Simple Summary
Sinonasal intestinal-type adenocarcinoma (ITAC) is an epithelial cancer of the nasal cavity and the paranasal sinuses, often related to work-related exposure. Because this cancer is asymptomatic, most patients with ITAC present with extensive tumors invading the surrounding tissue. In this study, genes encoding pluripotency-associated transcription factors, including KLF4, c-MYC, SOX2, OCT4, and NANOG (Yamanaka factors), were evaluated in malignant and non-malignant tissues of a cohort of 54 patients with ITAC, and their expressions were related to patient outcome. Our results show that a stemness phenotype with low expressions of KFL4, c-MYC, and NANOG and with high levels of SOX2 and OCT4 are predictors of a worse prognosis of ITAC. In multivariate analysis, c-MYC and OCT4 and the type of surgery were found to be predictors of the clinical outcome. To confirm the stemness role in ITAC, ALDH1A1 expression was also evaluated. Tumor positivity to c-MYC and ALDH1A1 was associated with longer disease-specific survival, suggesting their potential role in ITAC prediction.
Abstract
Background/Objectives: Sinonasal intestinal-type adenocarcinoma (ITAC) is a rare and aggressive tumor with a lack of specific symptoms, which leads to late diagnosis, and is characterized by frequent local recurrence and low survival rate. The stemness phenotype is one of the main causes leading to tumor proliferation, recurrence, and resistance to standard chemo/radiotherapy. Methods: In this study, genes encoding pluripotency-associated transcription factors, including KLF4, c-MYC, SOX2, OCT4 (Yamanaka factors), and NANOG were evaluated in malignant and non-malignant tissues of a cohort of 54 patients with ITAC, and their expression was related to patient outcome. The c-MYC, SOX2, and OCT4 levels were then confirmed in immunohistochemistry by adding ALDH1A1 as a factor involved in stemness. Results: KLF4, SOX2, and NANOG best distinguished cancer tissue from normal tissue with high sensibility and specificity. Low levels of KLF4, c-MYC, and NANOG and high expressions of SOX2 and OCT4 in tumor tissue correlated with poor overall survival (OS) and disease-free survival (DFS), respectively. Through multivariate analysis, type of surgery was found to be a significant prognostic factor along with c-MYC and OCT4. Notably, tumor positivity for c-MYC and ALDH1A1 was associated with longer disease-specific survival, thus suggesting their role as tumor suppressors. Conclusions: Our findings underline the stemness phenotype as a prognostic model for ITAC, supporting the clinical plausibility of Yamanaka factors in sinonasal cancer prediction.
1. Introduction
Sinonasal intestinal-type adenocarcinoma (ITAC) is a rare neoplasm with overall incidence of <1% of all neoplasms, accounting for <4% of malignancies in the sinonasal area [1,2,3]. This neoplasm occurs mainly in the nasal cavity, ethmoid sinuses, and maxillary sinuses and is strongly associated with occupational exposure to wood and leather dust [4,5]. ITAC, which mimics adenoma and adenocarcinoma from the intestinal mucosa, can be divided into four histological subtypes, papillary, colonic, solid and mucinous, and mixed histology can also occur [5,6]. Due to the lack of symptoms in the early stages, this tumor is commonly detected when invading surrounding tissues. Surgical resection with endonasal endoscopic approach represents the standard-of-care treatment [7]. However, the anatomical aspects often make it difficult to delineate clear surgical margins; therefore, post-operative radiation is commonly administered considering the high recurrence rate of this tumor type; and advanced-stage tumors are also treated with neoadjuvant chemotherapy [8]. Typically, the behavior of ITAC is often characterized by relapses, recurrence, and resistance after surgical and radiation therapies. Local recurrence occurs in up to 50% of the cancer cases with intracranial invasion being the most common cause of death [9], and the 5-year overall survival rate ranges from 40 to 70% [10].
Several studies reported on the most important prognostic factors in patients with ITAC in terms of their histopathological grading, referring to the pT classification [11,12,13,14,15]. However, although the clinical staging system was developed to predict the prognosis of the disease, it is mostly based on anatomical landmarks and does not consider characteristics that are related to its biology [16]. In fact, it is not clear why in some cases ITACs present with more aggressive behavior than other cases with the same histological features and clinical stage. The most likely explanation for different behaviors occurring among apparently similar ITAC cases is related to molecular features that play an important role in a patient’s final prognosis but are still not sufficiently clarified. We believe that uncovering these prognostic biomarkers will help in advancing treatment protocols in sinonasal malignancies.
In fact, although the quality of surgical resection remains the main prognostic factor for overall survival (OS) and disease-free survival (DFS), it will be very helpful to improve our knowledge about the specific biomarkers that are related to ITAC growth and invasive capacity which can help uncover new molecular targets for therapies. Although recent research revealed molecular factors involved in the pathogenesis of ITAC and proposed them as predictors of survival [17,18,19,20,21], there is still little known about biomarkers predicting the prognosis in sinonasal ITAC, and most of these factors need to be validated [22].
Recent evidence has highlighted the role of cancer stem cells (CSCs) as an important determinant of tumor growth. CSCs have been associated with tumor relapses, metastasis, and drug resistance after standard chemo/radiotherapy [23]. The biological activities of CSCs are regulated by several pluripotent transcription factors, known as the “Yamanaka factors”, which include KLF4, c-MYC, SOX2, OCT4, and NANOG [24]. Interestingly, CSCs account for only 0.01–2% of the total tumor mass. In addition, CSCs share features with normal stem cells, including important regulatory roles of transcription factors and signaling pathways. This makes isolation and identification of CSCs challenging [25].
To evaluate the stemness role in ITAC prognosis, we analyzed, for the first time, the expressions of the Yamanaka factors KLF4, c-MYC, SOX2, OCT4, and NANOG in a cohort of patients with ITAC and investigate their possible roles in influencing tumor properties and survival.
2. Materials and Methods
2.1. Patients and Tissue Specimens
A total of 54 patients with sinonasal ITAC who underwent surgery were recruited at the ENT Division of “Bellaria Hospital”, AUSL Bologna, Italy, between 2011 and 2017. Inclusion criteria were sinonasal ITAC, primary surgical treatment with complete excision of the tumor obtained by endonasal endoscopic resection (ER) or endonasal endoscopic resection with transnasal craniectomy (ERTC), complete clinical data, and a minimum of three years follow-up. Patients with previous or synchronous second malignancies, previous radiation therapy or chemotherapy, or who had died of post-operative complications were excluded from the study.
Each patient was characterized on demographic and clinical bases, including age, gender, occupational exposure, site of tumor, stage, grade, subtype, type of surgery, type of margins, adjuvant therapy, DFS, OS, and the follow-up period. The follow-up period lasted till May 2022 or until the patient’s death, with a median of 48 months and survival time ranging from 2.6 to 231 months. The sinonasal ITAC stages were determined in accordance with the American Joint Committee on Cancer TNM classification of malignant tumors [14]. According to the WHO classification [15], ITACs were classified into histological subtypes indicating well–moderate–poor differentiation, typical for the papillary, colonic, and solid subtypes. The mucinous type displays mucin-filled glands or cell clusters.
All patients had undergone complete clinical examination and were staged by multiplanar computer tomography (CT), contrast-enhanced magnetic resonance imaging (MRI) or contrast-enhanced CT whenever MRI was not possible, and positron emission tomography (PET)/CT in advanced-stage lesions. Tumor tissue and its adjacent non-malignant (NM) tissue were collected and stored at −80 °C.
All patients signed a written informed consent. The study was conducted according to the Helsinki Declaration, and the samples were processed after approval of the Ethical Committee of the Marche Regional Hospital, Ancona, Italy, Rec. no. 501 of 29 November 2011.
2.2. Quantitative RT-PCR
Total RNA was extracted from fresh-frozen tumor and non-malignant samples (30 mg) using the RNeasy Mini Kit (item no. 74004, Qiagen, Milan, Italy) according to the manufacturer’s instructions. The concentration and purity of RNA were determined by the Nanodrop 1000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA). RNA integrity was assessed by Qubit™ RNA IQ Assay Kits (Thermo Fisher Scientific, Waltham, MA, USA).
The KLF4, c-MYC, SOX2, OCT4, and NANOG first-strand cDNA were synthesized using a High-Capacity cDNA Reverse Transcription Kit (Life Technologies, Thermo Fisher Scientific, Waltham, MA, USA). The qRT-PCR was performed using the following primers: KLF4 (fw—CCC ACA CAG GTG AGA AAC CT; rw—ATG TGT AAG GCG AGG TGG TC); c-MYC (fw—ACT CTG AGG AGG AAC AAG AA; rw—GTC CAA CTT GAC CCT CTT GG); SOX2 (fw—AGC TAC AGC ATG ATG CAG GA; rw—GGT CAT GGA GTT GTA CTG CA); OCT4 (fw—AGC GAA CCA GTA TCG AGA AC; rw—GCC TCA AAA TCC TCT CGT TG); and NANOG (fw—TGA ACC TCA GCT ACA AAC AG; rw—CTG GAT GTT CTG GGT CTG GT). The genes were detected by RT-PCR using SYBR Select Master Mix (Life Technologies) in a Quant Studio 1 Real-Time PCR System (Applied Biosystem, Foster City, CA, USA). GAPDH was used as housekeeping gene (fw—TCC ACT GGC GTC TTC ACC; rw—GGC AGA GAT GAT GAC CCT TTT). Data were analyzed using the automatic cycle threshold (Ct) for the baseline and the threshold for the determination of the Ct. The samples were analyzed in duplicate, and samples with Ct values > 35 were excluded. The results were expressed as relative expression (2−ΔCt).
2.3. Immunohistochemical Analysis
Immunohistochemistry (IHC) and standard hematoxylin and eosin (H&E) staining were performed in formalin-fixed, paraffin-embedded (FFPE) tumor sections (2.5 µm). IHC was carried out by incubation with primary antibodies including anti-OCT4, anti-c-MYC IgGs, both from Dako (Camarillo, CA, USA), anti-SOX2, and anti-ADLH1A1 (Santa Cruz Biotechnology, Dallas, TX, USA). The sections were subsequently incubated with secondary antibodies (Dako, CA, USA) and visualized using the ultraView Universal DAB Detection kit (Dako, CA, USA). Nuclei were counterstained with hematoxylin. Images were acquired with an optical microscope (Zeiss, Axiocam MRc5 (Carl Zeiss Microscopy GmbH, Jena, Germany); magnification 400×). All sections and staining were assessed by an expert pathologist (GG).
2.4. Statistical Analysis
Results are expressed as mean ± standard deviation or as median and based on the interquartile range (IQR) and confidence interval (CI). The categorical variables were reported as fractions or percentages and compared with the chi-square method. Correlations among pluripotent factors and clinicopathological variables were performed by bivariate analysis according to the Sperman’s coefficient. Group comparisons were performed using the two-tailed Student’s t-test and analysis of variance (ANOVA), followed by post hoc Tukey analysis (more than two groups). Receiver operating characteristic (ROC) curve analysis was used to assess the diagnostic and prognostic sensitivity and specificity of pluripotent factors (KLF4, c-MYC, SOX2, OCT4, and NANOG), and the area under the ROC curve (AUC) was used as a diagnostic index and for prognostic accuracy. Survival analysis was applied to evaluate the cumulative probability of OS and DFS. OS was defined from the date of surgery to the time of death or to the last medical visit, while DFS was defined as the duration between the completion of treatment and the diagnosis of recurrence. According to the median value, each pluripotent factor was categorized in low (below median value) and high (above median value) expression groups. The cumulative incidence functions (CIF) of OS and DFS were estimated by the Kaplan–Meier method, and for each variable, the CIFs for different groups were compared using the log-rank test. The Cox proportional hazard model was performed in a univariate and multivariate analysis to assess the effect of prognostic factors (age, smoking, staging, histological subtype, and type of surgery) on OS and DFS. Insignificant prognostic factors were excluded from the model using backward elimination (Wald). The hazard ratios (HRs) with 95% confidence interval (CI) and p value were reported and visualized in the forest plots. The median follow-up was calculated according to the reverse Kaplan–Meier method. Probability values < 0.05 were considered significant. All statistical analyses were performed using the SPSS statistical package, version 25 (SPPS Inc., Chicago, IL, USA).
3. Results
3.1. Study Population
The enrolled population consisted of 54 ITAC patients, of which 93% were males, and the average age was 67 years (ranging from 33 to 92 years). Most patients were occupationally exposed to wood/leather (85%), and 44% were smokers. The tumors were in the ethmoid sinus; 3 tumors were classified as stage I, 16 as stage II, 23 as stage III, and 12 as stage IV. The ITAC included 18 papillary subtypes, 12 colonic subtypes, 15 mucinous subtypes, and 9 solid subtypes. Thirty-eight patients underwent ER and sixteen patients underwent ERTC. Intra-operative evaluation of the margins was performed, whenever possible, for radical resection. Adjuvant radiotherapy of the primary site with different techniques was delivered to 9 out of 54 patients. During the follow-up period, 22 patients (40%) developed a local relapse. The demographic and clinicopathological features are summarized in Table 1.

Table 1.
Demographic and clinicopathological characteristics of ITAC patients.
The study was conducted over a median (±SE) follow-up period of 42 ± 5 months [95% CI 32–52] and survival time ranging from 2.6 to 231 months. The 5-year OS was 65.3%, varying according to the histological subtype, with 80% for well-differentiated papillary subtype, 50% for the colonic subtype, 57% for the solid subtype, and 50% for the mucinous subtype.
3.2. KLF4, c-MYC, SOX2, OCT4, and NANOG Expression
Pluripotent factors were compared between tumor ITAC tissue and the adjacent non-malignant (NM) counterpart. KLF4, SOX2, and NANOG had low expressions in tumor tissue compared with its adjacent non-malignant (NM) counterpart, while no significant changes were found for c-MYC and OCT4 gene expressions (Figure 1). Receiver operating characteristic (ROC) curve analysis was performed to evaluate the ability of pluripotent factors to distinguish between ITAC and NM tissue. The area under the curve (AUC) of −0.719 [0.584–0.854] for KLF4, −0.875 [0.774–0.975] for SOX2, and −0.936 [0.871–0.997] for NANOG significantly differentiate ITAC tissues from non-tumorous tissues (Figure 2). Bivariate analysis revealed that SOX2 and OCT4 positively correlated with each other and negatively with KLF4, c-MYC, and NANOG. Only OCT4 correlated negatively with the tumor stage (Figure 3).
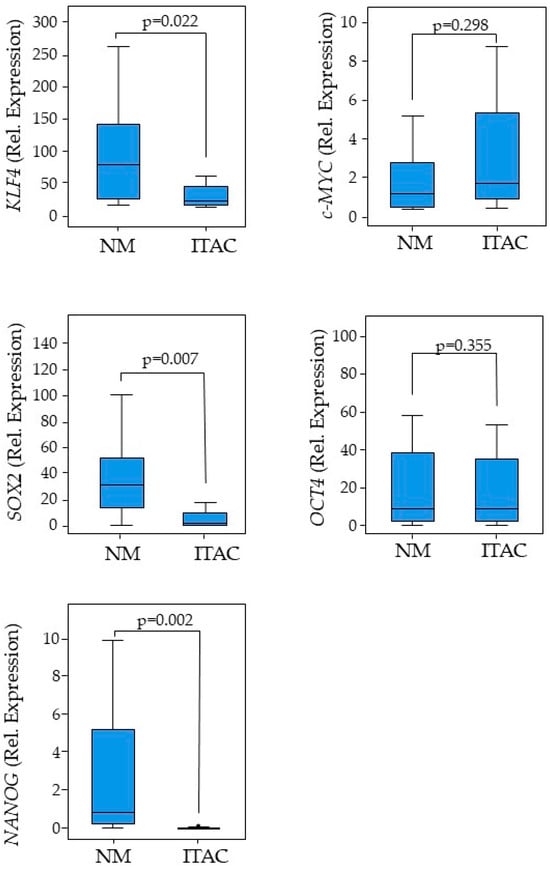
Figure 1.
Distribution of pluripotent factors. Expressions of KLF4, c-MYC, SOX2, OCT4, and NANOG in ITAC tissues and paired adjacent non-malignant (NM) tissues. Box-plots show the median and interquartile range. Comparisons between groups were determined by t-test analysis. Differences with p < 0.05 were considered statistically significant.
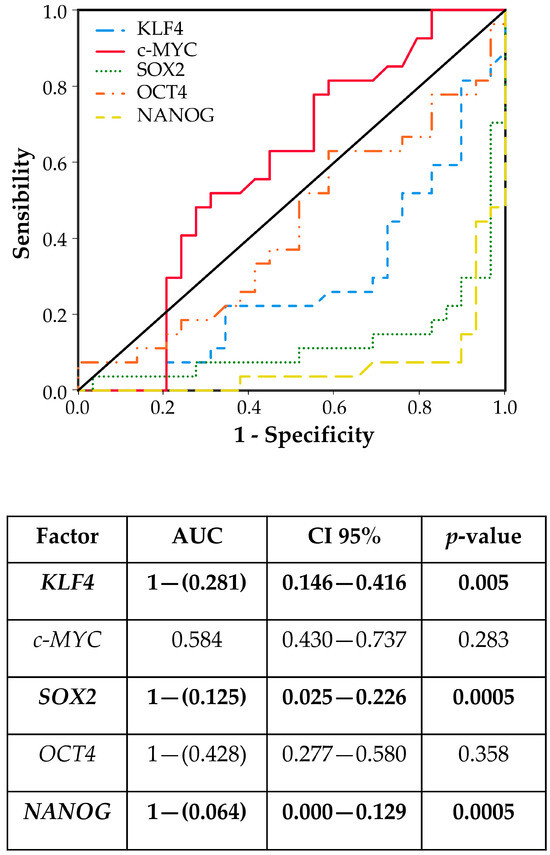
Figure 2.
The receiver operating characteristic (ROC) models and the area under curve (AUC) with confidence interval (CI) document the sensitivity and specificity in differentiating ITAC tissues from non-malignant mucosa tissues. Differences with p < 0.05 were considered statistically significant (marked in bold).
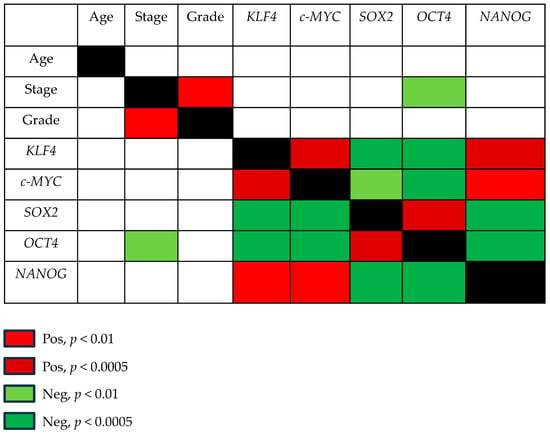
Figure 3.
Correlations among pluripotent factors and clinic-pathological parameters in ITAC. Correlations between KLF4, c-MYC, SOX2, OCT4, and NANOG with each other and with age, tumor stage, and grade were determined by Spearman’s test. p < 0.05 was considered significant. Significantly positive and negative correlations were highlighted in red and green, respectively.
3.3. Survival Analysis and Association with Clinicopathological Parameters
To evaluate whether gene expressions of pluripotent factors correlate with patient prognosis, patients were divided into high and low tumor gene expression level groups by the median value (below and above the median value). Kaplan–Meier curves for high and low expression groups identified a strong relationship between the expressions of KLF4, SOX2, OCT4, and NANOG and clinical prognosis. As shown in Figure 4, patients with high expressions of KLF4 and NANOG had significantly higher OS rates compared to those with low KLF4 and NANOG gene expressions (log-rank, p = 0.049 and p = 0.0005, respectively). Similarly, higher c-MYC also showed higher OS rates, but these differences did not reach statistical significance. Conversely, patients harboring higher expressions of SOX2 and OCT4 exhibited lower OS rates (log-rank, p = 0.004). A similar scenario was observed for DFS rates in univariate analysis.
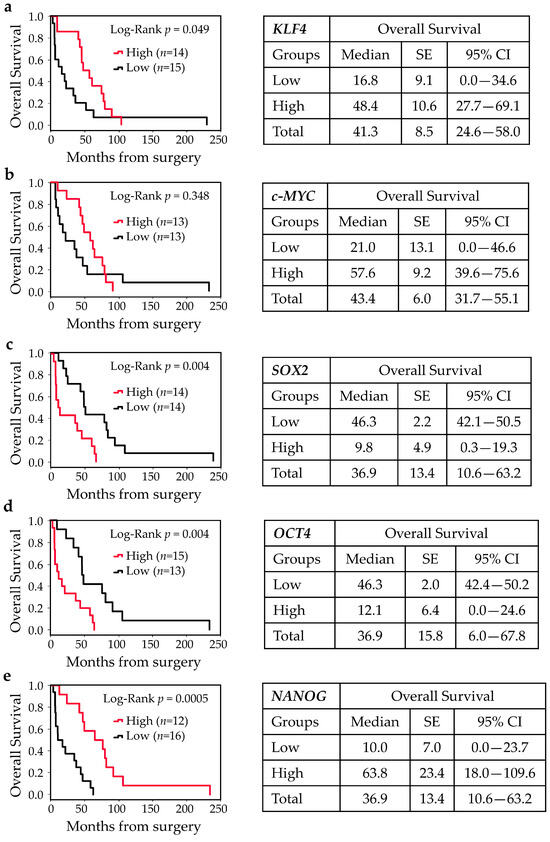
Figure 4.
Kaplan–Meier survival curves for ITAC stratified into two groups according to the median value for KLF4, c-MYC, SOX2, OCT4, and NANOG expressions. Low and high expressions of KLF4 (a), c-MYC (b), SOX2 (c), OCT4 (d), and NANOG (e) were associated with overall survival (OS). Comparisons between groups were made using log-rank test, and two-sided p < 0.05 was considered statistically significant. Median values, standard error (SE), and a 95% confidence interval (CI) [minimum–maximum] are summarized in the chart on the right.
Prognostic factors, including age, smoking, histological subtypes, tumor stage, and type of surgery, were evaluated by univariate analysis. Subsequently, significant predictors were included in multivariate analysis in association with pluripotent factors.
Histological subtypes and type of surgery were significant prognostic markers predictive of poor outcome in the univariate analyses. In the multivariate survival analysis, c-MYC and OCT4 levels in association with the type of surgery reached statistical significance (Table 2).
Table 2.
COX-regression analysis and forest plot for the subgroup analysis of the relationship between prognostic factors and OS or DFS.
Immunohistochemistry (IHC) staining of paraffin-embedded sections was performed next to confirm the relationship between c-MYC, SOX2, and OCT4 expressions and clinical–pathological parameters. To further address the stemness and CSC potential in ITAC, ALDH1A1 expression was also evaluated. No SOX2 positivity was found in ITAC tissue, while immunoreactivity was detected for OCT4 in 4 of 16 cases (25%) and for c-MYC in 8 of 16 cases (50%). c-MYC expression was considered low (negative or weak, n = 8) or high (moderate or strong, n = 8) for further statistical analysis. Survival analysis showed no statistically significant difference in OS and DFS between high and low c-MYC-score groups (p = 0.744). However, patients with high c-MYC expression had better OS compared with those with low c-MYC expression as shown in Figure 5.
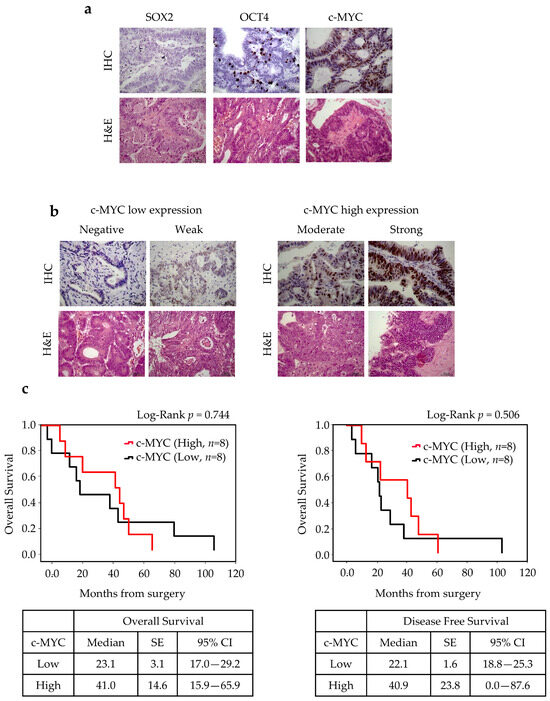
Figure 5.
SOX2, OCT4, c-MYC expressions in ITAC tissue and survival rates. (a) Immunohistochemical analysis of expressions of SOX2, OCT4, and c-MYC in primary ITAC specimens (magnification 400×). (b) c-MYC low and high expression groups. (c) The OS and DFS according to c-MYC expression using the Kaplan survival curve. Comparisons between groups were made using log-rank test, and two-sided p < 0.05 was considered statistically significant. Median values, standard error (SE), and a 95% confidence interval (CI) [minimum–maximum] are summarized in the chart on the right. Scale bar, 50 μm.
Tumor positivity to ALDH1A1 was found in 9 of 17 cases (52%), and its expression (cytoplasmatic or nuclear) was significantly associated with a favorable OS (p = 0.05) and DFS (p = 0.021) (Figure 6).
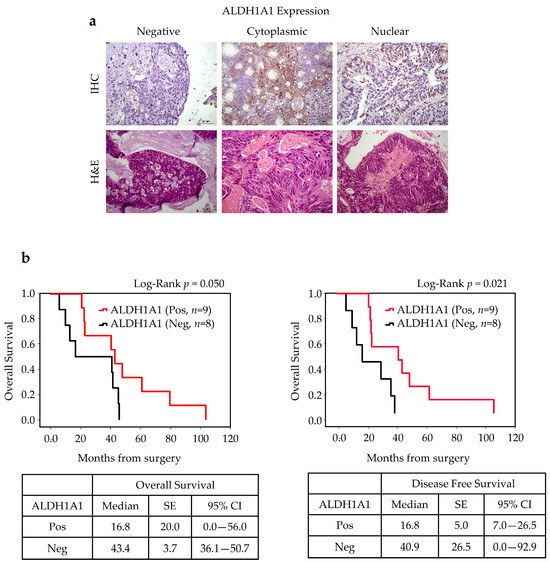
Figure 6.
ALDH1A1 expression in ITAC tissue and survival rates. (a) Immunohistochemical analysis of expression of ALDH1A1 in primary ITAC specimens (magnification 400×). (b) The OS and DFS according to ALDH1A1 positivity using the Kaplan survival curve. Comparisons between groups were made using log-rank test, and two-sided p < 0.05 was considered statistically significant. Median values, standard error (SE), and a 95% confidence interval (CI) [minimum–maximum] are summarized in the chart on the right. Scale bar, 50 μm.
4. Discussion
The results of the present study showed, for the first time, that the expressions of KLF4, SOX2, and NANOG are significantly downregulated in ITAC samples as compared with the adjacent non-pathological tissues (while no difference was found for c-MYC and OCT4) (p < 0.05). The high variability in the expression of pluripotent factors found in the adjacent non-malignant counterpart may be due to the paracrine effect of tumors. Furthermore, we found that patients with tumor overexpressing KLF4 and NANOG had significantly higher OS compared to those who showed lower KLF4 and NANOG expressions (log-rank, p = 0.049, and p = 0.0005, respectively). Conversely, subjects presenting increased expressions of SOX2 and OCT4 in tumor showed lower OS rates (log-rank, p = 0.004).
As previously reported [26], the types of surgery and histological subtypes were significant factors associated with ITAC prognosis. Interestingly, through multivariate analysis, the type of surgery was found to be a significant predictor over the histological subtypes. Better OS was observed in patients who underwent ERTC compared to patients who had ER (p = 0.005). Even though ERTC is a more invasive surgery approach, providing wider access to tumor mass, better visualization, and complete removal of tumors, it may result in prolonged survival of patients. According to a multidisciplinary treatment framework, few patients received RT as adjuvant therapy (17%), which was not associated with patient outcomes. In spite of this, there is still a lack of wide literature evaluating the expression of biomarkers in ITAC of the paranasal sinuses at present, likely due to the fact that ITAC is rather infrequent.
Perez Ordonez and colleagues investigated the role of DNA mismatch repair (MMR) gene defects or disruptions of E cadherin/β catenin complex in ITAC by testing the MMR gene products, E cadherin and β catenin, in a cohort of patients with sporadic ITACs. They found that the nuclear expressions of MLH1, MSH2, MSH3, and MSH6 were preserved in these tumors, suggesting that mutations or promoter methylation of MMR genes do not play a role in ITAC pathogenesis [27]. An important result was achieved by Kennedy et al., who found that sinonasal ITACs show a distinctive phenotype, with all cases expressing CK20, CDX 2, and villin and most ITACs also expressing CK7. For this reason, it can be assumed that the expression patterns of CK7, CK20, CDX 2, and villin could be used to distinguish these tumors from other non-ITACs of the sinonasal tract [28]. We studied the status of Mir-126 and found it reduced in ITACs compared to benign tumors, suggesting the potential role of this miRNA acting as a circulating biomarker for the detection of malignant transformation [21]. Recently, we also investigated the role of MiR-let-7 in ITAC and found that its downregulation was associated with advanced-stage (pT3 and pT4) and poorly differentiated (G3) cancer (p < 0.05) [18].
Recently, Veuger et al. [22] systematically reviewed potential prognostic markers of ITAC. This is based on over 20 publications that report a link between biomarkers and the prognosis of sinonasal ITACs. Of the examined biomarkers, expressions of the mucin antigen sialosyl-Tn, C-erbB-2 oncoprotein, TIMP3 methylation, TP53, VEGF, ANXA2, MUC1, and the mucinous histological subtype showed a significant negative correlation with survival. Interestingly, no biomarkers were found to positively correlate with prognosis.
To explore other pathways involved in the molecular pathogenesis of ITACs, in the current study, we investigated the expression of pluripotent factors including the “Yamanaka factors” and NANOG. In our study, high KLF4 expressions directly correlated with better survival rates. Given the role of KLF4 as a negative cell cycle regulator, persistent KLF4 expression could contrast the tumor growth. KLF4 is a versatile TF involved in the regulation of numerous cellular processes, including cell growth. It was reported that KLF4 is associated with growth arrest, and its overexpression induced cell cycle arrest in several cell lines [29]. A primary mechanism by which KLF4 regulates the cell cycle includes induction of the expression of CDKN1A and inhibition of the expressions of CCND1 and CCNB1, which are involved in the progression via the G1/S and G2/M boundaries in the cell cycle [30]. KLF4 expression was frequently found to be lost in various human cancer types [31], and its low expression in tumors supports its tumor-suppressive function. KLF4 has emerged in a recent analysis of lung adenocarcinoma (including 497 tumors and 54 adjacent normal tissue samples) as a possible marker. Low expression of KLF4 (together with other core genes) is significantly correlated with the poor OS of lung cancer patients. Burkitt lymphoma and oral squamous cell carcinoma (OSCC) present another subtype where KLF4’s onco-suppressive role has been recently demonstrated [32]. Its function as tumor suppressor was studied on the basis of gene expression and promoter methylation approaches. IHC demonstrates that KLF4 expression decreases from well-differentiated to moderately differentiated to poorly differentiated OSCC [33]. Overall, these findings appear to be in strong agreement with our results on KLF4 expression in ITAC patients.
Nevertheless, there is evidence supporting the role of KLF4 as an oncogene. For instance, high KLF4 expression has been shown for primary breast ductal carcinoma, being associated with cell migration and invasion [34]. Moreover, an increase in KLF4 expression has been reported in human head and neck squamous cell carcinoma, and its persistent expression was associated with poor prognosis [35]. Similarly, data from our analysis show that NANOG plays an agonist role in tumor growth. High levels of NANOG expression were associated with increased malignancy, and this has been observed in many types of cancers [36], including oral squamous cell carcinoma [37].
Notably, c-MYC and OCT4 are prognostic factors in multivariate analysis. Our findings show that higher expression of c-MYC is related to better OS. These data are in contradiction with the current literature reporting that c-MYC expression is associated with cancer progression and metastasis of various cancers [38]. However, beyond its well-known roles in cell growth and metabolism, c-MYC significantly controls apoptosis by activating or repressing various downstream pathways [39]. A higher level of c-MYC is required for apoptosis compared to the level required to trigger cell proliferation [40]. Therefore, while deregulated c-MYC can be a potent driver of cancer growth, its role in induction apoptosis can also be viewed as a protective mechanism for the organism.
Conversely, high expression of OCT4 is associated with poor prognosis. However, our research did not confirm this, as IHC analysis revealed only four positive cases. We can postulate that there is a post-transcriptional control mechanism that may affect OCT4 protein expression in tumors. Recently, OCT4 has emerged as a master regulator that controls pluripotency, self-renewal, and maintenance of stem cells [41]. High expression of OCT4 was linked to worse prognosis in patients with solid tumors including hepatocellular carcinoma, esophageal squamous cell carcinoma, gastric cancer, cervical cancer, and colorectal cancer [42]. Also, high expressions of OCT4 were observed in breast CSC-like cells (CD44+/CD24−) [43]. There is data showing that OCT4 expression is associated with poor clinical outcome in hormone receptor-positive breast cancer [44].
The expression of OCT4 parallels the expression of SOX2, showing a positive mutual correlation. Both OCT4 and SOX2 are master pluripotent factors serving as a molecular switch that drives the fate of CSCs during cancer progression, with proven clinical potential. In fact, SOX2 expression is much higher in tumor tissues than in normal tissues, and a high level of SOX2 correlates with poor prognosis [43]. Although we found low SOX2 expression in ITAC with respect to non-malignant tissue, its high-level expression within tumor was associated with poor prognosis. Modification or abnormal expression of SOX2 has been implicated in the occurrence, progression, invasion, and metastasis of breast and lung cancers [45]. Concerning the head and neck region, the expression of SOX2 was found much higher in laryngeal carcinoma tissues, and high SOX2 expression is associated with late clinical stage and early recurrence in laryngeal carcinoma. The expression of SOX2 affects the OS of patients, acting as an independent prognostic factor for laryngeal squamous cell carcinoma tissues of patients, indicating that SOX2 may present as a useful prognostic marker and a potential therapeutic target for laryngeal squamous cell carcinoma patients [46,47]. In sinonasal cancer, SOX2 protein expression was highly heterogeneous among different histologies, with SCC showing the highest protein expression [48]. In addition, SOX2 expression in association with βIII-tubulin is common in poorly differentiated sinonasal tumors [49].
Given the role of stemness in the development and progression of ITAC, ALDH1A1, a factor involved in the regulation of gene expression in CSCs, was also investigated in IHC. Although ALDH1A1 has been associated with tumor progression in different cancers [50], we identified a tumor suppressor role of ALDH1A1 in ITAC. Weak or moderate expression level of ALDH1A1 was significantly associated with longer disease-specific survival. A dual ALDH1A1 behavior has been described. ALDH1A1 overexpression was associated with either a better or a worse prognosis, depending on its expression. While weakly stained was associated with a better prognosis, strongly stained was associated with a worse prognosis [51].
5. Conclusions
Despite being limited by a low sample number, single-center design, and lack of validation in independent cohorts, our results highlight that a stemness phenotype with low expressions of KFL4, c-MYC, and NANOG and high levels of SOX2 and OCT4 can be used as a predictor of worse prognosis in ITAC. In multivariate analysis, high c-MYC and low OCT4 were associated with better clinical outcome. The association between c-MYC and ALDH1A1 positivity and favorable prognosis of ITAC suggest that rather than having a role in stemness, these factors act as tumor suppressors and may be used as markers of prognosis and response to treatment in ITAC patients.
Author Contributions
Conceptualization, F.M., A.V. and M.T.; methodology, L.V. and F.M.; validation, A.V., L.V., M.P.F., A.F. and E.A.; formal analysis, F.M. and M.T.; investigation, A.V., F.M.G., G.S., E.P. and G.I.; resources, M.R. and M.A.; data curation, M.R., L.S. and J.N.; writing—original draft preparation, M.T., M.R. and J.N.; writing—review and editing, J.N., M.R. and L.S.; supervision, M.R. All authors have read and agreed to the published version of the manuscript.
Funding
The study was supported by the grant of the Polytechnic University of Marche RSA—2024 to Marco Tomasetti and Federica Monaco and the grant PSA-2017-040020-R. SCIENT.A-2018 to Massimo Re.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Ethics Committee of the Marche Regional Hospital, Ancona, Italy, (protocol No. 501 of 29 September 2011).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ITAC | sinonasal intestinal-type adenocarcinoma |
| KLF4 | Krüppel-like factor 4 |
| SOX2 | SRY-box transcription factor 2 |
| OCT4 | octamer-binding transcription factor 4 |
| NANOG | Nanog homeobox |
| ALDH1A1 | Aldehyde dehydrogenases 1 family member A1 |
| OS | overall survival |
| DFS | disease-free survival |
| CSC | cancer stem cells |
| ER | endoscopic resection |
| ERTC | endonasal endoscopic resection with transnasal craniectomy |
| MRI | magnetic resonance imaging |
| CT | computer tomography |
| PET | positron emission tomography |
| CI | confidence interval |
| ROC | receiver operating characteristic |
| AUC | area under curve |
| CIF | cumulative incidence function |
| MMR | mismatch repair |
| OSCC | oral squamous cell carcinoma |
| IHC | immunohistochemistry |
| 5FU | 5-fluorouracil |
References
- Kim, J.; Chang, H.; Jeong, E.C. Sinonasal intestinal-type adenocarcinoma in the frontal sinus. Arch. Craniofac. Surg. 2018, 19, 210–213. [Google Scholar] [CrossRef]
- Llorente, J.L.; López, F.; Suárez, C.; Hermsen, M.A. Sinonasal carcinoma: Clinical, pathological, genetic and therapeutic advances. Nat. Rev. Clin. Oncol. 2014, 11, 460–472. [Google Scholar] [CrossRef]
- Riobello, C.; Sánchez-Fernández, P.; Cabal, V.N.; García-Marín, R.; Suárez-Fernández, L.; Vivanco, B.; Blanco-Lorenzo, V.; Álvarez Marcos, C.; López, F.; Llorente, J.L.; et al. Aberrant Signaling Pathways in Sinonasal Intestinal-Type Adenocarcinoma. Cancers 2021, 13, 5022. [Google Scholar] [CrossRef]
- Leivo, I.; Holmila, R.; Luce, D.; Steiniche, T.; Dictor, M.; Heikkilä, P.; Husgafvel-Pursiainen, K.; Wolff, H. Occurrence of Sinonasal Intestinal-Type Adenocarcinoma and Non-Intestinal-Type Adenocarcinoma in Two Countries with Different Patterns of Wood Dust Exposure. Cancers 2021, 13, 5245. [Google Scholar] [CrossRef] [PubMed]
- Maffeis, V.; Cappellesso, R.; Zanon, A.; Cazzador, D.; Emanuelli, E.; Martini, A.; Fassina, A. HER2 status in sinonasal intestinal-type adenocarcinoma. Pathol. Res. Pract. 2019, 215, 152432. [Google Scholar] [CrossRef]
- Thompson, L.D.R.; Franchi, A. New tumor entities in the 4th edition of the World Health Organization classification of head and neck tumors: Nasal cavity, paranasal sinuses and skull base. Virchows Arch. 2018, 472, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Meccariello, G.; Deganello, A.; Choussy, O.; Gallo, O.; Vitali, D.; De Raucourt, D.; Georgalas, C. Endoscopic nasal versus open approach for the management of sinonasal adenocarcinoma: A pooled-analysis of 1826 patients. Head Neck 2016, 38 (Suppl. 1), E2267–E2274. [Google Scholar] [CrossRef]
- Rampinelli, V.; Ferrari, M.; Nicolai, P. Intestinal-type adenocarcinoma of the sinonasal tract: An update. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 115–121. [Google Scholar] [CrossRef]
- Abu-Shama, Y.; Renard, S.; Nguyen, D.T.; Henrot, P.; Toussaint, B.; Rumeau, C.; Gallet, P.; Jankowski, R. Descriptive analysis of recurrences of nasal intestinal-type adenocarcinomas after radiotherapy. Head Neck 2022, 44, 1356–1367. [Google Scholar] [CrossRef]
- Camp, S.; Van Gerven, L.; Poorten, V.V.; Nuyts, S.; Hermans, R.; Hauben, E.; Jorissen, M. Long-term follow-up of 123 patients with adenocarcinoma of the sinonasal tract treated with endoscopic resection and postoperative radiation therapy. Head Neck 2016, 38, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Baptista Freitas, M.; Costa, M.; Freire Coelho, A.; Rodrigues Pereira, P.; Leal, M.; Sarmento, C.; Águas, L.; Barbosa, M. Sinonasal Adenocarcinoma: Clinicopathological Characterization and Prognostic Factors. Cureus 2024, 16, e56067. [Google Scholar] [CrossRef]
- Li, J.; Li, B.; Xu, J.; Wang, H.; Gao, Q.; Ye, F.; Xu, Y.; Wu, S.; Cheng, S.; Lu, Y.; et al. A retrospective review of non-intestinal-type adenocarcinoma of nasal cavity and paranasal sinus. Oncol. Lett. 2023, 25, 132. [Google Scholar] [CrossRef]
- Franchi, A.; Gallo, O.; Santucci, M. Clinical relevance of the histological classification of sinonasal intestinal type adenocarcinomas. Hum. Pathol. 1999, 30, 1140–1145. [Google Scholar] [CrossRef]
- Fiaux Camous, D.; Chevret, S.; Oker, N.; Turri Zanoni, M.; Lombardi, D.; Choussy, O.; Frederic, D.; Jorissen, M.; de Gabory, L.; Malard, O.; et al. Prognostic value of the seventh AJCC/UICC TNM classification of intestinal type ethmoid adenocarcinoma: Systematic review and risk prediction model. Head Neck 2017, 39, 668–678. [Google Scholar] [CrossRef]
- Leivo, I. Intestinal-Type Adenocarcinoma: Classification, Immunophenotype, Molecular Features and Differential Diagnosis. Head Neck Pathol. 2017, 11, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Burke, H.B. Predicting Clinical Outcomes Using Molecular Biomarkers. Biomark. Cancer 2016, 8, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Tomasetti, M.; Monaco, F.; Rubini, C.; Rossato, M.; De Quattro, C.; Beltrami, C.; Sollini, G.; Pasquini, E.; Amati, M.; Goteri, G.; et al. AGO2-RIP-Seq reveals miR-34/miR-449 cluster targetome in sinonasal cancers. PLoS ONE 2024, 19, e0295997. [Google Scholar] [CrossRef]
- Gioacchini, F.M.; Di Stadio, A.; De Luca, P.; Camaioni, A.; Pace, A.; Iannella, G.; Rubini, C.; Santarelli, M.; Tomasetti, M.; Scarpa, A.; et al. A pilot study to evaluate the expression of microRNA-let-7a in patients with intestinal-type sinonasal adenocarcinoma. Oncol. Lett. 2023, 2, 69. [Google Scholar] [CrossRef]
- Re, M.; Tomasetti, M.; Monaco, F.; Amati, M.; Rubini, C.; Foschini, M.P.; Sollini, G.; Gioacchini, F.M.; Pasquini, E.; Santarelli, L. NGS-based miRNome identifies miR-449 cluster as marker of malignant transformation of sinonasal inverted papilloma. Oral Oncol. 2021, 122, 105554. [Google Scholar] [CrossRef] [PubMed]
- Re, M.; Tomasetti, M.; Monaco, F.; Amati, M.; Rubini, C.; Sollini, G.; Bajraktari, A.; Gioacchini, F.M.; Santarelli, L.; Pasquini, E. MiRNome analysis identifying miR-205 and miR-449a as biomarkers of disease progression in intestinal-type sinonasal adenocarcinoma. Head Neck 2022, 44, 18–33. [Google Scholar] [CrossRef]
- Tomasetti, M.; Re, M.; Monaco, F.; Gaetani, S.; Rubini, C.; Bertini, A.; Pasquini, E.; Bersaglieri, C.; Bracci, M.; Staffolani, S.; et al. MiR-126 in intestinal-type sinonasal adenocarcinomas: Exosomal transfer of MiR-126 promotes anti-tumour responses. BMC Cancer 2018, 18, 896. [Google Scholar] [CrossRef]
- Veuger, J.; Kuipers, N.C.; Willems, S.M.; Halmos, G.B. Tumor Markers and Their Prognostic Value in Sinonasal ITAC/Non-ITAC. Cancers 2023, 15, 3201. [Google Scholar] [CrossRef] [PubMed]
- Najafi, M.; Farhood, B.; Mortezaee, K. Cancer stem cells (CSCs) in cancer progression and therapy. J. Cell. Physiol. 2019, 234, 8381–8395. [Google Scholar] [CrossRef] [PubMed]
- Van Schaijik, B.; Davis, P.F.; Wickremesekera, A.C.; Tan, S.T.; Itinteang, T. Subcellular localisation of the stem cell markers OCT4, SOX2, NANOG, KLF4 and c-MYC in cancer: A review. J. Clin. Pathol. 2018, 71, 88–91. [Google Scholar] [CrossRef]
- Yang, L.; Shi, P.; Zhao, G.; Xu, J.; Peng, W.; Zhang, J.; Zhang, G.; Wang, X.; Dong, Z.; Chen, F.; et al. Targeting cancer stem cell pathways for cancer therapy. Signal Transduct. Target Ther. 2020, 5, 8. [Google Scholar] [CrossRef] [PubMed]
- Dallan, I.; Fiacchini, G.; Tricò, D.; Barucco, M.; Turri-Zanoni, M.; Ferrari, M.; Di Girolami, L.; Schiavo, G.; Emanuelli, E.; Mattavelli, D.; et al. Sinonasal intestinal-type adenocarcinoma: Multi-institutional retrospective analysis based on 440 patients with long-term follow-up. Eur. J. Cancer 2025, 226, 115623. [Google Scholar] [CrossRef]
- Perez Ordonez, B.; Huynh, N.N.; Berean, K.W.; Jordan, R.C. Expression of mismatch repair proteins, beta catenin, and E cadherin in intestinal type sinonasal adenocarcinoma. J. Clin. Pathol. 2004, 57, 1080–1083. [Google Scholar] [CrossRef]
- Kennedy, M.T.; Jordan, R.C.; Berean, K.W.; Perez Ordonez, B. Expression pattern of CK7, CK20, CDX 2, and villin in intestinal type sinonasal adenocarcinoma. J. Clin. Pathol. 2004, 57, 932–937. [Google Scholar] [CrossRef]
- Ghaleb, A.M.; Yang, V.W. Kruppel-like factor 4 (KLF4): What we currently know. Gene 2017, 611, 27–37. [Google Scholar] [CrossRef]
- Shie, J.L.; Chen, Z.Y.; Fu, M.; Pestell, R.G.; Tseng, C.C. Gut-enriched Kruppel-like factor represses cyclin D1 promoter activity through Sp1 motif. Nucleic Acids Res. 2000, 28, 2969–2976. [Google Scholar] [CrossRef]
- Cai, W.; Jing, M.; Wen, J.; Guo, H.; Xue, Z. Epigenetic Alterations of DNA Methylation and miRNA Contribution to Lung Adenocarcinoma. Front. Genet. 2022, 13, 817552. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Liu, M.; Su, Y.; Zhou, X.; Liu, Y.; Zhang, X. The Janus-faced roles of Krüppel-like factor 4 in oral squamous cell carcinoma cells. Oncotarget 2015, 6, 44480–44494. [Google Scholar] [CrossRef]
- Yu, F.; Li, J.; Chen, H.; Fu, J.; Ray, S.; Huang, S.; Zheng, H.; Ai, W. Kruppel-like factor 4 (KLF4) is required for maintenance of breast cancer stem cells and for cell migration and invasion. Oncogene 2011, 30, 2161–2172. [Google Scholar] [CrossRef] [PubMed]
- Tai, S.K.; Yang, M.H.; Chang, S.Y.; Chang, Y.C.; Li, W.Y.; Tsai, T.L.; Wang, Y.F.; Chu, P.Y.; Hsieh, S.L. Persistent Kruppel-like factor 4 expression predicts progression and poor prognosis of head and neck squamous cell carcinoma. Cancer Sci. 2011, 102, 895–902. [Google Scholar] [CrossRef]
- Saito, M. Novel Roles of Nanog in Cancer Cells and Their Extracellular Vesicles. Cells 2022, 11, 3881. [Google Scholar] [CrossRef]
- Grubelnik, G.; Boštjančič, E.; Grošelj, A.; Zidar, N. Expression of NANOG and its regulation in oral squamous cell carcinoma. Biomed. Res. Int. 2020, 2020, 8573793. [Google Scholar] [CrossRef]
- Pedregal-Mallo, D.; Hermida-Prado, F.; Granda-Díaz, R.; Montoro-Jiménez, I.; Allonca, E.; Pozo-Agundo, E.; Álvarez-Fernández, M.; Álvarez-Marcos, C.; García-Pedrero, J.M.; Rodrigo, J.P. Prognostic significance of the pluripotency factors NANOG, SOX2, and OCT4 in head and neck squamous cell carcinomas. Cancers 2020, 12, 1794. [Google Scholar] [CrossRef]
- Nirala, B.K.; Yustein, J.T. The Role of MYC in Tumor Immune Microenvironment Regulation: Insights and Future Directions. Front. Biosci. 2025, 30, 37304. [Google Scholar] [CrossRef]
- Ahmadi, S.E.; Rahimi, S.; Zarandi, B.; Chegeni, R.; Safa, M. MYC: A multipurpose oncogene with prognostic and therapeutic implications in blood malignancies. J. Hematol. Oncol. 2021, 14, 121. [Google Scholar] [CrossRef]
- Muthalagu, N.; Junttila, M.R.; Wiese, K.E.; Wolf, E.; Morton, J.; Bauer, B.; Evan, G.I.; Eilers, M.; Murphy, D.J. BIM is the primary mediator of MYC-induced apoptosis in multiple solid tissues. Cell. Rep. 2014, 8, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Wang, Y.J. Multifaceted roles of OCT4 in tumor microenvironment: Biology and therapeutic implications. Oncogene 2025, 44, 1213–1229. [Google Scholar] [CrossRef]
- Zhao, X.; Lu, H.; Sun, Y.; Liu, L.; Wang, H. Prognostic value of octamer binding transcription factor 4 for patients with solid tumors: A meta-analysis. Medicine 2020, 99, e22804. [Google Scholar] [CrossRef]
- Wuebben, E.L.; Rizzino, A. The dark side of SOX2: Cancer—A comprehensive overview. Oncotarget 2017, 8, 44917–44943. [Google Scholar] [CrossRef]
- Gwak, J.M.; Kim, M.; Kim, H.J.; Jang, M.H.; Park, S.Y. Expression of embryonal stem cell transcription factors in breast cancer: Oct4 as an indicator for poor clinical outcome and tamoxifen resistance. Oncotarget 2017, 8, 36305–36318. [Google Scholar] [CrossRef]
- Hushmandi, K.; Saadat, S.H.; Mirilavasani, S.; Daneshi, S.; Aref, A.R.; Nabavi, N.; Raesi, R.; Taheriazam, A.; Hashemi, M. The multifaceted role of SOX2 in breast and lung cancer dynamics. Pathol. Res. Pract. 2024, 260, 155386. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.B.; Shen, X.H.; Li, L.; Zhang, Y.F.; Chen, G.Q. SOX2 overexpression correlates with poor prognosis in laryngeal squamous cell carcinoma. Auris Nasus Larynx 2013, 40, 481–486. [Google Scholar] [CrossRef] [PubMed]
- González-Márquez, R.; Llorente, J.L.; Rodrigo, J.P.; García-Pedrero, J.M.; Álvarez-Marcos, C.; Suárez, C.; Hermsen, M.A. SOX2 expression in hypopharyngeal, laryngeal, and sinonasal squamous cell carcinoma. Hum. Pathol. 2014, 45, 851–857. [Google Scholar] [CrossRef]
- Schröck, A.; Göke, F.; Wagner, P.; Bode, M.; Franzen, A.; Braun, M.; Huss, S.; Agaimy, A.; Ihrler, S.; Menon, R.; et al. Sex determining region Y-box 2 (SOX2) amplification is an independent indicator of disease recurrence in sinonasal cancer. PLoS ONE 2013, 8, e59201. [Google Scholar] [CrossRef] [PubMed]
- López, L.; Fernández-Vañes, L.; Cabal, V.N.; García-Marín, R.; Suárez-Fernández, L.; Codina-Martínez, H.; Lorenzo-Guerra, S.L.; Vivanco, B.; Blanco-Lorenzo, V.; Llorente, J.L.; et al. Sox2 and βIII-Tubulin as Biomarkers of Drug Resistance in Poorly Differentiated Sinonasal Carcinomas. J. Pers. Med. 2023, 13, 1504. [Google Scholar] [CrossRef]
- Yue, H.; Hu, Z.; Hu, R.; Guo, Z.; Zheng, Y.; Wang, Y.; Zhou, Y. ALDH1A1 in Cancers: Bidirectional Function, Drug Resistance, and Regulatory Mechanism. Front. Oncol. 2022, 12, 918778. [Google Scholar] [CrossRef]
- Sjöström, M.; Hartman, L.; Honeth, G.; Grabau, D.; Malmström, P.; Hegardt, C.; Fernö, M.; Niméus, E. Stem cell biomarker ALDH1A1 in breast cancer shows an association with prognosis and clinicopathological variables that is highly cut-off dependent. J. Clin. Pathol. 2015, 68, 1012–1019. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).