
Exploring Atypical Origins of Trismus: Surgical Solutions for Rare Pathologies—Insights from Rare Clinical Cases


 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
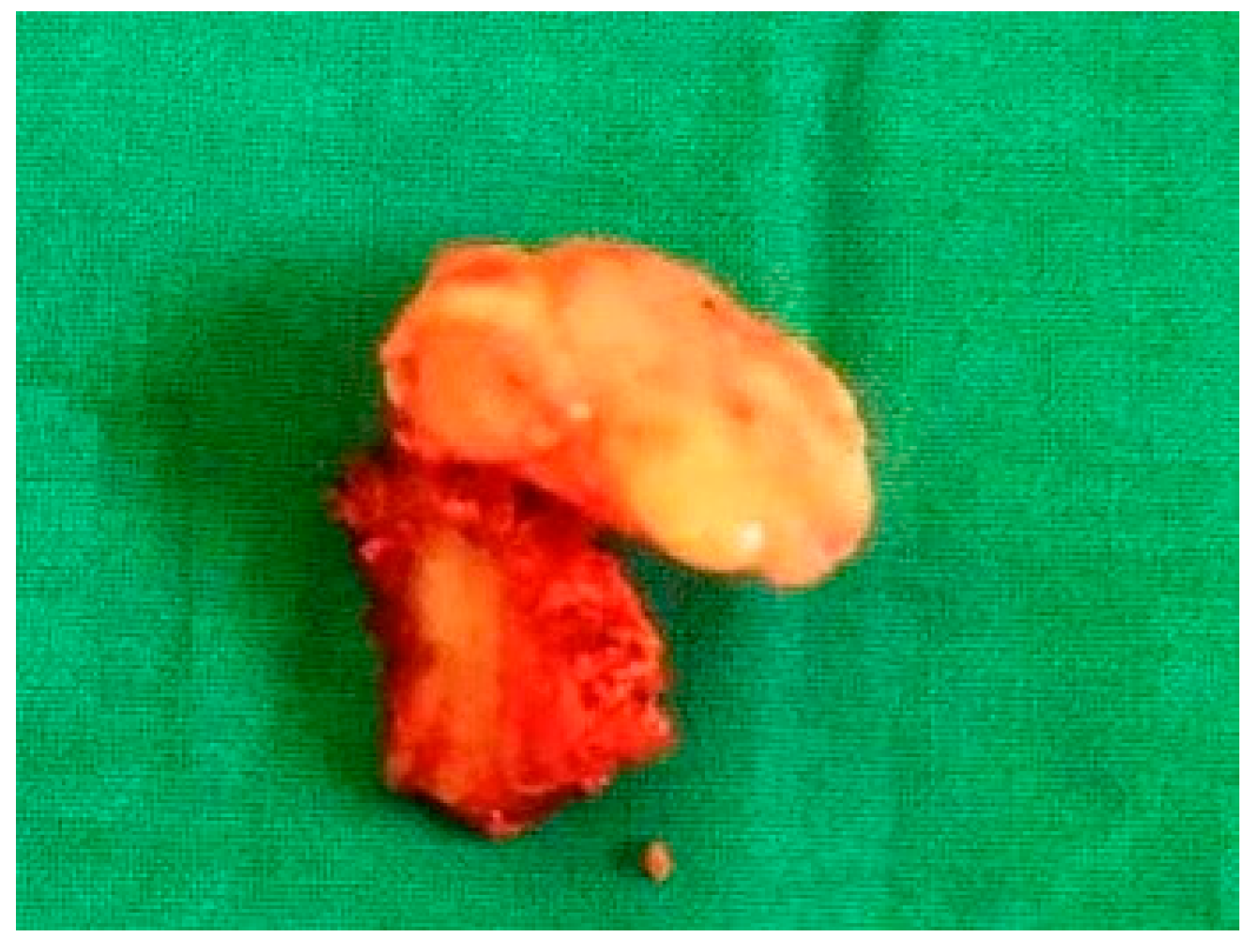
- Case 1
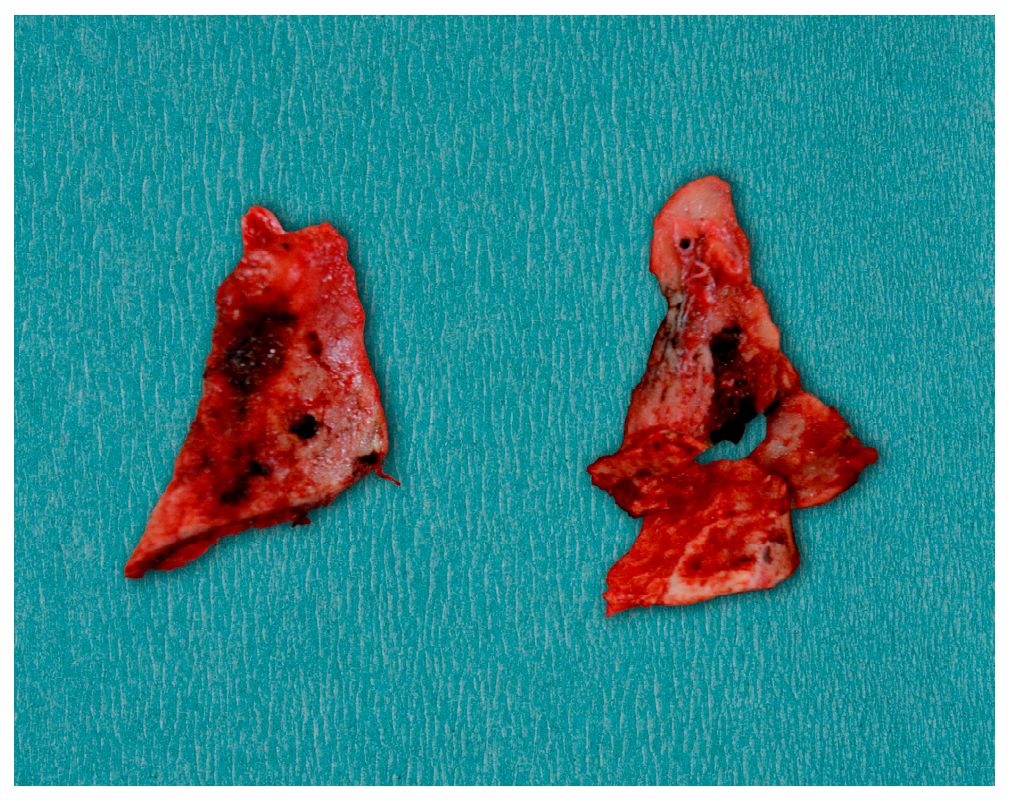
- Case 2
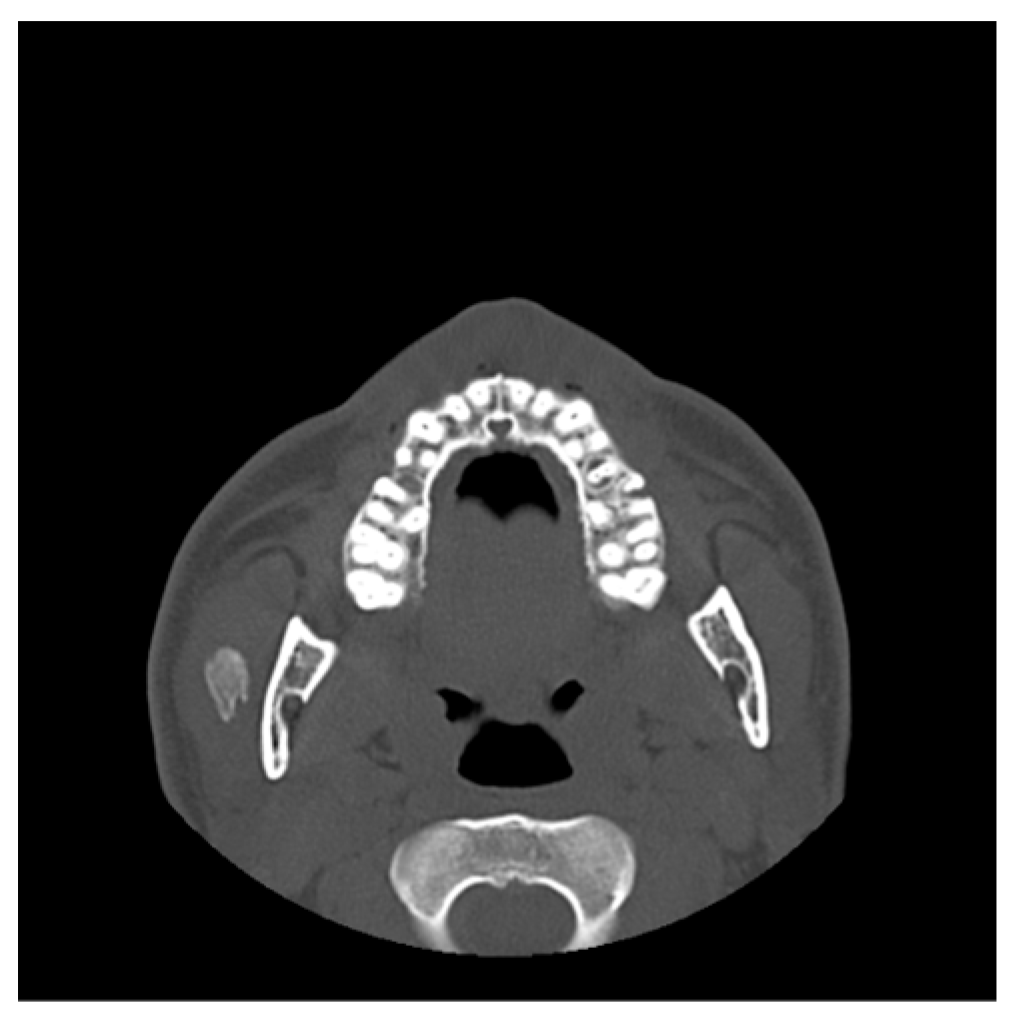
- Case 3
- Case 4
- Case 5
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CT | Computed tomography |
| MRI | Magnetic Resonance Imaging |
| OPG | Orthopantomogramm |
| TMJ | Temporomandibular joint |
| MIO | Maximum interincisal opening |
| CIS | Coronoid impingement syndrome |
| MOT | Myositis ossificans traumatica |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| SAG | Streptococcus anginosus group |
| ENT | Otorhinolaryngology (ear, nose, throat) |
References
- Poornima, G.; Poornima, C. Trismus. J. Health Sci. Res. 2014, 5, 15–20. [Google Scholar] [CrossRef]
- Dhanrajani, P.J.; Jonaidel, O. Trismus: Aetiology, Differential Diagnosis and Treatment. Diagnosis and Treatment. Dent. Update 2002, 29, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Rapidis, A.D.; Dijkstra, P.U.; Roodenburg, J.L.N.; Rodrigo, J.P.; Rinaldo, A.; Strojan, P.; Ferlito, A. Trismus in patients with head and neck cancer: Etiopathogenesis, diagnosis and management. Clin. Otolaryngol. 2015, 40, 516–526. [Google Scholar] [CrossRef]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef]
- Zieliński, G.; Pająk-Zielińska, B.; Ginszt, M. A Meta-Analysis of the Global Prevalence of Temporomandibular Disorders. J. Clin. Med. 2024, 13, 1365. [Google Scholar] [CrossRef]
- Mezitis, M.; Rallis, G.; Zacharides, N. The normal range of mouth opening. J. Oral Maxillofac. Surg. 1984, 47, 1028–1029. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.; Johansson, M.; Rydén, A.; Houltz, E.; Finizia, C. Impact of trismus on health-related quality of life and mental health. Head Neck 2015, 37, 1672–1679. [Google Scholar] [CrossRef]
- Luyk, N.H.; Steinberg, B. Aetiology and diagnosis of clinically evident jaw trismus. Aust. Dent. J. 1990, 35, 523–529. [Google Scholar] [CrossRef]
- Amin, B.; Chandra, S.B. Recognizing trismus symptoms, prevention, and treatment. Med. Sci. 2019, 8, 766–769. [Google Scholar] [CrossRef]
- Tveterås, K.; Kristense, S. The aetiology and pathogenesis of trismus. Clin. Otolaryngol. Allied Sci. 1986, 11, 383–387. [Google Scholar] [CrossRef]
- Siddiqui, L.; Khan, H.F.; Kanwal, S.S.; Mustafa, K.M. Evaluating the Impact of temporo-mandibular joint disorders on oral health related quality of life; A literature review. Int. Ann. Health Sci. 2024, 3, 4–11. [Google Scholar] [CrossRef]
- Małgorzata, P.; Małgorzata, K.M.; Karolina, C.; Gala, A. Diagnostic of Temporomandibular Disorders and Other Facial Pain Conditions-Narrative Review and Personal Experience. Medicina 2020, 56, 472. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.; Detamore, M.S.; Mercuri, L.G. Degenerative disorders of the temporomandibular joint: Etiology, diagnosis, and treatment. J. Dent. Res. 2008, 87, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Hilaire, H.; Weber, W.; Ramer, M.; Lumerman, H. Clinicopathologic conference: Trismus following dental treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 98, 261–266. [Google Scholar] [CrossRef]
- Skinner, A.M.; Rees, M.J. Congenital trismus secondary to masseteric fibrous bands: A 7-year follow-up report as an approach to management. J. Craniofac. Surg. 2004, 15, 709–713. [Google Scholar] [CrossRef]
- Hong, C.J.; Caulley, L.; Kohlert, S.; Graham, G.E.; McMillan, H.J.; Michaud, J.; Vaccani, J.P. Congenital Trismus From Brainstem Dysgenesis: Case Report and Review of Literature. Pediatrics 2016, 138, e20154605. [Google Scholar] [CrossRef]
- Campanella, G.; Artuso, G.; Murgia, M.S.; Orrù, G.; Casu, C. Severe Post-Traumatic Trismus Unresponsive to Drug Therapy in a 12-Year-Old Patient Treated with a Capacitive-Resistive Electrical Transfer Therapy: A Case Report. Oral 2022, 2, 173–181. [Google Scholar] [CrossRef]
- Managutti, A.; Patel, N.; Menat, S.; Kamala, R.; Patel, H. Post-traumatic-Zygomaticocoronoid Ankylosis: A Rare Clinical Case Report. IJSS Case Rep. Rev. 2015, 1, 4–6. [Google Scholar]
- Obradovic, B. Intraoral management of odontogenic infection associated with severe trismus under local anesthesia. Ann. Ital. Chir. 2021, 92, 116–118. [Google Scholar]
- Kim, H.-Y.; Chung, J.-W. Infectious Myositis of the Jaw Presenting as Trismus of Unknown Origin. J. Oral Med. Pain 2020, 45, 115–119. [Google Scholar] [CrossRef]
- Satheeshkumar, P.S.; Mohan, M.P.; Jacob, J. Restricted mouth opening and trismus in oral oncology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Anand, A.; Mathew, A.; Balasubramanian, D. Trismus in Head and Neck Cancer: Causes and Management. In Dysphagia Management in Head and Neck Cancers; Thankappan, K., Iyer, S., Menon, J., Eds.; Springer: Singapore, 2018; pp. 161–172. [Google Scholar] [CrossRef]
- Bouman, M.A.; Dijkstra, P.U.; Reintsema, H.; Roodenburg, J.L.; Werker, P.M. Surgery for extra-articular trismus: A systematic review. Br. J. Oral Maxillofac. Surg. 2016, 54, 253–259. [Google Scholar] [CrossRef]
- Shen, Y.W.; Shih, Y.H.; Fuh, L.J.; Shieh, T.M. Oral Submucous Fibrosis: A Review on Biomarkers, Pathogenic Mechanisms, and Treatments. Int. J. Mol. Sci. 2020, 21, 7231. [Google Scholar] [CrossRef]
- Chen, Y.-K.; Lin, L.-M.; Lin, C.-C. Osteoma of the mandibular coronoid process. Int. J. Oral Maxillofac. Surg. 1998, 27, 222–223. [Google Scholar] [CrossRef] [PubMed]
- Saikrishna, D.; Das, A.; Jha, C. Management of a case of osteoma of coronoid: A rare case report. Natl. J. Maxillofac. Surg. 2021, 12, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Lewars, L.J. Osteomas of the coronoid process. Oral Surg. Oral Med. Oral Pathol. 1959, 12, 490–496. [Google Scholar]
- Petronis, Z.; Janovskiene, A.; Leketas, M. Cancellous osteoma of the coronoid process: A literature review and rare case report. J. Oral Facial Pain Headache 2024, 38, 126–130. [Google Scholar] [CrossRef]
- Vashishth, S.; Garg, K.; Patil, P.; Sreenivasan, V. An unusual cause for trismus caused by mandibular coronoid osteoma: A case report. Imaging Sci. Dent. 2013, 43, 45–48. [Google Scholar] [CrossRef]
- Nah, K.S. Osteomas of the craniofacial region. Imaging Sci. Dent. 2011, 41, 107–113. [Google Scholar] [CrossRef]
- Jundt, G.; Bertoni, F.; Unni, K.K.; Saito, K.; Dehne, L.P. Benign tumours of bone and cartilage. In WHO Classification of Tumors: Pathology and Genetics of Head and Neck Tumours; Barnes, L., Eveson, J.W., Reichart, P., Sidransky, D., Eds.; IARC: Lyon, France, 2005; pp. 54–55. [Google Scholar]
- Wesley, R.K.; Cullen, C.L.; Bloom, W.S. Gardner’s syndrome with bilateral osteomas of coronoid process resulting in limited opening. Pediatr. Dentl. 1987, 9, 53–57. [Google Scholar]
- Woldenberg, Y.; Nash, M.; Bodner, L. Peripheral osteoma of the maxillofacial region. Diagnosis and management: A study of 14 cases. Med. Oral Patol. Oral Cir. Bucal. 2005, 10 (Suppl. S2), E139–E142. [Google Scholar] [PubMed]
- Dandriyal, R.; Giri, K.Y.; Pant, S.; Alam, S.; Joshi, A. Giant osteochondroma of the coronoid process. J. Maxillofac. Oral Surg. 2015, 14 (Suppl. S1), 412–416. [Google Scholar] [CrossRef] [PubMed]
- Lan, T.; Liu, X.; Liang, P.S.; Tao, Q. Osteochondroma of the coronoid process: A case report and review of the literature. Oncol. Lett. 2019, 18, 2270–2277. [Google Scholar] [CrossRef]
- Ghazizadeh, M.; Sheikhi, M.; Salehi, M.; Khaleghi, A. Bilateral coronoid hyperplasia causing painless limitation of mandibular movement. Radiol Case Rep. 2017, 13, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.; Chung, J.W. Coronoid Process Hyperplasia: A Rare Case of Restricted Mouth Opening Masquerading as Temporomandibular Disorder. J. Oral Med. Pain 2023, 48, 112–117. [Google Scholar] [CrossRef]
- Tavassol, F.; Spalthoff, S.; Essig, H.; Bredt, M.; Gellrich, N.C.; Kokemüller, H. Elongated coronoid process: CT-based quantitative analysis of the coronoid process and review of literature. Int. J. Oral Maxillofac. Surg. 2012, 41, 331–338. [Google Scholar] [CrossRef]
- Goh, Y.C.; Tan, C.C.; Lim, D. Coronoid hyperplasia: A review. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.; Lucchina, A.G.; Mortellaro, C.; Fama, A.; Galbiati, G.; Farronato, G.; Maspero, C. Bilateral Hyperplasia of the Coronoid Process in Pediatric Patients: What is the Gold Standard for Treatment? J. Craniofac. Surg. 2019, 30, 1058–1063. [Google Scholar] [CrossRef]
- Puche, M.; Guijarro-Martínez, R.; Pérez-Herrezuelo, G.; Miragall, L.; Iglesias, M.E.; Martínez-Costa, C. The hypothetical role of congenital hypotonia in the development of early coronoid hyperplasia. J. Craniomaxillofac. Surg. 2012, 40, e155–e158. [Google Scholar] [CrossRef]
- Khandavilli, S.D.; Pattni, N.; Naredla, P.R.; Williams, R. First case of bilateral coronoid hyperplasia in monozygotic twin sisters-a new aetiological perspective? Oral Maxillofac. Surg. 2016, 20, 441–443. [Google Scholar] [CrossRef]
- Parmentier, G.I.; Nys, M.; Verstraete, L.; Politis, C. A systematic review of treatment and outcomes in patients with mandibular coronoid process hyperplasia. J. Korean Assoc. Oral Maxillofac. Surg. 2022, 48, 133–148. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, E.F.C.; Maranhão, C.M.C.T.; Almeida, R.A.C.; Torres, B.C.A. Treatment of hyperplasia of the coronoid process of the mandible in adults: Analysis of 42 literature reports and illustrative case. RGO Rev. Gaúch Odontol. 2021, 69, e20210033. [Google Scholar] [CrossRef]
- Ozkaya, O.; Colak, O.; Sutcu, M.; Akan, M. The outcome of coronoidectomy in bilateral coronoid process hyperplasia. Cranio 2018, 36, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Fernández Ferro, M.; Fernández Sanromán, J.; Sandoval Gutierrez, J.; Costas López, A.; López de Sánchez, A.; Etayo Pérez, A. Treatment of bilateral hyperplasia of the coronoid process of the mandible. Presentation of a case and review of the literature. Med. Oral Patol. Oral Cir. Bucal. 2008, 13, E595–E598. [Google Scholar]
- Hanisch, M.; Hanisch, L.; Fröhlich, L.F.; Werkmeister, R.; Bohner, L.; Kleinheinz, J. Myositis ossificans traumatica of the masticatory muscles: Etiology, diagnosis and treatment. Head Face Med. 2018, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Palla, B.; Han, M.D.; Callahan, N. Myositis Ossificans Traumatica of the Head and Neck in a Child. J. Dent. Child. 2020, 87, 120–123. [Google Scholar]
- Anshika, R.; Hoogar, M.B.; Shilpi, S. Myositis ossificans of masseter muscle: A rare case. Int. J. Health Sci. Res. 2021, 11, 105–108. Available online: https://www.ijhsr.org/IJHSR_Vol.11_Issue.2_Feb2021/IJHSR015.pdf (accessed on 2 February 2021).
- Jović, S.; Brajković, D.; Borilović, M.; Marjanović, U.; Brkić, M.; Kozomara, R.; Stošić, S. Recurring myositis ossificans traumatica of temporal muscle: A case report. Vojnosanit. Pregl. 2021, 78, 255–260. [Google Scholar] [CrossRef]
- Spinzia, A.; Moscato, G.; Broccardo, E.; Castelletti, L.; Maglitto, F.; Orabona, G.D.; Piombino, P. A rare isolated unilateral myositis ossificans traumatica of the lateral pterygoid muscle: A case report. J. Med. Case Rep. 2014, 8, 230. [Google Scholar] [CrossRef]
- Torres, A.M.; Nardis, A.C.; da Silva, R.A.; Savioli, C. Myositis ossificans traumatica of the medial pterygoid muscle following a third molar extraction. Int. J. Oral Maxillofac. Surg. 2015, 44, 488–490. [Google Scholar] [CrossRef]
- Abbasi, A.J.; Taheri, M.M.; Asadi, A.; Bahrami, R.; Nikparto, N. Myositis ossificans traumatica of masticatory muscles: A case report and review of the literature. Oral Maxillofac. Surg. Cases 2024, 10, 100361. [Google Scholar] [CrossRef]
- Fité-Trepat, L.; Martos-Fernández, M.; Alberola-Ferranti, M.; Romanini-Montecino, C.; Saez-Barba, M.; Bescós-Atín, C. Myositis ossificans of the masseter muscle: A rare location. Report of a case and review of literature. J. Clin. Exp. Dent. 2016, 8, e210–e213. [Google Scholar] [CrossRef]
- Baur, D.A.; Altay, M.A.; Flores-Hidalgo, A.; Ort, Y.; Quereshy, F.A. Chronic osteomyelitis of the mandible: Diagnosis and management--an institution’s experience over 7 years. J. Oral Maxillofac. Surg. 2015, 73, 655–665. [Google Scholar] [CrossRef]
- Chun, J.Y.; Shim, Y.J. Osteomyelitis of the Mandibular Coronoid Process Mimicking a Temporomandibular Joint Disorder: A Case Report. J. Oral Med. Pain 2024, 49, 35–39. [Google Scholar] [CrossRef]
- Muraoka, H.; Ito, K.; Hirahara, N.; Ichiki, S.; Kondo, T.; Kaneda, T. Magnetic resonance imaging texture analysis in the quantitative evaluation of acute osteomyelitis of the mandibular bone. Dentomaxillofac. Radiol. 2022, 51, 20210321. [Google Scholar] [CrossRef] [PubMed]
- Gudmundsson, T.; Torkov, P.; Thygesen, T.H. Diagnosis and Treatment of Osteomyelitis of the Jaw—A Systematic Review (2002–2015) of the Literature. J. Dent. Oral Disord. 2017, 3, 1066. [Google Scholar] [CrossRef]
- Vargas-Rojas, D.C.; Rodriguez-Flores, A.; Moreno-Villalobos, D.; Chumpitaz-Cerrate, V.; Chávez-Rimache, L. Radical Surgical Approach to Chronic Suppurative Osteomyelitis: Case Report. Odovtos-Int. J. Dent. Sci. 2023, 26, 14–20. [Google Scholar] [CrossRef]
- Griffin, A.Τ.; Timbrook, Τ.; Harting, J.; Christensen, D. Streptococcus anginosus group and osteomyelitis: A single centre clinical experience. Postgrad. Med. J. 2013, 89, 262–265. [Google Scholar] [CrossRef]
- Tiwari, P.; Bera, R.N.; Kanojia, S.; Chauhan, N.; Hirani, M.S. Assessing the optimal imaging modality in the diagnosis of jaw osteomyelitis. A meta-analysis. Br. J. Oral Maxillofac. Surg. 2021, 59, 982–992. [Google Scholar] [CrossRef]
- Park, M.S.; Eo, M.Y.; Myoung, H.; Kim, S.M.; Lee, J.H. Early diagnosis of jaw osteomyelitis by easy digitalized panoramic analysis. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 6. [Google Scholar] [CrossRef]
- Salimi, F.; Motter, D.; Salimi, Z. Temporomandibular joint (TMJ) disorders as first clinical manifestations in external auditory canal cholesteatoma. A case report. Ann. Med. Surg. 2022, 74, 103287. [Google Scholar] [CrossRef] [PubMed]
- Mardinger, O.; Rosen, D.; Minkow, B.; Tulzinsky, Z.; Ophir, D.; Hirshberg, A. Temporomandibular joint involvement in malignant external otitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Tsuno, N.S.G.; Tsuno, M.Y.; Coelho Neto, C.A.F.; Noujaim, S.E.; Decnop, M.; Pacheco, F.T.; Souza, S.A.; Fonseca, A.P.A.; Garcia, M.R.T. Imaging the External Ear: Practical Approach to Normal and Pathologic Conditions. Radiographics 2022, 42, 522–540. [Google Scholar] [CrossRef]
- Abebe, A.A.; Birhanu, A.G. Methicillin Resistant Staphylococcus aureus: Molecular Mechanisms Underlying Drug Resistance Development and Novel Strategies to Combat. Infect Drug Resist. 2023, 16, 7641–7662. [Google Scholar] [CrossRef] [PubMed]
- Tuon, F.F.; Suss, P.H.; Telles, J.P.; Dantas, L.R.; Borges, N.H.; Ribeiro, V.S.T. Antimicrobial Treatment of Staphylococcus aureus Biofilms. Antibiotics 2023, 12, 87. [Google Scholar] [CrossRef]
- Weden, A.; Haig, H. Current thinking in physiotherapy for the management of idiopathic and postsurgical temporomandibular disorders: A narrative review. Br. J. Oral Maxillofac. Surg. 2024, 62, 588–593. [Google Scholar] [CrossRef]
- Sidebottom, A.J. How do I manage restricted mouth opening secondary to problems with the temporomandibular joint? Br. J. Oral Maxillofac. Surg. 2013, 51, 469–472. [Google Scholar] [CrossRef]
- Shulman, D.H.; Shipman, B.; Willis, F.B. Treating trismus with dynamic splinting: A cohort, case series. Adv. Ther. 2008, 25, 9–16. [Google Scholar] [CrossRef]
- Harris, B.N.; Kuhn, M.; Evangelista, L.; Davis, S. Speech and Swallow Therapy. In Complex Head and Neck Microvascular Surgery; Quimby, A., Parmar, S., Fernandes, R., Eds.; Springer: Cham, Switzerland, 2023; pp. 231–248. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age | Etiology | Imaging | Preoperative Interincisal Distance | Operative Intervention | Postperative Interincisal Distance | |
|---|---|---|---|---|---|---|---|
| 1 | Male | 48 | Osteoma of the coronoid process |
OPG CT | 19 mm | Coronoidectomy | 39 mm |
| 2 | Female | 10 | Bilateral hyperplasia of the coronoid processes |
OPG CT | 17 mm | Bilateral coronoidectomy | 45 mm |
| 3 | Male | 34 | Myositis ossificans traumatica | CT | 15 mm | Excision of calcified mass | 52 mm |
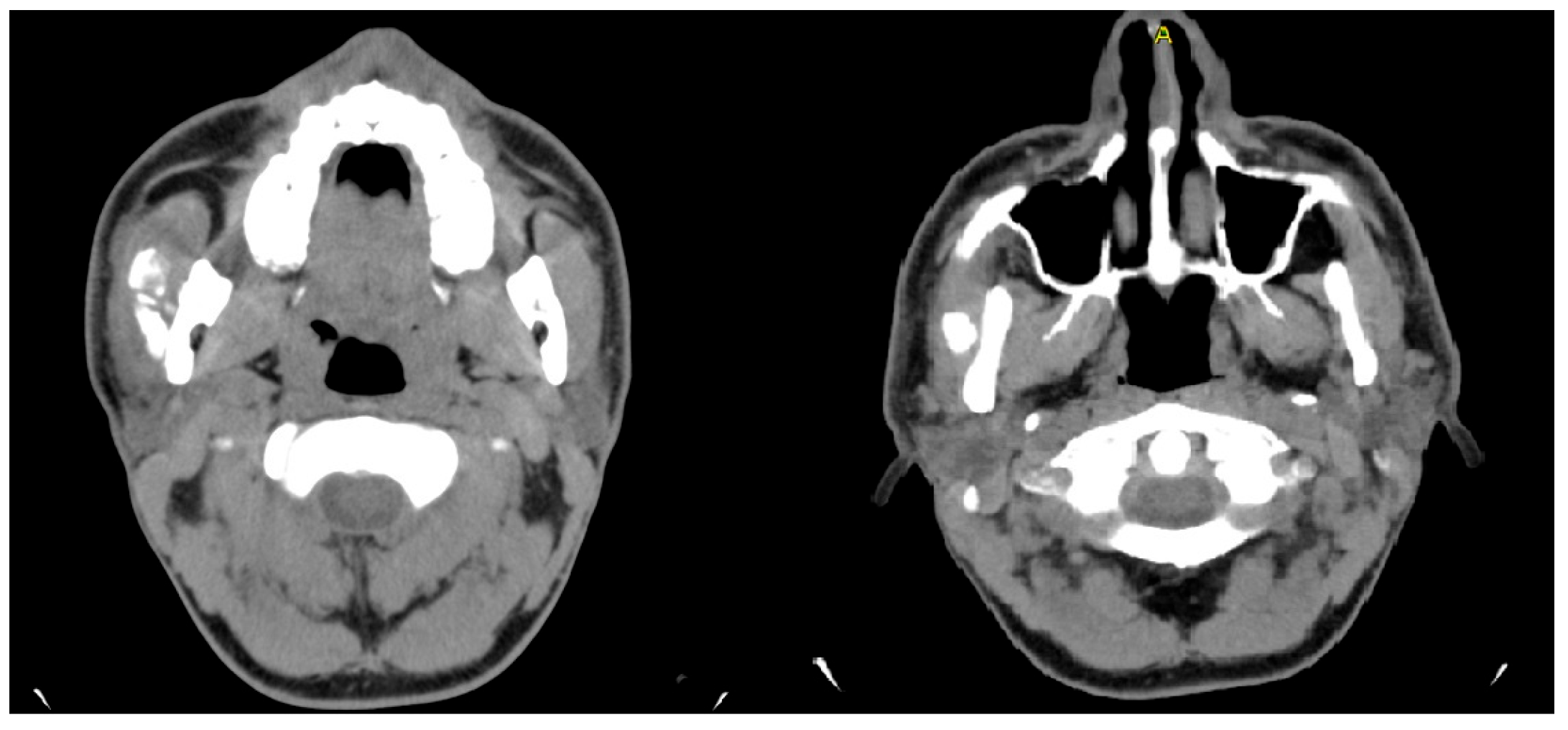
| 4 | Male | 44 | Chronic osteomyelitis of the mandible |
OPG CT/MRI | 13 mm | Incision and drainage of the abscess and surgical curettage | 48 mm |
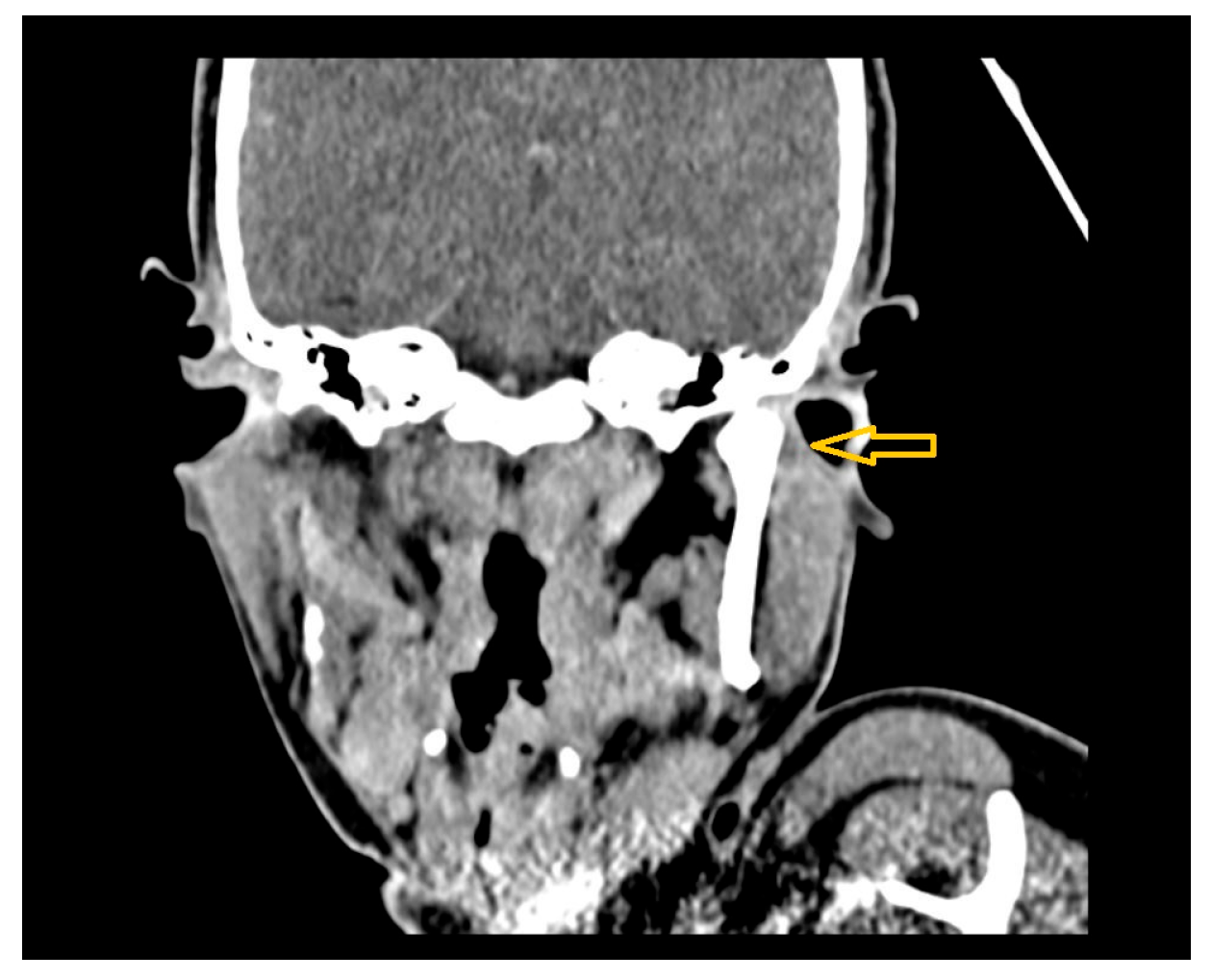
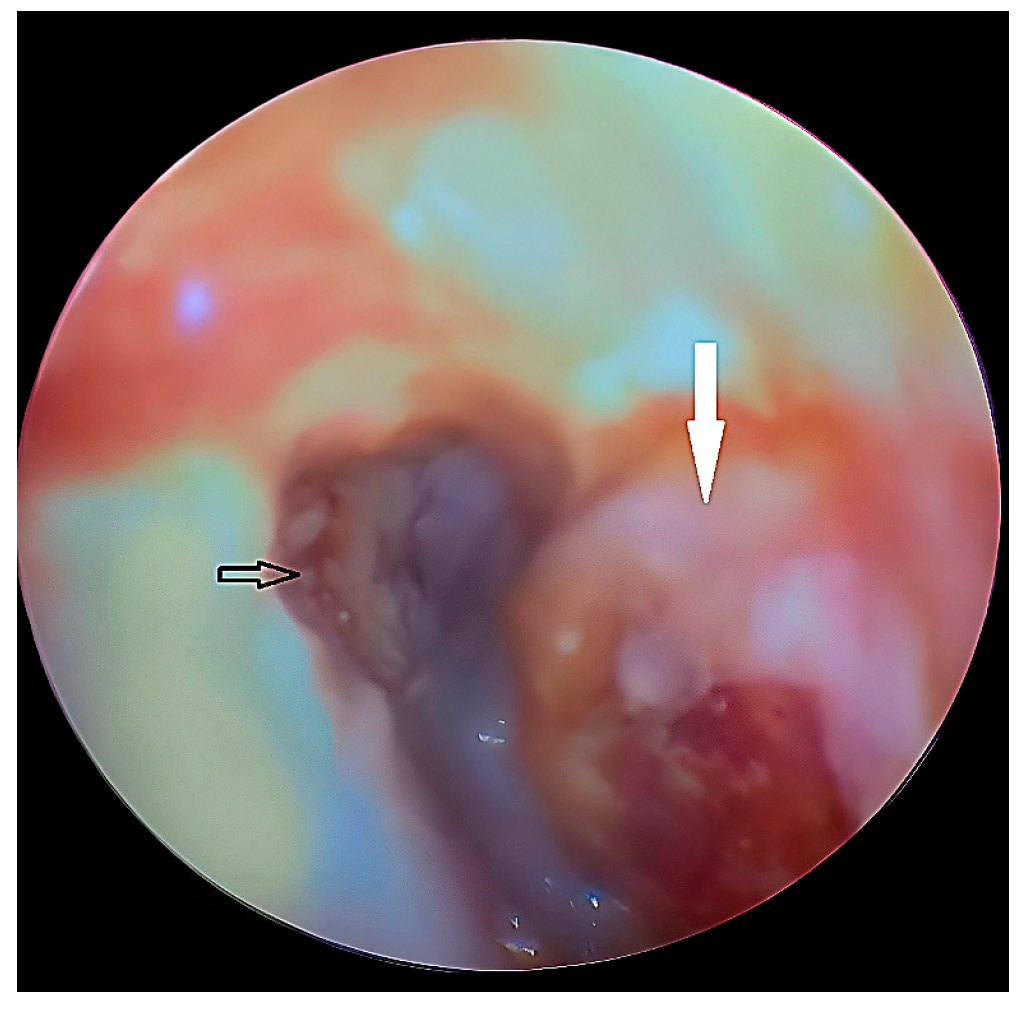
| 5 | Female | 45 | External auditory canal abscess |
OPG CT/MRI | 10 mm | Incision and drainage of the abscess | 51 mm |
| Category | Etiology | Examples |
|---|---|---|
| Intra-articular | Structural abnormalities or inflammation | TMJ ankylosis, arthritis, synovitis, Discus pathology |
| Extra-articular | Neoplastic | Osteoma, sarcoma, lymphoma |
| Traumatic | Myositis ossificans, mandibular fractures | |
| Infectious | Peritonsillar abscess, mandibular osteomyelitis | |
| Fibrotic | Submucous fibrosis, radiation-induced fibrosis | |
| Neurological | Tetanus, dystonia | |
| Iatrogenic | Postoperative complications, TMJ surgeries |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalaitsidou, I.; Gass, M.; Tatsis, D.; Khalil, S.; Schedeit, C.; Marjanowski, S.D.; Wiegner, S.; Schaller, B. Exploring Atypical Origins of Trismus: Surgical Solutions for Rare Pathologies—Insights from Rare Clinical Cases. Diagnostics 2025, 15, 1360. https://doi.org/10.3390/diagnostics15111360
Kalaitsidou I, Gass M, Tatsis D, Khalil S, Schedeit C, Marjanowski SD, Wiegner S, Schaller B. Exploring Atypical Origins of Trismus: Surgical Solutions for Rare Pathologies—Insights from Rare Clinical Cases. Diagnostics. 2025; 15(11):1360. https://doi.org/10.3390/diagnostics15111360
Chicago/Turabian StyleKalaitsidou, Ioanna, Mathieu Gass, Dimitris Tatsis, Sherin Khalil, Christian Schedeit, Simon David Marjanowski, Sarah Wiegner, and Benoît Schaller. 2025. "Exploring Atypical Origins of Trismus: Surgical Solutions for Rare Pathologies—Insights from Rare Clinical Cases" Diagnostics 15, no. 11: 1360. https://doi.org/10.3390/diagnostics15111360
APA StyleKalaitsidou, I., Gass, M., Tatsis, D., Khalil, S., Schedeit, C., Marjanowski, S. D., Wiegner, S., & Schaller, B. (2025). Exploring Atypical Origins of Trismus: Surgical Solutions for Rare Pathologies—Insights from Rare Clinical Cases. Diagnostics, 15(11), 1360. https://doi.org/10.3390/diagnostics15111360