Abstract
In this study, we aimed to determine the frequency and clinical impact of new ischemic lesions detected with diffusion-weighted-imaging-MRI (DWI-MRI) as well as the clinical outcomes after carotid artery stenting (CAS) using the simple flow blockage technique (SFB). This is a retrospective study with data extraction from a monocentric prospective clinical registry (from 2017 to 2019) of consecutive patients admitted for symptomatic cervical ICA stenosis or web. Herein, patients benefited from DWI-MRI before and within 48 h of CAS for symptomatic ICA stenosis or web. The primary endpoint was the frequency of new DWI-MRI ischemic lesions and the secondary (composite) endpoint was the rate of mortality, symptomatic stroke or acute coronary syndrome within 30 days of the procedure. All of the 82 CAS procedures were successfully performed. Among the 33 patients (40.2%) with new DWI-MRI ischemic lesions, 30 patients were asymptomatic (90.9%). Irregular carotid plaque surface with (n = 13, 44.8%) or without ulceration (n = 12, 60.0%) was associated with higher rates of new DWI-MRI lesions by comparison to patients with a regular plaque (n = 7, 25%) (p = 0.048) using the univariate analysis. Less than half of this CAS cohort using the SFB technique had new ischemic lesions detected with DWI-MRI. Among these patients, more than 90% were asymptomatic. Irregularity of the plaque seems to increase the risk of peri-procedural DWI-MRI lesions.
1. Introduction
Symptomatic carotid stenosis, defined as stenosis of the internal carotid artery (ICA) leading to recent symptoms of amaurosis fugax, transient ischemic attacks or acute ischemic stroke (AIS) ipsilateral to the lesion [1], carries a high risk of early recurrence and stroke and carotid revascularization is recommended [2]. Randomized controlled trials (EVA-3S, SPACE, and ICSS) comparing carotid endarterectomy (CEA) and carotid artery stenting (CAS) have shown a higher periprocedural risk of stroke with CAS than with CEA [3,4,5]. However, risks of stroke or death in patients younger than 70 years were similar in both treatment groups [6]. Therefore, CAS has been developed during the past two decades to treat symptomatic carotid and is often chosen for anatomic reasons (contralateral occlusion), for patients with high surgical risk (radiation injury, history of prior neck dissection, presence of tracheostomy) or with severe medical comorbidities (high risk for open surgery).
Carotid web (CW) leads to ischemic stroke secondary to blood flow stasis and subsequent embolization. In addition, optimal management strategies for secondary stroke prevention remain unclear. Due to the high stroke recurrence rate in medically managed symptomatic CW patients, carotid revascularization is currently performed, with no periprocedural complications or recurrent strokes in carotid revascularization management with CAS or CEA [7].
Moreover, the recent numerous randomized controlled trials (RCT) established mechanical thrombectomy as the gold standard for the treatment of AIS with large vessel occlusion, with the possibility of emergency carotid stenting in tandem occlusion [8]. This post-thrombectomy era led to an increased number of endovascular treatments of AIS during the past few years. Nevertheless, the current key point is the safety of CAS. During these last years, the technical and medical experience of the operators, as well as new innovative endovascular techniques, devices, and a better management of the antiplatelet therapies could reduce this procedural risk.
Indeed, the embolic protection technique during CAS as proximal balloon occlusion (PBA), and distal filter protection (DFP) can provide similar levels of protection from periprocedural stroke and 30-day mortality [9]. In the dynamic of developing the safest CAS procedure, an innovative approach (simple flow blockage technique [SFB]) was reported as a combination of proximal balloon occlusion and flow blockage, which is inspired from a mechanical thrombectomy technique [10].
Diffusion-weighted-imaging-MRI (DWI-MRI) remains the gold standard to evaluate acute stroke lesions even without any clinical significance. The objective of this study is to report the frequency of new ischemic lesions using DWI-MRI as well as their impact on clinical outcomes after consecutive carotid artery stenting (CAS) is performed with SFB in consecutive patients with AIS (without large vessel occlusion) and symptomatic carotid artery stenosis or carotid web.
2. Materials and Methods
2.1. Study Design
We carried out a retrospective study with data extraction from our prospective clinical registry of consecutive patients admitted for symptomatic ICA atherosclerotic stenosis or carotid web to our Comprehensive Stroke Center (CSC) from January 2017 to September 2019.
This study (reference study RECHMPL 18 0236, No. ID-RCB: 2018-A02651-54) was approved by a local ethics committee (Comité de Protection des Personnes (CPP) SUD-MEDITERRANEE III, UFR MEDECINE 186, chemin du Carreau de Lanes CS 83021 30908 NIMES Cedex 2), and registered on clinicaltrials.gov (NCT04421326).
In the context of carotid stenting using the simple flow blockage technique, we previously reported data from January 2015 to 2018 in 75 patients, focusing on the angiographic pattern [10]. In this previous study, only 40 patients (53.3% of the cohort) benefited from a MRI follow-up [10].
For this current study, focusing on a routine MRI protocol follow-up implemented in our center since January 2017 for CAS, we included 15 patients who were already analyzed in the previous study (from year 2017).
2.2. Inclusion Criteria
Consecutive patients were included if they fulfilled the following criteria: (I) AIS (hemispheric or retinal TIA), cerebral infarct in the anterior circulation without large vessel intracranial occlusion <3 months before admission; (II) pre-procedural (<1 month) brain DWI-MRI (diffusion-weighted-imaging-MRI) showing cytotoxic lesions of AIS and/or perfusion-MRI showing brain hypoperfusion; (III) ipsilateral atheromatous internal carotid artery stenosis >50% or carotid web. The diagnosis of carotid stenosis or web was performed on noninvasive imaging (CT and/or MRI); (IV) CAS for ICA atheromatous stenosis ≤50% was retained in the case of plaque instability as demonstrated by an intraplaque hemorrhage on dedicated black-blood MRI; (V) post-procedural (<48 h) brain DWI-MRI. The decision of endovascular treatment was retained after a multidisciplinary team meeting.
The exclusion criteria were: (1) Patients with intracranial large vessel occlusion; (2) patients with pre-stroke dependency defined as a modified Rankin score > 2; (3) patients with severe or fatal co-morbidities or life expectancy under 6 months; (4) patients treated endovascularly using a DFP device; and (5) patients with carotid artery stenosis at the acute phase of ischemic stroke caused by tandem occlusion.
2.3. Patient Management
2.3.1. Medical Management
All patients were hospitalized in the CSC for maintenance of hemodynamic function (objective of systolic blood pressure > 120 mmHg), and close monitoring of any neurological worsening. Anticoagulants and/or aspirin was left to the discretion of the stroke neurologist.
Clopidogrel (75 mg daily) was given within the days before CAS, with an assessment of platelet inhibition (PRU, Platelet Reactive Units) (VerifyNow, Instrumentation Laboratory, San Diego, CA, USA) before the procedure.
In cases of clopidogrel resistance (230–240 P2Y12 reaction units PRU by the VerifyNow P2Y12 assay or platelet inhibition rate < 20%) [10], prasugrel (20 mg) was given the day before the intervention and platelet inhibition was tested again before the procedure.
All patients had subsequently 3 months of dual antiplatelet medication (aspiring 75 mg), then lifelong aspirin.
In cases of emergency stenting for hemodynamic symptoms or early recurrence, a loading dose of platelet inhibitor (300 mg of clopidogrel or 20 mg of prasugrel) was administered and platelet inhibition was then assessed.
All procedures were performed via a femoral artery approach, and 150 IU/kg heparin was administered intravenously after the placement of the 9-French balloon guiding catheter (Concentric medical, Mountain View, CA, USA) into the targeted common carotid artery. The balloon guiding catheter was prepared according to the instructions provided by the manufacturer, using a combination of contrast agent with saline (50% by volume) to prepare balloon inflation media.
Atropine (0.01–0.02 mg/kg) was administered intravenously at the time of angioplasty, which was performed using a 4.0–7.0 mm balloon (Ultra-soft SV monorail balloon, Boston Scientific, Marlborough, MA, USA).
2.3.2. Simple Flow Blockage (SFB) Technique
All procedures were performed under conscious sedation by experienced interventional neuroradiologists. A baseline angiographic run was performed after the inflation of the balloon guiding catheter in the common carotid artery, and was allowed to determine the different angiographic patterns [10].
In all cases, flushing of the guiding catheter was temporarily interrupted during the critical steps (crossing of culprit lesions, stent deployment, angioplasty) to avoid antegrade embolization.
After a dangerous maneuver (crossing of culprit lesions, stent deployment, angioplasty), two steps were respected: (1) Pump aspiration (Penumbra, Alameda, CA, USA) set on the recommended vacuum pressure of −25.5 inches Hg (−86.4 kPa) via a rotating hemostatic valve (RHV) for approximately 10 s before balloon deflation, to avoid potential embolization from the stagnating column of blood distal to the balloon or from the guiding catheter itself; and (2) after balloon deflation, the RHV is opened for a few seconds and closed progressively during activation of the flushing line, to assure that the RHV is clean (aspiration is performed through it in prevention of the accumulated debris inside the RHV).
A DFP device was not used during any procedures in this study. The type of stent and the use of pre-dilation and post-dilation by balloon angioplasty were performed according to neurointerventionalists’ discretion.
Balloon angioplasty was not performed for web cases.
2.3.3. Follow-Up and Outcome
All patients were hospitalized in the CSC for at least 24 h following the intervention, with strict blood pressure monitoring and management (target level of <140/90 mmHg) and close monitoring of any neurological worsening.
Patients with preprocedural severe stenosis (>90%), severe contralateral stenosis or occlusion, or with periprocedural arterial hypertension were considered at high risk of reperfusion syndrome, leading to a stricter blood pressure monitoring and management with a target level of <120/80 mmHg. Patients were treated after the procedure with clopidogrel (75 mg daily) or with prasugrel (10 mg daily) in the case of clopidogrel resistance (in the absence of contraindication). This treatment was delayed by 6 to 24 h for patients treated with intravenous thrombolysis.
A post-procedural (<48 h) follow-up cerebral MRI was systematically performed after stenting.
Patients were discharged 48–72 h post-treatment, after a comprehensive neurological evaluation.
The primary endpoint was the retrospective assessment of new ischemic lesions detected by DWI-MRI by two neurointerventionalists (JFH and CD) blinded to the clinical outcomes and the procedure success (defined as the ability to successfully implant a carotid stent with <30% residual stenosis). The secondary (composite) endpoint was the rate of mortality, symptomatic stroke or acute coronary syndrome within 30 days of the procedure.
The new symptomatic stroke was defined as a neurological deficit, as explained by a new ischemic lesion on DWI.
2.4. MRI Evaluation
MRI scans were performed using a Siemens Avanto 1.5 T.
On the 1.5 T scanner, the sequence parameters were: TR = 24 ms, TE = 6.00 ms, flip angle = 90.3 directions of measurement, 16 cm FOV, 131 × 131 matrix, and 5 mm section thickness. Twelve-channel head coils were used. Foci of diffusion were measured in the longest axial axis. DWI b-value was b = 1000 for all studies. All patients were scanned with the same protocol before CAS and within the 48-h following the CAS procedure.
2.5. Data Collection
Patient’s characteristics, imaging data, treatment, and follow-up were prospectively collected at the CSC: (a) Clinical data: Age, gender, medication, and vascular risk factors (hypertension, hypercholesterolemia, diabetes, current smoking); (b) imaging data: Type of initial arterial imaging (MRA, CTA; type of carotid stenosis: Degree of stenosis, web, plaque surface characteristics (ulcerated, irregular)).
Pre- and post-procedural (<48 h) DWI-MRI (diffusion-weighted-MRI) were performed for all patients.
Data supplemental to the main text regarding data collection, patients’ management (medical management and SFB technique, follow-up, and outcome) can be found in Appendix A.
2.6. Statistical Analysis
Categorical variables were expressed as frequencies and percentages and continuous as mean (standard deviation) or median (interquartile range, IQR) in the case of non-normal distribution. Normality of distribution was assessed graphically and using the Shapiro-Wilk test. Rates of outcomes were estimated by calculating exact binomial 95% confidence intervals (CIs). Bivariate comparisons in main ICA lesions and treatment characteristics between patients with and without new cerebral lesions at DWI-MRI were conducted using the Chi-Square test (or Fisher’s exact test when the expected cell frequency was <5) for categorical variables, and Mann-Whitney U test for continuous variables as appropriate. Statistical testing was conducted at the two-tailed α-level of 0.05. Data were analyzed using the SAS software package, release 9.4 (SAS Institute, Cary, NC, USA).
3. Results
3.1. Patient Characteristics and Angiographic Patterns
From January 2017 to September 2019, 82 patients with symptomatic carotid artery atherosclerotic stenosis (n = 78) or symptomatic web (n = 4) were treated by CAS using the SFB technique in our CSC and benefited from a DWI-MRI before and within 48 h of the stenting procedure (see flowchart; Figure 1). Patient and treatment characteristics are reported in Table 1. Overall, the median age was 68 years (IQR, 59 to 75), 37 patients (45.1%) were men. Baseline median NIHSS was 5.6 (IQR, 1 to 18). CAS was performed after a median time from symptom of 7 days (IQR, 3 to 30 days). Among the 78 patients with atherosclerotic stenosis (95.1%), the median degree of carotid stenosis was 75% (IQR, 70 to 90), ulcerations were present in 63.7% of cases.
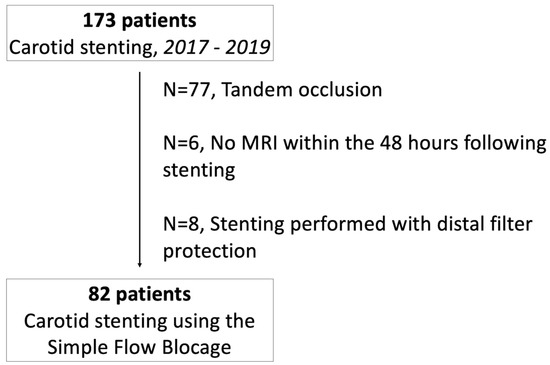
Figure 1.
Flow-Chart.

Table 1.
Patient and treatment characteristics of the 82 included patients with symptomatic carotid stenosis >50% or symptomatic web treated by CAS using SFB.
No resistance to clopidogrel was observed in this cohort.
Complete stagnation of the contrast column in the ICA (angiographic pattern 1) was observed in 28 patients (34.1%), retrograde wash-out of the internal carotid artery from the intracranial circulation toward the external carotid artery (pattern 2) in 27 patients (32.9%), and antegrade wash-out of contrast toward the intracranial circulation, via the external carotid artery or from the common carotid artery (pattern 3) was observed in the remaining 27 cases (32.9%). CAS was performed using Casper (Carotid Artery Stent designed to Prevent Embolic Release, MicroVention Inc., Tustin, CA, USA) (n = 18), Xact (Abbott Vascular, Abbott Park, IL, USA) (n = 53) or Precise (Cordis, Warren, NJ, USA) (n = 17) stents with a median procedure time of 35 min (IQR, 24 to 45 min). For 11 patients, two or three stents were used (see footnote of Table 1). All the CAS procedures were successfully achieved.
3.2. Clinical and DWI Outcomes
Within the 48 h after CAS, a total of 177 new cerebral lesions (134 punctiform lesions, 32 lesions ≤ 10 mm and 11 lesions > 10 mm) were detected by DWI-MRI in 33 patients (40.2%, 95%CI: 29.5 to 51.7%, Table 2). Thirty-one patients (37.8%) had at least one punctiform lesion, thirty-one (37.8%) had at least one ipsilateral lesion, and seven (8.5%) had at least one lesion > 10 mm.
Table 2.
DWI-MRI new lesions and clinical outcomes in 82 patients with symptomatic carotid stenosis >50% or symptomatic web treated by CAS using SFB.
Eight patients (9.8%) had contralateral lesions. Among these 33 patients, the baseline median NIHSS was 7.2 (IQR, 1 to 18). Thirty patients (36.6%) had new ischemic DWI-MRI lesions without new neurological symptoms or modification of the NIHSS during periprocedural follow-up. An example of the new punctiform ischemic DWI-MRI lesions is provided in Appendix B Figure A1.
Three patients had symptomatic ischemic strokes with NIHSS degradation in two patients (respectively from NIHSS 6 and 7 to NIHSS 10 to 9) and death from the reperfusion syndrome in one patient. The latter was known with history of hypertension and hypercholesterolemia, and presented with a symptomatic 75% left ICA stenosis. Baseline NIHSS was 18 and DWI-MRI showed no initial ischemic lesions and no intracranial large vessel occlusion. The CAS procedure was successfully performed 1 day from symptoms onset, but the patient presented pre-procedural hypertension leading to strict blood pressure monitoring after the CAS with a target level of <120/80 mmHg. The DWI-MRI performed 25 h from the CAS revealed symptomatic new cerebral lesions (punctiform and >10 mm) both in the ipsilateral and contralateral side without large intracranial vessel occlusion. Dual antiplatelet medication was continued. A neurologic deterioration occurred, and the 30-h CT revealed an intraparenchymal hemorrhage corresponding to a reperfusion syndrome. The patient died 34 h after the CAS (see Appendix B Figure A2).
No acute coronary syndrome was observed. Overall, the 30-day composite endpoint occurred in three patients (3.7%).
Association of ICA lesion and treatment characteristics with the presence of ≥1 new DWI-MRI lesions are reported in Table 3. Only carotid plaque surface characteristics were significantly associated with the presence of ≥1 new cerebral lesions; patients with irregular plaque with (n = 13, 44.8%) or without ulceration (n = 12, 60.0%) had a higher rate of new cerebral lesions by comparison to patients with regular plaque (n = 7, 25%) (p = 0.048).
Table 3.
Comparisons of ICA lesion and treatment characteristics between patients with and without new cerebral lesions detected by DWI-MRI.
4. Discussion
In this large cohort of 82 consecutive patients with symptomatic severe carotid stenosis or carotid web treated with a standardized procedure of stenting using the SFB technique, less than half of this CAS cohort had new ischemic lesions detected with DWI-MRI (n = 33; 40.2%), asymptomatic in 30 patients (90.9%). Three (3.7%) patients had a newly onset symptomatic ischemic stroke and one (1.2%) had a transient focal neurological deficit. Among the patients with newly onset symptomatic ischemic stroke, one patient (1.2%) experienced reperfusion syndrome.
Both CEA and CAS are known to have increased periprocedural complications in symptomatic patients. However, the risk-benefit balance tilts in favor of treatment, both with CAE [1] and CAS [11].
In a meta-analysis of three RCT (EVA-3S, SPACE, and ICSS), any stroke or death occurred significantly more often in the CAS group compared to the CEA group. Nevertheless, an analysis of individual patient data showed that risk with CAS was twice the risk of CEA in patients greater than age 70 but was the same under 70 [6]. In the same line, the risk for stroke, acute coronary syndrome or death with CAS significantly increased with age according to the CREST investigators [12].
The CREST [13,14] demonstrated equivalent composite outcomes (stroke, myocardial infarction, death) between CEA and CAS. However, the subgroup analysis suggested an increased risk of stroke with CAS. Similarly, a recent meta-analysis (Carotid Artery Stenting Versus Endarterectomy for Stroke Prevention: A Meta-Analysis of Clinical Trials) confirmed these findings [15].
However, over the past two decades, embolic protection devices emerged for CAS and allowed progressive improvements in terms of stroke and mortality rates [16].
More recently, and in contrast to the findings of CREST, Cole et al. suggested that 378,354 patients undergoing CEA had a higher rate of perioperative stroke than 57,273 patients undergoing CAS, primarily among symptomatic patients (8.1% versus 5.6%; odds ratio, 1.47 [CI: 1.29–1.68]; p < 0.001) [17].
Current guidelines advise proceeding with CEA for symptomatic carotid only if the surgeon’s rate for perioperative stroke or death is <6% [2,18]. In our cohort, perioperative stroke or death occurred for 3.7%, suggesting that progress of CAS, especially using the SFB technique, led to a very attractive approach for symptomatic carotid stenosis.
4.1. DWI Lesions
Clinical series [19] and systematic review [20] showed that patients treated by CAS have about three times more new ischemic lesions on DWI-MRI compared to the CAE group, respectively 37% and 50% in the CAS group, and 10% and 17% in the CAE group (p < 0.01).
However, the main weakness of these results is the heterogeneity in the use of the protective device, as well as differences in the used material (balloon, DFP).
Interestingly, in the ICSS-MRI sub-study, Gensicke et al. found that there was no significant difference in total lesion volume per patient between the CAS and CEA groups in the entire study population (p = 0.18). Among these patients with silent ischemic DWI-MRI lesions after treatment (CAS, n = 62 patients; CEA, n = 18), volumes of separate lesions were significantly smaller in the CAS group (median volume, 0.02 mL) than the CEA group (0.08 mL; p < 0.0001) [21].
In addition, it is known that a routine diagnostic angiography induces silent ischemic lesions. Bendszus et al. showed that 44% of patients with vasculopathy who benefited from a routine diagnostic angiography had silent embolisms compared to a group without vascular risk factors (13%) [22]. Accordingly, the 40% rate of patients experiencing DWI-MRI lesions after CAS in our cohort is comparable to what was reported in the literature.
4.2. Irregular/Ulcerated Stenosis and Degree of Stenosis
Our study suggests that plaque surface characteristics were significantly associated with the presence of ≥1 new DWI cerebral lesions. Indeed, patients with irregular plaque with (n = 13, 44.8%) or without ulceration (n = 12, 60.0%) had a higher rate of new cerebral lesions in comparison to patients with regular plaque (n = 7, 25%) (Table 3).
This is in accordance with other studies suggesting that the irregular plaque surface was associated with increased incidence of carotid stenting-associated ischemic lesions [23,24].
Exploratory analyses from EVA-3S [3,25], SPACE [26], and ICSS [27] cohorts did not show any significant association between the degree of stenosis and stroke after CAS or CAE with a 70% stenosis [26,27] or a 90% stenosis cut-off [3,25]. Interestingly, the ICSS cohort [27] evaluated fatal or disabling strokes of 3.9% and 6.7% after CAS and 9.6% and 6.2% after CAE, respectively, for an ipsilateral stenosis of 50–69% and 70–99% (p = 0.155).
According to our results using SFB and to the literature, the most important point associated with peri-procedural stroke in patients with stenosis > 50% may be the irregularity and not the severity of the stenosis after CAS.
4.3. Timing of Angioplasty
It is interesting to note that the delay from AIS onset and treatment with CAS was not associated with an increased risk of peri-procedural DWI-MRI lesions. Current guidelines are to pursue early revascularization within 14 days of AIS [2]. Due to the increasing risk of recurrence within the first 2 weeks after the first ischemic event of a symptomatic carotid stenosis, Liu et al. showed improved functional outcomes without increasing the rate of new AIS, myocardial infarction or death in the early CAS group (<1 week) compared to the delayed CAS at 1 month [28]. On the contrary, Song et al. evaluated CAS for 206 patients with moderate-to-severe stenosis and found a significantly higher rate of ipsilateral stroke or death (at 30 days) of 12.8% in the early CAS group (within 14 days) compared to only 0.8% in the delayed CAS group (mean timing of CAS was 52.6 ± 36.94 days) [29]. However, this finding did not extend beyond the 30-day follow-up period (31 days to 1 year), wherein there was no significant difference between groups. A post-hoc analysis with the CREST population did not find any relationship between timing and significant adverse events in the 583 patients in the CAS group [30], and this was in agreement to what we found in our study (Table 3).
Transcarotid artery revascularization (TCAR) with flow reversal was developed to mitigate the maneuvers at highest risk for causing stroke during transfemoral CAS.
Comparing TCAR to CEA across different age groups showed no significant differences in outcomes [31,32].
In comparison to transfemoral CAS for patients ≥ 80 years, TCAR was associated with a reduction in stroke risk, reduction in risk of stroke/death, and reduction in the risk of stroke/death/myocardial infarction of respectively 72%, 65%, and 76% [31,32]. However, these results must be set against the advances in the experience of interventional practitioners and their equipment, in particular the famous balloon-guiding-catheters. In addition, aspiration is now possible with mechanical thrombectomy devices and confirms the need to repeat randomized studies.
4.4. Study Limitations
There are several limitations in the current study. The number of patients in our analysis was relatively small and there was no CAE group for comparison.
Moreover, this study only focused on patients who benefited from a DWI-MRI before and within the 48-h following a CAS procedure.
However, this current CAS cohort only included symptomatic patients with symptomatic carotid stenosis or web which carries higher risk than asymptomatic carotid, with a known tendency for more silent ischemic lesions after CAS, suggesting that patients with symptomatic carotid had an increased micro-embolic risk during the CAS procedure [24].
5. Conclusions
In this study, less than half of the CAS cohort using the SFB technique had new ischemic lesions detected with DWI-MRI. Among these patients, more than 90% were asymptomatic. As a result, irregularity of the plaque seems to increase the risk of peri-procedural DWI-MRI lesions.
Author Contributions
Conceptualization, J.-F.H., C.A., F.C. and C.D.; methodology, J.-F.H., V.C. and C.D.; software, J.-F.H. and C.D.; validation, J.-F.H., C.A., V.C. and C.D.; formal analysis, J.-F.H. and C.D.; investigation, J.-F.H., M.M., F.-L.C. and C.D.; resources, V.C.; data curation, J.-F.H., C.A., F.C., M.M., F.-L.C., G.G., P.-H.L., I.D., J.L., I.M., N.G., L.C., M.C., V.C. and C.D.; writing—original draft preparation, J.-F.H., C.A. and C.D.; writing—review and editing, J.-F.H., C.A., F.C., M.M., F.-L.C., G.G., P.-H.L., I.D., J.L., I.M., N.G., L.C., M.C., V.C. and C.D.; visualization, J.-F.H., C.A. and C.D.; supervision, V.C. and C.D.; project administration, V.C. and C.D.; funding acquisition, V.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The local ethics committee approved the use of patient data for this retrospective analysis.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Appendix A.1. Data Collection
On the 1.5 T scanner, the sequence parameters were: TR = 24 ms, TE = 6.00 ms, flip angle = 90.3 directions of measurement, 16 cm FOV, 131 × 131 matrix, and 5 mm section thickness. Twelve-channel head coils were used. Foci of diffusion were measured in the longest axial axis. DWI b-value was b = 1000 for all studies.
Appendix A.2. Patients’ Management
Appendix A.2.1. Medical Management and Simple Flow Blockage Technique (SFB)
Clopidogrel (75 mg daily) was given within the days before CAS, with assessment of platelet inhibition (PRU, Platelet Reactive Units) (VerifyNow, Instrumentation Laboratory, San Diego, CA, USA) before the procedure.
In cases of clopidogrel resistance (230–240 P2Y12 reaction units PRU by the VerifyNow P2Y12 assay or platelet inhibition rate <20%), prasugrel (20 mg) was given the day before the intervention and platelet inhibition was tested again before the procedure.
All patients had subsequently 3 months of dual antiplatelet medication (aspiring 75 mg), then lifelong aspirin.
In cases of emergency stenting for hemodynamic symptoms or early recurrence, a loading dose of platelet inhibitor (300 mg of clopidogrel or 20 mg of prasugrel) was administered and platelet inhibition was then assessed.
All procedures were performed via a femoral artery approach, and 150 IU/kg heparin was administered intravenously after the placement of the 9-French balloon guiding catheter (Concentric medical, Mountain View, CA, USA) into the targeted common carotid artery. The balloon guiding catheter was prepared according to the instructions provided by the manufacturer, using a combination of contrast agent with saline (50% by volume) to prepare balloon inflation media.
Atropine (0.01–0.02 mg/kg) was administered intravenously at the time of angioplasty, which was performed using a 4.0–7.0 mm balloon (Ultra-soft SV monorail balloon, Boston Scientific, Marlborough, MA, USA).
All procedures were performed under conscious sedation by experienced interventional neuroradiologists. A baseline angiographic run was performed after the inflation of the balloon guiding catheter in the common carotid artery, and allowed to determine the different angiographic patterns.
In all cases, flushing of the guiding catheter was temporarily interrupted during the critical steps (crossing of culprit lesions, stent deployment, angioplasty) to avoid antegrade embolization.
After a dangerous maneuver (crossing of culprit lesions, stent deployment, angioplasty), two steps were respected: (1) Pump aspiration (Penumbra, Alameda, CA, USA) set on the recommended vacuum pressure of −25.5 inches Hg (−86.4 kPa) via a rotating hemostatic valve (RHV) for approximately 10 s before balloon deflation, to avoid potential embolization from the stagnating column of blood distal to the balloon or from the guiding catheter itself; and (2) after balloon deflation, the RHV is opened for a few seconds and closed progressively during activation of the flushing line, to assure that the RHV is clean (aspiration is performed through it in prevention of accumulated debris inside the RHV).
Appendix A.2.2. Follow-Up and Outcome
Patients with preprocedural severe stenosis (>90%), severe contralateral stenosis or occlusion, or with periprocedural arterial hypertension were considered at high risk of reperfusion syndrome, leading to a stricter blood pressure monitoring and management with a target level of <120/80 mmHg. Patients were treated after the procedure with clopidogrel (75 mg daily) or prasugrel (10 mg daily) in the case of clopidogrel resistance (in the absence of contraindication). This treatment was delayed by 6 to 24 h for patients treated with intravenous thrombolysis.
Appendix B

Figure A1.
Example of new punctiform ischemic DWI-MRI lesions for a patient with fluctuant left-sided hemiparesis. Initial MRI (5 h from onset) did not find any intracranial large vessel occlusion, but DWI-MRI depicted punctiform ischemic lesions in the right anterior junctional area. (A) Perfusion MRI showed a large right sylvian hypoperfusion (TMax > 6 s). (B) MR-angiography of supra-aortic arteries objectified a severe proximal ICA stenosis (C; white arrow) confirmed by DSA performed (130 h after onset) before (D; white arrow) a successful carotid artery stenting (E). DWI-MRI performed 24 h after CAS objectified new silent punctiform DWI-MRI lesions in the same right anterior junctional area (F).


Figure A2.
This patient presented right hemiparesis with a symptomatic 75% left ICA stenosis confirmed with angio-MR (A) without any ischemic brain lesions on the DWI-MRI performed 8 h from symptom onset (B,C), but perfusion MRI showed left sylvian hypoperfusion (TMax > 6 s) (D). Carotid artery stenting performed 1 day after symptom onset confirmed the ICA stenosis (E) and the stenting was successfully performed (F). However, the patient presented pre-procedural hypertension involving strict blood pressure monitoring after the CAS with a target level of <120/80 mmHg. The DWI-MRI performed 25 h from the CAS revealed symptomatic new cerebral lesions (punctiform and >10 mm) in the ipsilateral side (G,H) without large intracranial vessel occlusion. Dual antiplatelet medication was continued. However, the 30-h CT performed for a neurologic deterioration revealed an intraparenchymal hemorrhage (I) corresponding to a reperfusion syndrome.

References
- North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial Effect of Carotid Endarterectomy in Symptomatic Patients with High-Grade Carotid Stenosis. N. Engl. J. Med. 1991, 325, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef]
- Mas, J.-L.; Chatellier, G.; Beyssen, B.; Branchereau, A.; Moulin, T.; Becquemin, J.-P.; Larrue, V.; Lièvre, M.; Leys, D.; Bonneville, J.-F.; et al. Endarterectomy versus Stenting in Patients with Symptomatic Severe Carotid Stenosis. N. Engl. J. Med. 2006, 355, 1660–1671. [Google Scholar] [CrossRef] [PubMed]
- Ringleb, A.P.; Allenberg, J.R.; Bruckmann, H.; Eckstein, H.H.; Fraedrich, G.; Hartmann, M.; Hennerici, M.G.; Jansen, O.; Klein, E.G.; Kunze, A.; et al. 30 day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: A randomised non-inferiority trial. Lancet 2006, 368, 1239–1247. [Google Scholar] [CrossRef]
- International Carotid Stenting Study investigators; Ederle, J.; Dobson, J.; Featherstone, R.L.; Bonati, L.H.; Van Der Worp, H.B.; De Borst, G.J.; Lo, T.H.; Gaines, P.; Dorman, P.J.; et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): An interim analysis of a randomised controlled trial. Lancet 2010, 375, 985–997. [Google Scholar] [CrossRef] [PubMed]
- Carotid Stenting Trialists’ Collaboration; Bonati, L.H.; Dobson, J.; Algra, A.; Branchereau, A.; Chatellier, G.; Fraedrich, G.; Mali, W.P.; Zeumer, H.; Brown, M.M.; et al. Short-term outcome after stenting versus endarterectomy for symptomatic carotid stenosis: A preplanned meta-analysis of individual patient data. Lancet 2010, 376, 1062–1073. [Google Scholar] [CrossRef]
- Haussen, D.C.; Grossberg, J.A.; Bouslama, M.; Pradilla, G.; Belagaje, S.; Bianchi, N.; Allen, J.W.; Frankel, M.; Nogueira, R.G. Carotid Web (Intimal Fibromuscular Dysplasia) Has High Stroke Recurrence Risk and Is Amenable to Stenting. Stroke 2017, 48, 3134–3137. [Google Scholar] [CrossRef]
- Sivan-Hoffmann, R.; Gory, B.; Armoiry, X.; Goyal, M.; Riva, R.; Lab, C.; Lukaszewicz, A.-C.; Lehot, J.-J.; Derex, L.; Turjman, F. Stent-Retriever Thrombectomy for Acute Anterior Ischemic Stroke with Tandem Occlusion: A Systematic Review and Meta-Analysis. Eur. Radiol. 2016, 27, 247–254. [Google Scholar] [CrossRef]
- Omran, J.; Mahmud, E.; White, C.; Aronow, H.D.; Drachman, D.E.; Gray, W.; Abdullah, O.; Abu-Fadel, M.; Firwana, B.; Mishkel, G.; et al. Proximal balloon occlusion versus distal filter protection in carotid artery stenting: A meta-analysis and review of the literature. Catheter. Cardiovasc. Interv. 2016, 89, 923–931. [Google Scholar] [CrossRef]
- Dargazanli, C.; Mahmoudi, M.; Cappucci, M.; Collemiche, F.-L.; Labreuche, J.; Habza, O.; Gascou, G.; Lefèvre, P.-H.; Eker, O.; Mourand, I.; et al. Angiographic Patterns and Outcomes Achieved by Proximal Balloon Occlusion in Symptomatic Carotid Artery Stenosis Stenting. Clin. Neuroradiol. 2019, 30, 363–372. [Google Scholar] [CrossRef]
- Dietz, A.; Berkefeld, J.; Theron, J.G.; Schmitz-Rixen, T.; Zanella, F.E.; Turowski, B.; Steinmetz, H.; Sitzer, M. Endovascular Treatment of Symptomatic Carotid Stenosis Using Stent Placement. Stroke 2001, 32, 1855–1859. [Google Scholar] [CrossRef] [PubMed]
- Voeks, J.H.; Howard, G.; Roubin, G.S.; Malas, M.B.; Cohen, D.J.; Sternbergh, I.W.C.; Aronow, H.D.; Eskandari, M.K.; Sheffet, A.J.; Lal, B.K.; et al. Age and Outcomes After Carotid Stenting and Endarterectomy. Stroke 2011, 42, 3484–3490. [Google Scholar] [CrossRef]
- Brott, T.G.; Hobson, R.W.; Howard, G.; Roubin, G.S.; Clark, W.M.; Brooks, W.; Mackey, A.; Hill, M.D.; Leimgruber, P.P.; Sheffet, A.J.; et al. Stenting versus Endarterectomy for Treatment of Carotid-Artery Stenosis. N. Engl. J. Med. 2010, 363, 11–23. [Google Scholar] [CrossRef]
- Brott, T.G.; Howard, G.; Roubin, G.S.; Meschia, J.F.; Mackey, A.; Brooks, W.; Moore, W.S.; Hill, M.D.; Mantese, V.A.; Clark, W.M.; et al. Long-Term Results of Stenting versus Endarterectomy for Carotid-Artery Stenosis. N. Engl. J. Med. 2016, 374, 1021–1031. [Google Scholar] [CrossRef] [PubMed]
- Sardar, P.; Chatterjee, S.; Aronow, H.D.; Kundu, A.; Ramchand, P.; Mukherjee, D.; Nairooz, R.; Gray, W.A.; White, C.J.; Jaff, M.R.; et al. Carotid Artery Stenting Versus Endarterectomy for Stroke Prevention. J. Am. Coll. Cardiol. 2017, 69, 2266–2275. [Google Scholar] [CrossRef] [PubMed]
- Knappich, C.; Kuehnl, A.; Tsantilas, P.; Schmid, S.; Breitkreuz, T.; Kallmayer, M.; Zimmermann, A.; Eckstein, H.-H. The Use of Embolic Protection Devices Is Associated With a Lower Stroke and Death Rate After Carotid Stenting. JACC Cardiovasc. Interv. 2017, 10, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.S.; Mezher, A.W.; Catapano, J.S.; Godzik, J.; Baranoski, J.F.; Nakaji, P.; Albuquerque, F.C.; Lawton, M.T.; Little, A.S.; Ducruet, A.F. Nationwide Trends in Carotid Endarterectomy and Carotid Artery Stenting in the Post-CREST Era. Stroke 2020, 51, 579–587. [Google Scholar] [CrossRef]
- Brott, T.G.; Halperin, J.L.; Abbara, S.; Bacharach, J.M.; Barr, J.D.; Bush, R.L.; Cates, C.U.; Creager, M.A.; Fowler, S.B.; Friday, G.; et al. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: Executive Summary. Circulation 2011, 124, 489–532. [Google Scholar] [CrossRef]
- Bonati, L.H.; Jongen, L.M.; Haller, S.; Flach, H.Z.; Dobson, J.; Nederkoorn, P.J.; Macdonald, S.; Gaines, A.P.; Waaijer, A.; Stierli, P.; et al. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: A substudy of the International Carotid Stenting Study (ICSS). Lancet Neurol. 2010, 9, 353–362. [Google Scholar] [CrossRef]
- Schnaudigel, S.; Gröschel, K.; Pilgram, S.M.; Kastrup, A. New Brain Lesions after Carotid Stenting versus Carotid Endarterectomy. Stroke 2008, 39, 1911–1919. [Google Scholar] [CrossRef]
- Gensicke, H.; Zumbrunn, T.; Jongen, L.M.; Nederkoorn, P.J.; Macdonald, S.; Gaines, P.A.; Lyrer, P.A.; Wetzel, S.G.; van der Lugt, A.; Mali, W.P.T.M.; et al. Characteristics of Ischemic Brain Lesions After Stenting or Endarterectomy for Symptomatic Carotid Artery Stenosis. Stroke 2013, 44, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Bendszus, M.; Koltzenburg, M.; Burger, R.; Warmuth-Metz, M.; Hofmann, E.; Solymosi, L. Silent embolism in diagnostic cerebral angiography and neurointerventional procedures: A prospective study. Lancet 1999, 354, 1594–1597. [Google Scholar] [CrossRef]
- Kastrup, A.; Gröschel, K.; Schnaudigel, S.; Nägele, T.; Schmidt, F.; Ernemann, U. Target lesion ulceration and arch calcification are associated with increased incidence of carotid stenting-associated ischemic lesions in octogenarians. J. Vasc. Surg. 2008, 47, 88–95. [Google Scholar] [CrossRef]
- Spagnoli, L.G.; Mauriello, A.; Sangiorgi, G.; Fratoni, S.; Bonanno, E.; Schwartz, R.S.; Piepgras, D.G.; Pistolese, R.; Ippoliti, A.; Holmes, D.R. Extracranial Thrombotically Active Carotid Plaque as a Risk Factor for Ischemic Stroke. JAMA 2004, 292, 1845–1852. [Google Scholar] [CrossRef]
- Naggara, O.; Touzé, E.; Beyssen, B.; Trinquart, L.; Chatellier, G.; Meder, J.-F.; Mas, J.-L. Anatomical and Technical Factors Associated With Stroke or Death During Carotid Angioplasty and Stenting. Stroke 2011, 42, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, H.-H.; Ringleb, P.; Allenberg, J.-R.; Berger, J.; Fraedrich, G.; Hacke, W.; Hennerici, M.; Stingele, R.; Fiehler, J.; Zeumer, H.; et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: A multinational, prospective, randomised trial. Lancet Neurol. 2008, 7, 893–902. [Google Scholar] [CrossRef]
- Bonati, L.H.; Dobson, J.; Featherstone, R.L.; Ederle, J.; van der Worp, H.B.; de Borst, G.J.; Mali, W.P.T.M.; Beard, J.D.; Cleveland, T.; Engelter, S.T.; et al. Long-term outcomes after stenting versus endarterectomy for treatment of symptomatic carotid stenosis: The International Carotid Stenting Study (ICSS) randomised trial. Lancet 2014, 385, 529–538. [Google Scholar] [CrossRef]
- Liu, H.; Chu, J.; Zhang, L.; Liu, C.; Yan, Z.; Zhou, S. Clinical Comparison of Outcomes of Early versus Delayed Carotid Artery Stenting for Symptomatic Cerebral Watershed Infarction due to Stenosis of the Proximal Internal Carotid Artery. BioMed Res. Int. 2016, 2016, 6241546. [Google Scholar] [CrossRef]
- Song, K.S.; Kwon, O.-K.; Hwang, G.; Bae, H.-J.; Han, M.-K.; Kim, B.J.; Bang, J.S.; Oh, C.W. Early carotid artery stenting for symptomatic carotid artery stenosis. Acta Neurochir. 2015, 157, 1873–1878. [Google Scholar] [CrossRef]
- Meschia, J.F.; Hopkins, L.N.; Altafullah, I.; Wechsler, L.R.; Stotts, G.; Gonzales, N.R.; Voeks, J.H.; Howard, G.; Brott, T.G. Time From Symptoms to Carotid Endarterectomy or Stenting and Perioperative Risk. Stroke 2015, 46, 3540–3542. [Google Scholar] [CrossRef]
- Kwolek, C.J.; Jaff, M.R.; Leal, J.I.; Hopkins, L.N.; Shah, R.M.; Hanover, T.M.; Macdonald, S.; Cambria, R.P.; Flores, A.; Leal, I.; et al. Results of the ROADSTER multicenter trial of transcarotid stenting with dynamic flow reversal. J. Vasc. Surg. 2015, 62, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Dakour-Aridi, H.; Kashyap, V.S.; Wang, G.J.; Eldrup-Jorgensen, J.; Schermerhorn, M.L.; Malas, M.B. The impact of age on in-hospital outcomes after transcarotid artery revascularization, transfemoral carotid artery stenting, and carotid endarterectomy. J. Vasc. Surg. 2020, 72, 931–942. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).