
Encephalitis in Patients with COVID-19: A Systematic Evidence-Based Analysis

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Guideline
2.2. Search Strategies
2.3. Eligibility Criteria
2.4. Study Screening and Selection
2.5. Data Extraction
2.6. Quality Assessment
3. Results
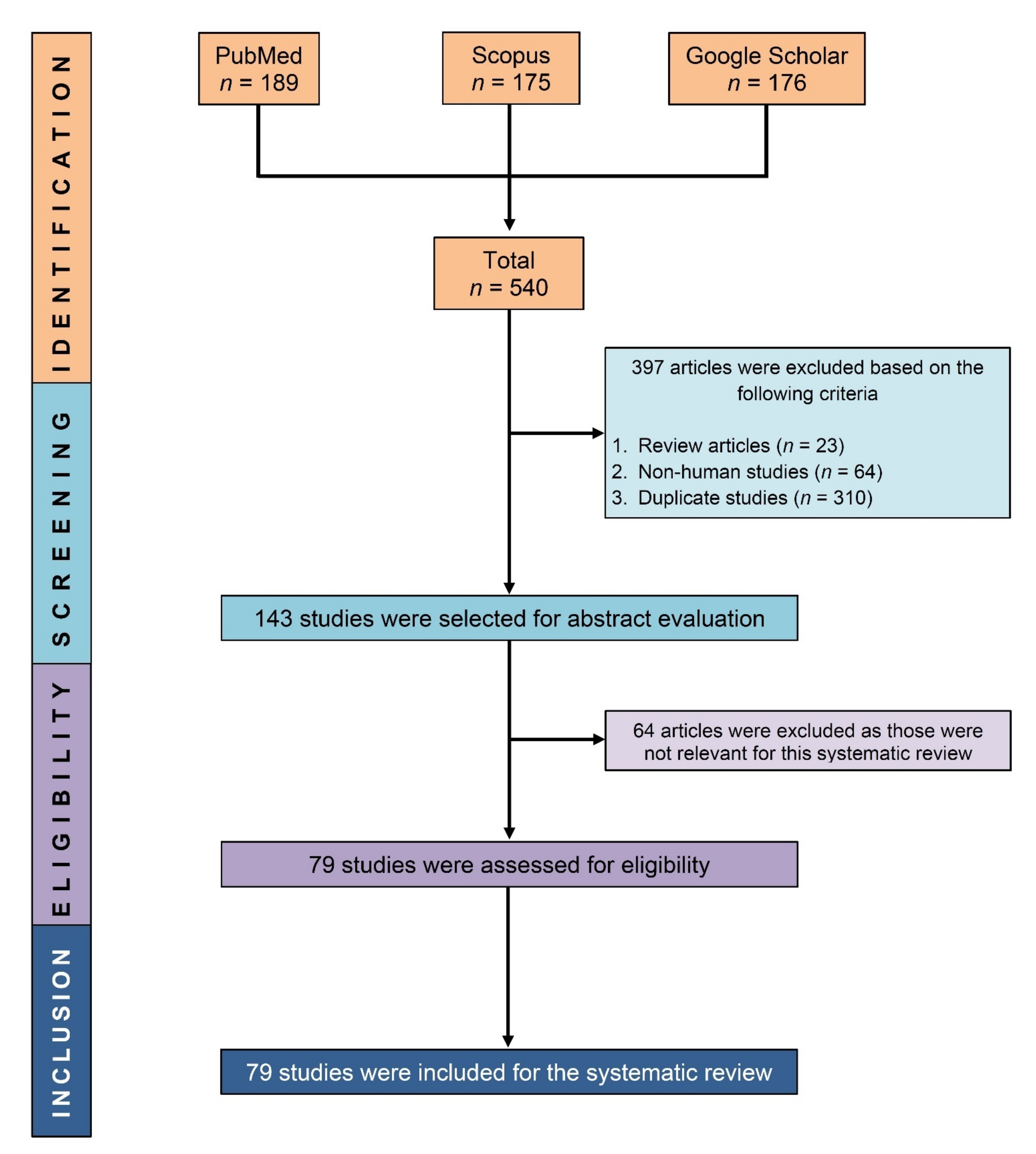
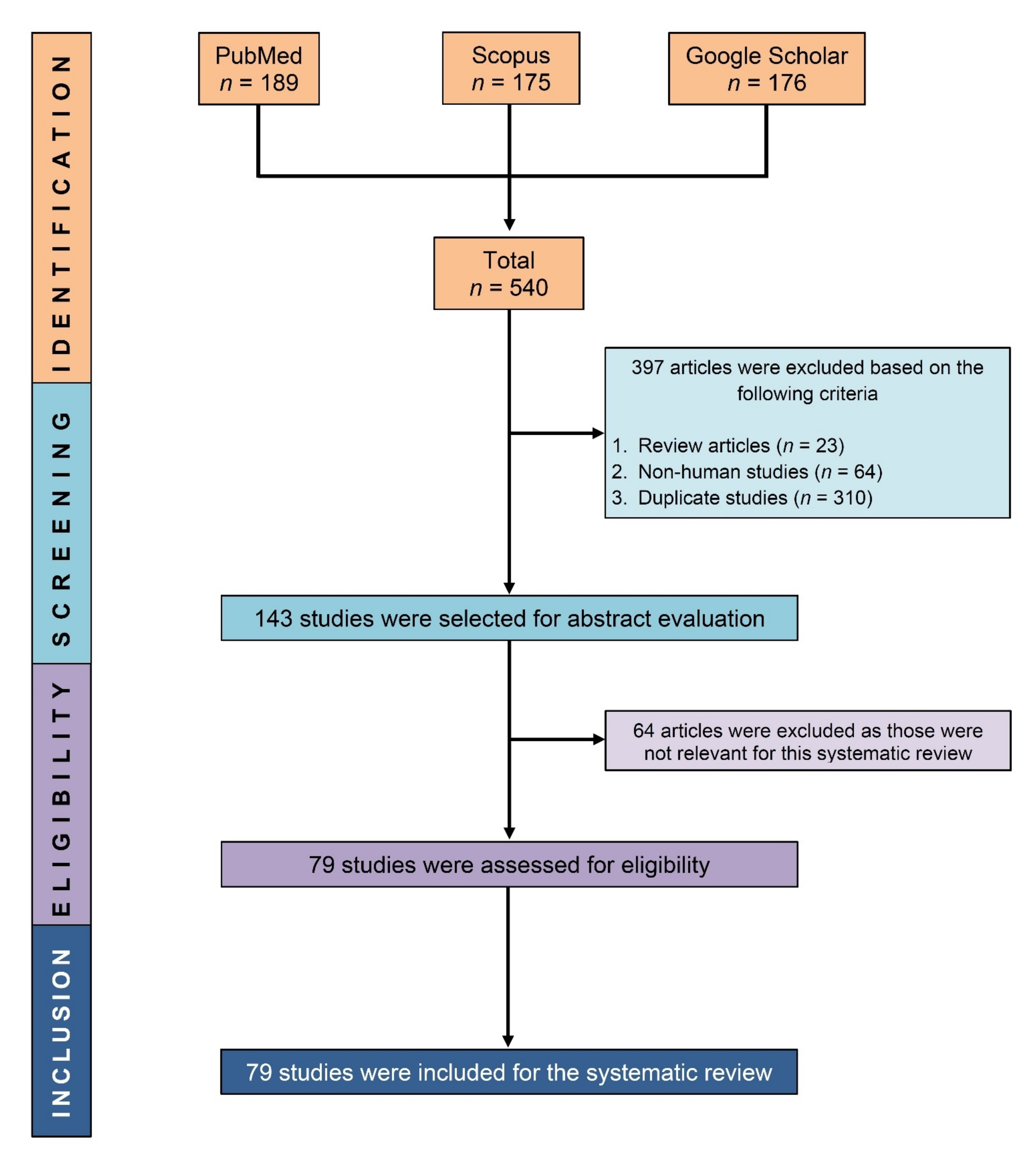
3.1. Study Selection
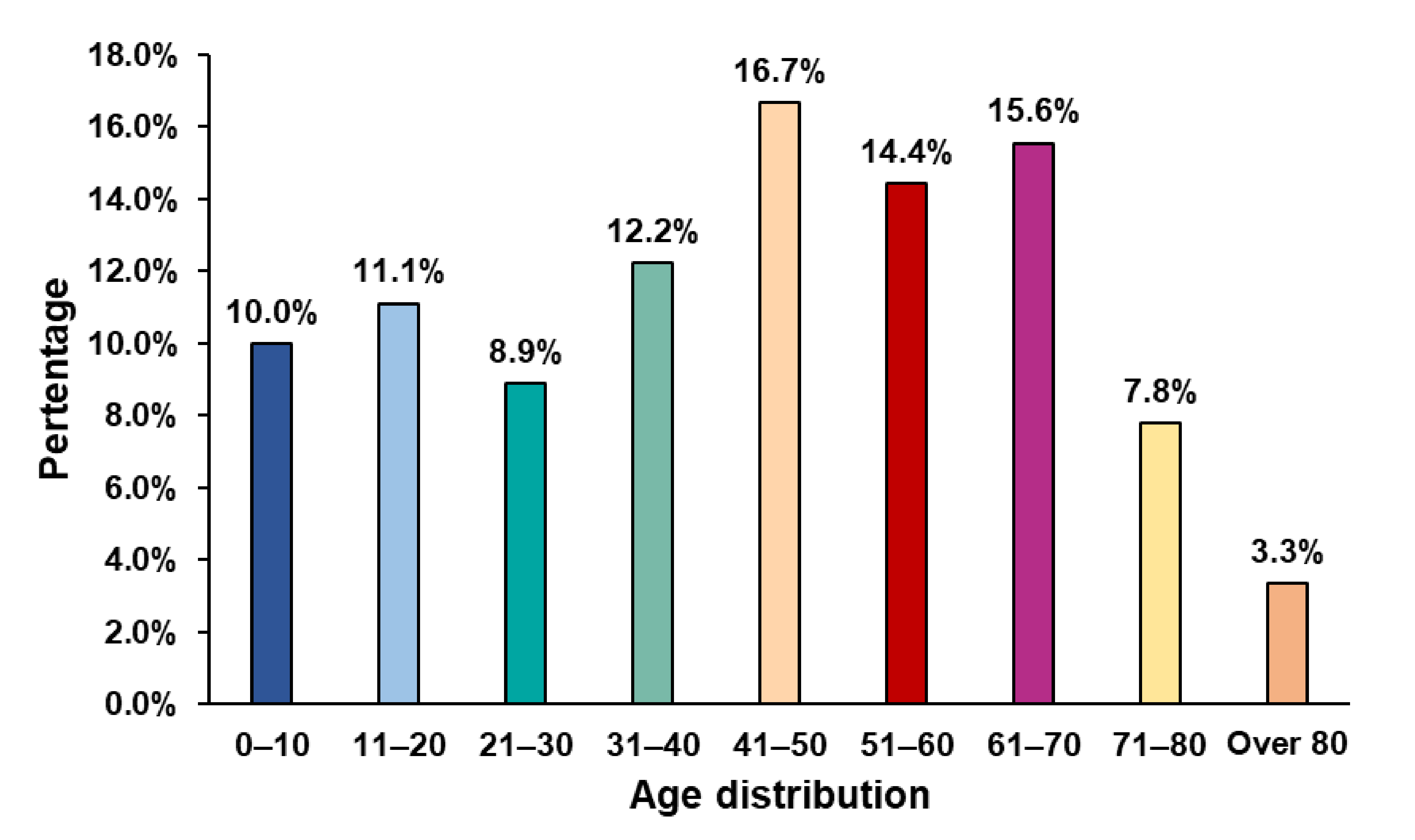
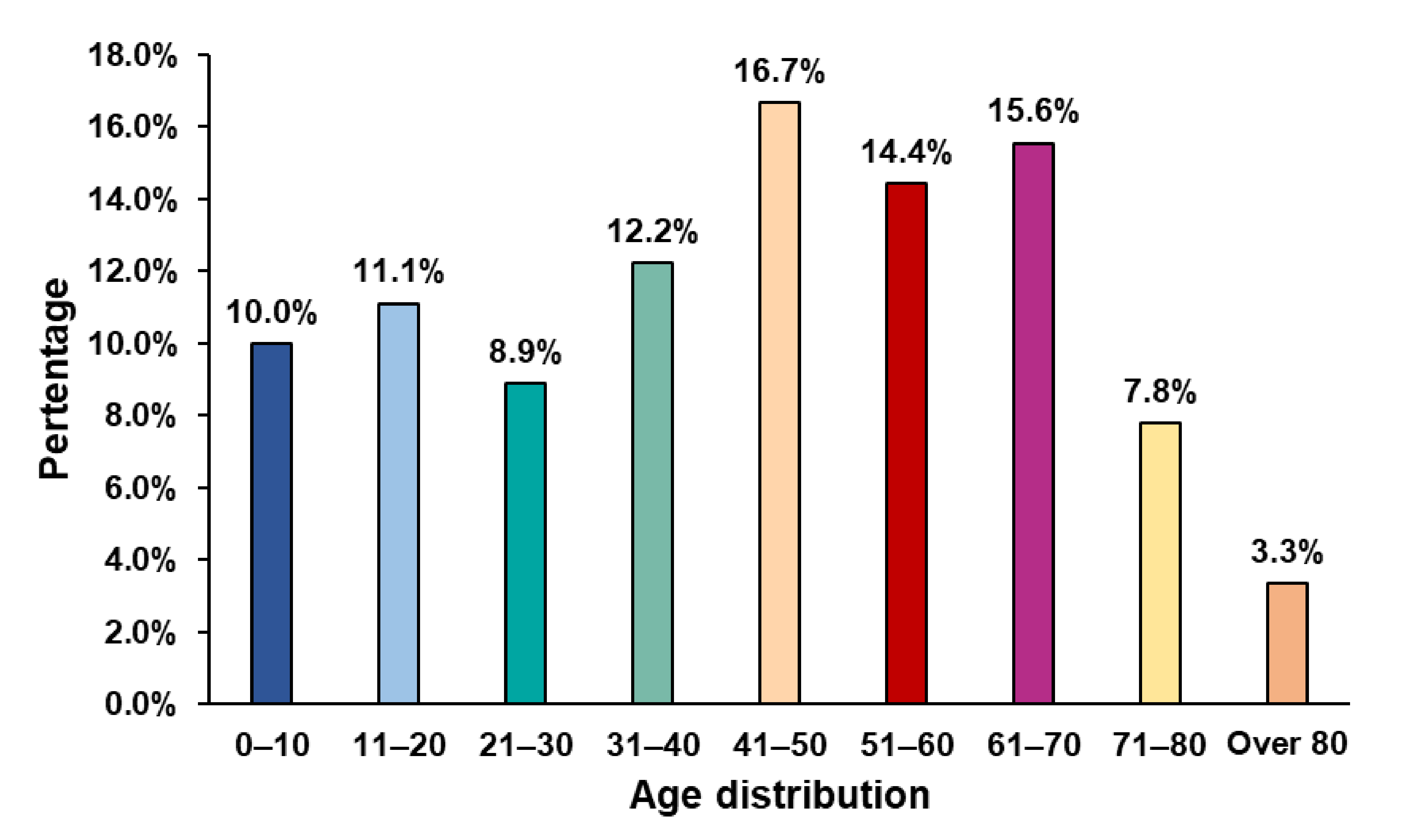
3.2. General Characteristics of the Included Studies
3.3. Evidence-Based Analyses
3.3.1. Infant to Children with COVID-19
3.3.2. Adolescents with COVID-19
3.3.3. Adults with COVID-19
Initial Presentation with Neurological and Respiratory Symptoms
Neurological and Psychiatric Manifestations
Particular Case of COVID-Linked Encephalitis
Managing Severe Cases
3.4. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO COVID-19 Dashboard. 2022. Available online: https://covid19.who.int (accessed on 9 August 2022).
- Zhou, Z.; Kang, H.; Li, S.; Zhao, X. Understanding the neurotropic characteristics of SARS-CoV-2: From neurological manifestations of COVID-19 to potential neurotropic mechanisms. J. Neurol. 2020, 267, 2179–2184. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Kundu, S.; Alam, S.S.; Hossan, T.; Kamal, M.A.; Hassan, R. Prevalence and characteristics of fever in adult and paediatric patients with coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis of 17515 patients. PLoS ONE 2021, 16, e0249788. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, F.; Fahriani, M.; Mamada, S.S.; Frediansyah, A.; Abubakar, A.; Maghfirah, D.; Fajar, J.K.; Maliga, H.A.; Ilmawan, M.; Bin Emran, T.; et al. Global prevalence of prolonged gastrointestinal symptoms in COVID-19 survivors and potential pathogenesis: A systematic review and meta-analysis. F1000Research 2021, 10, 301. [Google Scholar] [CrossRef] [PubMed]
- Cares-Marambio, K.; Montenegro-Jiménez, Y.; Torres-Castro, R.; Vera-Uribe, R.; Torralba, Y.; Alsina-Restoy, X.; Vasconcello-Castillo, L.; Vilaró, J. Prevalence of potential respiratory symptoms in survivors of hospital admission after coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Chronic Respir. Dis. 2021, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Saniasiaya, J.; Islam, A.; Abdullah, B. Prevalence and Characteristics of Taste Disorders in Cases of COVID-19: A Meta-analysis of 29,349 Patients. Otolaryngol. Neck Surg. 2020, 165, 33–42. [Google Scholar] [CrossRef]
- Saniasiaya, J.; Islam, A.; Abdullah, B. Prevalence of Olfactory Dysfunction in Coronavirus Disease 2019 (COVID-19): A Meta-analysis of 27,492 Patients. Laryngoscope 2020, 131, 865–878. [Google Scholar] [CrossRef]
- Islam, A.; Alam, S.S.; Kundu, S.; Hossan, T.; Kamal, M.A.; Cavestro, C. Prevalence of Headache in Patients with Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of 14,275 Patients. Front. Neurol. 2020, 11, 562634. [Google Scholar] [CrossRef]
- Natarajan, S.; Ganesh, R.; Palaniappan, N.; Kannan, L. SARS-CoV-2 Encephalitis in an Adolescent Girl. Indian Pediatr. 2020, 57, 1186–1187. [Google Scholar] [CrossRef]
- McAbee, G.N.; Brosgol, Y.; Pavlakis, S.; Agha, R.; Gaffoor, M. Encephalitis Associated with COVID-19 Infection in an 11-Year-Old Child. Pediatr. Neurol. 2020, 109, 94. [Google Scholar] [CrossRef]
- Zanin, L.; Saraceno, G.; Renisi, G.; Signorini, L.; Battaglia, L.; Ferrara, M.; Rasulo, F.A.; Panciani, P.P.; Fontanella, M.M. Delayed onset of fatal encephalitis in a COVID-19 positive patient. Int. J. Neurosci. 2021, 1–4. [Google Scholar] [CrossRef]
- Espíndola, O.M.; Brandão, C.O.; Gomes, Y.C.P.; Siqueira, M.; Soares, C.N.; Lima, M.A.S.D.; Leite, A.C.C.B.; Torezani, G.; Araujo, A.Q.C.; Silva, M.T.T. Cerebrospinal fluid findings in neurological diseases associated with COVID-19 and insights into mechanisms of disease development. Int. J. Infect. Dis. 2020, 102, 155–162. [Google Scholar] [CrossRef]
- Bodnar, B.; Patel, K.; Ho, W.; Luo, J.J.; Hu, W. Cellular mechanisms underlying neurological/neuropsychiatric manifestations of COVID-19. J. Med. Virol. 2020, 93, 1983–1998. [Google Scholar] [CrossRef]
- Venkatesan, A.; Geocadin, R.G. Diagnosis and management of acute encephalitis: A practical approach. Neurol. Clin. Pract. 2014, 4, 206–215. [Google Scholar] [CrossRef]
- Ellul, M.; Solomon, T. Acute encephalitis–diagnosis and management. Clin. Med. 2018, 18, 155. [Google Scholar] [CrossRef]
- Moriguchi, T.; Harii, N.; Goto, J.; Harada, D.; Sugawara, H.; Takamino, J.; Ueno, M.; Sakata, H.; Kondo, K.; Myose, N.; et al. A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int. J. Infect. Dis. 2020, 94, 55–58. [Google Scholar] [CrossRef]
- Abildúa, A.; Atienza, S.; Monteiro, G.; Aguirre, M.; Aguayo, L.; Álvarez, E.; García-Azorín, D.; Montesinos, I.; Lezama, L.; Pérez, M. Encephalopathy and encephalitis during acute SARS-CoV-2 infection. Spanish Society of Neurology COVID-19 Registry. Neurologia 2021, 36, 127–134. [Google Scholar] [CrossRef]
- Page, M.J.; E McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemio. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Ahsan, N.; Jafarpour, S.; Santoro, J.D. Myelin oligodendrocyte glycoprotein antibody encephalitis following severe acute respiratory syndrome coronavirus 2 in a pediatric patient. Clin. Exp. Pediatr. 2021, 64, 310–312. [Google Scholar] [CrossRef]
- Allahyari, F.; Hosseinzadeh, R.; Nejad, J.H.; Heiat, M.; Ranjbar, R. A case report of simultaneous autoimmune and COVID-19 encephalitis. J. Neurovirol. 2021, 27, 504–506. [Google Scholar] [CrossRef]
- Andrea, M.; Christian, M.; Lorenzo, M.; Francesco, D.; Walter, A.; Marco, M.; Andreina, B.; Maria, G.A.; Paolo, G.; Daniela, D.G.; et al. Unusual Presentation of COVID-19: Encephalitis and Syndrome of Inappropriate Anti-Diuretic Hormone Secretion. Int. J. Clin. Med. 2020, 11, 559–564. [Google Scholar] [CrossRef]
- Ayatollahi, P.; Tarazi, A.; Wennberg, R. Possible autoimmune encephalitis with claustrum sign in case of acute SARS-CoV-2 infection. Can. J. Neurol. Sci. 2021, 48, 430–432. [Google Scholar] [CrossRef]
- Ayuningtyas, T.; Natadidjaja, R.I.; Octaviani, C.; Sahli, F.; Adlani, H. Confirmed severe acute respiratory syndrome coronavirus 2 encephalitis in cerebrospinal fluid: A case report. J. Med Case Rep. 2022, 16, 1–4. [Google Scholar] [CrossRef]
- Ayuso, L.L.; Rubio, P.T.; Rosário, R.F.B.D.; Arroyo, M.L.G.; Sierra-Hidalgo, F. Bickerstaff encephalitis after COVID-19. J. Neurol. 2020, 268, 2035–2037. [Google Scholar] [CrossRef]
- Babar, A.; Lewandowski, U.; Capin, I.; Khariton, M.; Venkataraman, A.; Okolo, N.; Sharma, D. SARS-CoV-2 encephalitis in a 20-year old healthy female. Pediatr. Infect. Dis. J. 2020, 39, 320–321. [Google Scholar] [CrossRef]
- Benameur, K.; Agarwal, A.; Auld, S.C.; Butters, M.P.; Webster, A.S.; Ozturk, T.; Howell, J.C.; Bassit, L.C.; Velasquez, A.; Schinazi, R.F.; et al. Encephalopathy and Encephalitis Associated with Cerebrospinal Fluid Cytokine Alterations and Coronavirus Disease, Atlanta, Georgia, USA, 2020. Emerg. Infect. Dis. 2020, 26, 2016–2021. [Google Scholar] [CrossRef]
- Bernard-Valnet, R.; Pizzarotti, B.; Anichini, A.; Demars, Y.; Russo, E.; Schmidhauser, M.; Cerutti-Sola, J.; Rossetti, A.O.; Du Pasquier, R. Two patients with acute meningoencephalitis concomitant with SARS-CoV-2 infection. Eur. J. Neurol. 2020, 27, 43–44. [Google Scholar] [CrossRef]
- Bhavsar, S.M.; Agarwal, S.; Lewis, R.; Ganta, A.; Roshchina, Y.S.; Clouser, K.N.; Baer, A.Z.; Gliksman, F.; Piwoz, J.A. COVID-19 Infection Associated With Encephalitis in an Adolescent. Neurol. Clin. Pract. 2020, 11, e189–e192. [Google Scholar] [CrossRef]
- Bodro, M.; Compta, Y.; Llansó, L.; Esteller, D.; Doncel-Moriano, A.; Mesa, A.; Rodríguez, A.; Sarto, J.; Martínez-Hernandez, E.; Vlagea, A. Increased CSF levels of IL-1β, IL-6, and ACE in SARS-CoV-2–associated encephalitis. Neurology 2020, 7, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Burr, T.; Barton, C.; Doll, E.; Lakhotia, A.; Sweeney, M. N-Methyl-d-Aspartate Receptor Encephalitis Associated With COVID-19 Infection in a Toddler. Pediatr. Neurol. 2020, 114, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Cao, A.; Rohaut, B.; Le Guennec, L.; Saheb, S.; Marois, C.; Altmayer, V.; Carpentier, V.T.; Nemlaghi, S.; Soulie, M.; Morlon, Q.; et al. Severe COVID-19-related encephalitis can respond to immunotherapy. Brain 2020, 143, e102. [Google Scholar] [CrossRef] [PubMed]
- Casez, O.; Willaume, G.; Grand, S.; Nemoz, B.; Lupo, J.; Kahane, P.; Brion, J.-P. Teaching NeuroImages: SARS-CoV-2–Related Encephalitis: MRI Pattern of Olfactory Tract Involvement. Neurology 2021, 96, 645–646. [Google Scholar] [CrossRef] [PubMed]
- Chalil, A.; Baker, C.S.; Johnston, R.B.; Just, C.; Debicki, D.B.; Mayich, M.S.; Bosma, K.J.; Steven, D.A. Acute Hemorrhagic Encephalitis Related to COVID-19. Neurol. Clin. Pract. 2020, 11, e147–e151. [Google Scholar] [CrossRef] [PubMed]
- Cheraghali, F.; Tahamtan, A.; Hosseini, S.A.; Gharib, M.H.; Moradi, A.; Razavi Nikoo, H.; Tabarraei, A. Case report: Detection of SARS-CoV-2 from cerebrospinal fluid in a 34-month-old child with encephalitis. Front. Pediatrics 2021, 9, 565778. [Google Scholar] [CrossRef]
- Dahshan, A.; Abdellatef, A.A. Autoimmune encephalitis as a complication of COVID-19 infection: A case report. Egypt. J. Intern. Med. 2022, 34, 1–3. [Google Scholar] [CrossRef]
- Dono, F.; Carrarini, C.; Russo, M.; De Angelis, M.V.; Anzellotti, F.; Onofrj, M.; Bonanni, L. New-onset refractory status epilepticus (NORSE) in post SARS-CoV-2 autoimmune encephalitis: A case report. Neurol. Sci. 2021, 42, 35–38. [Google Scholar] [CrossRef]
- Duong, L.; Xu, P.; Liu, A. Meningoencephalitis without respiratory failure in a young female patient with COVID-19 infection in Downtown Los Angeles, early April 2020. Brain Behav. Immun. 2020, 87, 33. [Google Scholar] [CrossRef]
- Huang, Y.H.; Jiang, D.; Huang, J.T. SARS-CoV-2 Detected in Cerebrospinal Fluid by PCR in a Case of COVID-19 Encephalitis. Brain Behav. Immun. 2020, 87, 149. [Google Scholar] [CrossRef]
- Durovic, E.; Bien, C.; Bien, C.G.; Isenmann, S. MOG antibody-associated encephalitis secondary to Covid-19: Case report. BMC Neurol. 2021, 21, 1–5. [Google Scholar] [CrossRef]
- Efe, I.E.; Aydin, O.U.; Alabulut, A.; Çelik, O.; Aydin, K. COVID-19−Associated Encephalitis Mimicking Glial Tumor. World Neurosurg. 2020, 140, 46–48. [Google Scholar] [CrossRef]
- El Aoud, S.; Sorial, D.; Selmaoui, A.; Menif, I.; Lazard, M.; Hocine, M.S.; Thomas, L. A first case of Mild Encephalitis with Reversible Splenial Lesion (MERS) as a presenting feature of SARS-CoV-2. Rev. Neurol. 2021, 177, 139–141. [Google Scholar] [CrossRef]
- Elmouhib, A.; Benramdane, H.; Ahsayen, F.Z.; El Haddad, I.A.; El Ghalet, A.; Laaribi, I.; Bkiyar, H.; Nasri, S.; Skiker, I.; Housni, B. A case of limbic encephalitis associated with severely COVID-19 infection. Ann. Med. Surg. 2022, 74, 103274. [Google Scholar] [CrossRef]
- Esmaeili, S.; Abbasi, M.H.; Mojtahed, M.; Emamikhah, M.; Makiani, M.J.; Nazarian, H.; Mirzaasgari, Z. Acute disseminated encephalitis (ADEM) as the first presentation of COVID-19; a case report. Ann. Med. Surg. 2022, 77, 103511. [Google Scholar] [CrossRef]
- Etemadifar, M.; Salari, M.; Murgai, A.A.; Hajiahmadi, S. Fulminant encephalitis as a sole manifestation of COVID-19. Neurol. Sci. 2020, 41, 3027–3029. [Google Scholar] [CrossRef]
- Ferdosian, F.; Mohsenolhoseini, Z.; Fallah, R. Encephalitis Associated With COVID-19 in A 7-year-old Boy: A Case Report. Case Rep. Clin. Pract. 2022, 6, 246–250. [Google Scholar] [CrossRef]
- Freire-Álvarez, E.; Guillén, L.; Lambert, K.; Baidez, A.; García-Quesada, M.; Andreo, M.; Alom, J.; Masiá, M.; Gutiérrez, F. COVID-19-associated encephalitis successfully treated with combination therapy. Clin. Infect. Pract. 2020, 7–8, 100053. [Google Scholar] [CrossRef]
- Gaughan, M.; Connolly, S.; O’Riordan, S.; Tubridy, N.; McGuigan, C.; Kinsella, J.A. Pediatric Parainfectious Encephalitis Associated With COVID-19. Neurology 2021, 96, 541–544. [Google Scholar] [CrossRef]
- Ghosh, R.; Dubey, S.; Finsterer, J.; Chatterjee, S.; Ray, B.K. SARS-CoV-2-Associated Acute Hemorrhagic, Necrotizing Encephalitis (AHNE) Presenting with Cognitive Impairment in a 44-Year-Old Woman without Comorbidities: A Case Report. Am. J. Case Rep. 2020, 21, e925641. [Google Scholar] [CrossRef]
- Grimaldi, S.; Lagarde, S.; Harlé, J.-R.; Boucraut, J.; Guedj, E. Autoimmune encephalitis concomitant with SARS-CoV-2 infection: Insight from 18F-FDG PET imaging and neuronal autoantibodies. J. Nucl. Med. 2020, 61, 1726–1729. [Google Scholar] [CrossRef]
- Gunawardhana, C.; Nanayakkara, G.; Gamage, D.; Withanage, I.; Bandara, M.; Siriwimala, C.; Senaratne, N.; Chang, T. Delayed presentation of postinfectious encephalitis associated with SARS-CoV-2 infection: A case report. Neurol. Sci. 2021, 42, 3527–3530. [Google Scholar] [CrossRef]
- Haider, A.; Siddiqa, A.; Ali, N.; Dhallu, M. COVID-19 and the Brain: Acute Encephalitis as a Clinical Manifestation. Cureus 2020, 12, e10784. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.; Syed, F.; Ali, L.; Rajput, H.M.; Faisal, F.; Shahzad, W.; Badshah, M. Chorea as a presentation of SARS-CoV-2 encephalitis: A clinical case report. J. Mov. Disord. 2021, 14, 245. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Sahashi, Y.; Baba, Y.; Okura, H.; Shimohata, T. COVID-19-associated mild encephalitis/encephalopathy with a reversible splenial lesion. J. Neurol. Sci. 2020, 415, 116941. [Google Scholar] [CrossRef] [PubMed]
- Kahwagi, J.; Diagne, R.; Fall, M.; Basse, A.; Ndiaye, M.; Diop, A. Post infectious encephalitis at Covid19: About one pediatric observation and review of the literature. Rev. Neurol. 2020, 177, 132–134. [Google Scholar] [CrossRef]
- Kamal, Y.M.; Abdelmajid, Y.; Al Madani, A.A.R. Cerebrospinal fluid confirmed COVID-19-associated encephalitis treated successfully. BMJ Case Rep. 2020, 13, e237378. [Google Scholar] [CrossRef]
- Kasturiarachi, B.M.; Alsbrook, D.L.; Crook, J.; Shah, N. An Immunologic Storm: A Case of Encephalitis and Thrombotic Thrombocytopenic Purpura With Underlying Likely Sjogren’s Syndrome Induced by a COVID-19 Immune Response. Neurohospitalist 2022, 12, 529–535. [Google Scholar] [CrossRef]
- Khoo, A.; McLoughlin, B.; Cheema, S.; Weil, R.S.; Lambert, C.; Manji, H.; Zandi, M.S.; Morrow, J.M. Postinfectious brainstem encephalitis associated with SARS-CoV-2. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1013–1014. [Google Scholar]
- Kimura, M.; Hashiguchi, S.; Tanaka, K.; Hagiwara, M.; Takahashi, K.; Miyaji, Y.; Joki, H.; Doi, H.; Koga, M.; Takeuchi, H.; et al. Case Report: Takotsubo Cardiomyopathy in Bickerstaff Brainstem Encephalitis Triggered by COVID-19. Front. Neurol. 2021, 12, 822247. [Google Scholar] [CrossRef]
- Koh, S.; Kim, Y.S.; Kim, M.H.; Choi, Y.H.; Choi, J.Y.; Kim, T.-J. Encephalitis with status epilepticus and stroke as complications of non-severe COVID-19 in a young female patient: A case report. BMC Neurol. 2022, 22, 1–5. [Google Scholar] [CrossRef]
- Kumar, N.; Kumar, S.; Kumar, A.; Pati, B.K.; Kumar, A.; Singh, C.; Sarfraz, A. Acute necrotizing encephalitis as a probable association of covid-19. Indian J. Crit. Care 2020, 24, 991–994. [Google Scholar] [CrossRef]
- Kumar, V.H.; Natarajan, C.; Siddharth, M.; Shivabalan, S.; Gopinath, C.; Shyam, A.; Jean, M. Post covid pneumonia pulmonary fibrosis and encephalitis in a term neonate with prenatal exposure to SARS CoV-2: A case report. IDCases 2022, 27, e01414. [Google Scholar] [CrossRef]
- Marques, L.M.; Marques, S.R.; Costa, O.; Freitas, E.; Machado, Á. COVID-19-Associated Encephalitis: Two Case Reports. Cureus 2022, 14, e23243. [Google Scholar] [CrossRef]
- Mekheal, E.; Mekheal, M.; Roman, S.; Mikhael, D.; Mekheal, N.; Manickam, R. A Case Report of Autoimmune Encephalitis: Could Post-COVID-19 Autoimmunity Become a Lethal Health Issue? Cureus 2022, 14, e25910. [Google Scholar] [CrossRef]
- Meshref, M.; Hewila, I.M.; Mageed, S.A.; Morra, M.E. COVID-19 Associated With Encephalitis: Case Report and Review of Literature. Neurologist 2021, 26, 268. [Google Scholar] [CrossRef]
- Mierzewska-Schmidt, M.; Baranowski, A.; Szymanska, K.; Ciaston, M.; Kuchar, E.; PLoSki, R.; Kosinska, J.; Pagowska-Klimek, I. The case of fatal acute hemorrhagic necrotizing encephalitis in a two-month-old boy with Covid-19. Int. J. Infect. Dis. 2021, 116, 151–153. [Google Scholar] [CrossRef]
- Miqdad, M.A.; Enabi, S.; Alshurem, M.; Al-Musawi, T.; Alamri, A. COVID-19–Induced Encephalitis: A Case Report of a Rare Presentation With a Prolonged Electroencephalogram. Cureus 2021, 13, e14476. [Google Scholar] [CrossRef]
- Monti, G.; Giovannini, G.; Marudi, A.; Bedin, R.; Melegari, A.; Simone, A.M.; Santangelo, M.; Pignatti, A.; Bertellini, E.; Trenti, T.; et al. Anti-NMDA receptor encephalitis presenting as new onset refractory status epilepticus in COVID-19. Seizure 2020, 81, 18–20. [Google Scholar] [CrossRef]
- Morvan, A.-C.; Kerambrun, H. Fatal necrotizing encephalitis associated with COVID-19: A case report. Neurology 2021, 11, 214–215. [Google Scholar]
- Mullaguri, N.; Sivakumar, S.; Battineni, A.; Anand, S.; Vanderwerf, J. COVID-19 Related Acute Hemorrhagic Necrotizing Encephalitis: A Report of Two Cases and Literature Review. Cureus 2021, 13, e14236. [Google Scholar] [CrossRef]
- Oosthuizen, K.; Steyn, E.C.; Tucker, L.; Ncube, I.V.; Hardie, D.; Marais, S. SARS-CoV-2 encephalitis presenting as a clinical cerebellar syndrome: A case report. Neurology 2021, 97, 27–29. [Google Scholar] [CrossRef]
- Orsini, M.; Porto, F.H.D.G.; Nascimento, J.F.D. Neuropsychiatric presentation of Covid-19-related encephalitis: Case report. Psychiatry Res. Commun. 2021, 1, 100004. [Google Scholar] [CrossRef]
- Panariello, A.; Bassetti, R.; Radice, A.; Rossotti, R.; Puoti, M.; Corradin, M.; Moreno, M.; Percudani, M. Anti-NMDA receptor encephalitis in a psychiatric Covid-19 patient: A case report. Brain, Behav. Immun. 2020, 87, 179–181. [Google Scholar] [CrossRef]
- Picod, A.; Dinkelacker, V.; Savatovsky, J.; Trouiller, P.; Guéguen, A.; Engrand, N. SARS-CoV-2-associated encephalitis: Arguments for a post-infectious mechanism. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef]
- Pilotto, A.; Odolini, S.; Masciocchi, S.S.; Comelli, A.; Volonghi, I.; Gazzina, S.; Nocivelli, S.; Pezzini, A.; Focà, E.; Caruso, A.; et al. Steroid-Responsive Encephalitis in Coronavirus Disease 2019. Ann. Neurol. 2020, 88, 423–427. [Google Scholar] [CrossRef]
- Pizzanelli, C.; Milano, C.; Canovetti, S.; Tagliaferri, E.; Turco, F.; Verdenelli, S.; Nesti, L.; Franchi, M.; Bonanni, E.; Menichetti, F. Autoimmune limbic encephalitis related to SARS-CoV-2 infection: Case-report and review of the literature. Brain Behav. Immun. Health 2021, 12, 1–6. [Google Scholar] [CrossRef]
- Poursadeghfard, M.; Sharifian-Dorche, M.; Nemati, A.; Mowla, A. Simultaneous Encephalitis and Neuroretinitis After COVID-19 in a Young Adult: A Case Report. J. Neurol. Res. 2021, 11, 102–107. [Google Scholar] [CrossRef]
- Rebeiz, T.; Lim-Hing, K.; Khazanehdari, S.; Rebeiz, K. Behavioral Changes Without Respiratory Symptoms as a Presenting Sign of COVID-19 Encephalitis. Cureus 2020, 12, e10469. [Google Scholar] [CrossRef]
- Reddy, R. Status epilepticus in a young woman with suspected SARS-CoV-2 encephalitis. Crit. Care Med. 2021, 49, 107. [Google Scholar] [CrossRef]
- Sangare, A.; Dong, A.; Valente, M.; Pyatigorskaya, N.; Cao, A.; Altmayer, V.; Zyss, J.; Lambrecq, V.; Roux, D.; Morlon, Q.; et al. Neuroprognostication of Consciousness Recovery in a Patient with COVID-19 Related Encephalitis: Preliminary Findings from a Multimodal Approach. Brain Sci. 2020, 10, 845. [Google Scholar] [CrossRef]
- Sarmast, S.T.; Mohamed, A.S.; Amar, Z.; Sarwar, S.; Ahmed, Z. A Case of Acute Encephalitis in COVID-19 Patient: A Rare Complication. Cureus 2021, 13, e15636. [Google Scholar] [CrossRef]
- Sattar, S.B.A.; Haider, M.A.; Zia, Z.; Niazi, M.; Iqbal, Q.Z. Clinical, Radiological, and Molecular Findings of Acute Encephalitis in a COVID-19 Patient: A Rare Case Report. Cureus 2020, 12, e10650. [Google Scholar] [CrossRef]
- Sharma, R.; Nalleballe, K.; Shah, V.; Haldal, S.; Spradley, T.; Hasan, L.; Mylavarapu, K.; Vyas, K.; Kumar, M.; Onteddu, S.; et al. Spectrum of Hemorrhagic Encephalitis in COVID-19 Patients: A Case Series and Review. Diagnostics 2022, 12, 924. [Google Scholar] [CrossRef] [PubMed]
- Sofijanova, A.; Bojadzieva, S.; Duma, F.; Superlishka, E.; Murtezani, A.; Jordanova, O. Severe Encephalitis in Infant with COVID-19: A Case Report. Open Access Maced. J. Med Sci. 2020, 8, 514–517. [Google Scholar] [CrossRef]
- Wettervik, T.S.; Kumlien, E.; Rostami, E.; Howells, T.; von Seth, M.; Velickaite, V.; Lewén, A.; Enblad, P. Intracranial Pressure Dynamics and Cerebral Vasomotor Reactivity in Coronavirus Disease 2019 Patient With Acute Encephalitis. Crit. Care Explor. 2020, 2, e0197. [Google Scholar] [CrossRef] [PubMed]
- Tee, T.Y.; Thabit, A.A.M.; Khoo, C.S.; Shahrom, H.M.; Chan, E.Z.; Marzukie, M.M.; Kamaruddin, Z.A.C.; Thayan, R.; Chidambaram, S.K. Acute encephalitis associated with SARS-CoV-2 confirmed in cerebrospinal fluid: First case in Malaysia. J. Clin. Neurol. 2021, 17, 490. [Google Scholar] [CrossRef] [PubMed]
- Urso, L.; Distefano, M.G.; Cambula, G.; Colomba, A.I.; Nuzzo, D.; Picone, P.; Giacomazza, D.; Sicurella, L. The case of encephalitis in a COVID-19 pediatric patient. Neurol. Sci. 2021, 43, 105–112. [Google Scholar] [CrossRef]
- Valadez-Calderon, J.; Navarro, A.O.; Rodriguez-Chavez, E.; Vera-Lastra, O. Co-expression of anti-NMDAR and anti-GAD65 antibodies. A case of autoimmune encephalitis in a post-COVID-19 patient. Neurologia 2022, 37, 503. [Google Scholar] [CrossRef]
- Vandervorst, F.; Guldolf, K.; Peeters, I.; Vanderhasselt, T.; Michiels, K.; Berends, K.J.; Van Laethem, J.; Pipeleers, L.; Vincken, S.; Seynaeve, L. Encephalitis associated with the SARS-CoV-2 virus: A case report. Interdiscip. Neurosurg. 2020, 22, 1–3. [Google Scholar] [CrossRef]
- Woldie, I.L.; Brown, I.G.; Nwadiaro, N.F.; Patel, A.; Jarrar, M.; Quint, E.; Khokhotva, V.; Hugel, N.; Winger, M.; Briskin, A. Autoimmune Hemolytic Anemia in a 24-Year-Old Patient With COVID-19 Complicated by Secondary Cryptococcemia and Acute Necrotizing Encephalitis: A Case Report and Review of Literature. J. Med. Cases 2020, 11, 362–365. [Google Scholar] [CrossRef]
- Ye, M.; Ren, Y.; Lv, T. Encephalitis as a clinical manifestation of COVID-19. Brain Behav. Immun. 2020, 88, 945–946. [Google Scholar] [CrossRef]
- Zambreanu, L.; Lightbody, S.; Bhandari, M.; Hoskote, C.; Kandil, H.; Houlihan, C.F.; Lunn, M.P. A case of limbic encephalitis associated with asymptomatic COVID-19 infection. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1229–1230. [Google Scholar] [CrossRef]
- Zandifar, S.; Zandifar, Z. Acute Viral Encephalitis Associated with SARS-CoV-2. Ann. Clin. Case Rep. 2020, 5, 1–3. [Google Scholar]
- Zuhorn, F.; Omaimen, H.; Ruprecht, B.; Stellbrink, C.; Rauch, M.; Rogalewski, A.; Klingebiel, R.; Schäbitz, W.-R. Parainfectious encephalitis in COVID-19: “The Claustrum Sign”. J. Neurol. 2020, 268, 2031–2034. [Google Scholar] [CrossRef]
- Pilotto, A.; Masciocchi, S.; Volonghi, I.; Crabbio, M.; Magni, E.; De Giuli, V.; Caprioli, F.; Rifino, N.; Sessa, M.; Gennuso, M. Clinical presentation and outcomes of SARS-CoV-2 related encephalitis: The ENCOVID multicentre study. J. Infect. Dis. 2020, 223, 28–37. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Liotta, E.M.; Batra, A.; Clark, J.R.; Shlobin, N.A.; Hoffman, S.C.; Orban, Z.S.; Koralnik, I.J. Frequent neurologic manifestations and encephalopathy-associated morbidity in Covid-19 patients. Ann. Clin. Transl. Neurol. 2020, 7, 2221–2230. [Google Scholar] [CrossRef]
- Garg, R.K.; Paliwal, V.K.; Gupta, A. Encephalopathy in patients with COVID-19: A review. J. Med. Virol. 2020, 93, 206–222. [Google Scholar] [CrossRef]
- Kas, A.; Soret, M.; Pyatigoskaya, N.; Habert, M.-O.; Hesters, A.; Le Guennec, L.; Paccoud, O.; Bombois, S.; Delorme, C. The cerebral network of COVID-19-related encephalopathy: A longitudinal voxel-based 18F-FDG-PET study. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2543–2557. [Google Scholar] [CrossRef]
- Guo, K.; Wei, Y.; Yuan, M.; Wei, L.; Lu, J. Identifying the characteristics of brain glucose metabolism using normal 18F-FDG PET database in patients with temporal lobe epilepsy. Neurol. Sci. 2020, 41, 3219–3226. [Google Scholar] [CrossRef]
- Cani, I.; Barone, V.; D’Angelo, R.; Pisani, L.; Allegri, V.; Spinardi, L.; Malpassi, P.; Fasano, L.; Rinaldi, R.; Fanti, S.; et al. Frontal encephalopathy related to hyperinflammation in COVID-19. J. Neurol. 2020, 268, 16–19. [Google Scholar] [CrossRef]
- Hosseini, A.A.; Shetty, A.K.; Sprigg, N.; Auer, D.P.; Constantinescu, C.S. Delirium as a presenting feature in COVID-19: Neuroinvasive infection or autoimmune encephalopathy? Brain Behav. Immun. 2020, 88, 68–70. [Google Scholar] [CrossRef]
- Umapathi, T.; Quek, W.M.J.; Yen, J.M.; Khin, H.S.W.; Mah, Y.Y.; Chan, C.Y.J.; Ling, L.M.; Yu, W.-Y. Encephalopathy in COVID-19 patients; viral, parainfectious, or both? Eneurologicalsci 2020, 21, 100275. [Google Scholar] [CrossRef]
- Harmer, D.; Gilbert, M.; Borman, R.; Clark, K.L. Quantitative mRNA expression profiling of ACE 2, a novel homologue of angiotensin converting enzyme. FEBS Lett. 2002, 532, 107–110. [Google Scholar] [CrossRef]
- Lersy, F.; Anheim, M.; Willaume, T.; Chammas, A.; Brisset, J.-C.; Cotton, F.; Kremer, S. Cerebral vasculitis of medium-sized vessels as a possible mechanism of brain damage in COVID-19 patients. J. Neuroradiol. 2021, 48, 141–146. [Google Scholar] [CrossRef]
- Cantuti-Castelvetri, L.; Ojha, R.; Pedro, L.D.; Djannatian, M.; Franz, J.; Kuivanen, S.; van der Meer, F.; Kallio, K.; Kaya, T.; Anastasina, M. Neuropilin-1 facilitates SARS-CoV-2 cell entry and infectivity. Science 2020, 370, 856–860. [Google Scholar] [CrossRef] [PubMed]
- Kumari, P.; Rothan, H.A.; Natekar, J.P.; Stone, S.; Pathak, H.; Strate, P.G.; Arora, K.; Brinton, M.A.; Kumar, M. Neuroinvasion and encephalitis following intranasal inoculation of SARS-CoV-2 in K18-hACE2 mice. Viruses 2021, 13, 132. [Google Scholar] [CrossRef] [PubMed]
- Klingenstein, M.; Klingenstein, S.; Neckel, P.H.; Mack, A.F.; Wagner, A.P.; Kleger, A.; Liebau, S.; Milazzo, A. Evidence of SARS-CoV2 Entry Protein ACE2 in the Human Nose and Olfactory Bulb. Cells Tissues Organs 2021, 209, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Yan, R.; Zhang, Y.; Li, Y.; Xia, L.; Guo, Y.; Zhou, Q. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science 2020, 367, 1444–1448. [Google Scholar] [CrossRef]
- Chu, H.; Chan, J.F.-W.; Yuen, T.T.-T.; Shuai, H.; Yuan, S.; Wang, Y.; Hu, B.; Yip, C.C.-Y.; Tsang, J.O.-L.; Huang, X. Comparative tropism, replication kinetics, and cell damage profiling of SARS-CoV-2 and SARS-CoV with implications for clinical manifestations, transmissibility, and laboratory studies of COVID-19: An observational study. Lancet Microbe 2020, 1, e14–e23. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| No. | Study ID, Country [references] | No. of Patient | Age (Years), Gender | Confirmation of SARS-CoV-2 | Past Medical History | Severity of COVID-19 | Onset of Encephalitis from COVID-19 Presentation | Neurological and Psychiatric Symptoms | Type of Suspected or Confirmed Encephalitis | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Ahsan 2021, USA [20] | 1 | 7, F | Serology test positive (IgG in serum) | Healthy | Asymptomatic | Post-SARS-CoV-2 infection | 1st admission: status epilepticus, aphasia, encephalopathy; 2nd admission: headache, encephalopathy, slurred speech, altered mental status | Autoimmune encephalitis | Discharged and follow-up confirmed recovery with mild dysarthria |
| 2 | Allahyari 2021, Iran [21] | 1 | 18, F | RT-PCR positive | NR | NR | Initial presentation | Altered mental status, tonic-clonic seizures, confused state, minor meningismus, neck stiffness | Autoimmune encephalitis (SARS-CoV-2-mediated anti-NMDAR encephalitis) | Discharged with full recovery |
| 3 | Andrea 2020, Italy [22] | 1 | 79, F | RT-PCR positive | Rheumatoid arthritis | Mild | Initial presentation | Confusion, somnolence, psychomotor retardation, and cephalea | SARS-CoV-2-mediated encephalitis | Complete recovery in 15 days |
| 4 | Ayatollahi 2020, Canada [23] | 1 | 18, F | RT-PCR positive | NR | Mild | Initial presentation | Drowsiness and confusion, generalized tonic-clonic seizure, impaired orientation to time and place and recent memory | Autoimmune encephalitis | Near complete resolution of the claustrum hyperintensities following 1 month, no seizures following 7 weeks |
| 5 | Ayuningtyas 2022, Indonesia [24] | 1 | 34, F | RT-PCR positive | Obese | Severe | Initial presentation | Reduced consciousness, altered mental status aggressive behavior, seizure, headache | SARS-CoV-2-mediated encephalitis | Discharged with full recovery |
| 6 | Ayuso 2020, Spain [25] | 1 | 72, F | RT-PCR positive | Hypertension, hyperlipidemia, depression, and smoking | NR | Post-SARS-CoV-2 infection (after 8 days of discharge) | 1st admission: delirium; 2nd admission: dizziness, oscillopsia, inattention, disorientation, unsteadiness, myoclonus, and ataxia | Autoimmune encephalitis (SARS-CoV-2-mediated Bickerstaff encephalitis) | Discharged; after 2 months, very mild unsteadiness was observed |
| 7 | Babar 2020, USA [26] | 1 | 20, F | RT-PCR positive | Obesity and anxiety | Mild | Initial presentation | Acute altered mental status, confusion, ageusia, insomnia, hypervigilance, obsessive thinking, and urinary incontinence | SARS-CoV-2-mediated encephalitis | Near complete resolution of the neurological symptoms after 12 days of discharge |
| 8 | Benameur 2020, USA [27] | 3 | 31, F | RT-PCR positive | Sickle cell disease | Severe | Initial presentation | Various neurologic manifestations including myoclonus, affected brainstem reflexes, and encephalopathy | SARS-CoV-2-mediated encephalitis | Died |
| 34, M | Hypertension | Initial presentation | NR | |||||||
| 64, M | Hypertension | Initial presentation | Discharged without major neurologic sequelae | |||||||
| 9 | Bernard-Valnet 2020, Switzerland [28] | 2 | 64, F | RT-PCR positive | NR | Mild | Initial presentation | Tonic-clonic seizure, disorientation, strong attention deficit, verbal and motor perseverations and bilateral grasping, hyper-religiosity with mystic delusions, visual hallucinations, and non-convulsive status epilepticus | SARS-CoV-2-mediated meningoencephalitis | Resolution of her symptoms after 96 h of admission |
| 67, F | RT-PCR positive | NR | Mild | Initial presentation | Intense headache, drowsiness, confusion, motor perseverations, bilateral grasping, and aggressiveness | SARS-CoV-2-mediated meningoencephalitis | Discharged after 72 h without major neurologic symptoms | |||
| 10 | Bhavsar 2020, USA [29] | 1 | 16, M | RT-PCR positive | Healthy | Mild | Initial presentation | Initially intermittent headache; day 11: confusion, incoherent speech, seizure, and altered mental status, with inconsistent awareness of time and place | SARS-CoV-2-mediated encephalitis | Discharged after day 15 with improved mental status |
| 11 | Bodro 2020, Spain [30] | 2 | 25, M | RT-PCR positive | Healthy | NR | Initial presentation | Headache, left-side paresthesia and ipsilateral paresis, progressing to confusion and agitation | SARS-CoV-2-mediated encephalitis | Fully recovered within 2 days except for amnesia |
| 49, M | RT-PCR positive | Healthy | Mild | Initial presentation | Anomic aphasia, disorientation, confusion, and agitation | Fully recovered within 3 days except for amnesia | ||||
| 12 | Burr 2021, USA [31] | 1 | 23 months, F | RT-PCR positive | Healthy | NR | Initial presentation | Initial: fussiness, poor sleep; day 9: seizure, hyperkinetic movements, and mood lability | Autoimmune encephalitis (SARS-CoV-2-mediated anti-NMDAR encephalitis) | Discharged and fully recovered after 2 weeks |
| 13 | Cao 2020, France [32] | 5 | 49, M | RT-PCR positive | Rheumatoid purpura | Severe | Initial presentation | Headache and anosmia | SARS-CoV-2-mediated encephalitis | Improvement after 6 days of immunotherapy |
| 56, M | RT-PCR positive | Hypertension | Severe | Initial presentation | Improvement after 2 days of immunotherapy | |||||
| 61, M | RT-PCR positive | Pulmonary sarcoidosis and thrombocytopenia | Severe | Initial presentation | Improvement after 7 days of immunotherapy | |||||
| 37, M | RT-PCR positive | Obesity | Severe | Initial presentation | Died | |||||
| 77, F | RT-PCR positive | Obesity, hypertension and asthma | Severe | Initial presentation | Vegetative state | |||||
| 14 | Casez 2021, France [33] | 1 | 96, F | RT-PCR positive | NR | NR | Initial presentation | At onset: anosmia, dysgeusia; day 3: generalized epileptic seizures, and left hemiparesis | SARS-CoV-2-mediated encephalitis | NR |
| 15 | Chalil 2020, Canada [34] | 1 | 48, F | RT-PCR positive | Healthy | Severe | Initial presentation | Altered mental status | SARS-CoV-2-mediated acute hemorrhagic encephalitis | During the report, she was undergoing rehabilitation |
| 16 | Cheraghali 2021, Iran [35] | 1 | 34 months, child | RT-PCR positive | Healthy | NR | Initial presentation | Tonic-clonic seizures, and loss of consciousness | SARS-CoV-2-mediated encephalitis | Discharged with decerebrate posture |
| 17 | Dahshan 2022, Egypt [36] | 1 | 67, M | RT-PCR positive | Hypertension | NR | Post-SARS-CoV-2 infection (8 days after SARS-CoV-2 infection) | Acute confusion state, behavioral changes, agitation, and one attack of loss of consciousness | Autoimmune encephalitis | Discharged with full recovery |
| 18 | Dono 2021, Italy [37] | 1 | 81, M | RT-PCR positive | Mild hypertension | NR | Post-SARS-CoV-2 infection (on day 14 during her hospitalization for COVID-19 infection) | Since day 14: mild confusion with fluctuation of the mental status; day 16: myoclonic jerks and non-convulsive status epilepticus with coma | Suspected autoimmune encephalitis | Died |
| 19 | Duong 2020 and Huang 2020, USA [38,39] | 1 | 41, F | RT-PCR positive | T2DM and obesity | NR | Initial presentation | Seizure, lethargy, disorientation, agitation, and hallucination | SARS-CoV-2-mediated encephalitis | Mental status improved by hospital day 12 |
| 20 | Durovic 2021, Germany [40] | 1 | 22, M | RT-PCR positive | Healthy | NR | Post-SARS-CoV-2 infection (10 days after SARS-CoV-2 infection) | Severe headache, neck stiffness, general weakness, and a loss of smell and taste | Autoimmune encephalitis | Discharged with full recovery |
| 21 | Efe 2020, Turkey [41] | 1 | 35, F | RT-PCR positive | NR | NR | Initial presentation | Headache, nausea, dizziness, and drug-refractory seizures | SARS-CoV-2-mediated encephalitis | NR |
| 22 | El Aoud 2021, France [42] | 1 | 60, M | Serology test positive | Dyslipidemia | Mild | Initial presentation | Headache, disturbance of consciousness, and vertigo | SARS-CoV-2-mediated encephalitis | Discharged and recovered after 1 month |
| 23 | Elmouhib 2022, Morocco [43] | 1 | 54, F | RT-PCR positive | Healthy | Severe | Initial presentation | Altered mental state, dyspnea, altered consciousness | SARS-CoV-2-mediated autoimmune limbic encephalitis | Discharged with improved state |
| 24 | Esmaeili 2022, Iran [44] | 1 | 67, M | RT-PCR positive | Healthy | Severe | Initial presentation | Drowsiness, decreased level of consciousness, deep tendon reflexes were brisk, and plantar reflexes were upward | Acute disseminated encephalitis | Died |
| 25 | Etemadifar 2020, Iran [45] | 1 | 51, M | RT-PCR positive | Hypothyroidism and migraine | Mild | Initial presentation | For 3 days, episodic headache, nausea, and drowsiness, and generalized tonic-clonic seizure | SARS-CoV-2-mediated encephalitis | Died |
| 26 | Ferdosian 2021, Iran [46] | 1 | 7, M | RT-PCR positive | Controlled seizures | Mild | Initial presentation | Loss of consciousness, inability to speak | SARS-CoV-2-mediated encephalitis | Discharged with supportive treatment |
| 27 | Freire-Álvarez 2020, Spain [47] | 1 | 39, M | RT-PCR positive | NR | Mild | Initial presentation | Drowsiness, mental disorientation, inconsistent language disorder, and headache | SARS-CoV-2-mediated encephalitis | Following intravenous immunoglobulins and cytokine blockade with IL-6 receptor antagonist, the patient fully recovered after 30 days from admission |
| 28 | Gaughan 2021, Ireland [48] | 1 | 16, F | RT-PCR positive | Mild learning disability | Asymptomatic | Initial presentation | Visual and auditory hallucinations, cognitive difficulties, and high-frequency tremor | Autoimmune encephalitis | Discharged; at six months, showed significant improvements |
| 29 | Ghosh 2020, India [49] | 1 | 44, F | RT-PCR positive | Healthy | NR | Initial presentation | For 10 days: hypogeusia, hyposmia; then, confusion, disorientation, cognitive disorders, apraxia; then, tonic-clonic seizure and coma | SARS-CoV-2-mediated AHNE | Died |
| 30 | Grimaldi 2020, France [50] | 1 | 72, M | RT-PCR positive | Transient global amnesia | Mild | Initial presentation | Since day 17: action tremor, ataxia, dysarthria, and upper limb dysmetria and myoclonus | Autoimmune encephalitis | Improved and discharged at day 37 |
| 31 | Gunawardhana 2021, Sri Lanka [51] | 1 | 47, F | RT-PCR positive | Uncomplicated T2DM | Mild | Post-SARS-CoV-2 infection (4 weeks after SARS-CoV-2 infection) | Confusion and abnormal behavior, seizures, status epilepticus | SARS-CoV-2-mediated encephalitis | Discharged to home with only minor residual cognitive deficits |
| 32 | Haider 2020, USA [52] | 1 | 66, M | RT-PCR positive | Benign prostatic hypertrophy, fatty liver disease, and hypertension | NR | Initial presentation | Seizure; impaired orientation to time, place, and person; and persistent confusion | SARS-CoV-2-mediated encephalitis | Two months post-discharge, the patient showed significant improvements following rituximab |
| 33 | Hassan 2021, Pakistan [53] | 1 | 58, M | RT-PCR positive | Hypertension | Severe | Initial presentation | Acute chorea | SARS-CoV-2-mediated encephalitis | Discharged |
| 34 | Hayashi 2020, Japan [54] | 1 | 75, M | RT-PCR positive | Mild Alzheimer’s disease | Severe | Initial presentation | Left-dominant kinetic tremor in hands, alerted consciousness, dysmetria, ataxia, disorientation, and mild gait disturbance | SARS-CoV-2-mediated encephalitis | Died |
| 35 | Kahwagi 2021, Senegal [55] | 1 | 7, F | RT-PCR positive | NR | Mild | Post-SARS-CoV-2 infection (On day 6 during her hospitalization) | Initial: headache; day 6: generalized tonic-clonic seizures; day 9: gait and behavioral disturbance, confusional syndrome, osteotendinous, and hyperreflexia | SARS-CoV-2-mediated encephalitis | Complete recovery over the follow-up of 2 months |
| 36 | Kamal 2020, United Arab Emirates [56] | 1 | 31, M | RT-PCR positive | Healthy | Mild | Initial presentation | Day 3, behavioral disturbance; day 5: altered mental state, acute behavioral changes, severe confusion, fluctuations in the level of consciousness, and drowsiness | SARS-CoV-2-mediated encephalitis | Discharged; further follow-up confirmed good condition |
| 37 | Kasturiarachi 2022, USA [57] | 1 | 19, F | RT-PCR positive | Menorrhagia, learning disability, and remote suicidal ideation | NR | Post-SARS-CoV-2 infection (recent infection) | Headaches, vomiting, and psychosis, left gaze deviation and right hemiplegia, unable to follow commands or open her eyes spontaneously, seizures, hyperreflexia in the right upper and lower extremities, no hyperkinetic movements | Sjogren’s-associated encephalitis | Discharged with improved mental status but needed to be monitored closely as an outpatient |
| 38 | Khoo 2020, UK [58] | 1 | 65, F | RT-PCR positive | Alzheimer’s disease, osteoarthritis, and gastro-esophageal reflex disease | Mild | Post-SARS-CoV-2 infection (2 weeks after SARS-CoV-2 infection) | Week 2: widespread involuntary movements, diplopia, cognitive decline, speaking difficulties, increasing confusion; at entry: myoclonus, ocular movement disorder, aphasia, and perseveration | Autoimmune encephalitis | Discharged with improved neurological symptoms; back to baseline after 1 month from onset |
| 39 | Kimura 2021, Japan [59] | 1 | 68, F | RT-PCR positive | Hypertension | NR | Post-SARS-CoV-2 infection (2 weeks after SARS-CoV-2 infection) | Her eyes were fixed in position and complete flaccid paralysis with diminished tendon reflexes in all extremities; no pathological reflex | Autoimmune encephalitis (SARS-CoV-2-mediated Bickerstaff encephalitis) | Discharged with residual double vision and bilateral disturbance in abduction |
| 40 | Koh 2022, Republic of Korea [60] | 1 | 20, F | RT-PCR positive | Healthy | Moderate | Initial presentation | Tonic-clonic seizure On her left face and arm, drowsy mentality, personality change, dizziness, and somnolence | Suspected autoimmune encephalitis | Discharged with near-complete recovery |
| 41 | Kumar 2020, India [61] | 1 | 35, M | RT-PCR positive | Headache | NR | Initial presentation | 10 days before: headache; at entry: coma | SARS-CoV-2-mediated ANE | Died |
| 42 | Kumar 2022, India [62] | 1 | 9 days, neonate | RT-PCR positive | Respiratory distress, hypoxia | NR | Post-SARS-CoV-2 infection (MRI done after 42 days of illness) | Generalized hypotonia generalized seizures | SARS-CoV-2-mediated encephalitis | Discharged with tachypnoea without hypoxia |
| 43 | Marques 2022, Portugal [63] | 2 | 49, F | RT-PCR positive | Healthy | NR | Post-SARS-CoV-2 infection (6 days after SARS-CoV-2 infection) | Altered mental status, lethargic, not oriented to time and place, could not follow commands, neck rigidity, amnesia | SARS-CoV-2-mediated encephalitis | Two months post discharge, she was doing well, with no neurological signs and symptoms |
| 50, F | RT-PCR positive | Depression | NR | Post-SARS-CoV-2 infection (8 days after SARS-CoV-2 infection) | Restless, sometimes physically aggressive, mutism | Three months post discharge, she was doing well with no neurological signs and symptoms | ||||
| 44 | McAbee 2020, USA [11] | 1 | 11, M | RT-PCR positive | Healthy | Asymptomatic | Initial presentation | Status epilepticus | SARS-CoV-2-mediated encephalitis | Recovered within 6 days |
| 45 | Mekheal 2022, USA [64] | 1 | 88, F | NR | Hypertension | NR | Post-SARS-CoV-2 infection (2 months after SARS-CoV-2 infection) | Right leg weakness, dysarthria, altered mental status | Autoimmune encephalitis | NR |
| 46 | Meshref 2021, Egypt [65] | 1 | 66, F | RT-PCR positive | Chronic bronchitis and ischemic heart disease | NR | Initial presentation | Delirious state, confusion, fluctuant conscious level, and disorientation | SARS-CoV-2-mediated encephalitis | Discharged home with full consciousness, no neurological deficits |
| 47 | Mierzewska-Schmidt 2022, Poland [66] | 1 | 2 months, Boy | RT-PCR positive | Healthy | NR | Initial presentation | Irritability, nystagmus, agitation then apathy | SARS-CoV-2-mediated AHNE | The baby showed signs of brain death |
| 48 | Miqdad 2021, Saudi Arabia [67] | 1 | 36, M | RT-PCR positive | Glucose-6 phosphate dehydrogenase deficiency | NR | Initial presentation | Cognitive impairment and decreased responsiveness | SARS-CoV-2-mediated encephalitis | Discharged home with regular follow-up in the neurology clinic |
| 49 | Monti 2020, Italy [68] | 1 | 50, M | RT-PCR positive | Mild hypertension | Asymptomatic | Initial presentation | Confabulations and delirious ideas; day 4: impaired awareness and status epilepticus | Autoimmune encephalitis | Discharged after 4 months of hospitalization without neurological deficits |
| 50 | Moriguchi 2020, Japan [17] | 1 | 24, M | RT-PCR positive | NR | Mild | Initial presentation | Headache, consciousness disturbance, generalized seizures, and status epilepticus | SARS-CoV-2-mediated encephalitis | NR |
| 51 | Morvan 2020, France [69] | 1 | 56, M | RT-PCR positive | Malnutrition, renal lithiasis with left renal abscess and Mycobacterium abscessus pulmonary infection | NR | Initial presentation | Coma | SARS-CoV-2-mediated ANE | Died |
| 52 | Mullaguri 2021, USA [70] | 2 | 77, F | RT-PCR positive | Parkinson’s disease, cognitive impairment, and hypertension | Severe | Initial presentation | Oriented to self but not to place or time | SARS-CoV-2-mediated AHNE | Died |
| 68, F | RT-PCR positive | Chronic lymphocytic leukemia and hypertension | Severe | Post-SARS-CoV-2 infection (5 days after SARS-CoV-2 infection) | Comatose, persistent severe encephalopathy | Died | ||||
| 53 | Natarajan 2020, India [10] | 1 | 13, F | RT-PCR positive | Healthy | Mild | Initial presentation | Headache and generalized tonic-clonic seizure | SARS-CoV-2-mediated encephalitis | Discharged home in a normal neurological state |
| 54 | Oosthuizen 2021, South Africa [71] | 1 | 52, M | RT-PCR positive | Healthy | NR | Initial presentation | Multidirectional gaze-evoked nystagmus, dysarthria, and truncal and appendicular ataxia | SARS-CoV-2 mediated encephalitis | Discharged while walking independently, mild emotional lability persisted |
| 55 | Orsini 2021, Brazil [72] | 1 | 52, M | RT-PCR positive | Healthy | Severe | Initial presentation | Intense agitation, cognitive impairment, tonic-clonic seizure | SARS-CoV-2 mediated encephalitis | Died |
| 56 | Panariello 2020, Ecuador [73] | 1 | 23, M | NR | Healthy | Moderate | Initial presentation | Psychomotor agitation, anxiety, thought disorganization, persecutory delusions, dyskinesias and auditory hallucinations | Autoimmune encephalitis | Clinical condition improved |
| 57 | Picod 2020, France [74] | 1 | 58, F | Serology test positive | Hypertension and chronic kidney disease | Asymptomatic | Post-SARS-CoV-2 infection | Clonic seizure, aphasia, right-side hemiparesis, coma, and myoclonus | SARS-CoV-2-mediated encephalitis | Discharged from intensive care unit on day 17, with mild short-term memory impairment |
| 58 | Pilotto 2020, Italy [75] | 1 | 60, M | RT-PCR positive | Healthy | Mild | Initial presentation | First 5 days: irritability, confusion, and asthenia; day 4–5: cognitive fluctuation, at entry: severe akinetic syndrome, mutism, and inhibited, archaic reflexes | SARS-CoV-2-mediated encephalitis | Discharged with normal neurological features |
| 59 | Pizzanelli 2021, Italy [76] | 1 | 74, F | RT-PCR positive | Mild hypothyroidism | Severe | Initial presentation | Day 13: mild confusion and brief episode of impaired awareness; day 14: generalized tonic-clonic seizure | SARS-CoV-2-mediated autoimmune limbic encephalitis | Discharged on day 35 |
| 60 | Poursadeghfard 2021, Iran [77] | 1 | 18, F | RT-PCR positive | Healthy | NR | Initial presentation | Blurred vision, drowsy | SARS-CoV-2-mediated encephalitis | NR |
| 61 | Rebeiz 2020, USA [78] | 1 | 30 s, M | RT-PCR positive | History of alcohol abuse | Asymptomatic | Initial presentation | 1st admission: confusion, behavioral changes, psychotic features including hallucinations; 2nd admission: worsened mental status, non-verbal, progressive neurological deterioration, and seizures | SARS-CoV-2-mediated encephalitis | Died |
| 62 | Reddy 2021, USA [79] | 1 | 22, F | RT-PCR positive | Infantile seizures | Asymptomatic | Initial presentation | 2 days of headache; at entry: acute altered mental status; while hospitalized: status epilepticus | SARS-CoV-2-mediated encephalitis | Died |
| 63 | Sangare 2020, France [80] | 1 | 56, M | RT-PCR positive | Hypertension | Severe | Initial presentation | Vegetative state | SARS-CoV-2-mediated encephalitis | Discharged after 5.5 months, with mild attention deficit disorder |
| 64 | Sarmast 2022, Pakistan [81] | 1 | 63, F | RT-PCR positive | Hypothyroidism and diabetes mellitus | NR | Initial presentation | Confusion accompanied by restlessness, fearfulness, and visual hallucinations. She was anxious, agitated, and aggressive. Altered level of consciousness, slight tremors of the limbs, and psychomotor restlessness | SARS-CoV-2-mediated encephalitis | Two weeks post discharge, she was doing well, with no neurological signs and symptoms |
| 65 | Sattar 2020, Pakistan [82] | 1 | 44, M | RT-PCR positive | Healthy | Moderate | Initial presentation | Day 20: generalized tonic-clonic seizures and confusion | SARS-CoV-2-mediated encephalitis | Discharged on day 34 with normal neurological state |
| 66 | Sharma 2022, USA [83] | 3 | 43, M | RT-PCR positive | Healthy | Mild | Initial presentation | Bitemporal headache, tonic-clonic seizures, | Self-limiting hemorrhagic encephalitis | Discharged with occasional headaches |
| 43, M | RT-PCR positive | Healthy | Severe | Post-SARS-CoV-2 infection (5 days after SARS-CoV-2 infection) | Non-verbal, and had an episode of rapid eye fluttering and gaze deviation, acute respiratory distress syndrome | Self-limiting leukoencephalopathy | Discharged but complained about recurrent headaches | |||
| 52, M | RT-PCR positive | Diabetes, hypertension, and hyperlipidemia | Severe | Post-SARS-CoV-2 infection (3 weeks after SARS-CoV-2 infection) | Bifrontal headache, blurred vision, left- and right-sided ptosis, ischemic third and sixth nerve palsy | SARS-CoV-2-mediated encephalitis | Discharged with assistance. No light perception in the left eye with complete ophthalmoplegia, intact vision in the right eye with ptosis | |||
| 67 | Sofijanova 2020, Republic of Macedonia [84] | 1 | 9 months, infant | RT-PCR positive | NR | Severe | Initial presentation | Tonic-clonic seizures, disturbed consciousness, shortness of breath, weakened reaction to painful stimuli | NR | NR |
| 68 | Svedung Wettervik 2020, Sweden [85] | 1 | 40′s, F | RT-PCR positive | Healthy | Severe | Initial presentation | Coma | SARS-CoV-2-mediated AHLE | After TPE treatment for 5 days, patient showed clinical and biochemical improvements |
| 69 | Tee 2022, Malaysia [86] | 1 | 69, M | RT-PCR positive | Hypertension and atrial fibrillation | NR | Initial presentation | Altered behavior | SARS-CoV-2-mediated encephalitis | Subsequently remained well, with no neurological sequelae |
| 70 | Urso 2022, Italy [87] | 1 | 5, F | RT-PCR positive | Healthy | NR | Initial presentation | Neck swelling, right latero-cervical and painful lymphadenopathy, altered mental status, and drowsiness | SARS-CoV-2-mediated encephalitis | Discharged when COVID-19 test came back negative |
| 71 | Valadez-Calderon 2022, Mexico [88] | 1 | 28, M | NR | No history of chronic disease | Mild | Post-SARS-CoV-2 infection (2 weeks after SARS-CoV-2 infection) | Incoherent speech, somnolence, auditory hallucinations, suicidal ideation, and generalized tonic-clonic seizures | Autoimmune encephalitis (anti-NMDAR and anti-glutamic acid decarboxylase 65 co-expression) | Discharged home, but after six weeks-follow-up, he continues physical rehabilitation and presents neurological sequelae related to mood changes, irritability, and agitation episodes |
| 72 | Vandervorst 2020, Belgium [89] | 1 | 29, M | RT-PCR positive | Healthy | Moderate | Initial presentation | Confusion, disorientation in time and space, immediate and short-term memory deficits, concentration and attention difficulties, anxiety, paranoid delusions, followed by dysgeusia and anosmia | Suspected SARS-CoV-2-associated encephalitis | Improved during hospitalization |
| 73 | Woldie 2020, Canada [90] | 1 | 24, M | RT-PCR positive | AIHA | Severe | Post-SARS-CoV-2 infection (one week later at his follow-up appointment) | Persistent headache, decreased level of consciousness, and seizure activity. | SARS-CoV-2-mediated ANE | Died |
| 74 | Ye 2020, China [91] | 1 | NR, M | RT-PCR positive | NR | Moderate | Initial presentation | Confusion, altered consciousness | SARS-CoV-2 associated encephalitis | Discharged with cleared consciousness |
| 75 | Zambreanu 2020, UK [92] | 1 | 66, F | RT-PCR positive | NR | Mild | Initial presentation | Confusion, seizure, disoriented to time and place, amnestic and mild word-finding difficulties | Limbic encephalitis | Neurological recovery |
| 76 | Zandifar 2020, Iran [93] | 2 | 49, M | Not performed | NR | Severe | Initial presentation | Seizures; disorientation to place, time, and persons; and decrease of consciousness | Suspected SARS-CoV-2 associated encephalitis | Died |
| 39, M | RT-PCR positive | Moderate | Disoriented, agitated headache, tonic seizure, decreased consciousness and non-responsive verbal or painful commands | SARS-CoV-2 associated encephalitis | ||||||
| 77 | Zanin 2021, Italy [12] | 1 | 47, M | RT-PCR positive | Healthy | Mild | Initial presentation | Intense headache, epileptic seizures | SARS-CoV-2 associated encephalitis | Died |
| 78 | Zuhorn 2020, Germany [94] | 1 | 54, M | RT-PCR positive | Arterial hypertension, obesity (BMI 34 kg/m2), obstructive sleep apnea syndrome | Moderate | Initial presentation | Aggressiveness, Disorientation, and stupor | Parainfectious encephalitis | Recovered and was discharged with only mild cognitive impairment |
| No. | Study ID | Neuroimaging | Neurophysiology | Serum Analysis | CSF Analysis | Other Pathogen Investigation | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Brain CT Scan Result | Brain MRI Result | EEG Result | WBC | Total Protein (mg/dL) | Glucose (mg/dL) | SARS-CoV-2 | Other Explorations | ||||
| 1 | Ahsan 2021 | NR | Axial T2 showed left perirolandic cortex and posterior parietal lobe cerebral edema, and axial DWI showed restricted diffusion. | Cerebral slowing with left focal slowing | MOG IgG positive | Elevated | 48 | 46 | NR | OCB positive | Bacterial or viral pathogens were negative |
| 2 | Allahyari 2021 | Generalized brain edema | Generalized brain edema | NR | CRP 2+ | Elevated | 241 | 55 | Positive | Anti-NMDAR Positive, HSV 1 and HSV 2 DNA negative | NR |
| 3 | Andrea 2020 | Presented with non-specific diffuse cortical atrophy | NR | Triphasic waves were observed | Normal CRP and LDH, severe hyponatremia | Normal | 61 | 49 | Negative | None | HSV negative |
| 4 | Ayatollahi 2020 | Normal | 1st admittance: normal; 2nd admittance: signal hyperintensities on FLAIR and T2-weighted sequences in the claustrum bilaterally | 1st admittance: slow wave activity; 2nd admittance: moderate bilateral non-epileptiform abnormalities | Thrombocytopenia, normal RBC, WBC and hemoglobin, CRP. ANA, aPL, aCL, anti-dsDNA, and ANCA were negative | Elevated | 30 | 41 | Negative | None | HSV negative |
| 5 | Ayuningtyas 2022 | NR | No lesion or intracerebral or intracerebellar pathological enhancement was found | NR | Increased CRP level, and increased D-dimer level | Elevated | 108 | 63 | Positive | No Bacteria and AFB | Anti-HIV, HbSAg, anti-HCV, HSV, and CMV negative |
| 6 | Ayuso 2020 | Normal | 2nd admittance: hyperintense lesions in the caudal vermis and right flocculus, and contrast enhancement was observed in the floor of the fourth ventricle | Normal | Normal | Normal | 41 | 70 | NR | OCB, anti-Hu, anti-Yo, anti-Ri, anti-CV2, anti-Ma2, and anti-amphiphysin abs were negative | Anti-GD1 was positive. HIV, VZV, EBV, CMV, and Mycoplasma Pneumoniae were negative |
| 7 | Babar 2020 | Normal | Normal | Generalized slowing | Elevated CRP, ferritin, TPO ab, and D-dimer. Negative anti-NMDAR ab, anti-GAD ab, VGKC ab, ANA, ANCA, IgM anti-β2-GPI ab, anti-DNase B ab, anti-streptolysin ab, IL-1 β, IL-6, IL-10, IL-2, C3, and C4 | Normal | 18 | 74 | Negative | None | Gram bacteria negative |
| 8 | Benameur 2020 | NR | Cerebral hemispheric restricted diffusion and cerebral edema | NR | Increased levels of anti-S1 IgM; anti-E IgM, IL-6, IL-8, IL-10, IP-10, and TNF-α | Elevated | >200 | 40 | Negative | None | Influenza A virus positive, influenza B virus negative |
| NR | Splenium lesion and FLAIR recovery | Diffuse slowing | Normal | 37 | 111 | Negative | None | Bacterial or viral pathogens were negative | |||
| NR | Equivocal fluid-attenuated inversion recovery, FLAIR abnormality in the right temporal lobe | NR | Normal | 21 | 88 | Negative | None | Bacterial or viral pathogens were negative | |||
| 9 | Bernard-Valnet 2020 | NR | Normal | Nonconvulsive, focal status epilepticus, slowed theta background rhythm | NR | Mild elevated | 46.6 | NR | Negative | None | Bacterial or viral pathogens were negative |
| NR | Normal | NR | NR | Mild elevated | 46.1 | NR | Negative | None | |||
| 10 | Bhavsar 2020 | Normal | NR | Slow background without epileptiform discharges or seizures | Normal CBC, CRP and ESR, negative autoimmune encephalopathy antibody panel, hyponatremia | Elevated | 173 | 35 | Negative | None | Bacterial or viral pathogens were negative |
| 11 | Bodro 2020 | Normal | Normal | NR | Elevated D-dimer | Elevated | 105.5 | 80 | Negative | Elevated IL-1β, IL-6, ACE | Bacterial or viral pathogens were negative |
| Normal | Normal | NR | Elevated CRP, ferritin, LDH, and D-dimer, mild platelet reduction | Elevated | 115.5 | 54 | Negative | Elevated IL-6, ACE | NR | ||
| 12 | Burr 2021 | NR | Normal | NR | Normal CRP and ESR and positive NMDAR-IgG positivity | NR | 25 | 56 | Negative | None | Bacterial or viral pathogens were negative |
| 13 | Cao 2020 | NR | Bilateral hyperintense lesions in the deep and periventricular supratentorial white matter, either punctiform and slightly diffuse (cases 1–3) or diffuse and confluent (cases 4 and 5), associated with lesions in the pons for two patients (cases 1 and 2) | Unspecific slow-wave activity | Elevated IL-6 | normal | 32 | NR | Negative | Normal IL-6 | NR |
| Normal IL-6 | 26 | Negative | Normal IL-6 | ||||||||
| Elevated IL-6 | 115 | Negative | Elevated IL-6 | ||||||||
| Elevated IL-6 | 18 | Negative | None | ||||||||
| Elevated IL-6 | 18 | Negative | Normal IL-6 | ||||||||
| 14 | Casez 2021 | NR | Hyperintensity of the olfactory tracts on T2 fluid-attenuated inversion recovery, and diffusion-weighted imaging | NR | NR | 8 WBC | Normal | NR | Negative | None | NR |
| 15 | Chalil 2020 | Extensive bilateral parietal and occipital intraparenchymal hemorrhage and extensive edema causing hydrocephalus | Cortical gadolinium enhancement with hyper-intense T2 and FLAIR signal surrounding the hemorrhages | Mild diffuse slowing | Elevated D-dimer, CRP, and ferritin | Elevated | NR | NR | Negative | Elevated CSF IgG ratio | Negative for VZV, HSV, and ENV |
| 16 | Cheraghali 2021 | NR | Symmetric, cortical, and juxtacortical high T1 and T2 signal abnormality, in bilateral parieto-occipital lobes | NR | Elevated level of blood sugar, AST, ALT, ESR, LDH, and positive CRP test | Normal | 15 | 100 | Positive | Negative for bacterial growth | HSV 1 and HSV 2 negative |
| 17 | Dahshan 2022 | Normal | Normal | NR | NR | Normal | Normal | Normal | NR | HSV 1 and HSV 2 negative | NR |
| 18 | Dono 2021 | NR | Axial T2 fluid-attenuated inversion recovery (T2-FLAIR) and axial diffusion-weighted imaging showed hyperintense lesions of the bilateral parietal cortex, left temporal cortex, and right cingulate cortex | Epileptiform abnormalities, continuous sharp waves and spike-and-slow-wave complexes | Slight lymphocytopenia, elevated D-dimer, normal CRP | Elevated | 47 | 78 | Negative | OCB positive | HSV, EBV, CMV, and VZV were negative |
| 19 | Duong 2020 and Huang 2020 | Normal | NR | Generalized slowing with no epileptic discharges | Normal | Elevated | 100 | 120 | Positive | None | Negative for bacterial culture and HSV 1 |
| 20 | Durovic 2021 | NR | Multiple disseminated pathological T2 and FLAIR hyperintensities | NR | Lyme borreliosis and HIV was negative, MOG antibody positive | Elevated | 39.9 | 64 | Negative | HSV 1 and HSV 2 negative | Complete recovery over the follow-up of 2 months |
| 21 | Efe 2020 | NR | Hyperintense signal in the left temporal lobe in T2 and T2 FLAIR | NR | NR | NR | NR | NR | NR | None | NR |
| 22 | El Aoud 2021 | Normal | Focal hyperintense signal in the splenium of the corpus callosum on T2 FLAIR and diffusion-weighted images | Slow oscillations without epileptiform features | Lymphophenia, elevated CRP and ferritin, hypoalbuminemia, ANA, and ANCA were negative | normal | 49 | 55 | NR | None | Mycoplasma pneumoniae, syphilis, HIV, influenza A and B were negative |
| 23 | Elmouhib 2022 | Normal | High-signal intensity lesion on DWI, T2 FLAIR in the temporal lobes, without diffusion restriction on apparent diffusion coefficient map | NR | CRP at 200 mg/L with a negative PCT at 0.05 μg/L, ferritin at 2300 μg/L | Normal | 100 | 63 | NR | NR | NR |
| 24 | Esmaeili 2022 | NR | Extensive high signal lesions in T2W and FLAIR sequences on bilateral cerebral hemispheres, para-ventricular and subcortical white matter, middle cerebellar peduncles, centrum semi vale, corpus callosum, basal ganglia, thalami, midbrain, and pons. Post-contrast MRI showed sparse enhancements on midpart of the midbrain and left parietal lobe | NR | Elevated CRP and ESR, prothrombin time and partial thromboplastin time were normal | Normal | Normal | Normal | Negative | EBV, HSV, CMV, VZV negative | NR |
| 25 | Etemadifar 2020 | Generalized brain edema and signs of brain herniation | Generalized brain edema, downward herniation of cerebellar tonsils and brain stem, and FLAIR hyperintensities in bilateral cerebral cortices and corpus striatum | Normal | Leukocytosis, lymphopenia, elevated D-dimer | NR | NR | NR | NR | None | NR |
| 26 | Ferdosian 2021 | NR | Diffuse brain edema | NR | CPK: 42, LDH: 554, CRP: weakly +, ESR: 6. COVID-19 PCR was negative | Normal | 30 | 57 | Positive | HSV, Enterovirus negative | NR |
| 27 | Freire-Álvarez 2020 | Normal | Extensive involvement of the brain, including cortical and subcortical right frontal regions, right thalamus, bilateral temporal lobes and cerebral peduncles, with no leptomeningeal enhancement | NR | Elevated ferritin, IL-6, and D-dimer | Elevated | 198 | 48 | Negative | None | CMV, HSV 1 and 2, human HHV 6, HPeV, and VZV negative |
| 28 | Gaughan 2021 | NR | Two tiny punctate T2/FLAIR hyper-intensities in the centrum semiovale bilaterally | Delta slowing | Autoimmune antibody panel negative | NR | 43 | 52.2 | Negative | Autoimmune antibody panel negative | HSV and VZV negative |
| 29 | Ghosh 2020 | NR | Non-enhancing altered intensity lesions in the left high fronto-parietal and right posterior parietal areas with peri-lesional edema; isolated cortical venous thrombosis | NR | All blood parameters normal | Elevated | 60 | 70 | Negative | Elevated IgG index, and OCB negative | Bacterial or viral pathogens were negative |
| 30 | Grimaldi 2020 | NR | Normal | Symmetric diffuse background slowing | Elevated fibrinogen and CRP, IgG autoantibodies extremely high | Normal | 49 | NR | Negative | OCB negative and IgG autoantibodies | NR |
| 31 | Gunawardhana 2021 | Bi-frontal white matter oedema | T2 FLAIR hyperintensities in the periventricular white matter, mainly clustered around frontal and occipital horns. FLAIR hyperintensities were also noted in the splenium, basal ganglia, and ventral pons | Low wave discharges consistent with encephalitis | Hemoglobin, liver function tests, creatinine and electrolytes were within normal limits, inflammatory markers (ESR, CRP) were mildly elevated | Elevated | Normal | Normal | SARS-CoV-2 IgM and IgG antibodies are positive SARS-CoV-2 RNA negative | HSV 1 and HSV 2, Japanese encephalitis, VZV were negative | NR |
| 32 | Haider 2020 | Normal | Small acute/subacute lacunar infarcts and a patchy area of T2 bright signals in the cortical and periventricular regions, consistent with cerebritis | Global cerebral dysfunction and severe toxic metabolic encephalopathy | Autoimmune antibody panel negative | Normal | 77 | 86 | Negative | None | Bacterial or viral pathogens were negative |
| 33 | Hassan 2021 | NR | Mild periventricular ischemic changes | NR | Increased CRP, D-dimer, and serum ferritin | Normal | NR | NR | Positive | HSV, OCBs were negative | NR |
| 34 | Hayashi 2020 | NR | Abnormal hyperintensity in the splenium of corpus callosum on diffusion-weighted image | NR | Elevated CRP, lymphopenia | NR | NR | NR | NR | None | NR |
| 35 | Kahwagi 2021 | NR | Normal | Overall slowing of the pattern with the presence of diffuse pseudoperiodic complexes predominating in fronto-temporal area | Elevated CRP | Normal | 76 | NR | NR | None | NR |
| 36 | Kamal 2020 | Multiple hypodensities in the external capsules bilaterally, the insular cortex, and the deep periventricular white matter of the frontal lobes bilaterally | Abnormal signal intensity in the temporal lobe cortex bilaterally in a rather symmetrical fashion. In addition, the involvement of the parasagittal frontal lobes bilaterally was evident as well, displaying bright signals on T2-fluid-attenuated inversion recovery and T2-weighted images with corresponding diffusion restriction | Did not display any significant epileptic discharges, possibly due to the masking effect of lorazepam | Elevated D-dimer | Normal | 55 | 67 | Positive | Normal LA, RF, ANA and aCL | Mycobacterium Tuberculosis, Gram bacteria, HSV, HHV, and VZV were negative |
| 37 | Kasturiarachi 2022 | NR | Contrast-enhancing lesion in the left occipital, temporal, and frontal lobes, the vermis folia, and tectal plate colliculi; hyperperfusion on arterial spin labeling in the left hemisphere | Left hemispheric poly spike and waves | Elevated LDH, reticulocyte count and bilirubin, schistocytes, and low haptoglobin. Positive ANA, high anti-SSA (anti-Ro) and anti-SSB (anti-La) antibodies, and significantly elevated COVID-19 antibody | NR | NR | NR | Negative | Meningitis/encephalitis panel negative | NR |
| 38 | Khoo 2020 | NR | Normal | Normal | Elevated CRP and D-dimer | Normal | Normal | Normal | Negative | Anti-NMDAR ab and A panel of antineuronal abs and OCB were negative | NR |
| 39 | Kimura 2021 | NR | No significant abnormalities | No evidence of seizure activity nor response to photic and sound stimuli | Seropositive for anti–SARS-CoV-2 antibodies | Normal | 20 | 164 | Negative | OCBs positive | Campylobacter jejuni, Haemophilus influenzae, Mycoplasma pneumoniae, cytomegalovirus, and EBV negative |
| 40 | Koh 2022 | Patchy ground-glass opacities on bilateral lung fields, compatible with COVID-19 pneumonia | Diffuse cortical high signal intensities, especially on bilateral insula with increased arterial spin labeling signals | Repeated high-amplitude polymorphic delta activities from the right frontotemporal area evolving to generalized 1–2 Hz spike-wave discharges, suggesting an impending focal status epilepticus | IL-6 was mildly elevated to 21.7 pg/mL, CRP level normal | Elevated | NR | NR | Negative | Elevated IL-6 | HSV, VZV, enterovirus, tuberculosis, EBV, toxoplasmosis, and syphilis negative |
| 41 | Kumar 2020 | Hypodensities in both thalami and left caudate nucleus; left parasellar-middle cranial fossa mass | Left parasellar-middle cranial fossa mass (MRI was performed about 2 weeks earlier than CT) | NR | Leukocytosis | Normal | Elevated | NR | NR | None | HSV and VZV were negative |
| 42 | Kumar 2022 | NR | Subcortical volume loss (right occipital and left parieto occipital) with cystic changes, tiny hemorrhages at the caudothalamic groove with loss of myelination at the posterior limb of internal capsule | Normal | COVID Ig G And Ig M antibodies were positive | Normal | Normal | Normal | NR | NR | NR |
| 43 | Marques 2022 | Normal | Did not show any pathological changes | Moderate encephalopathy | Elevated LDH and d-dimers | Elevated | 82 | 59 | Negative | HSV, VZV, cytomegalovirus negative | HSV, HIV, VZV negative |
| Normal | Did not show any pathological changes | Mild encephalopathy, without epileptiform activity | HSV 1–2, HIV, and VZV Negative | Normal | 16 | 93 | Negative | HSV, VZV, cytomegalovirus negative | NR | ||
| 44 | McAbee 2020 | Negative | NR | Frontal intermittent delta activity | NR | Mild elevated | 97 | 92 | NR | None | NR |
| 45 | Mekheal 2022 | Without contrast, an old left cerebellar infarct, with no evidence of acute infarct or hemorrhage | Old infarct, acute infarct involving the left cerebellum, as well as an effacement of the left temporal horn and edema within the left pons, midbrain, left temporal lobe, and surrounding the basal ganglia | Moderate-severe diffuse encephalopathy without epileptiform discharges or seizures | Elevated ESR, CRP, and D-dimer, serum COVID-19 IgG antibody positive | Elevated | 145 | 75 | Negative | Meningitis/encephalitis panel by PCR were negative, including all microbial cultures | NR |
| 46 | Meshref 2021 | Right temporal hypo-dense area | Ill-defined area of faint low signal intensity lesion in T1, hyperintense in T2. FLAIR images showed partial restriction in DWI with no significant enhancement post IV gadolinium contrast injection, involving the right cerebral hemisphere, mainly at the temporal area, suggesting encephalitis | NR | NR | NR | Normal | Normal | NR | No bacterial growth, herpes virus was negative | NR |
| 47 | Mierzewska-Schmidt 2022 | NR | Diffuse areas of oedema associated with numerous symmetrical changes with punctate hemorrhages in basal ganglia, thalami, brainstem, and cerebral gray matter | NR | Low Hb 9.3 g/dL and Platelet count 183 × 103/μL, CRP 7.4 mg/L, D-dimers 0.97 | Elevated | 660.00 | < 10 | Positive | Elevated lactic acid, meningoencephalitis PCR panel was negative | All bacterial cultures were negative |
| 48 | Miqdad 2021 | Unremarkable | Normal | Different abnormalities suggestive of encephalitis | CRP, D-dimer, and procalcitonin were high | Elevated | 832 | 2.59 | NR | HSV PCR and gram stain negative | NR |
| 49 | Monti 2020 | NR | Normal | Abnormal | Elevated levels of IL-6 | Elevated | NR | NR | NR | OCB and anti-NMDAR ab positive, with elevated levels of IL-6 and IL-8 | Bacterial or viral pathogens were negative |
| 50 | Moriguchi 2020 | Normal | Diffusion -weighted images showed hyperintensity along the wall of inferior horn of right lateral ventricle. FLAIR images showed hyperintense signal changes in the right mesial temporal lobe and hippocampus with slight hippocampal atrophy | NR | Elevated levels of WBC and CRP | Mild elevated | NR | NR | Positive | NR | HSV and VZV were negative |
| 51 | Morvan 2020 | Acute hydrocephalus with diffuse cerebral edema, spontaneous bilateral thalamic hyperdensities, with discrete contrast enhancement and spontaneous hyperdensity in subarachnoidal spaces. | Hypersignal of both thalami brainstem and cerebellum with some hemorrhagic component on T2 sequences | NR | Elevated levels of CRP, fibrinogen, and D-dimer Low Hb, high AST, low factor V, high troponin, high creatinine, very low kaliemia | Normal | 79 | NR | Negative | None | HIV negative |
| 52 | Mullaguri 2021 | Axial sections of the brain showed punctate hemorrhages in the right frontal and left frontal and parietal areas | Axial section showed hyperintensities in bilateral centrum semiovale areas. MRI of the brain showing innumerable punctate microhemorrhages in the cerebellar peduncles and subcortical regions of bilateral hemispheres, including bilateral basal ganglia and internal capsules | NR | Hyponatremia (132 mMol/L), significant elevations in D-dimer, LDH, ferritin, CRP, and CK | NR | NR | NR | NR | NR | NR |
| 53 | Natarajan 2020 | NR | Normal | Normal | NR | Elevated | 86 | 77 | Negative | None | HSV, CMV, and VZV were negative |
| 54 | Oosthuizen 2021 | Central midbrain hypodensity | Features consistent with brainstem encephalitis | Normal | Elevated ESR | Elevated | 37 | 65 | Positive | Immunoglobulin G index 0.62, SARS-CoV-2 antibody negative | Tests for infections and malignancy negative |
| 55 | Orsini 2021 | NR | Normal | Normal | NR | Normal | 60 | 53 | Positive | Bacterial culture negative | NR |
| 56 | Panariello 2020 | Normal | NR | Theta activity at 6 Hz | Elevated CRP and D-dimer with negative ANA, ANCA, anti-ENA, aCL, and anti-β2-GPI abs | NR | 65.4 | 70 | Negative | Elevated IL-6 and anti-NMDAR ab | HSV, EBV, CMV, VZV, and enterovirus were negative |
| 57 | Picod 2020 | Normal | Bilateral lesions (hypersignal or enhancement of meninges, cortical and subcortical regions spread over the insula, the cingula, the medial part of occipital areas, and the internal part of the left-side temporal lobe) | Diffuse intermittent periodic activity | Moderately elevated IL-6 | Normal | 28 | NR | Negative | Elevated IL-6 and OCB negative | HSV negative |
| 58 | Pilotto 2020 | Normal | Normal | Generalized slowing, with decreased reactivity to acoustic stimuli | Elevated D-dimer, a wide immunological screening of immune-mediated encephalitis was negative | Mild elevated | 69.6 | NR | Negative | Slightly elevated IL-6, strongly elevated IL-8, TNF-α and β2M | Neurotropic viruses negative |
| 59 | Pizzanelli 2021 | Normal | Bilateral symmetrical mesial temporal lobes T2/FLAIR/DWI hyperintensities, with mild hippocampal thickening | Autoimmune panel for encephalitis negative | Elevated CRP and fibrinogen | Normal | 104 | 67 | Negative | OCB and autoimmune panel for encephalitis negative | Neurotropic viruses negative |
| 60 | Poursadeghfard 2021 | NR | FLAIR increased signal intensity in the cortical and subcortical regions of both mesial temporal lobe as well as both side hippocampal tails, with relative symmetrical appearance without evidence of significant enhancement or restricted DWI compatible with viral or autoimmune encephalitis | NR | NR | NR | NR | NR | NR | NR | Cat-scratch disease, toxoplasmosis, syphilis, Lyme disease, brucellosis, HIV, VZV, HSV, CMV, EBV, and hepatitis B and C were negative |
| 61 | Rebeiz 2020 | A questionable subarachnoid hemorrhage within the mesial parietal region and nonspecific hypoattenuation in the splenium of the corpus callosum | 1st MRI: DWI and FLAIR hyperintensity of the splenium of corpus callosum; 2nd MRI (after readmission): new abnormal T2/FLAIR hyperintense and restricted diffusion involving the left thalamus, right parasagittal frontal cortex, and bilateral genu of the corpus callosum | Generalized slowing | VES 27; Normal IL-6 and CRP | Elevated | 297 | 56 | Negative | None | Neurotropic viruses negative |
| 62 | Reddy 2021 | 4 days after admission: severe diffuse cerebral edema with cerebellar tonsillar herniation | No acute intracranial process | NR | NR | Normal | 108 | 88 | NR | None | Bacterial or viral pathogens were negative |
| 63 | Sangare 2020 | NR | Multiple small hemorrhagic lesions in the pontine tegmentum, bilateral subinsular region | Poorly reactive delta slow waves | NR | Normal | Normal | Normal | NR | None | NR |
| 64 | Sarmast 2022 | Unremarkable | Hyperintense signals in frontoparietal and parietotemporal lobes on FLAIR/T2 sequence | NR | Mildly elevated CRP, elevated LDH, CPK, ferritin, and D-dimer | Normal | 66 | 81 | Negative | VZV PCR, HSV 1–2 PCR, CMV PCR, bacterial antigen negative | Negative for HSV 1–2, HIV, enterovirus, and VZV virus |
| 65 | Sattar 2020 | Day 20: few scattered foci of white matter hypo-attenuation | Day 25: abnormal medial cortical signals in the bilateral frontal lobe region | NR | Autoimmune antibody panel negative | Mild elevated | 39 | 75 | Positive | CSF color pinkish | Bacterial or viral pathogens were negative |
| 66 | Sharma 2022 | left temporal hypodensity | Intense focal edema within the left hippocampus with mild restricted diffusion, postcontrast enhancement, and hemorrhage seen on susceptibility-weighted imaging | Normal | Creatinine of 1.3 mg/dL, CRP of 42.4 mg/L, ESR of 95 mm/h, CK 858 IU/L, D-Dimer of 1821 FEU, fibrinogen of 644 mg/dL, ferritin of 1352.9 ng/mL, LD of 392 IU/L, prothrombin time (PT/INR) of 1.3/15 | Elevated | 44 | 59 | NR | Gram stain, bacterial culture, and meningitis/ encephalitis panel were negative. VZV PCR, cryptococcal antigen, culture, AFB smear and culture, and CMV PCR were negative. VZV IgG elevated | NR |
| Small right temporal hyperdensity (0.6 cm diameter) suggestive of a hemorrhage with normal vasculature | Right anterior temporal lobe intraparenchymal hemorrhage; additional multiple scattered foci of susceptibility artifact particularly in the gray–white junctions and corpus callosum; and sulcal FLAIR hyperintensity in the right frontal, biparietal, and left temporal lobes | NR | Elevated IL-6, fibrinogen, and thrombocytopenia | Elevated | 118 | 28 | NR | Meningitis/encephalitis panel, AFB smear and culture, cryptococcal antigen, and VZV PCR, CMV PCR, CSF cytology were negative | NR | ||
| 1st admission: stenosis of the cavernous segment of the right ICA. 2nd admission: unremarkable | 1st admission: mild periventricular white matter disease. 2nd admission: multiple punctate foci of restricted diffusion in the bilateral frontal, parietal, occipital, and temporal lobes, mild meningeal enhancement of the anterior and middle cranial fossa, and opacification of multiple ethmoid and mastoid air cells | NR | 1st admission; creatinine of 1.4 mg/dL, ESR 111 mm/h, CRP 43.5 mg/L, and HbA1c 12.6%. 2nd admission: fibrinogen of >1000 mg/dL, ferritin of 743 ng/mL, ESR of >130 mm/h, CRP of 313 mg/L, PT/INR of 19/1.6, procalcitonin of 1.24 ng/mL, and antithrombin-3 activity of 62% | Elevated | 82 | 78 | NR | Borrelia burgdorferi IgM/IgG titer (0.09 LIV, 0.09 LIV), negative CSF ACE, VDRL, and cryptococcal antigen, EBV PCR positive | AIDP, myasthenia gravis, or vasculitis, secondary infections, mycoplasma IgM, anti-cardiolipin antibodies, B-2 glycoprotein, anti-Xa essay, HIV antibodies, hepatitis panel, serum cryoglobulin PAVAL, autoimmune encephalitis panel were negative | ||
| 67 | Sofijanova 2020 | Enlargement of the lateral ventricles, intraventricular masses, pronounced internal hydrocephalus. | NR | NR | Normal | NR | 202.7 | 91.4 | NR | None | NR |
| 68 | Svedung Wettervik 2020 | White matter brain edema with compressed convexity sulci | Increased white matter intensity on flair images, microhemorrhages with involvement of basal ganglia on susceptibility-weighted imaging | Pronounced, generalized slowing over both hemispheres, no electrographic epileptic activity | Mild increased IL-6 | Elevated | NR | 86.4 | Negative | Elevated levels of IL-6 | Negative for bacteria and neurotropic viruses |
| 69 | Tee 2022 | Noncontrast brain CT revealed an old right lenticular infarct | Performed 1 month later, normal findings | Performed 3 weeks later, normal findings | NR | Elevated | 116 | NR | Positive | NR | NR |
| 70 | Urso 2022 | NR | CNS involvement, suggestive of encephalitis | A slow base rhythm (theta-delta) together with synchronous bilateral potentials formed by slow waves with predominance on the right side. | NR | Normal | 27 | Normal | Negative | No bacterial or tuberculous infection | HSV1, varicella-zoster, EBV, and CMV were negative |
| 71 | Valadez- Calderon 2022, Mexico | NR | Hyperintensities in the bilateral anterior cingulate cortex and temporal lobes | Subcortical dysfunction in frontal, temporal, and occipital regions | Normal | Normal | Normal | Normal | Negative | NR | NR |
| 72 | Vandervorst 2020 | Normal | Asymmetric FLAIR hyperintensity of the left medial temporal cortex associated with mild gyral expansion | General excess of beta-rhythm | NR | Normal | Normal | Normal | Negative | None | Negative for enterovirus and HSV |
| 73 | Woldie 2020 | Non-specific symmetric cerebral enhancement | T2/FLAIR hyper intensity on the medial aspect of each temporal lobe, bilateral basal ganglia, and medial thalami consistent with severe acute necrotizing encephalitis | NR | Elevated LDH | NR | NR | NR | NR | NR | Positive for Cryptococcus neoformans |
| 74 | Ye 2020 | Normal | NR | NR | Low WBC and lymphocytes | Normal | 27 | 56.5 | negative | None | Negative for bacterial or tuberculous infection |
| 75 | Zambreanu 2020 | Normal | Non-enhancing, symmetrical T2 and FLAIR hyperintensities in mesial temporal lobes and medial thalami and to a lesser extent upper pons, as well as scattered subcortical white matter hyperintensities | NR | Elevated CRP, lymphopenia | Normal | 100 | 63 | Negative | Autoimmune antibody panel negative | Negative for streptococci, meningococcus, haemophilus, listeria, Escherichia coli, HSV 1 and 2, HHV6, enteroviruses, parechovirus, CMV, VZV, and Cryptococcus |
| 76 | Zandifar 2020 | Diffuse brain parenchymal edema and reduced lateral ventricles | NR | NR | Leukocytosis and lymphopenia | Mild elevated | 70 | 30 | Negative | None | NR |
| NR | Leukocytosis and lymphopenia and LDH elevated | Mild elevated | 74 | 33 | Positive | ||||||
| 77 | Zanin 2021 | Increasing vasogenic oedema in the right temporo-fronto-parietal region with extension to the capsular region, to the cerebral peduncle and in the ipsilateral mesencephalic region. Severe compressive effect on the right lateral ventricle | Severe vasogenic oedema of the white matter with 10 mm shift of the midline and compression of the right lateral ventricle; DWI: extensive cortical marked restriction | NR | Increased CRP and WBC with lymphopenia | NR | NR | NR | NR | None | NR |
| 78 | Zuhorn 2020 | NR | Signal alterations within the claustrum/external capsule region, showed reduced diffusion | NR | LDH, D-dimer, myoglobin, IL-6 and CRP, IgA and IgG positive for SARS-CoV-2 | Mild elevated | 39.6 | 57 | Negative | None | Negative for HSV, VZV, cytomegaly and Epstein Barr virus |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.A.; Cavestro, C.; Alam, S.S.; Kundu, S.; Kamal, M.A.; Reza, F. Encephalitis in Patients with COVID-19: A Systematic Evidence-Based Analysis. Cells 2022, 11, 2575. https://doi.org/10.3390/cells11162575
Islam MA, Cavestro C, Alam SS, Kundu S, Kamal MA, Reza F. Encephalitis in Patients with COVID-19: A Systematic Evidence-Based Analysis. Cells. 2022; 11(16):2575. https://doi.org/10.3390/cells11162575
Chicago/Turabian StyleIslam, Md Asiful, Cinzia Cavestro, Sayeda Sadia Alam, Shoumik Kundu, Mohammad Amjad Kamal, and Faruque Reza. 2022. "Encephalitis in Patients with COVID-19: A Systematic Evidence-Based Analysis" Cells 11, no. 16: 2575. https://doi.org/10.3390/cells11162575
APA StyleIslam, M. A., Cavestro, C., Alam, S. S., Kundu, S., Kamal, M. A., & Reza, F. (2022). Encephalitis in Patients with COVID-19: A Systematic Evidence-Based Analysis. Cells, 11(16), 2575. https://doi.org/10.3390/cells11162575