Abstract
Heart failure with preserved ejection fraction (HFpEF) is a heterogeneous clinical syndrome with multiple underlying mechanisms and comorbidities that leads to a variety of clinical phenotypes. The identification and characterization of these phenotypes are essential for better understanding the precise pathophysiology of HFpEF, identifying appropriate treatment strategies, and improving patient outcomes. Despite accumulating data showing the potentiality of artificial intelligence (AI)-based phenotyping using clinical, biomarker, and imaging information from multiple dimensions in HFpEF management, contemporary guidelines and consensus do not incorporate these in daily practice. In the future, further studies are required to authenticate and substantiate these findings in order to establish a more standardized approach for clinical implementation.
1. Introduction
Heart failure with preserved ejection fraction (HFpEF) is diagnosed as heart failure with a left ventricular ejection fraction (LVEF) of ≥50% and elevated left ventricular filling pressures at rest or during exercise after careful exclusion of conditions that may mimic HFpEF [1,2]. HFpEF is a complex clinical syndrome that differs from other cardiovascular diseases, as it is defined by a combination of symptoms, signs, and other manifestations rather than a specific diagnostic test.
There is currently little evidence supporting the effectiveness of conventional therapies utilized for HFpEF to reduce mortality rates, such as empagliflozin in the EMPEROR-Preserved trial and dapagliflozin in the DELIVER trial. However, emerging research suggests that treatment should be tailored to the specific comorbidities present in each patient [3]. Some of the most common comorbidities seen in patients with heart failure include coronary artery disease, atrial fibrillation (AF), obesity, diabetes, renal impairment, and pulmonary hypertension. Accordingly, HFpEF can be classified into different phenotypes based on various criteria, including underlying etiology, clinical characteristics, and comorbidities [3,4,5,6,7,8]. Detailed molecular signaling, gene ontology functional analysis, and the use of the Kyoto Encyclopedia of Genes and Genomes pathway also potentiate the precise mechanisms of action and targets of SGLT2 inhibitors in clinical practice [9,10]. A comprehensive understanding and the specific pathways identified from HFpEF phenotyping also facilitate animal experimental studies to address relevant pathophysiological signaling [11].
2. Clinical Entities
Several studies have examined the relationship between HFpEF and clinical entities and comorbidities. For example, in the TOPCAT trial, it was discovered that patients with HFpEF who had been previously hospitalized for heart failure exhibited a greater likelihood of experiencing cardiovascular death, heart failure hospitalization, or aborted cardiac arrest than their counterparts who did not have a history of hospitalization [12]. The utilization of clustering methods shows great potential in addressing the heterogeneity of HFpEF and uncovering sub-phenotypes. Unbiased clustering methods have been used in recent studies to categorize distinct phenotypes among patients with HFpEF, taking into account their clinical characteristics, echocardiographic observations, and biomarker concentrations (Table 1).

Table 1.
Machine learning (ML) and latent class analysis (LCA) phenotyping of HFpEF.
Since the amount of healthcare data generated on a daily basis is overwhelming for a contemporary doctor, far surpassing the computational capacity of the human brain [25], machine learning (ML) and artificial intelligence (AI), which may use interchangeably, are increasingly being used in medical research to identify sub-phenotypes of diseases such as HFpEF. Artificial intelligence (AI) techniques are increasingly being used in medical research to identify sub-phenotypes of diseases such as HFpEF. These methods utilize statistical algorithms to analyze complex relationships between various patient characteristics and create distinct clusters that define sub-phenotypes of the disease. One technique is supervised learning, where an algorithm is trained on a pre-labeled dataset to predict outcomes based on new data. For example, machine learning (ML), does not rely on pre-labeled data and instead uses algorithms to identify patterns and relationships within the data. Latent class analysis (LCA) is a model-based clustering technique used in medical research to identify sub-phenotypes of diseases. LCA relies on a probabilistic model to describe the distribution of data, which is used to derive clusters from the data based on the probabilities that certain cases belong to certain latent classes, and relies less on a distance measure to find the clusters. Overall, these techniques offer promising tools and research approaches to identify sub-phenotypes of diseases such as HFpEF and can help to improve diagnosis, treatment, and prognosis from multiple dimensions, including clinical data, biomarkers, or imaging studies [7,13,23,26,27,28,29,30,31,32]. Herein, we listed several key landmark studies unraveling AI-based learning and phenotyping among the HFpEF population.
One method to subtype HFpEF is based on the presence of underlying clinical entities or comorbidities that contribute to the development and progression of the disease, known as clinical phenotyping (Figure 1A) [8]. The identification of specific clinical entities and comorbidities associated with different HFpEF phenotypes may have important clinical implications, as it may help guide the development of targeted therapies for these subtypes. For example, patients with HFpEF and pulmonary vascular disease may benefit from therapies that target pulmonary hypertension, whereas patients with HFpEF and metabolic dysfunction may benefit from weight loss and metabolic management strategies. Further, it has been proposed that certain natriuretic peptide deficiency syndrome may exist in HFpEF (e.g., obesity related HFpEF) [33]. Despite experiencing abnormally high left ventricular filling pressure during exercise, patients with this condition may benefit from treatment with a Neprilysin inhibitor, such as Entresto/Sacubitril (ARNi) [34]. Taken collectively, the optimal management for HFpEF can be tailored and personalized, targeting precision medicine in clinical practice [13,29].
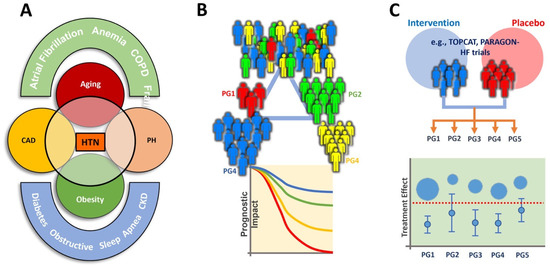
Figure 1.
Clinical phenotyping of HFpEF (A), AI-assisted or latent class analysis (LCA) HFpEF phenotyping (B), and treatment-based clustering (C). PG: phenogroup. Other abbreviations are as in Table 1. Panel (A) was modified and adopted [8].
Hwang et al. explored the implications of coronary artery disease (CAD) in HFpEF. The authors suggested that HFpEF patients with CAD have distinct clinical and pathophysiological characteristics compared with those without CAD. CAD may play a significant role in the progression of HFpEF, and a better understanding of this relationship could lead to the development of more effective treatments. This study provides insights into the clinical entity and underlying comorbidity of HFpEF, and it highlights the importance of considering these factors when defining and classifying HFpEF phenotypes [29].
Shah et al. identified distinct subgroups of HFpEF patients based on their comorbidities, including obesity-related comorbidities, metabolic syndrome, and pulmonary hypertension. This study showed that these subtypes had distinct clinical, biochemical, and imaging profiles, suggesting that they may represent different disease processes. The authors proposed that this phenomapping model-based clustering approach could be used to tailor treatments to individual patients and to improve outcomes in HFpEF [13] (Figure 1B).
Borlaug et al. investigated the associations between specific clinical entities, comorbidities, and HFpEF subtypes. Their study included 344 patients with HFpEF who were classified into four subtypes, based on the clinical entities or comorbidities present, as follows: (1) obesity-related, (2) hypertension-related, (3) diabetes-related, and (4) idiopathic. According to this research, the HFpEF subtype associated with obesity showed a greater prevalence of metabolic risk factors and more severe diastolic dysfunction compared to the other subtypes. The hypertension-related HFpEF subtype had a higher prevalence of left ventricular hypertrophy, concentric remodeling, and worse systolic function. The diabetes-related HFpEF subtype had a higher prevalence of diabetic nephropathy, worse systolic function, and more severe diastolic dysfunction. The idiopathic HFpEF subtype had a lower prevalence of comorbidities and less severe diastolic dysfunction than the other subtypes [8].
Uijl et al. proposed a five-cluster model, labeled Cluster 1 and Clusters 2–5, among 6909 HFpEF from the Swedish Heart Failure Registry (SwedeHF) and externally validated this in 2153 patients from the Chronic Heart Failure ESC-guideline based Cardiology practice Quality project (CHECK-HF) registry, as shown in Figure 2. Cluster 1 included young patients with low comorbidity burdens and the highest proportion of implantable devices. Cluster 2 included patients with AF and hypertension without diabetes. Cluster 3 included the oldest patients with the most cardiovascular comorbidities. Cluster 4 included patients with obesity, diabetes, and hypertension. Cluster 5 included older patients with ischemic heart disease, hypertension, and renal failure; these patients were most frequently prescribed diuretics. With this clustering, patients in the same cluster may have more homogeneity, which may contribute to more beneficial medical therapies. Patients in the young–low comorbidity burden cluster had the lowest event rates, while patients in the older–AF and cardio–renal clusters had the highest event rates [23].
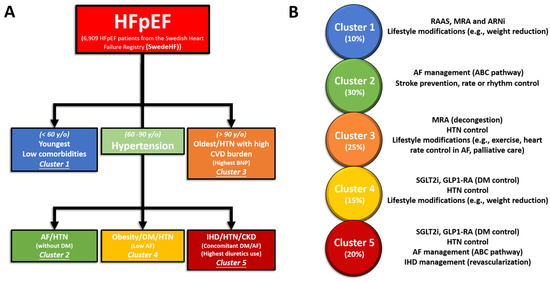
Figure 2.
Schematic diagram showing characteristics for the 5 major phenotypic clusters of HFpEF from SwedeHF (n = 6909) (A) calculated with an LCA and externally validated in CHECK-HF (n = 2153). Percentage and treatment strategies of these HFpEF populations in the whole study cohort (B).
3. Imaging
Cardiac imaging and measurement of the cardiac structure are critical aspects in diagnosing HFpEF, as the symptoms of this condition can be nonspecific. Non-invasive measures of cardiac structure and function can assist in improving diagnostic accuracy and differentiating the sub-phenotypes of HFpEF. Additionally, imaging can exclude alternative diagnoses that mimic HFpEF, such as hypertrophic cardiomyopathy, primary valvular heart disease, cardiac amyloidosis, and pericardial disease. While two-dimensional (2-D) transthoracic echocardiography is the most commonly used imaging modality, advanced imaging techniques, including cardiac magnetic resonance imaging and 2-D speckle tracking echocardiography, are used to identify distinct HFpEF phenotypes based on left ventricular structure and function [13,23,28,29,30,31,32,35]. Compared with standard 2-D echocardiography, three-dimensional (3-D) echocardiography provides a more reliable and reproducible evaluation of cardiac chamber volumes, mass, and shape, which are highly correlated with cardiac magnetic resonance imaging (CMR) [36]. CMR provides comprehensive information on morphology, function, perfusion, viability, and tissue characteristics. CMR can detect fibrosis, lipid content, and energy metabolism, making it a valuable tool for assessing suspected CAD and detecting coronary microvascular disease (CMD) in the future [37].
Several studies have investigated the use of echocardiography to identify the imaging-based phenotypes of HFpEF. Diastolic dysfunction, a hallmark feature of HFpEF, has been well adopted in the initial classification of HFpEF [38]. One study used a combination of 2-D speckle-tracking echocardiography and CMR to identify three distinct phenotypes based on left ventricular structure and function [38]. These phenotypes included left ventricular hypertrophy with preserved global longitudinal strain (GLS), left atrial enlargement with normal GLS, and normal left ventricular and left atrial structures with impaired GLS. The aforementioned study found that these phenotypes were associated with different clinical and biochemical features and may have different prognostic implications [23,35,38].
Another study evaluated left atrial function using 2-D speckle tracking echocardiography and found that left atrial strain was significantly decreased in patients with HFpEF compared with that in controls. The study also found that left atrial strain was independently associated with a higher risk of adverse events, including hospitalization and mortality [39].
Cardiac imaging and measures of cardiac structure and function are essential for diagnosing HFpEF, excluding alternative diagnoses, and identifying imaging-based phenotypes. Although 2-D echocardiography remains the most commonly used imaging modality, CMR and 3-D echocardiography offer more comprehensive information regarding cardiac structure and function. These imaging techniques may have important prognostic implications and help guide management strategies in patients with HFpEF.
4. Management of HFpEF Phenotype Based on “SwedeHF” and “CHECK-HF” Registries
Personalized management of different HFpEF phenotypes using clustering targeting more specific molecular or pathological etiology driving underlying mechanisms has been proposed in several studies [27,40,41,42]. For example, obesity-related HFpEF with or without hyperlipidemia or diabetes may benefit from combined sodium–glucose cotransporter-2 inhibitors (SGLT2i), mineralocorticoid receptor antagonists (MRA), and angiotensin receptors/neprilysin inhibitor (ARNi) due to an inner deficiency of effective natriuretic peptide from excessive visceral adiposity [43]. Herein, we provided an example of the possible therapeutic implications of performing phenotyping among the HFpEF population using findings from the “SwedeHF” and “CHECK-HF” registries [23]. Despite being promising, these studies may warrant further external validations that can be applicable across different races with wide clinical settings to show how these findings can be interpreted practically and implemented from the working hypotheses (Table 2). Thus, these findings and their implications should be discussed in the broadest context possible.
Table 2.
Simple summary table for management of specific HFpEF phenotypes based on the “SwedeHF” and “CHECK-HF” registries.
4.1. Cluster 1
Among the five clusters, patients with HFpEF in this group had a median age of 59 years and a relatively low burden of comorbidities, making them the youngest of the cohorts. The most common comorbidities in Cluster 1 were hypertension (46%) and obesity (42%). The principles of management for this group are to control blood pressure and reduce body weight. It is worth mentioning that cluster 1 includes patients who have recovered HFrEF, due to the higher percentage of implantable cardioverter-defibrillator or cardiac resynchronization therapy.
In addition to the implantable devices, quite a few medications have demonstrated an established efficacy in previous HFpEF trials. Those drugs were renin–angiotensin–aldosterone system (RAAS) antagonists such as angioten-sin-converting enzyme inhibitors (ACEis), angiotensin II receptor blockers (ARBs), mineralocorticoid receptor antagonists (MRAs), and angiotensin receptors/neprilysin inhibitor (ARNi), which could be considered as first-line agents for the management of HFpEF. Lifestyle modifications were strongly suggested for this cluster. Significant improvements in quality of life and exercise tolerance were observed as a result of weight reduction, which was found to be safe. In addition to these benefits, weight loss in patients with HFpEF has been shown to have a positive impact on cardiac function and metabolic parameters, potentially leading to reduced doses of diuretics, antihypertensive agents, and diabetes medications.
4.2. Cluster 2
The individuals belonging to Cluster 2 were relatively older compared to those in Cluster 1, having a median age of 77 years. This cluster included patients with HFpEF characterized by AF without diabetes. Principles of management for this cluster align with the AF Better Care (ABC) pathway, including rate/rhythm control in AF management, as follows: (A) avoiding thromboembolic events with the use of anticoagulation. (B) better management of symptoms with personalized, symptom-directed decisions on rate or rhythm control. Rate control involves the use of beta-blockers/non-dihydropyridine (DHP) calcium channel blockers (CCBs) (diltiazem or verapamil)/digoxin; rhythm control involves the use of amiodarone/dronedarone or AF ablation. (C) Effective management of cardiovascular and coexisting conditions, including attention to psychological factors and lifestyle. Following the ABC pathway has been shown to lead to improved outcomes, including decreased risks of all-cause mortality, cardiovascular mortality, stroke, and hospitalization due to cardiovascular reasons. It is important to avoid excessive rate control in patients with both HFpEF and AF, as it may diminish their chronotropic reserve. In a trial comparing strict (<80 bpm) and lenient (<110 bpm) rate control in patients with AF, which may have included individuals with undiagnosed HFpEF, no significant differences in outcomes were observed.
4.3. Cluster 3
Among the five clusters, Cluster 3 patients were the oldest (median age, 88 years) with the highest N-terminal pro b-type natriuretic peptide (NT-proBNP) values. It was reasonable to eliminate any meaningful clinical phenotyping for this cluster, as it presented with an anticipated higher risk for an ominous outcome. Clinically, the principle of for the elderly is to reduce hospitalization rates and improve quality of life. Decongestion of diuretics has been shown to reduce hospitalization rates. In the TOPCAT trial, spironolactone was associated with a decrease in heart failure hospitalization rates compared with the placebo [12]. This cluster can be effectively managed with measures such as controlling heart rate in patients with AF, optimizing blood pressure control, and implementing lifestyle interventions such as exercise training to enhance functional capacity. When life comes to an end, palliative care, including symptom management and psychological, emotional, and spiritual support, should be properly offered to patients and caregivers throughout the disease course, not only in advanced stages.
4.4. Cluster 4
Cluster 4 was composed of patients who had a median age of 71 years and were identified as having diabetes but not AF. Serum glucose control is the mainstay of this cluster. SGLT2 inhibitors have emerged as a critical component of HFrEF therapy as they possess favorable pleiotropic effects on various body parts such as the kidney, liver, pancreas, blood vessels, and adipose tissue, apart from their primary role as an antidiabetic medication. The EMPEROR-Preserved trial was groundbreaking in the study of HFpEF as it compared the effects of empagliflozin with a placebo in patients with ejection fractions above 40%, irrespective of whether they had diabetes or not. The trial demonstrated a significant reduction in the risk of heart failure-related hospitalizations and cardiovascular mortality, as well as an improvement in renal outcomes.
According to the DELIVER trial, dapagliflozin is superior to placebos in decreasing cardiovascular deaths and hospitalizations due to heart failure in patients with mildly reduced or preserved ejection fractions. Additionally, the study showed that dapagliflozin was effective in patients who previously had ejection fractions below 40% but later saw an increase to over 40%.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are also associated with positive cardiovascular effects. A recent meta-analysis involving 592 patients revealed that liraglutide was connected with significant enhancements in the left ventricular diastolic function.
4.5. Cluster 5
Cluster 5 was a union of Clusters 2 and 4. This cluster had a median age of 82 years, and its members had comorbidities of both diabetes and AF. In the DECLARE-TIMI 58 trial (Multicenter Trial to Evaluate the Effect of Dapagliflozin on the Incidence of Cardiovascular Events), dapagliflozin reduced the incidence of AF in patients with diabetes [44]. Efforts for Clusters 2 and 4 should be applied to this cluster, including the ABC pathway for the management of AF and SGLT2i for diabetes.
5. Management of Obesity-Related HFpEF Phenotype
Obesity as a common etiology and co-morbidity for HFpEF has been shown to induce activated sympathetic system and RAAS (and thus hyperaldosteronism with sodium retention) and further promote systemic inflammation [45,46], which may subsequently augment impaired cardiac filling conditions and aggravate unfavorable cardiac remodeling and HF progression [47,48]. Hence, HFrEF patients with central obesity are particularly prone to therapeutic benefits with eplerenone use [49].
Elevated circulating levels of aldosterone, either directly from adipocytes or released from the adrenal gland in response to leptin through the adipokines-cell-signaling molecules secreted (from central obesity or visceral adipose tissue), along with the attenuated anti-aldosterone effects from natriuretic peptides due to an increased neprilysin activity in obesity, may potentiate [50] the deleterious effect of neprilysin HF patients with obesity regardless of HF phenotypes [33]. This “leptin-aldosterone-neprilysin axis activation”, when observed in part as natriuretic peptide deficiency syndrome, as observed in obesity-related HFpEF pathophysiology, may exacerbate the interaction of leptin and aldosterone to promote sodium retention, plasma volume expansion, and regional (such as myocardial) and systemic inflammation and fibrosis (Figure 3) [23,33,43,51].
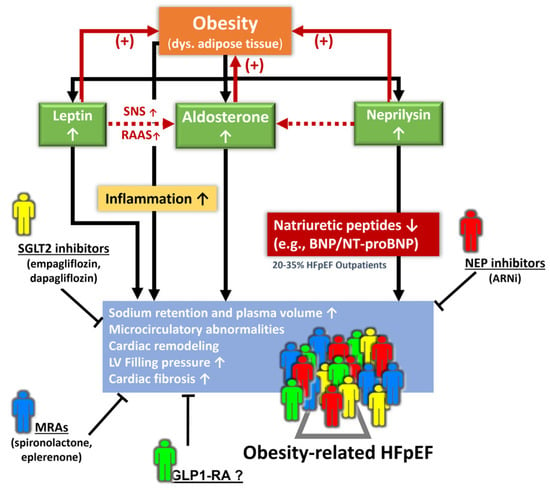
Figure 3.
Pathophysiological signaling from the leptin–aldosterone–neprilysin axis activation underlying obesity-related HFpEF and potential diverse phenotypes for pharmacological interventions. ARNi: angiotensin receptor-neprilysin inhibitor; Dys.: dysregulated; GLP1-RA: glucagon-like peptide-1 receptor agonist; MRA: mineralocorticoid receptor antagonist; NEP: neprilysin; RAAS: renin–angiotensin–aldosterone system; SNS: sympathetic nervous system.
Importantly, an activated leptin–aldosterone–neprilysin axis with sustained increases in aldosterone and neprilysin concentration may in turn accelerate the accumulation and inflammation of epicardial fat [52,53]. Recently, proteomics in the LIFE-Heart study (further verified in the Aldo-DHF validation cohort) targeting biomarkers involving volume expansion, myocardial fibrosis, and systemic inflammation has been shown to improve obesity-related HFpEF [54] phenotyping with a distinct biomarker signature. However, whether there may exist some clinical features (e.g., central obesity, region-specific adiposity, e.g., pericardial fat burden) with therapeutic implications using AI-assisted machine learning or clustering may warrant further research (Figure 3).
6. Conclusions
In summary, the identification and characterization of HFpEF phenotypes are important for guiding diagnosis, management, and research into novel treatment strategies. It was a prerequisite for us to identify that the presence of ischemic heart disease by itself induces prognostic implications. Given the complexity of HFpEF, a personalized approach to management that considers the underlying mechanisms and comorbidities in each patient is needed and might help to solve the puzzle of this challenging syndrome.
Author Contributions
Conceptualization and investigation, C.-L.H. and C.-T.T.; methodology and validation, H.-Y.S.; software and data curation, C.J.-Y.H.; formal analysis and resources, Y.-J.C.; writing—original draft preparation and visualization, C.-Y.L.; writing—review and editing, H.-I.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This study was further supported by the National Science Council (NSC) (101-2314-B-195-020, 103-2314-B-010-005-MY3, 103-2314-B-195-001-MY3, 101-2314-B-195-020-MY1), the Ministry of Science and Technology (MOST) (103-2314-B-195-006-MY3, 106-2314-B-195-008-MY2, 108-2314-B-195-018-MY2, 109-2314-B-715-008, 110-2314-B-715-009-MY1, 111-2314-B-715-013), MacKay Memorial Hospital (10271, 10248, 10220, 10253, 10375, 10358, E-102003, MMH-108-127, MMH-110-114, MMH-110-03), and MacKay Medical College (MMC-RD-109-1B-18, MMC-RD-108-2B-02; MMC-RD-109-1B-18; MMC-RD-110-CF-G001-02; MMC-RD-111-1B-P025; MMC-RD-111-CF-G001-02).
Institutional Review Board Statement
Ethical review and approval were waived for this study due to its review article nature and no study participants enrolled.
Data Availability Statement
Because of the review nature for this article, requests to access the dataset from qualified researchers are not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Gevaert, A.B.; Kataria, R.; Zannad, F.; Sauer, A.J.; Damman, K.; Sharma, K.; Shah, S.J.; Van Spall, H.G.C. Heart failure with preserved ejection fraction: Recent concepts in diagnosis, mechanisms and management. Heart 2022, 108, 1342–1350. [Google Scholar] [CrossRef]
- Vasan, R.S.; Levy, D. Defining diastolic heart failure: A call for standardized diagnostic criteria. Circulation 2012, 131, 1824–1831. [Google Scholar] [CrossRef] [PubMed]
- Reddy, Y.N.V.; Carter, R.E.; Obokata, M.; Redfield, M.M.; Borlaug, B.A. A simple, evidence-based approach to help guide diagnosis of heart failure with preserved ejection fraction. Circulation 2018, 138, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, M.A.; Shah, A.M.; Borlaug, B.A. Heart failure with preserved ejection fraction in perspective. Circ. Res. 2019, 124, 1598–1617. [Google Scholar] [CrossRef] [PubMed]
- Lindman, B.R.; Dávila-Román, V.G.; Mann, D.L.; McNulty, S.; Semigran, M.J.; Lewis, G.D.; de las Fuentes, L.; Joseph, S.M.; Vader, J.; Hernandez, A.F.; et al. Cardiovascular phenotype in HFpEF patients with or without diabetes: A RELAX trial ancillary study. J. Am. Coll. Cardiol. 2014, 64, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Samson, R.; Jaiswal, A.; Ennezat, P.V.; Cassidy, M.; Le Jemtel, T.H. Clinical Phenotypes in Heart Failure with Preserved Ejection Fraction. J. Am. Heart Assoc. 2016, 5, e002477. [Google Scholar] [CrossRef]
- Almengló, C.; Fu, X.; Flores-Arias, M.T.; Fernández, Á.L.; Viñuela, J.E.; Martínez-Cereijo, J.M.; Durán, D.; Rodríguez-Mañero, M.; González-Juanatey, J.R.; Eiras, S. Synergism between obesity and HFpEF on neutrophils phenotype and its regulation by adipose tissue-molecules and SGLT2i dapagliflozin. J. Cell. Mol. Med. 2022, 26, 4416–4427. [Google Scholar] [CrossRef]
- Wang, A.; Li, Z.; Zhuo, S.; Gao, F.; Zhang, H.; Zhang, Z.; Ren, G.; Ma, X. Mechanisms of Cardiorenal Protection with SGLT2 Inhibitors in Patients with T2DM Based on Network Pharmacology. Front. Cardiovasc. Med. 2022, 9, 857952. [Google Scholar] [CrossRef]
- Van Ham, W.B.; Kessler, E.L.; Oerlemans, M.I.F.J.; Handoko, M.L.; Sluijter, J.P.G.; van Veen, T.A.B.; den Ruijter, H.M.; de Jager, S.C.A. Clinical Phenotypes of Heart Failure with Preserved Ejection Fraction to Select Preclinical Animal Models. JACC Basic Transl. Sci. 2022, 7, 844–857. [Google Scholar] [CrossRef] [PubMed]
- Pitt, B.; Pfeffer, M.A.; Assmann, S.F.; Boineau, R.; Anand, I.S.; Claggett, B.; Clausell, N.; Desai, A.S.; Diaz, R.; Fleg, J.L.; et al. Spironolactone for heart failure with preserved ejection fraction. N. Engl. J. Med. 2014, 370, 1383–1392. [Google Scholar] [CrossRef]
- Shah, S.J.; Katz, D.H.; Selvaraj, S.; Burke, M.A.; Yancy, C.W.; Gheorghiade, M.; Bonow, R.O.; Huang, C.C.; Deo, R.C. Phenomapping for novel classification of heart failure with preserved ejection fraction. Circulation 2015, 131, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Martinez, S.; Duchateau, N.; Erdei, T.; Kunszt, G.; Aakhus, S.; Degiovanni, A.; Marino, P.; Carluccio, E.; Piella, G.; Fraser, A.G.; et al. Machine Learning Analysis of Left Ventricular Function to Characterize Heart Failure with Preserved Ejection Fraction. Circ. Cardiovasc. Imaging 2018, 11, e007138. [Google Scholar] [CrossRef] [PubMed]
- Przewlocka-Kosmala, M.; Marwick, T.H.; Dabrowski, A.; Kosmala, W. Contribution of Cardiovascular Reserve to Prognostic Categories of Heart Failure with Preserved Ejection Fraction: A Classification Based on Machine Learning. J. Am. Soc. Echocardiogr. 2019, 32, 604–615.e6. [Google Scholar] [CrossRef] [PubMed]
- Segar, M.W.; Patel, K.V.; Ayers, C.; Basit, M.; Tang, W.W.; Willett, D.; Berry, J.; Grodin, J.L.; Pandey, A. Phenomapping of patients with heart failure with preserved ejection fraction using machine learning-based unsupervised cluster analysis. Eur. J. Heart Fail. 2020, 22, 148–158. [Google Scholar] [CrossRef]
- Hedman, Å.K.; Hage, C.; Sharma, A.; Brosnan, M.J.; Buckbinder, L.; Gan, L.M.; Shah, S.J.; Linde, C.M.; Donal, E.; Daubert, J.-C.; et al. Identification of novel pheno-groups in heart failure with preserved ejection fraction using machine learning. Heart 2020, 106, 342–349. [Google Scholar] [CrossRef]
- Schrub, F.; Oger, E.; Bidaut, A.; Hage, C.; Charton, M.; Daubert, J.C.; Leclercq, C.; Linde, C.; Lund, L.; Donal, E. Heart failure with preserved ejection fraction: A clustering approach to a heterogenous syndrome. Arch. Cardiovasc. Dis. 2020, 113, 381–390. [Google Scholar] [CrossRef]
- Woolley, R.J.; Ceelen, D.; Ouwerkerk, W.; Tromp, J.; Figarska, S.M.; Anker, S.D.; Dickstein, K.; Filippatos, G.; Zannad, F.; Metra, M.; et al. Machine learning based on biomarker profiles identifies distinct subgroups of heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2021, 23, 983–991, Correction in Eur. J. Heart Fail. 2021, 1802. [Google Scholar] [CrossRef]
- Gu, J.; Pan, J.A.; Lin, H.; Zhang, J.F.; Wang, C.Q. Characteristics, prognosis and treatment response in distinct phenogroups of heart failure with preserved ejection fraction. Int. J. Cardiol. 2021, 323, 148–154. [Google Scholar] [CrossRef]
- Kao, D.P.; Lewsey, J.D.; Anand, I.S.; Massie, B.M.; Zile, M.R.; Carson, P.E.; McKelvie, R.S.; Komajda, M.; McMurray, J.J.V.; Lindenfeld, J. Characterization of subgroups of heart failure patients with preserved ejection fraction with possible implications for prognosis and treatment response. Eur. J. Heart Fail. 2015, 17, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.B.; Schrauben, S.J.; Zhao, L.; Basso, M.D.; Cvijic, M.E.; Li, Z.; Yarde, M.; Wang, Z.; Bhattacharya, P.T.; Chirinos, D.A.; et al. Clinical Phenogroups in Heart Failure with Preserved Ejection Fraction: Detailed Phenotypes, Prognosis, and Response to Spironolactone. JACC Heart Fail. 2020, 8, 172–184. [Google Scholar] [CrossRef] [PubMed]
- Uijl, A.; Savarese, G.; Vaartjes, I.; Dahlström, U.; Brugts, J.J.; Linssen, G.C.M.; van Empel, V.; Brunner-La Rocca, H.P.; Asselbergs, F.W.; Lund, L.H.; et al. Identification of distinct phenotypic clusters in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2021, 23, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Rucker, D.; Joseph, J. Defining the Phenotypes for Heart Failure with Preserved Ejection Fraction. Curr. Heart Fail. Rep. 2022, 19, 445–457. [Google Scholar] [CrossRef]
- Kresoja, K.P.; Unterhuber, M.; Wachter, R.; Thiele, H.; Lurz, P. A cardiologist’s guide to machine learning in cardiovascular disease prognosis prediction. Basic Res. Cardiol. 2023, 118, 10. [Google Scholar] [CrossRef]
- Casebeer, A.; Horter, L.; Hayden, J.; Simmons, J.; Evers, T. Phenotypic clustering of heart failure with preserved ejection fraction reveals different rates of hospitalization. J. Cardiovasc. Med. 2021, 22, 45–52. [Google Scholar] [CrossRef]
- Shah, S.J.; Kitzman, D.W.; Borlaug, B.A.; van Heerebeek, L.; Zile, M.R.; Kass, D.A.; Paulus, W.J. Phenotype-Specific Treatment of Heart Failure with Preserved Ejection Fraction: A Multiorgan Roadmap. Circulation 2016, 134, 73–90. [Google Scholar] [CrossRef]
- Zawadzka, M.M.; Grabowski, M.; Kapłon-Cieślicka, A. Phenotyping in heart failure with preserved ejection fraction: A key to find effective treatment. Adv. Clin. Exp. Med. 2022, 31, 1163–1172. [Google Scholar] [CrossRef]
- Hwang, S.J.; Melenovsky, V.; Borlaug, B.A. Implications of coronary artery disease in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 2014, 64, 1702–1713. [Google Scholar] [CrossRef]
- Tsujimoto, T.; Kajio, H. Spironolactone Use and Improved Outcomes in Patients with Heart Failure with Preserved Ejection Fraction with Resistant Hypertension. J. Am. Heart Assoc. 2020, 9, e018827. [Google Scholar] [CrossRef]
- Jackson, A.M.; Jhund, P.S.; Anand, I.S.; Düngen, H.-D.; Lam, C.S.P.; Lefkowitz, M.P.; Linssen, G.; Lund, L.H.; Maggioni, A.P.; Pfeffer, M.A.; et al. Sacubitril-valsartan as a treatment for apparent resistant hypertension in patients with heart failure and preserved ejection fraction. Eur. Heart J. 2021, 42, 3741–3752. [Google Scholar] [CrossRef] [PubMed]
- Karwath, A.; Bunting, K.V.; Gill, S.K.; Tica, O.; Pendleton, S.; Aziz, F.; Barsky, A.D.; Chernbumroong, S.; Duan, J.; Mobley, A.R.; et al. Redefining β-blocker response in heart failure patients with sinus rhythm and atrial fibrillation: A machine learning cluster analysis. Lancet 2021, 398, 1427–1435. [Google Scholar] [CrossRef] [PubMed]
- Verbrugge, F.H.; Omote, K.; Reddy, Y.N.V.; Sorimachi, H.; Obokata, M.; Borlaug, B.A. Heart failure with preserved ejection fraction in patients with normal natriuretic peptide levels is associated with increased morbidity and mortality. Eur. Heart J. 2022, 43, 1941–1951. [Google Scholar] [CrossRef] [PubMed]
- Packer, M. Leptin-Aldosterone-Neprilysin Axis: Identification of Its Distinctive Role in the Pathogenesis of the Three Phenotypes of Heart Failure in People with Obesity. Circulation 2018, 137, 1614–1631. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, S.F.; Hussain, I.; AbouEzzeddine, O.F.; Takahama, H.; Kwon, S.H.; Forfia, P.; Roger, V.L.; Redfield, M.M. Right ventricular function in heart failure with preserved ejection fraction: A community-based study. Circulation 2014, 130, 2310–2320. [Google Scholar] [CrossRef]
- Benameur, N.; Arous, Y.; Ben Abdallah, N.; Kraiem, T. Comparison between 3D Echocardiography and Cardiac Magnetic Resonance Imaging (CMRI) in the Measurement of Left Ventricular Volumes and Ejection Fraction. Curr. Med. Imaging Rev. 2019, 15, 654–660. [Google Scholar] [CrossRef]
- Liu, A.; Wijesurendra, R.S.; Liu, J.M.; Forfar, J.C.; Channon, K.M.; Jerosch-Herold, M.; Piechnik, S.K.; Neubauer, S.; Kharbanda, R.K.; Ferreira, V.M. Diagnosis of Microvascular Angina Using Cardiac Magnetic Resonance. J. Am. Coll. Cardiol. 2018, 71, 969–979, Retraction in J. Am. Coll. Cardiol. 2020, 76, 1916. [Google Scholar] [CrossRef]
- Obokata, M.; Reddy, Y.N.V.; Borlaug, B.A. Diastolic dysfunction and heart failure with preserved ejection fraction: Understanding mechanisms by using noninvasive methods. JACC Cardiovasc. Imaging 2019, 13, 245–257. [Google Scholar]
- Bolog, M.; Dumitrescu, M.; Luminiţa, M.; Romanoschi, F.; Păcuraru, E.; Râpă, A. Left Atrial Longitudinal Strain Evaluated by 2D Speckle Tracking Echocardiography Can Identify Patients with Heart Failure with Preserved Ejection Fraction. Intern. Med. 2019, 16, 7–19. [Google Scholar] [CrossRef]
- Aimo, A.; Senni, M.; Barison, A.; Panichella, G.; Passino, C.; Bayes-Genis, A.; Emdin, M. Management of heart failure with preserved ejection fraction: From neurohormonal antagonists to empagliflozin. Heart Fail. Rev. 2023, 28, 179–191. [Google Scholar] [CrossRef]
- Sotomi, Y.; Hikoso, S.; Nakatani, D.; Okada, K.; Dohi, T.; Sunaga, A.; Kida, H.; Sato, T.; Matsuoka, Y.; Kitamura, T.; et al. Medications for specific phenotypes of heart failure with preserved ejection fraction classified by a machine learning-based clustering model. Heart 2023. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Galli, E.; Bourg, C.; Kosmala, W.; Oger, E.; Donal, E. Phenomapping Heart Failure with Preserved Ejection Fraction Using Machine Learning Cluster Analysis: Prognostic and Therapeutic Implications. Heart Fail. Clin. 2021, 17, 499–518. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Kitzman, D.W. Obesity-Related Heart Failure with a Preserved Ejection Fraction: The Mechanistic Rationale for Combining Inhibitors of Aldosterone, Neprilysin, and Sodium-Glucose Cotransporter-2. JACC Heart Fail. 2018, 6, 633–639. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. DECLARE–TIMI 58 Investigators. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Marwick, T.H. Obesity cardiomyopathy: Pathogenesis and pathophysiology. Nat. Clin. Pract. Cardiovasc. Med. 2007, 4, 436–443. [Google Scholar] [CrossRef]
- Fontana, L.; Eagon, J.C.; Trujillo, M.E.; Scherer, P.E.; Klein, S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. Diabetes 2007, 56, 1010–1013. [Google Scholar] [CrossRef]
- Catena, C.; Colussi, G.; Brosolo, G.; Novello, M.; Sechi, L.A. Aldosterone and left ventricular remodeling. Horm. Metab. Res. 2015, 47, 981–986. [Google Scholar] [CrossRef]
- Abbasi, S.A.; Hundley, W.G.; Bluemke, D.A.; Jerosch-Herold, M.; Blankstein, R.; Petersen, S.E.; Rider, O.J.; Lima, J.A.; Allison, M.A.; Murthy, V.L.; et al. Visceral adiposity and left ventricular remodeling: The Multi-Ethnic Study of Atherosclerosis. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 667–676. [Google Scholar] [CrossRef]
- Olivier, A.; Pitt, B.; Girerd, N.; Lamiral, Z.; Machu, J.L.; McMurray, J.J.V.; Swedberg, K.; van Veldhuisen, D.J.; Collier, T.J.; Pocock, S.J.; et al. Effect of eplerenone in patients with heart failure and reduced ejection fraction: Potential effect modification by abdominal obesity: Insight from the EMPHASIS-HF trial. Eur. J. Heart Fail. 2017, 19, 1186–1197. [Google Scholar] [CrossRef]
- Gruden, G.; Landi, A.; Bruno, G. Natriuretic peptides, heart, and adipose tissue: New findings and future developments for diabetes research. Diabetes Care 2014, 37, 2899–2908. [Google Scholar] [CrossRef]
- Packer, M. Derangements in adrenergic-adipokine signalling establish a neurohormonal basis for obesity-related heart failure with a preserved ejection fraction. Eur. J. Heart Fail. 2018, 20, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Standeven, K.F.; Hess, K.; Carter, A.M.; Rice, G.I.; Cordell, P.A.; Balmforth, A.J.; Lu, B.; Scott, D.J.; Turner, A.J.; Hooper, N.M.; et al. Neprilysin, obesity and the metabolic syndrome. Int. J. Obes. 2011, 35, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Petramala, L.; Marinelli, C.; Calvieri, C.; Zinnamosca, L.; Concistrè, A.; Iannucci, G.; De Toma, G.; Letizia, C. Epicardial fat thickness and primary aldosteronism. Horm. Metab. Res. 2016, 48, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Kresoja, K.-P.; Rommel, K.-P.; Wachter, R.; Henger, S.; Besler, C.; Klöting, N.; Schnelle, M.; Hoffmann, A.; Büttner, P.; Ceglarek, U.; et al. Proteomics to improve phenotyping in obese patients with heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2021, 23, 1633–1644. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).