Abstract
Purpose: This study aimed to investigate the association between total serum cholesterol levels and outcomes upon discharge in patients after out-of-hospital cardiac arrest (OHCA). Methods: We performed a retrospective observational study using the Korean Cardiac Arrest Resuscitation Consortium (KoCARC) registry. Patients after OHCA whose total serum cholesterol levels were measured within 24 h after arriving at the emergency department were included in the analysis. The association between total serum cholesterol level and neurological outcomes upon discharge and survival to discharge was estimated. Results: Of the 12,321 patients after OHCA enrolled in the registry from October 2015 to June 2020, 689 patients were included. The poor neurologic outcome upon discharge group had a statistically significant lower total serum cholesterol level compared to the good neurologic outcome group (127.5 ± 45.1 mg/dL vs. 155.1 ± 48.9 mg/dL, p < 0.001). As a result of multivariate logistic regression analysis, the odds ratio for the neurologic outcome of total serum cholesterol levels was 2.00 (95% confidence interval [CI] 1.01–3.96, p = 0.045). The odds ratio for in-hospital death was 1.72 (95% CI 1.15–2.57, p = 0.009). Conclusions: Low total serum cholesterol levels could be associated with poor neurologic outcomes upon discharge and in-hospital death of patients hospitalized after OHCA.
1. Introduction
An ischemia-reperfusion injury occurs during cardiac arrest and return of spontaneous circulation (ROSC) after cardiopulmonary resuscitation (CPR), and these injuries are comprehensively referred to as post-cardiac arrest syndrome [1].
The pathophysiology of post-cardiac arrest syndrome is complex [2]. During the ischemia period, cellular oxygen storage due to low metabolism is reduced, and prolonged periods cause cellular and tissue damage. Oxidative free radicals are induced by reperfusion injury from chest compressions or ROSC. Oxidative free radicals result in disseminated endothelial injuries and apoptosis, and prolonged injuries lead to a systemic inflammatory response and multiple organ failure [3,4,5,6]. The pathophysiology of ischemia-reperfusion injury is similar to that of sepsis [7].
Hypercholesterolemia is associated with coronary artery disease and stroke. Atherosclerosis occurs when low-density lipoprotein (LDL) particles accumulate in the subendothelial space of the arteries, which causes coronary artery disease and stroke. In addition, untreated dyslipidemia is one of the strongest causes of in-hospital mortality due to coronary artery disease [8].
On the other hand, contrary to the generally accepted theories that low cholesterol levels are good, several studies have shown that low serum cholesterol level is associated with incidence of cancer risk and poor prognosis and mortality of patients of sepsis [9,10,11].
Cholesterol plays a major role in diseases causing critical illness. In general, severe diseases are associated with a catabolic stress state for the systemic inflammatory response [12]. Lipoproteins bind and remove toxic bacterial toxins and endotoxins during the systemic inflammatory response [13,14,15]. Patients with post-ROSC have systemic inflammatory responses similar to those in other patients who are critically ill.
The aim of this study was to assess the association between serum cholesterol levels and outcomes of patients hospitalized after out-of-hospital cardiac arrest (OHCA). We hypothesized that resuscitated patients with initial low serum cholesterol levels would have a poor outcome at survival to discharge.
2. Material and Methods
2.1. Study Design and Setting
This study was conducted as a multicenter retrospective observational study using the Korean Cardiac Arrest Resuscitation Consortium (KoCARC) registry, a nationwide OHCA registry based on the Utstein templates, and a hospital-based collaborative research network. In addition, it is a data collection system designed to effectively and professionally study evidence for strengthening the survival chain of patients who experience out-of-hospital cardiac arrest [16].
The KoCARC registry included patients who were brought to the participating emergency department by the emergency medical services with resuscitation efforts after OHCA. Patients who experience cardiac arrest of definite non-medical etiology, such as trauma, poisoning, burns, drowning, asphyxia, or hanging, were excluded. Patients with terminal stage illnesses documented in medical records, patients under hospice care, patients with previously documented do-not-resuscitate orders, and pregnant patients were also excluded.
The KoCARC is an organized collaborative research network, which consists of seven research committees, including Epidemiology and Preventive Research, Community Resuscitation Research, EMS Resuscitation Research, Hospital Resuscitation Research, Hypothermia and Post-resuscitation Care Research, Cardiac Care Resuscitation, and Pediatric Resuscitation Research Committees, in which each committee has core and supplemental variables.
The study was approved by the Institutional Review Board (IRB) of the participating hospitals. Informed consent was waived by the IRB due to the retrospective study. The project was registered at the ClinicalTrials.gov (identifier: NCT03222999).
2.2. Study Participants
We included patients enrolled in the KoCARC registry from October 2015 to June 2020. The following patients were included in this study: (1) adult patients aged ≥18 years, (2) patients who were hospitalized after OHCA and had successful ROSC at the hospital, (3) patients whose serum total cholesterol levels were measured within 24 h after arriving at the emergency department, and (4) patients with cerebral performance category (CPC) information upon discharge. This study excluded (1) patients aged <18 years, (2) patients who did not survive upon hospital admission, (3) patients who had prehospital ROSC, (4) patients whose serum total cholesterol levels were not measured within 24 h after arriving at the emergency department; and (5) patients without CPC information upon discharge.
2.3. Data Collection
The core variables and supplement variables of the KoCARC registry extracted in this study were as follows: (1) patient characteristics: age, sex, hypertension, diabetes, and dyslipidemia; (2) cardiac arrest characteristics: arrest place, witnessed cardiac arrest, bystander CPR, initial rhythm; (3) hospital information: target temperature management (TTM), CPC upon discharge, and survival to discharge; and (4) blood test results: sodium, potassium, albumin, glucose, total cholesterol, lactic acid levels, and arterial blood gas analysis results.
2.4. Primary and Secondary Outcomes
In this study, the primary outcome was the neurologic outcome upon discharge of a patient hospitalized after OHCA. In addition, survival to discharge was investigated as a secondary outcome. We also investigated factors that affected neurologic outcomes and mortality.
A good neurologic outcome was defined as CPC 1 and 2, whereas poor neurologic outcomes were defined as CPC 3–5.
2.5. Statistics
The data of the KoCARC registry were compiled using a standard spreadsheet application (Excel 2016; Microsoft, Redmond, WA, USA) and were analyzed using R (version 3.6.1, www.R-project.org). Kolmogorov–Smirnov tests were performed for normal distribution in all datasets. Descriptive statistics were used to describe the baseline characteristics of the study. Categorical variables were presented as frequencies and percentages and continuous variables as medians (quartiles) or mean ± standard deviation (SD). An independent t-test or Mann-Whitney U-test was used to compare continuous variables, and the Chi-square or Fisher’s exact tests were used for categorical variables. Differences were considered statistically significant when the p-value was less than 0.05.
We analyzed the area under the receiver operating characteristics curve (AU-ROC) to examine the prognostic performance of total cholesterol level for predicting the neurologic outcome and the survival to discharge. Cut-off values were determined using the Youden’s index with high specificity for predicting poor neurologic outcomes in the ROC curve analysis.
Multivariable logistic regression analysis was performed to determine the association between serum total cholesterol levels and neurologic outcomes or survival to discharge. All variables with p values < 0.05 in univariate comparisons were included in the multivariable regression analysis. A variable with a variance inflation factor of >10 was considered multicollinear and was removed from the variable set. We used a backward elimination, sequentially eliminating variables with a threshold of p > 0.10, to assess a final adjusted variable set. We used categorical variables based on the cut-off value obtained from Youden’s index to elucidate the type of association between the blood test results and neurologic outcomes for multivariable logistic regression analysis. In addition, age was converted into a categorical variable based on the age of 65 years and the standard of the elderly for logistic regression analysis. Logistic regression analysis results were presented as odds ratios (ORs) and 95% confidence intervals (CIs).
3. Results
3.1. Baseline Characteristics of OHCA Patients
From 1 October 2015 to 30 June 2020, 12,321 patients were enrolled in the KoCARC registry of the 33 participating hospitals. Except for those who died or were transferred out, 3382 patients survived upon admission after OHCA. We excluded patients who had prehospital ROSC (n = 510), had missing data for serum total cholesterol level (n = 1596), CPC score (n = 229), and other missing data (n = 328). Thus, a total of 689 patients were eligible for this study (Figure 1).
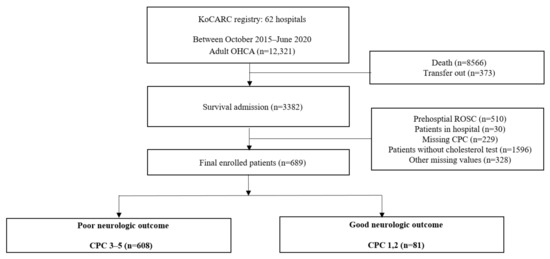
Figure 1.
Flow chart of the study (KoCARC, Korean Cardiac Arrest Resuscitation Consortium; OHCA, out-of-hospital cardiac arrest; ROSC, Return of spontaneous circulation; CPC, Cerebral Performance Category).
The clinical characteristics of the patients in the good neurologic outcome and poor neurologic outcome groups are summarized in Table 1. Of 689 patients who met the inclusion criteria, 81.

Table 1.
Baseline characteristics of out-of-hospital cardiac arrest patients with neurologic outcome.
Patients showed good neurologic outcomes. Patients with good neurologic outcomes were younger and had a low incidence of diabetes mellitus (DM). Incidences of witnessed cardiac arrest and initial shockable rhythm were significantly higher in the good neurologic outcome group than in the poor neurologic outcome group. Patients with lower potassium, higher albumin, higher pH, lower partial pressure of carbon dioxide (PaCO2), and lower lactate levels were associated with good neurologic outcomes compared to those in patients in the poor neurologic outcome group. In addition, patients with good neurologic outcomes had higher levels of total cholesterol than those with poor neurologic outcomes (127.5 ± 45.1 mg/dL vs. 155.1 ± 48.6 mg/dL, p <0.001).
The clinical characteristics stratified by survival to discharge are shown in Table 2. Patients who were alive at discharge had higher levels of total cholesterol than those who died in the hospital (124.0 ± 44.1 mg/dL vs 146.8 ± 47.7 mg/dL, p <0.001).
Table 2.
Baseline characteristics of out-of-hospital cardiac arrest patients with survival to discharge.
3.2. Prognostic Performance of Serum Total Cholesterol Levels for Neurologic Outcomes and Survival to Discharge
The prognostic performance of serum total cholesterol levels for predicting good neurologic outcomes at discharge for patients hospitalized after OHCA was analyzed using the ROC curve (Figure 2). The AUC of total cholesterol was 0.672 (95% CI: 0.613–0.701, p < 0.001). The optimal cut-off value of the total cholesterol level for predicting good neurologic outcomes using the Youden’s index was calculated as 119 mg/dL, and for predicting poor neurologic outcomes with high specificity was calculated as 58 mg/dL (Table 3).
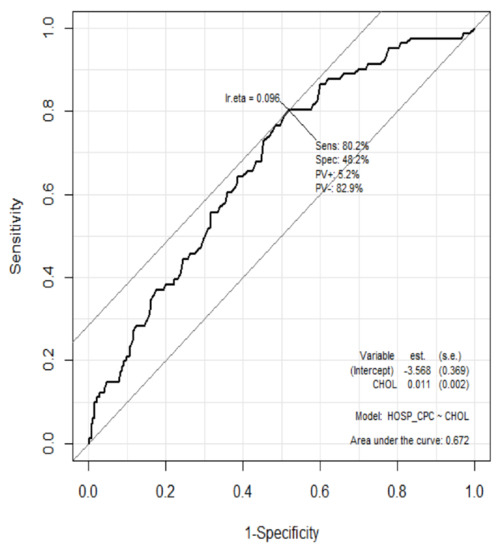
Figure 2.
Receiver operator characteristic curve for prediction of neurologic outcomes using total cholesterol levels.
Table 3.
Cut-off and diagnostic values of cholesterol for predicting neurologic outcome and survival.
In addition, the prognostic performance of serum total cholesterol levels for predicting good neurologic outcomes at discharge for patients hospitalized after OHCA was analyzed using the ROC curve (Figure 3). The AUC of total cholesterol was 0.646 (95% CI: 0.603–0.689, p <0.001).
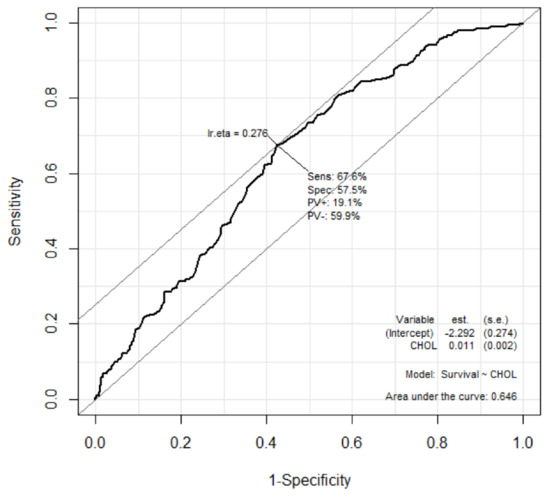
Figure 3.
Receiver operator characteristic curve for prediction of survival to discharge using total cholesterol levels. The optimal cut-off value of the total cholesterol level for predicting good neurologic outcomes using the Youden’s index was calculated as 126 mg/dL, and for predicting poor neurologic outcomes with high specificity was calculated as 58 mg/dL (Table 3).
3.3. Relationship between Serum Total Cholesterol Levels and Neurologic Outcomes or Survival to Discharge for Patients Hospitalized after OHCA
The following variables showed significant correlation with neurologic outcomes at hospital discharge for patients hospitalized after OHCA in the univariate analysis: age, DM, witnessed cardiac arrest, initial shockable rhythm, and potassium, albumin, total cholesterol, pH, PaCO2, and lactate levels. We performed a multivariate logistic regression analysis of the data of patients hospitalized after OHCA with good neurologic outcomes (Table 4). The factors that associated the neurologic outcomes at hospital discharge for patients hospitalized after OHCA were age, witnessed cardiac arrest, initial shockable rhythm, and albumin, total cholesterol, pH, and PaCO2 levels. The odds ratio for the neurological outcomes and total cholesterol level was 2.00 (95% CI: 1.01–3.96, p = 0.045).
Table 4.
Multivariate logistic regression of out-of-hospital cardiac arrest patients with neurologic outcome.
In addition, we analyzed the multivariate logistic regression analysis of the data of patients hospitalized after OHCA who survived to discharge (Table 5). The factors that associated the survival to discharge for patients hospitalized after OHCA were DM, initial shockable rhythm, TTM, albumin, total cholesterol, pH, and lactate. The odds ratio for the survival to discharge and total cholesterol level was 1.72 (95% CI 1.15–2.57, p = 0.009).
Table 5.
Multivariate logistic regression of out-of-hospital cardiac arrest patients with survival to discharge.
4. Discussion
In this study, we performed a multicenter retrospective observational study using the KoCARC registry. We assessed the association between serum cholesterol levels and outcomes of patients hospitalized after OHCA who had successful ROSC at the hospital. We performed a multivariate logistic regression of the data of patients hospitalized after OHCA with good neurologic outcomes, and the serum total cholesterol level was statistically significant as an independent factor (p = 0.045). A low initial serum total cholesterol level after ROSC was associated with poor neurological outcomes. In addition, a total cholesterol level higher than 119 mg/dL predicted a good neurologic outcome, and lower than 58 mg/dL predicted a poor neurologic outcome.
In previous studies, Chae et al. reported that a low total cholesterol level upon admission was associated with poor neurologic outcomes in patients with a post cardiac arrest syndrome (PCAS), and could be an easily obtained biomarker for neurologic outcome [17]. In addition, Lee et al. showed that the higher serum levels of total cholesterol and HDL within 1 h after ROSC were associated with good neurologic outcomes of patients with OHCA [18]. The results of this study are similar to those of previous studies. However, this study was meaningful in that it was a nationwide multicenter-based study and the number of samples was relatively large.
In the above studies, the median (interquartile range) of total cholesterol levels in the poor neurologic outcome group were 128 mg/dL (102–153) and 123.0 mg/dL (101.5–157.5), respectively. In this study, mean ± SD the total cholesterol level in the poor neurologic outcome group was 127.5 ± 45.1 mg/dL [17,18]. The definition of the level of hypocholesterolemia differs from each study [19,20]. Total cholesterol levels of patients in the poor outcome group in these studies are either lower or within the normal range according to interquartile range and standard deviation, but an absolute value of prediction for poor outcome cannot be established with these levels.
Most studies have focused on the risk of high cholesterol, such as a risk factor for coronary artery disease [8,21]. However, recent studies have presented roles for cholesterol in critically ill patients. There are several possible causes as to why low cholesterol levels may be associated with a poor neurological prognosis in systemic inflammatory critically ill patients, such as those with post-cardiac arrest syndrome.
First, systemic inflammation leads to an increase in proinflammatory cytokines and endotoxins. Lipoproteins can bind to and remove toxic endotoxins associated with the systemic inflammatory responses. In previous animal studies, transgenic mice with high HDL or LDL concentrations were resistant to the lipopolysaccharide (LPS) challenge [22], where lipoproteins reduced the cytokine response and led to reduced mortality [22,23]. Pajkrt et al. reported that injection of reconstituted HDL reduced tumor necrosis factor, interleukin 6 and 8 secreted by endotoxin in a human double-blind study [24].
In addition, cardiac arrest can lead to reduced total cholesterol levels due to decreased synthetic and secretory functions by liver damage [25]. Hosadurg et al. reported that the out-of-hospital sudden expected death group had lower total cholesterol than the control group [26]. In an animal study, total cholesterol levels before cardiac arrest were higher than those after ROSC [27].
It is important to predict the neurological prognosis of patients with ROSC after cardiac arrest. The 2020 American Heart Association (AHA) guidelines recommend using clinical findings, imaging modalities, and blood biomarkers to predict and evaluate the neurologic prognosis of patients who experience cardiac arrest [28]. Neuron-specific enolase and S-100B are the most commonly examined blood biomarkers for predicting neurologic outcomes. However, these markers are not routinely obtained and have low sensitivity and an inconsistent threshold for predicting neurologic outcomes after ROSC [28]. In this study and a previous study, total cholesterol levels showed potential as a predictor of neurologic outcomes in patients with ROSC after cardiac arrest [17]. Because testing for total cholesterol levels is performed routinely, medical costs can be lower than those of other biomarkers. In contrast, baseline total cholesterol levels prior to cardiac arrest in patients with ROSC vary. Patients may have normal cholesterol levels or have high total cholesterol levels due to hyperlipidemia, or, although the patients have hyperlipidemia, it may be the patients whose total cholesterol level was normal or lower than normal through treatment with statins. For these reasons, total cholesterol level might have little impact as a biomarker for predicting the neurological prognosis in patients who experience cardiac arrest.
However, although baseline total cholesterol levels vary among patients, low cholesterol levels might be a pre-existing risk factor for systemic inflammatory responses such as PCAS or sepsis. Lagrost et al. reported that a pre-existing low level of cholesterol before elective cardiac surgery with cardiopulmonary bypass may be a simple biomarker for the early identification of patients with a high risk of sepsis [29].
This finding showed the potential of low cholesterol itself as a risk factor for severe disease.
This study had several limitations. First, it is a retrospective observational study using a multicenter-based registry. Second, since this study was conducted in one country, it had to be limited by race and nationality. However, the KoCARC registry was used in order to represent South Korea better. Third, the outcome of this study was the evaluation of the neurological outcomes upon discharge and survival to discharge, and the mid- to long-term outcomes were not evaluated. Therefore, further studies are needed to investigate the association between total cholesterol levels and mid- to long-term neurologic and survival outcomes after OHCA. Fourth, of 12,321 OHCA patients, only 689 patients were included. More than 8500 people died, and missing values in blood tests such as total cholesterol were excluded among the surviving hospitalized patients. Because many patients were excluded, an opportunity for selection bias may arise. Fifth, because the cholesterol level is the result of a blood test within 24 h after ROSC, we did not investigate the association between serial changes in total cholesterol levels and outcomes of patients with ROSC. Sixth, because there was not enough information on HDL and LDL in the KoCARC registry, we could not investigate the relationship between detailed lipid profiles and the neurological outcomes and survival to discharge of patients who experience cardiac arrest. Finally, the KoCARC registry does not investigate information about the lipid lowering therapy of patients. So, we could not analyze the association between cholesterol level by lipid lowering therapy and the outcomes in this study.
5. Conclusions
Low total serum cholesterol levels within 24 h after arriving at the emergency department of patients after OHCA could be associated with poor neurologic outcomes upon discharge and in-hospital death. In addition, total serum cholesterol might be a biomarker for predicting neurologic outcomes or survival to discharge of hospitalized patients after OHCA.
Author Contributions
J.L.: Writing—Original draft, Data curation, Software, H.L.: Writing—Original draft, Methodology, J.O.: Supervision, Writing—Reviewing and Editing, T.H.L.: Conceptualization, H.K.: Validation, B.S.K.: Visualization, Y.C.: Data curation, Formal analysis. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Institutional Review Board (IRB) of Hanyang University Hospital (HYUH 2015-10-021-030).
Informed Consent Statement
Informed consent was waived by the IRB due to the retrospective study.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to acknowledge and thank to investigators from all participating hospitals of: KoCARC: Woon Yong Kwon (Seoul National University Hospital), Sang Kuk Han, Phil Cho Choi (Kangbuk Samsung Medical Center), Sang O Park, Jong Won Kim (Konkuk University Medical Center), Han Sung Choi, Jong Seok Lee (Kyung Hee University Hospital), Sung Hyuk Choi, Young Hoon Yoon (Korea University Guro Hospital), Su Jin Kim, Kap Su Han (Korea University Anam Hospital), Min Seob Sim, Gun Tak Lee (Samsung Medical Center), Shin Ahn (Asan Medical Center), Jong Whan Shin, Hui Jai Lee (SMG-SNU Boramae Medical Center), Keun Hong Park, Hahn Bom Kim (Seoul Medical Center), In Cheol Park, Yoo Seok Park (Yonsei University Severance Hospital), Tae Young Kong (Yonsei University Gangnam Severance Hospital), Chu Hyun Kim (Inje University Seoul Paik Hospital), Youngsuk Cho (Hallym University Kangdong Sacred Heart Hospital), Gu Hyun Kang, Yong Soo Jang (Hallym University Kangnam Sacred Heart Hospital), Seok Ran Yeom, Sung Wook Park (Pusan National University Hospital), Jae Hoon Lee (Dong-A University Hospital), Jae Yun Ahn (Kyungpook National University Hospital), Kyung Woo Lee, Tae Chang Jang (Daegu Catholic University Medical Center), Jae-hyug Woo (Gachon University Gil Medical Center), Woon Jeong Lee, Seon Hee Woo (The Catholic University of Korea Incheon St. Mary’s Hospital), Sung Hyun Yun, Jin Won Park (Catholic Kwandong University International St. Mary’s Hospital), Sun Pyo Kim, Yong Jin Park (Chosun University Hospital), Jin Woong Lee, Wonjoon Jeong (Chungnam National University Hospital), Sung Soo Park, Jae Kwang Lee (Konyang University Hospital), Ryeok Ahn, Wook Jin Choi (Ulsan University Hospital), Young Gi Min, Eun Jung Park (Ajou University Hospital), You Hwan Jo, Joong Hee Kim (Seoul National University Bundang Hospital), In Byung Kim, Ki Ok Ahn (Myongji Hospital), Han Jin Cho (Korea University Ansan Hospital), Seung Cheol Lee, Sang Hun Lee (Dongguk University Ilsan Hospital), Young Sik Kim (Bundang Jesaeng Hospital), Jin Sik Park (Sejong Hospital), Dai Han Wi (Wonkwang University Sanbon Hospital), Ok Jun Kim, Min Woo Kang (Cha University Bundang Medical Center), Sang Ook Ha, Won Seok Yang (Hallym University Pyeongchon Sacred Heart Hospital), Soon Joo Wang, Hang A Park (Hallym University Dongtan Sacred Heart Hospital), Jun Hwi Cho, Chan Woo Park (Kangwon National University Hospital), An Mu Eob, Tae Hun Lee (Hallym University Chuncheon Sacred Heart Hospital), Sang Chul Kim, Hoon Kim (Chungbuk National University Hospital), Han Joo Choi, Chan Young Koh (Dankook University Hospital), Hyung Jun Moon, Dong Kil Jeong (Soonchunhyang University Cheonan Hospital), Tae Oh Jung, Jae Chol Yoon (Chonbuk National University Hospital), Seung Yong Lee, Young Tae Park (Dongguk University Gyeongju Hospital), Jin Hee Jeong, Soo Hoon Lee (Gyeongsang National University Hospital), Ji Ho Ryu, Mun Ki Min (Pusan National University Yangsan Hospital), Won Kim, Yi Sang Moon (Cheju Halla General Hospital), Sung Wook Song, Woo Jung Kim (Jeju National University Hospital), Joon-myoung Kwon, Eui Hyuk Kang (Mediplex Sejong Hospital), Sang Chan Jin, Tae-kwon Kim (Keimyung University Dongsan Medical Center), Hyuk Joong Choi (Hanyang University Guri Hospital), Seong Chun Kim (Gyeongsang National University Changwon Hospital), In Soo Cho (Hanil General Hospital). To steering committee: comprised of following individuals: Sung Oh Hwang (Chair, Wonju Severance Christian Hospital), Sang Do Shin (Chair of Steering Committee, Seoul National University hospital), Hyuk Jun Yang (Advisory Committee, Gachon University Gil hospital), Sung Phil Chung (Data Safety and Management Board, Yonsei University Gangnam Severance Hospital), Sung Woo Lee (Security and Monitoring Board, Korea University Anam hospital), Kyung Jun Song (Secretariat, SMG-SNU Boramae Medical Center), Seung Sik Hwang (Epidemiology and Prevention Research Committee, Seoul National University), Gyu Chong Cho (Community Resuscitation Research Committee, Hallym University Kangdong Sacred Heart Hospital), Hyun Wook Ryoo (Emergency Medical Service Resuscitation Research Committee, Kyungpook National University Hospital), Kyoung Chul Cha (Hospital Resuscitation Research Committee, Wonju Severance Christian Hospital), Won Young Kim (Hypothermia and Post-Resuscitation Care Research Committee, Asan Medical Center), Sang Hoon Na (Cardiac Care Resuscitation Research Committee, Seoul National University Hospital), Young Ho Kwack (Pediatric Resuscitation Research Committee, Seoul National University hospital). To member of Secretariat: Jeong Ho Park (Seoul National University Hospital), Sun Young Lee (Seoul National University Hospital), and Sung Kyung Kim (Seoul National University Hospital). To National Fire Agency for providing prehospital EMS data. And to Korean Association of Cardiopulmonary Resuscitation (KACPR) for support.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Nolan, J.P.; Neumar, R.W.; Adrie, C.; Aibiki, M.; Berg, R.A.; Böttiger, B.W.; Callaway, C.; Clark, R.S.B.; Geocadin, R.G.; Jauch, E.C.; et al. Post-Cardiac Arrest Syndrome: Epidemiology, Pathophysiology, Treatment, and Prognostication: A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation 2008, 79, 350–379. [Google Scholar] [CrossRef]
- Uchino, H.; Ogihara, Y.; Fukui, H.; Chijiiwa, M.; Sekine, S.; Hara, N.; Elmér, E. Brain Injury Following Cardiac Arrest: Pathophysiology for Neurocritical Care. J. Intensive Care 2016, 4, 31. [Google Scholar] [CrossRef] [PubMed]
- Grace, P.A. Ischaemia-Reperfusion Injury. Br. J. Surg. 1994, 81, 637–647. [Google Scholar] [CrossRef]
- Gando, S.; Nanzaki, S.; Morimoto, Y.; Kobayashi, S.; Kemmotsu, O. Out-of-Hospital Cardiac Arrest Increases Soluble Vascular Endothelial Adhesion Molecules and Neutrophil Elastase Associated with Endothelial Injury. Intensive Care Med. 2000, 26, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Huet, O.; Dupic, L.; Batteux, F.; Matar, C.; Conti, M.; Chereau, C.; Lemiale, V.; Harrois, A.; Mira, J.-P.; Vicaut, E.; et al. Postresuscitation Syndrome: Potential Role of Hydroxyl Radical-Induced Endothelial Cell Damage. Crit. Care Med. 2011, 39, 1712–1720. [Google Scholar] [CrossRef]
- Adrie, C.; Adib-Conquy, M.; Laurent, I.; Monchi, M.; Vinsonneau, C.; Fitting, C.; Fraisse, F.; Dinh-Xuan, A.T.; Carli, P.; Spaulding, C.; et al. Successful Cardiopulmonary Resuscitation after Cardiac Arrest as a “Sepsis-like” Syndrome. Circulation 2002, 106, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, J. Pathophysiology of Sepsis. Am. J. Health-Syst. Pharm. 2002, 59 (Suppl. 1), S3–S8. [Google Scholar] [CrossRef]
- Montalescot, G.; Dallongeville, J.; Van Belle, E.; Rouanet, S.; Baulac, C.; Degrandsart, A.; Vicaut, E.; OPERA Investigators. STEMI and NSTEMI: Are They so Different? 1 Year Outcomes in Acute Myocardial Infarction as Defined by the ESC/ACC Definition (the OPERA Registry). Eur. Heart J. 2007, 28, 1409–1417. [Google Scholar] [CrossRef]
- Kitahara, C.M.; Berrington de González, A.; Freedman, N.D.; Huxley, R.; Mok, Y.; Jee, S.H.; Samet, J.M. Total Cholesterol and Cancer Risk in a Large Prospective Study in Korea. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 1592–1598. [Google Scholar] [CrossRef]
- Yamano, S.; Shimizu, K.; Ogura, H.; Hirose, T.; Hamasaki, T.; Shimazu, T.; Tasaki, O. Low Total Cholesterol and High Total Bilirubin Are Associated with Prognosis in Patients with Prolonged Sepsis. J. Crit. Care 2016, 31, 36–40. [Google Scholar] [CrossRef]
- Zhao, W.; An, Z.; Hong, Y.; Zhou, G.; Guo, J.; Zhang, Y.; Yang, Y.; Ning, X.; Wang, J. Low Total Cholesterol Level Is the Independent Predictor of Poor Outcomes in Patients with Acute Ischemic Stroke: A Hospital-Based Prospective Study. BMC Neurol. 2016, 16, 36. [Google Scholar] [CrossRef]
- McClave, S.A.; Martindale, R.G.; Vanek, V.W.; McCarthy, M.; Roberts, P.; Taylor, B.; Ochoa, J.B.; Napolitano, L.; Cresci, G.; A.S.P.E.N. Board of Directors; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). J. Parenter. Enteral Nutr. 2009, 33, 277–316. [Google Scholar] [CrossRef] [PubMed]
- Cirstea, M.; Walley, K.R.; Russell, J.A.; Brunham, L.R.; Genga, K.R.; Boyd, J.H. Decreased High-Density Lipoprotein Cholesterol Level Is an Early Prognostic Marker for Organ Dysfunction and Death in Patients with Suspected Sepsis. J. Crit. Care 2017, 38, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Lekkou, A.; Mouzaki, A.; Siagris, D.; Ravani, I.; Gogos, C.A. Serum Lipid Profile, Cytokine Production, and Clinical Outcome in Patients with Severe Sepsis. J. Crit. Care 2014, 29, 723–727. [Google Scholar] [CrossRef] [PubMed]
- Nagase, M.; Sakurai, A.; Sugita, A.; Matsumoto, N.; Kubo, A.; Miyazaki, Y.; Kinoshita, K.; Yamamoto, Y. Oxidative Stress and Abnormal Cholesterol Metabolism in Patients with Post-Cardiac Arrest Syndrome. J. Clin. Biochem. Nutr. 2017, 61, 108–117. [Google Scholar] [CrossRef]
- Kim, J.Y.; Hwang, S.O.; Shin, S.D.; Yang, H.J.; Chung, S.P.; Lee, S.W.; Song, K.J.; Hwang, S.S.; Cho, G.C.; Moon, S.W.; et al. Korean Cardiac Arrest Research Consortium (KoCARC): Rationale, Development, and Implementation. Clin. Exp. Emerg. Med. 2018, 5, 165–176. [Google Scholar] [CrossRef]
- Chae, M.K.; Lee, S.E.; Min, Y.G.; Park, E.J. Initial Serum Cholesterol Level as a Potential Marker for Post Cardiac Arrest Patient Outcomes. Resuscitation 2020, 146, 50–55. [Google Scholar] [CrossRef]
- Lee, H.Y.; Lee, D.H.; Lee, B.K.; Jeung, K.W.; Jung, Y.H.; Park, J.S.; Min, J.H.; Min, Y.I. The Association between Lipid Profiles and the Neurologic Outcome in Patients with Out-of-Hospital Cardiac Arrest. Resuscitation 2019, 145, 26–31. [Google Scholar] [CrossRef]
- Criqui, M.H. Very Low Cholesterol and Cholesterol Lowering. A Statement for Healthcare Professionals from the American Heart Association Task Force on Cholesterol Issues. Circulation 1994, 90, 2591. [Google Scholar] [CrossRef][Green Version]
- Hypolipidemia—Endocrine and Metabolic Disorders. Available online: https://www.merckmanuals.com/professional/endocrine-and-metabolic-disorders/lipid-disorders/hypolipidemia (accessed on 21 December 2021).
- Sever, P.S.; Dahlöf, B.; Poulter, N.R.; Wedel, H.; Beevers, G.; Caulfield, M.; Collins, R.; Kjeldsen, S.E.; Kristinsson, A.; McInnes, G.T.; et al. Prevention of Coronary and Stroke Events with Atorvastatin in Hypertensive Patients Who Have Average or Lower-than-Average Cholesterol Concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial--Lipid Lowering Arm (ASCOT-LLA): A Multicentre Randomised Controlled Trial. Lancet Lond. Engl. 2003, 361, 1149–1158. [Google Scholar] [CrossRef]
- Netea, M.G.; Demacker, P.N.; Kullberg, B.J.; Boerman, O.C.; Verschueren, I.; Stalenhoef, A.F.; van der Meer, J.W. Low-Density Lipoprotein Receptor-Deficient Mice Are Protected against Lethal Endotoxemia and Severe Gram-Negative Infections. J. Clin. Investig. 1996, 97, 1366–1372. [Google Scholar] [CrossRef] [PubMed]
- Levine, D.M.; Parker, T.S.; Donnelly, T.M.; Walsh, A.; Rubin, A.L. In Vivo Protection against Endotoxin by Plasma High Density Lipoprotein. Proc. Natl. Acad. Sci. USA 1993, 90, 12040–12044. [Google Scholar] [CrossRef] [PubMed]
- Pajkrt, D.; Doran, J.E.; Koster, F.; Lerch, P.G.; Arnet, B.; Van Der Poll, T.; Ten Cate, J.W.; Van Deventer, S.J.H. Antiinflammatory Effects of Reconstituted High-Density Lipoprotein during Human Endotoxemia. J. Exp. Med. 1996, 184, 1601–1608. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E. Critical Illness-Related Corticosteroid Insufficiency. Chest 2009, 135, 181–193. [Google Scholar] [CrossRef]
- Hosadurg, N.; Bogle, B.M.; Joodi, G.; Sadaf, M.I.; Pursell, I.; Mendys, P.M.; Mounsey, J.P.; Simpson, R.J. Lipid Profiles in Out-of-Hospital Sudden Unexpected Death. Mayo Clin. Proc. Innov. Qual. Outcomes 2018, 2, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Bleske, B.E.; Song, J.; Chow, M.S.S.; Kluger, J.; White, C.M. Hematologic and Chemical Changes Observed during and after Cardiac Arrest in a Canine Model—A Pilot Study. Pharmacotherapy 2001, 21, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Callaway, C.W.; Donnino, M.W.; Fink, E.L.; Geocadin, R.G.; Golan, E.; Kern, K.B.; Leary, M.; Meurer, W.J.; Peberdy, M.A.; Thompson, T.M.; et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S465–S482. [Google Scholar] [CrossRef]
- Lagrost, L.; Girard, C.; Grosjean, S.; Masson, D.; Deckert, V.; Gautier, T.; Debomy, F.; Vinault, S.; Jeannin, A.; Labbé, J.; et al. Low Preoperative Cholesterol Level Is a Risk Factor of Sepsis and Poor Clinical Outcome in Patients Undergoing Cardiac Surgery with Cardiopulmonary Bypass. Crit. Care Med. 2014, 42, 1065–1073. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).