Simple Summary
Ultrasound elastography is increasingly applied in thoracic imaging, but its clinical role remains unclear. This systematic review of 30 studies found that most research focused on transthoracic applications, particularly shear wave elastography for distinguishing malignant from benign pleural effusions or subpleural lesions, and surface wave elastography for assessing interstitial lung disease. However, substantial variation in methods, ultrasound techniques, and diagnostic thresholds restricts comparison across studies. Overall, elastography shows potential value in thoracic disease evaluation and procedural guidance, but standardized protocols and larger validation studies are needed before widespread clinical adoption.
Abstract
Introduction: Ultrasound elastography is increasingly used across medical imaging, yet its role in thoracic disease remains poorly defined. While both transthoracic ultrasonography (TUS) and endobronchial ultrasound (EBUS) offer real-time assessment of pleural and pulmonary structures, the diagnostic and clinical value of elastography in this context remains uncertain. Materials and Method: A systematic search of MEDLINE, EMBASE, and the Cochrane Library was conducted according to PRISMA guidelines (April 2023; updated January 2025). Original studies evaluating transthoracic or endobronchial elastography for pleural or pulmonary conditions were included. Data extraction and quality assessment were performed independently by three reviewers, with QUADAS-2 used to evaluate risk of bias. Results: Thirty studies met inclusion criteria. Twenty-eight evaluated TUS elastography and two examined EBUS. Shear wave elastography was most frequently applied, particularly for differentiating malignant from benign pleural effusion or subpleural lesions. Surface wave elastography demonstrated consistently higher stiffness values in patients with interstitial lung disease compared with healthy controls, correlating with radiological and functional disease severity. Elastography-guided pleural biopsy improved diagnostic yield compared with conventional ultrasound-guided biopsy. Overall, substantial methodological variation existed among scanning techniques, elastography modalities, reporting methods, and diagnostic thresholds, limiting cross-study comparison. Conclusions: Ultrasound elastography shows promise for evaluating pleural effusion and pulmonary lesions, procedural guidance, and interstitial lung disease possibly improving diagnostic possibilities with bedside evaluation and reducing patient exposure to radiation. However, methodological variation and limited high-quality evidence preclude clinical implementation. Standardized acquisition protocols and multicentre validation studies are necessary to define its diagnostic utility in thoracic imaging.
1. Introduction
Ultrasound is a well-established modality for investigating thoracic diseases. Thoracic ultrasound (TUS) can be performed at bedside, is non-invasive, and reduces patient exposure to ionizing radiation and, in some cases, contrast agents [1]. Several features can guide the diagnostic and therapeutic approach toward conditions such as pneumothorax, pleural effusion, parietal pleural abnormalities, and lung parenchymal pathology [2,3,4]. While several findings such as the pleural line, pleural effusion, B-lines, and consolidations are of clinical value, additional information when performing ultrasound examination on underlying disease could prove useful to risk stratification and diagnostic guidance [5,6]. Endobronchial ultrasound (EBUS) has transformed modern bronchoscopic practice, offering a relatively safe and minimally invasive modality for evaluating a wide range of intrathoracic diseases. This technology has expanded diagnostic and therapeutic options, particularly in the management of intrathoracic lymphadenopathy and pulmonary lesions [7]. While these modalities offer utility in detecting pleural and parenchymal abnormalities, they lack the ability to differentiate between different underlying pathologies giving rise to the same ultrasonographic presentation.
Elastography is based on the principle of tissue elasticity, and a tissue deformation by an external force can be measured. Depending on the modality in use, the deformation can be expressed as either longitudinal or shear waves [8,9,10]. Application is either determined as strain or shear wave measurements, but studies have also explored the use of surface wave elastography, especially in terms of assessing interstitial lung disease (ILD) [11,12].
A comprehensive guideline and recommendation for the use of elastography on several organs has been published by the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) [13,14]. The validation of elastography’s applicability to assess certain organs, e.g., liver fibrosis, focal breast lesion, and lymph node, is well established, but no current recommendations are available to direct the assessment of thoracic diseases. A recent systematic review by Vargas et al. in 2024 reviewed the current evidence regarding pleural effusion, pulmonary lesions, and ILD, which indicated a promising sign of implementation of ultrasound elastography in pleuropulmonary evaluation; however, studies lack standardization [15]. Although comprehensive, the review only identified 613 papers for screening and did not cover endobronchial elastography. Furthermore, as a novel ultrasonographic modality in respiratory medicine, new data on the evaluation of thoracic conditions are frequently published.
As such, a systematic review is warranted, and the aim of this study was to conduct a systematic literature search on transthoracic and endobronchial elastography and provide an overview of the current literature along with its capabilities to assess pulmonary and pleural conditions.
2. Materials and Methods
Prior to the literature search and data extraction, the project was registered at The International Database of Prospectively Registered Systematic Review of Health Related Outcomes (PROSPERO) (ID CRD42023420222). The work of this systematic review was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) to ensure appropriate reporting (Supplementary Table S1).
2.1. Eligibility Criteria
The following eligibility criteria were applied to ensure clinical relevance and methodological consistency.
- Inclusion criteria
- -
- Ultrasound elastography in all iterations, investigating thoracic conditions.
- Exclusion criteria
- -
- Animal studies;
- -
- Phantom studies;
- -
- Evaluation for lymph nodes, costal or intercostal structures;
- -
- Conference abstract or highlights report.
2.2. Search Strategy
The search strategy was developed in collaboration with a professional research librarian. The Patient-Intervention-Comparison-Outcome (PICO) outline was developed as shown:
- -
- Population: All humans who had their thorax assessed with any type of elastography.
- -
- Index test: Transthoracic or endoscopic ultrasound elastography.
- -
- Reference test: Diagnostic tests considered gold standards encompass, but were not limited to, pathology or cytology by transthoracic or endoscopic biopsy, microbiological studies or clinical follow-up elastography examination. For studies aiming at establishing reference values in healthy subjects, no reference standard was required.
- -
- Diagnosis of interest: Any pathology or description of physiological conditions of the thorax.
From this, the following search string was constructed:
- Block 1: Lung
- Lung [MeSH] OR Pulm* OR Lung* OR Pneu* OR Pleura [MeSH] OR Pleur*
- Block 2: Pulmonary embolism
- Elasticity Imaging Techniques [MeSH] OR Shearwav* OR Elastograph* OR Fibroscan*
A primary systematic search was conducted on the 21 April 2023 of MEDLINE, EMBASE, and Cochrane Library databases. Following systematic inclusion and exclusion of eligible articles, a second search was performed on the 15 January 2025 to ensure newly published relevant articles were included. No filters (e.g., date of publication or language) were applied. After removing duplicates, CK, RWN, and ADN independently evaluated articles based on title and abstract. Subsequent full text screening of articles deemed eligible by title and abstract was performed by CK and RWN. In case of disagreement, a third investigator, CF, decided if the article was eligible. A snowballing search of all included studies’ references were performed as a final search for eligible articles. Screening was performed in Covidence (Veritas Health Innovation Ltd., Melbourne, Australia). Included articles were managed with the use of EndNote 20 (Clarivate Analytics, Philadelphia, PA, USA).
2.3. Grouping of Included Studies
The included studies were categorized as transthoracic or endobronchial ultrasound elastography. Studies on thoracic ultrasound were further subcategorized into five groups:
- (A)
- Pleural effusion;
- (B)
- Pulmonary consolidations;
- (C)
- Interstitial lung disease;
- (D)
- Procedural guidance;
- (E)
- Other.
2.4. Risk of Bias and Quality Assessment
Assessment of quality and bias was performed on all included articles by CK and RWN using the Quality Assessment of Diagnostic Accuracy Studies-2 tool, QUADAS-2 [16].
3. Results
The systematic literature search generated a total of 3663 articles. Duplicates were identified in 389 instances, and 3193 articles were deemed irrelevant when screening title and abstract. This resulted in full text screening of 97 studies, of which 30 were eligible for inclusion. Of the 30 included articles, three were identified in the secondary search. Evaluation of the reference lists of included articles yielded no additional relevant articles. A summary of the search construction is available in Figure 1.
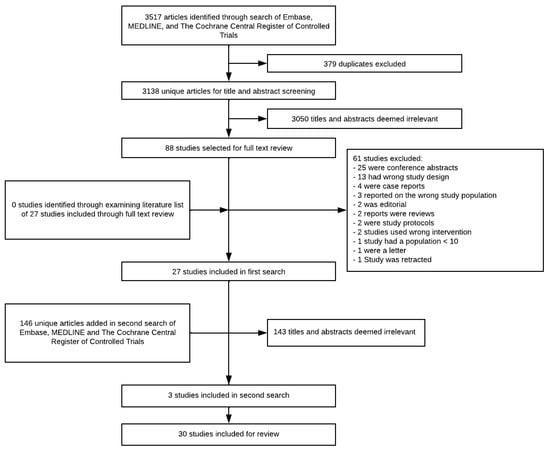
Figure 1.
PRISMA flowchart of search and exclusion of articles.
Of the 30 papers included, 28 reported on the use of TUS, while two investigated EBUS. Of the 28 papers investigating TUS elastography, eleven examined pulmonary lesions. Pulmonary effusion and ILD were investigated in four and seven papers, respectively.
3.1. TUS
- Pleural Effusion
Four papers investigated the utility of elastography in relation to pleural effusion from three different countries [17,18,19,20]. All studies applied Shear Wave Elastography (SWE). Two studies investigated the ability of SWE in differentiating malignant from benign effusions. The others assessed the ability of distinguishing transudative from exudative effusion or expandable from non-expandable lung (Table 1 and Table 2).

Table 1.
Studies regarding pleural effusion.
Table 2.
Results from studies regarding pleural effusion.
- B.
- Pulmonary Lesions
Eleven studies reported on pulmonary lesions assessed by TUS elastography [22,23,24,25,26,27,28,29,30,31,32]. These studies were published between 2013 and 2022 from five different countries. Six studies applied SWE as either two dimensional (2D-SWE) or point (pSWE) (Table 3). Eight studies investigated the ability to differentiate between malignant and benign subpleural lesions (Table 3 and Table 4). Additionally, pulmonary consolidation was also measured beneath pleural effusion by Petersen et al. and Nielsen et al. [19,20].
Table 3.
Studies regarding pulmonary lesions.
Table 4.
Results from studies regarding pulmonary lesions.
- C.
- Interstitial Lung Disease
Seven papers investigated the use of elastography in assessment of ILD (Table 5) [12,33,34,35,36,37,38]. All articles except one are case-control studies, describing utility of surface wave elastography. The majority of compared elastography findings to high-resolution computed tomography (HRCT), pulmonary function test (PFT), and clinical assessment.
Table 5.
Studies regarding interstitial lung disease.
Across the reviewed studies, ultrasound elastography consistently demonstrated higher stiffness values in patients with ILD compared with healthy controls. All studies using surface wave elastography at 100–200 Hz reported significantly elevated wave velocities in ILD. The modality utilizes measurements at the pleural line movements induced by external shaker and recorded with B-mode. Zhang et al. confirmed significant differences across six lung zones (p < 0.0001) [34,35,36,37]. Clay et al. reported that surface wave elastography velocities correlated with radiological fibrosis severity (Area Under the Curve [AUC] = 0.94), while Zhou et al. identified an optimal diagnostic cut-off of 5.47 m/s at 200 Hz, yielding 92% sensitivity and 89% specificity [12,37]. In an independent study, Huang et al. reported higher pleural line stiffness in Connective Tissue Disease (CTD)–associated ILD using 2D-SWE [38].
- D.
- Procedural Guidance
One study by Deng et al. investigated the use of elastography as procedural guidance for biopsy. A randomized controlled trial with 1:1 allocation was performed, and a total of 228 patients were included in the analysis. Patient were randomized to either thoracic ultrasound-guided or elastography-guided pleural biopsy. A cut-off value for target biopsy was set at a minimum of 47.25 kPa, indicating malignant pleural thickening. A significant greater sensitivity (80.49% vs. 50.00%, p = 0.007), and diagnostic yield (87.83% vs. 76.99%, p = 0.032) was observed with elastography-guided biopsy (Table 6).
Table 6.
Study regarding procedural guidance.
- E.
- Other
Five papers reported on conditions not encompassed by Sections A–D, exploring the elastographic value in the examination of chronic obstructive pulmonary disease (COPD), pneumothorax, and pulmonary edema (Table 7). Half of these articles (3/6) examined strain elastography (SE), while SWE and surface wave elastography were investigated in two papers each.
Table 7.
Studies regarding COPD, pulmonary edema, pneumothorax, and healthy aerated lung tissue.
Nouvenne et al. demonstrated in a feasibility study that SE values were higher in COPD than healthy smokers. Furthermore, examination of posterior basal zones demonstrated a valuable site for distinguishing between healthy non-smokers and COPD/smokers (AUC = 0.846, 95% confidence interval [CI] 0.73–0.93, p < 0.001) [42]. In patients undergoing general anesthesia, Girard et al. demonstrated a correlation between ventilation and pleural strain measured by SE and SWE. An excellent intraobserver agreement was observed, although interobserver agreement was moderate to good [40]. Among 30 patients suspected of pneumothorax, Bandelli et al. could confirm the lung point using SE in all patients, indicating the feasibility of clinical integration [41]. One healthy subject was investigated by Zhang et al. in a feasibility study of surface wave elastography, demonstrating the feasibility of surface wave elastography and that increased surface wave speeds measured corresponded to the amplified frequency of external mechanical vibration [44]. The basic principles of surface wave elastography are further examined in papers of ILD patients (Section C). Finally, Wiley et al. demonstrated on 14 patients a significant decrease in surface wave speed from admission to 1–2 days after diuretic therapy [43].
3.2. EBUS
- B.
- Pulmonary lesions
Two papers reported the use of elastography on pulmonary lesions during endobronchial investigation (Table 8) [29,30]. Diagnostic performance was moderate to good, with histopathological outcome as the diagnostic reference. Using a 4-point scoring system, He et al. demonstrated that malignant lesions exhibited a significantly higher score compared to non-malignant lesions. With an AUC of 0.793, an optimal cut-off point was set to be 2.5, with a sensitivity and specificity of 72.2% and 76.2%, respectively. The elastography grading score was superior compared to all other ultrasound modalities [29]. Zhi et al. performed elastography during EBUS and categorized it according to a 1–5 scale, with a dichotomous outcome of 1–3 classified as benign, while 4–5 was considered malignant. A cut-off of 6.5 was found optimal to ensure an AUC of 0.692, with a corresponding sensitivity and specificity of 83.5% and 52.6%, respectively. The intra- and interobserver agreement was found to be 0.951 and 0.886, respectively [30].
Table 8.
Studies regarding endobronchial elastography.
3.3. Risk of Bias and Quality Assessment
The overall risk of bias in studies included in this systematic review was deemed high, with unclear perspectives reported and the majority of thresholds not reported in advance (Supplementary Figure S1). Assessment of applicability was at a moderate-to-high level, but concerns regarding patient flow and patient selection were observed (Supplementary Figure S2).
4. Discussion
Based on the current evidence identified as part of this review, elastography seems to harbor potential in regard to examining pulmonary conditions. However, contemporary evidence does not allow definite assessment of the clinical utility and optimal implementation of this modality.
4.1. Clinical Implication
In the case of pleural effusion, SWE consistently demonstrated the capability to quantify biomechanical differences relevant to differentiating effusion etiologies. Studies attempting differentiation between malignant and benign effusions, as well as transudative versus exudative fluid, reported discriminative stiffness values that support potential clinical integration [17,18,19]. In cases in which thoracentesis or diagnostic tap is not possible, elastography could possibly provide additional clinical information to assess possible malignancy. Similarly, elastography-based assessment of an expandable versus non-expandable lung showed feasibility [20]. However, despite encouraging findings, the variability in acquisition conditions, ranging from controlled inpatient settings to emergency care environments, limits the generalizability of reported diagnostic thresholds.
Elastographic characterization of subpleural pulmonary lesions constitutes the most extensively studied domain. Across studies, both SE and SWE demonstrated the ability to distinguish malignant from benign lesions with moderate-to-good diagnostic performance [22,23,24,25,26,27,28,29,30,31,32]. Based on current data, elastographic assessment would not be a stand-alone single diagnostic test to rule in/out pulmonary malignancy. On the contrary, elastographic measurements could prove valuable in collected imaging assessment and could improve diagnostic pathways. More recent transitions from SE toward quantitative SWE have improved reproducibility and may offer more stable cut-off values than earlier qualitative approaches [22,29,30]. Nevertheless, the heterogeneity in ultrasound transducer types, patient positioning, breath-hold requirements, and Region-of-Interest (ROI) definition complicates the interpretation of pooled diagnostic accuracy, as highlighted by Kuo et al. [22]. Despite these limitations, the consistency of higher stiffness values in malignant lesions across studies suggests a meaningful diagnostic signal.
Only two studies have been published that have assessed EBUS elastography. The methodologies across EBUS elastography were innovative but methodologically diverse [21,45]. Diagnostic performance was moderate to good, showing promising steps. A difference in scoring model was observed between the two studies, but a high intra- and interobserver agreement is suggestive that EBUS elastography may improve identification of malignant lesions [21]. As to subpleural lesions, EBUS elastography could serve as a complementary modality to further enhance diagnostic yield. The area is understudied compared to transthoracic evaluation as elastography technology is still evolving and not yet widely integrated into standard bronchoscopic platforms. Comparative trials against existing modalities, assessment of learning curves, and evaluation of clinical impact on biopsy decision-making and patient outcomes would further clarify its utility and accelerate transition toward broader clinical adoption.
Evidence for elastographic assessment of ILD is primarily derived from lung surface wave elastography [12,33,34,35,36,37]. These findings indicate that elastography may provide a non-invasive adjunct for detecting fibrotic lung changes and potentially monitoring disease progression, ultimately saving patients from radiation with repetitive HRCTs. Although several studies indicate a correlation between surface wave measurement and ILD, the elastographic protocol is relatively new, not recognized in other settings, and inflicts procedural difficulties and observer variation
One study, a randomized controlled trial, evaluated elastography for procedural guidance. In this study, elastography-guided pleural biopsy significantly improved sensitivity and diagnostic yield compared with conventional ultrasound, suggesting a possible improvement in the diagnostic procedure [39]. Implementation of elastography could possibly secure an optimal diagnostic pathway for patients and reduce possible re-biopsy procedures, including reduced procedure-related complications. Replication is needed before this technique can be recommended for routine clinical use. Furthermore, the evaluation of elastographic differences in subtype malignant diseases has not been evaluated, which could lead to misinterpretation of optimal biopsy site if subtypes prove to have diverse properties.
4.2. Methodological Concerns
From a methodological perspective, several components are not standardized in current evidence published. Across all study categories, methodological variability represents the major constraint limiting evidence synthesis and clinical extrapolation.
In general, published studies were of single-center setting, limiting the external generalizability, and of small sample size with no prior power estimate. The elastographic acquisition protocols included variation in breath-hold instructions, diverse patient positioning and scanning protocols, with a minority of papers describing the ROI placement. Several different modalities of elastography have been investigated, emphasizing the wide range of elastographic methods but without standardization and thus complicating cross-study comparison [12,17,18,20,24,25,26,32,34,44]. In the evaluation of diagnostic methods, knowledge of intra- and interobserver variation is important to guide possible clinical implementation. Although high agreement was observed regarding reproducibility for the most part in the studies assessed, observer variability is inconsistently reported [17,18,22,27]. Lastly, as expressed in the risk-of-bias assessment, the concerns regarding patient selection, unclear thresholds, and insufficient reporting all further limit drawing definitive conclusions and future large-scale, standardized studies.
A more standardized framework for future transthoracic elastography studies should include a uniform ROI definition within the stiffest homogeneous lesion area, with ROI size reported and scaled-to-lesion dimensions. Breath-hold instructions—preferably at end-expiration—should be applied to limit motion artifact, alongside consistent patient positioning, probe orientation, and machine settings. Quantitative outputs should use clearly defined metrics (e.g., mean vs. maximum values, kPa vs. m/s), and qualitative scoring systems should be predefined. The methodology should be altered according to modality and target disease evaluated.
4.3. Limitations
While this systematic review summarizes current evidence on transthoracic and endobronchial elastography, several review-related limitations should be acknowledged. Despite a broad search strategy, some relevant studies—especially unpublished work—may have been missed. Substantial heterogeneity in study design, elastography technique, and reported outcomes prevented meta-analysis and limited the review to a qualitative synthesis. Screening and data extraction were conducted by a small team, introducing potential selection or extraction bias despite adjudication. Moreover, the long inclusion period spans major developments in elastography technology, complicating comparisons across studies. Finally, exclusion of conference abstracts may have introduced publication bias and have broadened the evidence base by capturing early or unpublished data, potentially affecting effect estimates or revealing less favorable findings. However, the variable rigor and higher risk of bias typical of gray sources might also have reduced overall certainty, leading to more cautious conclusions.
5. Conclusions
Elastography in different types of modalities shows some promise in examining pulmonary conditions. However, the collective evidence is characterized by notable methodological variability, precluding meaningful syntheses of the results, as well as significant risk of bias across multiple domains. Consequently, no overall conclusions on the clinical utility of elastography can be drawn. Adequately designed studies with standardized protocols and cut-off values are warranted to assess reproducibility, diagnostic performance, and optimal scanning protocols.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/cancers18020190/s1. Figure S1: Assessment of risk of bias; Figure S2: Applicability of studies; Table S1: PRISMA checklist. Reference [46] is cited in the supplementary materials.
Author Contributions
Conceptualization, C.F., C.B.L., and C.K.; methodology, C.F.; software, C.K.; validation, C.K., C.F., R.W.N., and A.D.N.; formal analysis, C.K., R.W.N., and A.D.N.; investigation, C.K.; resources, C.K.; data curation, C.K., R.W.N., and A.D.N.; writing—original draft preparation, C.K.; writing—review and editing, C.K., C.F., C.B.L., R.W.N., A.D.N., A.D.J., D.A., and T.J.A.; visualization, C.K.; supervision, C.F. and C.B.L.; project administration, C.K.; funding acquisition, none. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
C.K.: no conflicts of interest. R.W.N.: no conflicts of interest. C.F.: has received honoraria from GE Healthcare for a presentation on thoracic ultrasound. A.N.D.: no conflicts of interest. A.D.J.: no conflicts of interest. D.A.: no conflicts of interest. T.J.A.: honoraria from GlaxoSmithKline and AstraZeneca. C.B.L.: payment for lectures at educational events/symposia/courses organized by AstraZeneca, Chiesi Pharma, GlaxoSmithKline, and Boehringer Ingelheim.
References
- Marini, T.J.; Rubens, D.J.; Zhao, Y.T.; Weis, J.; O’Connor, T.P.; Novak, W.H.; Kaproth-Joslin, K.A. Lung Ultrasound: The Essentials. Radiol. Cardiothorac. Imaging 2021, 3, e200564. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Laursen, C.B.; Clive, A.; Hallifax, R.; Pietersen, P.I.; Asciak, R.; Davidsen, J.R.; Bhatnagar, R.; Bedawi, E.O.; Jacobsen, N.; Coleman, C.; et al. European Respiratory Society statement on thoracic ultrasound. Eur. Respir. J. 2021, 57, 2001519. [Google Scholar] [CrossRef] [PubMed]
- Jarman, R.D.; McDermott, C.; Colclough, A.; Bøtker, M.; Knudsen, L.; Harris, T.; Albaroudi, B.; Albaroudi, O.; Haddad, M.; Darke, R.; et al. EFSUMB Clinical Practice Guidelines for Point-of-Care Ultrasound: Part One (Common Heart and Pulmonary Applications) LONG VERSION. Ultraschall Med. 2023, 44, e1–e24. [Google Scholar] [CrossRef]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.; Goldstein, I.; Mourgeon, E.; Cluzel, P.; Grenier, P.; Rouby, J.J. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 2004, 100, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Reissig, A.; Copetti, R. Lung ultrasound in community-acquired pneumonia and in interstitial lung diseases. Respiration 2014, 87, 179–189. [Google Scholar] [CrossRef]
- Vilmann, P.; Clementsen, P.F.; Colella, S.; Siemsen, M.; De Leyn, P.; Dumonceau, J.-M.; Herth, F.J.; Larghi, A.; Vazquez-Sequeiros, E.; Hassan, C.; et al. Combined endobronchial and oesophageal endosonography for the diagnosis and staging of lung cancer. Eur. Respir. J. 2015, 46, 40–60. [Google Scholar] [CrossRef]
- Akhtar, R.; Sherratt, M.J.; Cruickshank, J.K.; Derby, B. Characterizing the elastic properties of tissues. Mater. Today 2011, 14, 96–105. [Google Scholar] [CrossRef]
- Parker, K.J.; Taylor, L.S.; Gracewski, S.; Rubens, D.J. A unified view of imaging the elastic properties of tissue. J. Acoust. Soc. Am. 2005, 117, 2705–2712. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Bolondi, L.; Duck, F.; Evans, D.H.; Ewertsen, C.; Fraser, A.G.; Gilja, O.H.; Jenssen, C.; Merz, E.; Nolsoe, C.; et al. History of Ultrasound in Medicine from its birth to date (2022), on occasion of the 50 Years Anniversary of EFSUMB. A publication of the European Federation of Societies for Ultrasound In Medicine and Biology (EFSUMB), designed to record the historical development of medical ultrasound. Med. Ultrason. 2022, 24, 434–450. [Google Scholar] [CrossRef]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef]
- Clay, R.; Bartholmai, B.J.; Zhou, B.; Karwoski, R.; Peikert, T.; Osborn, T.; Rajagopalan, S.; Kalra, S.; Zhang, X. Assessment of Interstitial Lung Disease Using Lung Ultrasound Surface Wave Elastography: A Novel Technique With Clinicoradiologic Correlates. J. Thorac. Imaging 2019, 34, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.M.; D’Onofrio, M.; Drakonaki, E.E.; et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 1: Basic principles and technology. Ultraschall Med. 2013, 34, 169–184. [Google Scholar] [CrossRef]
- Cosgrove, D.; Piscaglia, F.; Bamber, J.; Bojunga, J.; Correas, J.M.; Gilja, O.A.; Klauser, A.S.; Sporea, I.; Calliada, F.; Cantisani, V.; et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 2: Clinical applications. Ultraschall Med. 2013, 34, 238–253. [Google Scholar] [PubMed]
- Vargas-Ursúa, F.; Ramos-Hernández, C.; Pazos-Area, L.A.; Fernández-Granda, I.; Rodríguez-Otero, I.; Gómez-Corredoira, E.; Pintos-Louro, M.; Fernández-Villar, A. Current evidence for lung ultrasound elastography in the field of pneumology: A systematic review. ERJ Open Res. 2024, 10, 00081–02024. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Li, X.L.; Yin, Y.; Zhang, Q.; Zang, T.; Song, W.S.; Wang, X.M.; Kang, J.; Herth, F.J.F.; Hou, G. Ultrasound elastography: A novel tool for the differential diagnosis of pleural effusion. Eur. Respir. J. 2019, 54, 1802018. [Google Scholar] [CrossRef]
- Ozgokce, M.; Durmaz, F.; Yavuz, A.; Üney, İ.; Yildiz, H.; Arslan, H.; Dundar, I.; Havan, N.; Ogul, H. Shear-Wave Elastography in the Characterization of Pleural Effusions. Ultrasound Q. 2019, 35, 164–168. [Google Scholar] [CrossRef]
- Nielsen, R.W.; Falster, C.; Posth, S.; Jacobsen, N.; Licht, A.E.; Bhatnagar, R.; Laursen, C.B. Diagnostic Accuracy of Shear Wave Elastography in Predicting Malignant Origins of Pleural Effusions in Emergency Departments. Diagnostics 2025, 15, 225. [Google Scholar] [CrossRef]
- Petersen, J.K.; Fjaellegaard, K.; Rasmussen, D.B.; Alstrup, G.; Høegholm, A.; Sidhu, J.S.; Sivapalan, P.; Gerke, O.; Bhatnagar, R.; Clementsen, P.F.; et al. Ultrasound in the Diagnosis of Non-Expandable Lung: A Prospective Observational Study of M-Mode, B-Mode, and 2D-Shear Wave Elastography. Diagnostics 2024, 14, 204. [Google Scholar] [CrossRef]
- Zhi, X.; Wang, L.; Chen, J.; Zheng, X.; Li, Y.; Sun, J. Scoring model of convex probe endobronchial ultrasound multimodal imaging in differentiating benign and malignant lung lesions. J. Thorac. Dis. 2020, 12, 7645–7655. [Google Scholar] [CrossRef]
- Kuo, Y.W.; Chen, Y.L.; Wu, H.D.; Chien, Y.C.; Huang, C.K.; Wang, H.C. Application of transthoracic shear-wave ultrasound elastography in lung lesions. Eur. Respir. J. 2021, 57, 2002347. [Google Scholar] [CrossRef]
- Quarato, C.M.I.; Venuti, M.; Dimitri, L.; Lacedonia, D.; Simeone, A.; Mirijello, A.; De Cosmo, S.; Maiello, E.; Taurchini, M.; Scioscia, G.; et al. Transthoracic ultrasound shear wave elastography for the study of subpleural lung lesions. Ultrasonography 2022, 41, 93–105. [Google Scholar] [CrossRef]
- Alhyari, A.; Görg, C.; Dietrich, C.F.; Trenker, C.; Ludwig, M.; Safai Zadeh, E. Diagnostic Performance of Point Shear Wave Elastography Using Acoustic Radiation Force Impulse Technology in Peripheral Pulmonary Consolidations: A Feasibility Study. Ultrasound Med. Biol. 2022, 48, 778–785. [Google Scholar] [CrossRef]
- Adamietz, B.R.; Fasching, P.A.; Jud, S.; Schulz-Wendtland, R.; Anders, K.; Uder, M.; Wüst, W.; Rauh, C.; Meier-Meitinger, M. Ultrasound elastography of pulmonary lesions—A feasibility study. Ultraschall Med. 2014, 35, 33–37. [Google Scholar] [CrossRef]
- Boccatonda, A.; Susca, V.; Primomo, G.L.; Cocco, G.; Cinalli, S.; Di Resta, V.; Martino, L.; Mucilli, F.; Marinari, S.; Cipollone, F.; et al. Role of shear-wave and strain elastography to differentiate malignant vs benign subpleural lung lesions. Medicine 2021, 100, e24123. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Shen, M.; Zhang, Y.; Cong, Y.; Zu, H.; Chen, H.; Wang, Y. A Model for Predicting Malignant Sub-pleural Solid Masses Using Grayscale Ultrasound and Ultrasound Elastography. Ultrasound Med. Biol. 2021, 47, 1212–1218. [Google Scholar] [CrossRef]
- Lewen, H.; Aiyun, Z.; Cheng, Z.; Fan, X.; Minwei, L. Real-time shear wave elastography in differential diagnosis of benign and malignant peripheral lung masses. Chin. J. Med. Imaging Technol. 2019, 35, 687. [Google Scholar]
- Lim, C.K.; Chung, C.L.; Lin, Y.T.; Chang, C.H.; Lai, Y.C.; Wang, H.C.; Yu, C.J. Transthoracic Ultrasound Elastography in Pulmonary Lesions and Diseases. Ultrasound Med. Biol. 2017, 43, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Sperandeo, M.; Trovato, F.M.; Dimitri, L.; Catalano, D.; Simeone, A.; Martines, G.F.; Piscitelli, A.P.; Trovato, G.M. Lung transthoracic ultrasound elastography imaging and guided biopsies of subpleural cancer: A preliminary report. Acta Radiol. 2015, 56, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Lu, Y.; Ji, Q.; Zhou, H.; Zhou, X. The application of conventional us and transthoracic ultrasound elastography in evaluating peripheral pulmonary lesions. Exp. Ther. Med. 2018, 16, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Ozgokce, M.; Yavuz, A.; Akbudak, I.; Durmaz, F.; Uney, I.; Aydin, Y.; Yildiz, H.; Batur, A.; Arslan, H.; Dundar, I. Usability of Transthoracic Shear Wave Elastography in Differentiation of Subpleural Solid Masses. Ultrasound Q. 2018, 34, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Osborn, T.; Zhou, B.; Meixner, D.; Kinnick, R.R.; Bartholmai, B.; Greenleaf, J.F.; Kalra, S. Lung Ultrasound Surface Wave Elastography: A Pilot Clinical Study. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2017, 64, 1298–1304. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, B.; Bartholmai, B.; Kalra, S.; Osborn, T. A quantitative method for measuring the changes of lung surface wave speed for assessing disease progression of interstitial lung disease. Ultrasound Med. Biol. 2019, 45, 741–748. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, B.; Kalra, S.; Bartholmai, B.; Greenleaf, J.; Osborn, T. An Ultrasound Surface Wave Technique for Assessing Skin and Lung Diseases. Ultrasound Med. Biol. 2018, 44, 321–331. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, B.; Osborn, T.; Bartholmai, B.; Kalra, S. Lung Ultrasound Surface Wave Elastography for Assessing Interstitial Lung Disease. IEEE Trans. Biomed. Eng. 2019, 66, 1346–1352. [Google Scholar] [CrossRef]
- Zhou, B.; Bartholmai, B.J.; Kalra, S.; Osborn, T.G.; Zhang, X. Lung US Surface Wave Elastography in Interstitial Lung Disease Staging. Radiology 2019, 291, 479–484. [Google Scholar] [CrossRef]
- Huang, S.; Guo, R.; Yuan, X.; Tang, X.; Liu, T.; Xie, Q.; Qiu, L. Evaluation of connective tissue disease-related interstitial lung disease using ultrasound elastography: A preliminary study. Quant. Imaging Med. Surg. 2022, 12, 3778–3791. [Google Scholar] [CrossRef]
- Deng, M.; Xia, Y.; Ye, X.; Ma, J.; Zhao, S.; Zhang, Q.; Li, J.; Lin, J.; Jing, A.; Li, Z.Y.; et al. Ultrasonic Elastography-guided Pleural Biopsy versus Traditional Thoracic Ultrasound-guided Pleural Biopsy for the Diagnosis of Pleural Effusion: A Multicentre Randomized Trial. Eur. Respir. J. 2025, 66, 2501062. [Google Scholar] [CrossRef] [PubMed]
- Girard, M.; Roy Cardinal, M.-H.; Chassé, M.; Garneau, S.; Cavayas, Y.A.; Cloutier, G.; Denault, A.Y. Regional pleural strain measurements during mechanical ventilation using ultrasound elastography: A randomized, crossover, proof of concept physiologic study. Front. Med. 2022, 9, 935482. [Google Scholar] [CrossRef]
- Bandelli, G.P.; Levi, G.; Quadri, F.; Marchetti, G.P. “Elasto-lung point”: A new tool for the sonographic confirmation of pneumothorax. Clin. Respir. J. 2020, 14, 758–762. [Google Scholar] [CrossRef]
- Nouvenne, A.; Zanichelli, I.; Cerundolo, N.; Milanese, G.; Sverzellati, N.; Rendo, M.; Ridolo, E.; Scarlata, S.; Meschi, T.; Ticinesi, A. Thoracic Ultrasound Strain Elastosonography as a Noninvasive Biomarker of Chronic Obstructive Pulmonary Disease-Associated Lung Injury: A Feasibility Study. Respiration 2022, 101, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Wiley, B.M.; Zhou, B.; Pandompatam, G.; Zhou, J.; Kucuk, H.O.; Zhang, X. Lung Ultrasound Surface Wave Elastography for Assessing Patients With Pulmonary Edema. IEEE Trans. Biomed. Eng. 2021, 68, 3417–3423. [Google Scholar] [CrossRef]
- Zhang, X.; Qiang, B.; Hubmayr, R.D.; Urban, M.W.; Kinnick, R.; Greenleaf, J.F. Noninvasive ultrasound image guided surface wave method for measuring the wave speed and estimating the elasticity of lungs: A feasibility study. Ultrasonics 2011, 51, 289–295. [Google Scholar] [CrossRef] [PubMed]
- He, H.Y.; Chen, J.L.; Ma, H.; Zhu, J.; Wu, D.D.; Lv, X.D. Value of Endobronchial Ultrasound Elastography in Diagnosis of Central Lung Lesions. Med. Sci. Monit. 2017, 23, 3269–3275. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.