Tumour PD-L1 Expression in Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
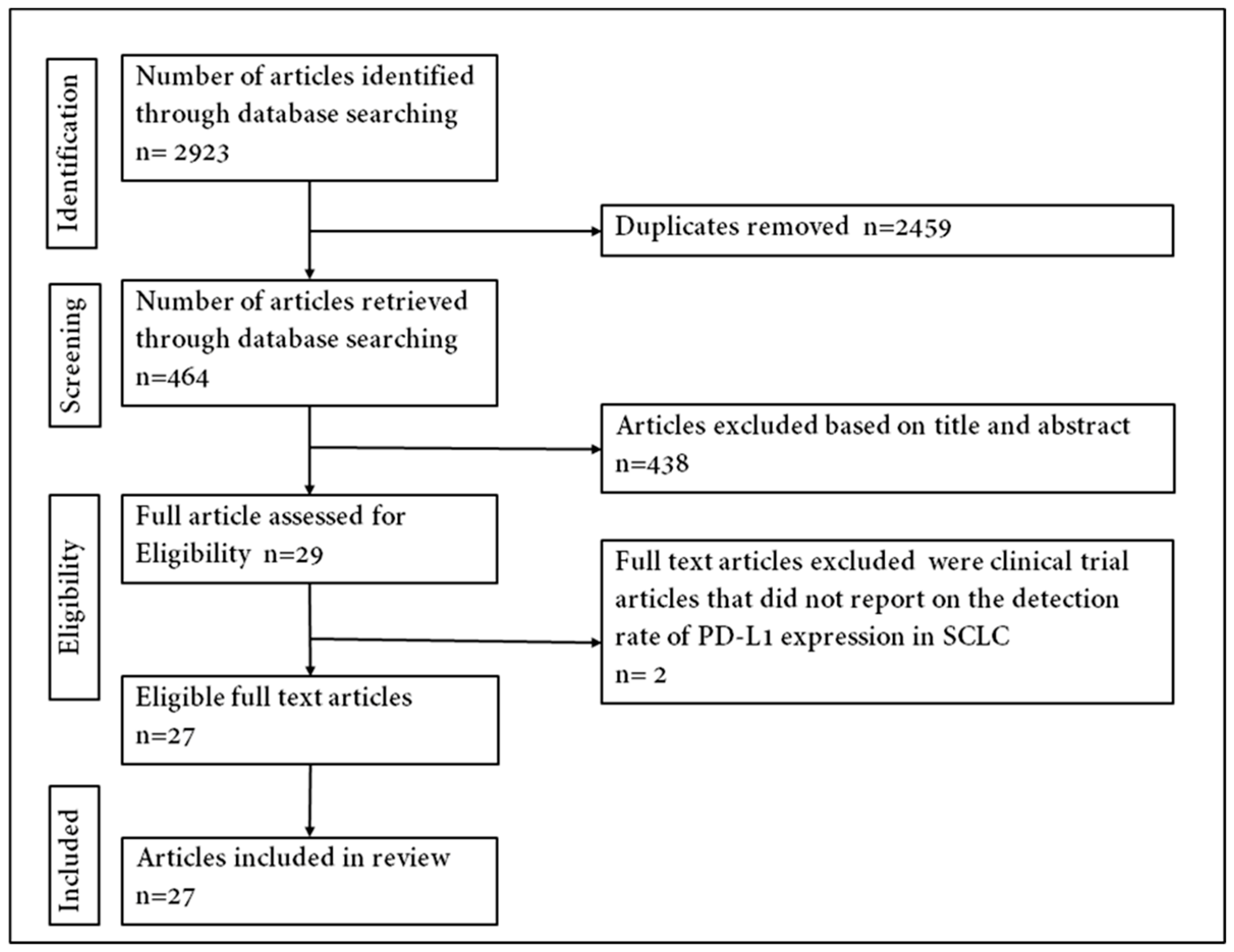
2.1. Search Strategy and Selection Criteria
2.2. Eligibility and Selection of Articles and Data Extraction
2.3. Data Analysis
3. Results
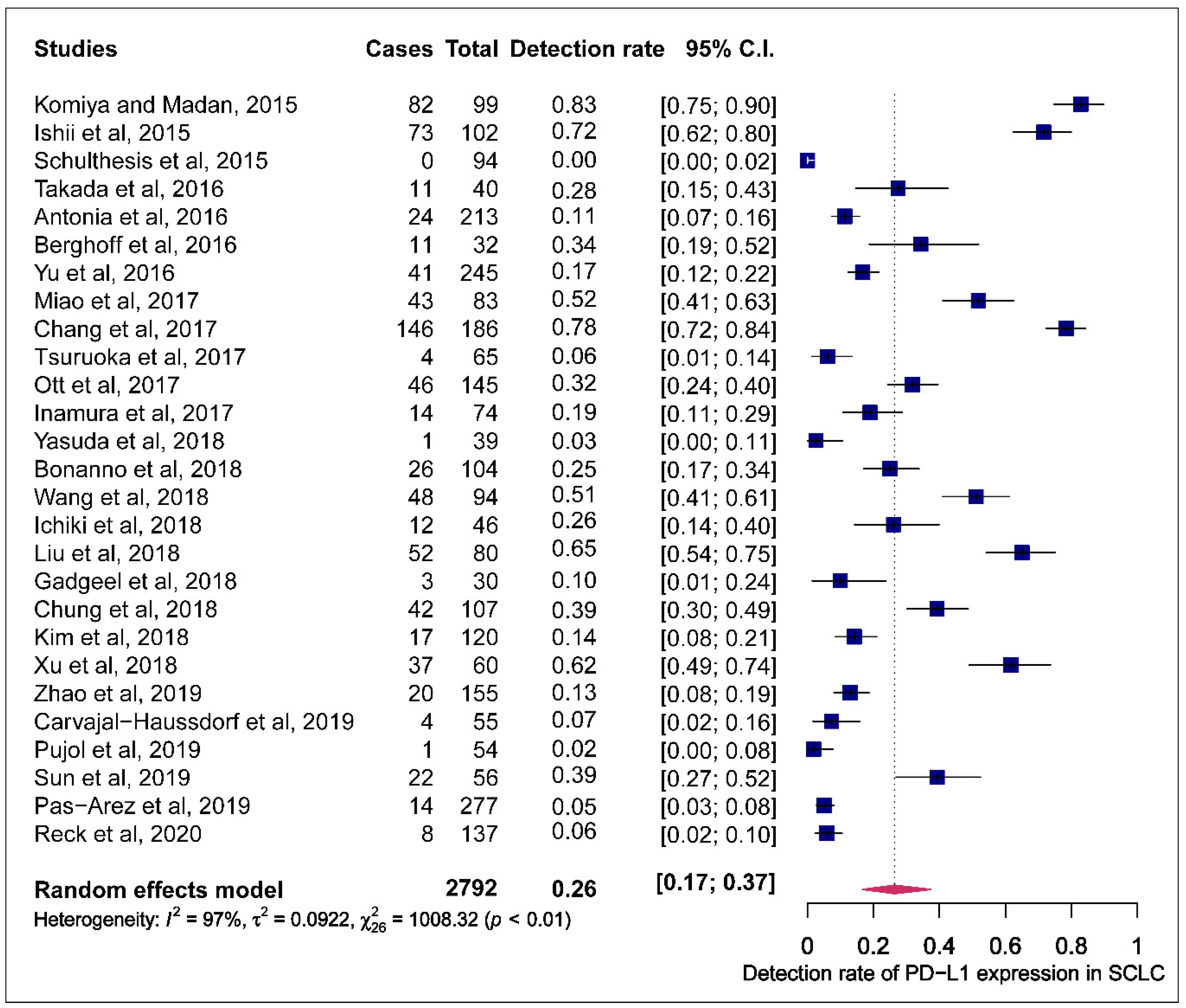
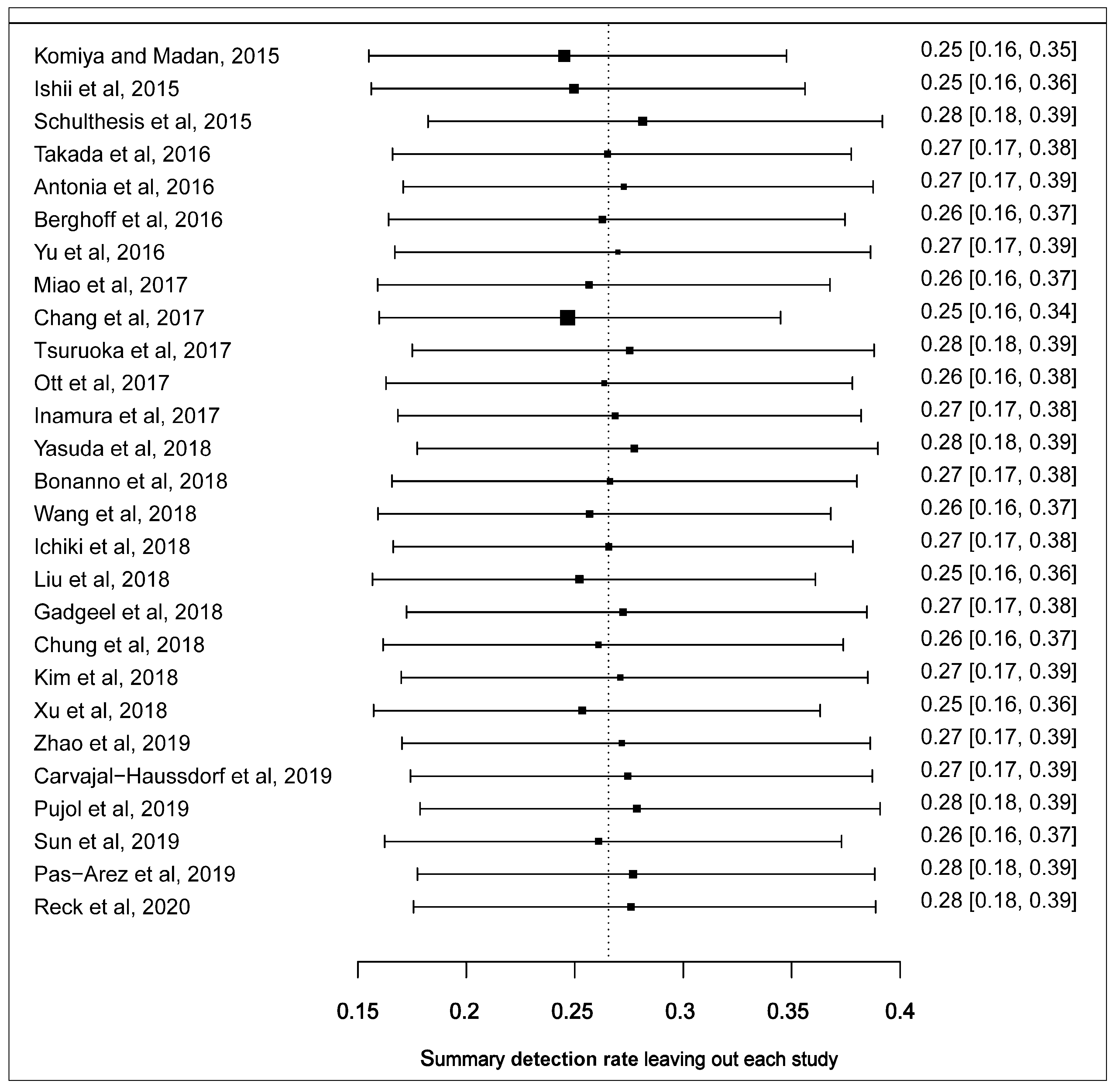
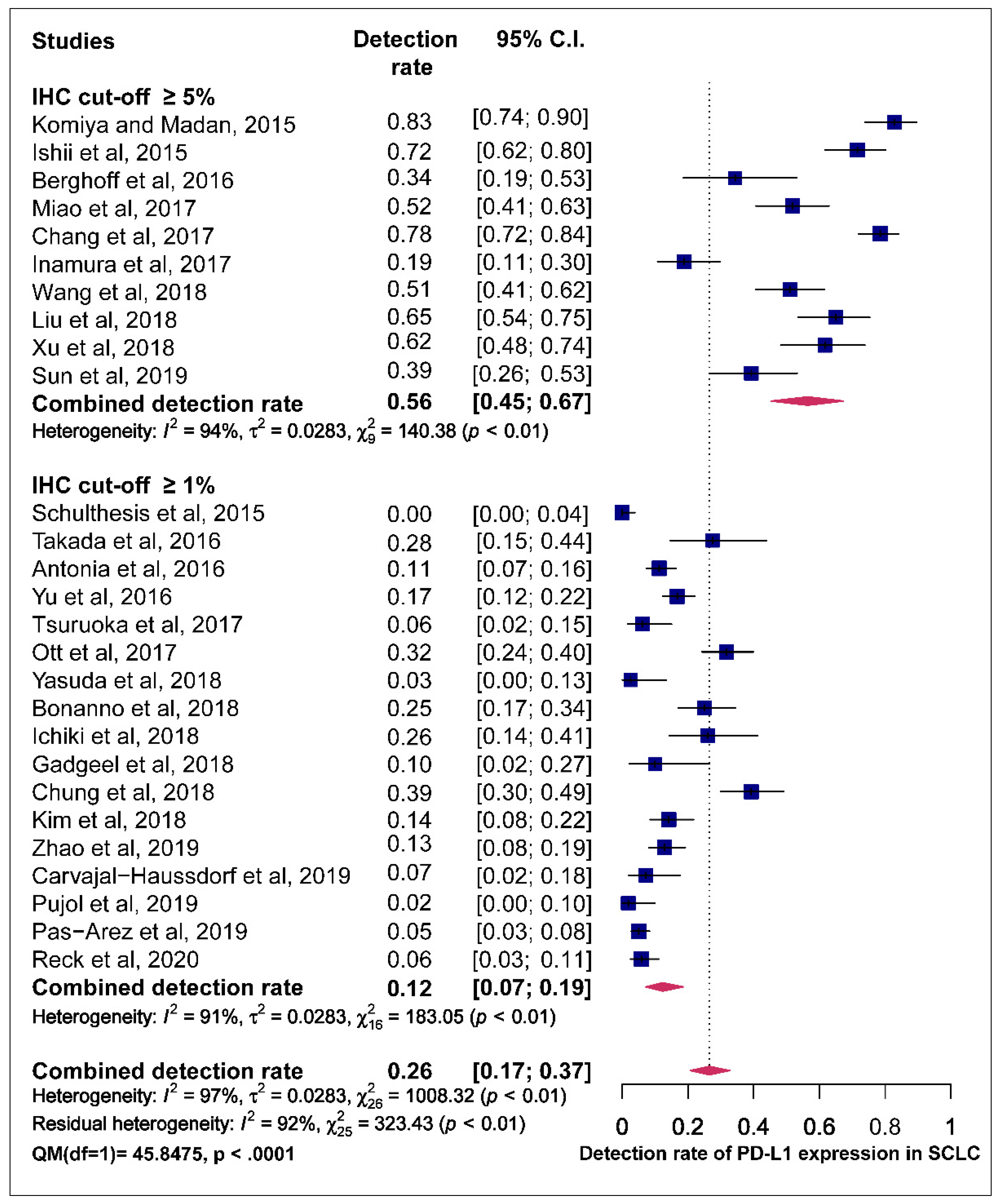
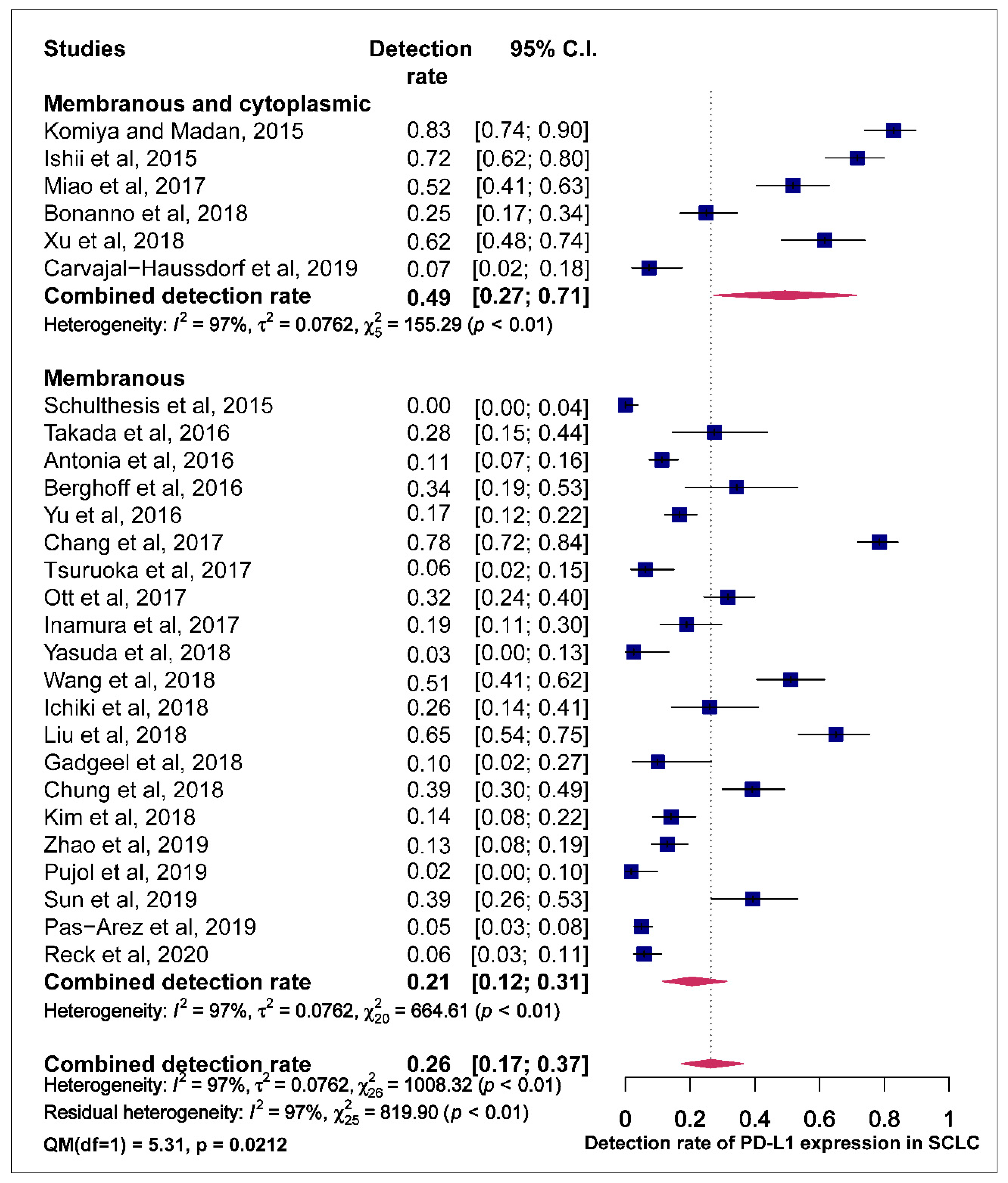
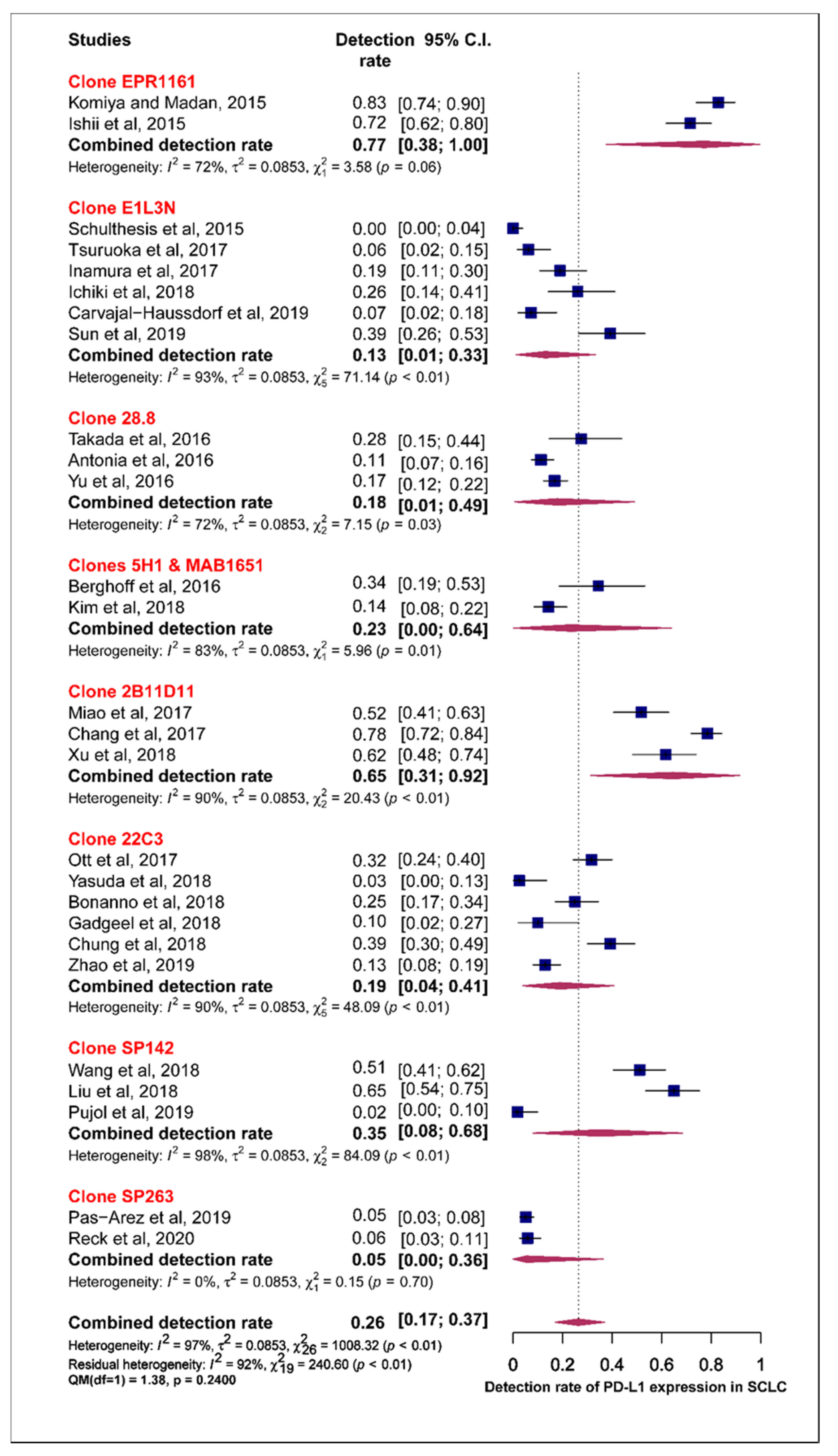
3.1. Prevalence of PD-L1 Expression in SCLC
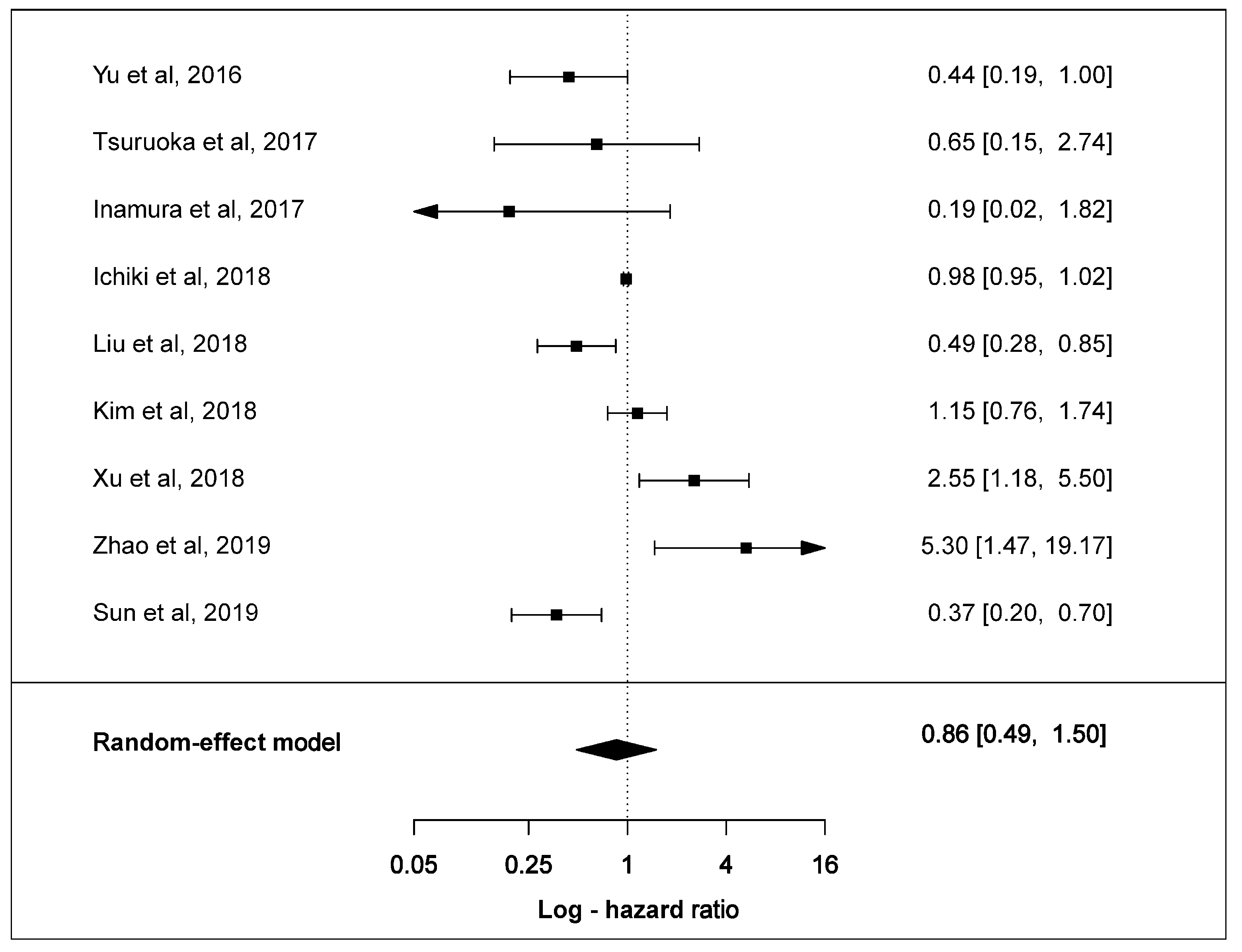
3.2. Effect of PD-L1 Expression in Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| PD-L1 | Programmed cell death ligand-1 |
| PD-1 | Programmed cell death-1 |
| SCLC | Small-cell lung cancer |
| NSCLC | Non-small cell lung cancer |
| ED-SCLC | Extensive diseased staged SCLC |
| TILS | Tumour infiltrating lymphocytes (TILs) |
| IHC | Immunohistochemistry |
| I2 | Heterogeneity |
| OS | Overall survival |
| HR | Hazard ratio |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D. Update on small cell carcinoma and its differentiation from squamous cell carcinoma and other non-small cell carcinomas. Mod. Pathol. 2012, 25, S18–S30. [Google Scholar] [CrossRef] [PubMed]
- Van Meerbeeck, J.P.; Fennell, D.A.; De Ruysscher, D.K. Small-cell lung cancer. Lancet 2011, 378, 1741–1755. [Google Scholar] [CrossRef]
- Lally, B.E.; Urbanic, J.J.; Blackstock, A.W.; Miller, A.A.; Perry, M.C. Small Cell Lung Cancer: Have We Made Any Progress Over the Last 25 Years? Oncology 2007, 12, 1096–1104. [Google Scholar] [CrossRef]
- Farago, A.F.; Keane, F.K. Current standards for clinical management of small cell lung cancer. Transl. Lung Cancer Res. 2018, 7, 69. [Google Scholar] [CrossRef]
- Pietanza, M.C.; Byers, L.A.; Minna, J.D.; Rudin, C.M. Small Cell Lung Cancer: Will Recent Progress Lead to Improved Outcomes? Clin. Cancer Res. 2015, 21, 2244–2255. [Google Scholar] [CrossRef]
- Jalal, S.I.; Lavin, P.; Lo, G.; Lebel, F.; Einhorn, L. Carboplatin and Etoposide With or Without Palifosfamide in Untreated Extensive-Stage Small-Cell Lung Cancer: A Multicenter, Adaptive, Randomized Phase III Study (MATISSE). J. Clin. Oncol. 2017, 35, 2619–2623. [Google Scholar] [CrossRef]
- Gelsomino, F.; Rossi, A.; Tiseo, M. MET and Small-Cell Lung Cancer. Cancers 2014, 6, 2100–2115. [Google Scholar] [CrossRef]
- Tiseo, M.; Boni, L.; Ambrosio, F.; Camerini, A.; Baldini, E.; Cinieri, S.; Brighenti, M.; Zanelli, F.; DeFraia, E.; Chiari, R.; et al. Italian, Multicenter, Phase III, Randomized Study of Cisplatin Plus Etoposide With or Without Bevacizumab as First-Line Treatment in Extensive-Disease Small-Cell Lung Cancer: The GOIRC-AIFA FARM6PMFJM Trial. J. Clin. Oncol. 2017, 35, 1281–1287. [Google Scholar] [CrossRef]
- Arriola, E.; Cañadas, I.; Arumí, M.; Rojo, F.; Rovira, A.; Albanell, J. Genetic changes in small cell lung carcinoma. Clin. Transl. Oncol. 2008, 10, 189–197. [Google Scholar] [CrossRef]
- Peifer, M.; Fernández-Cuesta, L.; Sos, M.L.; George, J.; Seidel, D.; Kasper, L.H.; Plenker, D.; Leenders, F.; Sun, R.; Zander, T.; et al. Integrative genome analyses identify key somatic driver mutations of small-cell lung cancer. Nat. Genet. 2012, 44, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Wistuba, I. Molecular genetics of small cell lung carcinoma. Semin. Oncol. 2001, 28, 3–13. [Google Scholar] [CrossRef]
- Mori, N.; Yokota, J.; Akiyama, T.; Sameshima, Y.; Okamoto, A.; Mizoguchi, H.; Toyoshima, K.; Sugimura, T.; Terada, M. Variable mutations of the RB gene in small-cell lung carcinoma. Oncogene 1990, 5, 1713–1717. [Google Scholar]
- William, W.N.; Glisson, B.S. Novel strategies for the treatment of small-cell lung carcinoma. Nat. Rev. Clin. Oncol. 2011, 8, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Spigel, D.R.; Socinski, M.A. Rationale for Chemotherapy, Immunotherapy, and Checkpoint Blockade in SCLC: Beyond Traditional Treatment Approaches. J. Thorac. Oncol. 2013, 8, 587–598. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef]
- Zhang, X.; Schwartz, J.-C.D.; Guo, X.; Bhatia, S.; Cao, E.; Chen, L.; Zhang, Z.-Y.; Edidin, M.A.; Nathenson, S.G.; Almo, S.C. Structural and functional analysis of the costimulatory receptor programmed death-1. Immunity 2004, 20, 337–347. [Google Scholar] [CrossRef]
- Riley, J.L. PD-1 signaling in primary T cells. Immunol. Rev. 2009, 229, 114–125. [Google Scholar] [CrossRef]
- Kazarian, M.; A Laird-Offringa, I. Small-cell lung cancer-associated autoantibodies: Potential applications to cancer diagnosis, early detection, and therapy. Mol. Cancer 2011, 10, 33. [Google Scholar] [CrossRef]
- Zaborowski, M.P.; Michalak, S. Cell-Mediated Immune Responses in Paraneoplastic Neurological Syndromes. Clin. Dev. Immunol. 2013, 2013, 1–11. [Google Scholar] [CrossRef]
- Rizvi, H.; Sanchez-Vega, F.; La, K.; Chatila, W.; Jonsson, P.; Halpenny, D.; Plodkowski, A.; Long, N.; Sauter, J.L.; Rekhtman, N.; et al. Molecular Determinants of Response to Anti–Programmed Cell Death (PD)-1 and Anti–Programmed Death-Ligand 1 (PD-L1) Blockade in Patients With Non–Small-Cell Lung Cancer Profiled With Targeted Next-Generation Sequencing. J. Clin. Oncol. 2018, 36, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Calvo, E.; López-Martín, J.; Bendell, J.; Eder, J.; Taylor, M.; Ott, P.; Pietanza, M.; Horn, L.; Jäger, D.; De Braud, F.; et al. 3098 Nivolumab (NIVO) monotherapy or in combination with ipilimumab (IPI) for treatment of recurrent small cell lung cancer (SCLC). Eur. J. Cancer 2015, 51, S633. [Google Scholar] [CrossRef]
- Ott, P.A.; Fernandez, M.E.E.; Hiret, S.; Kim, D.-W.; Moss, R.A.; Winser, T.; Yuan, S.; Cheng, J.D.; Piperdi, B.; Mehnert, J.M. Pembrolizumab (MK-3475) in patients (pts) with extensive-stage small cell lung cancer (SCLC): Preliminary safety and efficacy results from KEYNOTE-028. J. Clin. Oncol. 2015, 33, 7502. [Google Scholar] [CrossRef]
- Topalian, S.L.; Drake, C.G.; Pardoll, D.M. Immune Checkpoint Blockade: A Common Denominator Approach to Cancer Therapy. Cancer Cell 2015, 27, 450–461. [Google Scholar] [CrossRef]
- Antonia, S.J.; A López-Martin, J.; Bendell, J.; A Ott, P.; Taylor, M.; Eder, J.P.; Jäger, D.; Pietanza, M.C.; Le, D.T.; De Braud, F.; et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): A multicentre, open-label, phase 1/2 trial. Lancet Oncol. 2016, 17, 883–895. [Google Scholar] [CrossRef]
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-Line Atezolizumab plus Chemotherapy in Extensive-Stage Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Özgüroğlu, M.; Ji, J.H.; et al. Durvalumab plus platinum–etoposide versus platinum–etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): A randomised, controlled, open-label, phase 3 trial. Lancet 2019, 394, 1929–1939. [Google Scholar] [CrossRef]
- Yu, H.; Batenchuk, C.; Badzio, A.; Boyle, T.A.; Czapiewski, P.; Chan, D.C.; Lu, X.; Gao, D.; Ellison, K.; Kowalewski, A.A.; et al. PD-L1 Expression by Two Complementary Diagnostic Assays and mRNA In Situ Hybridization in Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 110–120. [Google Scholar] [CrossRef]
- Takada, K.; Toyokawa, G.; Okamoto, T.; Akamine, T.; Takamori, S.; Katsura, M.; Fujishita, T.; Shoji, F.; Oda, Y.; Maehara, Y. An Immunohistochemical Analysis of PD-L1 Protein Expression in Surgically Resected Small Cell Lung Cancer Using Different Antibodies and Criteria. Anticancer Res. 2016, 36, 3409–3412. [Google Scholar]
- Miao, L.; Lu, Y.; Xu, Y.; Zhang, G.; Huang, Z.; Gong, L.; Fan, Y. PD-L1 and c-MET expression and survival in patients with small cell lung cancer. Oncotarget 2017, 8, 53978–53988. [Google Scholar] [CrossRef][Green Version]
- Komiya, T.; Madan, R. PD-L1 expression in small cell lung cancer. Eur. J. Cancer 2015, 51, 1853–1855. [Google Scholar] [CrossRef] [PubMed]
- Schultheis, A.M.; Scheel, A.H.; Ozretić, L.; George, J.; Thomas, R.K.; Hagemann, T.; Zander, T.; Wolf, J.; Buettner, R. PD-L1 expression in small cell neuroendocrine carcinomas. Eur. J. Cancer 2015, 51, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, Y.; Ozasa, H.; Kim, Y.H. PD-L1 Expression in Small Cell Lung Cancer. J. Thorac. Oncol. 2018, 13, e40–e41. [Google Scholar] [CrossRef] [PubMed]
- Ishii, H.; Azuma, K.; Kawahara, A.; Yamada, K.; Imamura, Y.; Tokito, T.; Kinoshita, T.; Kage, M.; Hoshino, T. Significance of Programmed Cell Death-Ligand 1 Expression and its Association with Survival in Patients with Small Cell Lung Cancer. J. Thorac. Oncol. 2015, 10, 426–430. [Google Scholar] [CrossRef]
- McLaughlin, J.K.; Han, G.; Schalper, K.A.; Carvajal-Hausdorf, D.; Pelekanou, V.; Rehman, J.; Velcheti, V.; Herbst, R.S.; Lorusso, P.M.; Rimm, D.L. Quantitative Assessment of the Heterogeneity of PD-L1 Expression in Non–Small-Cell Lung Cancer. JAMA Oncol. 2016, 2, 46–54. [Google Scholar] [CrossRef]
- McLean, A.E.; Barnes, D.J.; Troy, L. Diagnosing Lung Cancer: The Complexities of Obtaining a Tissue Diagnosis in the Era of Minimally Invasive and Personalised Medicine. J. Clin. Med. 2018, 7, 163. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.D.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (Nos) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Ready, N.; Owonikoko, T.K.; Postmus, P.E.; Reck, M.; Peters, S.; Pieters, A.; Selvaggi, G.; Fairchild, J.P.; Govindan, R. CheckMate 451: A randomized, double-blind, phase III trial of nivolumab (nivo), nivo plus ipilimumab (ipi), or placebo as maintenance therapy in patients (pts) with extensive-stage disease small cell lung cancer (ED-SCLC) after first-line platinum-based doublet chemotherapy (PT-DC). J. Clin. Oncol. 2016, 34, TPS8579. [Google Scholar] [CrossRef]
- Horn, L.; Reck, M.; Gettinger, S.; Spigel, D.R.; Antonia, S.J.; Rupnow, B.A.; Pieters, A.; Selvaggi, G.; Fairchild, J.P.; Peters, S. CheckMate 331: An open-label, randomized phase III trial of nivolumab versus chemotherapy in patients (pts) with relapsed small cell lung cancer (SCLC) after first-line platinum-based chemotherapy (PT-DC). J. Clin. Oncol. 2016, 34, TPS8578. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Goldman, J.; Garassino, M.; Dvorkin, M.; Trukhin, D.; Statsenko, G.; Hotta, K.; Ji, J.; Hochmair, M.; Voitko, O.; et al. PD-L1 expression, patterns of progression and patient-reported outcomes (PROs) with durvalumab plus platinum-etoposide in ES-SCLC: Results from CASPIAN. Ann. Oncol. 2019, 30, v928–v929. [Google Scholar] [CrossRef]
- Reck, M.; Liu, S.; Mansfield, A.; Mok, T.; Scherpereel, A.; Reinmuth, N.; Garassino, M.; De Carpeno, J.; Califano, R.; Nishio, M.; et al. IMpower133: Updated overall survival (OS) analysis of first-line (1L) atezolizumab (atezo) + carboplatin + etoposide in extensive-stage SCLC (ES-SCLC). Ann. Oncol. 2019, 30, v710–v711. [Google Scholar] [CrossRef]
- Carvajal-Hausdorf, D.; Altan, M.; Velcheti, V.; Gettinger, S.N.; Herbst, R.S.; Rimm, D.L.; Schalper, K.A. Expression and clinical significance of PD-L1, B7-H3, B7-H4 and TILs in human small cell lung Cancer (SCLC). J. Immunother. Cancer 2019, 7, 65. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-L.; Yang, C.-Y.; Huang, Y.-L.; Wu, C.-T.; Yang, P.-C. High PD-L1 expression is associated with stage IV disease and poorer overall survival in 186 cases of small cell lung cancers. Oncotarget 2017, 8, 18021. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sun, J.-M.; Zhou, W.; Choi, Y.-L.; Choi, S.-J.; Kim, S.E.; Wang, Z.; Dolled-Filhart, M.; Emancipator, K.; Wu, D.; Weiner, R.; et al. Prognostic Significance of PD-L1 in Patients with Non–Small Cell Lung Cancer: A Large Cohort Study of Surgically Resected Cases. J. Thorac. Oncol. 2016, 11, 1003–1011. [Google Scholar] [CrossRef]
- Inamura, K.; Yokouchi, Y.; Kobayashi, M.; Ninomiya, H.; Sakakibara, R.; Nishio, M.; Okumura, S.; Ishikawa, Y. Relationship of tumor PD-L1 (CD274) expression with lower mortality in lung high-grade neuroendocrine tumor. Cancer Med. 2017, 6, 2347–2356. [Google Scholar] [CrossRef]
- Tsuruoka, K.; Horinouchi, H.; Goto, Y.; Kanda, S.; Fujiwara, Y.; Nokihara, H.; Yamamoto, N.; Asakura, K.; Nakagawa, K.; Sakurai, H.; et al. PD-L1 expression in neuroendocrine tumors of the lung. Lung Cancer 2017, 108, 115–120. [Google Scholar] [CrossRef]
- Bonanno, L.; Pavan, A.; Dieci, M.; Di Liso, E.; Schiavon, M.; Comacchio, G.; Attili, I.; Pasello, G.; Calabrese, F.; Rea, F.; et al. The role of immune microenvironment in small-cell lung cancer: Distribution of PD-L1 expression and prognostic role of FOXP3-positive tumour infiltrating lymphocytes. Eur. J. Cancer 2018, 101, 191–200. [Google Scholar] [CrossRef]
- Berghoff, A.S.; Ricken, G.; Wilhelm, D.; Rajky, O.; Widhalm, G.; Dieckmann, K.; Birner, P.; Bartsch, R.; Preusser, M. Tumor infiltrating lymphocytes and PD-L1 expression in brain metastases of small cell lung cancer (SCLC). J. Neuro Oncol. 2016, 130, 19–29. [Google Scholar] [CrossRef]
- Gadgeel, S.M.; Pennell, N.A.; Fidler, M.J.; Halmos, B.; Bonomi, P.; Stevenson, J.; Schneider, B.; Sukari, A.; Ventimiglia, J.; Chen, W.; et al. Phase II Study of Maintenance Pembrolizumab in Patients with Extensive-Stage Small Cell Lung Cancer (SCLC). J. Thorac. Oncol. 2018, 13, 1393–1399. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Lee, J.H.; Nam, S.J.; Ock, C.-Y.; Moon, J.-W.; Yoo, C.W.; Lee, G.K.; Han, J.-Y. Association of PD-L1 Expression with Tumor-Infiltrating Immune Cells and Mutation Burden in High-Grade Neuroendocrine Carcinoma of the Lung. J. Thorac. Oncol. 2018, 13, 636–648. [Google Scholar] [CrossRef]
- Wang, H.; Li, Z.; Dong, B.; Sun, W.; Yang, X.; Liu, R.; Zhou, L.; Huang, X.; Jia, L.; Lin, D. Prognostic significance of PD-L1 expression and CD8+ T cell infiltration in pulmonary neuroendocrine tumors. Diagn. Pathol. 2018, 13, 30. [Google Scholar] [CrossRef]
- Ichiki, Y.; Matsumiya, H.; Mori, M.; Kanayama, M.; Nabe, Y.; Taira, A.; Shinohara, S.; Kuwata, T.; Takenaka, M.; Hirai, A.; et al. Predictive factors of postoperative survival among patients with pulmonary neuroendocrine tumor. J. Thorac. Dis. 2018, 10, 6912–6920. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Lu, Z.; Wang, W.; Sun, X. Programmed death-ligand 1 positivity can predict improved survival and a lower risk of brain metastasis in patients with resectable small cell lung cancer. Oncol. Lett. 2018, 16, 2373–2381. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.C.; Lopez-Martin, J.A.; Kao, S.C.-H.; Miller, W.H.; Ros, W.; Gao, B.; Marabelle, A.; Gottfried, M.; Zer, A.; Delord, J.-P.; et al. Phase 2 study of pembrolizumab in advanced small-cell lung cancer (SCLC): KEYNOTE-158. J. Clin. Oncol. 2018, 36, 8506. [Google Scholar] [CrossRef]
- Xu, Y.; Cui, G.; Jiang, Z.; Li, N.; Zhang, X. Survival analysis with regard to PD-L1 and CD155 expression in human small cell lung cancer and a comparison with associated receptors. Oncol. Lett. 2019, 17, 2960–2968. [Google Scholar] [CrossRef]
- Zhao, X.; Kallakury, B.; Chahine, J.J.; Hartmann, D.; Zhang, Y.; Chen, Y.; Zhang, H.; Zhang, B.; Wang, C.; Giaccone, G. Surgical Resection of SCLC: Prognostic Factors and the Tumor Microenvironment. J. Thorac. Oncol. 2019, 14, 914–923. [Google Scholar] [CrossRef]
- Pujol, J.-L.; Greillier, L.; Audigier-Valette, C.; Moro-Sibilot, D.; Uwer, L.; Hureaux, J.; Guisier, F.; Carmier, D.; Madelaine, J.; Otto, J.; et al. A Randomized Non-Comparative Phase II Study of Anti-Programmed Cell Death-Ligand 1 Atezolizumab or Chemotherapy as Second-Line Therapy in Patients With Small Cell Lung Cancer: Results From the IFCT-1603 Trial. J. Thorac. Oncol. 2019, 14, 903–913. [Google Scholar] [CrossRef]
- Armstrong, S.A.; Liu, S.V. Immune Checkpoint Inhibitors in Small Cell Lung Cancer: A Partially Realized Potential. Adv. Ther. 2019, 36, 1826–1832. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Mutational landscape determines sensitivity to PD-1 blockade in non–small cell lung cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.-L. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef]
- George, J.; Lim, J.S.; Jang, S.J.; Cun, Y.; Ozretić, L.; Kong, G.; Leenders, F.; Lu, X.; Fernández-Cuesta, L.; Bosco, G.; et al. Comprehensive genomic profiles of small cell lung cancer. Nat. Cell Biol. 2015, 524, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xiaoxia, C.; Likun, H.; Jun, Q.; Tao, J.; Caicun, Z.; Maciej, C.; Yuchen, B.; Bai, Y.; Hou, L.; et al. PD-L1 expression and its effect on clinical outcomes of EGFR-mutant NSCLC patients treated with EGFR-TKIs. Cancer Biol. Med. 2018, 15, 434–442. [Google Scholar] [CrossRef]
- Cooper, W.A.; Tran, T.; Vilain, R.E.; Madore, J.; Selinger, C.I.; Kohonencorish, M.R.J.; Yip, P.; Yu, B.; O’Toole, S.A.; McCaughan, B.C.; et al. PD-L1 expression is a favorable prognostic factor in early stage non-small cell carcinoma. Lung Cancer 2015, 89, 181–188. [Google Scholar] [CrossRef]
- Schmidt, L.H.; Kümmel, A.; Görlich, D.; Mohr, M.; Bröckling, S.; Mikesch, J.H.; Grünewald, I.; Marra, A.; Schultheis, A.M.; Wardelmann, E. PD-1 and PD-L1 expression in NSCLC indicate a favorable prognosis in defined subgroups. PLoS ONE 2015, 10, e0136023. [Google Scholar] [CrossRef] [PubMed]
- Lantuejoul, S.; Damotte, D.; Hofman, V.; Adam, J. Programmed death ligand 1 immunohistochemistry in non-small cell lung carcinoma. J. Thorac. Dis. 2019, 11 (Suppl. 1), S89–S101. [Google Scholar] [CrossRef]
- Scheel, A.H.; Dietel, M.; Heukamp, L.C.; Jöhrens, K.; Kirchner, T.; Reu, S.; Rüschoff, J.; Schildhaus, H.-U.; Schirmacher, P.; Tiemann, M.; et al. Harmonized PD-L1 immunohistochemistry for pulmonary squamous-cell and adenocarcinomas. Mod. Pathol. 2016, 29, 1165–1172. [Google Scholar] [CrossRef]
- Rimm, D.L.; Han, G.; Taube, J.M.; Yi, E.S.; Bridge, J.A.; Flieder, D.B.; Homer, R.; West, W.W.; Wu, H.; Roden, A.C.; et al. A Prospective, Multi-institutional, Pathologist-Based Assessment of 4 Immunohistochemistry Assays for PD-L1 Expression in Non–Small Cell Lung Cancer. JAMA Oncol. 2017, 3, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, F.R.; McElhinny, A.; Stanforth, D.; Ranger-Moore, J.; Jansson, M.; Kulangara, K.; Richardson, W.; Towne, P.; Hanks, D.; Vennapusa, B.; et al. PD-L1 Immunohistochemistry Assays for Lung Cancer: Results from Phase 1 of the Blueprint PD-L1 IHC Assay Comparison Project. J. Thorac. Oncol. 2017, 12, 208–222. [Google Scholar] [CrossRef]
- Tsao, M.S.; Kerr, K.M.; Kockx, M.; Beasley, M.-B.; Borczuk, A.C.; Botling, J.; Bubendorf, L.; Chirieac, L.; Chen, G.; Chou, T.-Y.; et al. PD-L1 immunohistochemistry comparability study in real-life clinical samples: Results of Blueprint phase 2 project. J. Thorac. Oncol. 2018, 13, 1302–1311. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.-W.; Felip, E.; Pérez-Gracia, J.L.; Joo-Hang, K.; Molina, J.; Kim, J.-H.; Arvis, C.D.; Ahn, M.-J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Phillips, T.; Simmons, P.; Inzunza, H.D.; Cogswell, J.; Novotny, J.; Taylor, C.; Zhang, X. Development of an Automated PD-L1 Immunohistochemistry (IHC) Assay for Non–Small Cell Lung Cancer. Appl. Immunohistochem. Mol. Morphol. 2015, 23, 541–549. [Google Scholar] [CrossRef]
- Rebelatto, M.C.; Midha, A.; Mistry, A.; Sabalos, C.; Schechter, N.; Li, X.; Jin, X.; Steele, K.E.; Robbins, P.B.; Blake-Haskins, J.A.; et al. Development of a programmed cell death ligand-1 immunohistochemical assay validated for analysis of non-small cell lung cancer and head and neck squamous cell carcinoma. Diagn. Pathol. 2016, 11, 1–14. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Wu, P.; Wu, D.; Li, L.; Chai, Y.; Huang, J. PD-L1 and Survival in Solid Tumors: A Meta-Analysis. PLoS ONE 2015, 10, e0131403. [Google Scholar] [CrossRef] [PubMed]
- Pan, Z.-K.; Ye, F.; Wu, X.; An, H.-X.; Wu, J.-X. Clinicopathological and prognostic significance of programmed cell death ligand1 (PD-L1) expression in patients with non-small cell lung cancer: A meta-analysis. J. Thorac. Dis. 2015, 7, 462. [Google Scholar]
- Wang, A.; Wang, H.; Liu, Y.; Zhao, M.; Zhang, H.; Lu, Z.; Fang, Y.; Chen, X.; Liu, G. The prognostic value of PD-L1 expression for non-small cell lung cancer patients: A meta-analysis. Eur. J. Surg. Oncol. EJSO 2015, 41, 450–456. [Google Scholar] [CrossRef]
- Ota, K.; Azuma, K.; Kawahara, A.; Hattori, S.; Iwama, E.; Tanizaki, J.; Harada, T.; Matsumoto, K.; Takayama, K.; Takamori, S. Induction of PD-L1 expression by the EML4–ALK oncoprotein and downstream signaling pathways in non-small cell lung cancer. Clin. Cancer Res. 2015, 21, 4014–4021. [Google Scholar] [CrossRef]
- Zhang, M.; Li, G.; Wang, Y.; Wang, Y.; Zhao, S.; Haihong, P.; Zhao, H. PD-L1 expression in lung cancer and its correlation with driver mutations: A meta-analysis. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Killian, J.K.; Walker, R.L.; Suuriniemi, M.; Jones, L.; Scurci, S.; Singh, P.; Cornelison, R.; Harmon, S.; Boisvert, N.; Zhu, J.; et al. Archival fine-needle aspiration cytopathology (FNAC) samples: Untapped resource for clinical molecular profiling. J. Mol. Diagn. 2010, 12, 739–745. [Google Scholar] [CrossRef]
- Coley, S.M.; Crapanzano, J.P.; Saqi, A. FNA, core biopsy, or both for the diagnosis of lung carcinoma: Obtaining sufficient tissue for a specific diagnosis and molecular testing. Cancer Cytopathol. 2015, 123, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M. Detection of circulating tumor DNA in early-and late-stage human malignancies. Sci. Transl. Med. 2014, 6. [Google Scholar] [CrossRef]
- Malapelle, U.; Pisapia, P.; Rocco, D.; Smeraglio, R.; Di Spirito, M.; Bellevicine, C.; Troncone, G. Next generation sequencing techniques in liquid biopsy: Focus on non-small cell lung cancer patients. Transl. Lung Cancer Res. 2016, 5, 505–510. [Google Scholar] [CrossRef]
- Hodgkinson, C.L.; Morrow, C.J.; Li, Y.; Metcalf, R.L.; Rothwell, D.G.; Trapani, F.; Polanski, R.; Burt, D.J.; Simpson, K.L.; Morris, K.; et al. Tumorigenicity and genetic profiling of circulating tumor cells in small-cell lung cancer. Nat. Med. 2014, 20, 897–903. [Google Scholar] [CrossRef]
- Hamilton, G.; Moser, D.; Hochmair, M.J. Metastasis: Circulating Tumor Cells in Small Cell Lung Cancer. Trends Cancer 2016, 2, 159–160. [Google Scholar] [CrossRef]
- Acheampong, E.; Spencer, I.; Lin, W.; Ziman, M.; Millward, M.; Gray, E.S. Is the Blood an Alternative for Programmed Cell Death Ligand 1 Assessment in Non-Small Cell Lung Cancer? Cancers 2019, 11, 920. [Google Scholar] [CrossRef]
- Boffa, D.; Graf, R.P.; Salazar, M.C.; Hoag, J.; Lu, D.; Krupa, R.; Louw, J.; Dugan, L.; Wang, Y.; Landers, M.; et al. Cellular Expression of PD-L1 in the Peripheral Blood of Lung Cancer Patients is Associated with Worse Survival. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1139–1145. [Google Scholar] [CrossRef]
- Guibert, N.; Delaunay, M.; Lusque, A.; Boubekeur, N.; Rouquette, I.; Clermont, E.; Mourlanette, J.; Gouin, S.; Dormoy, I.; Favre, G.; et al. PD-L1 expression in circulating tumor cells of advanced non-small cell lung cancer patients treated with nivolumab. Lung Cancer 2018, 120, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Szafer-Glusman, E.; Hofman, V.; Chamorey, E.; Lalvée, S.; Selva, E.; Leroy, S.; Marquette, C.-H.; Kowanetz, M.; Hedge, P.; et al. Detection of PD-L1 in circulating tumor cells and white blood cells from patients with advanced non-small-cell lung cancer. Ann. Oncol. 2018, 29, 193–199. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References (Sample Size) | Samples | Stage of Disease | Antibody | IHC/QIF Evaluation (%) | PD-L1 Positivity Rate (%) | Prognosis (Cut-off Value, mOS, HR and p-Value) |
|---|---|---|---|---|---|---|
| Ott et al. 2017 [23] (n = 145) | Biopsy tissue (n = 132) Fresh tissue (n = 12) | Extensive | Clone 22C3 antibody (Merck & Co, Kenilworth, NJ, USA) | Membranous ≥ 1% | 31.7% (46/145) | n/a |
| Antonia et al., 2016 [25] (n = 213) | Biopsy tissue | Extensive | Clone 28-8; Epitomics Inc, Burlingame, CA, USA) | Membranous ≥ 1% | 11.3% (24/213) | n/a |
| Yu et al., 2016 [28] (n = 249) | Biopsy tissue | Extensive (n = 96) Limited (n = 98) | Clone SP142 Dako clone 28.8 pharmDx kit | Membranous ≥ 1% | 16.5 (41/245) | ≥1% PD-L1/TPS, mOS: 9.87 vs. 16.13 months, Log rank test p = 0.0511 HR = 0.44 (95% CI 0.18–1.07, p = 0.055 |
| Takada et al., 2016 [29] (n = 40) | Surgically-resected tissue | n/a | Clone E1L3N (Cell Signalling Technology, Cambridge, UK), | E1LN–membranous Allred, ≥1%, ≥5% | 22.5%, 27.5% 35.0% | N/E |
| Clone 28.8 (Abcam Cambridge, UK) Clone SP142, Spring Bioscience, Ventana Tuscon, AZ, USA) | 28.8-membranous Allred, ≥1%, ≥5% SP142-membranous Allred, ≥1%, ≥5% | 20.5%, 27.0%, 32.5% 15.%, 15.0%, 15.0% | N/E | |||
| Miao et al., 2017 [30] (n = 83) | Biopsy tissue | Extensive (n = 36) Limited (n = 47) | Clone 2B11D11/PD-L1/CD274 antibody, Clone SP66, SPRINGBIO, USA) | Membranous and/or cytoplasmic ≥ 5% | 51.8% (43/83) | ≥5% PD-L1/TPS (mOS, 17.0 vs. 9.0, Log rank test p = 0.018) HR not provided |
| Komiya and Madan, 2015 [31] (n = 99) | Unknown | n/a | EPR1161 (Abcam, Cambridge, UK) | Membranous and/or cytoplasmic ≥ 5% | 82.8% (82/99) | NE |
| Schultheis et al., 2015 [32] (n = 94) | Surgically-resected (n = 51), Biopsy (n = 43) | Extensive (n = 49), Limited (n = 49) | Clone 5H1 (Lieping Chen Laboratory, Yale University, New Haven, CT, USA) Clone E1L3N (Cell Signalling Technology, Cambridge, UK) | Membranous ≥ 1%, | 0.0% (0/94) | NE |
| Yasuda et al., 2018 [33] (n = 39) | Biopsy tissue | Extensive | Clone 22C3 pharmDX (Agilent Technologies, Santa Clara, CA, USA) 22C3 (Dako, Carptintera, CA, USA) | Membranous ≥ 1% | 2.5% (1/39) | N/E |
| Ishii et al., 2015 [34] (n = 102) | Biopsy tissue | Extensive (n = 61), Limited (n = 41) | EPR1161 (Abcam, Cambridge, UK) | Membranous and/or cell-surface ≥ 5% | 71.6% (73/102) | ≥5% PD-L1/TPS mOS: 16.3 vs. 7.3 months Log-rank test p < 0.001 HR not provided |
| Pas-Ares et al., 2019 [43] (n = 277) | Biopsy tissue | Extensive | Clone SP263 Ventana PD-L1 Assay | Membranous ≥ 1% | 5.1 (14/277) | n/a |
| Reck et al., 2020 [44] (n = 137) | Biopsy tissue | Extensive | Clone SP263 Ventana PD-L1 Assay | Membranous ≥ 1% | 5.8 (8/137) | n/a |
| Carvajal-Hausdorf et al., 2019 [45] (n = 55) | n/a | Limited (n = 23) Extensive (n = 32) | Clone E1L3N (Cell Signalling Technology, Cambridge, UK), | Membranous and/or cytoplasmic ≥ 1% | 7.3% (4/55) | NE |
| Chang et al., 2017 [46] (n = 186) | Biopsy tissue | Limited (n = 74) Extensive (112) | Clone 2B11D11, PD-L1/CD274 antibody (Cat/no.66248-1-Ig) Proteintech Group Inc Chicago, IL, USA | Membranous ≥ 5% | 78.0% (145/186) | HR = 0.17 (95% CI: 0.08–0.35, p < 0.001) |
| Sun et al., 2019 [47] (n = 56) | Surgically-resected/biopsy tissue | Limited (n = 25) Extensive (n = 31) | Clone E1L3N, diluted 1:100; #13684, Cell Signalling Technology) | Membranous ≥ 5% | 39.3% (22/56) | Overall survival (OS) ≥ 5% HR = 0.37(95% CI: 0.21–0.68), p = 0.002 |
| Inamura et al., 2017 [48] (n = 74) | Surgically-resected tissue | Extensive | Clone E1L3N (Cell Signalling Technology, Cambridge, UK), | Membranous ≥ 5% | 18.9% (14/74) | Lung-cancer-specific survival months, HR = 0.11 (95% CI: 0.006–0.52, p = 0.0020) Overall Survival (OS): HR = 0.19(95% CI: 0.10–1.30, p = 0.150) |
| Tsuruoka et al., 2017 [49] (n = 65) | Biopsy/cytology | Limited | Clone E1L3N (Cell Signalling Technology, Cambridge, UK), | Membranous ≥ 1% | 5.8% (4/65) | ≥1% PD-L1/TPS, mOS (38 vs. 140 months) Log rank test p = 0.067) HR= 0.65(95% CI: 0.16–2.71, p = 0.557) |
| Bonanno et al., 2018 [50] (n = 104) | Surgically-resected (n = 48) Biopsy tissue (n = 66) | Limited (n = 66) Extensive (n = 38) | Clone 22C3 (Dako, Carptintera, CA, USA) | Membranous ≥ 1% | 25.0% (26/104) | NE |
| Berghoff et al., 2016 [51] (n = 32) | Biopsy tissue | Extensive | Clone 5H1 (Lieping Chen Laboratory, Yale University, USA) (Dako, Glostrup, Denmark) | Membranous ≥ 5% | 34.4 (11/32) | ≥5% PD-L1/TPS mOS: 8 vs. 7 months Log rank test p = 0.662 HR not provided |
| Gadgeel et al., 2018 [52] (n = 30) | Biopsy tissue | Extensive | Clone 22C3 antibody (Dako, Carpinteria, CA, USA). | Membranous ≥ 1% | 10.0% (3/30) | n/a |
| Kim et al. 2018 [53] (n = 120) | Biopsy tissue | Limited (n = 39) Extensive (n = 81) | MAB1561/B7-H1/PD-L1 antibody (R&D Systems, Minneapolis, MN, USA | Membranous ≥ 1% | 14.2% (17/120) | ≥1% PD-L1/TPS, mOS: 12.0 vs. 18.0 months, HR = 1.15 (95% CI 0.76–1.73, p = 0.510 |
| Wang et al., 2018 [54] (n = 94) | Biopsy tissue | Extensive (n = 52) | Clone SP142; ZSGB-BIO, Beijing, China | Membranous and/or cytoplasmic ≥ 5% | 51.1% (48/94) | NE |
| Ichiki et al., 2018 [55] (n = 46) | Surgically-resected | Limited (n = 12) Extensive (n = 34) | Clone E1L3N, 1:800, Cell Signalling Technology, Inc., Danvers, MA, USA) | Membranous ≥ 1% | 26.1% (12/46) | Overall Survival (OS): HR = 0.98 (0.94–1.02), p = 0.268 |
| Liu et al., 2018 [56] (n = 80) | Surgically-resected | Limited (n = 80) | Clone SP142 (cat. no. 07309554001; 1:100; Spring Bioscience Corporation, Pleasanton, CA, USA | Membranous ≥ 5% | 65.0% (52/80) | Overall survival (OS) ≥ 5% HR = 0.49 (95% CI: 0.28–0.85), p = 0.0110 |
| Chung et al. 2018 [57] (n = 107) | Biopsy tissue | Extensive | Clone 22C3 pharmDx assay (Agilent Technologies) | Membranous ≥ 1% | 39.0% (42/107) | n/a |
| Xu et al., 2019 [58] (n = 60) | Surgically-resected | Limited (n = 20) Extensive (n = 40) | Clone 2B11D11 PD-L1/CD274 antibody (cat. no. 66248-1-Ig) (ProteinTech Group, Inc., Chicago, IL, USA) | Membranous and/or cytoplasmic ≥ 5% | 61.7% (37/60) | ≥5% PD-L1/TPS, mOS (22.13 vs. 22.03 months) Log rank test p = 0.781) HR = 2.55 (95% CI: 01.18–5.51), p = 0.017 |
| Zhao et al., 2019 [59] (n = 155) | Surgically-resected | Limited (n = 52) Extensive (n = 103) | Clone 22C3, PharmDx | Membranous ≥ 1% | 12.9% (20/155) | ≥5% PD-L1/TPS, mOS (12 vs. 57 months, Lo g rank test p = 0.007) HR= 5.30 (95% CI: 1.45–19.28), p = 0.011 |
| Pujol et al., 2018 [60] (n = 54) | Biopsy tissue | Extensive | SP142 PD-L1 immunohistochemistry assay (Ventana Medical Systems, Inc., Tucson, AZ, USA) | Membranous ≥ 1% | 1.8% (1/54) | n/a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acheampong, E.; Abed, A.; Morici, M.; Bowyer, S.; Amanuel, B.; Lin, W.; Millward, M.; S. Gray, E. Tumour PD-L1 Expression in Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis. Cells 2020, 9, 2393. https://doi.org/10.3390/cells9112393
Acheampong E, Abed A, Morici M, Bowyer S, Amanuel B, Lin W, Millward M, S. Gray E. Tumour PD-L1 Expression in Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis. Cells. 2020; 9(11):2393. https://doi.org/10.3390/cells9112393
Chicago/Turabian StyleAcheampong, Emmanuel, Afaf Abed, Michael Morici, Samantha Bowyer, Benhur Amanuel, Weitao Lin, Michael Millward, and Elin S. Gray. 2020. "Tumour PD-L1 Expression in Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis" Cells 9, no. 11: 2393. https://doi.org/10.3390/cells9112393
APA StyleAcheampong, E., Abed, A., Morici, M., Bowyer, S., Amanuel, B., Lin, W., Millward, M., & S. Gray, E. (2020). Tumour PD-L1 Expression in Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis. Cells, 9(11), 2393. https://doi.org/10.3390/cells9112393