Abstract
Coccidioidomycosis, caused by Coccidioides immitis and C. posadasii, causes significant morbidity and mortality, both in immunocompetent and immunocompromised people, mainly in endemic areas. The present work analyzed its epidemiology, diagnostic methods, and treatment by reviewing clinical cases published from 1950 to 2021. Fifty-nine articles were included, corresponding to 275 clinical cases. The results showed a higher incidence of coccidioidomycosis in the male gender than the female gender. The most affected age group was 31–40 years, and the most reported clinical presentation was disseminated with greater involvement in cutaneous and subcutaneous tissue, followed by the CNS, bone system, and peritoneum. The species most frequently reported was C. immitis. The most used treatment was azoles, followed by their combination with amphotericin B, monotherapy with amphotericin B, and alternative medicine. This work shows that epidemiological data outside the USA are still scarce. Serological tests are the preferred diagnostic method in daily medical practice, and cultures remain the gold standard. The treatment for coccidioidomycosis is ketoconazole and amphotericin B, individually or in combination.
1. Introduction
Coccidioidomycosis is a disease caused by the fungi Coccidioides immitis and C. posadasii and is considered endemic to the American continent. From an epidemiology standpoint, the most important areas include the southwestern United States, northern Mexico, Central America, and some parts of South America [1,2].
This mycosis causes significant morbidity and mortality, both in immunocompetent and immunocompromised people worldwide, mainly in endemic areas. Nevertheless, each region has specific epidemiological data. For instance, it has been shown that the incidence of coccidioidomycosis in the USA increased during the last two decades, both in endemic and non-endemic regions within the country. The Centers for Disease Control and Prevention (CDCs) reported a 58% increase in the incidence of coccidioidomycosis in Arizona from October 2017 to March 2018 compared to previous years, with California being the state with the highest reporting in 2017 [2]. However, it is worth noting that this disease does not require mandatory notification on the rest of the American continent, except Argentina. Therefore, data on the incidence of coccidioidomycosis are not accurate, and the information is limited to reports of disseminated or unusual clinical cases [1,2,3,4]. In Mexico, Coccidioides infection is considered to be as prevalent as in the endemic regions of the USA, with an average of 1500 cases reported per year, according to data reported from 1988 to 1994, where the mean incidence of coccidioidomycosis was 0.8 to 10.5 [1]. Still, this mycosis ceased to require mandatory notification as of 1994. Meanwhile, in Argentina, epidemiological studies have revealed the highest infection rates in the province of Catamarca (40%). Other areas with high infection rates are northwestern Córdoba (34%), the western part of Santiago del Estero (19.8%), and La Rioja (19.13%), which are neighboring provinces of Catamarca [5]. On the other hand, reports are scarce in Central American countries such as Guatemala and Honduras, even though the fungus has been noted. Likewise, in other South American countries, the incidence of this mycosis is unknown [1].
Typically, the infection begins when a susceptible host inhales the arthroconidia, considered the infective phase, present in the soil or air. Once in the host, they become spherules (parasitic phase) containing abundant endospores, and each of these can produce another spherule, thus remaining in the host [6].
Clinical forms. Coccidioidomycosis is divided into three categories: primary pulmonary form, progressive pulmonary form, and disseminated form. In primary pulmonary coccidioidomycosis, it is estimated that 60% of patients have asymptomatic infections that can only be detected by serological or skin tests when symptoms appear. Additionally, coccidioidomycosis infection’s primary respiratory signs and symptoms may be indistinguishable from those of common bacterial pneumonia. Likewise, in endemic regions, coccidioidal pneumonia can represent up to 29% of community-acquired pneumonia [7,8]. On the other hand, some patients may present with erythema nodosum or erythema multiforme, which are considered markers of favorable prognosis and occur more frequently in women [9]. Spontaneous regression of primary respiratory infections is also reported, even without antifungal treatment [10,11]. Progressive pulmonary coccidioidomycosis is generally chronic and develops after the first infection, the symptoms of which do not resolve after two months [12]. Disseminated coccidiomycosis is a rare clinical entity that develops in less than 5% of immunocompetent patients; however, dissemination is common in immunocompromised hosts, pregnant patients, and patients of African and Filipino ancestry. Furthermore, immunosuppression can be caused by different factors (administration of immunosuppressive drugs, organ transplants, cancer, chemotherapy, glucocorticoid administration, and AIDS), which can increase the possibility of acquiring severe forms of the infection. Another organ of dissemination most frequently related to it is the skin; in addition to the involvement of the central nervous system, this is the most serious form and occurs in 90% of these cases [13]. Meningitis is the most common clinical presentation; however, the musculoskeletal system, lymph nodes, and pericardium have also been reported to be dissemination sites [14].
It is crucial to mention that people who become infected and are asymptomatic show mild respiratory symptoms that can be confused with a cold; therefore, patients do not seek medical care. In contrast, cases that progress with moderate or severe lung disease can be mistaken for other pathologies of bacterial etiology, such as pneumonia and tuberculosis, making the diagnosis difficult [15]. Despite the diversity of tools that can be employed for diagnosing this disease, the methods are not available for daily use in clinical laboratories, which poses a challenge. The most commonly used laboratory tools for diagnosing and treating this mycosis are mentioned below.
Diagnosis coccidioidomycosis. The clinical laboratory plays a critical role in diagnosing coccidioidomycosis. It is relevant to mention that cultures are considered the gold standard method for diagnosing coccidioidomycosis; however, they should only be performed in Biosafety Level 3 laboratories (BSL-3s).
Cytology is another diagnostic option performed from sputum samples, bronchoalveolar lavage, or biopsy in cases of extrapulmonary involvement, in which mainly pathognomonic parasitic forms can be observed (spherules) [16,17,18,19].
Immunodiffusion (ID), or Ouchterlony double immunodiffusion (DID), is performed based on the antibodies’ and antigens’ ability to migrate in a semisolid matrix. It has been shown that this test can be very sensitive and specific for detecting distinct antibodies against Coccidioides, with a specificity greater than 95% [20,21].
Another method is the complement fixation test (CF), which provides a semiquantitative evaluation of coccidioidal IgG antibodies and can be performed with serum samples, cerebrospinal fluid (CSF), and other body fluids such as synovial and pleural fluid [22]. Complement fixation is a classic method to demonstrate the presence of antibodies in the patient’s serum.
Another test is the enzyme immunoassay (EIA), which is widely available and provides timely results. Therefore, it is the most commonly used test for the initial detection of coccidioidomycosis. EIAs can be qualitative or semiquantitative. On the other hand, although detecting IgM and IgG antibodies using EIA provides better sensitivity than other available tests for identifying early disease (ID and CF), it is less specific. It is also hampered by the possibility of false-positive results [23]. Therefore, positive EIA results should be confirmed with another test, such as ID or CF, although these are usually negative early in the disease. Thus, follow-up testing every one to two weeks is justified in suspected cases [24].
The skin test with Coccidioides antigens was used from the beginning of the history of this disease for clinical and epidemiological purposes. For this test, the spherusol antigen is used, which is approved by the Food and Drug Administration (FDA), USA [25]. A positive test (induration >5 mm at 48 h) indicates a current or past infection caused by Coccidioides.
Furthermore, a rapid lateral-flow assay (LFA) has been developed recently to detect coccidioidal antibodies that provide results in one hour (Sōna; IMMY, Norman, OK, USA). This assay is advantageous as it can be conducted with minimal training and laboratory equipment. However, a recent study in patients with early coccidioidomycosis showed markedly lower sensitivity for the LFA than the EIA test [26].
Numerous PCR-based methods have been developed and applied recently for detecting Coccidioides species from clinical samples and cultures (Table 1). However, only one has received FDA approval (GeneSTAT, St. George, UT, USA), granted only for bronchoalveolar and bronchial lavage samples [27].

Table 1.
Molecular methods used in the diagnosis of coccidioidomycosis.
Despite numerous laboratory tests being currently available, they clearly present limitations for basic investigation. In addition, affordability is another restriction, primarily in developing countries, where some of these options are not accessible, coupled with the lack of solid clinical data to support their use.
Treatment. On another subject, there is no single therapeutic scheme for coccidioidomycosis. It is recommended that treatment be individualized, especially for patients at risk of complications from severe forms of the disease. The literature shows that fluconazole and itraconazole are the most frequently used antifungals for the various manifestations of coccidioidomycosis. However, other antifungals may be an option for treatment. Among the triazoles are voriconazole, posaconazole, and isavuconazole, while amphotericin B, belonging to the group of polyenes, is also a therapeutic option [38]. It should be noted that amphotericin is currently available in various formulations: amphotericin deoxycholate B, liposomal amphotericin B, amphotericin B colloidal dispersion, and amphotericin B lipid complex, all of which are only available intravenously [39].
Thus, the present work analyzes the epidemiology of coccidioidomycosis, the diagnostic methods, and the treatment of this mycosis based on a review of coccidioidomycosis clinical cases published from 1950 to 2021.
2. Materials and Methods
A systematic search of coccidioidomycosis clinical cases published from 1950 to 2021 was performed in the Scopus, PubMed, ScienceDirect, MEDLINE, and SciELO databases, using the keywords “coccidioidomycosis”, “treatment”, “clinical cases”, and “diagnosis”. The inclusion criteria were clinical cases that reported at least two parameters of the patient’s epidemiological data (age, gender, and geographical origin) as well as the diagnostic method and treatment. Conversely, the exclusion criteria were clinical cases with more than one parameter of the patient’s epidemiological data missing (age, gender, and geographical origin) and clinical cases that did not report the diagnostic method or treatment. Figure 1 illustrates the searching process.
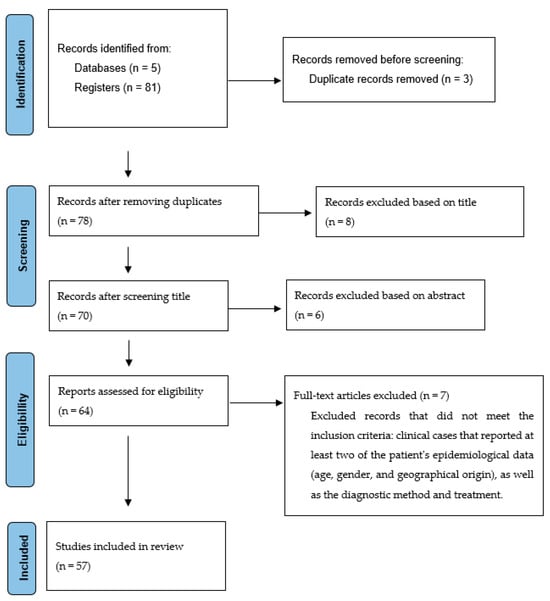
Figure 1.
Flow diagram showing the selection of studies.
The information obtained from the reviewed articles was organized in chronological order. For a better understanding, it was subdivided into tables with the patient’s epidemiological data (age, gender, and geographic origin of the patient). Patients with coccidioidomycosis were classified as having pulmonary or disseminated forms. Likewise, the diagnosis and treatment data were summarized in tables.
3. Results
The search yielded 81 articles on coccidioidomycosis clinical cases from 1950 to 2021. From this total, only 59 articles [17,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97] that included 275 clinical cases and met the inclusion criteria were considered for this review. According to the information obtained, a higher incidence of coccidioidomycosis was shown in the male gender at 89.92% (247), while the female gender presented at 10.18% (28). Regarding age, patients with coccidioidomycosis were found in the age range from newborns to 80 years, with the most affected age group being 31–40 years, while the least impacted was 11–20 years (Table 2).
Table 2.
Clinical cases published from 1950 to 2021.
The clinical presentation of coccidioidomycosis corresponded primarily to disseminated coccidioidomycosis (67.64%), while the frequency of pulmonary coccidioidomycosis was 32.36%. It should be mentioned that within the disseminated cases of the disease, cutaneous and subcutaneous tissue involvement were the most predominant (61), followed by involvement of the CNS (42, generally in the form of meningitis), bone system (39), peritoneum (30), joints (20), lymphatic system (7), genitourinary system (6), eye (4), spleen (4), liver (3), heart (2), thyroid (2), muscle (1), adrenal glands (1), prostate (1), and placenta (1) (Table 3).
Table 3.
Frequency of affected anatomical sites in patients with disseminated coccidioidomycosis.
On the other hand, in those cases where the isolation of the fungus was possible, the species most frequently reported was C. immitis, followed by Coccidioides spp. Likewise, data from this review showed that the most typically used diagnostic methods were direct examination of biological samples with KOH and serological methods, mainly immunodiffusion, complement fixation, and, to a lesser extent, EIA (Table 4).
Table 4.
Laboratory diagnostic tests.
The results of this review showed that the most commonly used treatment for coccidioidomycosis were azoles (57.82%), followed by the combination of azoles and amphotericin B (17.1%), monotherapy with amphotericin B (12.73%), and the use of alternative medicine (4.36%) (Table 5).
Table 5.
Treatment scheme used in cases of coccidioidomycosis.
At a deeper level, the most frequently used pharmacological regimen for treating pulmonary coccidioidomycosis was ketoconazole monotherapy (40), followed by fluconazole monotherapy (15), the combination of amphotericin B and ketoconazole (8), amphotericin B monotherapy (7), amphotericin B combined with fluconazole (6), itraconazole monotherapy (4), amphotericin B combined with itraconazole (2), voriconazole monotherapy (1), the combination of itraconazole and fluconazole (1), protoanemonin (1), and the use of non-steroidal anti-inflammatory drugs (1). Alternatively, the most widely used treatment for disseminated coccidioidomycosis was ketoconazole monotherapy (78), followed by the combination of amphotericin B and fluconazole (24), amphotericin B monotherapy (20), monotherapy with fluconazole (18), the combination of amphotericin B and ketoconazole (11), itraconazole monotherapy (7), amphotericin B combined with itraconazole (2), the combination of amphotericin B and azoles, a treatment not specified in the references (2), posaconazole monotherapy (1), fluconazole combined with itraconazole (1), and itraconazole combined with miconazole (1) (Table 2).
4. Discussion
This work reviews clinical cases of coccidioidomycosis published from 1950 to 2021 that provide epidemiological data, diagnostic methods, and treatment. The epidemiological data presented correspond mostly to cases reported in patients from the USA, showing how important this mycosis is in the country. In other countries, the publication of coccidioidomycosis clinical cases is not that relevant, and the reason behind this has not been clearly determined. In the USA, this mycosis is considered a public health problem. It is mandatory to notify in several states, mainly in endemic areas, which is not the case in other countries. For instance, in Mexico, since 1994, the disease has ceased to require mandatory notification, making epidemiological data scarce. In this review, only sixteen published works were found. That figure does not reflect the current situation of this mycosis, since other reports, which did not meet this review’s inclusion criteria, show an increased number of cases in the country. The same occurs in other countries of the American continent, such as Brazil, Venezuela, and Argentina, where this mycosis is considered significant [1]. In Mexico, specifically, we believe that this mycosis is very relevant since it shares the endemic geographic area of the fungus with the USA. Therefore, it should be expected to follow the same upward trend in the number of cases as the United States [3].
On the other hand, this review showed that the incidence of coccidioidomycosis was higher in the male gender than the female gender. Also, the most affected age group was 31–40 years, which coincides with data reported in Argentina, Venezuela, Brazil, and Mexico [4,5,98,99,100,101]. Likewise, the present work illustrated that the disseminated clinical form was the most predominant, mainly affecting cutaneous and subcutaneous tissue, the peritoneum, the CNS, and the bone system. However, it is worth mentioning that the primary pulmonary form, which in most cases resolves with a favorable outcome for the patient, is the most frequent clinical form of this mycosis and is not officially reported.
Furthermore, this work revealed that the most commonly used diagnostic methods for coccidioidomycosis were fungal identification through cultures and the complement fixation test. A previous study shows that serology has been maintained as the preferred method for an extended period [102], as well as obtaining cultures, even though coccidioidomycosis can be diagnosed through multiple tools. Notably, the complement fixation test, one of the most reported, is only performed in the USA. Unfortunately, this test has not been available for a long time in Central and South American countries, where cases of this mycosis have been described. In some countries, this test has been replaced by ELISA, using in-house antigens, which are also used to conduct gel immunodiffusion and capillary tube precipitation tests and are very useful for diagnosis, although few references document these assertions [103,104,105]. Likewise, other serological methods such as lateral-flow antibody assays [26], the detection of β-1,3-d-glucan [106], the use of recombinant antigens for antibody identification [107], the detection of coccidioidal metabolites in plasma and urine through specific liquid chromatography based on tandem mass spectrometry [108], as well as molecular methods, are not available in most countries or are not validated for routine use in the practice of mycological diagnosis, particularly molecular methods.
On the other hand, this work confirmed that the main therapeutic scheme for coccidioidomycosis is ketoconazole and amphotericin B, individually or in combination. However, ketoconazole appeared in the 1980s and was the first azole with demonstrable activity against Coccidioides spp. approved by the FDA for its treatment [39,109], so the cases reported in this work, during the period from 1980 to 1988, used ketoconazole as an antifungal agent choice; however, it is no longer used in the treatment of this mycosis due to the adverse effects it causes, including hepatotoxicity. Therefore, the cases published in subsequent years show that it was no longer used in the treatment of coccidioidomycosis, and only amphotericin B, fluconazole, itraconazole, and voriconazole were used (Table 2).
Nevertheless, some authors mention that no standard therapy effectively resolves the disease in all cases. Therefore, they suggest that the treatment of coccidioidomycosis should be highly individualized [38]. Also, it is essential to highlight that this treatment scheme applies mainly to cases diagnosed in the USA. In other countries, there is frequently no access to these antifungals due to their high cost, in addition to the fact that there is no reliable information on the number of coccidioidomycosis cases and how they are treated. Particularly in Mexico, this disease ceased to be notifiable in 1994, so there is no record of cases, and the few existing publications are restricted only to retrospective studies of this mycosis [110].
Currently, coccidioidomycosis poses a challenge with a significant impact on public health in countries where the disease is observed, mainly the United States of America, where more than 1,500,000 cases are registered per year (https://www.cdc.gov/fungal/diseases/coccidioidomycosis/statistics.html, accessed on 20 October 2023). Moreover, cases may be underreported in multiple countries on the American continent where this mycosis does not require a mandatory notification, aggravated by the fact that diagnostic tools are scarce.
On the other hand, although the literature highlights a significant advance in molecular methods as aids in diagnosing this mycosis, this study shows that they are not widely implemented as they are not available in all laboratories. More importantly, they are not validated methods. Also, therapeutic options are sometimes limited due to their high cost in several countries.
Despite efforts to develop diagnostic and therapeutic methods focused on preventing and combating coccidioidomycosis, even in countries like the USA, it continues to be a challenge and a public health problem. Meanwhile, the challenge is even greater in countries with fewer economic resources, as this mycosis is not even considered a public health problem. Therefore, sensitization has to be carried out among the health authorities in each country.
5. Conclusions
The analysis of clinical cases in Latin America shows that coccidioidomycosis has been increasing in recent years, and the geographical distribution of Coccidioides spp. is spreading. In other countries on the American continent, except for the United States, the threat of coccidioidomycosis is more insidious, as coccidioidomycosis is likely to be a much more significant threat than official or clinical records indicate. Therefore, continuous and extensive surveillance is necessary in the United States and the rest of the countries on the American continent to monitor trends and identify new potential areas of endemicity to inform public health authorities.
Likewise, this review reveals that the most frequently used diagnostic methods in daily medical practice are serological tests, especially the complement fixation test in the USA. In addition, culture remains the gold standard for diagnosing coccidioidomycosis, and the availability of these is probably due to socioeconomic conditions that do not allow the implementation of other more sensitive diagnostic techniques in other regions of the American continent.
In this work, the primary therapeutic regimen for coccidioidomycosis was ketoconazole and amphotericin B, individually or in combination. However, it should be considered that the use of ketoconazole was discontinued due to its hepatotoxic effects and replaced by other antifungals such as fluconazole, itraconazole, and voriconazole.
Based on the information obtained from this review, we consider that the development of new and faster diagnostic tools, as well as antifungal therapies directed at Coccidioides spp., is still necessary to advance the diagnosis and subsequent resolution of the disease, since knowledge about the epidemiology, diagnosis, and treatment of coccidioidomycosis can be used to guide future prevention and management strategies that minimize the morbidity and mortality caused by this mycosis.
Author Contributions
E.D.-E., M.d.R.R.-M. and A.A.L.-G.: conception and conceptualization of the review; A.A.L.-G., M.G.F.-D.-L., G.A.-A., E.P.S.-S., I.V.-P. and B.M.-R.: investigation; E.D.-E., M.d.R.R.-M. and A.A.L.-G.: preparation of the draft of the original manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
División de Investigación, Facultad de Medicina, Universidad Nacional Autónoma de México (FM/DI/068/2017).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Laniado-Laborín, R.; Arathoon, E.G.; Canteros, C.; Muñiz-Salazar, R.; Rendon, A. Coccidioidomycosis in Latin America. Med. Mycol. 2019, 57, S46–S55. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, N.; Kubat, R.C.; Poplin, V.; Adenis, A.A.; Denning, D.W.; Wright, L.; McCotter, O.; Schwartz, I.S.; Jackson, B.R.; Chiller, T.; et al. Re-drawing the maps for endemic mycoses. Mycopathologia 2020, 185, 843–865. [Google Scholar] [CrossRef] [PubMed]
- Hector, R.F.; Laniado-Laborin, R. Coccidioidomycosis-a fungal disease of the Americas. PLoS Med. 2005, 2, e2. [Google Scholar] [CrossRef] [PubMed]
- Baptista Rosas, R.C.; Riquelme, M. Epidemiología de la coccidioidomicosis en México [The epidemiology of coccidioidomycosis in Mexico]. Rev. Iberoam. Micol. 2007, 24, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Canteros, C.E.; Toranzo, A.; Ibarra-Camou, B.; David, V.; Carrizo, S.G.; Santillán-Iturres, A.; Serrano, J.; Fernández, N.; Capece, P.; Gorostiaga, J.; et al. La coccidioidomicosis en Argentina, 1892–2009 [Coccidioidomycosis in Argentina, 1892–2009]. Rev. Argent. Microbiol. 2010, 42, 261–268. [Google Scholar] [PubMed]
- Reyes-Montes, M.D.R.; Pérez-Huitrón, M.A.; Ocaña-Monroy, J.L.; Frías-De-León, M.G.; Martínez-Herrera, E.O.; Arenas, R.; Duarte-Escalante, E. The habitat of Coccidioides spp. and the role of animals as reservoirs and disseminators in nature. BMC Infect. Dis. 2016, 16, 550. [Google Scholar]
- Valdivia, L.; Nix, D.; Wright, M.; Lindberg, E.; Fagan, T.; Lieberman, D.; Stoffer, T.; Ampel, N.M.; Galgiani, J.N. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg. Infect. Dis. 2006, 12, 958–962. [Google Scholar] [CrossRef]
- Twarog, M.; Thompson, G.R., 3rd. Coccidioidomycosis: Recent updates. Semin. Respir. Crit. Care Med. 2015, 36, 746–755. [Google Scholar] [CrossRef]
- Stockamp, N.W.; Thompson, G.R., 3rd. Coccidioidomycosis. Infect. Dis. Clin. N. Am. 2016, 30, 229–246. [Google Scholar] [CrossRef]
- Malo, J.; Luraschi-Monjagatta, C.; Wolk, D.M.; Thompson, R.; Hage, C.A.; Knox, K.S. Update on the diagnosis of pulmonary coccidioidomycosis. Ann. Am. Thorac. Soc. 2014, 11, 243–253. [Google Scholar] [CrossRef]
- Galgiani, J.N.; Ampel, N.M.; Blair, J.E.; Catanzaro, A.; Geertsma, F.; Hoover, S.E.; Johnson, R.H.; Kusne, S.; Lisse, J.; MacDonald, J.D.; et al. 2016 Infectious Diseases Society of America (IDSA) Clinical practice guideline for the treatment of coccidioidomycosis. Clin. Infect. Dis. 2016, 63, e112–e146. [Google Scholar] [CrossRef] [PubMed]
- Ampel, N.M.; Hoover, S.E. Pathogenesis of coccidioidomycosis. Curr. Fungal Infect. 2015, 9, 253–258. [Google Scholar] [CrossRef]
- Parish, J.M.; Blair, J.E. Coccidioidomycosis. Mayo Clin. Proc. 2008, 83, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Arsura, E.L.; Bobba, R.K.; Reddy, C.M. Coccidioidal pericarditis: A case presentation and review of the literature. Int. J. Infect. Dis. 2005, 9, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, T.N.; Fierer, J. Coccidioides immitis and posadasii: A review of their biology, genomics, pathogenesis, and host immunity. Virulence 2018, 9, 1426–1435. [Google Scholar] [CrossRef] [PubMed]
- Raab, S.S.; Silverman, J.F.; Zimmerman, K.G. Fine-needle aspiration biopsy of pulmonary coccidiodomycosis. Spectrum of cytologic findings in 73 patients. Am. J. Clin. Pathol. 1993, 99, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, L.; Valero, G.; Padhye, A.A. Misleading manifestations of Coccidioides immitis in vivo. J. Clin. Microbiol. 1998, 36, 3721–3723. [Google Scholar] [CrossRef] [PubMed]
- Ke, Y.; Smith, C.W.; Salaru, G.; Joho, K.L.; Deen, M.F. Unusual forms of immature sporulating Coccidioides immitis diagnosed by fine-needle aspiration biopsy. Arch. Pathol. Lab. Med. 2006, 130, 97–100. [Google Scholar] [CrossRef]
- Schuetz, A.N.; Pisapia, D.; Yan, J.; Hoda, R.S. An atypical morphologic presentation of Coccidioides spp. in fine-needle aspiration of lung. Diagn. Cytopathol. 2012, 40, 163–167. [Google Scholar] [CrossRef]
- Smith, C.E.; Saito, M.T.; Beard, R.; Kepp, R.M.; Clark, R.W.; Eddie, B.U. Serological tests in the diagnosis and prognosis of coccidioidomycosis. Am. J. Hyg. 1950, 52, 1–21. [Google Scholar]
- Malo, J.; Holbrook, E.; Zangeneh, T.; Strawter, C.; Oren, E.; Robey, I.; Erickson, H.; Chahal, R.; Durkin, M.; Thompson, C.; et al. Enhanced antibody detection and diagnosis of coccidioidomycosis with the MiraVista IgG and IgM detection enzyme immunoassay. J. Clin. Microbiol. 2017, 55, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd; Sharma, S.; Bays, D.J.; Pruitt, R.; Engelthaler, D.M.; Bowers, J.; Driebe, E.M.; Davis, M.; Libke, R.; Cohen, S.H.; et al. Coccidioidomycosis: Adenosine deaminase levels, serologic parameters, culture results, and polymerase chain reaction testing in pleural fluid. Chest 2013, 143, 776–781. [Google Scholar] [CrossRef]
- Blair, J.E.; Currier, J.T. Significance of isolated positive IgM serologic results by enzyme immunoassay for coccidioidomycosis. Mycopathologia 2008, 166, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd. Pulmonary coccidioidomycosis. Semin. Respir. Crit. Care Med. 2011, 32, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.; Kernerman, S.M.; Sawtelle, B.G.; Rastogi, S.C.; Nielsen, H.S.; Ampel, N.M. A reformulated spherule-derived coccidioidin (Spherusol) to detect delayed-type hypersensitivity in coccidioidomycosis. Mycopathologia 2012, 174, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Donovan, F.M.; Ramadan, F.A.; Khan, S.A.; Bhaskara, A.; Lainhart, W.D.; Narang, A.T.; Mosier, J.M.; Ellingson, K.D.; Bedrick, E.J.; Saubolle, M.A.; et al. Comparison of a novel rapid lateral flow assay to enzyme immunoassay results for early diagnosis of coccidioidomycosis. Clin. Infect. Dis. 2021, 73, e2746–e2753. [Google Scholar] [CrossRef] [PubMed]
- Saubolle, M.A.; Wojack, B.R.; Wertheimer, A.M.; Fuayagem, A.Z.; Young, S.; Koeneman, B.A. Multicenter clinical validation of a cartridge-based real-time PCR system for detection of Coccidioides spp. in lower respiratory specimens. J. Clin. Microbiol. 2018, 56, e01277-17. [Google Scholar] [CrossRef]
- Stockman, L.; Clark, K.A.; Hunt, J.M.; Roberts, G.D. Evaluation of commercially available acridinium ester-labeled chemiluminescent DNA probes for culture identification of Blastomyces dermatitidis, Coccidioides immitis, Cryptococcus neoformans, and Histoplasma capsulatum. J. Clin. Microbiol. 1993, 31, 845–850. [Google Scholar] [CrossRef]
- Greene, D.R.; Koenig, G.; Fisher, M.C.; Taylor, J.W. Soil isolation and molecular identification of Coccidioides immitis. Mycologia 2000, 92, 406–410. [Google Scholar] [CrossRef]
- Fisher, M.C.; Koenig, G.L.; White, T.J.; Taylor, J.W. Molecular and phenotypic description of Coccidioides posadasii sp. nov., previously recognized as the non-California population of Coccidioides immitis. Mycologia 2002, 94, 73–84. [Google Scholar] [CrossRef]
- Bialek, R.; Kern, J.; Herrmann, T.; Tijerina, R.; Ceceñas, L.; Reischl, U.; González, G.M. PCR assays for identification of Coccidioides posadasii based on the nucleotide sequence of the antigen 2/proline-rich antigen. J. Clin. Microbiol. 2004, 42, 778–783. [Google Scholar] [CrossRef]
- Umeyama, T.; Sano, A.; Kamei, K.; Niimi, M.; Nishimura, K.; Uehara, Y. Novel approach to designing primers for identification and distinction of the human pathogenic fungi Coccidioides immitis and Coccidioides posadasii by PCR amplification. J. Clin. Microbiol. 2006, 44, 1859–1862. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tintelnot, K.; De Hoog, G.S.; Antweiler, E.; Losert, H.; Seibold, M.; Brandt, M.A.; Van Den Ende, A.H.; Fisher, M.C. Taxonomic and diagnostic markers for identification of Coccidioides immitis and Coccidioides posadasii. Med. Mycol. 2007, 45, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Binnicker, M.J.; Buckwalter, S.P.; Eisberner, J.J.; Stewart, R.A.; McCullough, A.E.; Wohlfiel, S.L.; Wengenack, N.L. Detection of Coccidioides species in clinical specimens by real-time PCR. J. Clin. Microbiol. 2007, 45, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Montes, M.D.R.; Frías-De-León, M.G.; Victoriano-Pastelín, I.; Acosta-Altamirano, G.; Duarte-Escalante, E. Design and evaluation of an AFLP molecular marker for the detection of Coccidioides spp. in biological samples. Braz. J. Infect. Dis. 2019, 23, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; Victor, T.R.; Marathe, A.; Sidamonidze, K.; Crucillo, K.L.; Chaturvedi, V. Real-time PCR assay for detection and differentiation of Coccidioides immitis and Coccidioides posadasii from culture and clinical specimens. PLoS Negl. Trop. Dis. 2021, 15, e0009765. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Li, X.; Lou, H.; Shang, X.; Mai, Y.; Yang, L.; Peng, F.; Fu, X. Detection of Coccidioides posadasii in a patient with meningitis using metagenomic next-generation sequencing: A case report. BMC Infect. Dis. 2021, 21, 968. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd; Lewis, J.S., 2nd; Nix, D.E.; Patterson, T.F. Current concepts and future directions in the pharmacology and treatment of coccidioidomycosis. Med. Mycol. 2019, 57, S76–S84. [Google Scholar] [CrossRef]
- Crum, N.F. Coccidioidomycosis: A contemporary review. Infect. Dis. Ther. 2022, 11, 713–742. [Google Scholar] [CrossRef]
- Conan, N.J., Jr.; Hyman, G.A. Disseminated coccidioidomycosis; treatment with protoanemonin. Am. J. Med. 1950, 9, 408–413. [Google Scholar] [CrossRef][Green Version]
- Fiese, M.J. Treatment of disseminated coccidioidomycosis with amphotericin B; report of a case. Calif. Med. 1957, 86, 119–120. [Google Scholar] [PubMed]
- Fiese, M.J.; Radding, J.; Cheu, S.; Steinbach, O.K. Disseminated coccidioidomycosis; treatment with ethyl vanillate; A preliminary report. Calif. Med. 1954, 80, 349–356. [Google Scholar] [PubMed]
- Mankiewicz, E.; Henderson, J.A.; Béland, J.E. Pulmonary coccidioidomycosis. Can. Med. Assoc. J. 1968, 99, 1003–1006. [Google Scholar] [PubMed]
- Glynn, K.P.; Alazraki, N.P.; Waltz, T.A. Coccidioidal meningitis. Intrathecal treatment with hyperbaric amphotericin B. Calif. Med. 1973, 119, 6–9. [Google Scholar] [PubMed]
- Sung, J.P. Treatment of disseminated coccidioidomycosis with miconazole. West. J. Med. 1976, 124, 61–64. [Google Scholar] [PubMed]
- Chowdhury, J.K.; Habibzadeh, A. Disseminated coccidioidomycosis with pericarditis. Successful treatment with amphotericin B. Chest 1977, 71, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.J.; Donovan, W.H. Combined intravenous miconazole and intrathecal amphotericin B for treatment of disseminated coccidioidomycosis. Chest 1979, 76, 235–236. [Google Scholar] [CrossRef]
- Graybill, J.R.; Lundberg, D.; Donovan, W.; Levine, H.B.; Rodriguez, M.D.; Drutz, D.J. Treatment of coccidioidomycosis with ketoconazole: Clinical and laboratory studies of 18 patients. Rev. Infect. Dis. 1980, 2, 661–673. [Google Scholar] [CrossRef]
- Galgiani, J.N.; Stevens, D.A.; Graybill, J.R.; Dismukes, W.E.; Cloud, G.A. Ketoconazole therapy of progressive coccidioidomycosis. Comparison of 400- and 800-mg doses and observations at higher doses. Am. J. Med. 1988, 84, 603–610. [Google Scholar] [CrossRef]
- Tucker, R.M.; Williams, P.L.; Arathoon, E.G.; Levine, B.E.; Hartstein, A.I.; Hanson, L.H.; Stevens, D.A. Pharmacokinetics of fluconazole in cerebrospinal fluid and serum in human coccidioidal meningitis. Antimicrob. Agents Chemother. 1988, 32, 369–373. [Google Scholar] [CrossRef]
- Godoy, J.; Correa, A.; De Guevara, E.; De Salcedo, M. Coccidioidomicosis sistémica: Informe de un caso en Colombia. Acta Med. Colomb. 1990, 15, 208–211. [Google Scholar]
- Jamidar, P.A.; Campbell, D.R.; Fishback, J.L.; Klotz, S.A. Peritoneal coccidioidomycosis associated with human immunodeficiency virus infection. Gastroenterology 1992, 102, 1054–1058. [Google Scholar] [CrossRef]
- Martínez Delgado, J.; Trujillo Lara, R.; Padua Gabriel, A.; del Rocío González, M.; Manriquez Covarrubias, L. Coccidioidomicosis pulmonar. Tratamiento quirúrgico de dos casos [Pulmonary coccidioidomycosis. Surgical treatment of 2 cases]. Gac. Med. Mex. 1993, 129, 53–56. [Google Scholar] [PubMed]
- Ismail, Y.; Arsura, E.L. Eosinophilic meningitis associated with coccidioidomycosis. West. J. Med. 1993, 158, 300–301. [Google Scholar] [PubMed]
- Perez, J.A., Jr.; Arsura, E.L. Peritoneal coccidioidomycosis diagnosed incidentally at herniorrhaphy. West. J. Med. 1993, 158, 406. [Google Scholar]
- Nickisch, S.A.; Izquierdo, L.; Vill, M.A.; Curet, L.; Wolf, G.C. Coccidioidal placentitis with normal umbilical artery velocimetry. Infect. Dis. Obstet. Gynecol. 1993, 1, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.A.; Anderson, A.E.; Kostroff, K. An unusual case of coccidioidomycosis. J. Clin. Microbiol. 1994, 32, 1063–1064. [Google Scholar] [CrossRef] [PubMed]
- Shawar, R.M.; Salyer, J.L.; Ballou, D.; Clarridge, J.E. Recovery of Coccidioides immitis from blood and abscess fluid using the BacT/alert system. Diagn. Microbiol. Infect. Dis. 1995, 21, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Jou, J.R.; Patel, S.; Yo, C.; Sadun, A.A.; Jou, J.R. Orbital coccidioidomyosis presenting as a lacrimal gland fossa mass. Br. J. Ophthalmol. 1995, 79, 1145–1146. [Google Scholar] [CrossRef]
- Bañuelos, A.F.; Williams, P.L.; Johnson, R.H.; Bibi, S.; Fredricks, D.N.; Gilroy, S.A.; Bhatti, S.U.; Aguet, J.; Stevens, D.A. Central nervous system abscesses due to Coccidioides species. Clin. Iinfect. Dis. 1996, 22, 240–250. [Google Scholar] [CrossRef]
- Sharma, O.P.; Arora, A. Coccidioidomycosis and sarcoidosis. Multiple recurrences. West. J Med. 1997, 166, 345–347. [Google Scholar] [PubMed]
- Vélez, A.; Robledo, M.; Builes, M.; Tobón, A.; Gómez, C.I.; Upegui, J.J.; Hincapié, M.I.; Moncada, L.E.; Arango, M.; Restrepo, A. El caso de infeciosas. Coccidioidomicosis pulmonar. Informe de un caso autóctono. Medicina UPB 1997, 16, 141–147. [Google Scholar]
- Cunningham, E.T., Jr.; Seiff, S.R.; Berger, T.G.; Lizotte, P.E.; Howes, E.L., Jr.; Horton, J.C. Intraocular coccidioidomycosis diagnosed by skin biopsy. Arch. Ophthal. 1998, 116, 674–677. [Google Scholar] [CrossRef]
- Zepeda, M.R.; Kobayashi, G.K.; Appleman, M.D.; Navarro, A. Coccidioides immitis presenting as a hyphal form in cerebrospinal fluid. J. Natl. Med. Assoc. 1998, 90, 435–436. [Google Scholar] [PubMed]
- Linsangan, L.C.; Ross, L.A. Coccidioides immitis infection of the neonate: Two routes of infection. Pediatr. Infect. Dis. J. 1999, 18, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Padua, A.G.; Martínez, O.V.; Velasco, R.V.; Calva, M.J.J.; Cicero, S.R. Tratamiento de la coccidioidomicosis pulmonar y pleural. Experiencia con seis casos en Torreón Coahuila. Enf. Infec. Microbiol 1999, 19, 133–138. [Google Scholar]
- Chowfin, A.; Tight, R. Female genital coccidioidomycosis (FGC), Addison’s disease and sigmoid loop abscess due to Coccidioides immitis; case report and review of literature on FGC. Mycopathologia 1999, 145, 121–126. [Google Scholar] [CrossRef]
- Charlton, V.; Ramsdell, K.; Sehring, S. Intrauterine transmission of coccidioidomycosis. Pediatr. Infect. Dis. J. 1999, 18, 561–563. [Google Scholar] [CrossRef]
- Goldberg, B.; Loeffler, A.M. Respiratory distress and a liver mass. Pediatr. Infect. Dis. J. 1999, 18, 1105–1114. [Google Scholar] [CrossRef]
- Polesky, A.; Kirsch, C.M.; Snyder, L.S.; LoBue, P.; Kagawa, F.T.; Dykstra, B.J.; Wehner, J.H.; Catanzaro, A.; Ampel, N.M.; Stevens, D.A. Airway coccidioidomycosis-report of cases and review. Clin. Infect. Dis. 1999, 28, 1273–1280. [Google Scholar] [CrossRef]
- Erly, W.K.; Labadie, E.; Williams, P.L.; Lee, D.M.; Carmody, R.F.; Seeger, J.F. Disseminated coccidioidomycosis complicated by vasculitis: A cause of fatal subarachnoid hemorrhage in two cases. Am. J. Neuroradiol. 1999, 120, 605–1608. [Google Scholar]
- Phillips, P.; Ford, B. Peritoneal coccidioidomycosis: Case report and review. Clin. Infect. Dis. 2000, 30, 971–976. [Google Scholar] [CrossRef] [PubMed]
- Hagman, H.M.; Madnick, E.G.; D’Agostino, A.N.; Williams, P.L.; Shatsky, S.; Mirels, L.F.; Tucker, R.M.; Rinaldi, M.G.; Stevens, D.A.; Bryant, R.E. Hyphal forms in the central nervous system of patients with coccidioidomycosis. Clin. Infect. Dis. 2000, 30, 349–353. [Google Scholar] [CrossRef] [PubMed]
- García, E.M.; Gaytán Martínez, J.E.; Casanova, L.J.; Fuentes Allen, J.L. Coccidioidomicosis diseminada: Manifestación inicial de SIDA en residente de área no endémica. Rev. Med. IMSS 2000, 38, 433–436. [Google Scholar]
- Saitoh, A.; Homans, J.; Kovacs, A. Fluconazole treatment of coccidioidal meningitis in children: Two case reports and a review of the literature. Pediatr. Infect. Dis. J. 2000, 19, 1204–1208. [Google Scholar] [CrossRef] [PubMed]
- Halsey, E.S.; Rasnake, M.S.; Hospenthal, D.R. Coccidioidomycosis of the male reproductive tract. Mycopathologia 2005, 159, 199–204. [Google Scholar] [CrossRef]
- Ruggles, D. Testicular coccidioidomycosis. Urol. Nurs. 2008, 28, 113–114. [Google Scholar] [PubMed]
- Batura-Gabryel, H.; Brajer, B. Coccidioidomycosis in a 38-year-old man: A case report. Pol. Arch. Med. Wewn. 2008, 118, 387–390. [Google Scholar] [CrossRef]
- Buijze, G.A.; Kok, P.; Botha-Scheepers, S.A.; Smith, S.J.; Sleeboom, H.P. Fungal disease of the western hemisphere: A patient with coccidioidomycosis. Eur. J. Intern. Med. 2009, 20, 319–322. [Google Scholar] [CrossRef]
- Cadena, J.; Hartzler, A.; Hsue, G.; Longfield, R.N. Coccidioidomycosis and tuberculosis coinfection at a tuberculosis hospital: Clinical features and literature review. Medicine 2009, 88, 66–76. [Google Scholar] [CrossRef]
- Homans, J.D.; Spencer, L. Itraconazole treatment of nonmeningeal coccidioidomycosis in children: Two case reports and review of the literature. Pediatr. Infect. Dis. J. 2010, 29, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Capoor, M.R.; Sen, B.; Varshney, P.; Verghese, M.; Shivaprakash, M.R.; Chakrabarti, A. Coccidioidomycosis masquerading as skeletal tuberculosis: An imported case and review of coccidioidomycosis in India. Trop. Doct. 2014, 44, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Matuk-Pérez, Y.; Rodríguez-Leyva, I.; Torres-Corzo, J.; Oros-Ovalle, C.; De La Rosa-Quiroz, C.E. Meningeal coccidioidomycosis: Case report and literature review. Rev. Mex. Neuroci. 2014, 15, 224–228. [Google Scholar]
- Saettele, T.M.; Jimenez, C.A. Pleural coccidioidomycosis. BMJ Case Rep. 2014, 24, bcr2014206380. [Google Scholar] [CrossRef] [PubMed]
- Satyanarayan, A.; Klotz, S.; Han, L.; Sobonya, R.; Zangeneh, T.T. Coccidioidomycosis of the genitourinary tract: A case report and discussion. Urology 2014, 84, e30–e31. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Coutiño, G.; Arce-Ramírez, M.; Medina, A.; Amarillas-Villalva, A.; Salas-Vargas, V.; Madrigal-Kazem, R.; Arenas, R. Coccidioidomicosis cutánea: Comunicación de seis casos mexicanos [Cutaneous coccidioidomycoses: Six Mexican cases report]. Rev. Chilena Infect. 2015, 32, 339–343. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Labarca-Acosta, M.; Santos-Bolívar, J.; Aragón-Charry, J.; Reyna-Villasmil, E. Coccidioidomicosis diseminada y embarazo. Reporte de un caso. Clin. Investig. Ginecol. Obstet. 2015, 42, 38–40. [Google Scholar] [CrossRef]
- Dworak, D.P.; Kapustiak, J.; Ehklassi, T.A.; Patrianakos, T.D. Primary cutaneous coccidioidomycosis of the eyelid: A case report. Ophthalmic. Plast. Reconstr. Surg. 2016, 32, e40–e41. [Google Scholar] [CrossRef]
- Araújo, P.S.R.; Souza Junior, V.R.; Padilha, C.E.; Oliveira, M.I.; Arraes, L.C.; Vieira, R.; Antunes, A.; Lima Neto, R.G.; Marsden, A. Coccidioidomycosis: First cases reported in Pernambuco, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2018, 60, e75. [Google Scholar] [CrossRef]
- De Alba, d.L.C.A. Derrame pleural por micosis endémica en un paciente de 8 años: Reporte de un caso. Neumol. Pediatr. 2018, 13, 32–34. [Google Scholar] [CrossRef]
- Manning, M.A.; Kuo, P.H.; Yeager, A.M. Disseminated coccidioidomycosis masquerading as recurrent lymphoma. BMJ Case Rep. 2018, bcr2018224965. [Google Scholar] [CrossRef] [PubMed]
- Nordstrom, B.; Sherpa, N.; Marshall, M.; Chawla, A.; Heidari, A.; Johnson, R. Coccidioidomycosis chorioretinitis. J. Investig. Med. High Impact Case Rep. 2019, 7, 2324709619881561. [Google Scholar] [CrossRef] [PubMed]
- Lynch, F.H.; Maly, C.J.; Unwala, R.; Blair, J.E.; DiCaudo, D.J.; Mangold, A.R. Disseminated coccidioidomycosis mimicking cicatricial alopecia. JAAD Case Rep. 2019, 5, 957–959. [Google Scholar] [CrossRef] [PubMed]
- Prichard, J.G.; Azimov, M.B.; Oregel, K.Z. Coccidioidomycosis and pulmonary emboli: A report of 5 cases. Am. J. Case Rep. 2020, 21, e924179. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.; Thauland, T.J.; Huang, A.Y.; Bun, C.; Fitzwater, S.; Krogstad, P.; Douine, E.D.; Nelson, S.F.; Lee, H.; Garcia-Lloret, M.I.; et al. Disseminated coccidioidomycosis treated with interferon-γ and dupilumab. N. Engl. J. Med. 2020, 382, 2337–2343. [Google Scholar] [CrossRef]
- Sakya, S.M.; Sakya, J.P.; Hallan, D.R.; Warraich, I. Spinal Coccidioidomycosis: A complication from medication noncompliance. Cureus 2020, 12, e9304. [Google Scholar] [CrossRef] [PubMed]
- Chee, D.; Moritz, A.W.; Profit, A.P.; Agarwal, A.N.; Anstead, G.M. Fatal coccidioidomycosis involving the lungs, brain, tongue, and adrenals in a cirrhotic patient. An autopsy case. ID Cases 2021, 23, e01049. [Google Scholar] [CrossRef] [PubMed]
- González-Benavides, J. Panorama de la coccidioidomicosis en Nuevo León de 1978 a 1988 [The panorama of coccidioidomycosis in Nuevo León from 1978 to 1988]. Gac. Med. Mex. 1991, 127, 427–433. [Google Scholar]
- Martínez Méndez, D.; Hernández Valles, R.; Alvarado, P.; Mendoza, M. Las micosis en Venezuela: Casuística de los grupos de trabajo en Micología (1984–2010) [Mycoses in Venezuela: Working groups in Mycology reported cases (1984–2010)]. Rev. Iberoam. Micol. 2013, 30, 39–46. [Google Scholar] [CrossRef]
- Morais, J.L.D.S.; Borges, M.C.M.; Cavalcante, L.M.M.B.; Motoyama, P.V.P.; Libório, M.P.; Távora, L.G.F. Coccidioidomycosis in a reference center in Northeast Brazil: Clinical/epidemiological profile and most common radiological findings. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200249. [Google Scholar] [CrossRef]
- Cordeiro, R.; Moura, S.; Castelo-Branco, D.; Rocha, M.F.; Lima-Neto, R.; Sidrim, J.J. Coccidioidomycosis in Brazil: Historical challenges of a neglected disease. J. Fungi 2021, 7, 85. [Google Scholar] [CrossRef] [PubMed]
- Ampel, N.M. Coccidioidomycosis: Changing concepts and knowledge gaps. J. Fungi 2020, 6, 354. [Google Scholar] [CrossRef] [PubMed]
- Filho, R.E.; Bandeira, S.P.; Brillhante, R.S.; Rocha, M.F.; Vasconcelos, I.M.; Pereira, M.L.; Castelo-Branco, D.d.S.; Rocha, F.A.; Camargo, Z.P.; Ramos, M.V.; et al. Biochemical characterization of an in-house Coccidioides antigen: Perspectives for the immunodiagnosis of coccidioidomycosis. Molecules 2012, 17, 7854–7863. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Paes, R.; Bernardes-Engemann, A.R.; da Silva Motta, B.; Pizzini, C.V.; de Abreu Almeida, M.; de Medeiros Muniz, M.; Dias, R.A.B.; Zancopé-Oliveira, R.M. Immunologic diagnosis of endemic mycoses. J. Fungi 2022, 8, 993. [Google Scholar] [CrossRef] [PubMed]
- Caceres, D.H.; Echeverri Tirado, L.C.; Bonifaz, A.; Adenis, A.; Gomez, B.L.; Banda Flores, C.L.; Canteros, C.E.; Wagner Santos, D.; Arathoon, E.; Ramirez Soto, E.; et al. Current situation of endemic mycosis in the Americas and the Caribbean: Proceedings of the first international meeting on endemic mycoses of the Americas (IMEMA). Mycoses 2022, 65, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd; Bays, D.J.; Johnson, S.M.; Cohen, S.H.; Pappagianis, D.; Finkelman, M.A. Serum (1→3)-β-D-glucan measurement in coccidioidomycosis. J. Clin. Microbiol. 2012, 50, 3060–3062. [Google Scholar] [CrossRef] [PubMed]
- Peng, T.; Zong, Y.; Johnson, M.D.; Menghani, S.V.; Lewis, M.L.; Galgiani, J.N. A quantitative enzyme-linked immunoassay (ELISA) to approximate complement-fixing antibody titers in serum from patients with coccidioidomycosis. Diagn. Microbiol. Infect. Dis. 2021, 99, 115198. [Google Scholar] [CrossRef] [PubMed]
- Jasbi, P.; Mitchell, N.M.; Shi, X.; Grys, T.E.; Wei, Y.; Liu, L.; Lake, D.F.; Gu, H. Coccidioidomycosis detection using targeted plasma and urine metabolic profiling. J. Proteome Res. 2019, 18, 2791–2802. [Google Scholar] [CrossRef]
- Sheehan, D.J.; Hitchcock, C.A.; Sibley, C.M. Current and emerging azole antifungal agents. Clin. Microbiol. Rev. 1999, 12, 40–79. [Google Scholar] [CrossRef]
- Laniado-Laborín, R. Coccidioidomycosis and other endemic mycoses in Mexico. Rev. Iberoam. Micol. 2007, 24, 249–258. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).