
Body Height Trajectories in Pediatric Competitive Athletes from 46 Different Sport Types

 , and
, and
Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; U.S. Department of Health and Human Services: Washington, DC, USA, 2018; Part F, Chapter 7. Youth. Available online: https://health.gov/sites/default/files/2019-09/13_F-7_Youth.pdf (accessed on 22 April 2022).
- Logan, K.; Cuff, S.; Council on Sports Medicine And Fitness; LaBella, C.R.; Brooks, M.A.; Canty, G.; Diamond, A.B.; Hennrikus, W.; Moffatt, K.; Nemeth, B.A.; et al. Organized sports for children, preadolescents, and adolescents. Pediatrics 2019, 143, e20190997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgopoulos, N.A.; Roupas, N.D.; Theodoropoulou, A.; Tsekouras, A.; Vagenakis, A.G.; Markou, K.B. The influence of intensive physical training on growth and pubertal development in athletes. Ann. N. Y. Acad. Sci. 2010, 1205, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M. Physical activity and training: Effects on stature and the adolescent growth spurt. Med. Sci. Sports Exerc. 1994, 26, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Theintz, G.E.; Howald, H.; Weiss, U.; Sizonenko, P.C. Evidence for a reduction of growth potential in adolescent female gymnasts. J. Pediatr. 1993, 122, 306–313. [Google Scholar] [CrossRef]
- Georgopoulos, N.A.; Theodoropoulou, A.; Roupas, N.D.; Armeni, A.K.; Koukkou, E.; Leglise, M.; Markou, K.B. Final height in elite male artistic gymnasts. J. Pediatr. Endocrinol. Metab. 2012, 25, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Erlandson, M.C.; Sherar, L.B.; Mirwald, R.L.; Maffulli, N.; Baxter-Jones, A.D.G. Growth and Maturation of Adolescent Female Gymnasts, Swimmers, and Tennis Players. Med. Sci. Sports Exerc. 2008, 40, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Caine, D.; Lewis, R.; O’Connor, P.; Howe, W.; Bass, S. Does gymnastics training inhibit growth of females? Clin. J. Sport Med. 2001, 11, 260–270. [Google Scholar] [CrossRef]
- Malina, R.M.; Baxter-Jones, A.D.G.; Armstrong, N.; Beunen, G.P.; Caine, D.; Daly, R.M.; Lewis, R.D.; Rogol, A.D.; Russell, K. Role of Intensive Training in the Growth and Maturation of Artistic Gymnasts. Sports Med. 2013, 43, 783–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pişkin, İ.E.; Gümüş, M.; Bayraktaroğlu, T.; Akalin, T.C.; Yamaner, F. Growth and pubertal development in adolescent male wrestlers. J. Sports Med. Phys. Fit. 2018, 58, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Matthews, B.L.; Bennell, K.; McKay, H.A.; Khan, K.M.; Baxter-Jones, A.D.G.; Mirwald, R.L.; Wark, J.D. The influence of dance training on growth and maturation of young females: A mixed longitudinal study. Ann. Hum. Biol. 2006, 33, 342–356. [Google Scholar] [CrossRef] [PubMed]
- Eisenmann, J.C.; Malina, R.M. Growth Status and Estimated Growth Rate of Young Distance Runners. Int. J. Sports Med. 2002, 23, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Mei, Z.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. CDC growth charts: United States. Adv. Data 2000, 314, 1–27. [Google Scholar]
- Goldstein, A.; Haelyon, U.; Krolik, E.; Sack, J. Comparison of Body Weight and Height of Israeli Schoolchildren with the Tanner and Centers for Disease Control and Prevention Growth Charts. Pediatrics 2001, 108, e108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butte, N.F.; Watson, K.B.; Ridley, K.; Zakeri, I.F.; Mcmurray, R.G.; Pfeiffer, K.A.; Crouter, S.E.; Herrmann, S.D.; Bassett, D.R.; Long, A.; et al. A youth compendium of physical activities: Activity codes and metabolic intensities. Med. Sci. Sports Exerc. 2018, 50, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Leek, D.; Carlson, J.A.; Cain, K.L.; Henrichon, S.; Rosenberg, D.; Patrick, K.; Sallis, J.F. Physical Activity During Youth Sports Practices. Arch. Pediatr. Adolesc. Med. 2011, 165, 294–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.; Berdel, D.; Nowak, D.; Heinrich, J.; Schulz, H. Sport Engagement by Accelerometry under Field Conditions in German Adolescents: Results from GINIPlus. PLoS ONE 2015, 10, e0135630. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Dos-Santos, M.R.; Lynch, K.R.; Agostinete, R.R.; Maillane-Vanegas, S.; Turi-Lynch, B.; Ito, I.H.; Luiz-De-Marco, R.; Rodrigues-Junior, M.A.; Fernandes, R.A. Prolonged Practice of Swimming Is Negatively Related to Bone Mineral Density Gains in Adolescents. J. Bone Metab. 2016, 23, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Krabak, B.J.; Roberts, W.O.; Tenforde, A.S.; Ackerman, E.K.; Adami, P.E.; Baggish, A.L.; Barrack, M.; Cianca, J.; Davis, I.; D’Hemecourt, P.; et al. Youth running consensus statement: Minimising risk of injury and illness in youth runners. Br. J. Sports Med. 2020, 55, 305–318. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| All Cohort (n = 2276) | Recurring Participants (n = 688) | |
|---|---|---|
| Age at first measurement (years) | 12.3 ± 2.6 | 11.4 ± 2.4 |
| Percent males | 71.3% | 70.9% |
| Height (cm) | 153 ± 16 | 149 ± 16 |
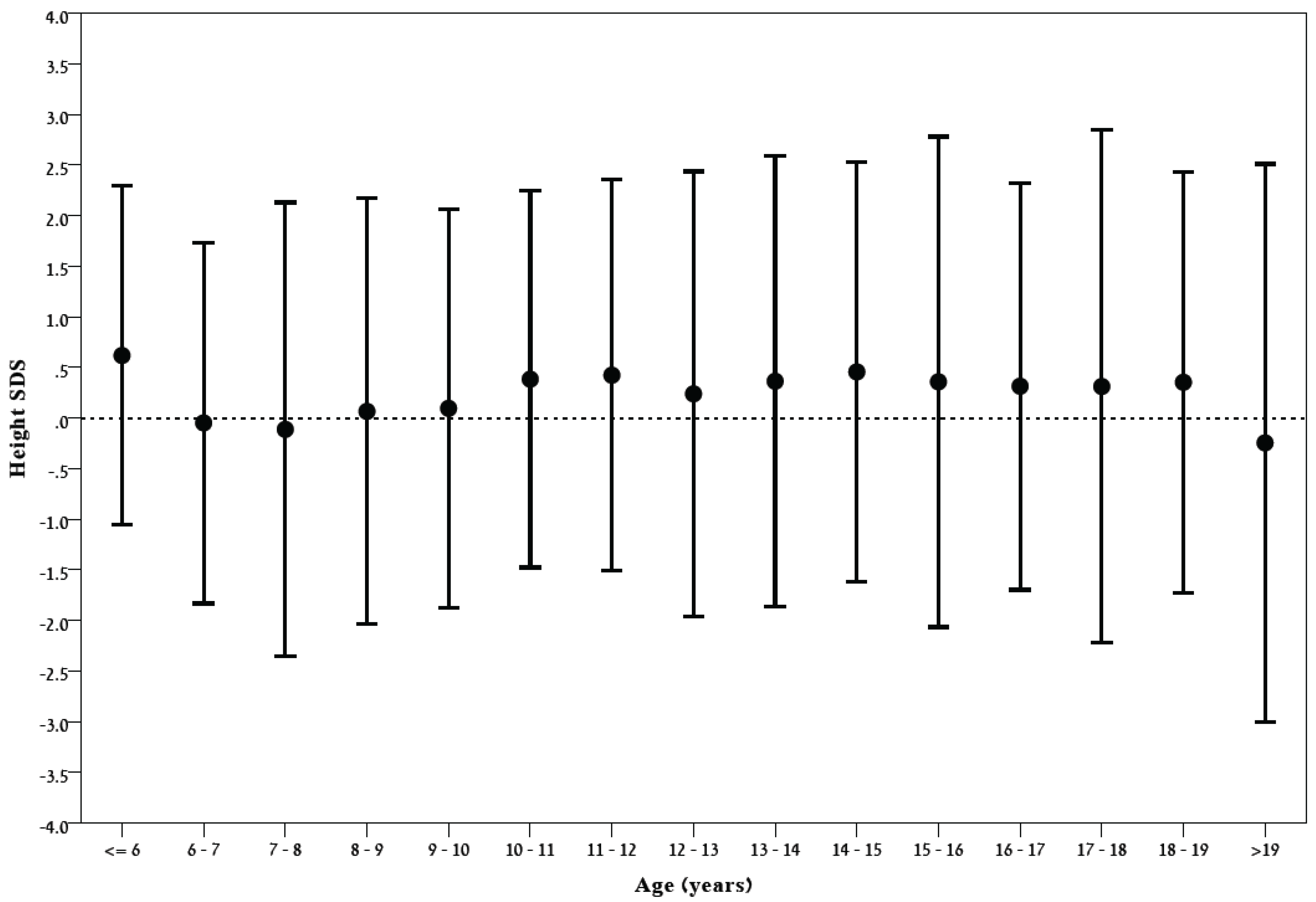
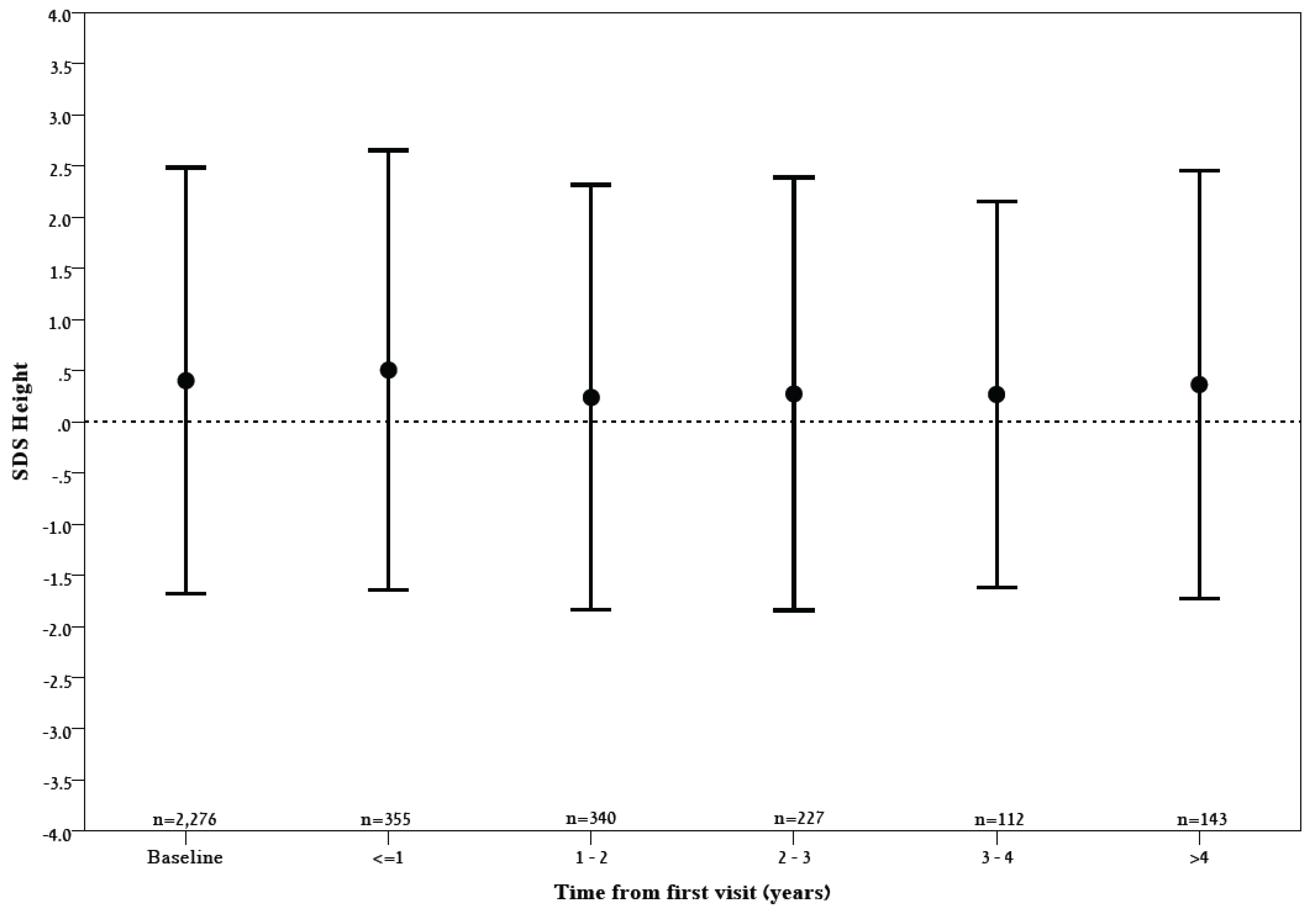
| Height SDS | 0.30 ± 1.05 * | 0.40 ± 1.04 * |
| BMI (kg/m2) | 19.3 ± 3.7 | 18.6 ± 3.1 |
| BMI SDS | 0.17 ± 0.97 * | 0.18 ± 0.94 * |
| Sport Type | Number of Participants | Baseline Height SDS (Mean ± SD) | Number of Measurements | B | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|---|
| Swimming | 61 (55% males) | 0.650 ± 0.821 | 181 | −0.126 | −0.186–−0.065 | <0.001 |
| Cycling | 51 (57% males) | 0.067 ± 1.143 | 116 | −0.228 | −0.371–−0.085 | 0.002 |
| Triathlon | 83 (66% males) | 0.164 ± 0.899 | 244 | −0.119 | −0.225–−0.012 | 0.029 |
| Gymnastics | 58 (12% males) | −0.533 ± 0.780 | 161 | −0.055 | −0.128–0.017 | 0.132 |
| Tennis | 82 (72% males) | 0.395 ± 0.948 | 231 | 0.061 | −0.034–0.156 | 0.209 |
| Basketball | 158 (100% males) | 0.976 ± 1.02 | 384 | 0.032 | −0.037–0.101 | 0.359 |
| Football | 24 (90% males) | 0.103 ± 0.894 | 61 | −0.058 | −0.151–0.035 | 0.221 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Efrati, R.; Leib, S.; Rimon, A.; Gelbart, M.; Yarom, Y.; Ziv-Baran, T.; Dubnov-Raz, G. Body Height Trajectories in Pediatric Competitive Athletes from 46 Different Sport Types. Appl. Sci. 2022, 12, 5033. https://doi.org/10.3390/app12105033
Efrati R, Leib S, Rimon A, Gelbart M, Yarom Y, Ziv-Baran T, Dubnov-Raz G. Body Height Trajectories in Pediatric Competitive Athletes from 46 Different Sport Types. Applied Sciences. 2022; 12(10):5033. https://doi.org/10.3390/app12105033
Chicago/Turabian StyleEfrati, Ran, Shiran Leib, Amir Rimon, Miri Gelbart, Yoni Yarom, Tomer Ziv-Baran, and Gal Dubnov-Raz. 2022. "Body Height Trajectories in Pediatric Competitive Athletes from 46 Different Sport Types" Applied Sciences 12, no. 10: 5033. https://doi.org/10.3390/app12105033
APA StyleEfrati, R., Leib, S., Rimon, A., Gelbart, M., Yarom, Y., Ziv-Baran, T., & Dubnov-Raz, G. (2022). Body Height Trajectories in Pediatric Competitive Athletes from 46 Different Sport Types. Applied Sciences, 12(10), 5033. https://doi.org/10.3390/app12105033