Does Perception of Motor Competence Mediate Associations between Motor Competence and Physical Activity in Early Years Children?




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Anthropometric Measures
2.2.2. Motor Competence
2.2.3. Perceived Motor Competence
2.2.4. Physical Activity
2.3. Statistical Analysis
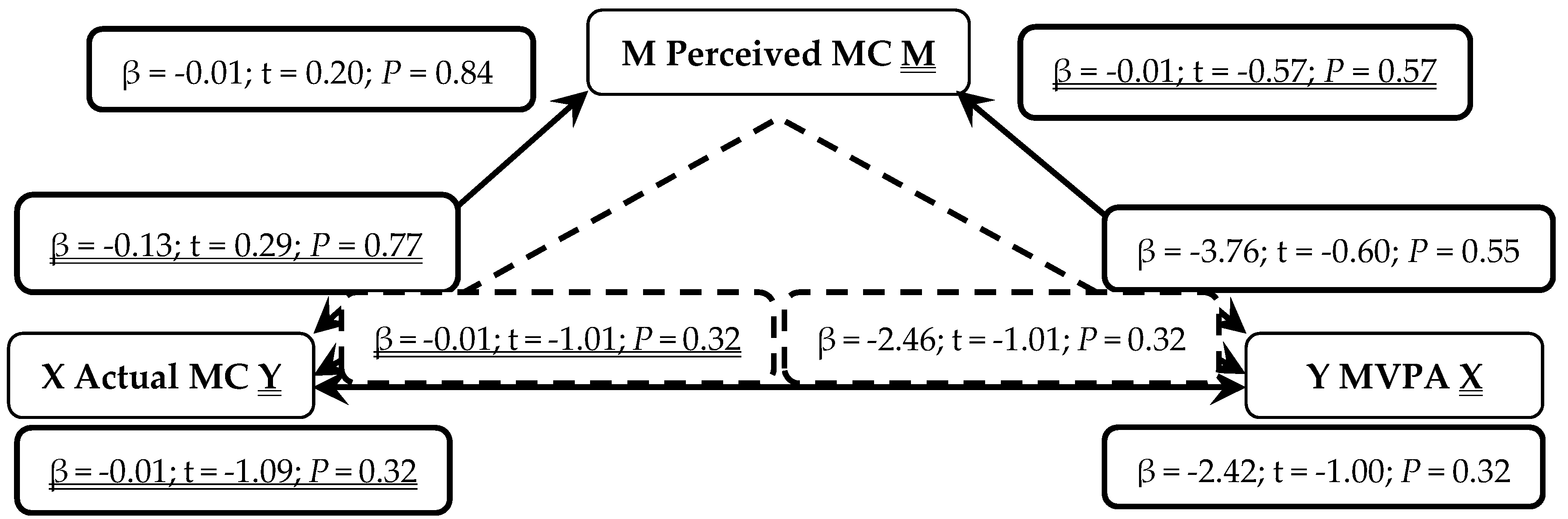
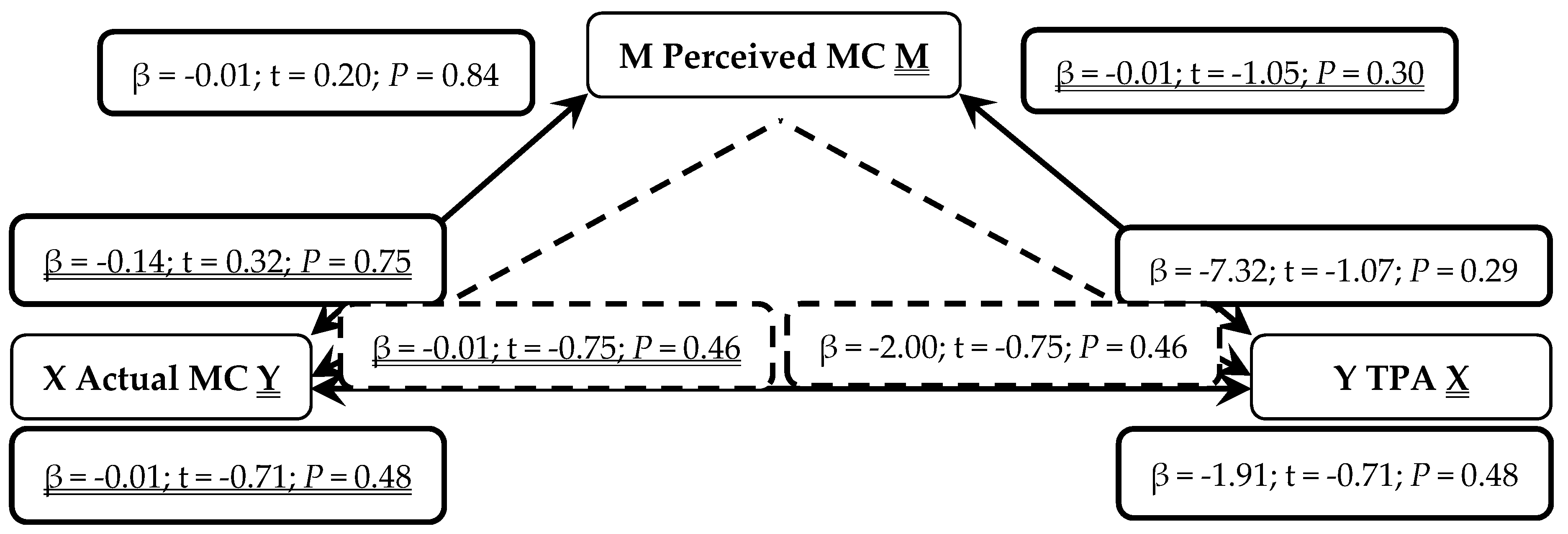
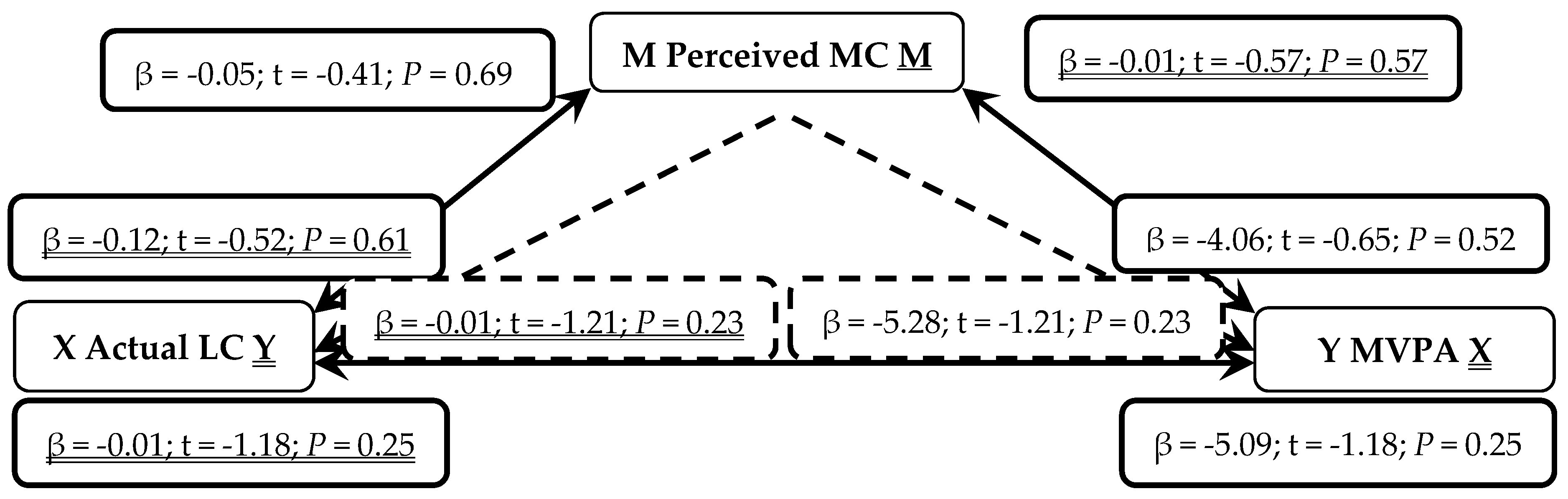
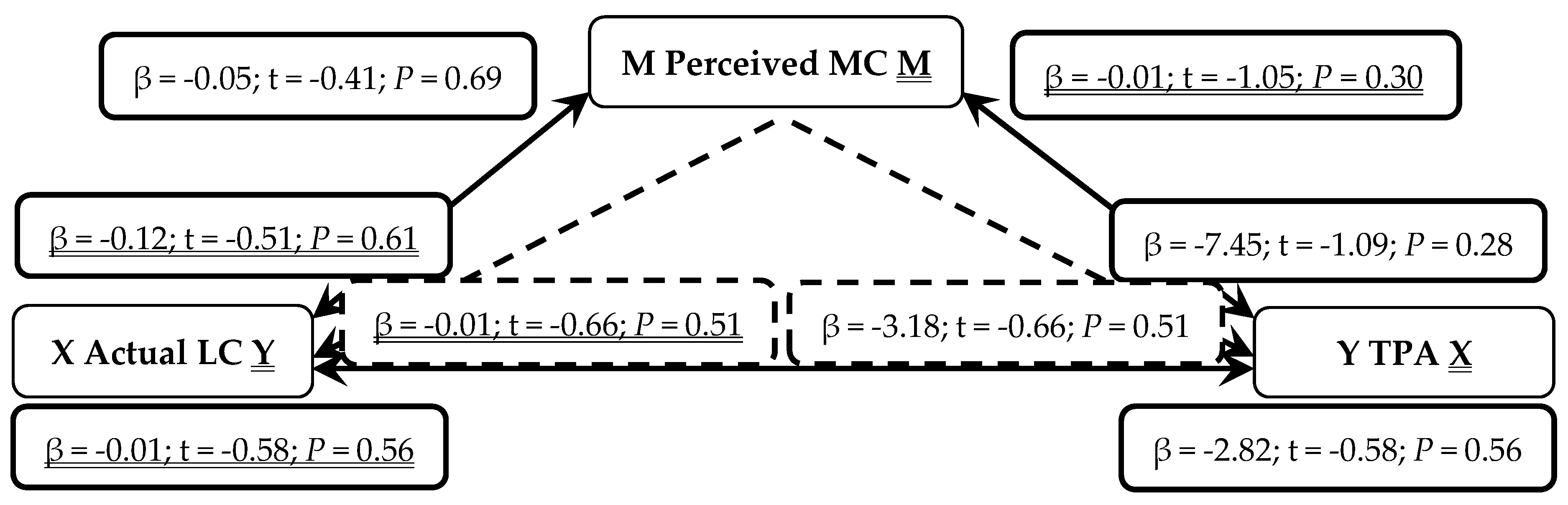
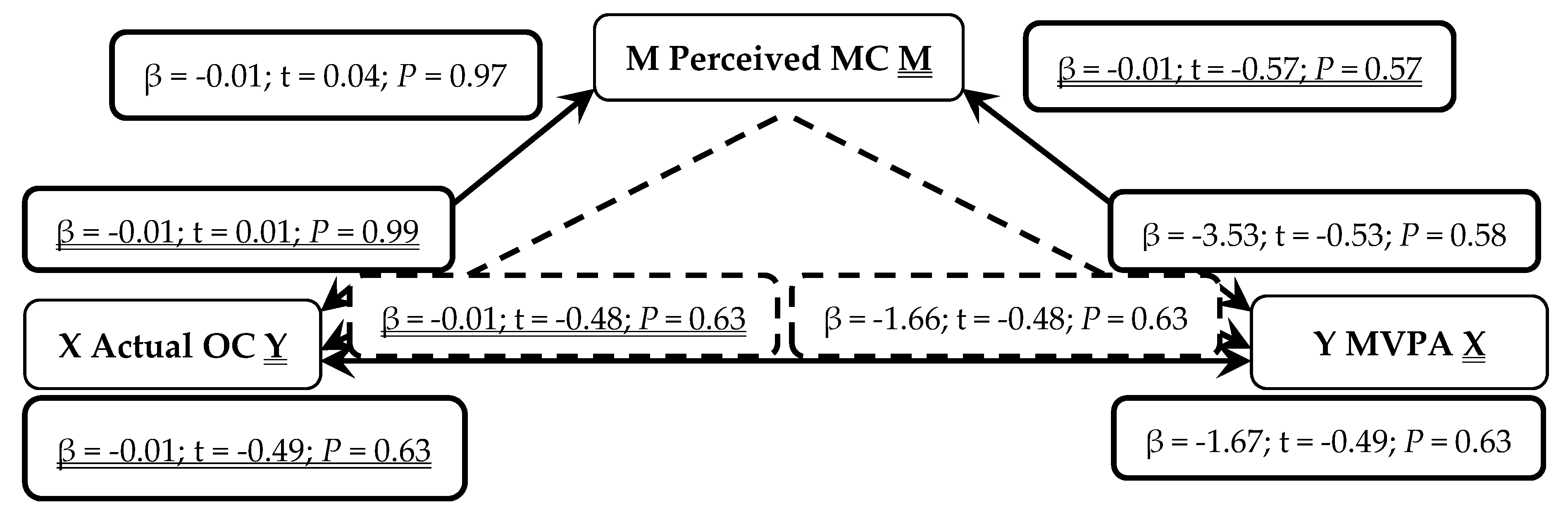
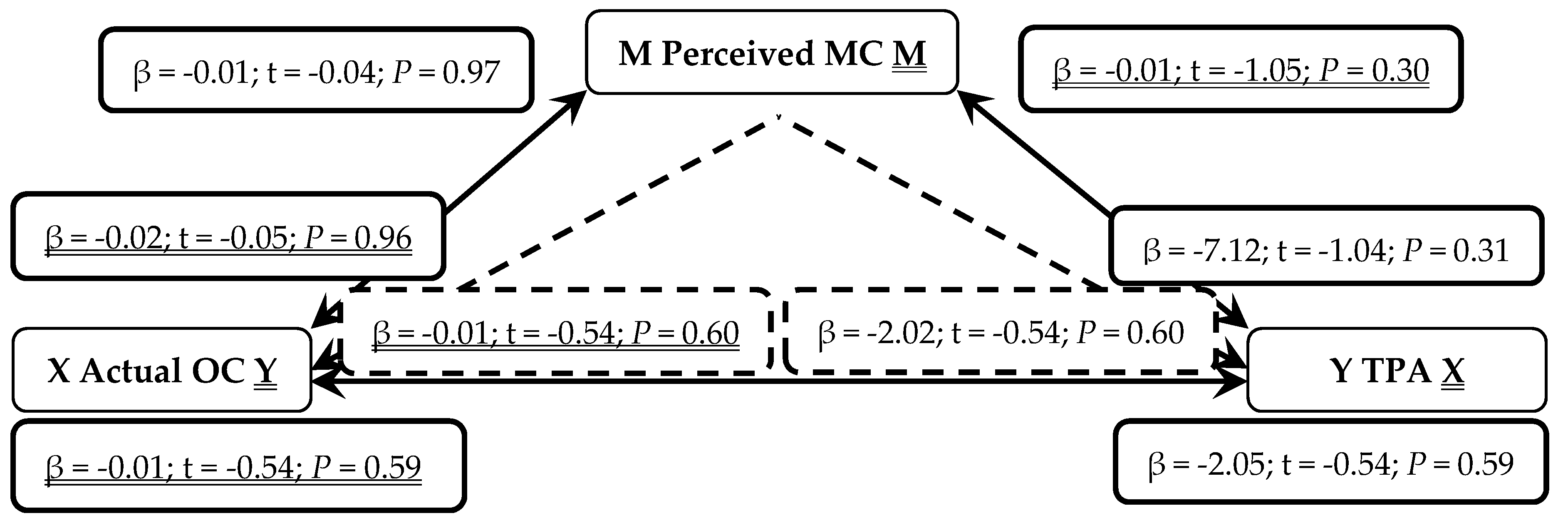
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Global Recommendations on Physical Activity for Health. Available online: http://www.who.int/dietphysicalactivity/publications/9789241599979/en/ (accessed on 6 September 2018).
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental Movement Skills in Children and Adolescents. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMA J. 2006, 174, 801–809. [Google Scholar] [CrossRef]
- LeGear, M.; Greyling, L.; Sloan, E.; Bell, R.I.; Williams, B.; Naylor, P.; Temple, V. A window of opportunity? Motor skills and perceptions of competence of children in Kindergarten. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 29. [Google Scholar] [CrossRef]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Hallal, P.C.; Andersen, L.B.; Bull, F.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Babic, M.J.; Morgan, P.J.; Plotnikoff, R.; Lonsdale, C.; White, R.L.; Lubans, D.R. Physical Activity and Physical Self-Concept in Youth: Systematic Review and Meta-Analysis. Sports Med. 2014, 44, 1589–1601. [Google Scholar] [CrossRef]
- Clark, J.E.; Metcalfe, J.S. The Mountain of Motor Development: A Metaphor; Motor Development: Research and Reviews; National Association of Sport and Physical Education: Reston, VA, USA, 2002; Volume 2, pp. 163–190. [Google Scholar]
- Haywood, K.M.; Getchell, N. Life Span. Motor Development; Human Kinetics Publishers: Champaign, IL, USA, 2009; Volume 5, pp. 5–52. [Google Scholar]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Epidemiology 2000, 32, 963–975. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Whitehead, S.H.; O’Donovan, T.M.; Nevill, M.E. Correlates of Participation in Physical Activity of Adolescent Girls: A Systematic Review of Recent Literature. J. Phys. Act. Health 2005, 2, 423–434. [Google Scholar] [CrossRef]
- Robinson, L.E. The relationship between perceived physical competence and fundamental motor skills in preschool children. Child 2011, 37, 589–596. [Google Scholar] [CrossRef]
- Foweather, L.; Knowles, Z.; Ridgers, N.D.; O’Dwyer, M.V.; Foulkes, J.D.; Stratton, G. Fundamental movement skills in relation to weekday and weekend physical activity in preschool children. J. Sci. Med. Sport 2015, 18, 691–696. [Google Scholar] [CrossRef]
- Noordstar, J.; van der Net, J.; Jak, S.; Helders, P.J.M. The change in perceived motor competence and motor task values during elementary school: A longitudinal cohort study. Br. J. Dev. Psychol. 2016, 34, 427–446. [Google Scholar] [CrossRef]
- Washburn, R.; Kolen, A. Children’s Self-Perceived and Actual Motor Competence in Relation to Their Peers. Children 2018, 5, 72. [Google Scholar] [CrossRef]
- Carroll, B.; Loumidis, J. Children’s perceived competence and enjoyment in physical education and physical activity outside school. Eur. Phys. Educ. Rev. 2001, 7, 24–43. [Google Scholar] [CrossRef]
- Barnett, L.M.; Morgan, P.J.; van Beurden, E.; Beard, J.R. Perceived sports competence mediates the relationship between childhood motor skill proficiency and adolescent physical activity and fitness: A longitudinal assessment. Int. J.f Behav. Nutr. Phys. Act. 2008, 5, 40. [Google Scholar] [CrossRef]
- Khodaverdi, Z.; Bahram, A.; Stodden, D.; Kazemnejad, A. The relationship between actual motor competence and physical activity in children: Mediating roles of perceived motor competence and health-related physical fitness. J. Sports Sci. 2016, 34. [Google Scholar] [CrossRef]
- Lopes, V.P.; Saraiva, L.; Goncalves, C.; Rodrigues, L.P. Association Between Perceived and Actual Motor Competence in Portuguese Children. J. Mot. Learn. Dev. 2018, 6, S366–S377. [Google Scholar] [CrossRef]
- Chan, C.H.; Ha, A.S.; Ng, J.Y.; Lubans, D.R. Associations between fundamental movement skill competence, physical activity and psychosocial determinants in Hong Kong Chinese children. J. Sports Sci. 2018. [Google Scholar] [CrossRef]
- Crane, J.R.; Foley, J.T.; Naylor, P.; Temple, V.A. Do perceptions of competence mediate the relationship between fundamental motor skill proficiency and physical activity levels of children in kindergarten? J. Phys. Act. Health 2015, 12, 954–961. [Google Scholar] [CrossRef]
- Roscoe, C.M.; James, R.S.; Duncan, M.J. Calibration of GENEActiv accelerometer wrist cut-points for the assessment of physical activity intensity of preschool aged children. Eur. J. Pediatr. 2017, 176, 1093–1098. [Google Scholar] [CrossRef]
- Ulrich, D.A. TGMD 2–Test of Gross Motor Development Examiner’s Manual; PRO-ED: Austin, TX, USA, 2000; Volume 2. [Google Scholar]
- Barnett, L.M.; Ridgers, N.D.; Zask, A.; Salmon, J. Face validity and reliability of a pictorial instrument for assessing fundamental movement skill perceived competence in young children. JSAMS 2015, 18, 98–102. [Google Scholar] [CrossRef]
- Diao, Y.; Dong, C.; Barnett, L.M.; Estevan, I.; Li, J.; Ji, L. Validity and Reliability of a Pictorial Instrument for Assessing Fundamental Movement Skill Perceived Competence in Chinese Children. J. Mot. Learn. Dev. 2018, 6, S223–S238. [Google Scholar] [CrossRef]
- Tiejens, M.; Dreiskaemper, D.; Utesch, T.; Schott, N.; Barnett, L.M.; Hinkley, T. Pictorial Scale of Physical Self-Concept for Younger Children (P-PSC-C): A Feasibility Study. J. Mot. Learn. Dev. 2018, 6, S391–S402. [Google Scholar] [CrossRef]
- Valentini, N.C.; Barnett, L.M.; Bandeira, P.F.R.; Nobre, G.C.; Zanella, L.W.; Sartori, R.F. The Pictorial Scale of perceived Movement Skill Competence: Determining Content and Construct Validity for Brazilian Children. J. Mot. Learn. Dev. 2018, 6, S189–S204. [Google Scholar] [CrossRef]
- Vanetsanou, F.; Kossyva, I.; Valentini, N.; Afthentopoulou, A.; Barnett, L.M. Validity and Reliability of the Pictorial Scale of Perceived Movement Skill Competence for Young Greek Children. J. Mot. Learn. Dev. 2018, 6, S239–S251. [Google Scholar] [CrossRef]
- Janz, K.F.; Letuchy, E.M.; Gilmore, J.M.E.; Burns, T.L.; Torner, J.C.; Willing, M.C.; Levy, S.M. Early physical activity provides sustained bone health benefits later in childhood. Med. Sci. Sports Exerc. 2010, 42, 1072. [Google Scholar] [CrossRef]
- Trost, S.G.; McIver, K.L.; Pate, R.R. Conducting accelerometer-based activity assessments in field-based research. Med. Sci. Sports Exerc. 2005, 37, 531–543. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Chaput, J.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Improving wear time compliance with a 24-hour waist-worn accelerometer protocol in the International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE). Int. J. Behav. Nutr. Phys. Act. 2015, 12, s12966. [Google Scholar] [CrossRef]
- Esliger, D.W.; Rowlands, A.V.; Hurst, T.L.; Catt, M.; Murray, P.; Eston, R.G. Validation of the GENEA Accelerometer. Med. Sci. Sports Exerc. 2011, 43, 1085–1093. [Google Scholar] [CrossRef]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and non-wear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357. [Google Scholar] [CrossRef]
- Phillips, L.R.; Parfitt, G.; Rowlands, A.V. Calibration of the GENEA accelerometer for assessment of physical activity intensity in children. J. Sci. Med. Sport 2013, 16, 124–128. [Google Scholar] [CrossRef]
- Department of Health. Start Active, Stay Active. Available online: https://www.gov.uk/government/publications/start-active-stay-active-a-report-on-physical-activity-from-the-four-home-countries-chiefmedical-officers (accessed on 6 September 2018).
- Preacher, K.J.; Hayes, A.R. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef]
- Harter, S. The Construction of the Self: A Developmental Perspective; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Estevan, I.; Molina-Garcia, J.; Abbott, G.; Bow, S.J.; Castillo, I.; Barnett, L.M. Evidence of Reliability and Validity for the Pictorial Scale of Perceived Movement Skill Competence in Spanish Children. J. Mot. Learn. Dev. 2018, 6, S205–S222. [Google Scholar] [CrossRef]
- Pesce, C.; Masci, I.; Marchetti, R.; Vannozzi, G.; Schmidt, M. When Children’s Perceived and Actual Motor Competence Mismatch: Sport Participation and Gender Differences. J. Mot. Learn. Dev. 2018, 6, S440–S460. [Google Scholar] [CrossRef]
- Clark, C.C.T.; Moran, J.; Drury, B.; Venetsanou, F.; Fernandes, J.F.T. Actual vs. Perceived Motor Competence in Children (8–10 Years): An Issue of Non-Veridicality. J. Funct. Morphol. Kinesiol. 2018, 3, 20. [Google Scholar] [CrossRef]
- Mcgrane, B.; Powell, D.; Belton, S.; Issartel, J. Investigation Into the Relationship Between Adolescents’ Perceived and Actual Fundamental Movement Skills and Physical Activity. J. Mot. Learn. Dev. 2018, 6, S424–S439. [Google Scholar] [CrossRef]
- Rose, E.; Larkin, D.; Parker, H.; Hands, B. Does Motor Competence Affect Self-Perceptions Differently for Adolescent Males and Females? Sage 2015, 1–9. [Google Scholar] [CrossRef]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.L.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sports Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef]
- Klingberg, B.; Schranz, N.; Barnett, L.M.; Booth, V.; Ferrar, K. The feasibility of fundamental movement skill assessments for pre-school aged children. J. Sports Sci. 2018, 7, 1–9. [Google Scholar] [CrossRef]
- Cools, W.; De Martelaer, K.; Samaey, C.; Andries, C. Movement skill assessment of typically developing preschool children: A review of seven movement skill assessment tools. J. Sports Sci. 2009, 8, 154–168. [Google Scholar]
- Simons, J.; Daly, D.; Theodorou, F.; Caron, C.; Simons, J.; Andoniadou, E. Validity and reliability of the TGMD-2 in 7–10-year-old Flemish children with intellectual disability. Adapt. Phys. Act. Q. 2008, 25, 71–82. [Google Scholar] [CrossRef]
- Schoeman, A.M.; Boulton, A.J.; Short, S.D. Determining power and sample size for simple and complex mediation models. Soc. Psychol. Pers. Sci. 2017, 8, 379–386. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Children n = 38 | Males n = 24 | Females n = 14 |
|---|---|---|---|
| Age (years) | 5.37 ± 0.79 | 5.44 ± 0.68 | 5.36 ± 0.71 |
| BMI (kg/m2) | 16.48 ± 3.06 | 16.18 ± 2.53 | 16.28 ± 2.53 |
| TPA (mins) | 260 ± 148 | 274 ± 152 | 241 ± 152 |
| MVPA (mins) | 212 ± 126 | 219 ± 128 | 207 ± 128 |
| TMC (out of 96) | 69.88 ± 8.49 | 61.19 ± 8.56 | 58.01 ± 8.56 |
| LC (out of 48) | 33.32 ± 4.46 | 33.34 ± 4.89 | 33.28 ± 4.89 |
| OC (out of 48) | 26.57 ± 6.61 a | 27.85 ± 6.35 | 24.73 ± 6.35 |
| Perceived MC (12–48) | 39.24 ± 4.01 a | 39.81 ± 3.80 | 38.42 ± 3.80 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hall, C.J.S.; Eyre, E.L.J.; Oxford, S.W.; Duncan, M.J. Does Perception of Motor Competence Mediate Associations between Motor Competence and Physical Activity in Early Years Children? Sports 2019, 7, 77. https://doi.org/10.3390/sports7040077
Hall CJS, Eyre ELJ, Oxford SW, Duncan MJ. Does Perception of Motor Competence Mediate Associations between Motor Competence and Physical Activity in Early Years Children? Sports. 2019; 7(4):77. https://doi.org/10.3390/sports7040077
Chicago/Turabian StyleHall, Charlotte J. S., Emma L. J. Eyre, Samuel W. Oxford, and Michael J. Duncan. 2019. "Does Perception of Motor Competence Mediate Associations between Motor Competence and Physical Activity in Early Years Children?" Sports 7, no. 4: 77. https://doi.org/10.3390/sports7040077
APA StyleHall, C. J. S., Eyre, E. L. J., Oxford, S. W., & Duncan, M. J. (2019). Does Perception of Motor Competence Mediate Associations between Motor Competence and Physical Activity in Early Years Children? Sports, 7(4), 77. https://doi.org/10.3390/sports7040077