Evidence for Establishing the Clinical Breakpoint of Cefquinome against Haemophilus Parasuis in China

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Results
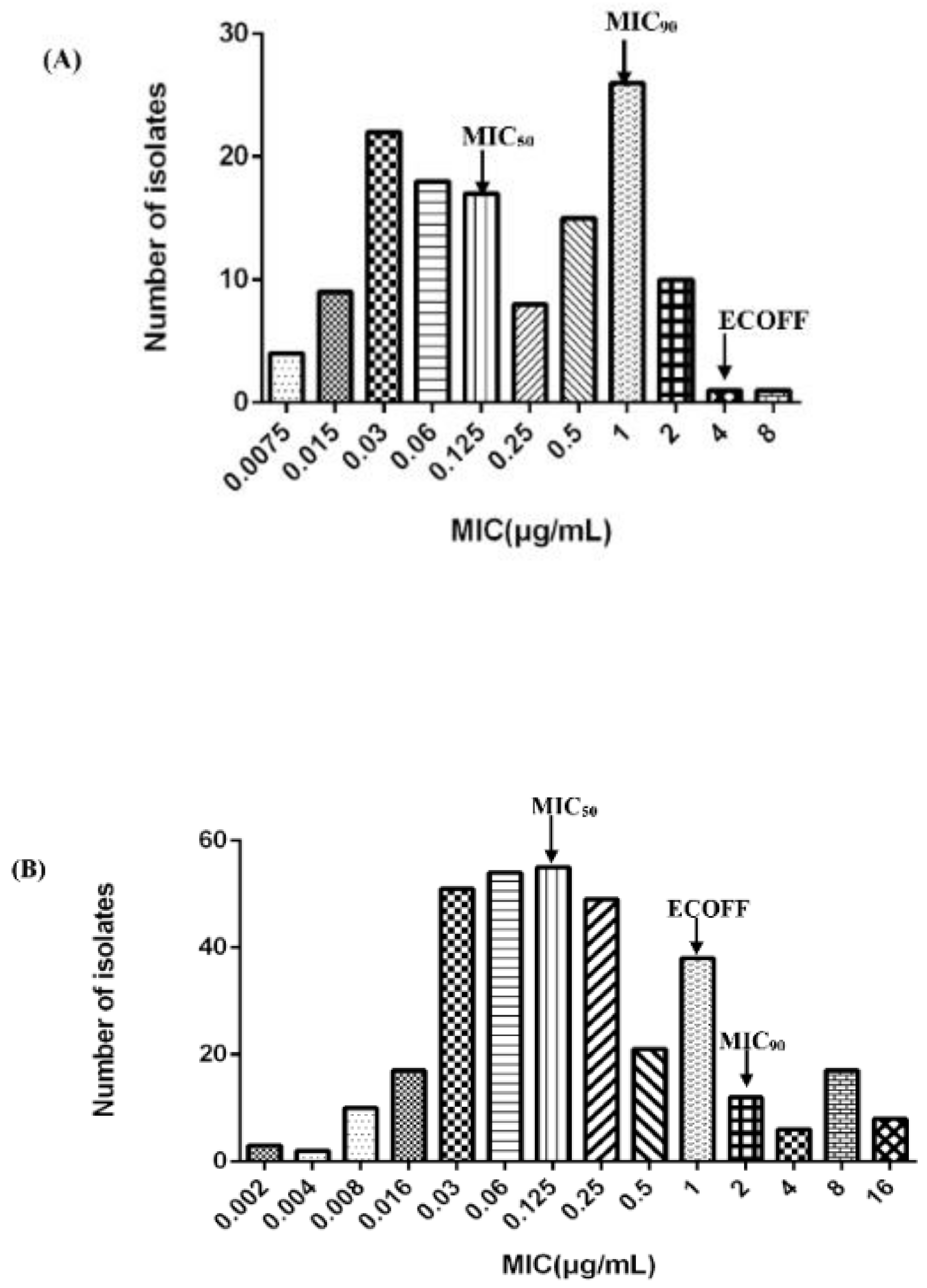
2.1. MIC Distribution of CEQ against H. parasuis and ECOFF Calculation
2.2. Selection of Strains and MIC and MBC
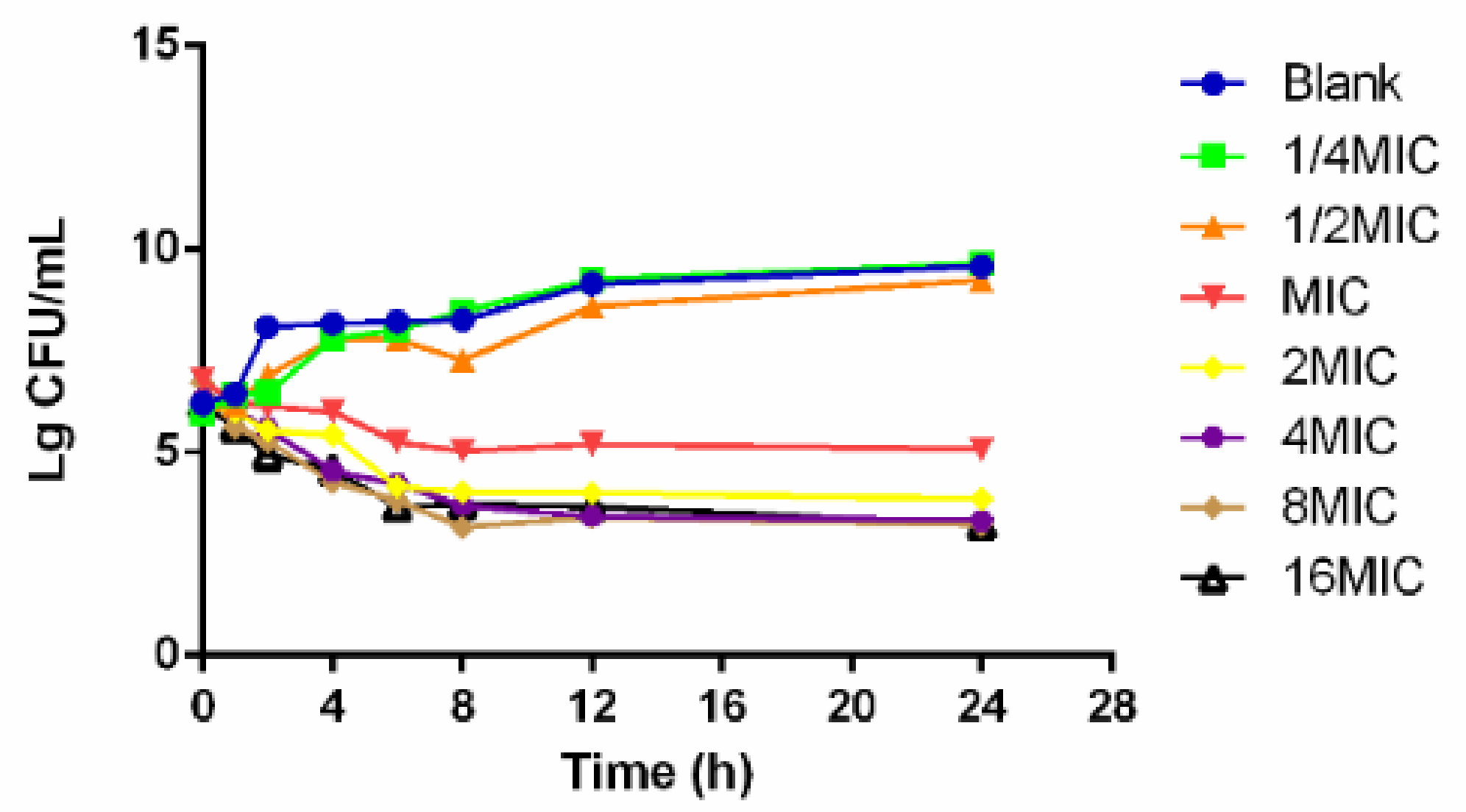
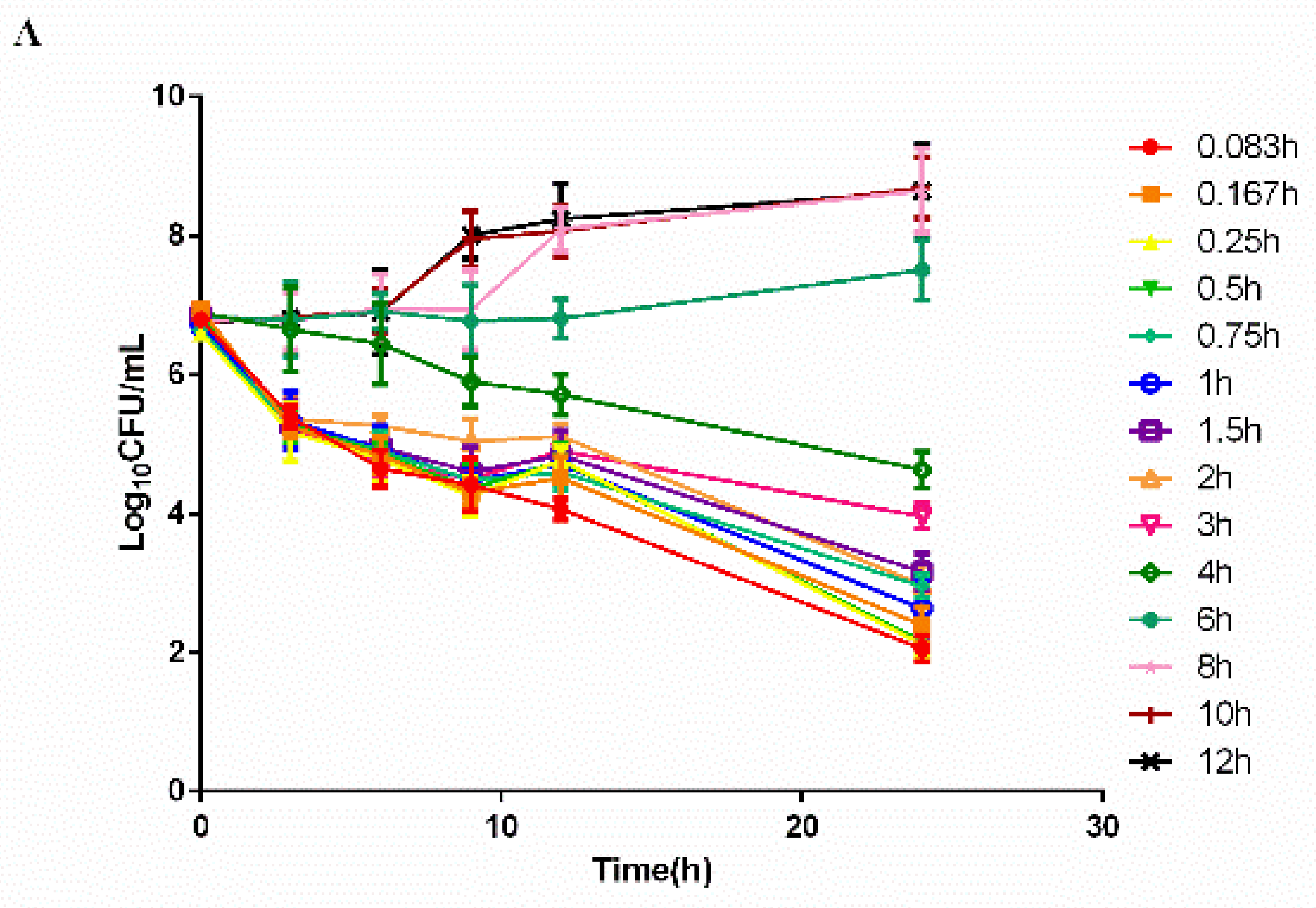
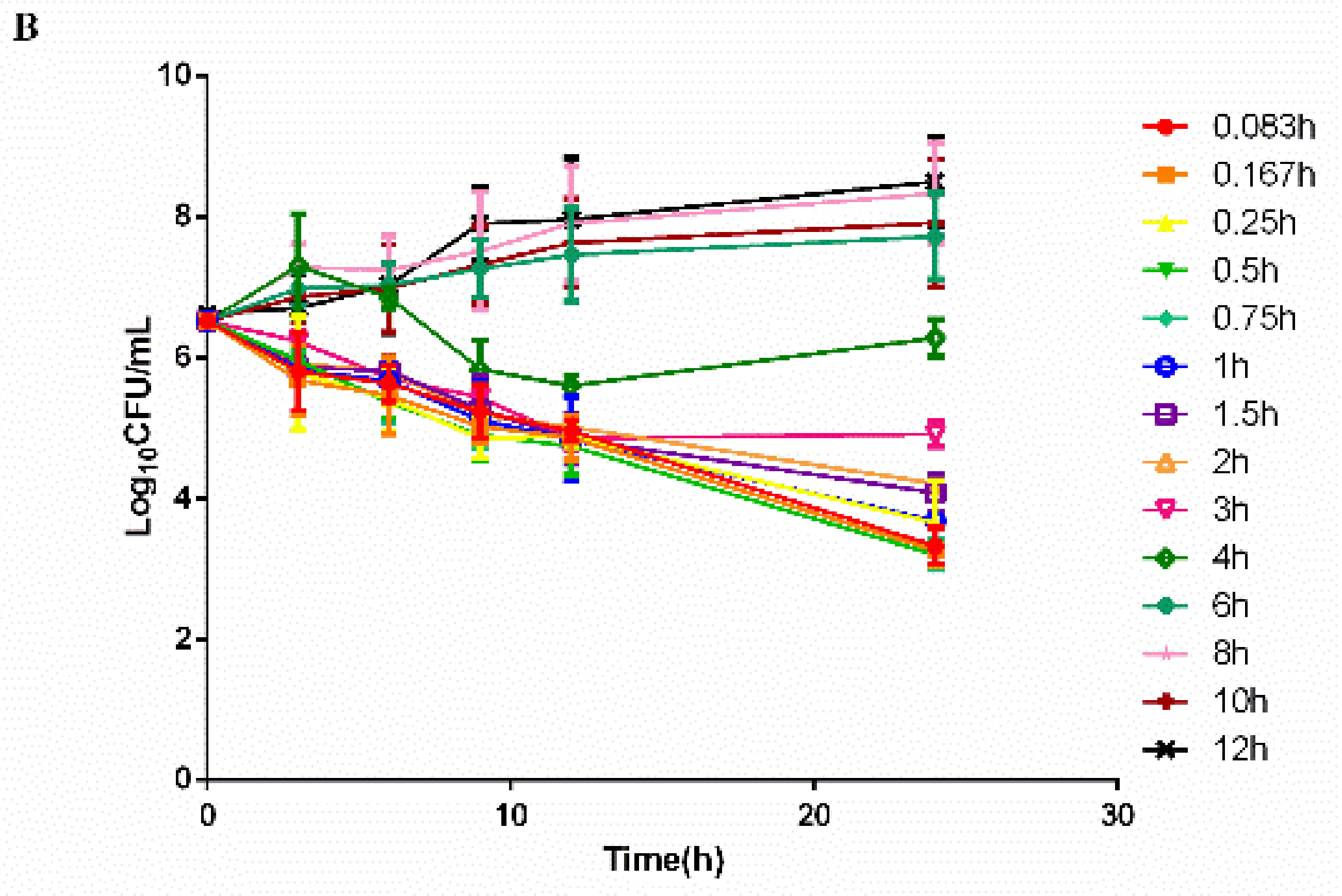
2.3. Time–Killing Curves
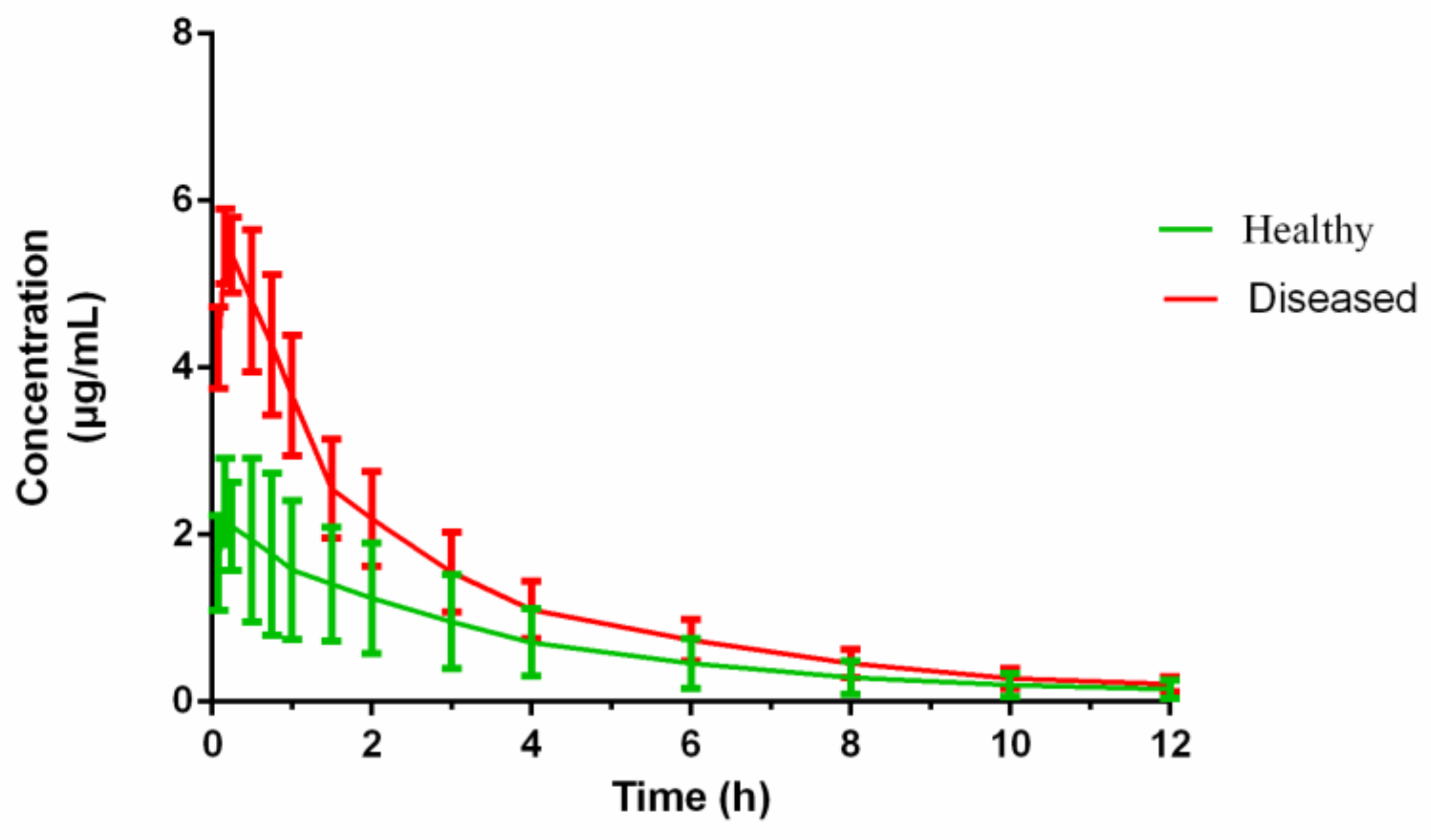
2.4. PK of Cefquinome
2.5. PK/PD Integration and Analysis
2.6. PK/PD Cutoff Calculation of Cefquinome against HPS42
2.7. Determination of the COCL
2.8. Establishment of CBP
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Strains and Antibiotic
4.3. MIC Distribution and ECOFF Determination
4.4. Selection of the Virulent Strains
4.5. Pharmacodynamics Experiments
4.5.1. Determination of MIC and MBC
4.5.2. Time–Killing Curves In Vitro and Ex Vivo
4.6. Pharmacokinetic Experiments
4.6.1. Sample
4.6.2. HPLC
4.7. PK/PD Integration Analysis
4.8. Monte-Carlo Analysis and PK/PD Cutoff Calculation
4.9. Clinical Cutoff
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Boeckel, T.P.; Pires, J.; Silvester, R.; Zhao, C.; Song, J.; Criscuolo, N.G.; Gilbert, M.; Bonhoeffer, S.; Laxminarayan, R. Global trends in antimicrobial resistance in animals in low- and middle-income countries. Science 2019, 365, eaaw1944. [Google Scholar] [CrossRef]
- Tenover, F.C. Mechanisms of Antimicrobial Resistance in Bacteria. Am. J. Med. 2006, 119, S3–S10. [Google Scholar] [CrossRef]
- Strasfeld, L.; Chou, S. Antiviral Drug Resistance: Mechanisms and Clinical Implications. Infect. Dis. Clin. 2010, 24, 809–833. [Google Scholar] [CrossRef]
- Toutain, P.; Bousquet-Mélou, A.; Damborg, P.; Ferran, A.A.; Mevius, D.; Pelligand, L.; Veldman, K.T.; Lees, P. En Route towards European Clinical Breakpoints for Veterinary Antimicrobial Susceptibility Testing: A Position Paper Explaining the VetCAST Approach. Front. Microbiol. 2017, 8, 2344. [Google Scholar] [CrossRef]
- Amano, H.; Shibata, M.; Kajio, N.; Morozumi, T. Pathologic Observations of Pigs Intranasally Inoculated with Serovar 1, 4 and 5 of Haemophilus parasuis Using Immunoperoxidase Method. J. Vet. Med. Sci. 1994, 56, 639–644. [Google Scholar] [CrossRef]
- Oliveira, S.; Pijoan, C. Haemophilus parasuis: New trends on diagnosis, epidemiology and control. Vet. Microbiol. 2004, 99, 1–12. [Google Scholar] [CrossRef]
- Kielstein, P.; Rappgabrielson, V.J. Designation of 15 Serovars of Haemophilus Parasuis on the Basis of Immunodiffusion Using Heat-Stable Antigen Extracts. J. Clin. Microbiol. 1992, 30, 862–865. [Google Scholar] [CrossRef]
- Macedo, N.; Rovira, A.; Torremorell, M. Haemophilus parasuis: Infection, immunity and enrofloxacin. Vet. Res. 2015, 46, 1–6. [Google Scholar] [CrossRef]
- EMA. Committe for Veterinary Medicinal Products Cefquinome (Extention to Pigs) Summary Reports (2). Available online: https://www.ema.europa.eu/en/documents/mrl-report/cefquinome-extension-pigs-summary-report-2-committee-veterinary-medicinal-products_en.pdf (accessed on 21 October 1999).
- Zhang, L.; Wu, X.; Huang, Z.; Zhang, N.; Wu, Y.; Cai, Q.; Shen, X.; Ding, H. Pharmacokinetic/pharmacodynamic assessment of cefquinome against Actinobacillus Pleuropneumoniae in a piglet tissue cage infection model. Vet. Microbiol. 2018, 219, 100–106. [Google Scholar] [CrossRef]
- Guo, C.; Liao, X.; Wang, M.; Wang, F.; Yan, C.; Xiao, X.; Sun, J.; Liu, Y.-H. In VivoPharmacodynamics of Cefquinome in a Neutropenic Mouse Thigh Model of Streptococcus suis Serotype 2 at Varied Initial Inoculum Sizes. Antimicrob. Agents Chemother. 2015, 60, 1114–1120. [Google Scholar] [CrossRef]
- Xiao, X.; Sun, J.; Chen, Y.; Huang, R.-J.; Huang, T.; Qiao, G.G.; Zhou, Y.-F.; Liu, Y.-H. In vitro dynamic pharmacokinetic/pharmacodynamic(PK/PD) modeling and PK/PD cutoff of cefquinome against Haemophilus parasuis. BMC Vet. Res. 2015, 11, 33. [Google Scholar] [CrossRef]
- Limbert, M.; Isert, D.; Klesel, N.; Markus, A.; Seeger, K.; Seibert, G.; Schrinner, E. Antibacterial activities in vitro and in vivo and pharmacokinetics of cefquinome (HR 111V), a new broad-spectrum cephalosporin. Antimicrob. Agents Chemother. 1991, 35, 14–19. [Google Scholar] [CrossRef]
- Zhang, B.; Lu, X.; Gu, X.; Li, X.; Gu, M.; Zhang, N.; Shen, X.; Ding, H.-Z. Pharmacokinetics and ex vivo pharmacodynamics of cefquinome in porcine serum and tissue cage fluids. Vet. J. 2014, 199, 399–405. [Google Scholar] [CrossRef]
- Matter, D.; Rossano, A.; Limat, S.; Vorlet-Fawer, L.; Brodard, I.; Perreten, V. Antimicrobial resistance profile of Actinobacillus pleuropneumoniae and Actinobacillus porcitonsillarum. Vet. Microbiol. 2007, 122, 146–156. [Google Scholar] [CrossRef]
- Toutain, P.; Sidhu, P.K.; Lees, P.; Rassouli, A.; Pelligand, L. VetCAST Method for Determination of the Pharmacokinetic-Pharmacodynamic Cut-Off Values of a Long-Acting Formulation of Florfenicol to Support Clinical Breakpoints for Florfenicol Antimicrobial Susceptibility Testing in Cattle. Front. Microbiol. 2019, 10, 1310. [Google Scholar] [CrossRef]
- Lei, Z.; Liu, Q.; Yang, S.; Yang, B.; Khaliq, H.; Li, K.; Ahmed, S.; Sajid, A.; Zhang, B.; Chen, P.; et al. PK-PD Integration Modeling and Cutoff Value of Florfenicol against Streptococcus suis in Pigs. Front. Pharmacol. 2018, 9, 2. [Google Scholar] [CrossRef]
- Schwarz, S.; Böttner, A.; Goosens, L.; Hafez, H.M.; Hartmann, K.; Kaske, M.; Kehrenberg, C.; Kietzmann, M.; Klarmann, D.; Klein, G. A Proposal of Clinical Breakpoints for Amoxicillin Applicable to Porcine Respiratory Tract Pathogens. Vet. Microbiol. 2008, 126, 178–188. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Disk and Dilution Susceptibility Tests for Bacteria Isolated from Animals. In Approved Standard Vet01-A4; CLSI: Wayne, PA, USA, 2013. [Google Scholar]
- Turnidge, D.J.; Martinez, M.N. Proposed Method for Estimating Clinical Cut-Off (Cocl) Values: An Attempt to Address Challenges Encountered When Setting Clinical Breakpoints for Veterinary Antimicrobial Agents. Vet. J. 1997, 228, 33. [Google Scholar] [CrossRef]
- Godinho, K.S.; Keane, S.G.; Nanjiani, A.I.; Benchaoui, A.H.; Sunderland, S.J.; Jones, M.A.; Weatherley, A.J.; Gootz, T.D.; Rowan, T.G. Minimum inhibitory concentrations of tulathromycin against respiratory bacterial pathogens isolated from clinical cases in European cattle and swine and variability arising from changes in in vitro methodology. Vet. Ther. Res. Appl. Vet. Med. 2005, 6, 113–121. [Google Scholar]
- Toutain, P.; Potter, T.; Pelligand, L.; Lacroix, M.; Illambas, J.; Lees, P. Standard PK/PD concepts can be applied to determine a dosage regimen for a macrolide: The case of tulathromycin in the calf. J. Vet. Pharmacol. Ther. 2016, 40, 16–27. [Google Scholar] [CrossRef]
- Toutain, P.-L.; Del Castillo, J.; Bousquet-Mélou, A. The pharmacokinetic–pharmacodynamic approach to a rational dosage regimen for antibiotics. Res. Vet. Sci. 2002, 73, 105–114. [Google Scholar] [CrossRef]
- Ahmad, I.; Hao, H.; Huang, L.; Sanders, P.; Wang, X.; Chen, D.; Tao, Y.; Xie, S.; Xiuhua, K.; Li, J.; et al. Integration of PK/PD for dose optimization of Cefquinome against Staphylococcus aureus causing septicemia in cattle. Front. Microbiol. 2015, 6, 588. [Google Scholar] [CrossRef]
- Zhao, Y.; Guo, L.; Li, J.; Huang, X.; Fang, B. Characterization of antimicrobial resistance genes inHaemophilus parasuisisolated from pigs in China. PeerJ 2018, 6, e4613. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, Q.; Li, J.; Lin, X.; Huang, X.; Fang, B. Epidemiology of Haemophilus parasuis isolates from pigs in China using serotyping, antimicrobial susceptibility, biofilm formation and ERIC-PCR genotyping. PeerJ 2018, 6, e5040. [Google Scholar] [CrossRef]
- Brogden, S.; Pavlović, A.; Tegeler, R.; Kaspar, H.; De Vaan, N.; Kehrenberg, C. Antimicrobial susceptibility of Haemophilus parasuis isolates from Germany by use of a proposed standard method for harmonized testing. Vet. Microbiol. 2018, 217, 32–35. [Google Scholar] [CrossRef]
- Aarestrup, F.M.; Seyfarth, A.M.; Angen, Ø. Antimicrobial susceptibility of Haemophilus parasuis and Histophilus somni from pigs and cattle in Denmark. Vet. Microbiol. 2004, 101, 143–146. [Google Scholar] [CrossRef]
- De La Fuente, A.M.; Tucker, A.; Navas, J.; Blanco, M.; Morris, S.; Gutiérrez-Martín, C. Antimicrobial susceptibility patterns of Haemophilus parasuis from pigs in the United Kingdom and Spain. Vet. Microbiol. 2007, 120, 184–191. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Ghannoum, M.A.; Alexander, B.D. Establishment and Use of Epidemiological Cutoff Values for Molds and Yeasts by Use of the Clinical and Laboratory Standards Institute M57 Standard. J. Clin. Microbiol. 2017, 55, 1262–1268. [Google Scholar] [CrossRef]
- Jaspers, S.; Aerts, M.; Verbeke, G.; Beloeil, P.-A. Estimation of the wild-type minimum inhibitory concentration value distribution. Stat. Med. 2013, 33, 289–303. [Google Scholar] [CrossRef]
- Kronvall, G. Normalized Resistance Interpretation as a Tool for Establishing Epidemiological MIC Susceptibility Breakpoints. J. Clin. Microbiol. 2010, 48, 4445–4452. [Google Scholar] [CrossRef]
- Meletiadis, J.; Curfs-Breuker, I.; Meis, J.F.; Mouton, J.W. In Vitro Antifungal Susceptibility Testing of Candida Isolates with the EUCAST Methodology, a New Method for ECOFF Determination. Antimicrob. Agents Chemother. 2017, 61, e02372-16. [Google Scholar] [CrossRef]
- Turnidge, J.; Paterson, D.L. Setting and Revising Antibacterial Susceptibility Breakpoints. Clin. Microbiol. Rev. 2007, 20, 391–408. [Google Scholar] [CrossRef]
- Joneberg, J.; Rylander, M.; Marcelo, F.; Galas, M.F.; Carlos, C.; Kronvall, G. Analysis of Parameters and Validation of Method for Normalized Interpretation of Antimicrobial Resistance. Int. J. Antimicrob. Agents 2003, 21, 525–535. [Google Scholar] [CrossRef]
- Kronvall, G.; Kahlmeter, G.; Myhre, E.; Galas, M. A new method for normalized interpretation of antimicrobial resistance from disk test results for comparative purposes. Clin. Microbiol. Infect. 2003, 9, 120–132. [Google Scholar] [CrossRef]
- Maurer, F.; Pohle, P.; Kernbach, M.; Sievert, D.; Hillemann, D.; Rupp, J.; Hombach, M.; Kranzer, K. Differential drug susceptibility patterns of Mycobacterium chimaera and other members of the Mycobacterium avium-intracellulare complex. Clin. Microbiol. Infect. 2019, 25, 379.e1–379.e7. [Google Scholar] [CrossRef]
- Lei, Z.; Liu, Q.; Qi, Y.; Yang, B.; Khaliq, H.; Xiong, J.; Moku, G.K.; Ahmed, S.; Li, K.; Zhang, H.; et al. Optimal Regimens and Cutoff Evaluation of Tildipirosin Against Pasteurella multocida. Front. Pharmacol. 2018, 9, 765. [Google Scholar] [CrossRef]
- Smith, P.; Kronvall, G. How many strains are required to set an epidemiological cut-off value for MIC values determined for bacteria isolated from aquatic animals? Aquac. Int. 2014, 23, 465–470. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Development of in Vitro Susceptibility Testing Criteria and Quality Control Parameters for Veterinary Antimicrobial Agents; Approved Guideline—Third Edition. CLSI Document (2008): M37-A3; CLSI: Wayne, PA, USA, 2008. [Google Scholar]
- El Garch, F.; De Jong, A.; Simjee, S.; Moyaert, H.; Klein, U.; Ludwig, C.; Marion, H.; Haag-Diergarten, S.; Richard-Mazet, A.; Thomas, V. Monitoring of Antimicrobial Susceptibility of Respiratory Tract Pathogens Isolated from Diseased Cattle and Pigs across Europe, 2009–2012: Vetpath Results. Vet. Microbiol. 2016, 194, 11–22. [Google Scholar] [CrossRef]
- Burch, D.; Sperling, D. Amoxicillin-current use in swine medicine. J. Vet. Pharmacol. Ther. 2018, 41, 356–368. [Google Scholar] [CrossRef]
- Oliveira, S.; Galina, L.; Pijoan, C. Development of a PCR test to diagnose Haemophilus parasuis infections. J. Vet. Diagn. Investig. 2001, 13, 495–501. [Google Scholar] [CrossRef]
- Zhang, P.; Hao, H.; Li, J.; Ahmad, I.; Cheng, G.; Chen, D.; Tao, Y.; Huang, L.; Wang, Y.; Dai, M.; et al. The Epidemiologic and Pharmacodynamic Cutoff Values of Tilmicosin against Haemophilus parasuis. Front. Microbiol. 2016, 7, 385. [Google Scholar] [CrossRef]
- Craig, W.A. State-of-the-Art Clinical Article: Pharmacokinetic/Pharmacodynamic Parameters: Rationale for Antibacterial Dosing of Mice and Men. Clin. Infect. Dis. 1998, 26, 1–10. [Google Scholar] [CrossRef]
- Sidhu, P.; Rassouli, A.; Illambas, J.; Potter, T.; Pelligand, L.; Rycroft, A.; Lees, P. Pharmacokinetic-pharmacodynamic integration and modelling of florfenicol in calves. J. Vet. Pharmacol. Ther. 2013, 37, 231–242. [Google Scholar] [CrossRef]
- Pelligand, L.; Lees, P.; Sidhu, P.K.; Toutain, P.-L. Semi-Mechanistic Modeling of Florfenicol Time-Kill Curves and in silico Dose Fractionation for Calf Respiratory Pathogens. Front. Microbiol. 2019, 10, 1237. [Google Scholar] [CrossRef]
- Sun, J.; Xiao, X.; Huang, R.J. In Vitro Dynamic Pharmacokinetic/Pharmacodynamic (Pk/Pd) Study and Copd of Marbofloxacin against Haemophilus Parasuis. BMC Vet. Res. 2015, 11, 293. [Google Scholar] [CrossRef]
- Moleres, J.; Santos-López, A.; Lázaro, I.; Labairu, J.; Prat, C.; Ardanuy, C.; González-Zorn, B.; Aragon, V.; Garmendia, J. Novel Blarob-1-Bearing Plasmid Conferring Resistance to Β-Lactams in Haemophilus Parasuis Isolates from Healthy Weaning Pigs. Appl. Environ. Microbiol. 2015, 81, 3255–3267. [Google Scholar] [CrossRef]
- Zhang, J.; Xu, C.; Shen, H.; Li, J.; Guo, L.; Cao, G.; Feng, S.; Liao, M. Biofilm formation in Haemophilus parasuis: Relationship with antibiotic resistance, serotype and genetic typing. Res. Vet. Sci. 2014, 97, 171–175. [Google Scholar] [CrossRef]
- Aarestrup, F.M.; Skov, R.L. Evaluation of ceftiofur and cefquinome for phenotypic detection of methicillin resistance in Staphylococcus aureus using disk diffusion testing and MIC-determinations. Vet. Microbiol. 2010, 140, 176–179. [Google Scholar] [CrossRef]
- Damborg, P.; Marskar, P.; Baptiste, K.E.; Guardabassi, L. Faecal shedding of CTX-M-producing Escherichia coli in horses receiving broad-spectrum antimicrobial prophylaxis after hospital admission. Vet. Microbiol. 2012, 154, 298–304. [Google Scholar] [CrossRef]
- Papich, M.G.; Lindeman, C. Cephalexin susceptibility breakpoint for veterinary isolates: Clinical Laboratory Standards Institute revision. J. Vet. Diagn. Investig. 2017, 30, 113–120. [Google Scholar] [CrossRef]
- EUCAST. European Committee on Antimicrobial Susceptibility Testing Reports. 2019. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_9.0_Breakpoint_Tables.pdf (accessed on 12 January 2019).
- Zhang, L.; Li, Y.; Wang, Y.; Sajid, A.; Ahmed, S.; Li, X. Integration of pharmacokinetic-pharmacodynamic for dose optimization of doxycycline against Haemophilus parasuis in pigs. J. Vet. Pharmacol. Ther. 2018, 41, 706–718. [Google Scholar] [CrossRef]
- Turnidge, J.; Kahlmeter, G.; Kronvall, G. Statistical characterisation of bacterial wild-type MIC value distributions and the determination of epidemiological cut-off values. Clin. Microbiol. Infect. 2006, 12, 418–425. [Google Scholar] [CrossRef]
- Yu, J.; Zhang, Y.; Du, Y.; Li, J.; Huang, B.; Sun, W.; Cong, X.; Peng, J.; Ren, S.; Gou, L.; et al. The BALB/c mouse infection model for improving the Haemophilus parasuis serotyping scheme. Res. Vet. Sci. 2016, 109, 166–168. [Google Scholar] [CrossRef]
- Toutain, P.-L. Pharmacokinetic/pharmacodynamic integration in drug development and dosage-regimen optimization for veterinary medicine. AAPS PharmSci 2002, 4, 160–188. [Google Scholar] [CrossRef]
- Trang, M.; Dudley, M.N.; Bhavnani, S.M. Use of Monte Carlo simulation and considerations for PK-PD targets to support antibacterial dose selection. Curr. Opin. Pharmacol. 2017, 36, 107–113. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Unit | Healthy | Infected |
|---|---|---|---|
| T1/2 | H | 3.52 ± 0.81 | 3.19 ± 0.92 |
| Tmax | H | 0.24 ± 0.12 | 0.26 ± 0.11 |
| Cmax | μg/mL | 2.53 ± 0.46 | 5.75 ± 0.59 |
| AUC 0–∞ | hr*μg/mL | 8.61 ± 2.68 | 15.52 ± 4.07 |
| Vz_F | mL/kg | 1.39 ± 0.74 | 0.63 ± 0.27 |
| Cl_F | mL/h/kg | 0.26 ± 0.09 | 0.14 ± 0.03 |
| MRTlast | H | 4.61 ± 0.68 | 3.59 ± 0.88 |
| Parameter | Unit | Healthy | Diseased |
|---|---|---|---|
| Emax | Log10CFU/mL | 1.71 | 2.10 |
| EC50 | Log10CFU/mL | 33.20 | 47.66 |
| E0 | Log10CFU/mL | −4.06 | −4.34 |
| N | _ | 3.61 | 3.45 |
| AUC24h/MIC for bacteriostatic (E = 0) | H | 23 | 39 |
| AUC24h/MIC for bactericidal (E = −3) | H | 41 | 70 |
| AUC24h/MIC for eradiction (E = −4) | H | 51 | 110 |
| MIC (μg/mL) | Success | Failure | Total | %Success ≤MIC | %Success >MIC | MaxDiff | AUC Success | AUC Total | CAR |
|---|---|---|---|---|---|---|---|---|---|
| 0.125 | 3 | 3 | 6 | 50.00 | 62.50 | −12.50 | 0.19 | 0.38 | 0.50 |
| 0.25 | 4 | 2 | 6 | 58.33 | 66.67 | −8.33 | 0.63 | 1.13 | 0.56 |
| 1 | 4 | 2 | 6 | 61.11 | 66.67 | −5.56 | 3.63 | 5.63 | 0.64 |
| 4 | 5 | 1 | 6 | 66.67 | 50.00 | 16.67 | 17.13 | 23.63 | 0.72 |
| 8 | 3 | 3 | 6 | 63.33 | 100.00 | −36.67 | 33.13 | 47.63 | 0.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mi, K.; Sun, D.; Li, M.; Hao, H.; Zhou, K.; Liu, Z.; Yuan, Z.; Huang, L. Evidence for Establishing the Clinical Breakpoint of Cefquinome against Haemophilus Parasuis in China. Pathogens 2021, 10, 105. https://doi.org/10.3390/pathogens10020105
Mi K, Sun D, Li M, Hao H, Zhou K, Liu Z, Yuan Z, Huang L. Evidence for Establishing the Clinical Breakpoint of Cefquinome against Haemophilus Parasuis in China. Pathogens. 2021; 10(2):105. https://doi.org/10.3390/pathogens10020105
Chicago/Turabian StyleMi, Kun, Da Sun, Mei Li, Haihong Hao, Kaixiang Zhou, Zhenli Liu, Zonghui Yuan, and Lingli Huang. 2021. "Evidence for Establishing the Clinical Breakpoint of Cefquinome against Haemophilus Parasuis in China" Pathogens 10, no. 2: 105. https://doi.org/10.3390/pathogens10020105
APA StyleMi, K., Sun, D., Li, M., Hao, H., Zhou, K., Liu, Z., Yuan, Z., & Huang, L. (2021). Evidence for Establishing the Clinical Breakpoint of Cefquinome against Haemophilus Parasuis in China. Pathogens, 10(2), 105. https://doi.org/10.3390/pathogens10020105