
Prevalence of JP2 and Non-JP2 Genotypes of Aggregatibacter actinomycetemcomitans and Oral Hygiene Practice of Kenyan Adolescents in Maasai Mara

 , ,
, , 
Abstract
1. Introduction
2. Results
2.1. Number of Maxillary and Mandibular Teeth Present in the Oral Cavity of Kenyan Adolescents
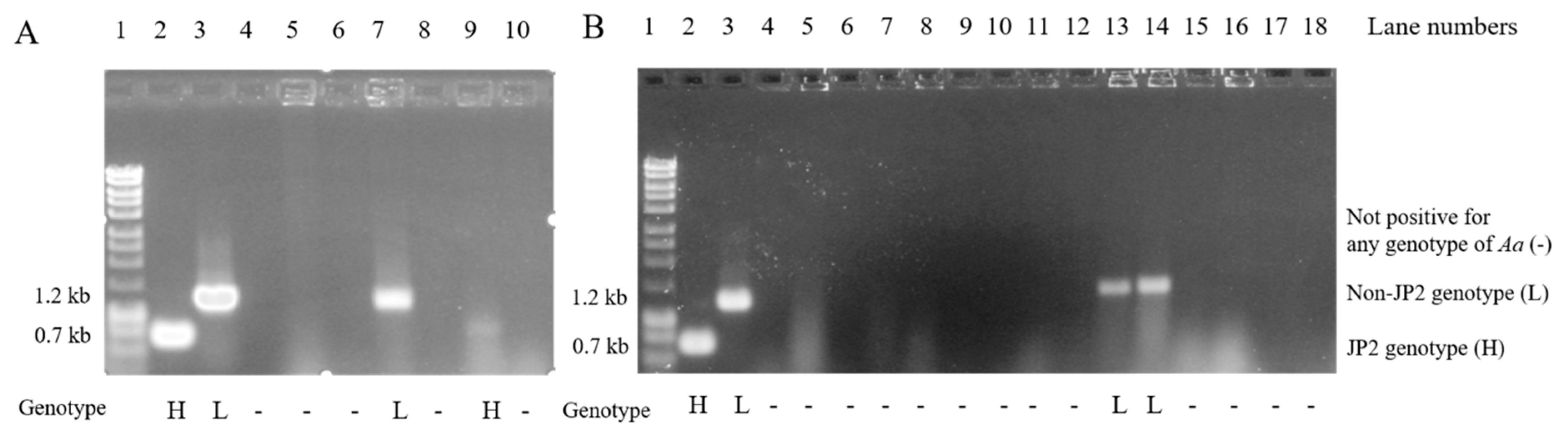
2.2. Prevalence of JP2 and Non-JP2 Genotypes of A. actinomycetemcomitans Among Adolescents Living in Maasai Mara
2.3. Answers to Questions on Oral Hygiene Tools and Hygiene Practices Used
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Face-to-Face Interview
4.3. Recording of the Presence of Maxillary and Mandibular Teeth in the Mouth
4.4. Procedure for Collecting and Analyzing Dental Plaque Samples
4.5. Data analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Baelum, V.; Scheutz, F. Periodontal diseases in Africa. Periodontology 2000 2002, 29, 79–103. [Google Scholar] [CrossRef] [PubMed]
- Haubek, D.; Ennibi, O.K.; Poulsen, K.; Vaeth, M.; Poulsen, S.; Kilian, M. Risk of aggressive periodontitis in adolescent carriers of the JP2 clone of Aggregatibacter (Actinobacillus) actinomycetemcomitans in Morocco: A prospective longitudinal cohort study. Lancet 2008, 371, 237–242. [Google Scholar] [CrossRef]
- Baelum, V.; Fejerskov, O.; Manji, F. Periodontal diseases in adult Kenyans. J. Clin. Periodontol. 1988, 15, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Höglund Åberg, C.; Kwamin, F.; Claesson, R.; Dahlen, G.; Johansson, A.; Haubek, D. Progression of attachment loss is strongly associated with presence of the JP2 genotype of Aggregatibacter actinomycetemcomitans: A prospective cohort study of a young adolescent population. J. Clin. Periodontol. 2014, 41, 232–241. [Google Scholar] [CrossRef]
- Bouziane, A.; Hamdoun, R.; Abouqal, R.; Ennibi, O. Global prevalence of aggressive periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 406–428. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, A.; Bouziane, A.; Erraji, S.; Lakhdar, L.; Rhissassi, M.; Miyazaki, H.; Ansai, T.; Iwasaki, M.; Ennibi, O. Etiology of aggressive periodontitis in individuals of African descent. Jpn. Dent. Sci. Rev. 2021, 57, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Brogan, J.M.; Lally, E.T.; Poulsen, K.; Kilian, M.; Demuth, D.R. Regulation of Actinobacillus actinomycetemcomitans leukotoxin expression: Analysis of the promoter regions of leukotoxic and minimally leukotoxic strains. Infect Immun. 1994, 62, 501–508. [Google Scholar] [CrossRef]
- Tsai, C.C.; Ho, Y.P.; Chou, Y.S.; Ho, K.Y.; Wu, Y.M.; Lin, Y.C. Aggregatibacter (Actinobacillus) actimycetemcomitans leukotoxin and human periodontitis—A historic review with emphasis on JP2. Kaohsiung J. Med. Sci. 2018, 34, 186–193. [Google Scholar] [CrossRef]
- Konig, M.F.; Abusleme, L.; Reinholdt, J.; Palmer, R.J.; Teles, R.P.; Sampson, K.; Rosen, A.; Nigrovic, P.A.; Sokolove, J.; Giles, J.T.; et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Sci. Trans. Med. 2016, 8, 369ra176. [Google Scholar] [CrossRef] [PubMed]
- Haubek, D.; Poulsen, K.; Kilian, M. Microevolution and patterns of dissemination of the JP2 clone of Aggregatibacter (Actinobacillus) actinomycetemcomitans. Infect. Immun. 2007, 75, 3080–3088. [Google Scholar] [CrossRef] [PubMed]
- Haubek, D.; Dirienzo, J.M.; Tinoco, E.M.; Westergaard, J.; López, N.J.; Chung, C.P.; Poulsen, K.; Kilian, M. Racial tropism of a highly toxic clone of Actinobacillus actinomycetemcomitans associated with juvenile periodontitis. J. Clin. Microbiol. 1997, 35, 3037–3042. [Google Scholar] [CrossRef]
- Haubek, D. The highly leukotoxic JP2 clone of Aggregatibacter actinomycetemcomitans: Evolutionary aspects, epidemiology and etiological role in aggressive periodontitis. APMIS 2010, 1–53. [Google Scholar] [CrossRef]
- Dahlen, G.; Basic, A.; Bylund, J. Importance of Virulence Factors for the Persistence of Oral Bacteria in the Inflamed Gingival Crevice and in the Pathogenesis of Periodontal Disease. J. Clin. Med. 2019, 8, 1339. [Google Scholar] [CrossRef]
- Burgess, D.; Huang, H.; Harrison, P.; Aukhil, I.; Shaddox, L. Aggregatibacter actinomycetemcomitans in African Americans with Localized Aggressive Periodontitis. JDR Clin. Trans. Res. 2017, 2, 249–257. [Google Scholar] [CrossRef]
- Albandar, J.M.; Rams, T.E. Risk factors for periodontitis in children and young persons. Periodontology 2000 2002, 29, 207–222. [Google Scholar] [CrossRef]
- Susin, C.; Haas, A.N.; Albandar, J.M. Epidemiology and demographics of aggressive periodontitis. Periodontology 2000 2014, 65, 27–45. [Google Scholar] [CrossRef]
- Claesson, R.; Gudmundson, J.; Aberg, C.H.; Haubek, D.; Johansson, A. Detection of a 640-bp deletion in the Aggregatibacter actinomycetemcomitans leukotoxin promoter region in isolates from an adolescent of Ethiopian origin. J. Oral Microbiol. 2015, 7, 26974. [Google Scholar] [CrossRef] [PubMed]
- Fine, D.H.; Markowitz, K.; Furgang, D.; Fairlie, K.; Ferrandiz, J.; Nasri, C.; McKiernan, M.; Gunsolley, J. Aggregatibacter actinomycetemcomitans and its relationship to initiation of localized aggressive periodontitis: Longitudinal cohort study of initially healthy adolescents. J. Clin. Microbiol. 2007, 45, 3859–3869. [Google Scholar] [CrossRef] [PubMed]
- Fine, D.H.; Patil, A.G.; Velusamy, S.K. Aggregatibacter actinomycetemcomitans (Aa) Under the Radar: Myths and Misunderstandings of Aa and Its Role in Aggressive Periodontitis. Front. Immunol. 2019, 10, 728. [Google Scholar] [CrossRef]
- Rylev, M.; Kilian, M. Prevalence and distribution of principal periodontal pathogens worldwide. J. Clin. Periodontol. 2008, 35, 346–361. [Google Scholar] [CrossRef] [PubMed]
- Orrù, G.; Marini, M.F.; Ciusa, M.L.; Isola, D.; Cotti, M.; Baldoni, M.; Piras, V.; Pisano, E.; Montaldo, C. Usefulness of real time PCR for the differentiation and quantification of 652 and JP2 Actinobacillus actinomycetemcomitans genotypes in dental plaque and saliva. BMC Infect. Dis. 2006, 6, 98. [Google Scholar] [CrossRef] [PubMed]
- Kissa, J.; Chemlali, S.; El Houari, B.; Amine, K.; Khlil, N.; Mikou, S.; Nadifi, S.; Albandar, J.M. Aggressive and chronic periodontitis in a population of Moroccan school students. J. Clin. Periodontol. 2016, 43, 934–939. [Google Scholar] [CrossRef]
- Claesson, R.; Hoglund-Aberg, C.; Haubek, D.; Johansson, A. Age-related prevalence and characteristics of Aggregatibacter actinomycetemcomitans in periodontitis patients living in Sweden. J. Oral Microbiol. 2017, 9, 1334504. [Google Scholar] [CrossRef] [PubMed]
- Childers, N.K.; Grenett, H.; Morrow, C.; Kumar, R.; Jezewski, P.A. Potential Risk for Localized Aggressive Periodontitis in African American Preadolescent Children. Pediatr. Dent. 2017, 39, 294–298. [Google Scholar] [PubMed]
- Stähli, A.; Sculean, A.; Eick, S. JP2 Genotype of Aggregatibacter actinomycetemcomitans in Caucasian Patients: A Presentation of Two Cases. Pathogens 2020, 9, 178. [Google Scholar] [CrossRef]
- World Migration Report. 2018. Available online: https://www.iom.int/wmr/world-migration-report-2018 (accessed on 8 December 2017).
- Mros, S.T.; Berglundh, T. Aggressive periodontitis in children: A 14–19-year follow-up. J. Clin. Periodontol. 2010, 37, 283–287. [Google Scholar] [CrossRef]
- Claesson, R.; Lagervall, M.; Höglund-Aberg, C.; Johansson, A.; Haubek, D. Detection of the highly leucotoxic JP2 clone of Aggregatibacter actinomycetemcomitans in members of a Caucasian family living in Sweden. J. Clin. Periodontol. 2011, 38, 115–121. [Google Scholar] [CrossRef]
- Burgess, D.K.; Huang, H.; Harrison, P.; Kompotiati, T.; Aukhil, I.; Shaddox, L.M. Non-Surgical Therapy Reduces Presence of JP2 Clone in Localized Aggressive Periodontitis. J. Periodontol. 2017, 88, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Pahumunto, N.; Ruangsri, P.; Wongsuwanlert, M.; Piwat, S.; Dahlen, G.; Teanpaisan, R. Virulence of Aggregatibacter actinomycetemcomitans serotypes and DGGE subtypes isolated from chronic adult periodontitis in Thailand. Anaerobe 2015, 36, 60–64. [Google Scholar] [CrossRef]
- Elamin, A.; Albandar, J.M.; Poulsen, K.; Ali, R.W.; Bakken, V. Prevalence of Aggregatibacter actinomycetemcomitans in Sudanese patients with aggressive periodontitis: A case-control study. J. Periodontal. Res. 2011, 46, 285–291. [Google Scholar] [CrossRef]
- Kwamin, F.; Gref, R.; Haubek, D.; Johansson, A. Interactions of extracts from selected chewing stick sources with Aggregatibacter actinomycetemcomitans. BMC Res. Notes 2012, 5, 203. [Google Scholar] [CrossRef]
- Ennibi, O.K.; Claesson, R.; Akkaoui, S.; Reddahi, S.; Kwamin, F.; Haubek, D.; Johansson, A. High salivary levels of JP2 genotype of Aggregatibacter actinomycetemcomitans is associated with clinical attachment loss in Moroccan adolescents. Clin. Exp. Dent. Res. 2019, 5, 44–51. [Google Scholar] [CrossRef]
- Krueger, E.; Brown, A.C. Aggregatibacter actinomycetemcomitans leukotoxin: From mechanism to targeted anti-toxin therapeutics. Mol. Oral Microbiol. 2020, 35, 85–105. [Google Scholar] [CrossRef] [PubMed]
- Ben Lagha, A.; Howell, A.; Grenier, D. Cranberry Proanthocyanidins Neutralize the Effects of Aggregatibacter actinomycetemcomitans Leukotoxin. Toxins 2019, 11, 662. [Google Scholar] [CrossRef]
- Ben Lagha, A.; LeBel, G.; Grenier, D. Dual action of highbush blueberry proanthocyanidins on Aggregatibacter actinomycetemcomitans and the host inflammatory response. BMC Complement. Altern. Med. 2018, 18, 10. [Google Scholar] [CrossRef]
- Chang, E.H.; Giaquinto, P.; Huang, J.; Balashova, N.V.; Brown, A.C. Epigallocatechin gallate inhibits leukotoxin release by Aggregatibacter actinomycetemcomitans by promoting association with the bacterial membrane. Mol. Oral Microbiol. 2020, 35, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Åberg, C.H.; Kwamin, F.; Claesson, R.; Johansson, A.; Haubek, D. Presence of JP2 and Non-JP2 Genotypes of Aggregatibacter actinomycetemcomitans and attachment loss in adolescents in Ghana. J. Periodontol. 2012, 83, 1520–1528. [Google Scholar] [CrossRef]
- Kemoli, A.; Gjorup, H.; Norregaard, M.M.; Lindholm, M.; Mulli, T.; Johansson, A.; Haubek, D. Prevalence and impact of infant oral mutilation on dental occlusion and oral health-related quality of life among Kenyan adolescents from Maasai Mara. BMC Oral Health 2018, 18, 173. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, K.; Ennibi, O.K.; Haubek, D. Improved PCR for detection of the highly leukotoxic JP2 clone of Actinobacillus actinomycetemcomitans in subgingival plaque samples. J. Clin. Microbiol. 2003, 41, 4829–4832. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Tooth | Permanent Teeth Present | Permanent Teeth Absent | Primary Teeth Present | ||
|---|---|---|---|---|---|
| Types | Bilateral | Bilateral | Unilateral | Bilateral | Unilateral |
| M3 max a | 88 | 170 | 24 | - | - |
| M2 max | 278 | 2 | 4 | - | - |
| M1 max | 279 | 0 | 5 | - | - |
| P2 max | 276 | 0 | 1 | 4 | 3 |
| P1 max | 279 | 0 | 4 | 1 | 0 |
| C max | 269 | 4 | 7 | 2 | 2 |
| I2 max | 274 | 6 | 3 | 0 | 1 |
| I1 max | 282 | 0 | 2 | 0 | 0 |
| M3 mand a | 107 | 154 | 21 | - | - |
| M2 mand | 277 | 3 | 4 | - | - |
| M1 mand | 276 | 2 | 6 | - | - |
| P2 mand | 280 | 0 | 1 | 0 | 3 |
| P1 mand | 282 | 0 | 1 | 0 | 1 |
| C mand | 267 | 5 | 10 | 1 | 1 |
| I2 mand | 263 | 5 | 14 | 0 | 2 |
| I1 mand | 108 | 164 | 12 | 0 | 0 |
| Questions | Yes (%) | No (%) | Missing Data (%) |
|---|---|---|---|
| Do you have your own toothbrush? | 254 (89.4) | 28 (9.9) | 2 (0.7) |
| Do you brush your teeth every day? | 282 (99.3) | 2 (0.7) | 0 (0.0) |
| Do you brush in the morning? | 271 (95.4) | 12 (4.2) | 1 (0.4) |
| Do you brush at lunchtime? | 164 (57.7) | 120 (42.2) | 0 (0.0) |
| Do you brush in the evening? | 179 (63.0) | 105 (37.0) | 0 (0.0) |
| Do you brush at other times of the day? | 6 (2.1) | 278 (97.9) | 0 (0.0) |
| Do you use tooth floss? | 1 (0.4) | 263 (92.6) | 20 (7.0) |
| Do you use toothpicks? | 171 (60.2) | 92 (32.4) | 21 (7.4) |
| Do you use mouth rinse? | 1 (0.4) | 264 (93.0) | 19 (6.7) |
| Do you clean with other things? | 205 (72.2) | 2 (0.7) | 77 (27.1) |
| Do you have toothpaste in your home? | 221 (77.8) | 60 (21.1) | 3 (1.1) |
| Do you use toothpaste? | 230 (80.1) | 53 (18.7) | 1 (0.4) |
| Do you use toothpaste with fluoride? * | 217 (95.4) | 54 (19.0) | 2 (0.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haubek, D.; Mulli, T.; Kemoli, A.; Lindholm, M.; Gjørup, H.; Nørregaard, M.-L.M.; Johansson, A. Prevalence of JP2 and Non-JP2 Genotypes of Aggregatibacter actinomycetemcomitans and Oral Hygiene Practice of Kenyan Adolescents in Maasai Mara. Pathogens 2021, 10, 488. https://doi.org/10.3390/pathogens10040488
Haubek D, Mulli T, Kemoli A, Lindholm M, Gjørup H, Nørregaard M-LM, Johansson A. Prevalence of JP2 and Non-JP2 Genotypes of Aggregatibacter actinomycetemcomitans and Oral Hygiene Practice of Kenyan Adolescents in Maasai Mara. Pathogens. 2021; 10(4):488. https://doi.org/10.3390/pathogens10040488
Chicago/Turabian StyleHaubek, Dorte, Tonnie Mulli, Arthur Kemoli, Mark Lindholm, Hans Gjørup, Marie-Louise Milvang Nørregaard, and Anders Johansson. 2021. "Prevalence of JP2 and Non-JP2 Genotypes of Aggregatibacter actinomycetemcomitans and Oral Hygiene Practice of Kenyan Adolescents in Maasai Mara" Pathogens 10, no. 4: 488. https://doi.org/10.3390/pathogens10040488
APA StyleHaubek, D., Mulli, T., Kemoli, A., Lindholm, M., Gjørup, H., Nørregaard, M.-L. M., & Johansson, A. (2021). Prevalence of JP2 and Non-JP2 Genotypes of Aggregatibacter actinomycetemcomitans and Oral Hygiene Practice of Kenyan Adolescents in Maasai Mara. Pathogens, 10(4), 488. https://doi.org/10.3390/pathogens10040488