
Radiomics and Artificial Intelligence in Radiotheranostics: A Review of Applications for Radioligands Targeting Somatostatin Receptors and Prostate-Specific Membrane Antigens
 , ,
, ,  ,
,
Abstract
1. Introduction
2. Radiomics and AI Workflow
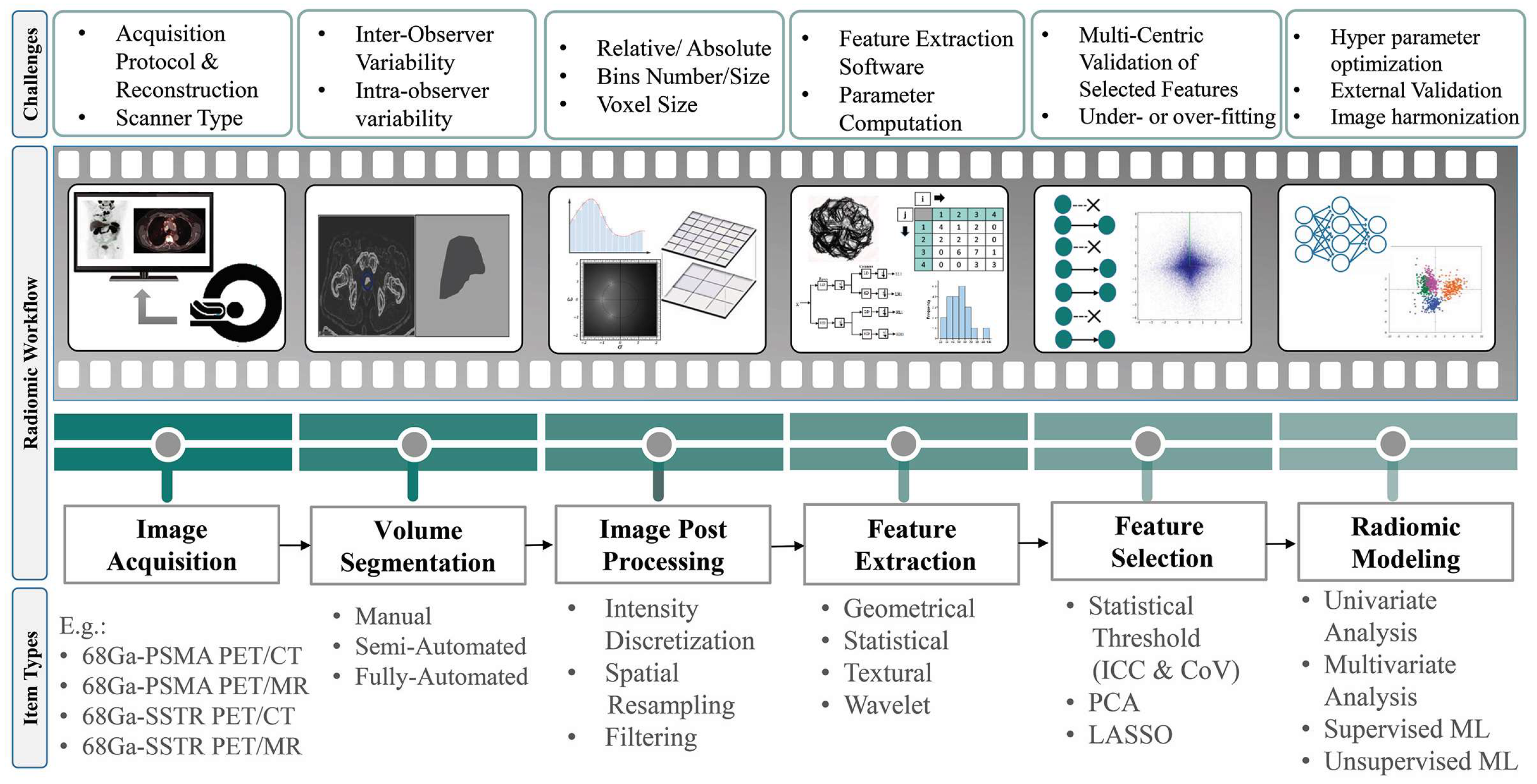
- Geometric or shape features: based on the segmented regions.
- Statistical or intensity features: computed using intensity values in each image region.
- Textural features (TFs): quantification of image intensity and regularity via mathematical functions.
- Wavelet or high-order features: the image transformation process is essential to obtain these features.
3. Application of Radiomics and AI in 68GA SSTR and PSMA Image-Guided RPTS
3.1. RPT Response Assessment
3.1.1. 68Ga/177Lu-SSTR
3.1.2. 68Ga/177Lu-PSMA
3.2. Restaging
3.3. Segmentation
3.4. Dose Prediction
4. Application of Radiomics and AI in [18F]PSMA PET/CT Image-Guided RPTS
4.1. RPT Response Assessment
4.2. Segmentation
5. Application of Radiomics and AI in 64Cu SSTR and PSMA Image-Guided RPTS
5.1. RPT Response Assessment
5.2. Segmentation
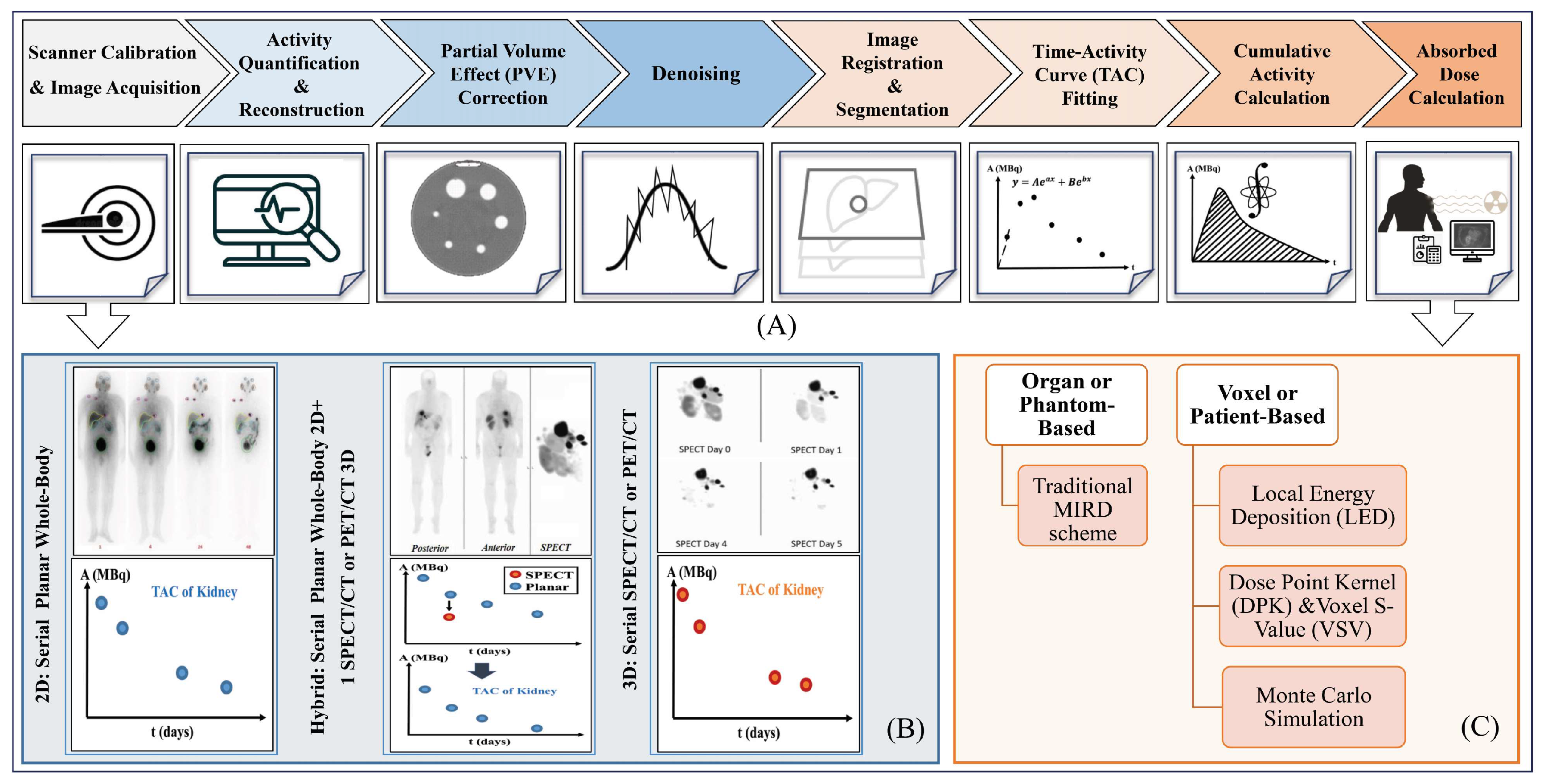
6. Dosimetry Workflow and Treatment Planning
7. Role of AI in Dosimetry Workflow of 177Lu-SSTR and PSMA RPT
7.1. Image Acquisition and Quantification
7.2. Image Segmentation
7.3. Dose Estimation
8. Role of AI in Dosimetry Workflow of 90Y SSTR and PSMA RPT
9. Clinical Perspectives on Radiomics and AI
10. Discussion and Future Directions
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Li, T.; Ao, E.C.; Lambert, B.; Brans, B.; Vandenberghe, S.; Mok, G.S. Quantitative imaging for targeted radionuclide therapy dosimetry-technical review. Theranostics 2017, 7, 4551. [Google Scholar] [CrossRef] [PubMed]
- Teker, F.; Elboga, U. Is SUVmax a useful marker for progression-free survival 177 in patients with metastatic GEP-NET receiving Lu-DOTATATE therapy? Hell. J. Nucl. Med. 2021, 24, 122–131. [Google Scholar] [PubMed]
- Huizing, D.; Aalbersberg, E.A.; Versleijen, M.W.; Tesselaar, M.E.; Walraven, I.; Lahaye, M.J.; de Wit van der Veen, B.J.; Stokkel, M.P. Early response assessment and prediction of overall survival after peptide receptor radionuclide therapy. Cancer Imaging 2020, 20, 57. [Google Scholar] [CrossRef] [PubMed]
- Jeelani, S.; Reddy, R.J.; Maheswaran, T.; Asokan, G.; Dany, A.; Anand, B. Theranostics: A treasured tailor for tomorrow. J. Pharm. Bioallied Sci. 2014, 6 (Suppl. S1), S6. [Google Scholar] [CrossRef] [PubMed]
- Sjögreen Gleisner, K.; Chouin, N.; Gabina, P.M.; Cicone, F.; Gnesin, S.; Stokke, C.; Konijnenberg, M.; Cremonesi, M.; Verburg, F.A.; Bernhardt, P. EANM dosimetry committee recommendations for dosimetry of 177Lu-labelled somatostatin-receptor-and PSMA-targeting ligands. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1778–1809. [Google Scholar] [CrossRef] [PubMed]
- Khazaei, Z.; Jarrahi, A.M.; Momenabadi, V.; Ghorat, F.; Adineh, H.; Sohrabivafa, M.; Goodarzi, E. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide stomach cancers and their relationship with the human development index (HDI). World Cancer Res. J. 2019, 6, e1257. [Google Scholar]
- Dy, G.W.; Gore, J.L.; Forouzanfar, M.H.; Naghavi, M.; Fitzmaurice, C. Global burden of urologic cancers, 1990–2013. Eur. Urol. 2017, 71, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Steele, C.B.; Li, J.; Huang, B.; Weir, H.K. Prostate cancer survival in the United States by race and stage (2001–2009): Findings from the CONCORD-2 study. Cancer 2017, 123, 5160–5177. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Moul, J.W.; Carroll, P.R. The changing face of prostate cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 8146–8151. [Google Scholar] [CrossRef]
- Jones, W.; Griffiths, K.; Barata, P.C.; Paller, C.J. PSMA theranostics: Review of the current status of PSMA-targeted imaging and radioligand therapy. Cancers 2020, 12, 1367. [Google Scholar] [CrossRef]
- Rahbar, K.; Afshar-Oromieh, A.; Jadvar, H.; Ahmadzadehfar, H. PSMA theranostics: Current status and future directions. Mol. Imaging 2018, 17, 1536012118776068. [Google Scholar] [CrossRef]
- Ahmadzadehfar, H.; Aryana, K.; Pirayesh, E.; Farzanehfar, S.; Assadi, M.; Fallahi, B.; Shafiei, B.; Ayati, N.; Amoui, M. The Iranian Society of Nuclear Medicine practical guideline on radioligand therapy in metastatic castration-resistant prostate cancer using 177Lu-PSMA. Iran. J. Nucl. Med. 2018, 26, 2. [Google Scholar]
- Shakeri, S.; Askari, E.; Zarehparvar, S.; Farahmandfar, F.; Norouzbeigi, N.; Salek, R.; Aryana, K. [68Ga] Ga-PSMA-11 PET/CT for staging and patient management of high-risk prostate cancer: A single-center experience from Iran. Iran. J. Nucl. Med. 2022, 30, 33–39. [Google Scholar]
- Liberini, V.; Laudicella, R.; Balma, M.; Nicolotti, D.G.; Buschiazzo, A.; Grimaldi, S.; Lorenzon, L.; Bianchi, A.; Peano, S.; Bartolotta, T.V. Radiomics and artificial intelligence in prostate cancer: New tools for molecular hybrid imaging and theragnostics. Eur. Radiol. Exp. 2022, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- FDA. FDA Approves Pluvicto for Metastatic Castration-Resistant Prostate Cancer. 2022. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pluvicto-metastatic-castration-resistant-prostate-cancer (accessed on 23 March 2022).
- Fallahi, B.; Khademi, N.; Karamzade-Ziarati, N.; Fard-Esfahani, A.; Emami-Ardekani, A.; Farzanefar, S.; Eftekhari, M.; Beiki, D. 99mTc-PSMA SPECT/CT versus 68Ga-PSMA PET/CT in the evaluation of metastatic prostate cancer. Clin. Nucl. Med. 2021, 46, e68–e74. [Google Scholar] [CrossRef] [PubMed]
- Harsini, S.; Fallahi, B.; Ziarati, N.K.; Razi, A.; Amini, E.; Emami-Ardekani, A.; Fard-Esfahani, A.; Parizi, M.K.; Farzanehfar, S.; Beiki, D. A Prospective Study on [68Ga]-PSMA PET/CT Imaging in Newly Diagnosed Intermediate-and High-Risk Prostate Cancer. Asia Ocean. J. Nucl. Med. Biol. 2021, 9, 101. [Google Scholar]
- Das, S.; Dasari, A. Epidemiology, incidence, and prevalence of neuroendocrine neoplasms: Are there global differences? Curr. Oncol. Rep. 2021, 23, 43. [Google Scholar] [CrossRef]
- Taal, B.; Visser, O. Epidemiology of neuroendocrine tumours. Neuroendocrinology 2004, 80 (Suppl. S1), 3–7. [Google Scholar] [CrossRef]
- Virgolini, I.; Ambrosini, V.; Bomanji, J.B.; Baum, R.P.; Fanti, S.; Gabriel, M.; Papathanasiou, N.D.; Pepe, G.; Oyen, W.; De Cristoforo, C. Procedure guidelines for pet/ct tumour imaging with 68Ga-dota-conjugated peptides: 68Ga-dota-toc, 68Ga-dota-noc, 68Ga-dota-tate. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 2004–2010. [Google Scholar] [CrossRef]
- FDA. FDA Approves Lutetium Lu, F. 177 Dotatate for Treatment of GEP-NETS. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-lutetium-lu-177-dotatate-treatment-gep-nets (accessed on 26 January 2018).
- Miller, C.; Rousseau, J.; Ramogida, C.F.; Celler, A.; Rahmim, A.; Uribe, C.F. Implications of physics, chemistry and biology for dosimetry calculations using theranostic pairs. Theranostics 2022, 12, 232. [Google Scholar] [CrossRef]
- Yousefirizi, F.; Decasez, P.; Amyar, A.; Ruan, S.; Saboury, B.; Rahmim, A. Artificial Intelligence-Based Detection, Classification and Prediction/Prognosis in PET Imaging: Towards Radiophenomics. arXiv 2021, arXiv:2110.10332. [Google Scholar]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.; Deist, T.M.; Peerlings, J.; De Jong, E.E.; Van Timmeren, J.; Sanduleanu, S.; Larue, R.T.; Even, A.J.; Jochems, A. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Ray, S. A quick review of machine learning algorithms. In Proceedings of the 2019 International Conference on Machine Learning, Big Data, Cloud and Parallel Computing (COMITCon), Faridabad, India, 14–16 February 2019; IEEE: New York, NY, USA, 2019; pp. 35–39. [Google Scholar]
- Alzubaidi, L.; Zhang, J.; Humaidi, A.J.; Al-Dujaili, A.; Duan, Y.; Al-Shamma, O.; Santamaría, J.; Fadhel, M.A.; Al-Amidie, M.; Farhan, L. Review of deep learning: Concepts, CNN architectures, challenges, applications, future directions. J. Big Data 2021, 8, 1–74. [Google Scholar] [CrossRef]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.; Dekker, A.; Fenstermacher, D. Radiomics: The process and the challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef] [PubMed]
- Reuzé, S.; Schernberg, A.; Orlhac, F.; Sun, R.; Chargari, C.; Dercle, L.; Deutsch, E.; Buvat, I.; Robert, C. Radiomics in nuclear medicine applied to radiation therapy: Methods, pitfalls, and challenges. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1117–1142. [Google Scholar] [CrossRef]
- Orlhac, F.; Nioche, C.; Klyuzhin, I.; Rahmim, A.; Buvat, I. Radiomics in PET imaging: A practical guide for newcomers. PET Clin. 2021, 16, 597–612. [Google Scholar] [CrossRef]
- Bradshaw, T.J.; Boellaard, R.; Dutta, J.; Jha, A.K.; Jacobs, P.; Li, Q.; Liu, C.; Sitek, A.; Saboury, B.; Scott, P.J. Nuclear medicine and artificial intelligence: Best practices for algorithm development. J. Nucl. Med. 2022, 63, 500–510. [Google Scholar] [CrossRef]
- Herrmann, K.; Schwaiger, M.; Lewis, J.S.; Solomon, S.B.; McNeil, B.J.; Baumann, M.; Gambhir, S.S.; Hricak, H.; Weissleder, R. Radiotheranostics: A roadmap for future development. Lancet Oncol. 2020, 21, e146–e156. [Google Scholar] [CrossRef]
- Kręcisz, P.; Czarnecka, K.; Królicki, L.; Mikiciuk-Olasik, E.b.; Szymański, P. Radiolabeled peptides and antibodies in medicine. Bioconjugate Chem. 2020, 32, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Benešová, M.; Reischl, G. Production of radionuclides: Cyclotrons and reactors. Nucl. Med. Mol. Imaging 2021, 1, 52–65. [Google Scholar]
- Berry, D.J.; Ma, Y.; Ballinger, J.R.; Tavaré, R.; Koers, A.; Sunassee, K.; Zhou, T.; Nawaz, S.; Mullen, G.E.; Hider, R.C. Efficient bifunctional gallium-68 chelators for positron emission tomography: Tris (hydroxypyridinone) ligands. Chem. Commun. 2011, 47, 7068–7070. [Google Scholar] [CrossRef] [PubMed]
- Rinne, S.S.; Vorobyeva, A. Radiometals—Chemistry and radiolabeling. In Reference Module in Biomedical Sciences; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Arabi, H.; Zaidi, H. Applications of artificial intelligence and deep learning in molecular imaging and radiotherapy. Eur. J. Hybrid Imaging 2020, 4, 17. [Google Scholar] [CrossRef] [PubMed]
- Grubmüller, B.; Senn, D.; Kramer, G.; Baltzer, P.; D’Andrea, D.; Grubmüller, K.H.; Mitterhauser, M.; Eidherr, H.; Haug, A.R.; Wadsak, W. Response assessment using 68Ga-PSMA ligand PET in patients undergoing 177Lu-PSMA radioligand therapy for metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1063–1072. [Google Scholar] [CrossRef]
- Khurshid, Z.; Ahmadzadehfar, H.; Gaertner, F.C.; Papp, L.; Zsóter, N.; Essler, M.; Bundschuh, R.A. Role of textural heterogeneity parameters in patient selection for 177Lu-PSMA therapy via response prediction. Oncotarget 2018, 9, 33312. [Google Scholar] [CrossRef]
- Acar, E.; Leblebici, A.; Ellidokuz, B.E.; Başbınar, Y.; Kaya, G.Ç. Machine learning for differentiating metastatic and completely responded sclerotic bone lesion in prostate cancer: A retrospective radiomics study. Br. J. Radiol. 2019, 92, 20190286. [Google Scholar] [CrossRef]
- Seifert, R.; Kessel, K.; Schlack, K.; Weber, M.; Herrmann, K.; Spanke, M.; Fendler, W.P.; Hadaschik, B.; Kleesiek, J.; Schäfers, M. PSMA PET total tumor volume predicts outcome of patients with advanced prostate cancer receiving [177Lu] Lu-PSMA-617 radioligand therapy in a bicentric analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1200–1210. [Google Scholar] [CrossRef]
- Widjaja, L.; Werner, R.A.; Ross, T.L.; Bengel, F.M.; Derlin, T. PSMA expression predicts early biochemical response in patients with metastatic castration-resistant prostate cancer under 177Lu-PSMA-617 radioligand therapy. Cancers 2021, 13, 2938. [Google Scholar] [CrossRef]
- Gafita, A.; Calais, J.; Grogan, T.R.; Hadaschik, B.; Wang, H.; Weber, M.; Sandhu, S.; Kratochwil, C.; Esfandiari, R.; Tauber, R. Nomograms to predict outcomes after 177Lu-PSMA therapy in men with metastatic castration-resistant prostate cancer: An international, multicentre, retrospective study. Lancet Oncol. 2021, 22, 1115–1125. [Google Scholar] [CrossRef]
- Khreish, F.; Wiessner, M.; Rosar, F.; Ghazal, Z.; Sabet, A.; Maus, S.; Linxweiler, J.; Bartholomä, M.; Ezziddin, S. Response assessment and prediction of progression-free survival by 68Ga-PSMA-11 PET/CT based on tumor-to-liver ratio (TLR) in patients with mCRPC undergoing 177Lu-PSMA-617 radioligand therapy. Biomolecules 2021, 11, 1099. [Google Scholar] [CrossRef] [PubMed]
- Moazemi, S.; Erle, A.; Khurshid, Z.; Lütje, S.; Muders, M.; Essler, M.; Schultz, T.; Bundschuh, R.A. Decision-support for treatment with 177Lu-PSMA: Machine learning predicts response with high accuracy based on PSMA-PET/CT and clinical parameters. Ann. Transl. Med. 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Moazemi, S.; Essler, M.; Schultz, T.; Bundschuh, R.A. Predicting treatment response in prostate cancer patients based on multimodal PET/CT for clinical decision support. In Proceedings of the International Workshop on Multimodal Learning for Clinical Decision Support, Strasbourg, France, 1 October 2021; pp. 22–35. [Google Scholar]
- Moazemi, S.; Erle, A.; Lütje, S.; Gaertner, F.C.; Essler, M.; Bundschuh, R.A. Estimating the potential of radiomics features and radiomics signature from pretherapeutic PSMA-PET-CT scans and clinical data for prediction of overall survival when treated with 177Lu-PSMA. Diagnostics 2021, 11, 186. [Google Scholar] [CrossRef]
- Roll, W.; Schindler, P.; Masthoff, M.; Seifert, R.; Schlack, K.; Bögemann, M.; Stegger, L.; Weckesser, M.; Rahbar, K. Evaluation of 68Ga-PSMA-11 PET-MRI in Patients with Advanced Prostate Cancer Receiving 177Lu-PSMA-617 Therapy: A Radiomics Analysis. Cancers 2021, 13, 3849. [Google Scholar] [CrossRef]
- Rosar, F.; Wenner, F.; Khreish, F.; Dewes, S.; Wagenpfeil, G.; Hoffmann, M.A.; Schreckenberger, M.; Bartholomä, M.; Ezziddin, S. Early molecular imaging response assessment based on determination of total viable tumor burden in [68Ga] Ga-PSMA-11 PET/CT independently predicts overall survival in [177Lu] Lu-PSMA-617 radioligand therapy. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1584–1594. [Google Scholar] [CrossRef] [PubMed]
- Gafita, A.; Wang, H.; Robertson, A.; Armstrong, W.R.; Zaum, R.; Weber, M.; Yagubbayli, F.; Kratochwil, C.; Grogan, T.R.; Nguyen, K. Tumor sink effect in 68Ga-PSMA-11 PET: Myth or Reality? J. Nucl. Med. 2022, 63, 226–232. [Google Scholar] [CrossRef]
- Hartrampf, P.E.; Krebs, M.; Peter, L.; Heinrich, M.; Ruffing, J.; Kalogirou, C.; Weinke, M.; Brumberg, J.; Kübler, H.; Buck, A.K. Reduced Segmentation of Lesions Is Comparable to Whole-Body Segmentation for Response Assessment by PSMA PET/CT: Initial Experience with the Keyhole Approach. Biology 2022, 11, 660. [Google Scholar] [CrossRef]
- Pathmanandavel, S.; Crumbaker, M.; Yam, A.O.; Nguyen, A.; Rofe, C.; Hovey, E.; Gedye, C.; Kwan, E.M.; Hauser, C.; Azad, A.A. 177Lu-PSMA-617 and Idronoxil in Men with End-Stage Metastatic Castration-Resistant Prostate Cancer (LuPIN): Patient Outcomes and Predictors of Treatment Response in a Phase I/II Trial. J. Nucl. Med. 2022, 63, 560–566. [Google Scholar] [CrossRef]
- Giesel, F.L.; Schneider, F.; Kratochwil, C.; Rath, D.; Moltz, J.; Holland-Letz, T.; Kauczor, H.-U.; Schwartz, L.H.; Haberkorn, U.; Flechsig, P. Correlation between SUVmax and CT radiomic analysis using lymph node density in PET/CT-based lymph node staging. J. Nucl. Med. 2017, 58, 282–287. [Google Scholar] [CrossRef]
- Moazemi, S.; Khurshid, Z.; Erle, A.; Lütje, S.; Essler, M.; Schultz, T.; Bundschuh, R.A. Machine learning facilitates hotspot classification in PSMA-PET/CT with nuclear medicine specialist accuracy. Diagnostics 2020, 10, 622. [Google Scholar] [CrossRef]
- Erle, A.; Moazemi, S.; Lütje, S.; Essler, M.; Schultz, T.; Bundschuh, R.A. Evaluating a machine learning tool for the classification of pathological uptake in whole-body PSMA-PET-CT scans. Tomography 2021, 7, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Hinzpeter, R.; Baumann, L.; Guggenberger, R.; Huellner, M.; Alkadhi, H.; Baessler, B. Radiomics for detecting prostate cancer bone metastases invisible in CT: A proof-of-concept study. Eur. Radiol. 2022, 32, 1823–1832. [Google Scholar] [CrossRef] [PubMed]
- Hammes, J.; Täger, P.; Drzezga, A. EBONI: A tool for automated quantification of bone metastasis load in PSMA PET/CT. J. Nucl. Med. 2018, 59, 1070–1075. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Gafita, A.; Vollnberg, B.; Tetteh, G.; Haupt, F.; Afshar-Oromieh, A.; Menze, B.; Eiber, M.; Rominger, A.; Shi, K. Deep neural network for automatic characterization of lesions on 68Ga-PSMA-11 PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Seifert, R.; Herrmann, K.; Kleesiek, J.; Schäfers, M.; Shah, V.; Xu, Z.; Chabin, G.; Grbic, S.; Spottiswoode, B.; Rahbar, K. Semiautomatically quantified tumor volume using 68Ga-PSMA-11 PET as a biomarker for survival in patients with advanced prostate cancer. J. Nucl. Med. 2020, 61, 1786–1792. [Google Scholar] [CrossRef] [PubMed]
- Xue, S.; Gafita, A.; Afshar-Oromieh, A.; Eiber, M.; Rominger, A.; Shi, K. Voxel-wise prediction of post-therapy dosimetry for 177Lu-PSMA I&T therapy using deep learning. Soc. Nucl. Med. 2020, 61, 1424. [Google Scholar]
- Xue, S.; Gafita, A.; Drobnjakovic, M.; Afshar-Oromieh, A.; Birindelli, G.; Eiber, M.; Rominger, A.; Shi, K. PBPK pre-trained deep learning for voxel-wise prediction of post-therapy dosimetry for 177Lu-PSMA therapy. Soc. Nucl. Med. 2021, 62, 1174. [Google Scholar]
- Xue, S.; Gafita, A.; Dong, C.; Zhao, Y.; Tetteh, G.; Menze, B.H.; Ziegler, S.; Weber, W.; Afshar-Oromieh, A.; Rominger, A. Application of machine learning to pretherapeutically estimate dosimetry in men with advanced prostate cancer treated with 177Lu-PSMA I&T therapy. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4064–4072. [Google Scholar]
- Xue, S.; Gafita, A.; Dong, C.; Zhao, Y.; Tetteh, G.; Menze, B.H.; Ziegler, S.; Weber, W.; Afshar-Oromieh, A.; Rominger, A. Proof-of-concept Study to Estimate Individual Post-Therapy Dosimetry in Men with Advanced Prostate Cancer Treated with 177Lu-PSMA I&T Therapy. Res. Sq. 2022; online ahead of print. [Google Scholar]
- Werner, R.A.; Lapa, C.; Ilhan, H.; Higuchi, T.; Buck, A.K.; Lehner, S.; Bartenstein, P.; Bengel, F.; Schatka, I.; Muegge, D.O. Survival prediction in patients undergoing radionuclide therapy based on intratumoral somatostatin-receptor heterogeneity. Oncotarget 2017, 8, 7039. [Google Scholar] [CrossRef]
- Werner, R.A.; Ilhan, H.; Lehner, S.; Papp, L.; Zsótér, N.; Schatka, I.; Muegge, D.O.; Javadi, M.S.; Higuchi, T.; Buck, A.K. Pre-therapy somatostatin receptor-based heterogeneity predicts overall survival in pancreatic neuroendocrine tumor patients undergoing peptide receptor radionuclide therapy. Mol. Imaging Biol. 2019, 21, 582–590. [Google Scholar] [CrossRef]
- Önner, H.; Abdülrezzak, Ü.; Tutuş, A. Could the skewness and kurtosis texture parameters of lesions obtained from pretreatment Ga-68 DOTA-TATE PET/CT images predict receptor radionuclide therapy response in patients with gastroenteropancreatic neuroendocrine tumors? Nucl. Med. Commun. 2020, 41, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.; Kessler, L.; Schaarschmidt, B.; Fendler, W.P.; Lahner, H.; Antoch, G.; Umutlu, L.; Herrmann, K.; Rischpler, C. Treatment-related changes in neuroendocrine tumors as assessed by textural features derived from 68Ga-DOTATOC PET/MRI with simultaneous acquisition of apparent diffusion coefficient. BMC Cancer 2020, 20, 326. [Google Scholar] [CrossRef] [PubMed]
- Ortega, C.; Wong, R.K.; Schaefferkoetter, J.; Veit-Haibach, P.; Myrehaug, S.; Juergens, R.; Laidley, D.; Anconina, R.; Liu, A.; Metser, U. Quantitative 68Ga-DOTATATE PET/CT parameters for the prediction of therapy response in patients with progressive metastatic neuroendocrine tumors treated with 177Lu-DOTATATE. J. Nucl. Med. 2021, 62, 1406–1414. [Google Scholar] [CrossRef]
- Atkinson, C.; Ganeshan, B.; Endozo, R.; Wan, S.; Aldridge, M.D.; Groves, A.M.; Bomanji, J.B.; Gaze, M.N. Radiomics-based texture analysis of 68Ga-DOTATATE positron emission tomography and computed tomography images as a prognostic biomarker in adults with neuroendocrine cancers treated with 177Lu-DOTATATE. Front. Oncol. 2021, 11, 2942. [Google Scholar] [CrossRef] [PubMed]
- Liberini, V.; Rampado, O.; Gallio, E.; De Santi, B.; Ceci, F.; Dionisi, B.; Thuillier, P.; Ciuffreda, L.; Piovesan, A.; Fioroni, F. 68Ga-DOTATOC PET/CT-based radiomic analysis and PRRT outcome: A preliminary evaluation based on an exploratory radiomic analysis on two patients. Front. Med. 2021, 7, 601853. [Google Scholar] [CrossRef]
- Laudicella, R.; Comelli, A.; Liberini, V.; Vento, A.; Stefano, A.; Spataro, A.; Crocè, L.; Baldari, S.; Bambaci, M.; Deandreis, D. [68Ga] DOTATOC PET/CT Radiomics to Predict the Response in GEP-NETs Undergoing [177Lu] DOTATOC PRRT: The “Theragnomics” Concept. Cancers 2022, 14, 984. [Google Scholar] [CrossRef] [PubMed]
- Liberini, V.; De Santi, B.; Rampado, O.; Gallio, E.; Dionisi, B.; Ceci, F.; Polverari, G.; Thuillier, P.; Molinari, F.; Deandreis, D. Impact of segmentation and discretization on radiomic features in 68Ga-DOTA-TOC PET/CT images of neuroendocrine tumor. EJNMMI Phys. 2021, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Wehrend, J.; Silosky, M.; Xing, F.; Chin, B.B. Automated liver lesion detection in 68Ga DOTATATE PET/CT using a deep fully convolutional neural network. EJNMMI Res. 2021, 11, 98. [Google Scholar] [CrossRef]
- Akhavanallaf, A.; Peterson, A.B.; Fitzpatrick, K.; Roseland, M.; Wong, K.K.; El-Naqa, I.; Zaidi, H.; Dewaraja, Y.K. The predictive value of pretherapy [68Ga] Ga-DOTA-TATE PET and biomarkers in [177Lu] Lu-PRRT tumor dosimetry. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 2984–2996. [Google Scholar] [CrossRef]
- Plachouris, D.; Eleftheriadis, V.; Nanos, T.; Papathanasiou, N.; Sarrut, D.; Papadimitroulas, P.; Savvidis, G.; Vergnaud, L.; Salvadori, J.; Imperiale, A. A radiomic-and dosiomic-based machine learning regression model for pretreatment planning in 177Lu-DOTATATE therapy. Med. Phys. 2023, 50, 7222–7235. [Google Scholar] [CrossRef]
- Kratochwil, C.; Stefanova, M.; Mavriopoulou, E.; Holland-Letz, T.; Dimitrakopoulou-Strauss, A.; Afshar-Oromieh, A.; Mier, W.; Haberkorn, U.; Giesel, F. SUV of [68Ga] DOTATOC-PET/CT predicts response probability of PRRT in neuroendocrine tumors. Mol. Imaging Biol. 2015, 17, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Ezziddin, S.; Lohmar, J.; Yong-Hing, C.J.; Sabet, A.; Ahmadzadehfar, H.; Kukuk, G.; Biersack, H.-J.; Guhlke, S.; Reichmann, K. Does the pretherapeutic tumor SUV in 68Ga DOTATOC PET predict the absorbed dose of 177Lu octreotate? Clin. Nucl. Med. 2012, 37, e141–e147. [Google Scholar] [CrossRef]
- Violet, J.; Jackson, P.; Ferdinandus, J.; Sandhu, S.; Akhurst, T.; Iravani, A.; Kong, G.; Kumar, A.R.; Thang, S.P.; Eu, P. Dosimetry of 177Lu-PSMA-617 in metastatic castration-resistant prostate cancer: Correlations between pretherapeutic imaging and whole-body tumor dosimetry with treatment outcomes. J. Nucl. Med. 2019, 60, 517–523. [Google Scholar] [CrossRef]
- Bruvoll, R.; Blakkisrud, J.; Mikalsen, L.; Connelly, J.; Stokke, C. Correlations between [68Ga] Ga-DOTA-TOC uptake and absorbed dose from [177Lu] Lu-DOTA-TATE. Cancers 2022, 15, 1134. [Google Scholar] [CrossRef] [PubMed]
- Scarpa, L.; Buxbaum, S.; Kendler, D.; Fink, K.; Bektic, J.; Gruber, L.; Decristoforo, C.; Uprimny, C.; Lukas, P.; Horninger, W. The 68Ga/177Lu theragnostic concept in PSMA targeting of castration-resistant prostate cancer: Correlation of SUVmax values and absorbed dose estimates. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 788–800. [Google Scholar] [CrossRef]
- Stenvall, A.; Gustafsson, J.; Larsson, E.; Roth, D.; Sundlöv, A.; Jönsson, L.; Hindorf, C.; Ohlsson, T.; Sjögreen Gleisner, K. Relationships between uptake of [68Ga] Ga-DOTA-TATE and absorbed dose in [177Lu] Lu-DOTA-TATE therapy. EJNMMI Res. 2022, 12, 75. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zang, J.; Wang, H.; Liu, Q.; Li, F.; Lin, Y.; Huo, L.; Jacobson, O.; Niu, G.; Fan, X. Pretherapeutic 68Ga-PSMA-617 PET may indicate the dosimetry of 177Lu-PSMA-617 and 177Lu-EB-PSMA-617 in main organs and tumor lesions. Clin. Nucl. Med. 2019, 44, 431. [Google Scholar] [CrossRef] [PubMed]
- Kassar, M.; Drobnjakovic, M.; Birindelli, G.; Xue, S.; Gafita, A.; Wendler, T.; Afshar-Oromieh, A.; Navab, N.; Weber, W.; Eiber, M. PBPK-Adapted Deep Learning for Voxel-Wise Organ Dosimetry Prediction. Nukl.-Nucl. Med. 2022, 61, 178. [Google Scholar]
- Werner, R.A.; Derlin, T.; Lapa, C.; Sheikbahaei, S.; Higuchi, T.; Giesel, F.L.; Behr, S.; Drzezga, A.; Kimura, H.; Buck, A.K. 18F-labeled, PSMA-targeted radiotracers: Leveraging the advantages of radiofluorination for prostate cancer molecular imaging. Theranostics 2020, 10, 1–16. [Google Scholar] [CrossRef]
- Jeitner, T.M.; Babich, J.W.; Kelly, J.M. Advances in PSMA theranostics. Transl. Oncol. 2022, 22, 101450. [Google Scholar] [CrossRef]
- Giesel, F.L.; Hadaschik, B.; Cardinale, J.; Radtke, J.; Vinsensia, M.; Lehnert, W.; Kesch, C.; Tolstov, Y.; Singer, S.; Grabe, N. F-18 labelled PSMA-1007: Biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Szabo, Z.; Mena, E.; Rowe, S.P.; Plyku, D.; Nidal, R.; Eisenberger, M.A.; Antonarakis, E.S.; Fan, H.; Dannals, R.F.; Chen, Y. Initial evaluation of [18F] DCFPyL for prostate-specific membrane antigen (PSMA)-targeted PET imaging of prostate cancer. Mol. Imaging Biol. 2015, 17, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Knorr, K.; Spohn, F.; Will, L.; Maurer, T.; Flechsig, P.; Neels, O.; Schiller, K.; Amaral, H.; Weber, W.A. Detection efficacy of 18F-PSMA-1007 PET/CT in 251 patients with biochemical recurrence of prostate cancer after radical prostatectomy. J. Nucl. Med. 2019, 60, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Cardinale, J.; Schäfer, M.; Neels, O.; Benešová, M.; Mier, W.; Haberkorn, U.; Kopka, K.; Kratochwil, C. 18F-labelled PSMA-1007 shows similarity in structure, biodistribution and tumour uptake to the theragnostic compound PSMA-617. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1929–1930. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.B.; Song, I.H.; Kim, S.Y.; Ko, H.Y.; Kil, H.S.; Chi, D.Y.; Giesel, F.L.; Kopka, K.; Hoepping, A.; Chun, J.-H. Preclinical Evaluation of a Companion Diagnostic Radiopharmaceutical, [18F] PSMA-1007, in a Subcutaneous Prostate Cancer Xenograft Mouse Model. Mol. Pharm. 2022, 20, 1050–1060. [Google Scholar] [CrossRef] [PubMed]
- Pattison, D.A.; Debowski, M.; Gulhane, B.; Arnfield, E.G.; Pelecanos, A.M.; Garcia, P.L.; Latter, M.J.; Lin, C.Y.; Roberts, M.J.; Ramsay, S.C. Prospective intra-individual blinded comparison of [18F] PSMA-1007 and [68 Ga] Ga-PSMA-11 PET/CT imaging in patients with confirmed prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 763–776. [Google Scholar] [CrossRef]
- Saule, L.; Radzina, M.; Liepa, M.; Roznere, L.; Lioznovs, A.; Ratniece, M.; Mamis, E.; Vjaters, E. Recurrent Prostate Cancer Diagnostics with 18F-PSMA-1007 PET/CT: A Systematic Review of the Current State. Diagnostics 2022, 12, 3176. [Google Scholar] [CrossRef]
- Grünig, H.; Maurer, A.; Thali, Y.; Kovacs, Z.; Strobel, K.; Burger, I.A.; Müller, J. Focal unspecific bone uptake on [18F]-PSMA-1007 PET: A multicenter retrospective evaluation of the distribution, frequency, and quantitative parameters of a potential pitfall in prostate cancer imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4483–4494. [Google Scholar] [CrossRef]
- Fanti, S.; Goffin, K.; Hadaschik, B.A.; Herrmann, K.; Maurer, T.; MacLennan, S.; Oprea-Lager, D.E.; Oyen, W.J.; Rouvière, O.; Mottet, N. Consensus statements on PSMA PET/CT response assessment criteria in prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 469–476. [Google Scholar] [CrossRef]
- Schmidkonz, C.; Cordes, M.; Schmidt, D.; Bäuerle, T.; Goetz, T.I.; Beck, M.; Prante, O.; Cavallaro, A.; Uder, M.; Wullich, B. 68Ga-PSMA-11 PET/CT-derived metabolic parameters for determination of whole-body tumor burden and treatment response in prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1862–1872. [Google Scholar] [CrossRef]
- Unterrainer, L.M.; Beyer, L.; Zacherl, M.J.; Gildehaus, F.J.; Todica, A.; Kunte, S.C.; Holzgreve, A.; Sheikh, G.T.; Herlemann, A.; Casuscelli, J. Total Tumor Volume on 18F-PSMA-1007 PET as Additional Imaging Biomarker in mCRPC Patients Undergoing PSMA-Targeted Alpha Therapy with 225Ac-PSMA-I&T. Biomedicines 2022, 10, 946. [Google Scholar]
- Draulans, C.; De Roover, R.; van der Heide, U.A.; Kerkmeijer, L.; Smeenk, R.J.; Pos, F.; Vogel, W.V.; Nagarajah, J.; Janssen, M.; Isebaert, S. Optimal 68Ga-PSMA and 18F-PSMA PET window levelling for gross tumour volume delineation in primary prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Spohn, S.K.; Kramer, M.; Kiefer, S.; Bronsert, P.; Sigle, A.; Schultze-Seemann, W.; Jilg, C.A.; Sprave, T.; Ceci, L.; Fassbender, T.F. Comparison of manual and semi-automatic [18F] PSMA-1007 PET based contouring techniques for intraprostatic tumor delineation in patients with primary prostate cancer and validation with histopathology as standard of reference. Front. Oncol. 2020, 10, 600690. [Google Scholar] [CrossRef] [PubMed]
- Mittlmeier, L.M.; Brendel, M.; Beyer, L.; Albert, N.L.; Todica, A.; Zacherl, M.J.; Wenter, V.; Herlemann, A.; Kretschmer, A.; Ledderose, S.T. Feasibility of Different Tumor Delineation 18F-PSMA-1007 Approaches PET/CT Imaging for in Prostate Cancer Patients. Front. Oncol. 2021, 11, 663631. [Google Scholar] [CrossRef] [PubMed]
- Lau, Y.C.; Chen, S.; Ho, C.L.; Cai, J. Reliability of gradient-based segmentation for measuring metabolic parameters influenced by uptake time on 18F-PSMA-1007 PET/CT for prostate cancer. Front. Oncol. 2022, 12, 897700. [Google Scholar] [CrossRef] [PubMed]
- Trägårdh, E.; Enqvist, O.; Ulén, J.; Jögi, J.; Bitzén, U.; Hedeer, F.; Valind, K.; Garpered, S.; Hvittfeldt, E.; Borrelli, P. Freely available, fully automated ai-based analysis of primary tumour and metastases of prostate cancer in whole-body [18f]-psma-1007 pet-ct. Diagnostics 2022, 12, 2101. [Google Scholar] [CrossRef]
- Johnbeck, C.B.; Knigge, U.; Loft, A.; Berthelsen, A.K.; Mortensen, J.; Oturai, P.; Langer, S.W.; Elema, D.R.; Kjaer, A. Head-to-head comparison of 64Cu-DOTATATE and 68Ga-DOTATOC PET/CT: A prospective study of 59 patients with neuroendocrine tumors. J. Nucl. Med. 2017, 58, 451–457. [Google Scholar] [CrossRef]
- Mirzaei, S.; Revheim, M.-E.; Raynor, W.; Zehetner, W.; Knoll, P.; Zandieh, S.; Alavi, A. 64Cu-DOTATOC PET-CT in patients with neuroendocrine tumors. Oncol. Ther. 2020, 8, 125–131. [Google Scholar] [CrossRef]
- Delpassand, E.S.; Ranganathan, D.; Wagh, N.; Shafie, A.; Gaber, A.; Abbasi, A.; Kjaer, A.; Tworowska, I.; Núñez, R. 64Cu-DOTATATE PET/CT for imaging patients with known or suspected somatostatin receptor–positive neuroendocrine tumors: Results of the first US prospective, reader-masked clinical trial. J. Nucl. Med. 2020, 61, 890–896. [Google Scholar] [CrossRef]
- Cai, Z.; Anderson, C.J. Chelators for copper radionuclides in positron emission tomography radiopharmaceuticals. J. Label. Compd. Radiopharm. 2014, 57, 224–230. [Google Scholar] [CrossRef]
- Han, X.-D.; Liu, C.; Liu, F.; Xie, Q.-H.; Liu, T.-L.; Guo, X.-Y.; Xu, X.-X.; Yang, X.; Zhu, H.; Yang, Z. 64Cu-PSMA-617: A novel PSMA-targeted radio-tracer for PET imaging in gastric adenocarcinoma xenografted mice model. Oncotarget 2017, 8, 74159. [Google Scholar] [CrossRef] [PubMed]
- Grubmüller, B.; Baum, R.P.; Capasso, E.; Singh, A.; Ahmadi, Y.; Knoll, P.; Floth, A.; Righi, S.; Zandieh, S.; Meleddu, C. 64Cu-PSMA-617 PET/CT imaging of prostate adenocarcinoma: First in-human studies. Cancer Biother. Radiopharm. 2016, 31, 277–286. [Google Scholar] [CrossRef]
- Carlsen, E.A.; Johnbeck, C.B.; Binderup, T.; Loft, M.; Pfeifer, A.; Mortensen, J.; Oturai, P.; Loft, A.; Berthelsen, A.K.; Langer, S.W. 64Cu-DOTATATE PET/CT and prediction of overall and progression-free survival in patients with neuroendocrine neoplasms. J. Nucl. Med. 2020, 61, 1491–1497. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, E.A.; Johnbeck, C.B.; Loft, M.; Pfeifer, A.; Oturai, P.; Langer, S.W.; Knigge, U.; Ladefoged, C.N.; Kjaer, A. Semiautomatic tumor delineation for evaluation of 64Cu-DOTATATE PET/CT in patients with neuroendocrine neoplasms: Prognostication based on lowest lesion uptake and total tumor volume. J. Nucl. Med. 2021, 62, 1564–1570. [Google Scholar] [CrossRef]
- Carlsen, E.A.; Lindholm, K.; Hindsholm, A.; Gæde, M.; Ladefoged, C.N.; Loft, M.; Johnbeck, C.B.; Langer, S.W.; Oturai, P.; Knigge, U. A convolutional neural network for total tumor segmentation in [64Cu] Cu-DOTATATE PET/CT of patients with neuroendocrine neoplasms. EJNMMI Res. 2022, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Danieli, R.; Milano, A.; Gallo, S.; Veronese, I.; Lascialfari, A.; Indovina, L.; Botta, F.; Ferrari, M.; Cicchetti, A.; Raspanti, D. Personalized Dosimetry in Targeted Radiation Therapy: A Look to Methods, Tools and Critical Aspects. J. Pers. Med. 2022, 12, 205. [Google Scholar] [CrossRef] [PubMed]
- James, S.S.; Bednarz, B.; Benedict, S.; Buchsbaum, J.C.; Dewaraja, Y.; Frey, E.; Hobbs, R.; Grudzinski, J.; Roncali, E.; Sgouros, G. Current status of radiopharmaceutical therapy. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 891–901. [Google Scholar] [CrossRef]
- Sgouros, G.; Bodei, L.; McDevitt, M.R.; Nedrow, J.R. Radiopharmaceutical therapy in cancer: Clinical advances and challenges. Nat. Rev. Drug Discov. 2020, 19, 589–608. [Google Scholar] [CrossRef]
- Alam, M.R.; Singh, S.B.; Thapaliya, S.; Shrestha, S.; Deo, S.; Khanal, K. A Review of 177Lutetium-PSMA and 225Actinium-PSMA as Emerging Theranostic Agents in Prostate Cancer. Cureus 2022, 14, e29369. [Google Scholar] [CrossRef]
- Rathke, H.; Flechsig, P.; Mier, W.; Bronzel, M.; Mavriopoulou, E.; Hohenfellner, M.; Giesel, F.L.; Haberkorn, U.; Kratochwil, C. Dosimetry estimate and initial clinical experience with 90Y-PSMA-617. J. Nucl. Med. 2019, 60, 806–811. [Google Scholar] [CrossRef]
- Uccelli, L.; Boschi, A.; Cittanti, C.; Martini, P.; Panareo, S.; Tonini, E.; Nieri, A.; Urso, L.; Caracciolo, M.; Lodi, L. 90Y/177Lu-DOTATOC: From preclinical studies to application in humans. Pharmaceutics 2021, 13, 1463. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.A.; Thomas, S.R.; Stubbs, J.B.; Stabin, M.G.; Hays, M.T.; Koral, K.F.; Robertson, J.S.; Howell, R.W.; Wessels, B.W.; Fisher, D.R. MIRD pamphlet no. 16: Techniques for quantitative radiopharmaceutical biodistribution data acquisition and analysis for use in human radiation dose estimates. J. Nucl. Med. 1999, 40, 37S–61S. [Google Scholar]
- Dewaraja, Y.K.; Frey, E.C.; Sgouros, G.; Brill, A.B.; Roberson, P.; Zanzonico, P.B.; Ljungberg, M. MIRD pamphlet no. 23: Quantitative SPECT for patient-specific 3-dimensional dosimetry in internal radionuclide therapy. J. Nucl. Med. 2012, 53, 1310–1325. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, M.; Celler, A.; Konijnenberg, M.W.; Eckerman, K.F.; Dewaraja, Y.K.; Sjögreen-Gleisner, K. MIRD pamphlet no. 26: Joint EANM/MIRD guidelines for quantitative 177Lu SPECT applied for dosimetry of radiopharmaceutical therapy. J. Nucl. Med. 2016, 57, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Bolch, W.E.; Bouchet, L.G.; Robertson, J.S.; Wessels, B.W.; Siegel, J.A.; Howell, R.W.; Erdi, A.K.; Aydogan, B.; Costes, S.; Watson, E.E. MIRD pamphlet no. 17: The dosimetry of nonuniform activity distributions—Radionuclide S values at the voxel level. J. Nucl. Med. 1999, 40, 11S–36S. [Google Scholar]
- Bolch, W.E.; Eckerman, K.F.; Sgouros, G.; Thomas, S.R. MIRD pamphlet no. 21: A generalized schema for radiopharmaceutical dosimetry—Standardization of nomenclature. J. Nucl. Med. 2009, 50, 477–484. [Google Scholar] [CrossRef]
- Furhang, E.E.; Chui, C.S.; Sgouros, G. A Monte Carlo approach to patient-specific dosimetry. Med. Phys. 1996, 23, 1523–1529. [Google Scholar] [CrossRef]
- Brosch-Lenz, J.; Yousefirizi, F.; Zukotynski, K.; Beauregard, J.-M.; Gaudet, V.; Saboury, B.; Rahmim, A.; Uribe, C. Role of AI in Theranostics: Towards Routine Personalized Radiopharmaceutical Therapies. arXiv 2021, arXiv:2107.13913. [Google Scholar]
- Arabi, H.; AkhavanAllaf, A.; Sanaat, A.; Shiri, I.; Zaidi, H. The promise of artificial intelligence and deep learning in PET and SPECT imaging. Phys. Medica 2021, 83, 122–137. [Google Scholar] [CrossRef]
- Santoro, L.; Mora-Ramirez, E.; Trauchessec, D.; Chouaf, S.; Eustache, P.; Pouget, J.-P.; Kotzki, P.-O.; Bardiès, M.; Deshayes, E. Implementation of patient dosimetry in the clinical practice after targeted radiotherapy using [177Lu-[DOTA0, Tyr3]-octreotate. EJNMMI Res. 2018, 8, 103. [Google Scholar] [CrossRef]
- Hippeläinen, E.; Tenhunen, M.; Mäenpää, H.; Sohlberg, A. Quantitative accuracy of 177 Lu SPECT reconstruction using different compensation methods: Phantom and patient studies. EJNMMI Res. 2016, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Rydén, T.; Van Essen, M.; Marin, I.; Svensson, J.; Bernhardt, P. Deep-learning generation of synthetic intermediate projections improves 177Lu SPECT images reconstructed with sparsely acquired projections. J. Nucl. Med. 2021, 62, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Odland, A.; Server, A.; Saxhaug, C.; Breivik, B.; Groote, R.; Vardal, J.; Larsson, C.; Bjørnerud, A. Volumetric glioma quantification: Comparison of manual and semi-automatic tumor segmentation for the quantification of tumor growth. Acta Radiol. 2015, 56, 1396–1403. [Google Scholar] [CrossRef]
- Starmans, M.P.; van der Voort, S.R.; Tovar, J.M.C.; Veenland, J.F.; Klein, S.; Niessen, W.J. Radiomics: Data mining using quantitative medical image features. In Handbook of Medical Image Computing and Computer Assisted Intervention; Elsevier: Amsterdam, The Netherlands, 2020; pp. 429–456. [Google Scholar]
- van Heeswijk, M.M.; Lambregts, D.M.; van Griethuysen, J.J.; Oei, S.; Rao, S.-X.; de Graaff, C.A.; Vliegen, R.F.; Beets, G.L.; Papanikolaou, N.; Beets-Tan, R.G. Automated and semiautomated segmentation of rectal tumor volumes on diffusion-weighted MRI: Can it replace manual volumetry? Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Gudi, S.; Ghosh-Laskar, S.; Agarwal, J.P.; Chaudhari, S.; Rangarajan, V.; Paul, S.N.; Upreti, R.; Murthy, V.; Budrukkar, A.; Gupta, T. Interobserver variability in the delineation of gross tumour volume and specified organs-at-risk during IMRT for head and neck cancers and the impact of FDG-PET/CT on such variability at the primary site. J. Med. Imaging Radiat. Sci. 2017, 48, 184–192. [Google Scholar] [CrossRef]
- Uribe, C.; Peterson, A.; Van, B.; Fedrigo, R.; Carlson, J.; Sunderland, J.; Frey, E.; Dewaraja, Y.K. An international study of factors affecting variability of dosimetry calculations, part 1: Design and early results of the SNMMI dosimetry challenge. J. Nucl. Med. 2021, 62 (Suppl. S3), 36S–47S. [Google Scholar] [CrossRef]
- Jackson, P.; Hardcastle, N.; Dawe, N.; Kron, T.; Hofman, M.S.; Hicks, R.J. Deep learning renal segmentation for fully automated radiation dose estimation in unsealed source therapy. Front. Oncol. 2018, 8, 215. [Google Scholar] [CrossRef]
- Ryden, T.; van Essen, M.; Svensson, J.; Bernhardt, P. Deep learning-based SPECT/CT quantification of 177Lu uptake in the kidneys. J. Nucl. Med. 2020, 61, 1401. [Google Scholar]
- Nazari, M.; Jiménez-Franco, L.D.; Schroeder, M.; Kluge, A.; Bronzel, M.; Kimiaei, S. Automated and robust organ segmentation for 3D-based internal dose calculation. EJNMMI Res. 2021, 11, 53. [Google Scholar] [CrossRef]
- Tsougos, I.; Loudos, G.; Georgoulias, P.; Theodorou, K.; Kappas, C. Patient-specific internal radionuclide dosimetry. Nucl. Med. Commun. 2010, 31, 97–106. [Google Scholar] [CrossRef]
- Lee, M.S.; Hwang, D.; Kim, J.H.; Lee, J.S. Deep-dose: A voxel dose estimation method using deep convolutional neural network for personalized internal dosimetry. Sci. Rep. 2019, 9, 10308. [Google Scholar] [CrossRef] [PubMed]
- Götz, T.I.; Schmidkonz, C.; Chen, S.; Al-Baddai, S.; Kuwert, T.; Lang, E.W. A deep learning approach to radiation dose estimation. Phys. Med. Biol. 2020, 65, 035007. [Google Scholar] [CrossRef] [PubMed]
- Melodia, L. Deep Learning Estimation of Absorbed Dose for Nuclear Medicine Diagnostics. arXiv 2018, arXiv:1805.09108. [Google Scholar]
- Götz, T.I.; Lang, E.W.; Schmidkonz, C.; Kuwert, T.; Ludwig, B. Dose voxel kernel prediction with neural networks for radiation dose estimation. Z. Für Med. Phys. 2021, 31, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Akhavanallaf, A.; Shiri, I.; Arabi, H.; Zaidi, H. Whole-body voxel-based internal dosimetry using deep learning. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 670–682. [Google Scholar] [CrossRef]
- Li, Z.; Fessler, J.A.; Mikell, J.K.; Wilderman, S.J.; Dewaraja, Y.K. DblurDoseNet: A deep residual learning network for voxel radionuclide dosimetry compensating for single-photon emission computerized tomography imaging resolution. Med. Phys. 2022, 49, 1216–1230. [Google Scholar] [CrossRef]
- Vinjamuri, S.; Gilbert, T.; Banks, M.; McKane, G.; Maltby, P.; Poston, G.; Weissman, H.; Palmer, D.; Vora, J.; Pritchard, D. Peptide receptor radionuclide therapy with 90Y-DOTATATE/90Y-DOTATOC in patients with progressive metastatic neuroendocrine tumours: Assessment of response, survival and toxicity. Br. J. Cancer 2013, 108, 1440–1448. [Google Scholar] [CrossRef]
- Wright, C.L.; Zhang, J.; Tweedle, M.F.; Knopp, M.V.; Hall, N.C. Theranostic imaging of Yttrium-90. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef]
- Elschot, M.; Lam, M.G.; van den Bosch, M.A.; Viergever, M.A.; de Jong, H.W. Quantitative monte carlo–based 90y spect reconstruction. J. Nucl. Med. 2013, 54, 1557–1563. [Google Scholar] [CrossRef]
- Dewaraja, Y.K.; Chun, S.Y.; Srinivasa, R.N.; Kaza, R.K.; Cuneo, K.C.; Majdalany, B.S.; Novelli, P.M.; Ljungberg, M.; Fessler, J.A. Improved quantitative 90Y bremsstrahlung SPECT/CT reconstruction with Monte Carlo scatter modeling. Med. Phys. 2017, 44, 6364–6376. [Google Scholar] [CrossRef]
- Xiang, H.; Lim, H.; Fessler, J.A.; Dewaraja, Y.K. A deep neural network for fast and accurate scatter estimation in quantitative SPECT/CT under challenging scatter conditions. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2956–2967. [Google Scholar] [CrossRef] [PubMed]
- Phan, V.C.; Ho, T.T.; Le, T.A.; Nguyen, D.T.; Nguyen, D.K.; Nguyen, H.H. A convolutional neural network for Y90 SPECT/CT scatter estimation. Nucl. Sci. Technol. 2021, 11, 9–13. [Google Scholar] [CrossRef]
- Lim, H.; Chun, I.Y.; Dewaraja, Y.K.; Fessler, J.A. Improved low-count quantitative PET reconstruction with an iterative neural network. IEEE Trans. Med. Imaging 2020, 39, 3512–3522. [Google Scholar] [CrossRef]
- Shao, W.; Rowe, S.P.; Du, Y. Artificial intelligence in single photon emission computed tomography (SPECT) imaging: A narrative review. Ann. Transl. Med. 2021, 9. [Google Scholar] [CrossRef]
- Pandit-Taskar, N.; Iravani, A.; Lee, D.; Jacene, H.; Pryma, D.; Hope, T.; Saboury, B.; Capala, J.; Wahl, R.L. Dosimetry in clinical radiopharmaceutical therapy of cancer: Practicality versus perfection in current practice. J. Nucl. Med. 2021, 62 (Suppl. S3), 60S–72S. [Google Scholar] [CrossRef] [PubMed]
- Guezennec, C.; Bourhis, D.; Orlhac, F.; Robin, P.; Corre, J.-B.; Delcroix, O.; Gobel, Y.; Schick, U.; Salaün, P.-Y.; Abgral, R. Inter-observer and segmentation method variability of textural analysis in pre-therapeutic FDG PET/CT in head and neck cancer. PLoS ONE 2019, 14, e0214299. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Abdalah, M.; Ashrafinia, S.; Beukinga, J.; Bogowicz, M.; Dinh, C.; Götz, M.; Hatt, M.; Leijenaar, R.; Lenkowicz, J. Results from the image biomarker standardisation initiative. Radiother. Oncol. 2018. [Google Scholar] [CrossRef]
- Jha, A.K.; Bradshaw, T.J.; Buvat, I.; Hatt, M.; Prabhat, K.; Liu, C.; Obuchowski, N.F.; Saboury, B.; Slomka, P.J.; Sunderland, J.J. Nuclear medicine and artificial intelligence: Best practices for evaluation (the RELAINCE guidelines). J. Nucl. Med. 2022, 63, 1288–1299. [Google Scholar] [CrossRef]
- Babak, S. Artificial Intelligence in Nuclear Medicine: Opportunities, Challenges, and Responsibilities Toward a Trustworthy Ecosystem. J. Nucl. Med. 2023, 64, 188–196. [Google Scholar] [CrossRef]
- Afshar, P.; Mohammadi, A.; Plataniotis, K.N.; Oikonomou, A.; Benali, H. From handcrafted to deep-learning-based cancer radiomics: Challenges and opportunities. IEEE Signal Process. Mag. 2019, 36, 132–160. [Google Scholar] [CrossRef]
- Dewaraja, Y.K.; Mirando, D.M.; Peterson, A.; Niedbala, J.; Millet, J.D.; Mikell, J.K.; Frey, K.; Wong, K.K.; Wilderman, S.; Nelson, A.S. A pipeline for automated voxel dosimetry: Application in patients with multi-SPECT/CT imaging following 177Lu peptide receptor radionuclide therapy. J. Nucl. Med. 2022, 63, 1665–1672. [Google Scholar] [CrossRef] [PubMed]
- Björnsson, B.; Borrebaeck, C.; Elander, N.; Gasslander, T.; Gawel, D.R.; Gustafsson, M.; Jörnsten, R.; Lee, E.J.; Li, X.; Lilja, S. Digital twins to personalize medicine. Genome Med. 2020, 12, 4. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Boussard, T.; Macklin, P.; Greenspan, E.J.; Gryshuk, A.L.; Stahlberg, E.; Syeda-Mahmood, T.; Shmulevich, I. Digital twins for predictive oncology will be a paradigm shift for precision cancer care. Nat. Med. 2021, 27, 2065–2066. [Google Scholar] [CrossRef] [PubMed]
- Rahmim, A.; Brosch-Lenz, J.; Fele-Paranj, A.; Yousefirizi, F.; Soltani, M.; Uribe, C.; Saboury, B. Theranostic digital twins for personalized radiopharmaceutical therapies: Reimagining theranostics via computational nuclear oncology. Front. Oncol. 2022, 12, 1062592. [Google Scholar] [CrossRef]
- Rahmim, A.; Bradshaw, T.J.; Buvat, I.; Dutta, J.; Jha, A.K.; Kinahan, P.E.; Li, Q.; Liu, C.; McCradden, M.D.; Saboury, B. Issues and Challenges in Applications of Artificial Intelligence to Nuclear Medicine--The Bethesda Report (AI Summit 2022). arXiv 2022, arXiv:2211.03783. [Google Scholar]
- Abdollahi, H.; Rahmim, A. Digital Twins for Personalized Healthcare: Application to Radiopharmaceutical Therapies. Front. Biomed. Technol. 2022, 10, 1–5. [Google Scholar] [CrossRef]
- Brosch-Lenz, J.; Uribe, C.; Rahmim, A.; Saboury, B. Theranostic Digital Twins: An indispensable prerequisite for personalized cancer care. J. Nucl. Med. 2022, 64, 501. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Therapeutic Radioisotopes | Diagnostic Radioisotopes-Pharmaceuticals | |
|---|---|---|
| SSTRs Target/NET | PSMA Target/mCRPC | |
| 177Lu | [68Ga]Ga-DOTA-TATE PET | [68Ga]Ga-PSMA-617 PET |
| [68Ga]Ga-DOTA-TOC PET | [68Ga]Ga-PSMA-I&T PET | |
| [68Ga]Ga-PSMA-11 PET | ||
| [64Cu]Cu-DOTA-TATE PET | [64Cu]Cu-PSMA-617 PET | |
| [64Cu]Cu-DOTA-TOC PET | ||
| No Clinical Match | [18F]PSMA-617 PET | |
| No Clinical Match | [44Sc]Sc-PSMA-617 PET | |
| 225Ac | [177Lu]Lu-DOTA-TATE SPECT | [177Lu]Lu-PSMA-617 SPECT |
| [177Lu]Lu-DOTA-TOC SPECT | ||
| 90Y | [177Lu]Lu-DOTA-TATE SPECT | [177Lu]Lu-PSMA-617 SPECT |
| [177Lu]Lu-DOTA-TOC SPECT | [177Lu]Lu-J591 SPECT | |
| [111In]In-DOTA-TATE SPECT | [111In]In-J591 SPECT | |
| [111In]In-DOTA-TOC SPECT | ||
| # | First Author, Year [Ref] | Radiopharmaceutical, Modality | # Pats | Site | Utility | Feature Class | Stats, ML/DL Algorithms | Software | Finding RFs | Result | Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Grubmüller et al., 2018 [39] | [68Ga]Ga-PSMA-11 PET/CT | 38 | 77 primary prostate and metastatic LNs, bone and visceral metastases | OS prediction | First order (shape and intensity) | Unavailable Cox proportional hazards model, KM, and Cohen’s kappa (κ) | Hermes Hybrid3D (Hermes Medical Solutions, Stockholm) | TTV | TTV was significantly associated with OS, and its changes were significantly associated with PSA response (p = 0.58), contrary to SUVmean changes (p = 0.15) | PSMA-TTV is a promising tool for RPT response evaluation |
| 2 | Khurshid et al., 2018 [40] | [68Ga]Ga-PSMA-11 PET/CT | 70 | 118 primary prostate and metastatic LNs, bone and liver metastases | Therapy response prediction | First order (intensity)/second order (texture) | Spearman correlation | NM | NGLCM (Entropy and homogeneity) | Entropy (r = -0.327) and homogeneity (r = 0.315) TFs of bone lesions correlated with ∆PSA | Better treatment response for more heterogeneous lesions |
| 3 | Acar et al., 2019 [41] | [68Ga]Ga-PSMA-11 PET/CT | 75 | 257 metastatic bone lesions | Therapy response prediction | First order (shape and intensity)/second order (texture) | Decision tree, discriminant analysis, SVM, KNN, and ensemble classifier | LIFEx | GLZLM_SZHGE and histogram-based kurtosis | Weighted KNN achieved the best classification performance with AUC = 0.76 (ACU = 73.5%, SE = 73.5%, SP = 73.7%) | Metastatic or responded sclerotic bone lesions discrimination using CT texture analysis and ML |
| 4 | Seifert et al., 2020 [42] | [68Ga]Ga-PSMA-11 PET/CT | 110 | 136 metastatic LNs, bone and visceral (liver, lung, and pleura) lesions | OS prediction/restaging/Seg | First order (shape and intensity)/ | Univariate and multivariate regression, Spearman correlation, and Mann–Whitney U tests | MIWBAS, V.1.0, Siemens | PSMA-TV | Lesion number (HR = 1.255), PSMA-TV (HR =1.299), and PSMA-TLQ (HR = 1.326) prognosticators of OS | - Baseline PSMA-PET TV was a significant negative prognosticator of OS in prostate cancer before RPT - In comparison with PSMA-TV, PSMA-TLQ was an independent and superior prognosticator of OS |
| 5 | Widjaja et al., 2021 [43] | [68Ga]Ga-PSMA-11 PET/CT | 71 | 208 primary prostate and metastatic LNs, bone, liver, and soft tissue lesions | Biochemical response prediction | First order (shape and intensity) | Kruskal–Wallis, Fisher’s exact, and KM | syngo.via; V50B; Siemens | SUVmax | SUVmax was an independent predictor for early PSA response in the treatment course | Higher PSMA expression was related to a better early biochemical response |
| 6 | Gafita et al., 2021 [44] | [68Ga]Ga-PSMA-11 PET/CT | 414 | 463 metastatic LNs, bone, and liver lesions | OS and PFS prediction | First order (intensity) | LASSO, Wilcoxon, and Mann–Whitney | qPSMA V.1.0 | SUVmean | PSM SUV: correlated significantly with tumor PSMA expression | - Higher PSMA expression correlated with longer OS and PSA-PFS - Patients with metastatic bone disease had shorter OS and PSA-PFS |
| 7 | Khreish et al., 2021 [45] | [68Ga]Ga-PSMA-11 PET/CT | 51 | 322 primary prostate and metastatic LNs, bone, liver, and soft tissue lesions | PFS prediction | First order (intensity) | KM, Cox proportional-hazards modeling, Spearman, and Cohen’s κ | NM | TLR | ΔTLR and ΔSUV significantly correlated with ΔPSA. Univariate analysis: SUVpeak failed to predict survival Multivariable analysis: TLR was independently associated with PFS | TLR (normalization of the total lesion PSMA over healthy liver tissue uptake) biomarker can be a predictor of PFS in RPT |
| 8 | Moazemi et al., 2021 [46] | [68Ga]Ga-PSMA-11 PET/CT | 83 | 2070 primary prostate and metastatic lesions | Therapy response prediction | First order (intensity)/second order (texture) | 5 ML classifiers (linear, RBF, and polynomial kernel SVMs), ET, and random forest) | InterView Fusion (V. 3.08.005) | Task I: PET (Min and Correlation) and CT (Min, Coarseness, and Busyness) | Strong correlations between ML SVM classifier (RBF kernel) on a selection of RFs and clinical parameters with ΔPSA (with AUC = 80%, SE = 75%, and SP = 75%) | RFs were superior to clinical parameters in terms of correlation with ΔPSA |
| 9 | Moazemi et al., 2021 [47] | [68Ga]Ga-PSMA-11 PET/CT | 100 | 2067 pathological hotspots | Therapy response prediction/auto Seg | First order (shape and intensity)/second order (texture) | UNet and 6 ML classifiers (logistic regression, SVM (linear, polynomial, RBF kernels), ET, and random forest) | PyRadiomics Library | 14 features from both PET and CT modalities | Seg. task (0.88 precision, 0.77 recall, and 0.82 Dice). In predicting the response task, logistic regression performed the best (with AUC = 0.73, SE = 0.81, and SP = 0.58) | In 177Lu-PSMA RPT, the facilitated automated decision support tool has an assistant potential for patient screening |
| 10 | Moazemi et al., 2021 [48] | [68Ga]Ga-PSMA-11 PET/CT | 83 | 2070 primary prostate and metastatic lesions | OS prediction/restaging | First order (shape and intensity)/second order (texture) | LASSO regression and KM estimator | InterView Fusion (V. 3.08.005) | PET kurtosis and SUVmin | The relevant RFs significantly correlated with OS (r = 0.2765, p = 0.0114) | 68Ga-PSMA-PET/CT scans and patient-specific clinical parameters have the potential for the prediction of OS in advanced PC patients under 177Lu-PSMA RPT |
| 11 | Roll et al., 2021 [49] | [68Ga]Ga-PSMA-11 PET/MRI | 21 | 49 metastatic lesions in bone, LNs, liver, and lung | Biochemical response and OS prediction | First order (intensity) | KM analysis and log-rank test | 3D slicer, V.4.11.2 | T2-weighted (interquartile range) | The logistic regression model revealed the highest accuracy (AUC = 0.83) | There was a high survival for patients with a biochemical response and higher T2 interquartile range values |
| 12 | Rosar et al., 2022 [50] | [68Ga]Ga-PSMA-11 PET/CT | 66 | 139 metastatic lesions in bone, LNs, liver, and other soft tissue | OS prediction | First order (shape and intensity) | Spearman’s rank correlation and KM | Syngo. Via (Enterprise VB 40B, Siemens, Erlangen, Germany) | TLP | There was a strong correlation between ∆PSA and ∆TLP (r = 0.702) | TLP (summed products of volume × uptake (SUVmean) of all lesions) biomarker independently and strongly predicted OS |
| 13 | Gafita et al., 2022 [51] | [68Ga]Ga-PSMA-11 PET/CT | 406 | normal liver, spleen, salivary gland and kidney, and metastatic lesions in bone, LNs, and visceral organs | Therapy response prediction/restaging | First order (shape and intensity) | Spearman CC and Kruskal–Wallis testing | qPSMA | PSMA-VOL | Salivary glands, kidneys, and liver: a moderate and negative correlation between PSMA-VOL and SUVmean Spleen: a weak correlation between PSMA-VOL and SUVmean | Decreasing the activity concentration in OARs due to the tumor sequestration affecting the biodistribution of 68Ga-PSM showed the tumor sink effect |
| 14 | Hartrampf et al., 2022 [52] | [68Ga]Ga-PSMA-11 PET/CT | 65 | 144 primary prostate and metastatic bone, LNs, liver, and lung lesion | Therapy response assessment | First order (shape and intensity) | Shapiro–Wilk tests and Spearman’s rank CC | FIJI (ImageJ) | ΔPSMA-TV | ΔPSA was correlated with ΔSUVmaxall (r = 0.51), ΔPSMA-TVall (r ≥ 0.59), ΔPSMA-TV10 (r ≥ 0.57), and ΔPSMA-TV5 (r ≥ 0.53) | The RPT response assessment was possible through PSMA-TV |
| 15 | Pathmanandav et al., 2022 [53] | [68Ga]Ga-PSMA-11 PET/CT/[18F]FDG PET/CT | 56 | 92 metastatic lesions in bone, LNs, and visceral organs | Therapy response prediction | First order (shape and intensity) | KM, Cox proportional-hazards regression, logistic regression, and LASSO | MIM | PSMA_TV and SUVmean | PSMA SUVmean was an independent predictor of treatment response, but SUVmax was not | A higher SUVmean correlated with treatment response, but a higher PSMA_TV was associated with worse OS |
| 16 | Giesel et al., 2017 [54] | [18F]FDG PET/CT, [68Ga]Ga-PSMA-11 PET/CT, and [68Ga]Ga-DOTA-TOC PET/CT | 148 (40 PCa) | 254 metastatic LNs | Restaging | First order (shape and intensity) | 2-sided paired-sample t-test, 2-sided Wilcoxon signed-rank testing | In-house (developed at the Fraunhofer Institute for Medical Image Computing) | PET (SUVmax) CT (short-axis diameter (SAD) and Histogram) | CT densities correlated with the PET uptake (with a 7.5 HU threshold to discriminate between malignant and benign LNs infiltration) and 20 HU to exclude benign LN | CT density measurements and PET uptake analysis increased the differentiation between malignant and benign LN |
| 17 | Moazemi et al., 2020 [55] | [68Ga]Ga-PSMA-11 PET/CT | 72 | 2419 hotspots in normal kidney, bladder and salivary glands, and metastatic lesions | Restaging | First order (shape and intensity)/second order (texture) | 5 ML classifiers (SVM (linear, RBF, and polynomial kernels), ET, and random forest) | InterView FUSION (V3.08.005) | PET (kurtosis; busyness, and coarseness) | AUC = 0.98, (SE = 0.94 and SP = 0.89) ET and RF showed the best results | Using ML and considering features from both the CT and PET images outperformed using either separately |
| 18 | Erle et al., 2021 [56] | [68Ga]Ga-PSMA-11 PET/CT | 87 | 2452 hotspots in normal liver, kidney, lacrimal and salivary glands, and metastatic lesions | Restaging | First order (intensity)/second order (texture) | SVM (linear kernel), ET, and random forest | InterView FUSION | 77 RFs | The ET classifier resulted in (AUC = 0.95, SE = 0.95, and SP = 0.80) | Combining manual and ML-based diagnoses has the potential to predict hotspot labels with high sensitivity |
| 19 | Hinzpeter et al., 2021 [57] | [68Ga]Ga-PSMA-11 PET/CT | 67 | 205 bone metastases | Restaging | First order (intensity)/ second order (texture) | Gradient-boosted tree | 3D Slicer, V.4.11 | 11 most important and independent features2 | Model classification AUC = 0.85 (with SE = 78% and SP = 93%) | The distinction of healthy bone from metastatic bone accurately using PET/CT texture analysis and ML |
| 20 | Hammes et al., 2018 [58] | [68Ga]Ga-PSMA-11 PET/CT | 38 | 100 metastatic bone lesions | Staging/therapy response prediction/Seg | First order (intensity) | Linear regression and ANOVA | NA | SUVmax and SUVmean | SUVmax, r2 = 0.97; SUVmean, r2= 0.88; lesion count, r2 = 0.97; HU threshold: not significant | EBONI has the potential to semi-automatically quantify TVs in PSMA PET/CT in a fast (3 min per scan), robust, and reproducible manner |
| 21 | Zhao et al., 2019 [59] | [68Ga]Ga-PSMA-11 PET/CT | 193 | 1756 primary prostate and metastatic lesions in bone and LNs | Staging/restaging/Seg | NA | 2.5DU-Net | NA | NA | Bone lesion detection (precision = 99%, recall = 99%, and F1 score = 99%), LN lesion detection (precision = 94%, recall = 89%, and F1 score = 92%) | CNN has the potential to automatically segment disease sites on 68Ga-PSMA PET/CT images to confirm whether a voxel is a lesion or not |
| 22 | Seifert et al., 2020 [60] | [68Ga]Ga-PSMA-11 PET/CT | 40 | 100 metastatic lesions in the bone, LNs, liver, and lung | Seg/OS prediction | First order (shape and intensity) | Seg: GAN t-tests, log-rank tests, Cox regression, ICC, Pearson correlation | MIWBAS, V.1.0 | PET_TV50 | PSMATV50: R2 = 1.000 and SUVmax: R2 = 0.988 | PSMATV50 was a significant predictor of OS |
| 23 | Xue et al., 2020 [61] | [68Ga]Ga-PSMA-11 PET/CT | 30 | Main organs and tumor lesions | Dose prediction | NA | GAN | NA | NA | The dual-input-model is able to synthesize dose maps with MAPE of 18.94% ± 5.65% | AI is capable of estimating voxel-wise posttherapy dosimetry both qualitatively and quantitatively |
| 24 | Xue et al., 2021 [62] | [68Ga]Ga-PSMA-11 PET/CT | 34 | Main organs and tumor lesions | Dose Prediction | NA | GAN | NA | NA | DVH: MAE = 21.2 ± 10.8% (=24.0 ± 10.0% without pre-training) to the ground truth | Using the PBRK model along with a pre-therapeutic PET/CT image may improve the development of AI for dose prediction |
| 25 | Xue et al., 2022 [63,64] | [68Ga]Ga-PSMA-11 PET/CT | 23 | WB, kidney, liver, spleen, and salivary gland | Dose prediction | First order (shape and intensity) | RFR and ANN | NA | SUVmax and TV | The dose prediction based on the literature population means had a significantly larger MAPE for each organ compared to the optimal ML methods Average prediction error for kidneys = 15.76% | It is possible to estimate the dose before RPT, which may support the treatment planning role |
| # | First Author, Year [Ref] | Radiopharmaceutical, Modality | # pats | Site | Utility | Feature Class | Stats, ML/DL Algorithms | Software | Finding RFs | Result | Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Werner et al., 2017 [65] | [68Ga]Ga-DOTA-TATE PET/CT | 142 | 872 primary tumors of GEP-NETs (pancreatic, stomach, and intestine), lung and metastatic lesions in LNs, bone, liver, and lung | OS and PFS prediction | First order (intensity)/second order (texture) | Cox multi-parametric regression, Youden index, and KM | Interview FUSION | Entropy, correlation, short zone emphasis and homogeneity | Eight statistically independent TFs for time-to-progression and time-to-death were identified with Cox analysis, among which it was entropy that predicted both PFS and OS | The prognostic performance of intratumoral TFs analysis outperformed conventional PET parameters |
| 2 | Werner et al., 2018 [66] | [68Ga]Ga-DOTA-TATE/DOTA-TOC PET/CT | 31 | 162 metastatic lesions in LNs, bone, liver, and lung | OS prediction | First order (intensity)/second order (texture) | Youden index, KM, multivariate Cox hazard analysis, and relative risks | Interview Fusion | Entropy | SUVmean/max was not able to prognosticate Entropy was a significant RF to distinct high- and low-risk groups | Unlike conventional PET parameters, higher entropy (a texture feature) values were associated with more prolonged survival |
| 3 | Önner et al., 2020 [67] | [68Ga]Ga-DOTA-TATE PET/CT | 22 | 326 primary tumors of the pancreas, stomach, intestine, and metastatic lesions in LNs, bone, liver, and lung | Treatment response prediction | First order (intensity)/second order (texture) | Kolmogorov–Smirnov, Mann–Whitney U, and Youden index | LIFEx | Skewness and kurtosis | AUC: for skewness and kurtosis (0.619 and 0.518, resp.) | Skewness and kurtosis predicted PRRT response |
| 4 | Weber et al., 2020 [68] | [68Ga]Ga-DOTA-TOC PET/MRI | 9 PRRT | 80 metastatic liver lesions | Treatment response prediction | First order (intensity)/second order (texture) | Mann–Whitney test | LIFEx | ADC maps (lesion vol and entropy) | No PET parameter values predicted PRRT response In the treatment responders group: a significant decrease in ADCmaps_lesion volumes and ADCmaps_entropy | No parameters of PET or ADC maps predicted PRRT response. However, the study sample size was small, so further research is suggested |
| 5 | Ortega et al., 2021 [69] | [68Ga]Ga-DOTA-TATE PET/CT | 91 | 872 primary tumors of GEP-NETs (pancreatic, intestine, and stomach), lung and metastatic lesions in LNs, bone, liver, and lung | PFS prediction | First order (intensity)/second order (texture) | 2-sided Wilcoxon rank sum test and Cox proportional hazards model | PACS system with fusion software (Mirada Medical) | Multivariate analysis: mean SUVmax and mean lesion SUVmax/liver SUVmax | Significantly higher mean SUVmax in responders than that in non-responders A higher mean SUVmax and mean SUVmax tumor-to-liver ratio was associated with therapy response - Higher kurtosis values were observed in non-responders than in responders (mean 8.6 vs. 5.8) | SSTR expression and tumor heterogeneity metrics associated with PFS |
| 6 | Atkinson et al., 2021 [70] | [68Ga]Ga-DOTA-TATE PET/CT | 44 | GEP-NETs primary tumors (pancreatic, stomach, intestine), lung, thyroid and phaeochromocytoma/paraganglioma and metastatic lesions in LNs, bone, liver, lung, peritoneum, and brain | OS and PFS prediction | First order (intensity)/second order (texture) | Univariate KM and multivariate Cox regression | TexRAD, Cambridge, UK | CT-coarse kurtosis, PET_entropy, and PET_skewness | SUVmax and SUVmean were not significant in outcome prediction Higher kurtosis, higher entropy, and lower skewness: predict shorter PFS CT-TA (coarse kurtosis): independently predicates PFS (HR = 2.57 and CI = 1.22–5.38) PET-TA (unfiltered skewness): independently predicates OS (HR = 9.05, 95% CI = 1.19–68.91) | Texture analysis yielded prognostic biomarkers that had the potential to assess outcomes in NETs patients with more aggressive diseases |
| 7 | Liberini et al., 2021 [71] | [68Ga]Ga-DOTA-TATE PET/CT and [18F]FDG PET/CT | 2 | 22 metastatic lesions in LNs, bone, and liver | Prognosis prediction | First order (intensity)/second order (texture) | Mann–Whitney, Pearson correlation matrix, and PCA | LIFE xV.5.10 (IMIV/CEA, Orsay, France) | TLSREwb-50 and SRETVwb-50 | Mann–Whitney test: 28 RFs showed significant differences between the two patients Pearson correlation matrix: identified seven second-order RFs, with poor correlation with SUVmax and PET vol. | Defining inter-patient heterogeneity and therapy response prediction may be possible using RFs |
| 8 | Laudicella et al., 2022 [72] | [68Ga]Ga-DOTA-TOC PET/CT | 38 | 324 metastatic lesions in LNs, bone, liver, and other soft tissues | Treatment response prediction | First order (intensity)/second order (texture) | t-test, Mann– Whitney U, and Youden index | LIFEx | HISTO_Skewness and HISTO_Kurtosis | HISTO_Skewness and HISTO_Kurtosis: able to predict the response (AUC ROC, SE., and SP. of 0.745, 80.6%, 67.2% and 0.722, 61.2%, 75.9%, resp.) SUVmax was not able to predict the response (AUC= 0.523) | The developed theragnomics (THERAGNOstics + radiOMICS) predictive model was superior to conventional quantitative parameters to predict the GEP-NET lesion’s response to 177Lu-DOTA-TOC PRRT |
| 9 | Giesel et al., 2017 [54] | [18F]FDG PET/CT, [68Ga]Ga-PSMA-11 PET/CT, and [68Ga]Ga-DOTA-TOC PET/CT | 148 (35 GEP-NET) | 217 metastatic LNs | Restaging | First order (shape and intensity) | 2-sided paired-sample t-testing, 2-sided Wilcoxon signed-rank testing | In-house (developed at the Fraunhofer Institute for Medical Image Computing) | PET (SUVmax), CT (short-axis diameter (SAD) and histogram) | CT densities correlated with the PET uptake (with a 7.5 HU threshold to discriminate between malignant and benign LNs infiltration and 20 HU to exclude benign LN) | CT density measurements and PET uptake analysis increased the differentiation between malignant and benign LNs |
| 10 | Liberini et al., 2021 [73] | [68Ga]Ga-DOTA-TOC PET/CT | 49 | 60 primary tumors of GEP-NETs (pancreatic, stomach, intestine) and metastatic lesions in LNs, liver, and other soft tissues | Prognosis prediction/seg./restaging | First order (intensity)/second order (texture) | Pearson’s CCs, DSC, ICC, and coefficient of variance | LifeX V.4.81 (IMIV/CEA, Orsay, France) | GLZLM (also called GLSZM) features and zones with low gray-level (SZLGE and LZLGE), and SUVmax thresh. of 40% | SAEB seg. and operators: DSC mean= 0.75 ± 0.11 (0.45–0.92), SAEB seg. and 4 manual segs.= 0.78 ± 0.09 (0.36–0.97) | Superior RFs stability among operators was provided using SUVmax thresholds of 40% but led to a possible biological information loss SAEB performed better than manual segmentation; however, further validation is suggested |
| 11 | Wehrend et al., 2021 [74] | [68Ga]Ga-DOTA-TATE PET/CT | 125 | 223 liver lesions | Seg | NA | CNN: 2D U-Net Stats: F1 score | MIM (V. 7.03) | NA | Highest precision-recall AUC (0.73 ± 0.03): using a noise filter (15-pixel) Highest mean PPV (0.94 ± 0.01): 20-pixel filter Highest mean F1 score (0.79 ± 0.01): 20-pixel filter Highest mean SE. (0.74 ± 0.02): 5-pixel filter | DNN can automatically facilitate the detection of hepatic metastases For further validation, it suggested the need for more studies with larger sample sizes |
| 12 | Akhavanallaf et al., 2023 [75] | [68Ga]Ga-DOTA-TATE PET/CT | 25 | 90 NETs: 75 liver, 11 LNs, 3 primary pancreas tumors, and 1 chest tumor | Dose prediction | First order (shape and intensity) | Spearman rank correlation, univariate linear regression model, ElasticNet and permutation-based RF variable-importance feature selection | NM | SUVmean, TLSUVmean (SUVmean of total-lesion-burden), and SUVpeak | Tumor dose prediction using an optimal trivariate RF model composed of SUVmean, TLSUVmean, and total liver SUVmean: R2 = 0.64, MAE = 0.73 Gy/GBq, and MRAE = 0.20 | PET-based metrics combined with ML models can improve dose prediction, which may be useful for stratifying patients and personalizing treatment |
| 13 | Plachouris et al., 2023 [76] | [68Ga]Ga-DOTA-TOC PET/CT | 20 | 3412 features from 4 OARs (liver, spleen, and left- and right kidneys) | Dose prediction | First order (intensity)/second order (texture) + dosiomic features | Multivariate analysis and nine supervised linear and non-linear-based ML regression algorithms: linear, ridge, extra tree, AdaBoost, gradient boost, random forest, decision tree, SVR, and XGBoost regression algorithms trained for every OAR | PyRadiomics Library | Differed for each OAR (Table 3 in [76]) | Wavelet-based features had highly correlated predictive value More precise prediction using non-linear-based ML regression algorithms than linear-based ones | The combination of radiomics and dosiomics may be useful for individualized molecular radiotherapy response assessment and OAR dose prediction |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yazdani, E.; Geramifar, P.; Karamzade-Ziarati, N.; Sadeghi, M.; Amini, P.; Rahmim, A. Radiomics and Artificial Intelligence in Radiotheranostics: A Review of Applications for Radioligands Targeting Somatostatin Receptors and Prostate-Specific Membrane Antigens. Diagnostics 2024, 14, 181. https://doi.org/10.3390/diagnostics14020181
Yazdani E, Geramifar P, Karamzade-Ziarati N, Sadeghi M, Amini P, Rahmim A. Radiomics and Artificial Intelligence in Radiotheranostics: A Review of Applications for Radioligands Targeting Somatostatin Receptors and Prostate-Specific Membrane Antigens. Diagnostics. 2024; 14(2):181. https://doi.org/10.3390/diagnostics14020181
Chicago/Turabian StyleYazdani, Elmira, Parham Geramifar, Najme Karamzade-Ziarati, Mahdi Sadeghi, Payam Amini, and Arman Rahmim. 2024. "Radiomics and Artificial Intelligence in Radiotheranostics: A Review of Applications for Radioligands Targeting Somatostatin Receptors and Prostate-Specific Membrane Antigens" Diagnostics 14, no. 2: 181. https://doi.org/10.3390/diagnostics14020181
APA StyleYazdani, E., Geramifar, P., Karamzade-Ziarati, N., Sadeghi, M., Amini, P., & Rahmim, A. (2024). Radiomics and Artificial Intelligence in Radiotheranostics: A Review of Applications for Radioligands Targeting Somatostatin Receptors and Prostate-Specific Membrane Antigens. Diagnostics, 14(2), 181. https://doi.org/10.3390/diagnostics14020181