
Elevated Interleukin-6 Levels in the Circulation and Peritoneal Fluid of Patients with Ovarian Cancer as a Potential Diagnostic Biomarker: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Quality Assessment
2.4. Data Collection and Extraction
2.5. Data Analysis and Statistics
3. Results
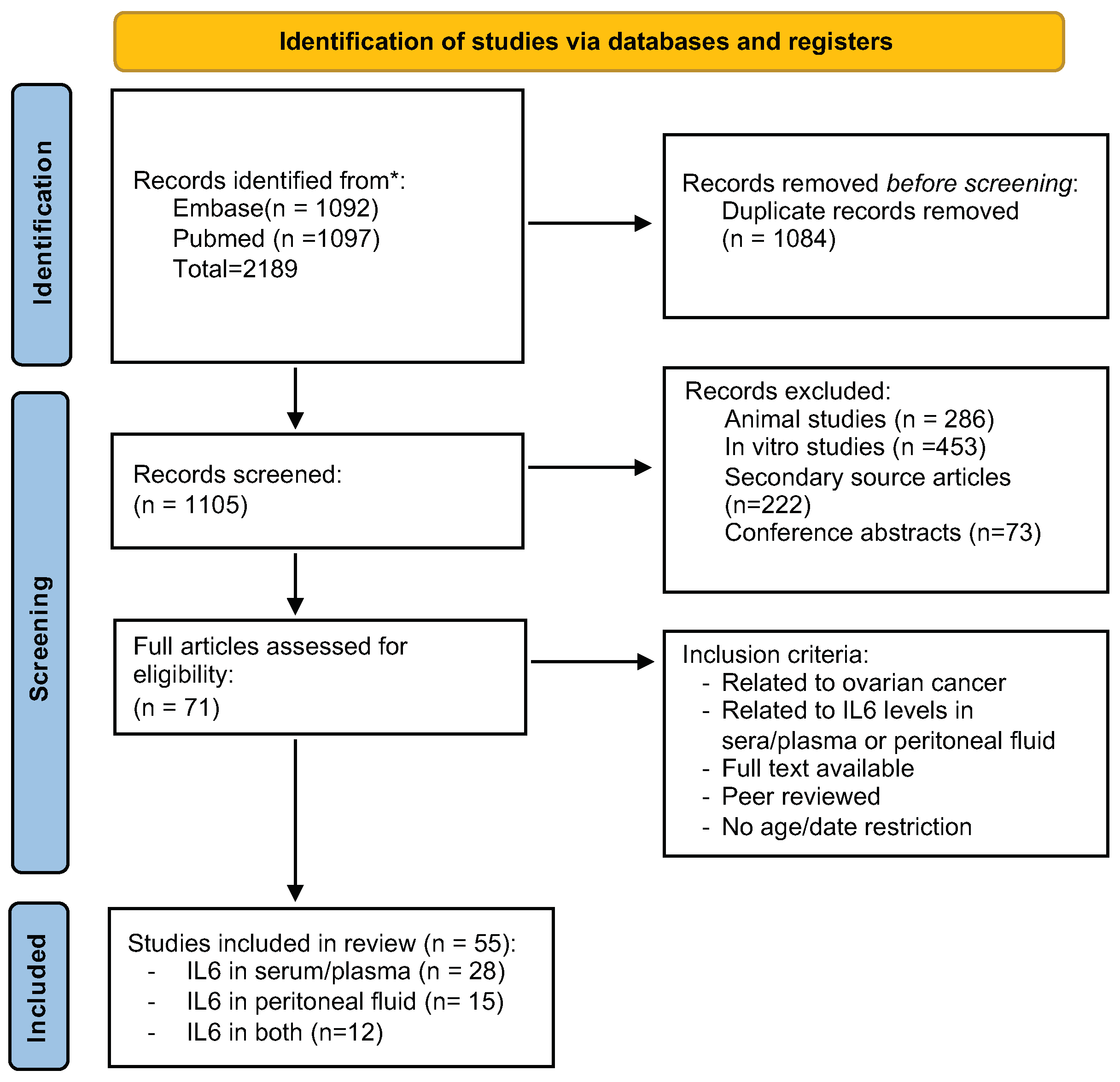
3.1. Study Selection and Characterization
3.2. STROBE Checklist
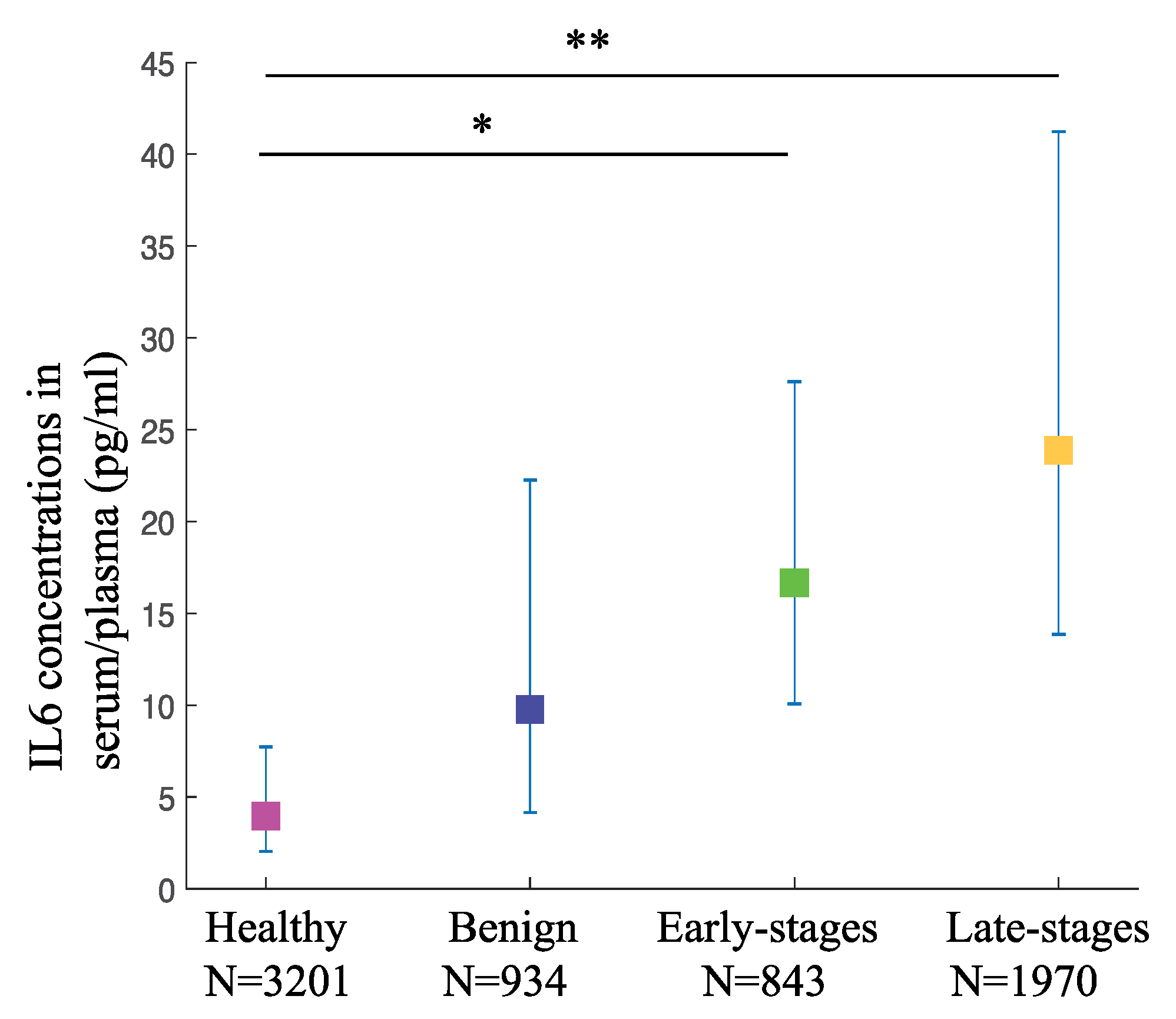
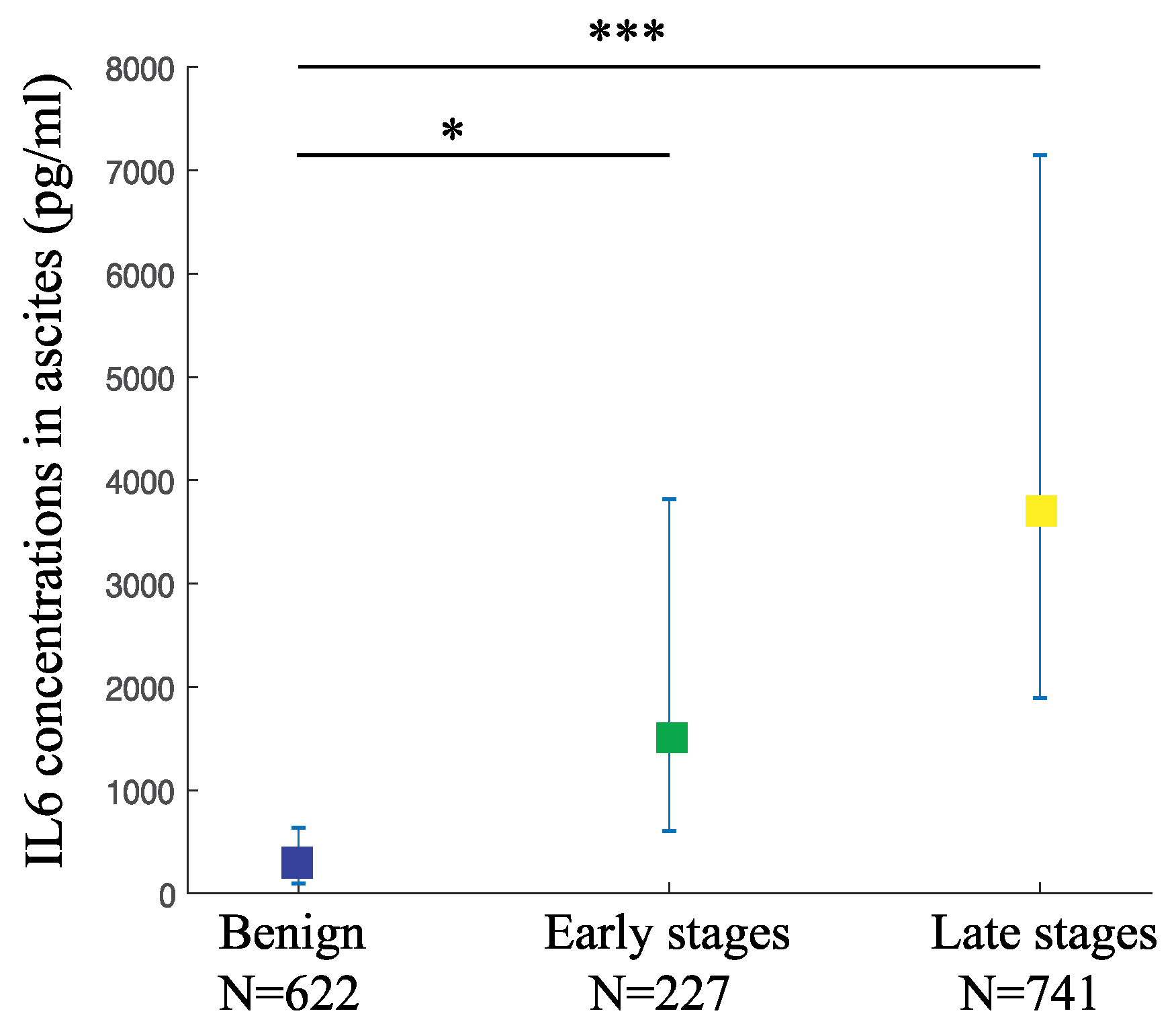
3.3. IL6 Levels in the Circulation and Ascites
3.4. Sensitivities and Specificities
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Jelovac, D.; Armstrong, D.K. Recent progress in the diagnosis and treatment of ovarian cancer. CA Cancer J. Clin. 2011, 61, 183–203. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.S.; Rubin, S.C. Screening for ovarian cancer in the general population. Best Pract. Res. Clin. Obs. Gynaecol. 2006, 20, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Lengyel, E. Ovarian cancer development and metastasis. Am. J. Pathol. 2010, 177, 1053–1064. [Google Scholar] [CrossRef]
- Parsa, N. Environmental factors inducing human cancers. Iran. J. Public Health 2012, 41, 1–9. [Google Scholar] [PubMed]
- Van Cott, C. Cancer Genetics. Surg. Clin. N. Am. 2020, 100, 483–498. [Google Scholar] [CrossRef] [PubMed]
- Dion, L.; Mimoun, C.; Nyangoh Timoh, K.; Bendifallah, S.; Bricou, A.; Collinet, P.; Touboul, C.; Ouldamer, L.; Azaïs, H.; Dabi, Y.; et al. Ovarian Cancer in the Elderly: Time to Move towards a More Logical Approach to Improve Prognosis—A Study from the FRANCOGYN Group. J. Clin. Med. 2020, 9, 1339. [Google Scholar] [CrossRef]
- Toss, A.; Tomasello, C.; Razzaboni, E.; Contu, G.; Grandi, G.; Cagnacci, A.; Schilder, R.J.; Cortesi, L. Hereditary ovarian cancer: Not only BRCA 1 and 2 genes. BioMed Res. Int. 2015, 2015, 341723. [Google Scholar] [CrossRef]
- Duggan, M.A.; Anderson, W.F.; Altekruse, S.; Penberthy, L.; Sherman, M.E. The Surveillance, Epidemiology, and End Results (SEER) Program and Pathology: Toward Strengthening the Critical Relationship. Am. J. Surg. Pathol. 2016, 40, e94–e102. [Google Scholar] [CrossRef]
- Ma, X.; Yu, H. Global burden of cancer. Yale J. Biol. Med. 2006, 79, 85–94. [Google Scholar] [PubMed]
- Ataseven, B.; Harter, P.; Grimm, C.; Heitz, F.; Heikaus, S.; Traut, A.; Kahl, A.; Kurzeder, C.; Prader, S.; du Bois, A. The revised 2014 FIGO staging system for epithelial ovarian cancer: Is a subclassification into FIGO stage IVA and IVB justified? Gynecol. Oncol. 2016, 142, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Trabert, B.; DeSantis, C.E.; Miller, K.D.; Samimi, G.; Runowicz, C.D.; Gaudet, M.M.; Jemal, A.; Siegel, R.L. Ovarian cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, F.; Barber, H.R.K. Ovarian Carcinoma: Etiology, Diagnosis, and Treatment, 3th ed.; Springer: New York, NY, USA, 1992. [Google Scholar] [CrossRef]
- Gumusoglu, E. The Role of Circulating Biomarkers in the Early Diagnosis of Ovarian Cancer; IntechOpen: London, UK, 2018. [Google Scholar]
- Meyer, T.; Rustin, G.J.S. Role of tumour markers in monitoring epithelial ovarian cancer. Br. J. Cancer 2000, 82, 1535–1538. [Google Scholar] [CrossRef]
- Muyldermans, M.; Cornillie, F.J.; Koninckx, P.R. CA125 and endometriosis. Hum. Reprod. Update 1995, 1, 173–187. [Google Scholar] [CrossRef] [PubMed]
- Montagnana, M.; Danese, E.; Giudici, S.; Franchi, M.; Guidi, G.C.; Plebani, M.; Lippi, G. HE4 in Ovarian Cancer; Elsevier Science & Technology: Amsterdam, The Netherlands, 2011; Volume 55, pp. 1–20. [Google Scholar]
- Bristow, R.E.; Santillan, A.; Diaz-Montes, T.P.; Gardner, G.J.; Giuntoli, R.L.; Meisner, B.C.; Frick, K.D.; Armstrong, D.K. Centralization of care for patients with advanced-stage ovarian cancer: A cost-effectiveness analysis. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2007, 109, 1513–1522. [Google Scholar] [CrossRef] [PubMed]
- Nassir, M.; Darb-Esfahani, S.; Richter, R.; Chekerov, R.; Hall, C.; Muallem, M.Z.; Denkert, C.; Stamatian, F.; Fotopoulou, C.; Sehouli, J.; et al. HE4 Tissue Expression in Borderline Ovarian Tumors: A Pilot Study by the Tumorbank Ovarian Cancer Network. Anticancer Res. 2013, 33, 1673–1677. [Google Scholar]
- Moore, R.G.; Miller, M.C.; Eklund, E.E.; Lu, K.H.; Bast, R.C.; Lambert-Messerlian, G. Serum levels of the ovarian cancer biomarker HE4 are decreased in pregnancy and increase with age. Am. J. Obstet. Gynecol. 2012, 206, 349.e1–349.e7. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.A.; Abdou, A.M. Diagnostic accuracy of CA125 and HE4 in ovarian carcinoma patients and the effect of confounders on their serum levels. Curr. Probl. Cancer 2019, 43, 450–460. [Google Scholar] [CrossRef]
- Browning, L.; Patel, M.R.; Horvath, E.B.; Tawara, K.; Jorcyk, C.L. IL-6 and ovarian cancer: Inflammatory cytokines in promotion of metastasis. Cancer Manag. Res. 2018, 10, 6685–6693. [Google Scholar] [CrossRef]
- Quinn, K.M.; Kartikasari, A.E.R.; Cooke, R.E.; Koldej, R.M.; Ritchie, D.S.; Plebanski, M. Impact of age-, cancer-, and treatment-driven inflammation on T cell function and immunotherapy. J. Leukoc. Biol. 2020, 108, 953–965. [Google Scholar] [CrossRef] [PubMed]
- Unver, N.; McAllister, F. IL-6 family cytokines: Key inflammatory mediators as biomarkers and potential therapeutic targets. Cytokine Growth Factor Rev. 2018, 41, 10–17. [Google Scholar] [CrossRef]
- Partridge, E.E.; Barnes, M.N. Epithelial ovarian cancer: Prevention, diagnosis, and treatment. CA Cancer J. Clin. 1999, 49, 297–320. [Google Scholar] [CrossRef] [PubMed]
- Kampan, N.C.; Madondo, M.T.; Reynolds, J.; Hallo, J.; McNally, O.M.; Jobling, T.W.; Stephens, A.N.; Quinn, M.A.; Plebanski, M. Pre-operative sera interleukin-6 in the diagnosis of high-grade serous ovarian cancer. Sci. Rep. 2020, 10, 2213. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto, T. Interleukin-6: Discovery of a pleiotropic cytokine. Arthritis Res Ther. 2006, 8 (Suppl. S2), S2. [Google Scholar] [CrossRef] [PubMed]
- Autelitano, D.J.; Raineri, L.; Knight, K.; Bannister, K.; Rice, G.E. Performance of a multianalyte test as an aid for the diagnosis of ovarian cancer in symptomatic women. J. Transl. Med. 2012, 10, 45. [Google Scholar] [CrossRef] [PubMed]
- Giuntoli, R.L., 2nd; Webb, T.J.; Zoso, A.; Rogers, O.; Diaz-Montes, T.P.; Bristow, R.E.; Oelke, M. Ovarian cancer-associated ascites demonstrates altered immune environment: Implications for antitumor immunity. Anticancer Res. 2009, 29, 2875–2884. [Google Scholar]
- Kartikasari, A.E.R.; Huertas, C.S.; Mitchell, A.; Plebanski, M. Tumor-Induced Inflammatory Cytokines and the Emerging Diagnostic Devices for Cancer Detection and Prognosis. Front. Oncol. 2021, 11, 692142. [Google Scholar] [CrossRef]
- Šimundić, A.M. Measures of Diagnostic Accuracy: Basic Definitions. Ejifcc 2009, 19, 203–211. [Google Scholar]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef]
- Luo, D.H.; Wan, X.; Liu, J.M.; Tong, T.J. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Baratloo, A.; Hosseini, M.; Negida, A.; El Ashal, G. Part 1: Simple Definition and Calculation of Accuracy, Sensitivity and Specificity. Emergency 2015, 3, 48–49. [Google Scholar] [PubMed]
- Wallace, B.C.; Schmid, C.H.; Lau, J.; Trikalinos, T.A. Meta-Analyst: Software for meta-analysis of binary, continuous and diagnostic data. BMC Med. Res. Methodol. 2009, 9, 80. [Google Scholar] [CrossRef]
- Sanna, E.; Tanca, L.; Cherchi, C.; Gramignano, G.; Oppi, S.; Chiai, M.G.; Macciò, A.; Madeddu, C. Decrease in Neutrophil-to-Lymphocyte Ratio during Neoadjuvant Chemotherapy as a Predictive and Prognostic Marker in Advanced Ovarian Cancer. Diagnostics 2021, 11, 1298. [Google Scholar] [CrossRef] [PubMed]
- Micheli, D.C.; Jammal, M.P.; Martins-Filho, A.; Côrtes, J.R.X.D.M.; Souza, C.N.D.; Nomelini, R.S.; Murta, E.F.C.; Tavares-Murta, B.M. Serum cytokines and CXCR2: Potential tumour markers in ovarian neoplasms. Biomarkers 2020, 25, 474–482. [Google Scholar] [CrossRef]
- de Lima, C.A.; Silva Rodrigues, I.S.; Martins-Filho, A.; Côbo Micheli, D.; Martins Tavares-Murta, B.; Candido Murta, E.F.; Simões Nomelini, R. Cytokines in peritoneal fluid of ovarian neoplasms. J. Obstet. Gynaecol. 2020, 40, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, I.S.S.; Martins-Filho, A.; Micheli, D.C.; Lima, C.A.; Tavares-Murta, B.M.; Murta, E.F.C.; Nomelini, R.S. IL-6 and IL-8 as Prognostic Factors in Peritoneal Fluid of Ovarian Cancer. Immunol. Investig. 2020, 49, 510–521. [Google Scholar] [CrossRef] [PubMed]
- Wertel, I.; Suszczyk, D.; Pawłowska, A.; Bilska, M.; Chudzik, A.; Skiba, W.; Paduch, R.; Kotarski, J. Prognostic and Clinical Value of Interleukin 6 and CD45(+)CD14(+) Inflammatory Cells with PD-L1(+)/PD-L2(+) Expression in Patients with Different Manifestation of Ovarian Cancer. J. Immunol. Res. 2020, 2020, 1715064. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Chen, C.; Wang, S.; Li, X.; Fan, T. Efficacy of bevacizumab combined with nedaplatin in the treatment of ovarian cancer and its effects on tumor markers and immunity of patients. J. BUON 2020, 25, 80–86. [Google Scholar]
- Crispim, P.C.A.; Jammal, M.P.; Antão, P.K.A.; Micheli, D.C.; Tavares-Murta, B.M.; Murta, E.F.C.; Nomelini, R.S. IL6, IL8, and IL10 in the distinction of malignant ovarian neoplasms and endometriomas. Am. J. Reprod. Immunol. 2020, 84, e13309. [Google Scholar] [CrossRef]
- Shi, J.; Huo, R.; Li, N.; Li, H.; Zhai, T.; Li, H.; Shen, B.; Ye, J.; Fu, R.; Di, W. CYR61, a potential biomarker of tumor inflammatory response in epithelial ovarian cancer microenvironment of tumor progress. BMC Cancer 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Li, G.; Zhang, K.; Gong, F.; Jin, H. A study on changes and clinical significance of blood glucose, blood lipid and inflammation in patients with ovarian cancer. J. BUON 2019, 24, 2322–2326. [Google Scholar]
- Dalal, V.; Kumar, R.; Kumar, S.; Sharma, A.; Kumar, L.; Sharma, J.B.; Roy, K.K.; Singh, N.; Vanamail, P. Biomarker potential of IL-6 and VEGF-A in ascitic fluid of epithelial ovarian cancer patients. Clin. Chim. Acta 2018, 482, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Bellone, S.; Siegel, E.R.; Altwerger, G.; Menderes, G.; Bonazzoli, E.; Egawa-Takata, T.; Pettinella, F.; Bianchi, A.; Riccio, F.; et al. A novel multiple biomarker panel for the early detection of high-grade serous ovarian carcinoma. Gynecol. Oncol. 2018, 149, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Inflammatory and Nutritional Serum Markers as Predictors of Peri-operative Morbidity and Survival in Ovarian Cancer. Anticancer Res. 2017, 37. [CrossRef]
- Martins-Filho, A.; Jammal, M.P.; Micheli, D.C.; Tavares-Murta, B.M.; Etchebehere, R.M.; Murta, E.F.C.; Nomelini, R.S. Role of Intracystic Cytokines and Nitric Oxide in Ovarian Neoplasms. Scand. J. Immunol. 2017, 86, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Cantón-Romero, J.C.; Miranda-Díaz, A.G.; Bañuelos-Ramírez, J.L.; Carrillo-Ibarra, S.; Sifuentes-Franco, S.; Castellanos-González, J.A.; Rodríguez-Carrizalez, A.D. Markers of Oxidative Stress and Inflammation in Ascites and Plasma in Patients with Platinum-Sensitive, Platinum-Resistant, and Platinum-Refractory Epithelial Ovarian Cancer. Oxidative Med. Cell. Longev. 2017, 2017, 2873030. [Google Scholar] [CrossRef]
- Sanguinete, M.M.M.; Oliveira, P.H.; Martins-Filho, A.; Micheli, D.C.; Tavares-Murta, B.M.; Murta, E.F.C.; Nomelini, R.S. Serum IL-6 and IL-8 Correlate with Prognostic Factors in Ovarian Cancer. Immunol. Investig. 2017, 46, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Hao, C.J.; Li, J.; Liu, P.; Li, X.L.; Hu, Y.Q.; Sun, J.C.; Wei, Y. Effects of the balance between type 1 and type 2 T helper cells on ovarian cancer. Genet. Mol. Res. 2016, 15. [Google Scholar] [CrossRef]
- Mikuła-Pietrasik, J.; Uruski, P.; Szubert, S.; Moszyński, R.; Szpurek, D.; Sajdak, S.; Tykarski, A.; Książek, K. Biochemical composition of malignant ascites determines high aggressiveness of undifferentiated ovarian tumors. Med. Oncol. 2016, 33, 94. [Google Scholar] [CrossRef]
- Chudecka-Głaz, A.M.; Cymbaluk-Płoska, A.A.; Menkiszak, J.L.; Pius-Sadowska, E.; Machaliński, B.B.; Sompolska-Rzechuła, A.; Rzepka-Górska, I.A. Assessment of selected cytokines, proteins, and growth factors in the peritoneal fluid of patients with ovarian cancer and benign gynecological conditions. Onco Targets Ther. 2015, 8, 471–485. [Google Scholar] [CrossRef]
- Block, M.S.; Maurer, M.J.; Goergen, K.; Kalli, K.R.; Erskine, C.L.; Behrens, M.D.; Oberg, A.L.; Knutson, K.L. Plasma immune analytes in patients with epithelial ovarian cancer. Cytokine 2015, 73, 108–113. [Google Scholar] [CrossRef]
- Matsuo, K.; Hasegawa, K.; Yoshino, K.; Murakami, R.; Hisamatsu, T.; Stone, R.L.; Previs, R.A.; Hansen, J.M.; Ikeda, Y.; Miyara, A.; et al. Venous thromboembolism, interleukin-6 and survival outcomes in patients with advanced ovarian clear cell carcinoma. Eur. J. Cancer 2015, 51, 1978–1988. [Google Scholar] [CrossRef]
- Ose, J.; Schock, H.; Tjønneland, A.; Hansen, L.; Overvad, K.; Dossus, L.; Clavel-Chapelon, F.; Baglietto, L.; Boeing, H.; Trichopolou, A.; et al. Inflammatory Markers and Risk of Epithelial Ovarian Cancer by Tumor Subtypes: The EPIC Cohort. Cancer Epidemiol. Biomark. Prev. 2015, 24, 951–961. [Google Scholar] [CrossRef] [PubMed]
- Lane, D.; Matte, I.; Garde-Granger, P.; Laplante, C.; Carignan, A.; Rancourt, C.; Piché, A. Inflammation-regulating factors in ascites as predictive biomarkers of drug resistance and progression-free survival in serous epithelial ovarian cancers. BMC Cancer 2015, 15, 492. [Google Scholar] [CrossRef] [PubMed]
- Trabert, B.; Pinto, L.; Hartge, P.; Kemp, T.; Black, A.; Sherman, M.E.; Brinton, L.A.; Pfeiffer, R.M.; Shiels, M.S.; Chaturvedi, A.K.; et al. Pre-diagnostic serum levels of inflammation markers and risk of ovarian cancer in the prostate, lung, colorectal and ovarian cancer (PLCO) screening trial. Gynecol. Oncol. 2014, 135, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Cândido, E.B.; Silva, L.M.; Carvalho, A.T.; Lamaita, R.M.; Filho, R.M.; Cota, B.D.; da Silva-Filho, A.L. Immune response evaluation through determination of type 1, type 2, and type 17 patterns in patients with epithelial ovarian cancer. Reprod. Sci. 2013, 20, 828–837. [Google Scholar] [CrossRef] [PubMed]
- Poole, E.M.; Lee, I.M.; Ridker, P.M.; Buring, J.E.; Hankinson, S.E.; Tworoger, S.S. A prospective study of circulating C-reactive protein, interleukin-6, and tumor necrosis factor α receptor 2 levels and risk of ovarian cancer. Am. J. Epidemiol. 2013, 178, 1256–1264. [Google Scholar] [CrossRef]
- Dobrzycka, B.; Mackowiak-Matejczyk, B.; Terlikowska, K.M.; Kulesza-Bronczyk, B.; Kinalski, M.; Terlikowski, S.J. Serum levels of IL-6, IL-8 and CRP as prognostic factors in epithelial ovarian cancer. Eur. Cytokine Netw. 2013, 24, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Matte, I.; Lane, D.; Laplante, C.; Rancourt, C.; Piché, A. Profiling of cytokines in human epithelial ovarian cancer ascites. Am. J. Cancer Res. 2012, 2, 566–580. [Google Scholar]
- Clendenen, T.V.; Lundin, E.; Zeleniuch-Jacquotte, A.; Koenig, K.L.; Berrino, F.; Lukanova, A.; Lokshin, A.E.; Idahl, A.; Ohlson, N.; Hallmans, G.; et al. Circulating Inflammation Markers and Risk of Epithelial Ovarian Cancer. Cancer Epidemiol. Biomark. Prev. 2011, 20, 799–810. [Google Scholar] [CrossRef]
- Sen, S.; Kuru, O.; Akbayir, O.; Oguz, H.; Yasasever, V.; Berkman, S. Determination of serum CRP, VEGF, Leptin, CK-MB, CA-15-3 and IL-6 levels for malignancy prediction in adnexal masses. J. Turk. Ger. Gynecol. Assoc. 2011, 12, 214–219. [Google Scholar] [CrossRef]
- Yigit, R.; Figdor, C.G.; Zusterzeel, P.L.; Pots, J.M.; Torensma, R.; Massuger, L.F. Cytokine analysis as a tool to understand tumour-host interaction in ovarian cancer. Eur. J. Cancer 2011, 47, 1883–1889. [Google Scholar] [CrossRef]
- Edgell, T.; Martin-Roussety, G.; Barker, G.; Autelitano, D.J.; Allen, D.; Grant, P.; Rice, G.E. Phase II biomarker trial of a multimarker diagnostic for ovarian cancer. J. Cancer Res. Clin. Oncol. 2010, 136, 1079–1088. [Google Scholar] [CrossRef] [PubMed]
- Nowak, M.; Glowacka, E.; Szpakowski, M.; Szyllo, K.; Malinowski, A.; Kulig, A.; Tchorzewski, H.; Wilczynski, J. Proinflammatory and immunosuppressive serum, ascites and cyst fluid cytokines in patients with early and advanced ovarian cancer and benign ovarian tumors. Neuro Endocrinol. Lett. 2010, 31, 375–383. [Google Scholar] [PubMed]
- Napoletano, C.; Bellati, F.; Landi, R.; Pauselli, S.; Marchetti, C.; Visconti, V.; Sale, P.; Liberati, M.; Rughetti, A.; Frati, L.; et al. Ovarian cancer cytoreduction induces changes in T cell population subsets reducing immunosuppression. J. Cell. Mol. Med. 2010, 14, 2748–2759. [Google Scholar] [CrossRef]
- Tsai-Turton, M.; Santillan, A.; Lu, D.; Bristow, R.E.; Chan, K.C.; Shih Ie, M.; Roden, R.B. p53 autoantibodies, cytokine levels and ovarian carcinogenesis. Gynecol. Oncol. 2009, 114, 12–17. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Amonkar, S.D.; Bertenshaw, G.P.; Chen, T.-H.; Bergstrom, K.J.; Zhao, J.; Seshaiah, P.; Yip, P.; Mansfield, B.C. Development and Preliminary Evaluation of a Multivariate Index Assay for Ovarian Cancer. PLoS ONE 2009, 4, e4599. [Google Scholar] [CrossRef]
- Macciò, A.; Madeddu, C.; Massa, D.; Astara, G.; Farci, D.; Melis, G.B.; Mantovani, G. Interleukin-6 and leptin as markers of energy metabolicchanges in advanced ovarian cancer patients. J. Cell. Mol. Med. 2009, 13, 3951–3959. [Google Scholar] [CrossRef] [PubMed]
- Lutgendorf, S.K.; Weinrib, A.Z.; Penedo, F.; Russell, D.; DeGeest, K.; Costanzo, E.S.; Henderson, P.J.; Sephton, S.E.; Rohleder, N.; Lucci, J.A., 3rd; et al. Interleukin-6, cortisol, and depressive symptoms in ovarian cancer patients. J. Clin. Oncol. 2008, 26, 4820–4827. [Google Scholar] [CrossRef]
- Kavsak, P.A.; Lee, A.; Hirte, H.; Young, E.; Gauldie, J. Cytokine elevations in acute coronary syndrome and ovarian cancer: A mechanism for the up-regulation of the acute phase proteins in these different disease etiologies. Clin. Biochem. 2008, 41, 607–610. [Google Scholar] [CrossRef]
- Lambeck, A.J.A.; Crijns, A.P.G.; Leffers, N.; Sluiter, W.J.; Ten Hoor, K.A.; Braid, M.; Van Der Zee, A.G.J.; Daemen, T.; Nijman, H.W.; Kast, W.M. Serum Cytokine Profiling as a Diagnostic and Prognostic Tool in Ovarian Cancer: A Potential Role for Interleukin 7. Clin. Cancer Res. 2007, 13, 2385–2391. [Google Scholar] [CrossRef]
- Chechlinska, M.; Kaminska, J.; Markowska, J.; Kramar, A.; Steffen, J. Peritoneal fluid cytokines and the differential diagnosis of benign and malignant ovarian tumors and residual/recurrent disease examination. Int. J. Biol. Markers 2007, 22, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, E.S.; Lutgendorf, S.K.; Sood, A.K.; Anderson, B.; Sorosky, J.; Lubaroff, D.M. Psychosocial factors and interleukin-6 among women with advanced ovarian cancer. Cancer 2005, 104, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Macciò, A.; Madeddu, C.; Massa, D.; Mudu, M.C.; Lusso, M.R.; Gramignano, G.; Serpe, R.; Melis, G.B.; Mantovani, G. Hemoglobin levels correlate with interleukin-6 levels in patients with advanced untreated epithelial ovarian cancer: Role of inflammation in cancer-related anemia. Blood 2005, 106, 362–367. [Google Scholar] [CrossRef]
- Gorelik, E. Multiplexed Immunobead-Based Cytokine Profiling for Early Detection of Ovarian Cancer. Cancer Epidemiol. Biomark. Prev. 2005, 14, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Daraï, E.; Detchev, R.; Hugol, D.; Quang, N.T. Serum and cyst fluid levels of interleukin (IL) -6, IL-8 and tumour necrosis factor-alpha in women with endometriomas and benign and malignant cystic ovarian tumours. Hum. Reprod. 2003, 18, 1681–1685. [Google Scholar] [CrossRef] [PubMed]
- Dobryszycka, W.; Katnik-Prastowska, I.; Gerber, J.; Lemańska, K.; Utko, K.; Rozdolski, K. Serum haptoglobin, CA 125 and interleukin 6 levels in malignant and non-malignant tumors of the ovary. Arch. Immunol. Ther. Exp. Warsz 1999, 47, 229–236. [Google Scholar]
- Tempfer, C.; Zeisler, H.; Sliutz, G.; Haeusler, G.; Hanzal, E.; Kainz, C. Serum Evaluation of Interleukin 6 in Ovarian Cancer Patients. Gynecol. Oncol. 1997, 66, 27–30. [Google Scholar] [CrossRef]
- Scambia, G.; Testa, U.; Benedetti Panici, P.; Foti, E.; Martucci, R.; Gadducci, A.; Perillo, A.; Facchini, V.; Peschle, C.; Mancuso, S. Prognostic significance of interleukin 6 serum levels in patients with ovarian cancer. Br. J. Cancer 1995, 71, 354–356. [Google Scholar] [CrossRef] [PubMed]
- Plante, M.; Rubin, S.C.; Wong, G.Y.; Federici, M.G.; Finstad, C.L.; Gastl, G.A. Interleukin-6 level in serum and ascites as a prognostic factor in patients with epithelial ovarian cancer. Cancer 1994, 73, 1882–1888. [Google Scholar] [CrossRef]
- Schröder, W.; Ruppert, C.; Bender, H.G. Concomitant measurements of interleukin-6 (IL-6) in serum and peritoneal fluid of patients with benign and malignant ovarian tumors. Eur. J. Obstet. Gynecol. Reprod. Biol. 1994, 56, 43–46. [Google Scholar] [CrossRef]
- van der Zee, A.G.; de Cuyper, E.M.; Limburg, P.C.; de Bruijn, H.W.; Hollema, H.; Bijzet, J.; Krans, M.; de Vries, E.G. Higher levels of interleukin-6 in cystic fluids from patients with malignant versus benign ovarian tumors correlate with decreased hemoglobin levels and increased platelet counts. Cancer 1995, 75, 1004–1009. [Google Scholar] [CrossRef]
- Moradi, M.M.; Carson, L.F.; Weinberg, B.; Haney, A.F.; Twiggs, L.B.; Ramakrishnan, S. Serum and ascitic fluid levels of interleukin-1, interleukin-6, and tumor necrosis factor-alpha in patients with ovarian epithelial cancer. Cancer 1993, 72, 2433–2440. [Google Scholar] [CrossRef]
- Gastl, G.; Plante, M.; Finstad, C.L.; Wong, G.Y.; Federici, M.G.; Bander, N.H.; Rubin, S.C. High IL-6 levels in ascitic fluid correlate with reactive thrombocytosis in patients with epithelial ovarian cancer. Br. J. Haematol. 1993, 83, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Berek, J.S.; Chung, C.; Kaldi, K.; Watson, J.M.; Knox, R.M.; Martínez-Maza, O. Serum interleukin-6 levels correlate with disease status in patients with epithelial ovarian cancer. Am. J. Obstet. Gynecol. 1991, 164, 1038–1042. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Number of Studies | Pooled Weighted Mean (pg/mL) | 95% Confident Interval | p-Value (Post-Hoc: OC vs. Healthy Controls | p-Value (Post-Hoc OC vs. Benign Controls |
|---|---|---|---|---|---|
| Healthy controls | 20 | 3.96 | 2.02–7.73 | ||
| Benign controls | 21 | 9.62 | 4.16–22.26 | ||
| Early-stage OC | 20 | 16.67 | 10.06–27.61 | 0.018 | 0.650 |
| Late-stage OC | 20 | 23.88 | 13.84–41.23 | 0.002 | 0.225 |
| Type | Number of Studies | Pooled Weighted Mean (pg/mL) | 95% Confident Interval | p-Value (Post-Hoc OC vs. Benign) |
|---|---|---|---|---|
| Benign | 16 | 247.33 | 96.2–636.0 | |
| Early-stage OC | 11 | 1519.21 | 604.6–3817.7 | 0.0195 |
| Late-stage OC | 13 | 3676.92 | 1891.7–7146.7 | 0.0002 |
| Type | Number of Studies | Sensitivity | Specificity | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall | 95% CI | p-Value | τ2 | Overall | 95% CI | p-Value | τ2 | ||
| Serum/plasma IL6 for mixed stages | 7 | 76.7% | 0.646–0.856 | <0.001 | 0.433 | 72% | 0.638–0.790 | <0.001 | 0.165 |
| Ascitic IL6 for mixedstages | 5 | 84% | 0.710–0.919 | <0.001 | 0.492 | 74% | 0.646–0.826 | <0.001 | 0.112 |
| IL6 as one of the combined marker for early stage OC | Gorelik et al., 2005 | 84.1% | Combined with CA124, GCSF, EGF and VEGF | 75.7% | Combined with CA124, GCSF, EGF and VEGF | ||||
| Han et al., 2018 | 84.2% | Combined with CA125, HE4 and ECAD | 95.7% | Combined with CA125, HE4 and ECAD | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amer, H.; Kartikasari, A.E.R.; Plebanski, M. Elevated Interleukin-6 Levels in the Circulation and Peritoneal Fluid of Patients with Ovarian Cancer as a Potential Diagnostic Biomarker: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 1335. https://doi.org/10.3390/jpm11121335
Amer H, Kartikasari AER, Plebanski M. Elevated Interleukin-6 Levels in the Circulation and Peritoneal Fluid of Patients with Ovarian Cancer as a Potential Diagnostic Biomarker: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(12):1335. https://doi.org/10.3390/jpm11121335
Chicago/Turabian StyleAmer, Hina, Apriliana E. R. Kartikasari, and Magdalena Plebanski. 2021. "Elevated Interleukin-6 Levels in the Circulation and Peritoneal Fluid of Patients with Ovarian Cancer as a Potential Diagnostic Biomarker: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 12: 1335. https://doi.org/10.3390/jpm11121335
APA StyleAmer, H., Kartikasari, A. E. R., & Plebanski, M. (2021). Elevated Interleukin-6 Levels in the Circulation and Peritoneal Fluid of Patients with Ovarian Cancer as a Potential Diagnostic Biomarker: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 11(12), 1335. https://doi.org/10.3390/jpm11121335