Abstract
The inflammatory myofibroblastic tumor (IMT) is a rare tumor that can develop in any systemic organ. Its features are generally benign, but it often resembles malignancies and is treated surgically. Our patient was an 82-year-old female complaining of abdominal discomfort. Computed tomography demonstrated a 5 cm, ill-enhanced mass at the pancreas head. Upper gastrointestinal endoscopy revealed a duodenal submucosal tumor with apical erosion. Endoscopic ultrasonography (EUS) demonstrated a heterogeneous, low-echoic pancreas mass without clear margins. Fine-needle aspiration biopsy (FNAB) demonstrated spindle myofibroblastic tissues with lymphoplasmacyte and eosinophil infiltration, confirming an IMT diagnosis. Surprisingly, the tumor spontaneously regressed in one month without medication. Histological diagnosis using EUS-FNAB is essential for the rare pancreatic solid tumor like IMT.
1. Introduction
The inflammatory myofibroblastic tumor (IMT) is a rare tumorous lesion that can develop in any systemic organ. It has a relatively young onset (mainly in newborns to young adults) and consists histologically of proliferative myofibroblastic tissues with heavy infiltration of inflammatory cells, mainly lymphocytes and plasma cells [1]. It often shows benign biological behaviors, but it is sometimes accompanied by somatic mutations in clinically important genes [2,3,4,5] that can cause metastasis and/or recurrence [2,5]. The differential diagnosis from malignancies is therefore difficult, especially in high-aged cases, and most IMTs are surgically resected before finally being diagnosed [2,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26].
Anti-inflammatory agents, such as corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDS), are effective for some IMTs [27,28], and a small proportion of IMTs regress spontaneously [27,28,29,30,31,32,33,34,35,36,37,38]. To date, several cases of pancreatic IMTs have been reported [6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26], but histologically proven cases (proven for myofibroblastic component) with spontaneous remission have hardly been reported.
2. Case Presentation
An 82-year-old Japanese female was referred to our hospital after a month of complaints of upper abdominal discomfort. First, she visited the nearest hospital and underwent upper gastrointestinal endoscopy that pointed multiple erosions and an extrinsic compression at the posterior pylorus. Medication had been initiated using nizatidine, rebamipide and oxetacaine, but it was not effective. She had a history of hypertension, but her family history was unremarkable. Blood tests showed modestly elevated IgG (1950 mg/dL, normal range: 870–1700 mg/dL) and C-reactive protein (0.43 mg/dL, normal range: ≤ 0.3 mg/dL) but normal readings for other factors, including serum tumor markers (carcinoembryonic antigen, carbohydrate antigen, and soluble IL-2 receptor), HbA1c, and IgG4 (66.1 mg/dL, normal: 4.5–117 mg/dL). Enhanced computed tomography (CT) demonstrated an ill-enhanced mass, 5 cm in size but with unclear margins, located at the pancreas head (Figure 1a,b). Upper gastrointestinal endoscopy revealed a submucosal tumor (SMT) with an apical erosion approximately 1.5 cm in size at the duodenal bulbs (Figure 2). Several faintly enlarged lymph nodes were seen around the pancreas head, but no nodules suggestive of metastasis were visible in the liver or the lungs. Endoscopic ultrasonography (EUS) demonstrated a heterogeneous, low-echoic mass at the pancreas head and body, but no adhesion to the common bile duct. EUS elastography revealed a hardness of the pancreas lesion (Figure 3). Forceps biopsy (Radial Jaw™4, Boston Scientific Japan, 2.2 mm, Tokyo, Japan) from the duodenal SMT was not informative, but EUS-guided fine needle aspiration biopsy (FNAB) showed abundant spindle myofibroblast tissues with eosinophilic and lymphoplasmacytic cell infiltration (Figure 4). FNAB was performed with two punctures from the duodenal bulbs, with each puncture performed with 10 strokes using a 22-gauge Franseen-tip needle (Acquire™, Boston Scientific Japan) with 10 mL of negative pressure. No malignant cells were seen. The spindle cells were positive for anti-smooth muscle antibody (ASMA) and desmin but negative for discovered on GIST-1 (DOG-1), c-Kit, CD34, S-100, and ALK. Only six IgG4-positive cells were recognized in high-powered views, and no obliterative phlebitis or storiform fibrosis was detected. These findings led to the diagnosis of IMT.
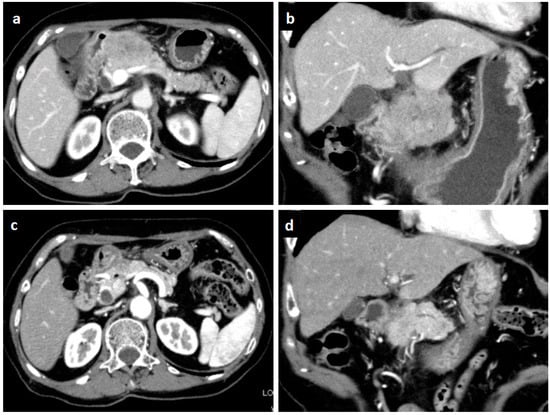
Figure 1.
Enhanced computed tomography. An irregular-margined, low-attenuated mass 5 cm in size was seen at the pancreas head (horizontal view (a), coronal view (b)). One month after the histological diagnosis, the pancreatic mass was markedly shrunken spontaneously (horizontal view (c), coronal view (d)).
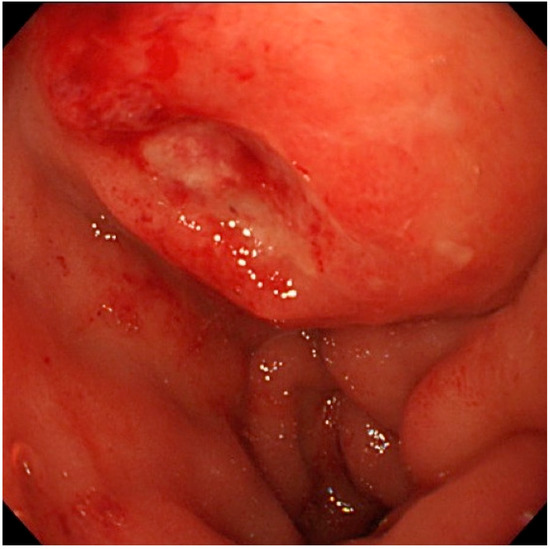
Figure 2.
Endoscopic view of the duodenal bulbs. A hemispheric submucosal tumor with apical erosion was recognized.
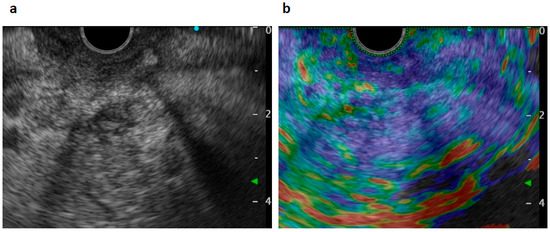
Figure 3.
Endoscopic ultrasonography (EUS) views. A heterogeneous low-echoic mass was seen by scanning from the duodenal bulbs (a). Elastography showed a heterogeneously hard mass lesion at the pancreas head (b).
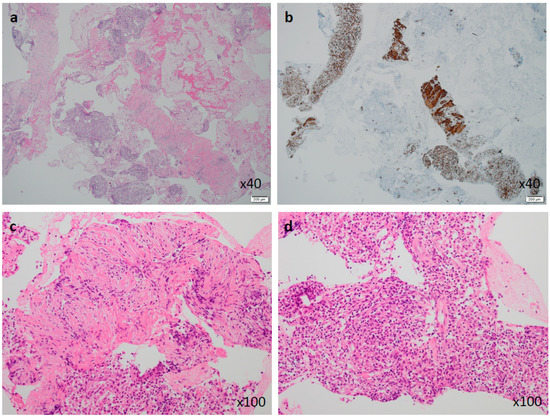
Figure 4.
Tissues obtained by EUS-guided fine needle aspiration biopsy (EUS-FNAB). Low-power view of hematoxylin-eosin (HE) staining showed mixed components of dense myofibroblastic tissues and aggregated inflammatory cells (×40). (a) Anti-smooth muscle actin was diffusely positive in the myofibroblastic components (×40). (b) High-power views showed a myofibroblastic cell component (c) and an inflammatory cell component (d) without malignant cells (HE, ×100).
Ten days after FNAB, positron emission tomography showed abnormal 18F-fluorodeoxyglucose uptake (SUVmax: 6.95); however, the pancreatic lesion seemed to have shrunk to 2.5 cm in size (Figure 5). Magnetic resonance imaging (MRI) demonstrated an obviously minimized tumorous lesion at the pancreas head (Figure 6). The mass lesion was visible as an iso-intensity signal in a T1-weighted image and as a faintly low-intensity signal in a T2-weighted image, while it was ill enhanced in an EOB image and the signal was heterogeneously repressed in a diffusion-weighted image. A subsequent CT, conducted one month after the FNAB, revealed further minimization of the pancreatic mass (Figure 1c,d). The images obtained in the next two months showed that the tumor had almost vanished. The tumor was no longer visible at the sixth month. During the post-diagnosis course, no medication was administered other than regularly taken hypotensive drugs. A written informed consent was obtained from the patient.
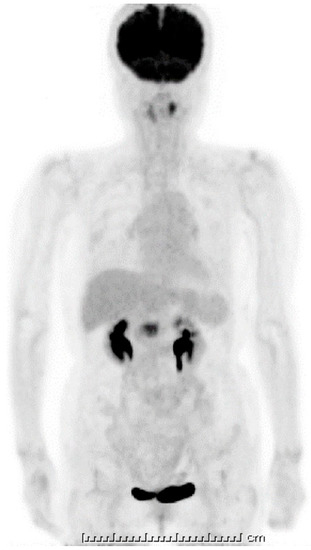
Figure 5.
18F-fluorodeoxyglucose positron emission tomography (FDG-PET). A strong uptake of FDG was visible at the pancreas head (SUVmax: 6.95); however, this looked smaller when compared with the initial computed tomography (CT) image. The one unit of under bar is indicating 1cm and total bar length is 25 cm.
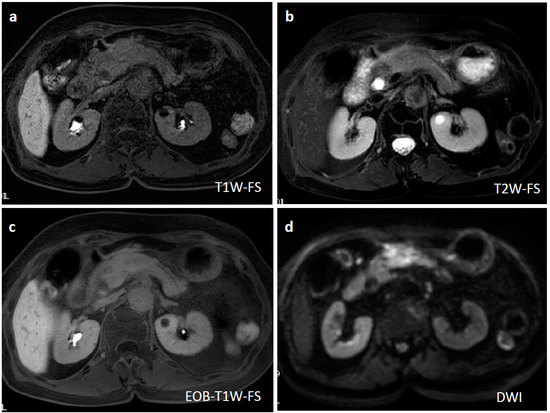
Figure 6.
Magnetic resonance imaging (MRI) at two weeks after EUS-FNAB and three weeks after the initial CT. A T1-weighted MRI showed an iso-intensity signal (a), a T2-weighted image showed a faint low-intensity signal (b), a gadoxetate sodium-injected MRI demonstrated a slightly weak enhancement (c), and a diffusion-weighted MRI revealed heterogeneously repressed diffusion ability at the pancreatic lesion (d).
3. Discussion
Our English literature survey on PubMed using the keywords “inflammatory myofibroblastic tumor” with “pancreas” or “pancreatic” listed 167 citations. By excluding other inflammatory pancreatic pseudotumors (such as other mass-forming pancreatitis and autoimmune pancreatitis) and histology-unproven cases, 27 cases of histologically confirmed IMTs (positive for histologically proven myofibroblastic tissue) were listed (Table 1). The classical term “inflammatory pseudotumor (IPT)” often includes other etiologies, such as IgG4-related, autoimmune-related, and infection-causing inflammatory lesions [39]; therefore, we only listed the histologically proven pancreatic IMTs and not the IPTs. Including the current case, the mean age at diagnosis of all cases was 40.0 years, and a subtle predominance of male gender was evident (17 males and 11 females). The pancreatic mass lesions were mostly located in the pancreas head (20 in the head, two in the body, four in the tail, and two in the body and tail) and had a mean size of 4.7 cm. Abdominal pain or discomfort was the most frequent symptom (56%, 15/27), with jaundice the second most frequent (44%), followed by anorexia or weight loss (26%), and nausea or vomiting (15%). One case had stable disease, one case had a recurrence in the lung, and one case died of sepsis, but the other 22 (88%) cases did not show recurrence after resection or remission (Table 1).

Table 1.
Reported cases of inflammatory myofibroblastic tumor (IMT) of the pancreas (English literature).
These data for pancreatic, IMTs differ greatly from the data of 730 IMT cases in 93 articles summarized by Nonaka et al. [1] who reported a younger onset (mean 29.6 years, range: 0–87 years), a nearly equal gender ratio, favored organs (commonest in lung, followed by the urinary bladder, mesentery, omentum, retroperitoneum, pelvis, gastrointestinal tract, and liver), larger size (mean 5.9 cm, range 0.4–36 cm), varied symptoms (strongly related to the location, but 19% were accompanied by systemic symptoms including fever, malaise, weight loss, and anemia), and different outcomes (local recurrence: 22%; metastasis: 3%; death from disease: 2%; and no recurrence: 67%). This trend became more apparent when comparing 59 cases of systemic IMTs with histological atypia [5], as these had younger onset (mean age: 13.2 years old, ≥20 years old: 29%), an even gender ratio (29 male and 30 female), large tumor size (mean: 7.8 cm), similar location (abdomen and pelvis: 64%, lung: 22%, head and neck: 8%, and extremity: 5%), and poorer outcomes (recurrence: 56%; metastasis: 10%; death from disease: 10%; and no recurrence: 42% in an average of 3.6 years of follow up). Thus, a wide range of variation exists in the nature of IMTs, and the adult pancreatic IMTs may have a relatively benign nature.
The biological marker of IMTs, including histological atypia, ganglion-like cells, TP53 expression, and aneuploidy pattern, have been correlated with more aggressive clinical behavior [40]. Coffin et al. also suggested that ALK (anaplastic lymphoma kinase) expression is another prognostic indicator of IMTs. The ALK (2p23) gene is activated by gene rearrangement in 50–70% of IMTs and ALK gene rearrangement is correlated with ALK expression, as determined by immunochemistry [41]. The absence of ALK expression in IMT was associated with a higher age of the patients [5]. All six of the observed metastases developed in 59 IMTs that were negative for ALK expression, and they developed before 20 years of age (mean age: 13.2 years), indicating a metastatic potential for ALK-negative IMTs in the younger subset [5]. The current case of a pancreatic IMT was in a patient of high age (82 years) and showed no histological atypia, ganglion-like cells, or ALK expression. Therefore, ALK expression as a clinical indicator in IMTs in older patients needs further evaluation.
IMTs show spontaneous regression in a minor fraction of patients, although the actual incidence is unclear due to surgical interventions and asymptomatic/undetected cases. To date, 13 cases of spontaneously regressed IMTs have been reported in various organs, but not in the pancreas (Table 2) [27,28,29,30,31,32,33,34,35,36,37,38]. As mentioned above, reported cases of pancreatic pseudotumors or those without proven myofibroblastic tissues were not listed [15,23]. Of the 13 cases, corticosteroids and/or NSAIDs were used in six cases and were effective in five cases. This phenomenon leads us to question the neoplastic nature of this tumor. IMTs often expand in size to invade multiple organs; therefore, when an accurate diagnosis can be made, conservative treatments should be recommended for older patients.
Table 2.
Reported cases of inflammatory fibroblastic tumor (IMT) with spontaneous and/or drug-used remission (English literature).
An accurate diagnosis of pancreatic IMTs cannot be made by image examinations alone, as most cases mimic malignancies (Table 1) and no IMT serum markers are commercially available. EUS-FNA demonstrates a fairly high diagnostic ability (nearly 95% sensitivity and specificity) for solid malignant pancreatic lesions [42,43]. The use of thick core biopsy needles [44] and high-negative-pressure aspiration methods [45] has increased the acquisition rate for obtaining core tissue samples. This, in turn, has enabled the determination of the probable nature of the whole pancreatic mass and even the classification of intermediate inflammatory and neoplastic conditions, such as IMTs. In the present case, we performed a conventional EUS-FNA but used a 22-gauge Franseen needle, and our pathologist was able to diagnose IMT (Figure 4). Other similar conditions, such as other inflammatory pseudotumors (IgG4-related [39,46], autoimmune-related [47], and infection-related [39] masses) and spindle cell tumors (malignant fibrous histiocytoma [47], sarcomatoid anaplastic large cell lymphoma, spindle cell carcinoma, inflammatory leiomyosarcoma, and pleomorphic liposarcoma) [5], must be carefully ruled out by multiple immunohistochemical tests.
In conclusion, we have reported a rare case of pancreatic IMT demonstrating spontaneous remission. Our aim was to emphasize the importance of accurate diagnosis that includes histology obtained by EUS-FNA. Further accumulation of cases is needed to clarify the biological behavior of pancreatic IMTs.
Author Contributions
H.M. drafted, and H.M., S.S. and K.U. clinically managed the course; K.S. made pathological diagnosis; K.T., H.I. and H.O. provided beneficial comments from the viewpoints of gastroenterologists and endoscopists; and H.O. supervised the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| IMT | inflammatory myofibroblastic tumor |
| NSAIDS | non-steroidal anti-inflammatory drugs |
| CT | computed tomography |
| SMT | submucosal tumor |
| EUS | endoscopic ultrasonography |
| FNAB | fine needle aspiration biopsy |
| ASMA | anti-smooth muscle antibody |
| MRI | magnetic resonance imaging |
| IPT | inflammatory pseudotumor |
| ALK | anaplastic lymphoma kinase |
References
- Nonaka, D.; Birbe, R.; Rosai, J. So-called inflammatory myofibroblastic tumour: A proliferative lesion of fibroblastic reticulum cells? Histopathology 2005, 46, 604–613. [Google Scholar] [CrossRef]
- Gleason, B.C.; Hornick, J.L. Inflammatory myofibroblastic tumours: Where are we now? J. Clin. Pathol. 2008, 61, 428–437. [Google Scholar] [CrossRef]
- Yamamoto, H.; Oda, Y.; Saito, T.; Sakamoto, A.; Miyajima, K.; Tamiya, S.; Tsuneyoshi, M. p53 Mutation and MDM2 amplification in inflammatory myofibroblastic tumours. Histopathology 2003, 42, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Yoshida, A.; Taguchi, K.; Kohashi, K.; Hatanaka, Y.; Yamashita, A.; Mori, D.; Oda, Y. ALK, ROS1 and NTRK3 gene rearrangements in inflammatory myofibroblastic tumours. Histopathology 2016, 69, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Coffin, C.M.; Hornick, J.L.; Fletcher, C.D. Inflammatory myofibroblastic tumor: Comparison of clinicopathologic, histologic, and immunohistochemical features including ALK expression in atypical and aggressive cases. Am. J. Surg. Pathol. 2007, 31, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Shankar, K.R.; Losty, P.D.; Khine, M.M.; Lamont, G.L.; McDowell, H.P. Pancreatic inflammatory tumour: A rare entity in childhood. J. R. Coll. Surg. Edinb. 1998, 43, 422–423. [Google Scholar] [PubMed]
- Walsh, S.V.; Evangelista, F.; Khettry, U. Inflammatory myofibroblastic tumor of the pancreaticobiliary region: Morphologic and immunocytochemical study of three cases. Am. J. Surg. Pathol. 1998, 22, 412–418. [Google Scholar] [CrossRef]
- McClain, M.B.; Burton, E.M.; Day, D.S. Pancreatic pseudotumor in an 11-year-old child: Imaging findings. Pediatr Radiol. 2000, 30, 610–613. [Google Scholar] [CrossRef]
- Wreesmann, V.; van Eijck, C.H.; Naus, D.C.; van Velthuysen, M.L.; Jeekel, J.; Mooi, W.J. Inflammatory pseudotumour (inflammatory myofibroblastic tumour) of the pancreas: A report of six cases associated with obliterative phlebitis. Histopathology 2001, 38, 105–110. [Google Scholar] [CrossRef]
- Yamamoto, H.; Watanabe, K.; Nagata, M.; Tasaki, K.; Honda, I.; Watanabe, S.; Soda, H.; Takenouti, T. Inflammatory myofibroblastic tumor (IMT) of the pancreas. J. Hepatobiliary Pancreat Surg. 2002, 9, 116–119. [Google Scholar] [CrossRef]
- Esposito, I.; Bergmann, F.; Penzel, R.; di Mola, F.F.; Shrikhande, S.; Buchler, M.W.; Friess, H.; Otto, H.F. Oligoclonal T-cell populations in an inflammatory pseudotumor of the pancreas possibly related to autoimmune pancreatitis: An immunohistochemical and molecular analysis. Virchows Arch. 2004, 444, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Pungpapong, S.; Geiger, X.J.; Raimondo, M. Inflammatory myofibroblastic tumor presenting as a pancreatic mass: A case report and review of the literature. JOP 2004, 5, 360–367. [Google Scholar] [PubMed]
- Dulundu, E.; Sugawara, Y.; Makuuchi, M. Inflammatory myofibroblastic tumor of the pancreas--a case report. Biosci. Trends 2007, 1, 167–169. [Google Scholar] [PubMed]
- Sim, A.; Lee, M.W.; Nguyen, G.K. Inflammatory myofibroblastic tumour of the pancreas. Can. J. Surg. 2008, 51, E23–E24. [Google Scholar] [PubMed]
- Dagash, H.; Koh, C.; Cohen, M.; Sprigg, A.; Walker, J. Inflammatory myofibroblastic tumor of the pancreas: A case report of 2 pediatric cases—steroids or surgery? J. Pediatr Surg. 2009, 44, 1839–1841. [Google Scholar] [CrossRef] [PubMed]
- Hassan, K.S.; Cohen, H.I.; Hassan, F.K.; Hassan, S.K. Unusual case of pancreatic inflammatory myofibroblastic tumor associated with spontaneous splenic rupture. World J. Emerg. Surg. 2010, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Schutte, K.; Kandulski, A.; Kuester, D.; Meyer, F.; Wieners, G.; Schulz, H.U.; Malfertheiner, P. Inflammatory Myofibroblastic Tumor of the Pancreatic Head: An Unusual Cause of Recurrent Acute Pancreatitis - Case Presentation of a Palliative Approach after Failed Resection and Review of the Literature. Case Rep. Gastroenterol. 2010, 4, 443–451. [Google Scholar] [CrossRef]
- Tomazic, A.; Gvardijancic, D.; Maucec, J.; Homan, M. Inflammatory myofibroblastic tumor of the pancreatic head—A case report of a 6 months old child and review of the literature. Radiol. Oncol. 2015, 49, 265–270. [Google Scholar] [CrossRef]
- Panda, D.; Mukhopadhyay, D.; Datta, C.; Chattopadhyay, B.K.; Chatterjee, U.; Shinde, R. Inflammatory Myofibroblastic Tumor Arising in the Pancreatic Head: A Rare Case Report. Indian J. Surg. 2015, 77, 538–540. [Google Scholar] [CrossRef]
- Zanchi, C.; Giurici, N.; Martelossi, S.; Cheli, M.; Sonzogni, A.; Alberti, D. Myofibroblastic Tumor of the Pancreatic Head: Recurrent Cholangitis. J. Pediatr Gastroenterol. Nutr. 2015, 61, e28–e29. [Google Scholar] [CrossRef]
- Battal, M.; Kartal, K.; Tuncel, D.; Bostanci, O. Inflammatory myofibroblastic pancreas tumor: A case report. Clin. Case Rep. 2016, 4, 1122–1124. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Bu, X.; Tian, F. Inflammatory myofibroblastic tumor in the head of the pancreas with anorexia and vomiting in a 69-year-old man: A case report. Oncol. Lett. 2016, 12, 1546–1550. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.K.; Lin, Y.C.; Yeh, M.L.; Chen, Y.S.; Su, Y.T.; Tsai, C.C. Inflammatory myofibroblastic tumors of the pancreas in children: A case report and literature review. Medicine (Baltimore) 2017, 96, e5870. [Google Scholar] [CrossRef] [PubMed]
- Berhe, S.; Goldstein, S.; Thompson, E.; Hackam, D.; Rhee, D.S.; Nasr, I.W. Challenges in Diagnosis and Management of Pancreatic Inflammatory Myofibroblastic Tumors in Children. Pancreas 2019, 48, e27–e29. [Google Scholar] [CrossRef] [PubMed]
- Lacoste, L.; Galant, C.; Gigot, J.F.; Lacoste, B.; Annet, L. Inflammatory myofibroblastic tumor of the pancreatic head. JBR-BRR 2012, 95, 267–269. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kroft, S.H.; Stryker, S.J.; Winter, J.N.; Ergun, G.; Rao, M.S. Inflammatory pseudotumor of the pancreas. Int. J. Pancreatol 1995, 18, 277–283. [Google Scholar] [PubMed]
- Przkora, R.; Bolder, U.; Schwarz, S.; Jauch, K.W.; Spes, J.; Andreesen, R.; Mackensen, A. Regression of nonresectable inflammatory myofibroblastic tumours after treatment with nonsteroidal anti-inflammatory drugs. Eur. J. Clin. Investig. 2004, 34, 320–321. [Google Scholar] [CrossRef] [PubMed]
- Shatzel, J.; Wooten, K.; Ankola, A.; Cheney, R.T.; Morrison, C.D.; Skitzki, J.J. Inflammatory myofibroblastic tumor of the mesentery: A clinical dilemma. Int. J. Clin. Oncol. 2012, 17, 380–384. [Google Scholar] [CrossRef]
- Galindo, J.; Lassaletta, L.; Garcia, E.; Gavilan, J.; Allona, M.; Royo, A.; Patron, M. Spontaneous hearing improvement in a patient with an inflammatory myofibroblastic tumor of the temporal bone. Skull Base 2008, 18, 411–415. [Google Scholar] [CrossRef][Green Version]
- Mattei, P.; Barnaby, K. Rapid regression of duodenal inflammatory myofibroblastic tumor after intravenous ketorolac: Case report and review of the literature. J. Pediatr. Surg. 2008, 43, 1196–1199. [Google Scholar] [CrossRef]
- Sugiyama, K.; Nakajima, Y. Inflammatory myofibroblastic tumor in the mediastinum mimicking a malignant tumor. Diagn. Interv. Radiol. 2008, 14, 197–199. [Google Scholar] [PubMed]
- Bilaceroglu, S.; Gursoy, S.; Yucel, N.; Ozbilek, E. Inflammatory myofibroblastic tumor presenting as a large mass and a spontaneously resolving nodule in the lung. J. Bronchol. Interv. Pulmonol. 2009, 16, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Fragoso, A.C.; Eloy, C.; Estevao-Costa, J.; Campos, M.; Farinha, N.; Lopes, J.M. Abdominal inflammatory myofibroblastic tumor a clinicopathologic study with reappraisal of biologic behavior. J. Pediatr. Surg. 2011, 46, 2076–2082. [Google Scholar] [CrossRef] [PubMed]
- Calaway, A.C.; Gondim, D.; Idrees, M.; Boris, R.S. Spontaneous resolution of inflammatory myofibroblastic tumor of the kidney. Can. J. Urol. 2014, 21, 7582–7585. [Google Scholar] [PubMed]
- Zhao, J.J.; Ling, J.Q.; Fang, Y.; Gao, X.D.; Shu, P.; Shen, K.T.; Qin, J.; Sun, Y.H.; Qin, X.Y. Intra-abdominal inflammatory myofibroblastic tumor: Spontaneous regression. World J. Gastroenterol. 2014, 20, 13625–13631. [Google Scholar] [CrossRef] [PubMed]
- Markovic Vasiljkovic, B.; Plesinac Karapandzic, V.; Pejcic, T.; Djuric Stefanovic, A.; Milosevic, Z.; Plesinac, S. Follow-Up Imaging of Inflammatory Myofibroblastic Tumor of the Uterus and Its Spontaneous Regression. Iran. J. Radiol. 2016, 13, e12991. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, K.; Sasaki, M.; Kojima, M.; Tsuruzono, K.; Matsumoto, K.; Wakayama, A.; Yoshimine, T. Spontaneous Regression of Inflammatory Pseudotumor in the Cauda Equina: A Case Report. Nmc Case Rep. J. 2016, 3, 111–114. [Google Scholar] [CrossRef]
- Habib, L.; Son, J.H.; Petris, C.; Kazim, M. Spontaneous regression of inflammatory myofibroblastic tumor of the orbit: A case report and review of literature. Orbit 2017, 36, 178–182. [Google Scholar] [CrossRef]
- Goldsmith, P.J.; Loganathan, A.; Jacob, M.; Ahmad, N.; Toogood, G.J.; Lodge, J.P.; Prasad, K.R. Inflammatory pseudotumours of the liver: A spectrum of presentation and management options. Eur. J. Surg. Oncol. 2009, 35, 1295–1298. [Google Scholar] [CrossRef]
- Hussong, J.W.; Brown, M.; Perkins, S.L.; Dehner, L.P.; Coffin, C.M. Comparison of DNA ploidy, histologic, and immunohistochemical findings with clinical outcome in inflammatory myofibroblastic tumors. Mod. Pathol. 1999, 12, 279–286. [Google Scholar]
- Coffin, C.M.; Patel, A.; Perkins, S.; Elenitoba-Johnson, K.S.; Perlman, E.; Griffin, C.A. ALK1 and p80 expression and chromosomal rearrangements involving 2p23 in inflammatory myofibroblastic tumor. Mod. Pathol. 2001, 14, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Matsubayashi, H.; Matsui, T.; Yabuuchi, Y.; Imai, K.; Tanaka, M.; Kakushima, N.; Sasaki, K.; Ono, H. Endoscopic ultrasonography guided-fine needle aspiration for the diagnosis of solid pancreaticobiliary lesions: Clinical aspects to improve the diagnosis. World J. Gastroenterol. 2016, 22, 628–640. [Google Scholar] [CrossRef] [PubMed]
- Ishiwatari, H.; Sato, J.; Fujie, S.; Sasaki, K.; Kaneko, J.; Satoh, T.; Matsubayashi, H.; Kishida, Y.; Yoshida, M.; Ito, S.; et al. Gross visual inspection by endosonographers during endoscopic ultrasound-guided fine needle aspiration. Pancreatology 2019, 19, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Fujie, S.; Ishiwatari, H.; Sasaki, K.; Sato, J.; Matsubayashi, H.; Yoshida, M.; Ito, S.; Kawata, N.; Imai, K.; Kakushima, N.; et al. Comparison of the Diagnostic Yield of the Standard 22-Gauge Needle and the New 20-Gauge Forward-Bevel Core Biopsy Needle for Endoscopic Ultrasound-Guided Tissue Acquisition from Pancreatic Lesions. Gut Liver 2019, 13, 349–355. [Google Scholar] [CrossRef]
- Sato, J.; Ishiwatari, H.; Sasaki, K.; Fujie, S.; Kaneko, J.; Satoh, T.; Matsubayashi, H.; Kishida, Y.; Yoshida, M.; Ito, S.; et al. Benefit of high negative pressure during endoscopic ultrasound-guided fine-needle aspiration with standard 22-gauge needles for pancreatic lesions: A retrospective comparative study. Scand. J. Gastroenterol. 2019, 54, 108–113. [Google Scholar] [CrossRef]
- Yamamoto, H.; Yamaguchi, H.; Aishima, S.; Oda, Y.; Kohashi, K.; Oshiro, Y.; Tsuneyoshi, M. Inflammatory myofibroblastic tumor versus IgG4-related sclerosing disease and inflammatory pseudotumor: A comparative clinicopathologic study. Am. J. Surg. Pathol. 2009, 33, 1330–1340. [Google Scholar] [CrossRef]
- Mizukami, H.; Yajima, N.; Wada, R.; Matsumoto, K.; Kojima, M.; Kloppel, G.; Yagihashi, S. Pancreatic malignant fibrous histiocytoma, inflammatory myofibroblastic tumor, and inflammatory pseudotumor related to autoimmune pancreatitis: Characterization and differential diagnosis. Virchows Arch. 2006, 448, 552–560. [Google Scholar] [CrossRef]






© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).