


Ultrasound Imaging of the Articularis Genus Muscle: Implications for Ultrasound-Guided Suprapatellar Recess Injection
 ,
,  , , , , and
, , , , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Material and Methods
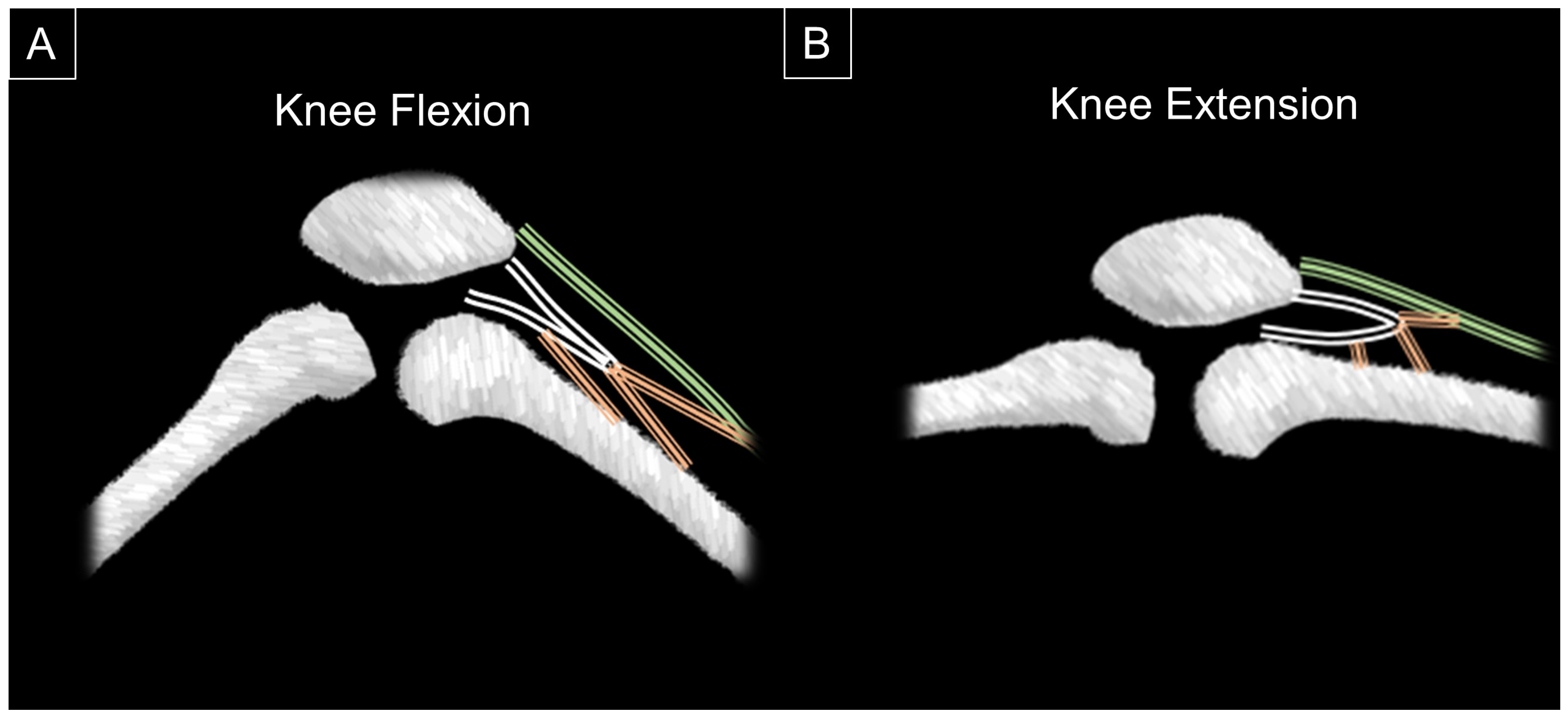
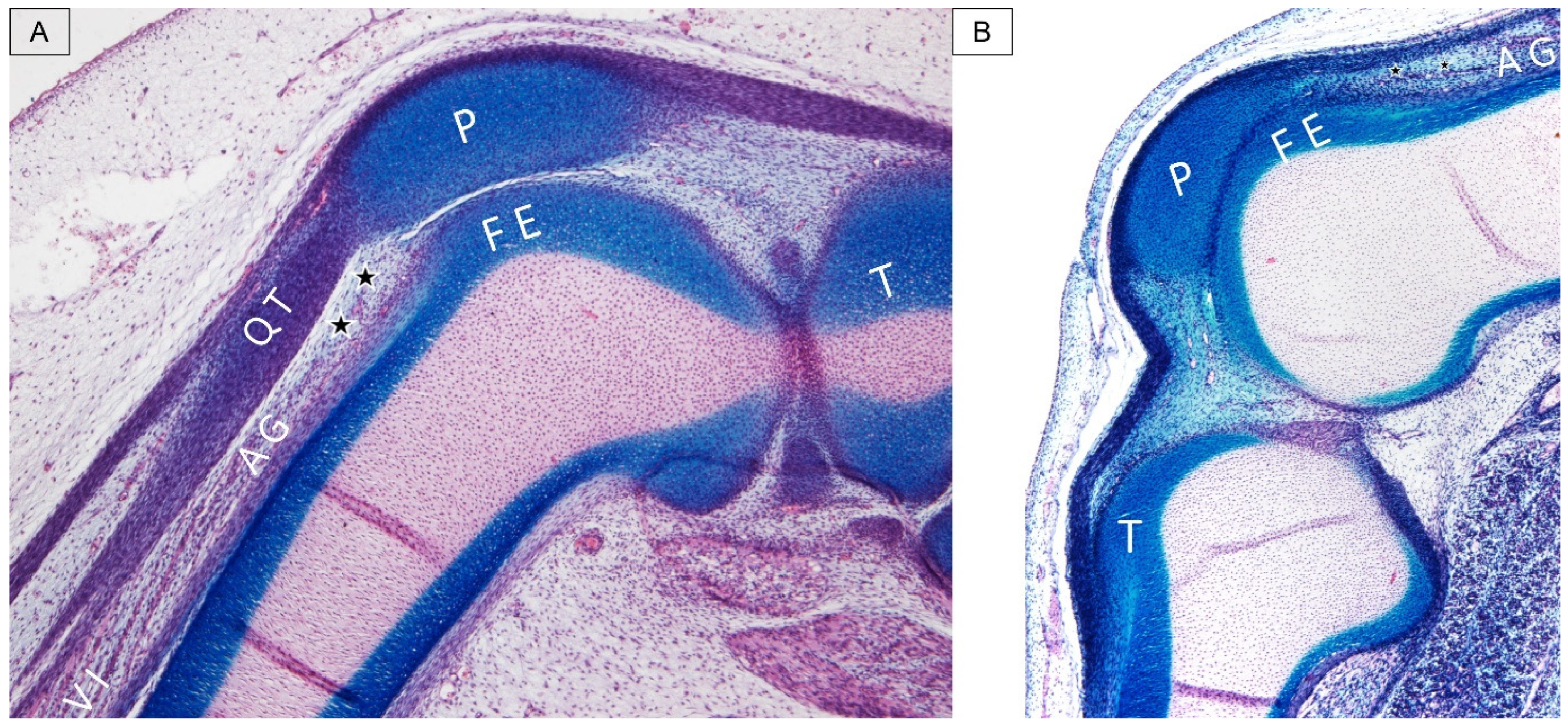
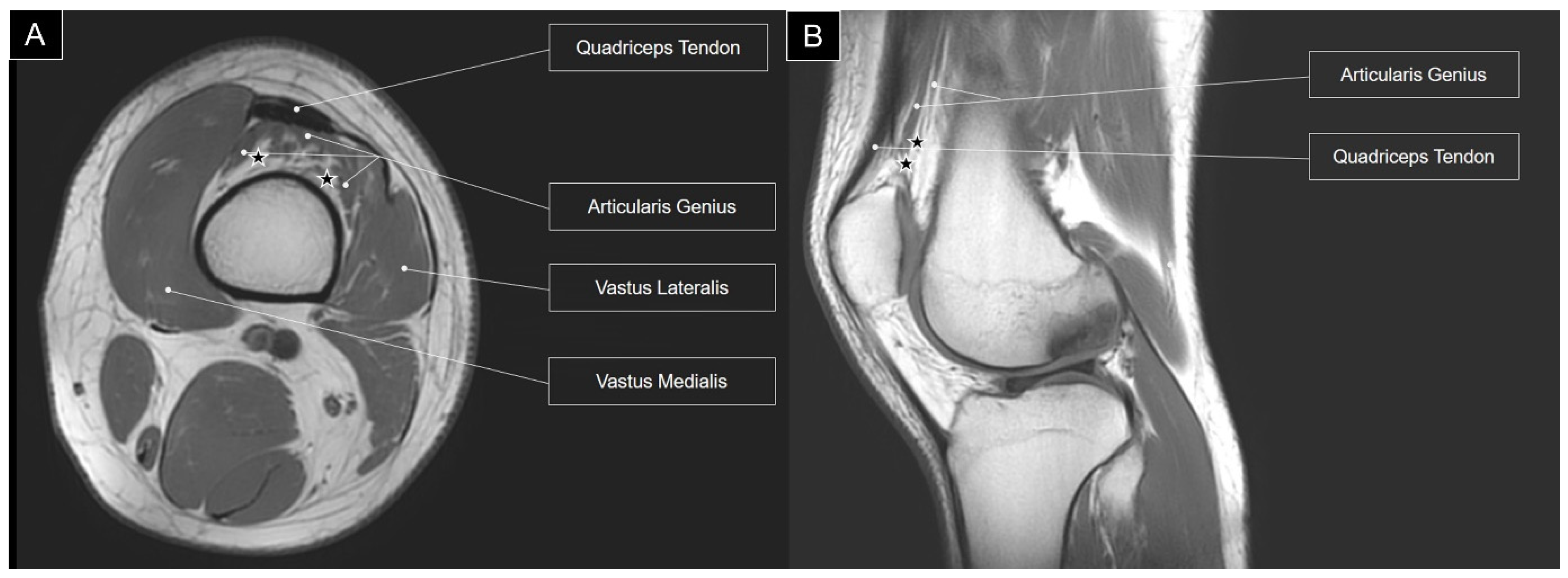
3. Anatomic Elaboration of Articularis Genus
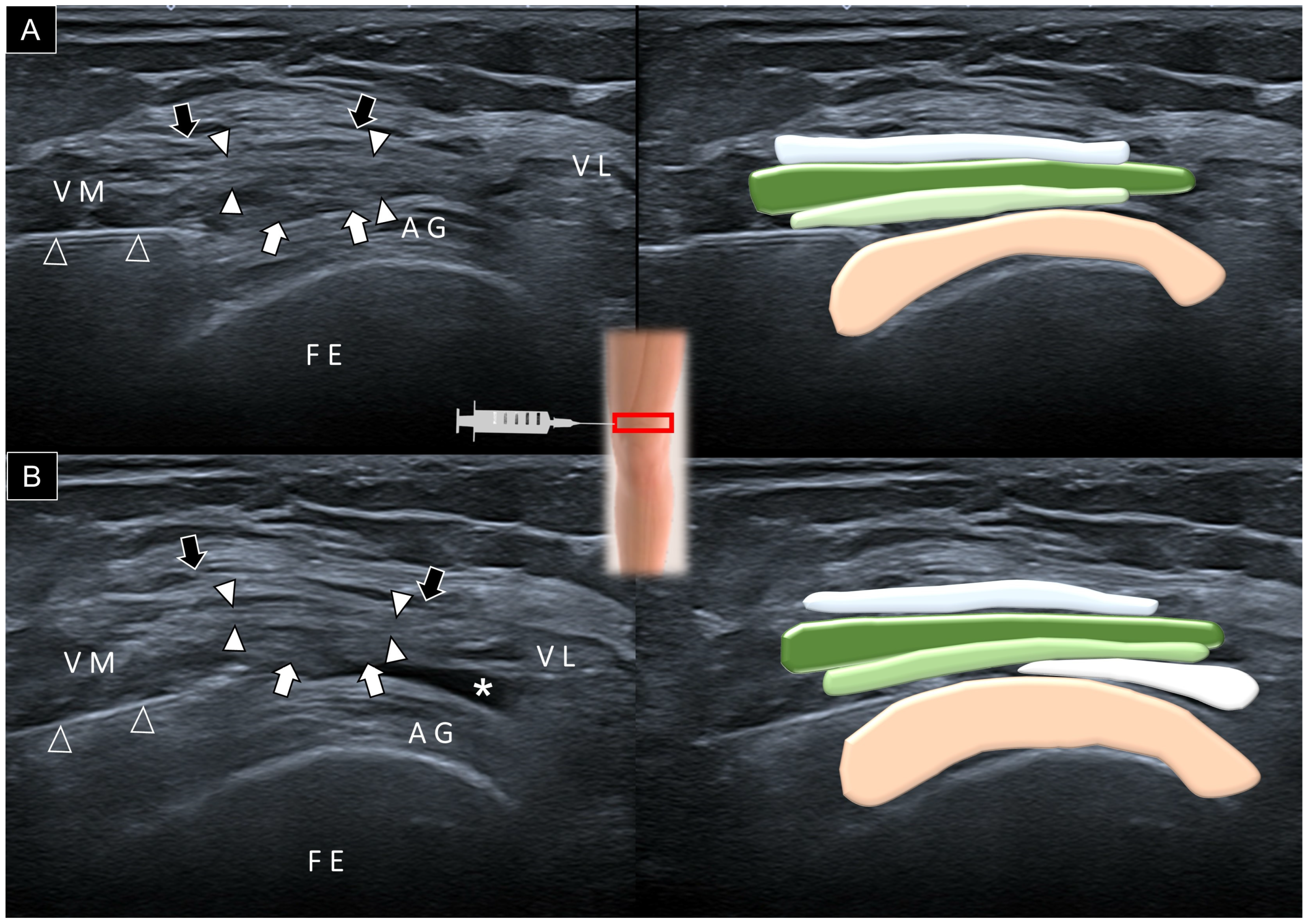
4. Sonoanatomy of Articularis Genus
5. Implication of Ultrasound-Guided Injection
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fenn, S.; Datir, A.; Saifuddin, A. Synovial recesses of the knee: MR imaging review of anatomical and pathological features. Skelet. Radiol. 2009, 38, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Chagas-Neto, F.A.; Taneja, A.K.; Gregio-Junior, E.; Nogueira-Barbosa, M.H. In-Plane Ultrasound-Guided Knee Injection Through a Lateral Suprapatellar Approach: A Safe Technique. Ultrasound Q. 2017, 33, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Lueders, D.R.; Smith, J.; Sellon, J.L. Ultrasound-Guided Knee Procedures. Phys. Med. Rehabil. Clin. N. Am. 2016, 27, 631–648. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Stecco, C.; Güvener, O.; Mezian, K.; Ricci, V.; Jačisko, J.; Novotný, T.; Kara, M.; Chang, K.V.; Dughbaj, M.; et al. EURO-MUSCULUS/USPRM Dynamic Ultrasound Protocols for Knee. Am. J. Phys. Med. Rehabil. 2023, 102, e67–e72. [Google Scholar] [CrossRef] [PubMed]
- Grob, K.; Gilbey, H.; Manestar, M.; Ackland, T.; Kuster, M.S. The Anatomy of the Articularis Genus Muscle and Its Relation to the Extensor Apparatus of the Knee. JBJS Open Access 2017, 2, e0034. [Google Scholar] [CrossRef] [PubMed]
- Woodley, S.J.; Latimer, C.P.; Meikle, G.R.; Stringer, M.D. Articularis genus: An anatomic and MRI study in cadavers. J. Bone Jt. Surg. 2012, 94, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Takahashi, Y.M. articularis genus. Observations on arrangement and consideration of function. Surg. Radiol. Anat. 1987, 9, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Maricar, N.; Parkes, M.J.; Callaghan, M.J.; Felson, D.T.; O’Neill, T.W. Where and how to inject the knee—A systematic review. Semin. Arthritis Rheum. 2013, 43, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Ertilav, E.; Sarı, S.; Ertilav, D.; Aydın, O.N. Comparison of radiological and clinical results of knee intra-articular injections with two ultrasonography-guided approach techniques: A randomized controlled study. Arch. Rheumatol. 2023, 38, 230–237. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, W.-T.; Chang, K.-V.; Naňka, O.; Mezian, K.; Ricci, V.; Wang, B.; Özçakar, L. Ultrasound Imaging of the Articularis Genus Muscle: Implications for Ultrasound-Guided Suprapatellar Recess Injection. Diagnostics 2024, 14, 183. https://doi.org/10.3390/diagnostics14020183
Wu W-T, Chang K-V, Naňka O, Mezian K, Ricci V, Wang B, Özçakar L. Ultrasound Imaging of the Articularis Genus Muscle: Implications for Ultrasound-Guided Suprapatellar Recess Injection. Diagnostics. 2024; 14(2):183. https://doi.org/10.3390/diagnostics14020183
Chicago/Turabian StyleWu, Wei-Ting, Ke-Vin Chang, Ondřej Naňka, Kamal Mezian, Vincenzo Ricci, Bow Wang, and Levent Özçakar. 2024. "Ultrasound Imaging of the Articularis Genus Muscle: Implications for Ultrasound-Guided Suprapatellar Recess Injection" Diagnostics 14, no. 2: 183. https://doi.org/10.3390/diagnostics14020183
APA StyleWu, W.-T., Chang, K.-V., Naňka, O., Mezian, K., Ricci, V., Wang, B., & Özçakar, L. (2024). Ultrasound Imaging of the Articularis Genus Muscle: Implications for Ultrasound-Guided Suprapatellar Recess Injection. Diagnostics, 14(2), 183. https://doi.org/10.3390/diagnostics14020183