1. Introduction
VR technology has applications in a wide range of fields, including entertainment, gaming, and, more recently, healthcare. The healthcare sector has increasingly recognized the potential of VR, with a particular focus on its use in cognitive-behavioral therapy (CBT) to address various mental health conditions [
1,
2]. VR’s immersive and interactive nature offers a highly personalized and engaging therapeutic experience, effectively simulating real-life situations and environments [
3]. The inclusion of features like safety ensures patients can explore these virtual environments without risks, further enhancing the overall quality and effectiveness of therapeutic applications in a secure environment.
Studies have demonstrated the versatility of VR in healthcare, showcasing its ability to assess neurocognitive deficits, study clinical symptoms, and provide cognitive rehabilitation, social skills training interventions, and virtual reality-assisted therapies for conditions like psychosis. The impact of this technology extends to addressing mental health issues and healthcare-related challenges, such as schizophrenia [
4,
5].
While VR holds promise in healthcare, it is essential to acknowledge that it is still a relatively new and evolving technology [
5,
6]. Therefore, VR treatments require thorough testing and validation through clinical trials and scientific studies to ensure their safety, effectiveness, and suitability for clinical use [
7]. These research efforts are essential to establishing evidence-based guidelines for VR’s integration into healthcare, ultimately ensuring that patients receive the highest standard of care.
Schizophrenia is a complex mental disorder that profoundly affects an individual’s perception of reality, thought processes, emotions, and behavior [
6]. Its symptoms can be broadly categorized into two main groups: positive and negative. Positive symptoms encompass delusions, hallucinations, disordered thinking, and abnormal behaviors that often blur the line between reality and imagination. These symptoms can make it challenging for individuals to discern what is real from what is not [
8]. On the other hand, negative symptoms involve a reduction or loss of typical mental functions and behaviors that healthy individuals possess [
9,
10]. This category includes diminished emotional expression, social withdrawal, lack of motivation (avolition), decreased speech output, and an impaired ability to experience pleasure (anhedonia). Negative symptoms can be particularly debilitating for individuals with schizophrenia, leading to a loss of interest in daily activities, social isolation, and difficulties with tasks like employment or academic performance [
8]. Notably, these symptoms often prove less responsive to medication than positive symptoms [
4].
Treatment for negative symptoms of schizophrenia commonly includes a combination of antipsychotic medications, CBT, and lifestyle adjustments [
4,
11]. This multifaceted approach is necessary to address the lack of motivation, social withdrawal, and difficulties in initiating and maintaining daily activities, which are characteristic of these debilitating symptoms [
9,
10]. Thus, these interventions aim to improve the overall quality of life for individuals with schizophrenia and enhance their psychosocial integration. Yet, CBT has been explored for schizophrenia treatment with mixed results. While it has shown promise in reducing symptom severity and improving functioning, limitations include variable effectiveness, cognitive impairments, and resistance to insight. The integration of VR games in schizophrenia treatment holds potential benefits, such as enhanced engagement, simulated environments for exposure therapy, and personalized interventions [
12].
Overall, VR CBT has the potential to be a powerful tool for treating neurological and psychological disorders like schizophrenia, but further research and improvements are needed to make it more accessible and effective [
5,
6,
13,
14].
This research area is actively striving to develop practical and readily available solutions for both patients and healthcare practitioners. Correspondingly, upon examination of related work and available technologies, it was designed and implemented a system that encompasses an immersive VR game. The system must be played by a patient accompanied by their therapist, who can watch and assist in the gameplay. To assess the usability of the game, tests with 21 healthy subjects were performed. Thus, the goal for this investigation is to evaluate the usability of an immersive VR serious game intended to treat negative symptoms, while also analyzing its outcomes to further support the validation of VR technology in the context of CBT treatments.
In this study, our objective is to investigate whether VR can yield benefits in the treatment of negative symptoms in schizophrenia. We aim to identify current limitations in VR treatments, explore areas for potential improvement, and examine the impact of realism on the overall VR experience.
This article extends our work presented in the 11th International Conference on Serious Games and Applications for Health (SeGAH), in Athens, Greece [
15]. The rest of the paper is structured as follows.
Section 2 presents a brief review of the existing research papers on the same subject. In
Section 3, it is described the methodology used to achieve the results of the study.
Section 4 reveals the results obtained. In
Section 5 an analysis is made of the obtained results. Finally, in
Section 6, major conclusions are drawn and directions for future work are suggested.
2. State-of-the-Art
While VR serious games are gaining popularity for treating various psychological issues, for instance the treatment of anxiety in studies [
16,
17], our research exclusively centers on addressing the negative symptoms of schizophrenia. By focusing our work in this particular area, we want to have a significant impact on people dealing with the difficult challenges associated with schizophrenia.
CBT approaches offer a diverse range of methods for enhancing the social and functional skills of individuals, particularly those dealing with schizophrenia. These approaches encompass individual conversations, group sessions, and the innovative use of immersive VR technology. Notably, studies in this field have focused on employing VR to improve social skills and alleviate negative symptoms associated with the condition.
Among the studies, several noteworthy immersive VR programs have emerged to address the unique challenges faced by schizophrenia patients in social settings. These include GameChange [
3], soskitrain [
4], Multimodal Adaptive Social Intervention in Virtual Reality (MASI-VR) [
9], Social Skills Training VR (SST-VR) [
13], Virtual Reality Virtual Training System (VRVTS) [
18], Fruit Pioneer [
19] and VR Social Cognition and Interaction Training (VR-SCIT) [
20] each with its distinct approach and objectives.
GameChange [
3], for instance, stands out as an automated VR game specifically designed to help individuals cope with social avoidance in everyday situations. It does so without requiring the presence of a therapist, allowing patients to practice and develop their social skills independently. This approach utilizes immersive VR scenarios that mimic real-life experiences, including grocery shopping, visiting a bar, and going to a doctor’s office. The research involved conducting two sessions with six patients to assess the game’s usability, focusing on its level of immersiveness, user-friendliness, and overall engagement.
Similarly, soskitrain [
4] aims to enhance daily functioning and social skills by offering a platform for social interaction practice. This immersive VR program provides scenarios like managing a store, simulating various environments such as a house, boutique store, bus stop, bar, cafeteria, grocery store, and market. The program progressively increases the game’s difficulty to target a wide range of social skills, including facial emotion recognition, customer interaction, conversation, and emotion regulation. It used a repeated measures design to study the impact of a combined social skills training intervention, including traditional methods and a VR program. Statistical analyses assess changes over time, with a focus on significant improvements and intervention effectiveness.
MASI-VR [
9] was composed of social missions of varying difficulty levels. Participants freely explored the virtual space, interacting with avatars, and engaged in consequence-free social interactions. Participants recruited from outpatient day facilities underwent pre-training assessments, ten MASI-VR sessions, and a post-training assessment. Assessments covered intellectual ability, psychiatric symptoms, and social functioning, conducted by trained personnel not involved in participant training. The study aimed to evaluate the feasibility and acceptability of improving social functioning in schizophrenia by encouraging patients to initiate conversations with strangers for information-seeking purposes.
SST-VR [
13] allows patients to engage in VR-based practice sessions to improve conversational, emotional, and assertiveness skills. Much like the other VR studies, it uses immersive simulations of common social scenarios to provide a safe and stress-free environment for skill development. The study randomized 91 participants with schizophrenia into VR-based and Traditional-based interventions. Both groups had 10 sessions over five weeks, focusing on social skills. Outcomes included role-play tests and self-report on assertiveness and relationship skills. Post-session measures assessed motivation and generalization. The goal was to compare the effectiveness of VR to traditional role-play social skills training in schizophrenia.
In VRVTS [
18], the game makes players act as salespeople and use their skills to manage a store efficiently. This addition to the VR studies enriches the range of scenarios for patients to practice their social and functional skills. The study employed a single-blinded randomized clinical trial design to assess the impact of vocational rehabilitation programs on patients with schizophrenia. Participants were randomly assigned to three groups: VR-based, therapist-administered, and conventional. Outcome assessments were conducted by blinded assessors, and statistical analyses included descriptive statistics. The aim was also to evaluate the effectiveness of the programs.
The game Fruit Pioneer [
19] involved slicing different kinds of fruits while avoiding obstacles like iron balls. Participants were randomized using sealed envelopes, with blinding of participants and outcome assessors. The outcomes were assessed through demographic questionnaires and cognitive assessments before and after the intervention. The study aimed to evaluate the effectiveness of VR serious games treatments as a complementary intervention for cognitive improvement in schizophrenia patients.
In VR-SCIT [
20], a game about office stories, players completed activities to enhance emotion recognition, by judging what kind of emotion was being presented to them, to avoid jumping to conclusions, by trying to understand the context of a situation, and to practice social strategies, by practicing the learned skills in real-life scenarios. Participants were randomly assigned to one of three groups: VR group, standard treatment group, or waiting-list. Assessments included psychopathology, neuropsychological tests, social functioning, and social cognition measures. Statistical analyses were performed to assess group differences and intervention effects. The study aimed to explore the potential benefits of VR-SCIT for individuals with schizophrenia.
In these VR studies, participants can receive performance feedback and customizable challenges tailored to their specific needs, enhancing their skill development throughout the process [
3,
4,
18]. Moreover, certain games offer the option for players to review their performance and scores at the end of each session, enabling them to track their progress [
21].
When comparing VR serious games to CBT, VR brings reliable, risk-free, and accessible medical data, simulating workplace dynamics and enhancing knowledge retention. However, it requires patients to obtain computer skills. CBT treatments offer globally recognized strategies but may lack on-site applicability and patient involvement. The choice depends on context, with VR targeting a wider demographic and cognitive treatments emphasizing doctor-patient relationships [
12].
Overall, the use of VR technology in these studies offers a promising avenue for schizophrenia patients to improve their social functioning and clinical outcomes. These VR games create a safe and immersive environment that allows individuals to practice and enhance their social and functional skills, ultimately leading to a better quality of life for those living with schizophrenia.
Within a previous research investigation, we studied interventions tailored for patients with negative symptoms of schizophrenia, which underlined the potential of VR games. This study was centered on the identification of crucial game features, ranging from interaction modality to immersion and adaptation. Our in-depth review pointed out the remarkable capacity of VR systems when employed in conjunction with conventional therapy approaches, demonstrating their ability to generate sustained, enduring results while simultaneously keeping patients engaged and motivated [
22].
3. Material and Methods
This study constituted a singular, non-randomized controlled trial aimed at evaluating the usability, effectiveness, and safety of developing a VR game therapy for the management of negative symptoms associated with schizophrenia.
3.1. Sample
In this initial phase of trials, a group of twenty-one healthy individuals participated. In order to be eligible, participants needed to meet specific inclusion criteria, which were as follows:
Age between 18 and 60 years.
Completion of at least middle school education.
Absence of any prior medical history related to schizophrenia or other relevant mental disorders.
Capacity to provide written informed consent.
This trial was not intended for the target audience, which would be schizophrenic patients since it would require prior safety testing and approval. So, the participants were volunteers with backgrounds in fields such as healthcare, computer science, and design.
As shown in
Table 1, most of the participants were male (6 females and 15 males), with an average age of 27.2 years and an average of 15.7 years of education, indicating that, on average, they had completed at least a bachelor’s degree. Among the participants, ten had at least completed High School (education level 3), eight held a bachelor’s degree (education level 6), one held a master’s degree (education level 7) and two held a PhD degree (education level). The education level was organized according to the International Standard Classification of Education (ISCED) [
23]. Of the twenty-one participants, only two were employed in the healthcare sector, while the rest primarily had backgrounds in the field of informatics.
Regarding their relevant experience, most participants reported a high level of computer proficiency (n = 18), indicating daily usage for advanced tasks. In terms of experience with VR, the sample displayed a more diverse range of experiences. Approximately half of the participants had never used immersive VR, while the other half had some level of experience, either having used it fewer than five times or more frequently.
3.2. Hardware and Software Required
The device chosen to perform this study was the Meta Quest 2 (
www.meta.com, accessed on 14 October 2022), a standalone VR headset.
Table 2 presents its main specifications of hardware.
Being a standalone device, the Quest 2 stands out for its portability, allowing users more freedom to play anywhere and without the need to invest in additional expensive hardware like a desktop computer. The lack of cables is also an advantage, preventing users from tripping over them while playing. However, this brings disadvantages such as, the dependency on a battery that lasts up to 3 h and graphics resolutions restrained by the system components.
Moving on to more specific details, Quest 2 offers 3 measures to set up the Interpupillary Distances (IPD), which allows users to adjust the device to better fit their size. In terms of display, the horizontal field of view of Quest 2 has only 89°. Despite the smaller field of view, the device boasts a high display resolution, contributing to a clearer and more immersive visual experience.
As for the input, it tracks the position of the Head Mounted Display (HMD) with the position of the controllers and the input of each button on the controllers. Quest 2 also allows users to use their hands as controllers, although not all games have that feature implemented.
The headset’s integrated Operative System (OS) is based on Android, so any kind of software meant to be used in the headset needs to be developed specifically for it. The Unity game engine (
www.unity.com, accessed on 14 October 2022) allows developers to create games and build them directly on the Android system.
3.3. Predefined Game Features
These kinds of games offer several advantages in treating schizophrenia. Notably, they allow patients to repetitively engage in a safer, controlled environment, facilitating skill training with constant feedback and motivating challenges. The immersive nature of these games, depicting real-life scenarios and providing well-defined objectives, promotes patient motivation and engagement. This, in turn, encourages more frequent training sessions, aiding in the recovery of autonomy.
Game features were defined in collaboration with a healthcare unit considering related works, the systematic literature review [
22], considering the development tools available and the needs of the target audience. The following game features were identified as relevant to be present on the prototype:
Immersivity: When moving from regular therapy to VR, therapy can take advantage of how immersive it can become. The more immersed the patients feel, the more they will feel that the situation is real. And, since CBT is based on the use of scenarios to train skills to be used in real situations, if patients are completely immersed in the scenario, therapy can be more effective.
Realism: Games often simplify how we perform interactions with objects. However, when playing with the goal of improving skills to be used in real life such simplification can be a disadvantage, since in this case interactions should be as close to real ones as much as possible so that players learn the desired abilities the correct way. Objectives should remain easily comprehensible, aiming to avoid player frustration in completing goals. However, the manner in which players achieve these objectives should align more closely with real-world methods rather than relying on the conventional button-press mechanics commonly found in most games.
Portability: The easier it is to set up a device and play a game at various locations the more portable the device will be. For instance, a standalone device is more portable than a pc-powered device since it does not require the use of cables to connect to a desk computer. Consequently, it is important to add portability to VR game therapies as it will fasten the distribution of this kind of treatments.
Tutorial: Patients need tutorials to understand the rules and mechanics of the game. They provide detailed instructions on subjects like how to move around or interact with objects. Without them, patients might find it frustrating to learn to play the game, which can lead to a negative gaming experience, especially when considering that patients never interacted with the system before and probably many of them never interacted with VR headsets before.
Feedback: The importance of feedback lies in the ability to help patients improve their performance. It can be given as visual or auditory cues and gives information on choices and how they affect the game’s progress. Without feedback, patients may feel lost, since it is a way of knowing what they are doing right and what they need to improve.
Therefore, these features play a crucial role in ensuring that patients have an effective, enjoyable, and engaging experience while playing the game therapy.
3.4. System Structure
Figure 1 describes the structure behind the developed system. The two players who will be interacting with the system are the main player, the patient who will be directly playing the game, and the therapist, who will be watching the gameplay and assisting the patient in whatever they need. The main player will be interacting with the game through the controllers and watching it through the VR headset. Meanwhile, the headset will be casting the gameplay through a closed channel that can be watched on the therapist’s computer. Thus, there are two User Interfaces (UI), one in an immersive environment and displayed in the VR headset and other displayed in a usual display screen. Also, since the headset is a standalone it will be running directly the game developed with Unity (version 2020.3.33f1) and built for the headset’s OS.
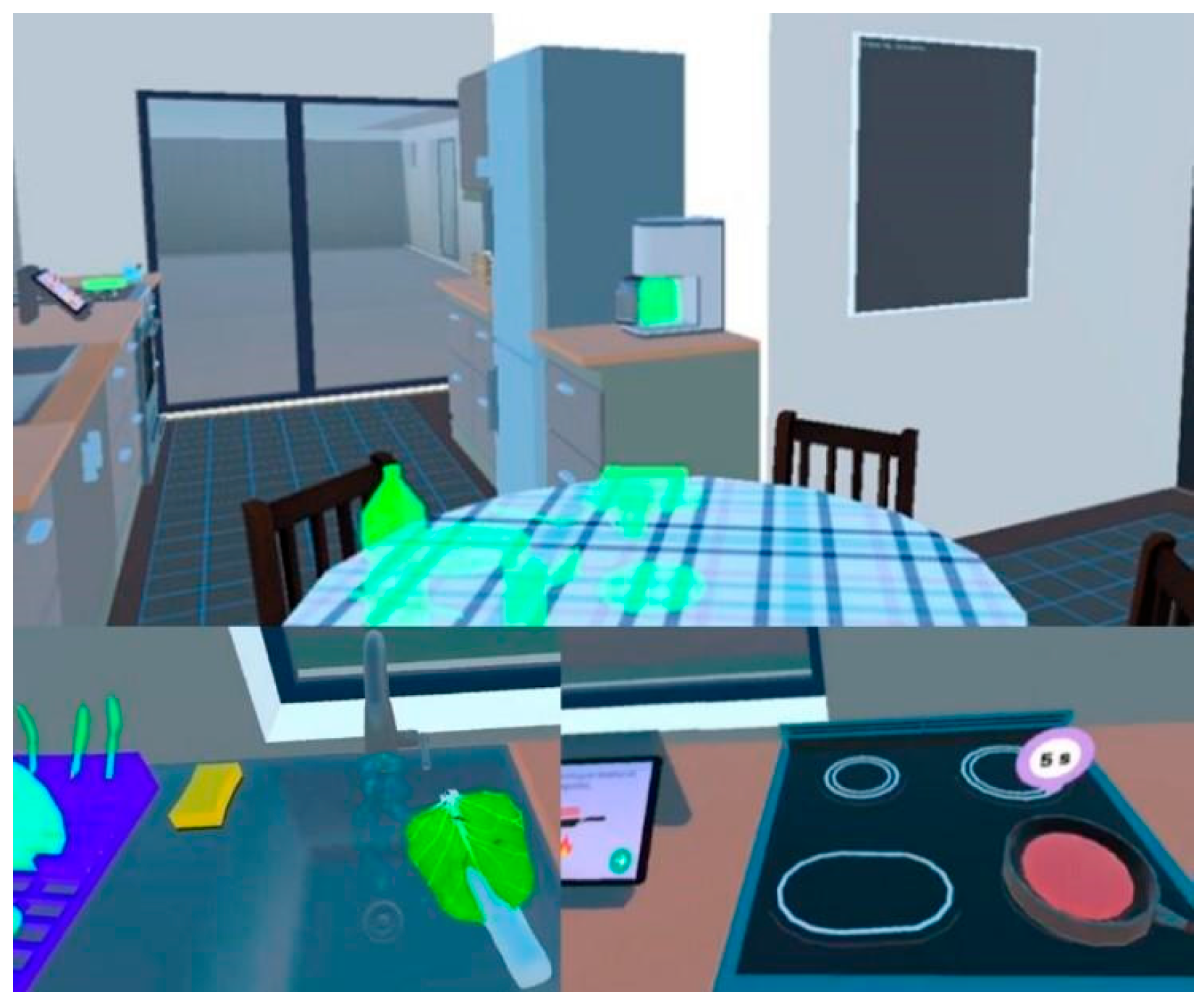
3.5. Game Description
The game developed emphasizes the training of cognitive and behavioral skills by using immersive virtual reality technology. Like conventional non-VR treatments, this approach centers on simulating and repeating daily life activities. Patients must role-play a scenario that involves completing tasks related to activities such as cooking or cleaning. The scenario chosen for the prototype was a kitchen, as it is a location where everyone spends a considerable amount of time every day. Additionally, it offers versatility, as it facilitates the completion of a wide range of tasks. It recreates real-life scenarios, offering a safe and controlled space for patients to train their skills.
It was designed to assist individuals with schizophrenia in regaining their independence. More specifically it was designed to treat the symptom of avolition, since it makes individuals struggle to initiate simple behaviors to carry out the tasks they want or need to perform. The concepts within the game are intentionally simplified, providing enough information for players to recognize daily life interactions while making the experience engaging. For instance, to make coffee only requires putting a mug under the coffee machine and turning it on by clicking on a button, leaving implied that in real life it requires more steps like adding water, adding coffee capsules and cleaning the machine.
Players begin with an in-game tutorial that introduces them to the game’s basic mechanics. This tutorial helps patients grasp how to interact with the virtual environment and perform actions like picking up objects, opening drawers, and operating appliances.
Following the completion of the tutorial, players move to the kitchen area, where they have the option to select a level to play.
Figure 2 displays the kitchen scene together with examples of gameplay. Each level is represented by a meal, either breakfast or lunch. Once the level is chosen, players are presented with a series of sequential steps to cook and serve the selected dish. These steps are presented on a board, and players are instructed to follow them in the specified order. When a step is executed correctly, it is automatically marked as correct on the board, accompanied by a positive sound reinforcing the belief that the step was completed correctly. These steps are intentionally designed to be realistic and progressively more challenging, allowing patients to gradually enhance their skills and boost their confidence, while still being manageable for individuals with schizophrenia. The level of difficulty for each step was assessed by:
If the step requires the player to find an object, how easily can it be found;
- ◯
Example: Objects displayed on the counter can be found more easily than the ones hidden inside the cabinets;
The presence of explicit sub-steps within a step description;
- ◯
Example: If it tells the player to pick up one object and then place it on the correspondent place;
The presence of implicit sub-steps within a step description;
- ◯
Example: If it tells the player to cook a certain food, the player needs to find out how to properly use the stove and cook it;
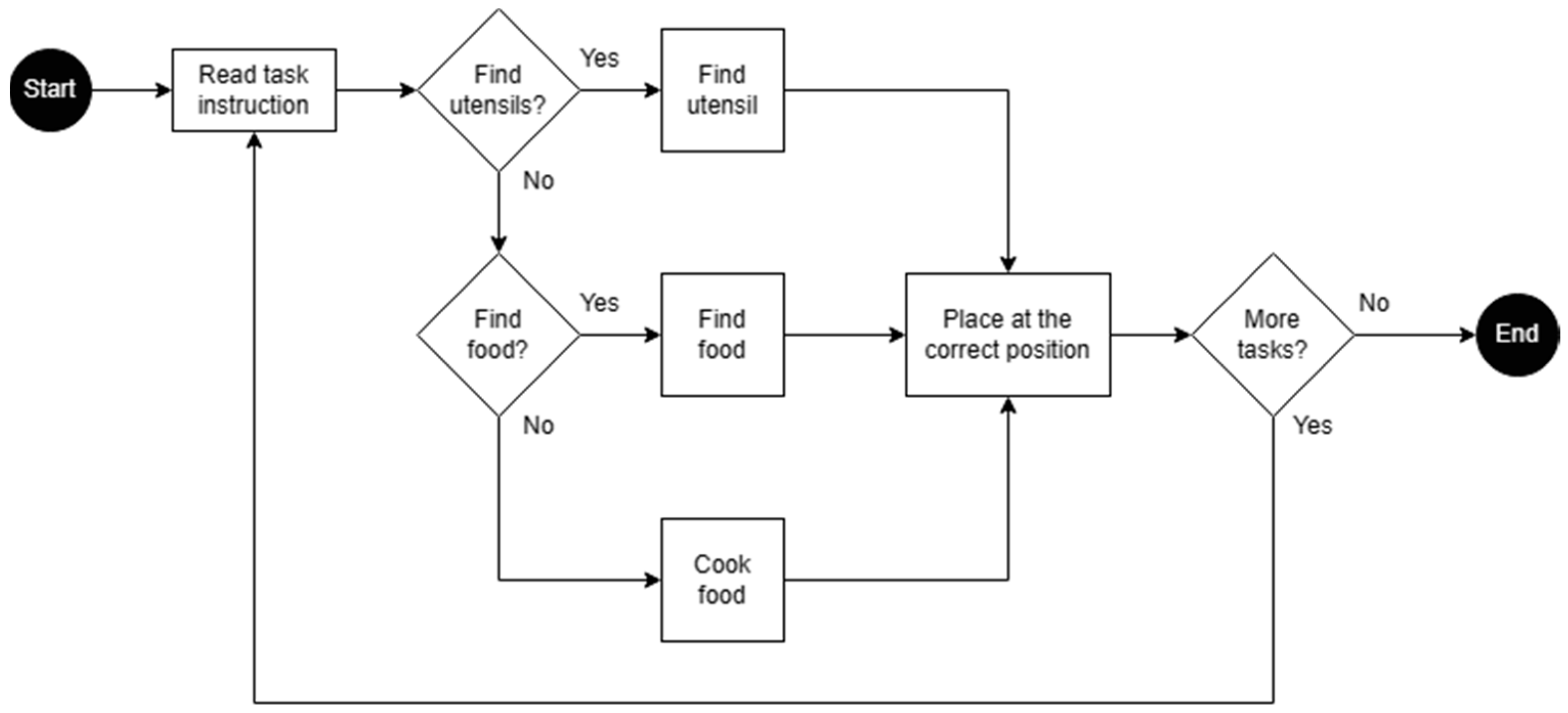
The game interactions follow the logic shown in
Figure 3. Each level begins in the kitchen, where players read a list of tasks that they must complete to complete the level. Tasks fall into three types: finding a specific utensil, finding a specific food item, or cooking a designated dish. To complete a task, players either find an object or figure out the cooking process of a food, and then place it in a predefined place. After each task is completed, they check the list again to read the next one. The level is over once every task is completed.
Overall, the game offers players a feeling of fulfillment as they advance through the different steps and eventually complete the preparation of the requested meal. This sense of achievement can contribute to an increase in confidence and motivation, which are crucial elements in CBT treatments.
3.6. Procedures
Each trial session followed a consistent structure, starting with an introductory briefing on the research, the game and the testing procedures, followed by obtaining written informed consent from participants.
Then, the researcher instructed them on the game controls and helped them put on the HMD. While they were playing, the researcher observed, recorded their performance and guided them through the tutorial. Once they felt ready, they proceeded to play the two game levels, breakfast and lunch, in that order.
Upon completing the game, participants filled out a survey concerning their overall user experience (UX). Finally, if a participant’s occupation was connected to the healthcare field, such as being a doctor, they were also interviewed on their professional perspective regarding the game and its potential applicability in real treatment sessions.
3.7. Instrumentation
3.7.1. Immersive VR Game Therapy
To evaluate the game’s usability, participants were observed while completing two distinct tasks, denoted as Task A and Task B. These tasks correspond to the levels, breakfast and lunch respectively, which involved the preparation of two meals, one of relatively low difficulty and the other more challenging. The difficulty of each task was assessed based on the number of steps involved and the complexity of each step.
The objectives of these tasks were: firstly, to determine if players could comprehend and execute the game’s instructions; secondly, to assess if participants demonstrated skill improvement; and finally, to observe how participants responded to varying levels of difficulty. Throughout the completion of both tasks, the researcher meticulously documented various aspects including:
Task Effectiveness: quantified as the percentage of task completion. It measures how effectively the tasks are performed and shows whether the desired outcomes were achieved.
Completion time: the time from start to end of a level. It indicates how long it takes to complete the task.
Errors: the number of unsuccessful attempts at in-game actions. It shows every single wrong action made by the participant.
Mistakes: instances where participants struggled to comprehend game instructions. It is a more specific type of error and shows game flaws.
Assists: refer to the level of support or help needed to complete the tasks. Shows the frequency of requests for help to complete a step.
3.7.2. Survey
Furthermore, in order to assess the system’s usability, participants were required to complete a survey that was structured into four distinct sections:
Personal Information: The initial section collected demographic information, including gender, age, educational background and occupation.
UX: Within this section, participants responded to ten specific questions that delved into different aspects of the game, seeking their feedback on elements such as immersion level and difficulty.
Satisfaction: Using the System Usability Scale (SUS) [
24], this portion measured the subjects’ overall satisfaction with the system. The SUS score ranges from 0 to 100, with scores above 71 indicating acceptability and scores exceeding 85 considered excellent.
Suggestions: An optional open-ended question was provided, allowing participants to express their personal opinions about the game and share suggestions for potential improvements.
3.7.3. Interview
To assess the game’s effectiveness and safety from a medical point of view, interviews were conducted exclusively with the two participants working in healthcare professions. While they did not specialize in schizophrenia symptomatology, both had previous experience with schizophrenia patients.
The interviews involved discussions and questions aimed at obtaining their medical perspective on the game, particularly regarding its advantages, level of challenge, safety, and automation. These individuals were interviewed on the following topics:
Their overall opinion about the system.
The system’s impact on cognitive treatments.
The system’s level of complexity.
The presence of any potential risks.
The necessity for therapist support.
4. Results
4.1. Tests
During the tests, Task effectiveness was measured by assessing the participants’ ability to navigate and complete designated challenges within the VR environment. The importance of evaluating task effectiveness lies in its direct correlation with the game’s capacity to engage users in therapeutic activities and facilitate meaningful experiences. As our results approach 100%, indicating near-perfect task effectiveness, it signifies the game’s remarkable proficiency in achieving its intended objectives.
Most participants demonstrated their ability to complete both Tasks successfully within a reasonable time frame, as the average completion time for both Tasks was below 10 min. Errors, which were automatically recorded by the game, occurred more frequently than mistakes, with common issues including difficulties in locating the correct objects, failed attempts at guessing the next step, and understanding how to complete certain steps. Despite these challenges, only four participants failed to complete both Tasks successfully, and their reasons for failure varied, ranging from exceeding the 20-min time limit, giving up during Task B, to encountering a bug in the game that prevented them from moving forward.
It is worth noting that the low mean number of assists in Task A and B indicated that the game effectively guided players, reducing their reliance on therapist assistance. However, the data showed that only 8 participants completed Task A without any assistance, and merely 2 of them completed both tasks independently, highlighting that some level of guidance was often required.
The study also revealed that while participants generally found the tasks easy to complete, their performance declined in Task B, suggesting that it presented a greater challenge as intended. Despite potential challenges such as bugs, stress, and time constraints, the overall test results were positive, emphasizing the effectiveness of the game in helping participants complete the tasks and improve their problem-solving skills.
The findings from the study, as presented in
Table 3 below, illustrate the participants’ performance during the tasks.
Although the results provided valuable insights into evaluating participant performance, it’s crucial to highlight that there was no continuous assessment of performance throughout the game execution by the participants. This was due to the limited timeframe of the testing session, which lasted only one day. The evaluation predominantly centered on assessing performance in terms of task execution.
4.2. Survey
In terms of the participants’ performance, a quick learning curve was observed, where even the subjects with the least experience with games, and VR in specific, managed to complete each meal quite fast with little to no assistance. Furthermore, the tutorial together with the researcher’s explanation worked well on teaching them the basics of the game. In fact, using the VR controllers was the skill that caused the most trouble to learn, probably because of a lack of experience in console gaming. Overall, participants found the game engaging, enjoyable, and easy to use.
4.2.1. UX Results
Question 1 and Question 3 yielded unanimous responses, with a unanimous 100% agreement among all participants. This unanimous consensus highlights that all study participants found the game’s movement system to be user-friendly and intuitive. Moreover, it shows that all game objects, despite their design being minimalist, were easily recognizable by participants. This shared perspective underscores the effectiveness of the game’s design in making interaction and object identification a seamless and intuitive experience for all users.
The level of graphic realism in the game was analyzed with respect to its influence on the perceived level of immersion among the subjects, considering their previous experience with VR, based on the survey responses displayed in
Figure 4. Initially, it was anticipated that graphic realism would not affect the level of immersion. However, the responses from the participants were not uniform, yielding a varied range of opinions. While six participants believed that the level of graphic realism had no impact on immersion, nine others disagreed and thought it did. Six additional participants remained neutral, suggesting that they perceived these aspects as independent of each other.
Furthermore, Task B, which was intentionally designed to present a greater challenge than Task A, was agreed upon by most participants (n = 13) as being more challenging. Interestingly, a minority (n = 4) expressed an opposing viewpoint, suggesting that as they improved their skills in the game, Task B appeared less difficult. Nevertheless, an examination of the data in
Table 3, revealed that the difficulty level did not diminish. It did not diminish since task effectiveness decreased and all the other variables increased, which would not happen if the level of difficulty had maintained or even decreased. For instance, the mean number of errors committed by participants in Task B compared to Task A was almost five times higher, going from 2.2 to 9.8. This observation implies that, despite the participants’ increasing familiarity with the game, they encountered increased difficulties as they advanced.
4.2.2. SUS Results
The SUS evaluation scored 88.7 out of 100, which is considered an excellent grade and shows that the system has very good usability. Systems rated this high are considered to have a user-friendly design, are efficient, require fewer support and training needs and present lower error rates.
Regarding the survey responses, as seen in
Figure 5, they exhibited a high degree of uniformity, showing a consensus among participants regarding their views on the game. For instance, questions 3, 7, and 8 demonstrated unanimity with 100% of the choices falling into either the “agree” or “disagree” category. The responses further indicated that the system was perceived as user-friendly and seamlessly integrated. Ultimately, the results aligned with the expectations, affirming that participants’ levels of agreement and disagreement on the survey were consistent.
Additionally, the game left a good impression on the participants. A total of 20 participants reported feeling confident during gameplay, while 17 found the game engaging and suitable for regular play.
Despite the good results, there was one individual who said the system was overly complex. This observation underscores the importance of further development in this area.
4.3. Interview
Discussions with the healthcare professionals about the system conveyed a positive consensus of their opinions. They found the system to be engaging and challenging, with a manageable learning curve. They believed the system could have a positive impact on CBT treatments and significantly improve the daily lives of patients, indicating a promising therapeutic potential.
Regarding the system’s level of complexity, they agreed that, in general, there were no overly complex components. Yet, while there was an initial struggle related to understanding the game controls, this difficulty lessened over time. This suggests that the system was well-designed and approachable, particularly for patients undergoing cognitive treatments.
However, the professionals did express concerns about potential safety risks associated with the system. As seen from the data presented in
Table 4, in response to question 3. One participant highlighted a potential danger related to the game’s portrayal of interacting with hot food without using kitchen utensils. They were concerned that this aspect of the system might influence patients to mimic such behavior in real life, potentially leading to serious consequences. This underscores the importance of addressing safety issues within the system.
In terms of the necessity for therapist support, they agreed that therapist support was not always necessary. They found that, except for the initial stages when patients were learning to play the game, the system was self-sufficient. This suggests that the system could be used as a therapeutic tool with reduced dependence on continuous professional oversight, making it more accessible for patients undergoing cognitive treatments.
4.4. Analysis of Our System and Other Similar Systems
In relation to the sample, it’s important to note that while all other studies specifically examined patients diagnosed with schizophrenia, our study took a different approach. Although our research did not exclusively focus on individuals with schizophrenia, it successfully incorporated a broader range of participants, including healthcare professionals. So, our study achieved a slightly larger sample size (n = 21). Studies [
13,
18] stand out for having a bigger sample size of over 90 participants.
Regarding the duration of the study trials, it is important to note that our study falls short in comparison to others. While some studies conducted from 6 [
3] to 16 [
4] sessions over several weeks, our investigation was limited to only one session.
Regarding immersion and interaction, [
9,
18] stand out as the only studies not using a HMD, therefore not being immersive. Our system together with [
3], stand out for using two HMD controllers, providing a more realistic interaction with the game than the keyboard and mouse used in [
9,
18]. Additionally, facial [
4], voice [
4,
13], and motion [
13] recognition were explored in two studies for alternative forms of interaction.
As for realism, all studies have chosen a more realistic approach in terms of scenarios and tried to achieve a realistic form of interaction with the combination of controllers, to interact with the game using virtual hands, and body recognition, to interact with the game through body movements. To compare the studies in terms of realism, an evaluation was made on how realistic their approach was. Three levels of realism (low, medium, and high) were given based on factors such as immersiveness, in-game movement, interaction with objects or people, and game goals.
In terms of portability, we selected the Meta Quest 2 for our study due to its exceptional ease of transportation, allowing the convenient administration of the treatment in a home setting. It is noteworthy that, aside from our research, only one other study [
3] acknowledged the importance of treatment portability. [
20] also used a standalone device, the Pico Goblin2 All-In-One, which opens up better opportunities for treatment portability, yet did not acknowledge that possibility.
Regarding tutorials, our investigation revealed that, apart from our own work, only one study [
18] has implemented a tutorial, a key feature in the learning process for any game.
And, finally, in all studies except [
4,
19,
20], feedback was successfully integrated, underscoring the effort to integrate mechanisms within the game that can enhance the player’s experience and performance.
Table 5 provides a comprehensive overview of the analysis conducted on our system, offering a comparative perspective with those discussed in our state-of-the-art. Studies that did not provide information on a feature were marked with “--”.
5. Discussion
This study showed that VR can be used as a more modern approach to CBT treatments for mental health conditions, like schizophrenia. The immersive aspect of VR inherently makes treatments more engaging, thus increasing its attendance rate. Controllers and the HMD provide a more realistic interaction with the games, allowing patients to participate in immersive roleplay in a more natural and intuitive way. Since the target of the treatment was negative symptoms, which affect the daily life of patients with schizophrenia, using role-plays that portray a day-to-day situation, such as daily kitchen activities, seems to be the best approach, especially when targeting avolition. The use of standalone devices, like the Meta Quest 2, offers a chance for promoting treatment portability, since it provides the opportunity to increase treatment distribution and decrease its costs, increasing its availability to patients. In addition, the only type of performance issue displayed by the device was with the control tracking when the room had too much sunlight coming in. The use of other features such as the tutorial, helps players to get used to the game mechanics more quickly. The addition of feedback, by showing players their correct and incorrect actions, not only helps them to improve their skills, but it also supports the idea of treatment portability, by making patients less dependent on the therapist’s assistance.
Our sample consisted mostly of males (15 males and 6 females), raising concerns about gender imbalance bias. The two major concerns include sampling bias and generalizability issues. Firstly, our sample’s gender ratio does not reflect the global distribution among people diagnosed with schizophrenia. Also, drawing generalized conclusions from a non-representative sample may yield misleading results. Nonetheless, we believe that educational background and familiarity with technology are more likely to have a greater influence on results than gender. And, since our current sample doesn’t accurately represent individuals with schizophrenia, we can only make assumptions to improve our system and plan to conduct future tests with actual schizophrenia patients for a more accurate assessment.
The findings indicate that most of the implemented game features were agreed to be intuitive and user-friendly by all participants. However, perceptions varied regarding the impact of graphic realism on immersion. And in regard to system difficulty, Task B was generally recognized as more challenging, although some participants believed it became easier as they improved their skills, a notion contradicted by the data which revealed increased errors. These results underscore the effective design of the game while highlighting the complex interplay between graphic realism, task difficulty, and user experience in the context of the study.
Also, participants displayed enjoyment while playing, finding it easy to play and understanding the game tasks quickly, which can be considered a positive outcome. These assumptions were then validated by the survey’s responses where participants agreed that the system was engaging, easy to use, and well-integrated. Such results support the goals of this study to understand how to develop more effective systems to assist in the treatment of negative symptoms of schizophrenia.
However, there were indications for future improvements, such as the level of complexity of the system, level of difficulty and level of realism. Perhaps the learning curve for complexity and difficulty should increase more slowly to keep up with the players’ skills. In regard to the level of realism, it seems to mostly depend on the players’ preference, but further research is needed to understand the target audience preferences.
The interview analysis suggests that the developed serious game has the potential to be effective in the treatment of schizophrenia. It does not seem overly difficult for patients, considering that they might have more difficulty adapting to games than the healthier subjects tested. And the need for a therapist to guide patients throughout the game might not always be necessary. However, it also indicates that certain modifications are needed to ensure patient safety while playing the game.
On the down side, unlike the other selected studies, our sample was not composed of patients with a lived experience of psychosis, and our number of trial sessions was lower. Yet, our study was able to incorporate all the predefined game features, including immersiveness, realism, portability, tutorials, and feedback. While immersiveness, realism, and feedback were the most explored features by other studies, our emphasis on portability and tutorials distinguishes our research from others in the field. Also, most analyzed studies had in-game activities and goals based on training social interactions with other individuals, while our approach did not follow the social training strategy. Instead, we place a strong emphasis on realistic interactions and comprehension of sequences of activities. Everyday household routines, encompassing tasks like meal preparation and organization of objects, serve as the inspiration for our approach.
There is one major limitation in this study that can be addressed in future research, the sample. The sample, which ideally would be composed only of medical experts and patients with schizophrenia, affected the reliability of the resulting data. However, using real patients for testing was beyond the scope of this preliminary study. Also, due to the study’s relatively brief duration, we could only complete one stage of implementation and testing. This limitation hinders our capacity to extrapolate long-term effects and refine the developed solution.
6. Conclusions
In conclusion, modern technologies are becoming increasingly present in our lives at distinct levels, either for pure entertainment or something as serious as management of resources. When applied to the health sector, it can also be beneficial. In particular, the treatment of schizophrenia can benefit from it, by updating existing treatment techniques, automating its process, and decreasing its distribution costs. Challenges in VR interventions for schizophrenia include the lack of standardization, limited accessibility due to cost, difficulty with acceptance and adherence, and a lack of consensus on outcome measures. Our innovative approach focused on identifying key features for VR game therapies, such as immersiveness, realism, portability, tutorials and feedback, features we believe should be the standard in this kind of system. We have studied how standalone VR devices, in particular Meta Quest 2, can be used to lower treatment cost and increase portability. Also, we have tested those features by developing a VR game focused on daily household activities, using realistic interactions for better skill building, something we have not yet seen in this field. Hopefully, this study will contribute to fastening the process of testing, creation and adaptation of existing treatments to this type of system.
Finally, this study still leaves space for future improvements on the prototype and its validity. For instance, the addition of more levels in different rooms with a more substantial variety of tasks, user customization of the house or interface, social interactions with virtual avatars and the storage of data on a remote database. Furthermore, it would be of immense value to validate the developed game by testing it with patients diagnosed with schizophrenia and more medical professionals. Such tests would provide a more insightful understanding of which features work the best and which ones still need improvement. Yet, the study was aimed at the evaluation of the game’s usability, with plans for a subsequent phase dedicated to conducting the study with patients.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}