
Multi-Steroid Profiling and Machine Learning Reveal Androgens as Candidate Biomarkers for Endometrial Cancer Diagnosis: A Case-Control Study


Simple Summary
Abstract

1. Introduction
2. Materials and Methods
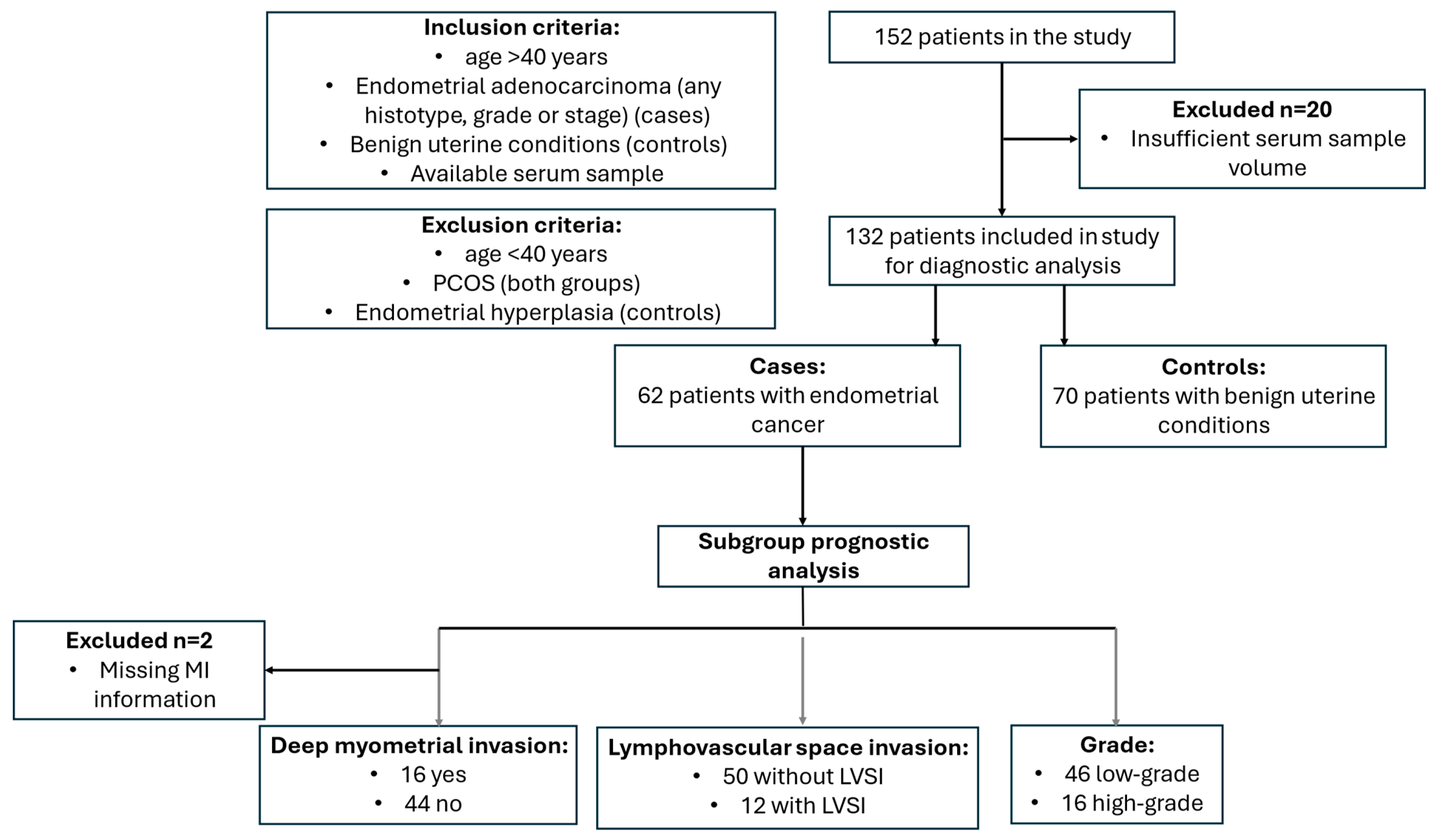
2.1. Study Population
2.2. Multi-Steroid Profiling of Serum Samples by LC-MS/MS
2.2.1. Sample Preparation
2.2.2. LC-MS/MS Analysis
2.3. Measurement of Serum CA-125 and HE4 Levels
2.4. Statistical Analysis
3. Results
3.1. Description of the Cohort
3.2. Preoperative Steroid Hormone Levels Differ Between Patients with EC and Women with Benign Uterine Conditions
3.3. Preoperative 11-Oxyandrogen Levels Differ Between Tumor Grades
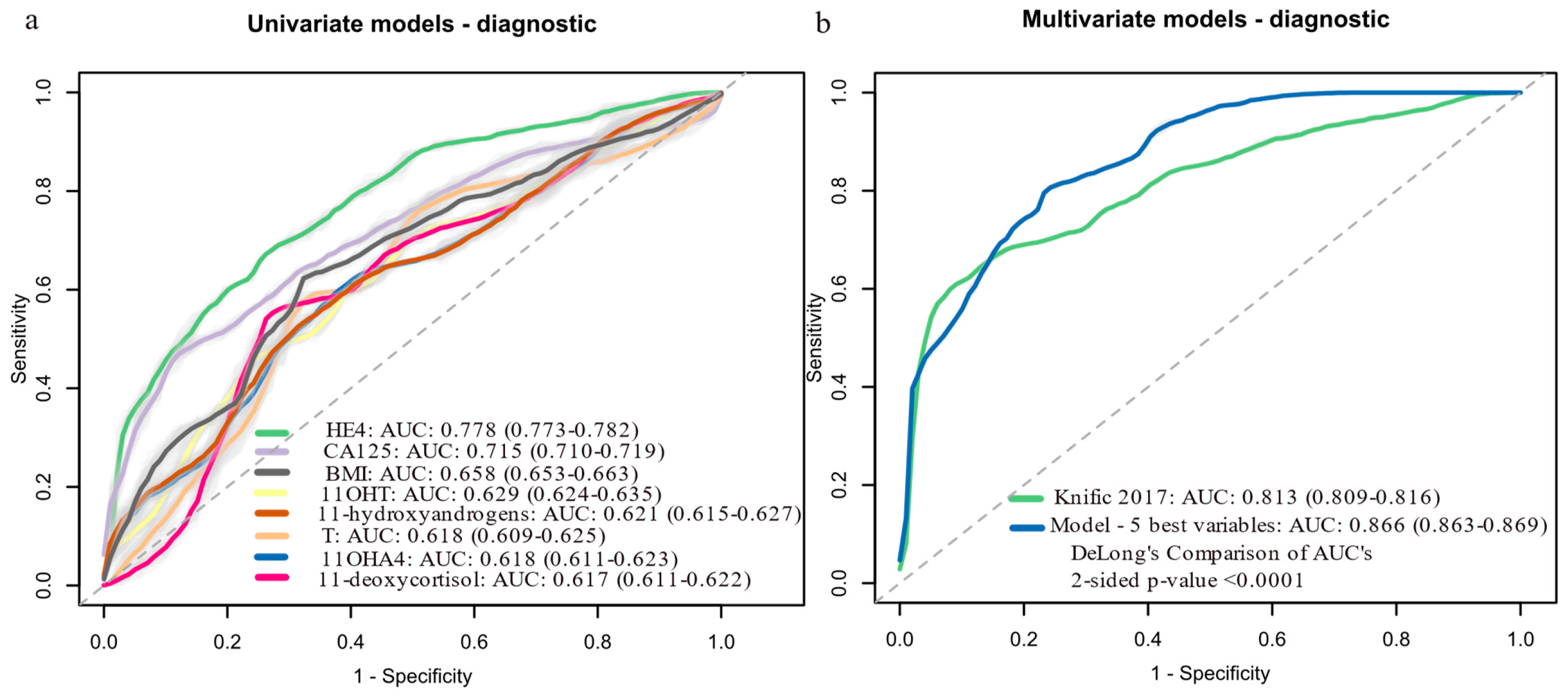
3.4. Development of Machine Learning Diagnostic Models Based on Preoperative Serum Steroid Levels
3.5. Development of Machine Learning Prognostic Models Based on Preoperative Serum Steroid Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 11KA4 | 11-keto-androstenedione |
| 11OHA4 | 11β-hydroxy-androstenedione |
| 11OHT | 11β-hydroxytestosterone |
| A4 | Androstenedione |
| AUC | Area under the receiver operating curve |
| BMI | Body mass index |
| CA-125 | Cancer antigen 125 |
| DHEA | Dehydroepiandrosterone |
| DHT | 5α-dihydrotestosterone |
| dMMR | missmatch repair deficient |
| DSS | Disease-specific survival |
| EC | Endometrial cancer |
| ESI | Electrospray ionization |
| FIGO | International Federation of Gynecology and Obstetrics |
| HE4 | Human epidydymis protein 4 |
| IQR | Interquartile range |
| LC-MS/MS | Liquid chromatography–tandem mass spectrometry |
| LLOQ | Lower limit of quantification |
| LVSI | Lymphovascular space invasion |
| MI | Myometrial invasion |
| MRI | Magnetic resonance imaging |
| MTBE | tert-butyl methyl ether |
| NSMP | Non-specific molecular profile |
| PCOS | Polycystic ovary syndrome |
| QC | Quality control |
| REM | Risk of Endometrial Malignancy |
| SMAC | Steorid Metabolome Analysiss Core |
| T | Testosterone |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Bokhman, J.V. Two pathogenetic types of endometrial carcinoma. Gynecol. Oncol. 1983, 15, 10–17. [Google Scholar] [CrossRef]
- Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; Benz, C.C.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Oaknin, A.; Bosse, T.J.; Creutzberg, C.L.; Giornelli, G.; Harter, P.; Joly, F.; Lorusso, D.; Marth, C.; Makker, V.; Mirza, M.R.; et al. Endometrial cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 860–877. [Google Scholar] [CrossRef]
- Crosbie, E.J.; Kitson, S.J.; McAlpine, J.N.; Mukhopadhyay, A.; Powell, M.E.; Singh, N. Endometrial cancer. Lancet 2022, 399, 1412–1428. [Google Scholar] [CrossRef] [PubMed]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12. [Google Scholar] [CrossRef]
- Clarke, M.A.; Long, B.J.; Del Mar Morillo, A.; Arbyn, M.; Bakkum-Gamez, J.N.; Wentzensen, N. Association of Endometrial Cancer Risk With Postmenopausal Bleeding in Women: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2018, 178, 1210–1222. [Google Scholar] [CrossRef]
- Long, B.; Clarke, M.A.; Morillo, A.D.M.; Wentzensen, N.; Bakkum-Gamez, J.N. Ultrasound detection of endometrial cancer in women with postmenopausal bleeding: Systematic review and meta-analysis. Gynecol. Oncol. 2020, 157, 624–633. [Google Scholar] [CrossRef]
- Plotti, F.; Capriglione, S.; Scaletta, G.; Luvero, D.; Lopez, S.; Nastro, F.F.; Terranova, C.; De Cicco Nardone, C.; Montera, R.; Angioli, R. Implementing the Risk of Endometrial Malignancy Algorithm (REM) adding obesity as a predictive factor: Results of REM-B in a single-center survey. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 225, 51–56. [Google Scholar] [CrossRef]
- Njoku, K.; Pierce, A.; Chiasserini, D.; Geary, B.; Campbell, A.E.; Kelsall, J.; Reed, R.; Geifman, N.; Whetton, A.D.; Crosbie, E.J. Detection of endometrial cancer in cervico-vaginal fluid and blood plasma: Leveraging proteomics and machine learning for biomarker discovery. EBioMedicine 2024, 102, 105064. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Ma, J.; Zhang, J.; Cao, J.; Hu, X.; Huang, Y.; Wang, R.; Wu, J.; Di, W.; Qian, K.; et al. Identification and validation of serum metabolite biomarkers for endometrial cancer diagnosis. EMBO Mol. Med. 2024, 16, 988–1003. [Google Scholar] [CrossRef]
- Troisi, J.; Raffone, A.; Travaglino, A.; Belli, G.; Belli, C.; Anand, S.; Giugliano, L.; Cavallo, P.; Scala, G.; Symes, S.; et al. Development and Validation of a Serum Metabolomic Signature for Endometrial Cancer Screening in Postmenopausal Women. JAMA Netw. Open 2020, 3, e2018327. [Google Scholar] [CrossRef] [PubMed]
- Knific, T.; Vouk, K.; Smrkolj, Š.; Prehn, C.; Adamski, J.; Rižner, T.L. Models including plasma levels of sphingomyelins and phosphatidylcholines as diagnostic and prognostic biomarkers of endometrial cancer. J. Steroid Biochem. Mol. Biol. 2018, 178, 312–321. [Google Scholar] [CrossRef]
- Lee, M.S.; Moon, M.H.; Kim, S.Y.; Jang, S.; Oh, S.; Cho, J.Y. Preoperative risk stratification in women with endometrial cancer: A comparison of contrast-enhanced MR imaging and diffusion-weighted MR imaging. Eur. J. Radiol. 2022, 150, 110276. [Google Scholar] [CrossRef] [PubMed]
- Frumovitz, M.; Singh, D.K.; Meyer, L.; Smith, D.H.; Wertheim, I.; Resnik, E.; Bodurka, D.C. Predictors of final histology in patients with endometrial cancer. Gynecol. Oncol. 2004, 95, 463–468. [Google Scholar] [CrossRef]
- Visser, N.C.M.; Reijnen, C.; Massuger, L.F.A.G.; Nagtegaal, I.D.; Bulten, J.; Pijnenborg, J.M.A. Accuracy of Endometrial Sampling in Endometrial Carcinoma: A Systematic Review and Meta-analysis. Obstet. Gynecol. 2017, 130, 803–813. [Google Scholar] [CrossRef]
- Body, N.; Lavoué, V.; De Kerdaniel, O.; Foucher, F.; Henno, S.; Cauchois, A.; Laviolle, B.; Leblanc, M.; Levêque, J. Are preoperative histology and MRI useful for classification of endometrial cancer risk? BMC Cancer 2016, 16, 498. [Google Scholar] [CrossRef]
- Cabrera, S.; Bebia, V.; López-Gil, C.; Luzarraga-Aznar, A.; Denizli, M.; Salazar-Huayna, L.; Abdessayed, N.; Castellví, J.; Colas, E.; Gil-Moreno, A. Molecular classification improves preoperative risk assessment of endometrial cancer. Gynecol. Oncol. 2024, 189, 56–63. [Google Scholar] [CrossRef]
- Reijnen, C.; Visser, N.C.; Kasius, J.C.; Boll, D.; Geomini, P.M.; Ngo, H.; Van Hamont, D.; Pijlman, B.M.; Vos, M.C.; Bulten, J.; et al. Improved preoperative risk stratification with CA-125 in low-grade endometrial cancer: A multicenter prospective cohort study. J. Gynecol. Oncol. 2019, 30, e70. [Google Scholar] [CrossRef]
- Brennan, D.J.; Hackethal, A.; Metcalf, A.M.; Coward, J.; Ferguson, K.; Oehler, M.K.; Quinn, M.A.; Janda, M.; Leung, Y.; Freemantle, M.; et al. Serum HE4 as a prognostic marker in endometrial cancer—A population based study. Gynecol. Oncol. 2014, 132, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Neilson, A.; Jamieson, A.; Chiu, D.; Leung, S.; Lum, A.; Kommoss, S.; Huntsman, D.G.; Talhouk, A.; Gilks, C.B.; McAlpine, J.N. Serum CA125 levels in the context of ProMisE molecular classification provides pre-operative prognostic information that can direct endometrial cancer management. Gynecol. Oncol. 2025, 193, 1–11. [Google Scholar] [CrossRef]
- Knific, T.; Osredkar, J.; Smrkolj, Š.; Tonin, I.; Vouk, K.; Blejec, A.; Frković Grazio, S.; Rižner, T.L. Novel algorithm including CA-125, HE4 and body mass index in the diagnosis of endometrial cancer. Gynecol. Oncol. 2017, 147, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Rizner, T.L.; Adamski, J. Paramount importance of sample quality in pre-clinical and clinical research—Need for standard operating procedures (SOPs). J. Steroid Biochem. Mol. Biol. 2019, 186, 1–3. [Google Scholar] [CrossRef]
- Schiffer, L.; Shaheen, F.; Gilligan, L.C.; Storbeck, K.-H.; Hawley, J.M.; Keevil, B.G.; Arlt, W.; Taylor, A.E. Multi-steroid profiling by UHPLC-MS/MS with post-column infusion of ammonium fluoride. J. Chromatogr. B 2022, 1209, 123413. [Google Scholar] [CrossRef] [PubMed]
- Schiffer, L.; Kempegowda, P.; Sitch, A.J.; Adaway, J.E.; Shaheen, F.; Ebbehoj, A.; Singh, S.; McTaggart, M.P.; O’Reilly, M.W.; Prete, A.; et al. Classic and 11-oxygenated androgens in serum and saliva across adulthood: A cross-sectional study analyzing the impact of age, body mass index, and diurnal and menstrual cycle variation. Eur. J. Endocrinol. 2023, 188, lvac017. [Google Scholar] [CrossRef]
- Kuhn, M. Building Predictive Models in R Using the caret Package. J. Stat. Softw. 2008, 28, 1–26. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Pernigoni, N.; Zagato, E.; Calcinotto, A.; Troiani, M.; Mestre, R.P.; Calì, B.; Attanasio, G.; Troisi, J.; Minini, M.; Mosole, S.; et al. Commensal bacteria promote endocrine resistance in prostate cancer through androgen biosynthesis. Science 2021, 374, 216–224. [Google Scholar] [CrossRef]
- Devendran, S.; Méndez-García, C.; Ridlon, J.M. Identification and characterization of a 20β-HSDH from the anaerobic gut bacterium Butyricicoccus desmolans ATCC 43058. J. Lipid Res. 2017, 58, 916–925. [Google Scholar] [CrossRef]
- Winter, J.; Morris, G.N.; O’Rourke-Locascio, S.; Bokkenheuser, V.D.; Mosbach, E.H.; Cohen, B.I.; Hylemon, P.B. Mode of action of steroid desmolase and reductases synthesized by Clostridium “scindens” (formerly Clostridium strain 19). J. Lipid Res. 1984, 25, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Zimmermann-Kogadeeva, M.; Wegmann, R.; Goodman, A.L. Mapping human microbiome drug metabolism by gut bacteria and their genes. Nature 2019, 570, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, G.; Gong, R.; Xi, Y. Gut microbiome dysbiosis in patients with endometrial cancer vs. healthy controls based on 16S rRNA gene sequencing. Current microbiology 2023, 80, 239. [Google Scholar] [CrossRef]
- Dahmani, C.; Caron, P.; Simonyan, D.; Turcotte, V.; Grégoire, J.; Plante, M.; Guillemette, C. Circulating adrenal 11-oxygenated androgens are associated with clinical outcome in endometrial cancer. Front. Endocrinol. 2023, 14, 1156680. [Google Scholar] [CrossRef] [PubMed]
- Gjorgoska, M.; Šturm, L.; Lanišnik Rižner, T. Pre-receptor regulation of 11-oxyandrogens differs between normal and cancerous endometrium and across endometrial cancer grades and molecular subtypes. Front. Endocrinol. 2024, 15, 1404804. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Douglas, I.; Forbes, H.; dos-Santos-Silva, I.; Leon, D.A.; Smeeth, L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 5·24 million UK adults. Lancet 2014, 384, 755–765. [Google Scholar] [CrossRef]
- Schiffer, L.; Oestlund, I.; Snoep, J.L.; Gilligan, L.C.; Taylor, A.E.; Sinclair, A.J.; Singhal, R.; Freeman, A.; Ajjan, R.; Tiganescu, A.; et al. Inhibition of the glucocorticoid-activating enzyme 11β-hydroxysteroid dehydrogenase type 1 drives concurrent 11-oxygenated androgen excess. FASEB J. 2024, 38, e23574. [Google Scholar] [CrossRef]
- O’Reilly, M.W.; Kempegowda, P.; Walsh, M.; Taylor, A.E.; Manolopoulos, K.N.; Allwood, J.W.; Semple, R.K.; Hebenstreit, D.; Dunn, W.B.; Tomlinson, J.W.; et al. AKR1C3-Mediated Adipose Androgen Generation Drives Lipotoxicity in Women with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2017, 102, 3327–3339. [Google Scholar] [CrossRef]
- Turcu, A.F.; Rege, J.; Auchus, R.J.; Rainey, W.E. 11-Oxygenated androgens in health and disease. Nat. Rev. Endocrinol. 2020, 16, 284–296. [Google Scholar] [CrossRef]
- Lukanova, A.; Lundin, E.; Micheli, A.; Arslan, A.; Ferrari, P.; Rinaldi, S.; Krogh, V.; Lenner, P.; Shore, R.E.; Biessy, C.; et al. Circulating levels of sex steroid hormones and risk of endometrial cancer in postmenopausal women. Int. J. Cancer 2004, 108, 425–432. [Google Scholar] [CrossRef]
- Michels, K.A.; Brinton, L.A.; Wentzensen, N.; Pan, K.; Chen, C.; Anderson, G.L.; Pfeiffer, R.M.; Xu, X.; Rohan, T.E.; Trabert, B. Postmenopausal Androgen Metabolism and Endometrial Cancer Risk in the Women’s Health Initiative Observational Study. JNCI Cancer Spectr. 2019, 3, pkz029. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.E.; Key, T.J.; Dossus, L.; Rinaldi, S.; Cust, A.; Lukanova, A.; Peeters, P.H.; Onland-Moret, N.C.; Lahmann, P.H.; Berrino, F. Endogenous sex hormones and endometrial cancer risk in women in the European Prospective Investigation into Cancer and Nutrition (EPIC). Endocr. Relat. Cancer 2008, 15, 485–497. [Google Scholar] [CrossRef]
- Clendenen, T.V.; Hertzmark, K.; Koenig, K.L.; Lundin, E.; Rinaldi, S.; Johnson, T.; Krogh, V.; Hallmans, G.; Idahl, A.; Lukanova, A.; et al. Premenopausal Circulating Androgens and Risk of Endometrial Cancer: Results of a Prospective Study. Horm. Cancer 2016, 7, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Pavlič, R.; Vidic, S.; Anko, M.; Knific, T.; Büdefeld, T.; Marton, K.; Sinreih, M.; Poschner, S.; Jäger, W.; Frković-Grazio, S.; et al. Altered Profile of E1-S Transporters in Endometrial Cancer: Lower Protein Levels of ABCG2 and OSTβ and Up-Regulation of SLCO1B3 Expression. Int. J. Mol. Sci. 2021, 22, 3819. [Google Scholar] [CrossRef] [PubMed]
- Sinreih, M.; Hevir, N.; Rižner, T.L. Altered expression of genes involved in progesterone biosynthesis, metabolism and action in endometrial cancer. Chem. Biol. Interact. 2013, 202, 210–217. [Google Scholar] [CrossRef]
- Hojnik, M.; Kenda Šuster, N.; Smrkolj, Š.; Frković Grazio, S.; Verdenik, I.; Rižner, T.L. AKR1C3 Is Associated with Better Survival of Patients with Endometrial Carcinomas. J. Clin. Med. 2020, 9, 4105. [Google Scholar] [CrossRef]
- Ito, K.; Suzuki, T.; Akahira, J.-i.; Moriya, T.; Kaneko, C.; Utsunomiya, H.; Yaegashi, N.; Okamura, K.; Sasano, H. Expression of androgen receptor and 5α-reductases in the human normal endometrium and its disorders. Int. J. Cancer 2002, 99, 652–657. [Google Scholar] [CrossRef]
- Šmuc, T.; Rižner, T.L. Aberrant pre-receptor regulation of estrogen and progesterone action in endometrial cancer. Mol. Cell. Endocrinol. 2009, 301, 74–82. [Google Scholar] [CrossRef]
- Kamal, A.M.; Bulmer, J.N.; DeCruze, S.B.; Stringfellow, H.F.; Martin-Hirsch, P.; Hapangama, D.K. Androgen receptors are acquired by healthy postmenopausal endometrial epithelium and their subsequent loss in endometrial cancer is associated with poor survival. Br. J. Cancer 2016, 114, 688–696. [Google Scholar] [CrossRef]
- Tangen, I.L.; Onyango, T.B.; Kopperud, R.; Berg, A.; Halle, M.K.; Øyan, A.M.; Werner, H.M.J.; Trovik, J.; Kalland, K.H.; Salvesen, H.B.; et al. Androgen receptor as potential therapeutic target in metastatic endometrial cancer. Oncotarget 2016, 7, 49289–49298. [Google Scholar] [CrossRef]
- Pavlič, R.; Gjorgoska, M.; Hafner, E.; Sinreih, M.; Gajser, K.; Poschner, S.; Jäger, W.; Rižner, T.L. In the Model Cell Lines of Moderately and Poorly Differentiated Endometrial Carcinoma, Estrogens Can Be Formed via the Sulfatase Pathway. Front. Mol. Biosci. 2021, 8, 743403. [Google Scholar] [CrossRef] [PubMed]
- Barr, C.E.; Njoku, K.; Jones, E.R.; Crosbie, E.J. Serum CA125 and HE4 as Biomarkers for the Detection of Endometrial Cancer and Associated High-Risk Features. Diagnostics 2022, 12, 2834. [Google Scholar] [CrossRef]
- Antonsen, S.L.; Høgdall, E.; Christensen, I.J.; Lydolph, M.; Tabor, A.; Loft Jakobsen, A.; Fagö-Olsen, C.L.; Andersen, E.S.; Jochumsen, K.; Høgdall, C. HE4 and CA125 levels in the preoperative assessment of endometrial cancer patients: A prospective multicenter study (ENDOMET). Acta Obstet. Gynecol. Scand. 2013, 92, 1313–1322. [Google Scholar] [CrossRef] [PubMed]
- Gong, S.; Quan, Q.; Meng, Y.; Wu, J.; Yang, S.; Hu, J.; Mu, X. The value of serum HE4 and CA125 levels for monitoring the recurrence and risk stratification of endometrial endometrioid carcinoma. Heliyon 2023, 9, e18016. [Google Scholar] [CrossRef]
- O’Toole, S.A.; Huang, Y.; Norris, L.; Power Foley, M.; Shireen, R.; McDonald, S.; Kamran, W.; Ibrahim, N.; Ward, M.; Thompson, C.; et al. HE4 and CA125 as preoperative risk stratifiers for lymph node metastasis in endometrioid carcinoma of the endometrium: A retrospective study in a cohort with histological proof of lymph node status. Gynecol. Oncol. 2021, 160, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Behrouzi, R.; Barr, C.E.; Crosbie, E.J. HE4 as a Biomarker for Endometrial Cancer. Cancers 2021, 13, 4764. [Google Scholar] [CrossRef]
- Degez, M.; Caillon, H.; Chauviré-Drouard, A.; Leroy, M.; Lair, D.; Winer, N.; Thubert, T.; Dochez, V. Endometrial cancer: A systematic review of HE4, REM and REM-B. Clin. Chim. Acta 2021, 515, 27–36. [Google Scholar] [CrossRef]
- He, Y.; Wang, J.; Ma, C.X.; Kang, Y.H. Role of Human Epididymis Protein 4 (HE4) in Determining Survival of Patients With Endometrial Cancer: A Meta-Analysis. Technol. Cancer Res. Treat. 2020, 19, 1533033820971660. [Google Scholar] [CrossRef]
- Tangen, I.L.; Fasmer, K.E.; Konings, G.F.; Jochems, A.; Delvoux, B.; Xanthoulea, S.; Stokowy, T.; Strand, E.; Berg, H.F.; Auriola, S.; et al. Blood steroids are associated with prognosis and fat distribution in endometrial cancer. Gynecol. Oncol. 2019, 152, 46–52. [Google Scholar] [CrossRef]
- Forsse, D.; Forsse, D.; Tangen, I.L.; Tangen, I.L.; Fasmer, K.E.; Fasmer, K.E.; Halle, M.K.; Halle, M.K.; Viste, K.; Almås, B.; et al. Blood steroid levels predict survival in endometrial cancer and reflect tumor estrogen signaling. Gynecol. Oncol. 2019, 156, 400–406. [Google Scholar] [CrossRef]
- Romano, A.; Rižner, T.L.; Werner, H.M.J.; Semczuk, A.; Lowy, C.; Schröder, C.; Griesbeck, A.; Adamski, J.; Fishman, D.; Tokarz, J. Endometrial cancer diagnostic and prognostic algorithms based on proteomics, metabolomics, and clinical data: A systematic review. Front. Oncol. 2023, 13, 1120178. [Google Scholar] [CrossRef] [PubMed]
- Tea Lanišnik Rižner, A.R. The discovery of biomarkers for endometrial cancer: Update over the last years. Expert Rev. Mol. Diagn. IERO 2025, IERO 2505546. [Google Scholar] [CrossRef]
- Ura, B.; Capaci, V.; Aloisio, M.; Di Lorenzo, G.; Romano, F.; Ricci, G.; Monasta, L. A Targeted Proteomics Approach for Screening Serum Biomarkers Observed in the Early Stage of Type I Endometrial Cancer. Biomedicines 2022, 10, 1857. [Google Scholar] [CrossRef]
- Ura, B.; Biffi, S.; Monasta, L.; Arrigoni, G.; Battisti, I.; Di Lorenzo, G.; Romano, F.; Aloisio, M.; Celsi, F.; Addobbati, R.; et al. Two Dimensional-Difference in Gel Electrophoresis (2D-DIGE) Proteomic Approach for the Identification of Biomarkers in Endometrial Cancer Serum. Cancers 2021, 13, 3639. [Google Scholar] [CrossRef] [PubMed]
- Enroth, S.; Berggrund, M.; Lycke, M.; Lundberg, M.; Assarsson, E.; Olovsson, M.; Stålberg, K.; Sundfeldt, K.; Gyllensten, U. A two-step strategy for identification of plasma protein biomarkers for endometrial and ovarian cancer. Clin. Proteom. 2018, 15, 38. [Google Scholar] [CrossRef]
- Tarney, C.M.; Wang, G.; Bateman, N.W.; Conrads, K.A.; Zhou, M.; Hood, B.L.; Loffredo, J.; Tian, C.; Darcy, K.M.; Hamilton, C.A.; et al. Biomarker panel for early detection of endometrial cancer in the Prostate, Lung, Colorectal, and Ovarian cancer screening trial. Am. J. Obstet. Gynecol. 2019, 221, 472.e1–472.e10. [Google Scholar] [CrossRef]
- Celsi, F.; Monasta, L.; Arrigoni, G.; Battisti, I.; Licastro, D.; Aloisio, M.; Di Lorenzo, G.; Romano, F.; Ricci, G.; Ura, B. Gel-Based Proteomic Identification of Suprabasin as a Potential New Candidate Biomarker in Endometrial Cancer. Int. J. Mol. Sci. 2022, 23, 2076. [Google Scholar] [CrossRef]
- Ceylan, Y.; Akpınar, G.; Doger, E.; Kasap, M.; Guzel, N.; Karaosmanoglu, K.; Kopuk, S.Y.; Yucesoy, I. Proteomic analysis in endometrial cancer and endometrial hyperplasia tissues by 2D-DIGE technique. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101652. [Google Scholar] [CrossRef]
- Akkour, K.; Alanazi, I.O.; Alfadda, A.A.; Alhalal, H.; Masood, A.; Musambil, M.; Rahman, A.M.A.; Alwehaibi, M.A.; Arafah, M.; Bassi, A.; et al. Tissue-Based Proteomic Profiling in Patients with Hyperplasia and Endometrial Cancer. Cells 2022, 11, 2119. [Google Scholar] [CrossRef]
- Hishinuma, E.; Shimada, M.; Matsukawa, N.; Shima, Y.; Li, B.; Motoike, I.N.; Shibuya, Y.; Hagihara, T.; Shigeta, S.; Tokunaga, H.; et al. Identification of predictive biomarkers for endometrial cancer diagnosis and treatment response monitoring using plasma metabolome profiling. Cancer Metab. 2023, 11, 16. [Google Scholar] [CrossRef]
- Ihata, Y.; Miyagi, E.; Numazaki, R.; Muramatsu, T.; Imaizumi, A.; Yamamoto, H.; Yamakado, M.; Okamoto, N.; Hirahara, F. Amino acid profile index for early detection of endometrial cancer: Verification as a novel diagnostic marker. Int. J. Clin. Oncol. 2014, 19, 364–372. [Google Scholar] [CrossRef]
- Njoku, K.; Campbell, A.E.; Geary, B.; MacKintosh, M.L.; Derbyshire, A.E.; Kitson, S.J.; Sivalingam, V.N.; Pierce, A.; Whetton, A.D.; Crosbie, E.J. Metabolomic Biomarkers for the Detection of Obesity-Driven Endometrial Cancer. Cancers 2021, 13, 718. [Google Scholar] [CrossRef] [PubMed]
- Audet-Delage, Y.; Villeneuve, L.; Grégoire, J.; Plante, M.; Guillemette, C. Identification of Metabolomic Biomarkers for Endometrial Cancer and Its Recurrence after Surgery in Postmenopausal Women. Front. Endocrinol. 2018, 9, 87. [Google Scholar] [CrossRef] [PubMed]
- Troisi, J.; Sarno, L.; Landolfi, A.; Scala, G.; Martinelli, P.; Venturella, R.; Di Cello, A.; Zullo, F.; Guida, M. Metabolomic Signature of Endometrial Cancer. J. Proteome Res. 2018, 17, 804–812. [Google Scholar] [CrossRef]
- Bahado-Singh, R.O.; Lugade, A.; Field, J.; Al-Wahab, Z.; Han, B.; Mandal, R.; Bjorndahl, T.C.; Turkoglu, O.; Graham, S.F.; Wishart, D.; et al. Metabolomic prediction of endometrial cancer. Metabolomics 2017, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Gu, M.; Chen, X.; Sun, Y.; Wang, L.; Shu, H.; Qian, C. A metabolomic signature of FIGO stage I and II endometrial cancer. Neoplasma 2021, 68, 1283–1291. [Google Scholar] [CrossRef]
- Yan, X.; Zhao, W.; Wei, J.; Yao, Y.; Sun, G.; Wang, L.; Zhang, W.; Chen, S.; Zhou, W.; Zhao, H.; et al. A serum lipidomics study for the identification of specific biomarkers for endometrial polyps to distinguish them from endometrial cancer or hyperplasia. Int. J. Cancer 2022, 150, 1549–1559. [Google Scholar] [CrossRef]
- Schuhn, A.; Tobar, T.W.; Gahlawat, A.W.; Hauke, J.; Baumann, L.; Okun, J.G.; Nees, J. Potential of blood-based biomarker approaches in endometrium and breast cancer: A case-control comparison study. Arch. Gynecol. Obstet. 2022, 306, 1623–1632. [Google Scholar] [CrossRef]
- Cheng, S.-C.; Chen, K.; Chiu, C.-Y.; Lu, K.-Y.; Lu, H.-Y.; Chiang, M.-H.; Tsai, C.-K.; Lo, C.-J.; Cheng, M.-L.; Chang, T.-C.; et al. Metabolomic biomarkers in cervicovaginal fluid for detecting endometrial cancer through nuclear magnetic resonance spectroscopy. Metabolomics 2019, 15, 146. [Google Scholar] [CrossRef]
- Yi, R.; Xie, L.; Wang, X.; Shen, C.; Chen, X.; Qiao, L. Multi-Omic Profiling of Multi-Biosamples Reveals the Role of Amino Acid and Nucleotide Metabolism in Endometrial Cancer. Front. Oncol. 2022, 12, 861142. [Google Scholar] [CrossRef] [PubMed]
- Troisi, J.; Mollo, A.; Lombardi, M.; Scala, G.; Richards, S.M.; Symes, S.J.K.; Travaglino, A.; Neola, D.; de Laurentiis, U.; Insabato, L.; et al. The Metabolomic Approach for the Screening of Endometrial Cancer: Validation from a Large Cohort of Women Scheduled for Gynecological Surgery. Biomolecules 2022, 12, 1229. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Cao, M.; Liu, C.; Zhang, C.; Li, C.; Cheng, W.; Zhang, S.; Zhang, H.; Zhu, W. Three plasma-based microRNAs as potent diagnostic biomarkers for endometrial cancer. Cancer Biomark. 2021, 31, 127–138. [Google Scholar] [CrossRef]
- Torres, A.; Torres, K.; Pesci, A.; Ceccaroni, M.; Paszkowski, T.; Cassandrini, P.; Zamboni, G.; Maciejewski, R. Diagnostic and prognostic significance of miRNA signatures in tissues and plasma of endometrioid endometrial carcinoma patients. Int. J. Cancer 2013, 132, 1633–1645. [Google Scholar] [CrossRef]
- Liu, J.; Hu, D.; Lin, Y.; Chen, X.; Yang, R.; Li, L.; Zhan, Y.; Bao, H.; Zang, L.; Zhu, M.; et al. Early detection of uterine corpus endometrial carcinoma utilizing plasma cfDNA fragmentomics. BMC Med. 2024, 22, 310. [Google Scholar] [CrossRef]
- Zou, J.; Wang, E. eTumorType, An Algorithm of Discriminating Cancer Types for Circulating Tumor Cells or Cell-Free DNAs in Blood. Genom. Proteom. Bioinform. 2017, 15, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Ashley, C.W.; Selenica, P.; Patel, J.; Wu, M.; Nincevic, J.; Lakhman, Y.; Zhou, Q.; Shah, R.H.; Berger, M.F.; Da Cruz Paula, A.; et al. High-Sensitivity Mutation Analysis of Cell-Free DNA for Disease Monitoring in Endometrial Cancer. Clin. Cancer Res. 2023, 29, 410–421. [Google Scholar] [CrossRef]
- Yayla Abide, C.; Bostanci Ergen, E.; Cogendez, E.; Kilicci, C.; Uzun, F.; Ozkaya, E.; Karateke, A. Evaluation of complete blood count parameters to predict endometrial cancer. J. Clin. Lab. Anal. 2018, 32, e22438. [Google Scholar] [CrossRef]
- Marin, A.-G.; Filipescu, A.G.; Petca, R.C.; Vlădăreanu, R.; Petca, A. Clinical Correlations between Serological Markers and Endometrial Cancer. Cancers 2024, 16, 1935. [Google Scholar] [CrossRef]
- Ronsini, C.; Iavarone, I.; Vastarella, M.G.; Della Corte, L.; Andreoli, G.; Bifulco, G.; Cobellis, L.; De Franciscis, P. SIR-EN-New Biomarker for Identifying Patients at Risk of Endometrial Carcinoma in Abnormal Uterine Bleeding at Menopause. Cancers 2024, 16, 3567. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable (Median (IQR) or n(%)) | Controls (n = 70; 100%) | Cases (n = 62; 100%) | p-Value ‡ |
|---|---|---|---|
| Age (years) | 64.0 (55.0–71.0) | 64.5 (59.3–71.0) | 0.624 |
| BMI (kg/m2) | 27.4 (23.8–30.5) | 30.4 (27.2–35.2) | 0.005 |
| BMI category | |||
| Normal (<25 kg/m2) | 25 (35.7%) | 14 (22.6%) | 0.055 |
| Overweight (25–30 kg/m2) | 26 (37.2%) | 19 (30.6%) | |
| Obese (≥30 kg/m2) | 19 (27.1%) | 29 (46.8%) | |
| Menopausal status | |||
| Premenopausal | 8 (11.4%) | 2 (3.2%) | 0.148 |
| Postmenopausal | 62 (88.6%) | 60 (96.8%) | |
| Diabetes type 2 | |||
| Yes | 10 (14.3%) | 9 (14.5%) | 0.900 |
| No | 60 (85.7%) | 52 (83.8%) | |
| Missing data | 0 (0%) | 1 (1.6%) | |
| Arterial hypertension | |||
| Yes | 40 (57.1%) | 38 (61.3%) | 0.473 |
| No | 30 (42.9) | 23 (37.1%) | |
| Missing data | 0 (0%) | 1 1.6%) | |
| Hormonal therapy in the past | |||
| Yes | 2 (2.9%) | 1 (1.6%) | 0.100 |
| No | 67 (95.7%) | 59 (95.2%) | |
| Missing data | 1 (1.4%) | 2 (3.2%) | |
| Medication intake | |||
| Yes | 46 (65.7%) | 45 (72.6%) | 0.508 |
| No | 24 (34.3%) | 17 (27.4%) | |
| Smoking status | |||
| Nonsmoker | 45 (64.3%) | 45 (72.6%) | 0.170 |
| Ever-smoker | 20 (28.6%) | 11 (17.7%) | |
| Missing data | 5 (7.1%) | 6 (9.7%) | |
| Tumor biomarkers | |||
| CA-125 (kU/L) | 13.0 (9.1–19.0) | 21.7 (13.4–34.5) | <0.001 |
| HE4 (pmol/L) | 55.6 (45.6–69.7) | 86.0 (64.7–130.4) | <0.001 |
| Controls (n = 70; 100%) | Cases (n = 62; 100%) | p-Value | |||
|---|---|---|---|---|---|
| Analyte | Median | IQR | Median | IQR | |
| 11-oxyandrogens (nM) | |||||
| 11OHA4 | 13.29 | 10.30–17.56 | 16.62 | 11.88–21.14 | 0.010 |
| 11KA4 | 5.84 | 4.31–6.99 | 5.40 | 3.78–7.95 | 0.810 |
| 11OHT | 0.75 | 0.49–1.06 | 1.00 | 0.66–1.48 | 0.006 |
| 11KT | 1.64 | 1.11–2.02 | 1.73 | 1.10–2.20 | 0.564 |
| Classic androgens (nM) | |||||
| DHEA | 9.29 | 6.96–14.39 | 10.98 | 7.53–18.14 | 0.123 |
| A4 | 2.99 | 2.28–4.06 | 3.67 | 2.70–4.68 | 0.029 |
| T | 0.77 | 0.58–1.30 | 1.18 | 0.81–1.65 | 0.010 |
| Glucocorticoids (nM) | |||||
| 17α-hydroxy-progesterone | 0.95 | 0.66–1.42 | 1.28 | 0.83–1.85 | 0.041 |
| 11-deoxycortisol | 1.07 | 0.73–1.60 | 1.66 | 0.93–2.37 | 0.012 |
| Cortisol | 370.3 | 257.70–495.30 | 420.7 | 298.60–602.10 | 0.055 |
| Cortisone | 64.62 | 53.27–75.86 | 64.98 | 55.73–72.94 | 0.995 |
| Mineralocorticoids (nM) | |||||
| Corticosterone | 9.45 | 5.69–16.96 | 11.54 | 6.16–22.54 | 0.127 |
| LVSI | Deep MI a | |||||
|---|---|---|---|---|---|---|
| Analyte (Median (IQR)) | Negative (n = 50; 81%) | Positive (n = 12; 19%) | p-Value | No (n = 44, 73%) | Yes (n = 16, 27%) | p-Value |
| 11-oxyandrogens (nM) | ||||||
| 11OHA4 | 16.40 (11.75–20.61) | 19.51 (14.84–29.40) | 0.187 | 16.77 (10.80–21.71) | 16.89 (15.26–21.88) | 0.483 |
| 11KA4 | 5.07 (3.76–7.82) | 5.95 (5.19–8.33) | 0.269 | 4.85 (3.72–7.98) | 6.04 (4.72–8.05) | 0.367 |
| 11OHT | 0.99 (0.65–1.42) | 1.18 (0.74–1.48) | 0.782 | 1.00 (0.63–1.53) | 0.97 (0.76–1.44) | 0.848 |
| 11KT | 1.67 (1.10–2.20) | 1.88 (1.10–2.15) | 0.838 | 1.78 (0.92–2.31) | 1.73 (1.23–1.97) | 0.821 |
| Classic androgens (nM) | ||||||
| DHEA | 11.25 (7.72–18.17) | 9.82 (5.98–15.31) | 0.364 | 11.73 (7.91–20.01) | 9.16 (7.25–12.27) | 0.116 |
| A4 | 3.61 (2.79–4.68) | 4.31 (2.49–4.68) | 0.972 | 3.67 (2.79–5.12) | 3.53 (2.64–4.40) | 0.559 |
| T | 1.19 (0.84–1.65) | 1.05 (0.65–1.28) | 0.402 | 1.15 (0.79–1.65) | 1.14 (0.77–1.27) | 0.353 |
| Glucocorticoids (nM) | ||||||
| 17α-hydroxy-progesterone | 1.28 (0.82–1.72) | 1.24 (0.87–1.99) | 0.762 | 1.25 (0.82–1.88) | 1.41 (0.84–1.80) | 0.763 |
| 11-deoxycortisol | 1.64 (0.83–2.37) | 1.69 (1.26–2.06) | 0.831 | 1.64 (0.89–2.43) | 1.75 (1.15–2.33) | 0.780 |
| Cortisol | 396.9 (275.3–589.8) | 497.7 (422.5–646.1) | 0.125 | 401.5 (281.1–620.7) | 438.0 (362.2–594.9) | 0.688 |
| Cortisone | 64.45 (54.37–72.94) | 68.96 (60.73–72.81) | 0.465 | 65.86 (52.18–73.92) | 63.43 (60.76–68.34) | 0.973 |
| Mineralocorticoids (nM) | ||||||
| Corticosterone | 10.66 (5.41–23.55) | 14.76 (11.62–21.75) | 0.144 | 10.83 (5.90–24.80) | 13.61 (9.86–20.21) | 0.493 |
| Tumor biomarkers | ||||||
| CA-125 (kU/L) | 20.26 (13.10–30.75) | 39.66 (21.37–57.32) | 0.018 | 21.82 (12.37–34.85) | 23.99 (19.69–35.77) | 0.285 |
| HE4 (pmol/L) | 79.46 (61.84–103.92) | 131.51 (114.60–366.27) | 0.001 | 79.46 (61.35–114.95) | 118.95 (87.42–188.53) | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gjorgoska, M.; Taylor, A.E.; Smrkolj, Š.; Rižner, T.L. Multi-Steroid Profiling and Machine Learning Reveal Androgens as Candidate Biomarkers for Endometrial Cancer Diagnosis: A Case-Control Study. Cancers 2025, 17, 1679. https://doi.org/10.3390/cancers17101679
Gjorgoska M, Taylor AE, Smrkolj Š, Rižner TL. Multi-Steroid Profiling and Machine Learning Reveal Androgens as Candidate Biomarkers for Endometrial Cancer Diagnosis: A Case-Control Study. Cancers. 2025; 17(10):1679. https://doi.org/10.3390/cancers17101679
Chicago/Turabian StyleGjorgoska, Marija, Angela E. Taylor, Špela Smrkolj, and Tea Lanišnik Rižner. 2025. "Multi-Steroid Profiling and Machine Learning Reveal Androgens as Candidate Biomarkers for Endometrial Cancer Diagnosis: A Case-Control Study" Cancers 17, no. 10: 1679. https://doi.org/10.3390/cancers17101679
APA StyleGjorgoska, M., Taylor, A. E., Smrkolj, Š., & Rižner, T. L. (2025). Multi-Steroid Profiling and Machine Learning Reveal Androgens as Candidate Biomarkers for Endometrial Cancer Diagnosis: A Case-Control Study. Cancers, 17(10), 1679. https://doi.org/10.3390/cancers17101679