviewing and editing, I.G., L.A.V.P. and H.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Croatian Science Foundation, grant number IP-2020-02-9423.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. An improved version of the cervical vertebral maturation (CVM) method for the assessment of mandibular growth. Angle Orthod. 2002, 72, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. Treatment and posttreatment craniofacial changes after rapid maxillary expansion and facemask therapy. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Ball, G.; Woodside, D.; Tompson, B.; Hunter, W.S.; Posluns, J. Relationship between cervical vertebral maturation and mandibular growth. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e455–e461. [Google Scholar] [CrossRef]
- Björk, A.; Krebs, A.; Solow, B. A method for epidemiological registration of malocclusion. Acta Odontol. Scand. 1964, 22, 27–41. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.T.; Yanniello, G.J. Mandibular growth changes and maturation of cervical vertebrae—A longitudinal cephalometric study. Angle Orthod. 1988, 58, 179–184. [Google Scholar] [CrossRef]
- So, L.L. Skeletal maturation of the hand and wrist and its correlation with dental development. Aust. Orthod. J. 1997, 15, 1–9. [Google Scholar]
- Yuan, J.T.; Furdock, R.J.; Benedick, A.; Liu, R.W. Estimating Skeletal Maturity by Segmented Linear Modeling of Key AP Knee Radiographic Parameters. J. Pediatr. Orthop. 2022, 42, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Sahin, R.; Kazadal, C. The Relationship Between Ossification in Metacarpophalangeal Sesamoids of the Thumb and the Period of Puberty: A Radiographic Study. Medeni. Med. J. 2022, 37, 300–305. [Google Scholar] [CrossRef]
- Paschoini, V.L.; Nunes, D.C.; Matias, M.; Nahás-Scocate, A.C.R.; Feres, M.F.N. Accuracy of dental calcification stages for the identification of craniofacial pubertal growth spurt: Proposal of referral parameters. Eur. Arch. Paediatr. Dent. 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Szemraj-Folmer, A.; Wojtaszek-Słomińska, A.; Racka-Pilszak, B.; Kuc-Michalska, M. Assessment of the duration of the pubertal growth spurt in patients with skeletal open bite: A cross-sectional study. J. Orofac. Orthop. 2021, 82, 92–98. [Google Scholar] [CrossRef]
- Al Khal, H.A.; Wong, R.W.; Rabie, A.B. Elimination of hand-wrist radiographs for maturity assessment in children needing orthodontic therapy. Skelet. Radiol. 2008, 37, 195–200. [Google Scholar] [CrossRef]
- Hagg, U.; Taranger, J. Skeletal stages of the hand and wrist as indicators of the pubertal growth spurt. Acta Odontol. Scand. 1980, 38, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, P.S.; Mosdol, A.; Ding, Y.; Bleka, O.; Rolseth, V.; Straumann, G.H.; Skjerven-Martinsen, M.; Delaveris, G.J.M.; Vist, G.E. A systematic review of the agreement between chronological age and skeletal age based on the Greulich and Pyle atlas. Eur. Radiol. 2019, 29, 2936–2948. [Google Scholar] [CrossRef]
- Bjork, A.; Helm, S. Prediction of the age of maximum puberal growth in body height. Angle Orthod. 1967, 37, 134–143. [Google Scholar] [CrossRef]
- Fekonja, A. Evaluation of the eruption of permanent teeth and their association with malocclusion. Clin. Exp. Dent. Res. 2022, 8, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Fishman, L.S. Maturational patterns and prediction during adolescence. Angle Orthod. 1987, 57, 178–193. [Google Scholar] [CrossRef] [PubMed]
- Lamparski, D.G. Skeletal age assessment utilizing cervical vertebrae. Am. J. Orthod. 1975, 67, 458–459. [Google Scholar] [CrossRef]
- Hassel, B.; Farman, A.G. Skeletal maturation evaluation using cervical vertebrae. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 58–66. [Google Scholar] [CrossRef]
- Franchi, L.; Baccetti, T.; McNamara, J.A., Jr. Mandibular growth as related to cervical vertebral maturation and body height. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 335–340. [Google Scholar] [CrossRef]
- Thomas, L.A.; Thomas, L.R.; Balla, S.B.; Gopalaiah, H.; Kanaparthi, A.; Sai Sravanthi, G.; Palla, A.; Galic, I. Above or below 14 years? An orthopantomographic study based on chronological course of eruption of mandibular premolars and second molars in a sample of south Indian children. Leg. Med. 2021, 48, 101814. [Google Scholar] [CrossRef] [PubMed]
- Kelmendi, J.; Cameriere, R.; Kocani, F.; Galic, I.; Mehmeti, B.; Vodanovic, M. The third molar maturity index in indicating the legal adult age in Kosovar population. Int. J. Leg. Med. 2018, 132, 1151–1159. [Google Scholar] [CrossRef]
- Rozylo-Kalinowska, I.; Kalinowski, P.; Kozek, M.; Galic, I.; Cameriere, R. Validity of the third molar maturity index I(3M) for indicating the adult age in the Polish population. Forensic Sci. Int. 2018, 290, 352.e1–352.e6. [Google Scholar] [CrossRef] [PubMed]
- Balla, S.B.; Banda, T.R.; Galic, I.; Naga, N.M.; Naishadham, P.P. Validation of Cameriere’s third molar maturity index alone and in combination with apical maturity of permanent mandibular second molar for indicating legal age of 14 years in a sample of South Indian children. Forensic Sci. Int. 2019, 297, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Balla, S.B.; Chinni, S.S.; Galic, I.; Alwala, A.M.; Machani, P.; Cameriere, R. A cut-off value of third molar maturity index for indicating a minimum age of criminal responsibility: Older or younger than 16 years? J. Forensic Leg. Med. 2019, 65, 108–112. [Google Scholar] [CrossRef] [PubMed]
- da Luz, L.C.P.; Anzulovic, D.; Benedicto, E.N.; Galic, I.; Brkic, H.; Biazevic, M.G.H. Accuracy of four dental age estimation methodologies in Brazilian and Croatian children. Sci. Justice 2019, 59, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Galic, I.; Pacifici, A.; Carbone, D.; Pacifici, L.; Jeroncic, A.; Cameriere, R. Age estimation by the Cameriere’s normalized measurements (CNM) of the single permanent mandibular tooth on a panoramic radiograph. Leg. Med. 2017, 26, 65–72. [Google Scholar] [CrossRef]
- Brkic, H.; Galic, I.; Vodanovic, M.; Dumancic, J.; Mehdi, F.; Anic Milosevic, S. The Cameriere, Haavikko, Demirjian, and Willems methods for the assessment of dental age in Croatian children. Int. J. Leg. Med. 2022, 136, 1685–1696. [Google Scholar] [CrossRef] [PubMed]
- Galic, I.; Vodanovic, M.; Jankovic, S.; Mihanovic, F.; Nakas, E.; Prohic, S.; Galic, E.; Brkic, H. Dental age estimation on Bosnian-Herzegovinian children aged 6–14 years: Evaluation of Chaillet’s international maturity standards. J. Forensic Leg. Med. 2013, 20, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Galic, I.; Vodanovic, M.; Cameriere, R.; Nakas, E.; Galic, E.; Selimovic, E.; Brkic, H. Accuracy of Cameriere, Haavikko, and Willems radiographic methods on age estimation on Bosnian-Herzegovian children age groups 6–13. Int. J. Leg. Med. 2011, 125, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Dadgar, S.; Hadian, H.; Ghobadi, M.; Sobouti, F.; Rakhshan, V. Correlations among chronological age, cervical vertebral maturation index, and Demirjian developmental stage of the maxillary and mandibular canines and second molars. Surg. Radiol. Anat. 2021, 43, 131–143. [Google Scholar] [CrossRef]
- Bittencourt, M.V.; Cericato, G.; Franco, A.; Girão, R.; Lima, A.P.B.; Paranhos, L. Accuracy of dental development for estimating the pubertal growth spurt in comparison to skeletal development: A systematic review and meta-analysis. Dentomaxillofac. Radiol. 2018, 47, 20170362. [Google Scholar] [CrossRef] [PubMed]
- Wittschieber, D.; Vieth, V.; Wierer, T.; Pfeiffer, H.; Schmeling, A. Cameriere’s approach modified for pelvic radiographs: A novel method to assess apophyseal iliac crest ossification for the purpose of forensic age diagnostics. Int. J. Leg. Med. 2013, 127, 825–829. [Google Scholar] [CrossRef]
- Cameriere, R.; Brogi, G.; Ferrante, L.; Mirtella, D.; Vultaggio, C.; Cingolani, M.; Fornaciari, G. Reliability in age determination by pulp/tooth ratio in upper canines in skeletal remains. J. Forensic Sci. 2006, 51, 861–864. [Google Scholar] [CrossRef]
- Cameriere, R.; Cingolani, M.; Giuliodori, A.; De Luca, S.; Ferrante, L. Radiographic analysis of epiphyseal fusion at knee joint to assess likelihood of having attained 18 years of age. Int. J. Leg. Med. 2012, 126, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Cameriere, R.; Cunha, E.; Wasterlain, S.N.; De Luca, S.; Sassaroli, E.; Pagliara, F.; Nuzzolese, E.; Cingolani, M.; Ferrante, L. Age estimation by pulp/tooth ratio in lateral and central incisors by peri-apical X-ray. J. Forensic Leg. Med. 2013, 20, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Cameriere, R.; De Angelis, D.; Ferrante, L.; Scarpino, F.; Cingolani, M. Age estimation in children by measurement of open apices in teeth: A European formula. Int. J. Leg. Med. 2007, 121, 449–453. [Google Scholar] [CrossRef]
- Cameriere, R.; Ferrante, L.; Cingolani, M. Age estimation in children by measurement of open apices in teeth. Int. J. Leg. Med. 2006, 120, 49–52. [Google Scholar] [CrossRef]
- Cameriere, R.; Ferrante, L.; De Angelis, D.; Scarpino, F.; Galli, F. The comparison between measurement of open apices of third molars and Demirjian stages to test chronological age of over 18 year olds in living subjects. Int. J. Leg. Med. 2008, 122, 493–497. [Google Scholar] [CrossRef]
- Cameriere, R.; Ferrante, L.; Mirtella, D.; Cingolani, M. Carpals and epiphyses of radius and ulna as age indicators. Int. J. Leg. Med. 2006, 120, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Cameriere, R.; Giuliodori, A.; Zampi, M.; Galic, I.; Cingolani, M.; Pagliara, F.; Ferrante, L. Age estimation in children and young adolescents for forensic purposes using fourth cervical vertebra (C4). Int. J. Leg. Med. 2015, 129, 347–355. [Google Scholar] [CrossRef]
- Cameriere, R.; Scendoni, R.; Ferrante, L.; Mirtella, D.; Oncini, L.; Cingolani, M. An Effective Model for Estimating Age in Unaccompanied Minors under the Italian Legal System. Healthcare 2023, 11, 224. [Google Scholar] [CrossRef]
- Zolotenkova, G.V.; Rogachev, A.I.; Pigolkin, Y.I.; Edelev, I.S.; Borshchevskaya, V.N.; Cameriere, R. Age Classification in Forensic Medicine Using Machine Learning Techniques. Sovrem. Tekhnol. V Meditsine 2022, 14, 15–22. [Google Scholar] [CrossRef]
- Spinas, E.; Melis, G.; Zerman, N.; De Luca, S.; Cameriere, R. Age Assessment in Children and Adolescents by Measuring the Open Apices in Teeth: A New Sardinian Formula. Dent. J. 2022, 10, 50. [Google Scholar] [CrossRef]
- Scendoni, R.; Ribeiro, I.L.A.; Cingolani, M.; Giovagnoni, A.; Curzi, M.; Fedeli, P.; Cameriere, R. A new analytical cut-off point for determining 18 years of age using MRI on medial clavicular epiphysis. Leg. Med. 2022, 54, 102010. [Google Scholar] [CrossRef]
- Pereira, C.P.; Belo, C.; Sardinha, J.; Santos, R.; Salvado, F.; Cameriere, R. Quantitative and Qualitative Approaches for Dental Age Assessment in Sub Adult Portuguese Population: European Regression Formula and Demirjian Stages. Acta Stomatol. Croat. 2022, 56, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Kihara, E.; Galic, I.; Nyamunga, D.; Mehdi, F.; Velandia Palacio, L.A.; Cameriere, R. Validation of the Italian, European, North German, Malaysian, and South African black formulas on Cameriere method using panoramic radiographs in Kenyan children. Int. J. Leg. Med. 2022, 136, 1495–1506. [Google Scholar] [CrossRef]
- Angelakopoulos, N.; De Luca, S.; Oliveira-Santos, I.; Ribeiro, I.L.A.; Bianchi, I.; Balla, S.B.; Kis, H.C.; Jimenez, L.G.; Zolotenkova, G.; Yusof, M.Y.P.; et al. Third molar maturity index (I(3M)) assessment according to different geographical zones: A large multi-ethnic study sample. Int. J. Leg. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Palmela Pereira, C.; Rodrigues, A.; Santos, A.; Salvado, F.; Santos, R.; Cameriere, R. Cut-off for the legal ages in the Portuguese Population by Third Maturity Index: Measures of Accuracy. Arch. Oral Biol. 2021, 125, 105089. [Google Scholar] [CrossRef]
- Angelakopoulos, N.; Galic, I.; Balla, S.B.; Kis, H.C.; Gomez Jimenez, L.; Zolotenkova, G.; Mohd Yusof, M.Y.P.; Hadzic Selmanagic, A.; Pandey, H.; Palmela Pereira, C.; et al. Comparison of the third molar maturity index (I(3M)) between left and right lower third molars to assess the age of majority: A multi-ethnic study sample. Int. J. Leg. Med. 2021, 135, 2423–2436. [Google Scholar] [CrossRef]
- Gulsahi, A.; Cehreli, S.B.; Galic, I.; Ferrante, L.; Cameriere, R. Age estimation in Turkish children and young adolescents using fourth cervical vertebra. Int. J. Leg. Med. 2020, 134, 1823–1829. [Google Scholar] [CrossRef] [PubMed]
- World Medical, A. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Ferrante, L.; Cameriere, R. Statistical methods to assess the reliability of measurements in the procedures for forensic age estimation. Int. J. Leg. Med. 2009, 123, 277–283. [Google Scholar] [CrossRef]
- Muggeo, V.M. Estimating regression models with unknown break-points. Stat. Med. 2003, 22, 3055–3071. [Google Scholar] [CrossRef]
- R Core Team R. R: A Language and Environment for Statistical Computing; R Core Team R.: Vienna, Austria, 2020. [Google Scholar]
- Sodeifian, G.; Ansari, K. Optimization of Ferulago Angulata oil extraction with supercritical carbon dioxide. J. Supercrit. Fluids 2011, 57, 38–43. [Google Scholar] [CrossRef]
- Sodeifian, G.; Ardestani, N.S.; Sajadian, S.A.; Ghorbandoost, S. Application of supercritical carbon dioxide to extract essential oil from Cleome coluteoides Boiss: Experimental, response surface and grey wolf optimization methodology. J. Supercrit. Fluids 2016, 114, 55–63. [Google Scholar] [CrossRef]
- Faragalli, A.; Skrami, E.; Bucci, A.; Gesuita, R.; Cameriere, R.; Carle, F.; Ferrante, L. Combining Bayesian Calibration and Copula Models for Age Estimation. Int. J. Environ. Res. Public Health 2023, 20, 1201. [Google Scholar] [CrossRef]
- Cameriere, R.; De Luca, S.; Soriano Vazquez, I.; Kis, H.C.; Pigolkin, Y.; Kumagai, A.; Ferrante, L. A full Bayesian calibration model for assessing age in adults by means of pulp/tooth area ratio in periapical radiography. Int. J. Leg. Med. 2021, 135, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, L.; Skrami, E.; Gesuita, R.; Cameriere, R. Bayesian calibration for forensic age estimation. Stat. Med. 2015, 34, 1779–1790. [Google Scholar] [CrossRef]
- Nestman, T.S.; Marshall, S.D.; Qian, F.; Holton, N.; Franciscus, R.G.; Southard, T.E. Cervical vertebrae maturation method morphologic criteria: Poor reproducibility. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 182–188. [Google Scholar] [CrossRef]
- Perinetti, G.; Perillo, L.; Franchi, L.; Di Lenarda, R.; Contardo, L. Maturation of the middle phalanx of the third finger and cervical vertebrae: A comparative and diagnostic agreement study. Orthod. Craniofac. Res. 2014, 17, 270–279. [Google Scholar] [CrossRef]
- Santiago, R.C.; de Miranda Costa, L.F.; Vitral, R.W.; Fraga, M.R.; Bolognese, A.M.; Maia, L.C. Cervical vertebral maturation as a biologic indicator of skeletal maturity. Angle Orthod. 2012, 82, 1123–1131. [Google Scholar] [CrossRef]
- Perinetti, G.; Contardo, L. Reliability of Growth Indicators and Efficiency of Functional Treatment for Skeletal Class II Malocclusion: Current Evidence and Controversies. BioMed Res. Int. 2017, 2017, 1367691. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).