
Assessment of Fetal Dose and Health Effect to the Fetus from Breast Cancer Radiotherapy during Pregnancy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
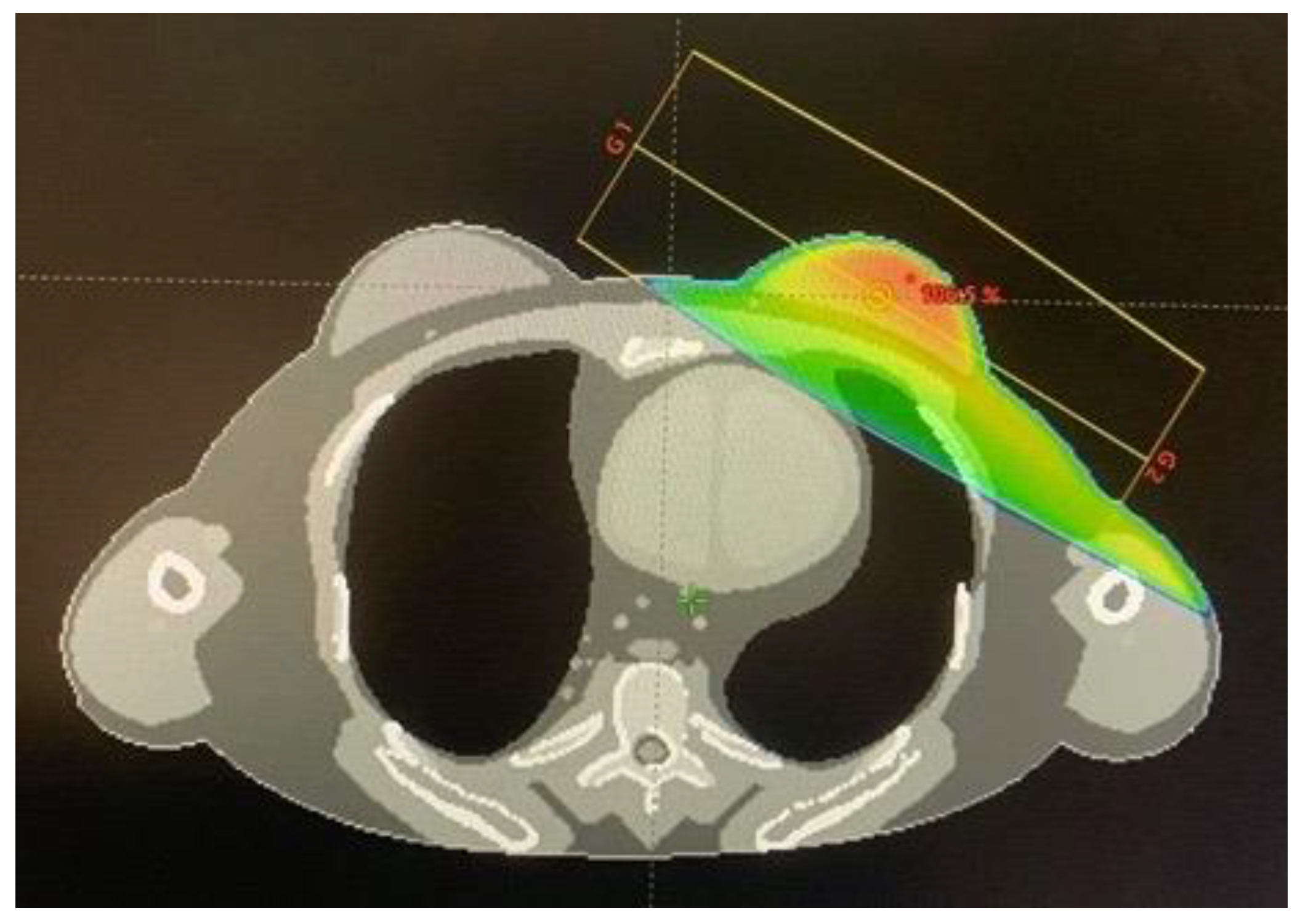
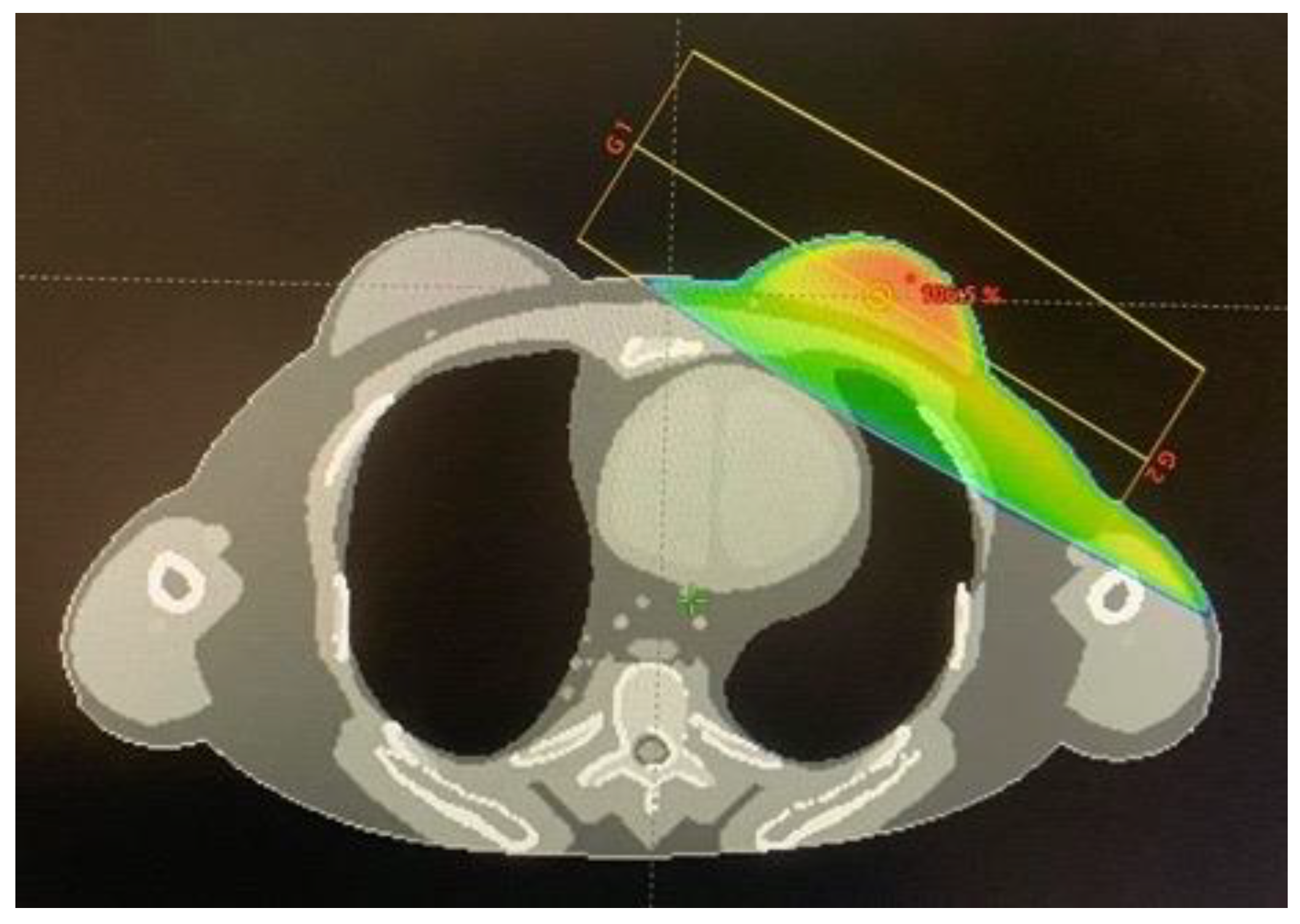
2.1. Treatment Planning
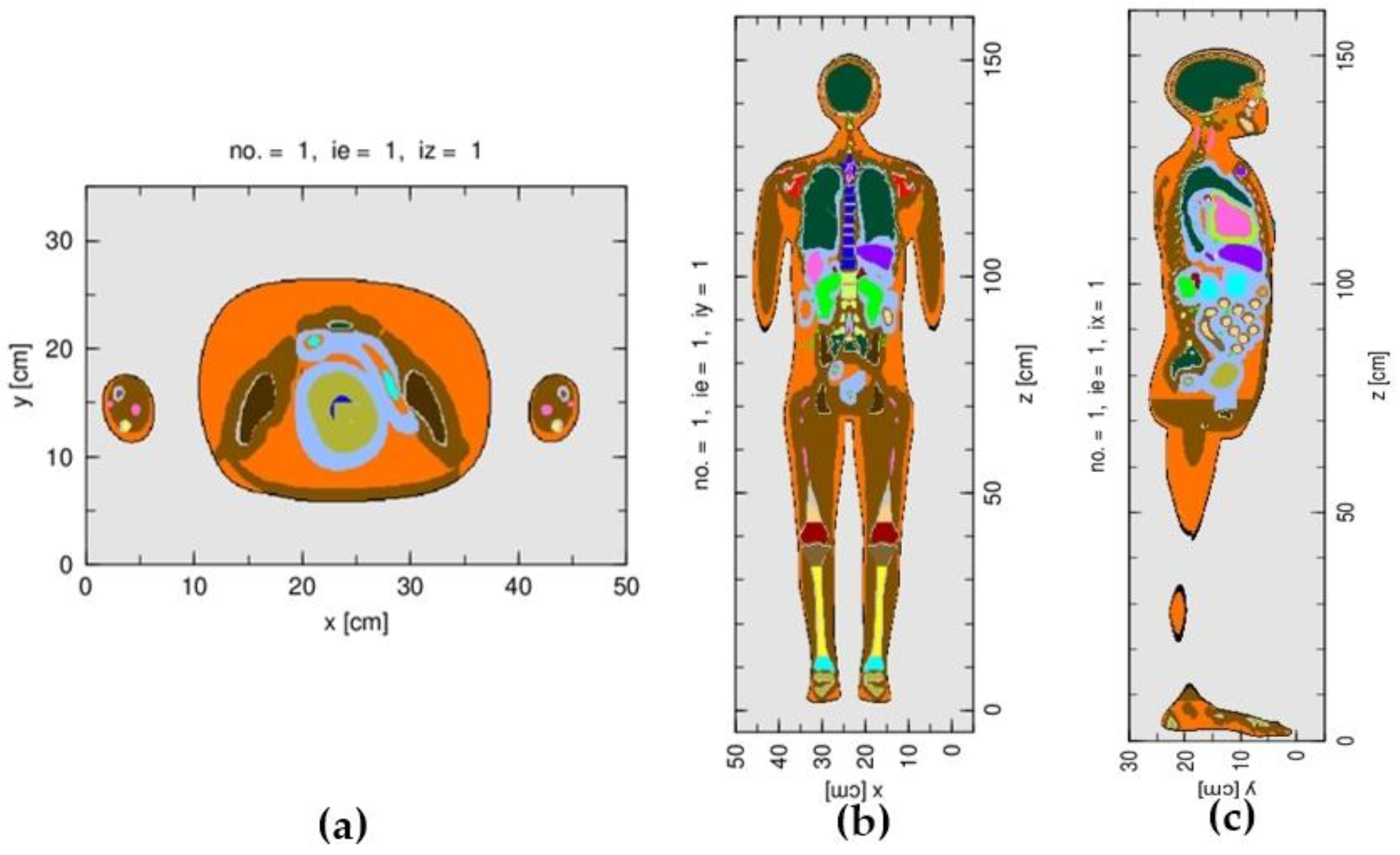
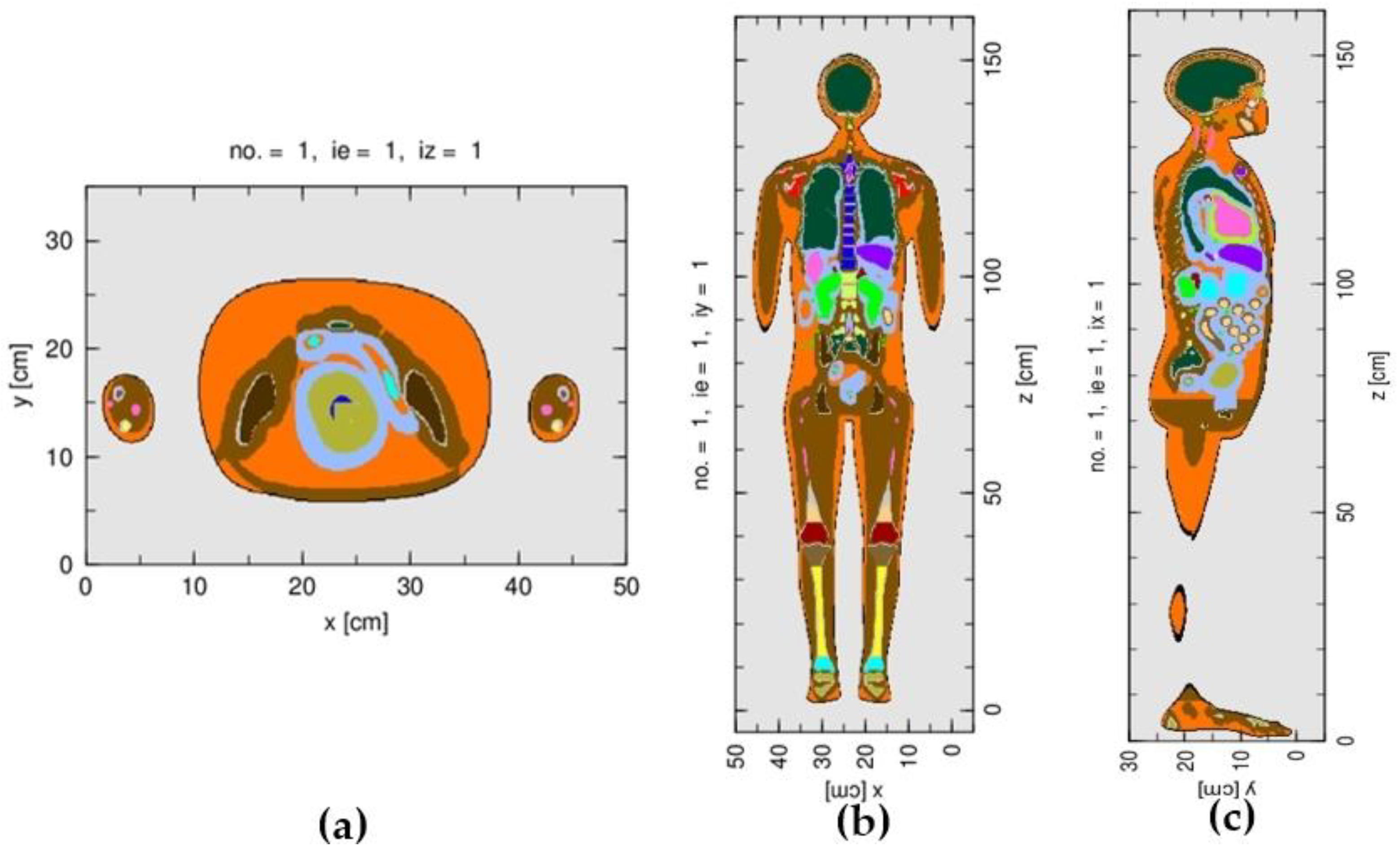
2.2. Monte Carlo Simulation
2.3. Evaluation of Deterministic Effect and Stochastic Effect
3. Results
3.1. Determination of Fetal Dose
3.2. Deterministic Effects and Stochastic Effects of the Fetus
4. Discussion
4.1. Determination of Fetal Dose
4.1.1. Comparison of the Monte Carlo Simulation and the Treatment Plan
4.1.2. Fetal Dose Evaluation Using the Monte Carlo Simulation
4.2. Fetal Deterministic Effect and Stochastic Effect
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stovall, M.; Blackwell, C.; Cundiff, J.; Novack, D.; Palta, J.; Wagner, L.; Webster, E.; Shalek, R. Fetal dose from radiotherapy with photon beams: Report of AAPM Radiation Therapy Committee Task Group No 36. Med. Phys. 1995, 22, 63–82. [Google Scholar] [CrossRef] [PubMed]
- Mazonakis, M.; Tzedakis, A.; Damilakis, J. Monte Carlo Simulation of Radiotherapy for Breast Cancer in Pregnant Patients: How to Reduce the Radiation Dose and Risks to Fetus? Radiat. Prot. Dosim. 2017, 175, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Antypas, C.; Sandilos, P.; Kouvaris, J.; Balafouta, E.; Karinou, E.; Kollaros, N.; Vlahos, L. Fetal dose evaluation during breast cancer radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 995–999. [Google Scholar] [CrossRef]
- Labby, Z.; Barraclough, B.; Bayliss, R.; Besemer, E.; Dunkerley, D.; Howard, S. Radiation treatment planning and delivery strategies for a pregnant brain tumor patient. J. Appl. Clin. Med. Phys. 2018, 19, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Kry, S.; Bednarz, B.; Howell, R.; Dauer, L.; Followill, D.; Klein, E.; Paganetti, H.; Wang, B.; Wuu, C.; Xu, X. AAPM TG 158: Measurement and calculation of doses outside the treated volume from external-beam radiation therapy. Med. Phys. 2017, 44, 391–429. [Google Scholar] [CrossRef]
- Paulbeck, C.; Griffin, K.; Lee, C.; Cullings, H.; Egbert, S.D.; Funamoto, S.; Sato, T.; Endo, A.; Hertel, N.; Bolch, W.E. Dosimetric Impact of a New Computational Voxel Phantom Series for the Japanese Atomic Bomb Survivors: Pregnant Females. Radiat. Res. 2019, 192, 538–561. [Google Scholar]
- Emami, B.; Lyman, J.; Brown, A.; Coia, L.; Goitein, M.; Munzenrider, J.; Shank, B.; Solin, L.; Wesson, M. Tolerance of normal tissue to therapeutic radiation. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 109–112. [Google Scholar] [CrossRef]
- Sato, T.; Iwamoto, Y.; Hashimoto, S.; Ogawa, T.; Furuta, T.; Abe, S.; Kai, T.; Tsai, P.; Matsuda, N.; Iwase, H. Features of Particle and Heavy Ion Transport code System (PHITS) version 3.02. J. Nucl. Sci. Technol. 2018, 55, 684–690. [Google Scholar] [CrossRef]
- Varian Medical System. TrueBeam Monte Carlo Data Package Version 1.1; Varian Medical System: Palo Alto, CA, USA, 2014. [Google Scholar]
- Suwanbut, P.; Liamsuwan, T.; Nantajit, D.; Masa-nga, W.; Tannanonta, C. Validation of the 6 MV TrueBeam linear accelerator model for out-of-field radiation dose calculation using PHITS Monte Carlo code. J. Assoc. Med. Sci. 2021, 54, 32–42. [Google Scholar]
- Centers for Disease Control and Prevention: Radiation and Pregnancy. Available online: https://www.cdc.gov/nceh/radiation/emergencies/prenatalphysician.htm (accessed on 5 August 2020).
- Pregnancy and Medical Radiation; ICRP Publication 84; Annals of the ICRP; ICRP: Ottawa, ON, Canada, 2000; Volume 30, pp. 1–43.
- Andreas, J.; Oscar, M.; Jeanneret-Sozzi, W.; Bochud, F.; Moeckli, R. Evaluation of organ-specific peripheral doses after 2-dimensional, 3-dimensional and hybrid intensity modulated radiation therapy for breast cancer based on Monte Carlo and convolution/superposition algorithms: Implications for secondary cancer risk assessment. Radiother. Oncol. 2013, 106, 33–41. [Google Scholar]
- Hughes, J.; Elizabeth, L.; Kadeer, F.; Alves, A.; Shaw, M.; Supple, J.; Keehan, S.; Gibbons, F.; Lehmann, J.; Kron, T. Calculation algorithms and penumbra: Underestimation of dose in organs at risk in dosimetry audits. Med. Phys. 2021, 47, 777–780. [Google Scholar] [CrossRef] [PubMed]
- Shine, N.S.; Paramu, R.; Gopinath, M.; Bos, R.; Jayadevan, P. Out-of-Field Dose Calculation by a Commercial Treatment Planning System and Comparison by Monte Carlo Simu.ulation for Varian TrueBeam. J. Med. Phys. 2019, 44, 156–175. [Google Scholar] [CrossRef] [PubMed]
- Chow, J.; Grigorov, G.N. Surface dosimetry for oblique tangential photon beams: A Monte Carlo simulation study. Med. Phys. 2008, 35, 70–76. [Google Scholar] [CrossRef]
- Bednarz, B.; Xu, G. A feasibility study to calculate unshielded fetal doses to pregnant patients in 6-MV photon treatments using Monte Carlo methods and anatomically realistic phantoms. Med. Phys. 2008, 35, 3054–3061. [Google Scholar] [CrossRef]
- Kry, S.F.; Starkschall, G.; Antolak, J.; Salehpour, M. Evaluation of the accuracy of fetal dose estimates using TG-36 data. Med. Phys. 2007, 34, 1193–1197. [Google Scholar] [CrossRef]
- Mazzola, R.; Corradini, S.; Eidemüeller, M.; Figlia, V.; Fiorentino, A.; Giaj-Levra, N.; Nicosia, L.; Ricchetti, F.; Rigo, M.; Musola, M.; et al. Modern radiotherapy in cancer treatment during pregnancy. Crit. Rev. Oncol. Hematol. 2019, 136, 13–19. [Google Scholar] [CrossRef]
- Owrangi, A.M.; Roberts, D.A.; Covington, E.; Hayman, J.; Masi, K.; Lee, C.; Moran, J.; Prisciandaro, J. Revisiting fetal dose during radiation therapy: Evaluating treatment techniques and a custom shield. J. Appl. Clin. Med. Phys. 2016, 17, 34–46. [Google Scholar] [CrossRef]
- Mazonakis, M.; Varveris, H.; Fasoulaki, M.; Damilakis, J. Radiotherapy of Hodgkin’s disease in early pregnancy: Embryo dose measurements. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2003, 66, 333–339. [Google Scholar] [CrossRef]
- Atarod, M.; Shokrani, P. Monte Carlo Study of Fetal Dosimetry Parameters for 6 MV Photon Beam. J. Med. Signals Sens. 2013, 3, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Mazonakis, M.; Tzedakis, A.; Varveris, C.; Damilakis, J. Radiotherapy for supradiaphragmatic Hodgkin’s disease: Determination of the proper fetal shielding conditions using Monte Carlo methodology. Phys. Med. 2011, 27, 181–187. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Structures | Criteria |
|---|---|
| Target (Left breast, whole breast) | D100 = 95% prescribed dose |
| Left lung | DMean < 20 Gy |
| Right lung | DMean < 20 Gy |
| Total lung | DMean < 20 Gy |
| Heart | DMean < 6 Gy |
| Esophagus | DMean < 34 Gy |
| Spinal cord | DMax < 45 Gy |
| Structures | Volume in TPS (cm3) | Volume in MC (cm3) | Mean Dose in TPS (Gy) | Mean Dose in MC (Gy) | % Dose Difference |
|---|---|---|---|---|---|
| Target (Left breast, whole breast) | 142.9 | 141.21 | 46.59 | 46.59 ± 0.18 | - |
| Left lung | 1172.8 | 1133.9 | 3.23 | 3.45 ± 0.02 | −6.38 |
| Total lung | 2505.0 | 2530.0 | 1.49 | 1.69 ± 0.01 | −11.83 |
| Esophagus | 32.8 | 31.3 | 0.21 | 0.27 ± 0.02 | −22.22 |
| Heart | 540.7 | 543.6 | 1.66 | 2.13 ± 0.02 | −22.07 |
| Right lung | 1446.2 | 1396.1 | 0.07 | 0.26 ± 0.01 | −73.08 |
| Spinal cord | 40.2 | 41.5 | 0.01 | 0.13 ± 0.01 | −92.31 |
| Small intestine | - | 976.2 | - | 0.11 ± 2.22 × 10−3 | - |
| Uterus | - | 169.3 | - | 0.04 ± 3.08 × 10−3 | - |
| Fetus | - | 3.2 | - | 3.37 × 10−3 ± 2.66 × 10−3 | - |
| Urinary bladder | - | 77.4 | - | 0.03 ± 3.72 × 10−3 | - |
| NCRP Report No. 174 (6th to 13th Weeks) | ||
| Radiation dose | Effect | |
| <0.10 Gy | Non-cancer health effects not detectable | |
| 0.10–0.50 Gy | Growth restriction possible | |
| >0.50 Gy | Probability of miscarriage may increase, depending on dose Growth restriction is likely | |
| AAPM TG-36 | ||
| Radiation dose | Risk | |
| <0.05 Gy | Little risk of damage | |
| 0.05–0.1 Gy | Risk uncertain | |
| 0.1–0.5 Gy | Significant risk of damage | |
| >0.5 Gy | High risk of damage during all trimester | |
| ICRP Publication 84 | ||
| Absorbed dose to conceptus above natural background | Probability that the child will have no malformation | Probability that the child will not develop cancer2 |
| (mGy) | (%) | (%) |
| 0 | 97 | 99.7 |
| 0.5 | 97 | 99.7 |
| 1 | 97 | 99.7 |
| 2.5 | 97 | 99.7 |
| 5 | 97 | 99.7 |
| 10 | 97 | 99.6 |
| 50 | 97 | 99.4 |
| 100 | 97 | 99.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suwanbut, P.; Liamsuwan, T.; Nantajit, D.; Masa-nga, W.; Tannanonta, C. Assessment of Fetal Dose and Health Effect to the Fetus from Breast Cancer Radiotherapy during Pregnancy. Life 2022, 12, 84. https://doi.org/10.3390/life12010084
Suwanbut P, Liamsuwan T, Nantajit D, Masa-nga W, Tannanonta C. Assessment of Fetal Dose and Health Effect to the Fetus from Breast Cancer Radiotherapy during Pregnancy. Life. 2022; 12(1):84. https://doi.org/10.3390/life12010084
Chicago/Turabian StyleSuwanbut, Pattarakan, Thiansin Liamsuwan, Danupon Nantajit, Wilai Masa-nga, and Chirapha Tannanonta. 2022. "Assessment of Fetal Dose and Health Effect to the Fetus from Breast Cancer Radiotherapy during Pregnancy" Life 12, no. 1: 84. https://doi.org/10.3390/life12010084
APA StyleSuwanbut, P., Liamsuwan, T., Nantajit, D., Masa-nga, W., & Tannanonta, C. (2022). Assessment of Fetal Dose and Health Effect to the Fetus from Breast Cancer Radiotherapy during Pregnancy. Life, 12(1), 84. https://doi.org/10.3390/life12010084