Abstract
Here, we describe a case of an asymptomatic 73-year-old female patient who suffered from type A acute aortic dissection with epiaortic arteries involvement and underwent surgical operation 9 years ago. A follow-up color Doppler ultrasound revealed a right vertebral artery intermittent flow reversal due to innominate artery dissection. To our knowledge, no previous studies have reported this intermittent flow reversal; therefore, supra-aortic trunks should be considered among the possible causes of vertebral artery flow reversal.
Keywords:
vertebral artery; flow reversal; intermittent; sporadic; irregular; dissection; flap; innominate artery 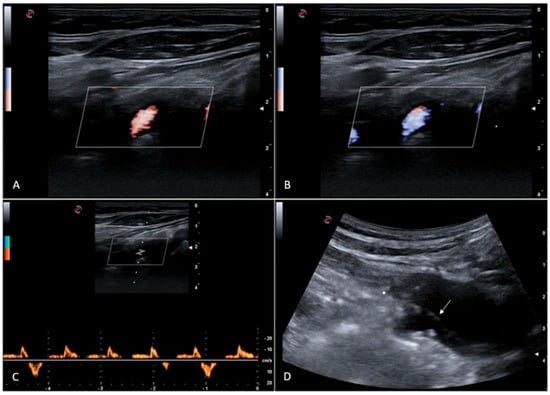
Figure 1.
Color Doppler ultrasound shows antegrade (A) and retrograde (B) right vertebral artery flow; Doppler spectral waveform shows intermittent and irregular right vertebral artery flow reversal (C). Innominate artery dissection can be demonstrated ((D), Figure S1), with a dissection flap just near the right subclavian artery origin. It can be supposed that dissection flap irregular movements can cause a sporadic reduction of end-systolic subclavian artery pressure, which could be at the base of the random right vertebral artery flow reversal occurrence. The 73-year-old female patient was asymptomatic at the time of the ultrasound examination; she suffered from spontaneous type A acute aortic dissection with epiaortic arteries involvement and underwent surgical operation 9 years ago. Type A aortic dissection is a life-threatening surgical emergency with a suggested incidence of about 5 per 100,000 person-years, sometimes associated with supra-aortic trunk involvement [1,2,3,4]. Long-term outcomes of this disease are improving over time, and it is known that sometimes false channels remain patent after surgery [5,6]. A previous study reported an aortic dissection extending to the innominate and right common carotid arteries which showed blood passing from the false lumen of the distal right common carotid artery into the true lumen with antegrade flow in the false lumen but reverse flow in the true channel, the latter supplying the subclavian artery [7]. To our knowledge, no previous studies have reported this intermittent flow reversal; therefore, supra-aortic trunks dissection should be considered among the possible causes of vertebral artery flow reversal.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/diagnostics15131668/s1, Figure S1: Computed tomography angiography image of type A acute aortic dissection with innominate artery involvement.
Author Contributions
Conceptualization, C.T. and A.Q.; methodology, C.T., A.Q., M.F., S.L., A.A.M., D.B., G.C., G.L., A.R., F.P., G.A., A.C., I.C., E.D.C. and N.S.; data curation, C.T., A.Q., M.F., S.L., A.A.M., D.B., G.C., G.L., A.R., F.P., G.A. and A.C.; writing—original draft preparation, C.T., A.Q., M.F., S.L., A.A.M., D.B., G.C., G.L., A.R., F.P., G.A., A.C., I.C., E.D.C. and N.S.; writing—review and editing, C.T., A.Q., M.F., S.L., A.A.M., D.B., G.C., G.L., A.R., F.P., G.A., A.C., I.C., E.D.C. and N.S.; supervision, G.A., A.C., I.C., E.D.C. and N.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Munir, W.; Chong, J.H.; Harky, A.; Bashir, M.; Adams, B. Type A aortic dissection: Involvement of carotid artery and impact on cerebral malperfusion. Asian Cardiovasc. Thorac. Ann. 2021, 29, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Corvino, A.; Lonardo, V.; Tafuri, D.; Cocco, G.; Pizzi, A.D.; Boccatonda, A.; Corvino, F.; Costantino, T.G.; Horer, T.; Catalano, O. Aortic dissection: How to identify it during an abdominal ultrasound examination and achieve a potentially lifesaving diagnosis. J. Clin. Ultrasound 2024, 52, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Arslan, Ü.; Jalalzai, I. A Narrative Review of Biomarkers and Imaging in the Diagnosis of Acute Aortic Syndrome. Diagnostics 2025, 15, 183. [Google Scholar] [CrossRef] [PubMed]
- di Gioia, C.R.T.; Ascione, A.; Carletti, R.; Giordano, C. Thoracic Aorta: Anatomy and Pathology. Diagnostics 2023, 13, 2166. [Google Scholar] [CrossRef] [PubMed]
- Bacour, N.; Grewal, S.; Theijsse, R.T.; Klautz, R.J.M.; Grewal, N. From Survival to Recovery: Understanding the Life Impact of an Acute Aortic Dissection Through Activity, Sleep, and Quality of Life. J. Clin. Med. 2025, 14, 859. [Google Scholar] [CrossRef] [PubMed]
- Bing, F.; Rodière, M.; Martinelli, T.; Monnin-Bares, V.; Chavanon, O.; Bach, V.; Baguet, J.P.; Ferretti, G.R.; Thony, F. Type A acute aortic dissection: Why does the false channel remain patent after surgery? Vasc. Endovascular. Surg. 2014, 48, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, P.; Giannesini, C.; Amah, G.; Kevorkian, J.P.; Woimant, F.; Levy, B.I. Doppler sonograpy with dynamic testing in a case of aortic dissection extending to the innominate and right common carotid arteries. Neuroradiology 2003, 45, 472–475. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).