
Developing Cancer Quality of Care Indicators to Quantify the Impact of a Global Destabilization of the Care System (COLLAT-COVID)

 , , ,
, , ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
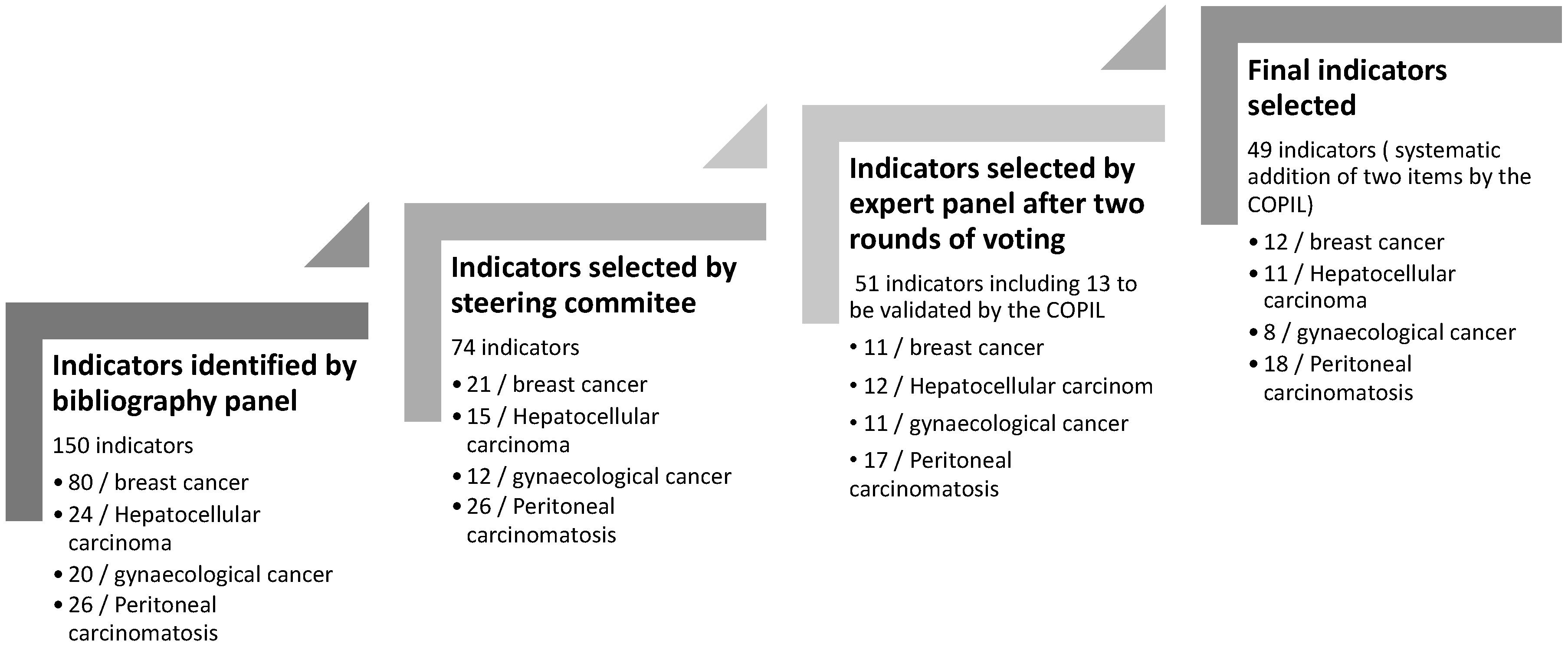
3.1. Quality Indicator Selection Process
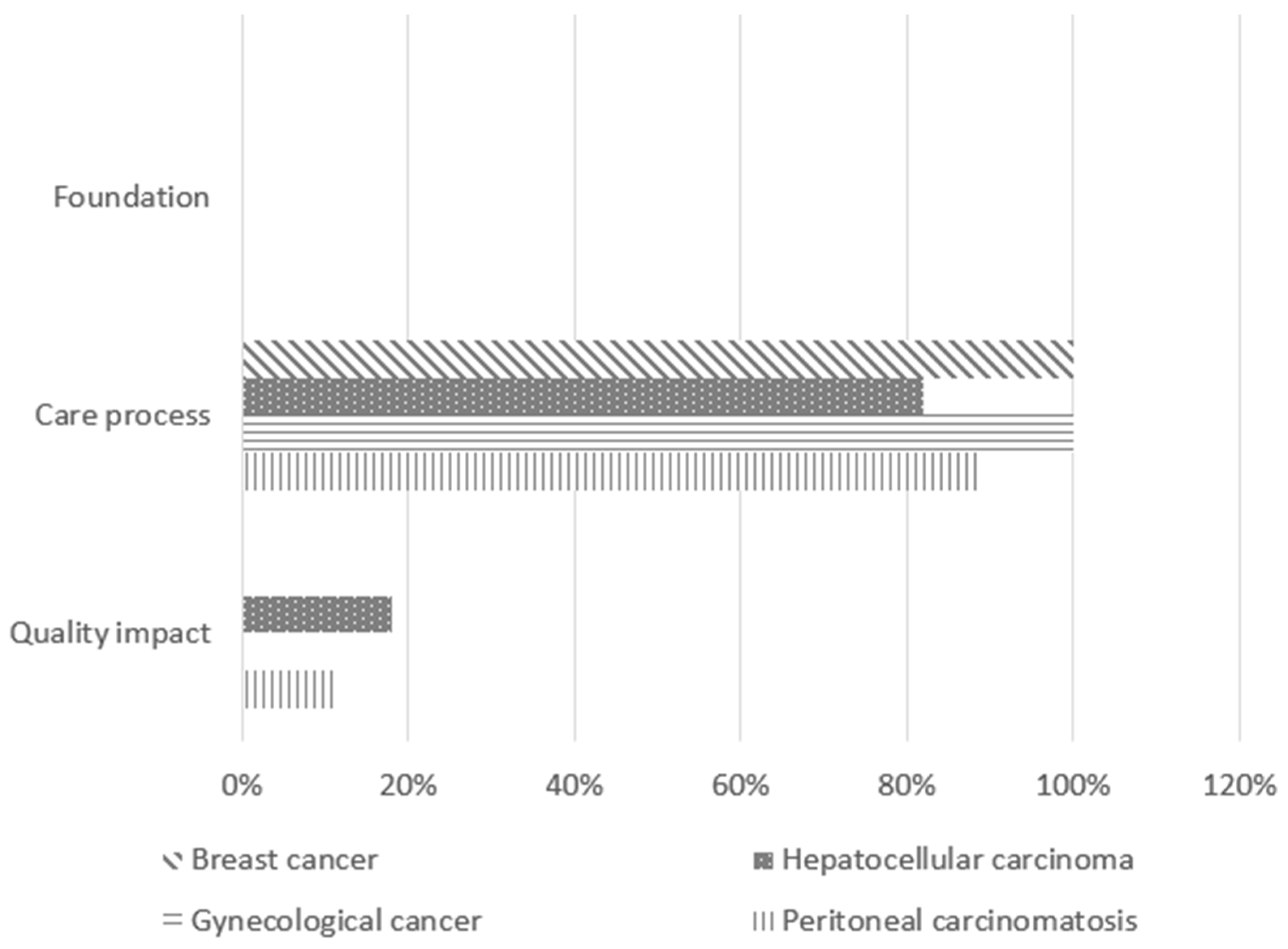
3.2. Nature of Validated Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| QIs | Quality indicators |
Appendix A

{kind=link}
{kind=link}
| Indicator Title | Type of Indicator | Numerator | Denominator | Inclusion Criteria | Exclusion Criteria | Data Sources | Bibliographic References |
|---|---|---|---|---|---|---|---|
| Stage at diagnosis | Care process Staging | Number of women at each stage by UICC 8th edition | Number of women diagnosed with invasive non-metastatic breast cancer | Age > 18 Invasive non-metastatic carcinoma of the breast | Cancer at another location during the year Neoadjuvant chemotherapy or hormone therapy | Electronic Health Record (EHR) | [28,29] |
| Proportion of women with MRI in invasive lobular carcinoma | Care process Diagnosis | Number of patients with non-metastatic invasive lobular carcinoma who had an MRI with treatment | Number of patients treated for non-metastatic invasive lobular carcinoma | Age > 18 Diagnosis of invasive lobular carcinoma | Metastatic cancer | EHR SNDS (National Health Data System) | [30] |
| Number of women diagnosed with invasive non-metastatic breast cancer/week | Care process Diagnosis | Number of women diagnosed with invasive non-metastatic breast cancer/week | Number of women diagnosed with breast cancer/week | Age > 18 Invasive non-metastatic breast carcinoma | EHR | Added by the bibliographic panel. | |
| Proportion of women who had their first treatment (surgery, chemotherapy, or hormone therapy) within 6 weeks or less of the date of the mammogram preceding treatment | Care process Therapeutic delay | Number of women who had their first treatment within 6 weeks or less of the date of the mammogram | Number of women having had a mammogram followed by treatment | Age > 18 Ductal carcinoma in situ or invasive non-metastatic invasive carcinoma of the breast Have had a mammogram Have had a biopsy Have received at least one treatment | History of contralateral breast cancer Other cancers diagnosed in the same year Chaining problem between different AMDB stays | EHR SNDS | [21,31] |
| Proportion of women with ductal carcinoma in situ or invasive non-metastatic breast cancer whose time between surgery and first additional treatment (chemotherapy or radiotherapy) is within the expected timeframe | Care process Therapeutic delay | Time between surgery and radiotherapy < 12 weeks of radiotherapy Time between surgery and chemotherapy < 6 weeks if chemotherapy | Invasive breast carcinoma (CIM-10): C50; C500; C506; C508; C509 + Chirurgie (CCAM): QEFA001; QEFA003; QEFA004; QEFA005; QEFA007; QEFA008; QEFA010; QEFA012; QEFA013; QEFA017; QEFA020. QEFA015 | Age > 18 Invasive non-metastatic breast carcinoma operated on and having had additional treatment | History of contralateral breast cancer Cancer at another location during the year | SNDS | [30,32,33,34,35] |
| Proportion of neoadjuvant chemotherapy | Care process Treatment | Number of women receiving intravenous chemotherapy before surgery for invasive breast cancer | Number of women diagnosed with invasive non-metastatic breast cancer | Age > 18 Invasive non-metastatic breast carcinoma | History of breast cancer Cancer at another location during the year | SNDS | [32] |
| Time between biopsy and first surgery (excluding neoadjuvant chemotherapy) | Care process Therapeutic delay | Number of women who had surgery within 4 weeks or less of the date of the pathological report | Number of women who had a mammogram followed by a diagnosis of invasive non-metastatic breast cancer treated by primary surgery (no neoadjuvant chemotherapy or hormone therapy) during the given period | Age > 18 Invasive non-metastatic breast carcinoma | Neoadjuvant chemotherapy or hormone therapy Cancer at another location during the year | SNDS | [21,30] |
| Proportion of women for whom the time between the end of adjuvant chemotherapy and the start of radiotherapy was less than 6 weeks | Care process Therapeutic delay | Number of women with invasive non-metastatic breast carcinoma who had radiotherapy within 6 weeks of completing adjuvant chemotherapy | Number of women with invasive non-metastatic breast carcinoma who have had chemotherapy followed by radiotherapy | Age > 18 Invasive non-metastatic breast carcinoma Have had adjuvant chemotherapy Have had radiotherapy after adjuvant chemotherapy | History of contralateral breast cancer Cancer at another location during the year Surgical revision (mastectomy or axillary dissection) between chemotherapy and radiotherapy | SNDS | [30] |
| Proportion of women with a delay between the initial biopsy and the first surgery of less than 3 months | Care process Therapeutic delay | Number of women a delay between the initial biopsy with a diagnosis of cancer and surgery below 3 months | Number of women with invasive non-metastatic breast carcinoma treated with upfront surgery | Age > 18 Invasive non-metastatic breast carcinoma with upfront surgery | Cancer at another location during the year | EHR SNDS | [21,31] |
| Proportion of women who received radiotherapy after breast-conserving surgery for ductal carcinoma in situ or invasive non-metastatic breast cancer | Care process Treatment | Number of women with ductal carcinoma in situ or invasive non-metastatic breast cancer who had radiotherapy after conservative surgery | Number of women with ductal carcinoma in situ or invasive non-metastatic breast cancer who have undergone conservative surgery | Age > 18 Ductal carcinoma in situ or invasive non-metastatic breast cancer | History of contralateral breast cancer Cancer at another location during the year | SNDS | [30] |
| Number of consultations with a psychologist or psychiatrist | Care process Treatment | Number of consultations with a psychologist or psychiatrist (SF-12 mental, HAD, EORTC) | Number of women with ductal carcinoma in situ or invasive non-metastatic breast cancer | Age > 18, justifying psychological, psychiatric, or psychiatric care | _ | EHR | Added by the bibliographic panel |
| Number of new files presented to specialist MTDMs | Care process Diagnosis | Number of new files presented to specialist MTDMs | Number of women diagnosed with breast cancer | All new patients presented to specialist MTDMs for breast cancer | _ | EHR | Added by the bibliographic panel |
| Indicator Title | Type of Indicator | Numerator | Denominator | Inclusion Criteria | Exclusion Criteria | Data Sources | Bibliographic References |
|---|---|---|---|---|---|---|---|
| Proportion of patients diagnosed with hepatocellular carcinoma (HCC) who received curative treatment | Care process Treatment | Number of patients with HCC receiving curative treatment (resection/local ablation/liver transplantation, LT) | Total number of patients with HCC | All new HCC + resection/local ablation/LT within 1 year | _ | SNDS (MID) Health data warehouse (HDW) | [36,37,38,39] |
| Proportion of patients on the HCC transplant waiting list eligible for waiting treatment and treated during the waiting phase | Care process Treatment | Number of patients on the transplant waiting list for active HCC with treatment on hold | Number of patients on the transplant waiting list with active HCC and preserved liver function | Patient on the transplant waiting list with active HCC | Registration with a “non-treatable HCC” component | ABM, excluding an untreatable HCC component | [36,37,38,39] |
| Proportion of patients receiving post-treatment monitoring after resection or TPC | Care process Treatment | Number of patients with cross-sectional abdominal imaging/3 months within 2 years of resection/local ablation | Number of patients treated by resection/local ablation/ transplant | Patient treated by resection/local ablation/ transplant | _ | EHR | [36,40] |
| Perioperative mortality (90 days) after liver resection in cirrhotic patients | Quality impact | Number of deaths within 90 days of HCC resection | Number of resections for HCC | All new HCC + surgical resection | _ | SNDS | [39] |
| Perioperative mortality (90 days) after liver transplantation for HCC | Quality impact | Number of deaths within 90 days of liver transplantation for HCC | Number of transplants for HCC | Liver transplant for HCC | _ | SNDS | [39] |
| Number of new HCC files presented to specialist liver MDTMs | Care process Diagnosis | Number of new HCC files presented to specialist liver MDTMs | Number of patients diagnosed with HCC | All new HCC presented to the liver specialist MDTMs | _ | EHR | [41] |
| Time between first diagnostic imaging and MDTM presentation | Care process Diagnosis | Time between the first imaging describing a liver nodule and the date of the first MDTM presentation | Number of patients with a first imaging exam describing a liver nodule who were subsequently presented at an MDTM during the given period | All new HCC presented to the liver specialist MDTMs | _ | EHR | [42] |
| Time between first MDTMs and first treatment | Care process Therapeutic delay | Time between the first presentation at MDTMs and the first treatment | Number of patients who were presented at an MDTM and subsequently received a first treatment during the given period | All new HCC presented to the liver specialist MDTMs | _ | EHR | [42] |
| Percentage of patients with histological evidence of HCC | Care process Diagnosis | Percentage of patients with histological confirmation of HCC | Total number of patients diagnosed with HCC | All new HCC presented to the liver specialist MDTMs | _ | DPI | [42] |
| Proportion of patients on the list for HCC transplants | Care process Treatment | Number of patients transplanted for HCC | Number of patients on the list for HCC | Patient on the list for HCC | MELD > 20 | ABM | [36,37,38,39] |
| Number of consultations with a psychologist or psychiatrist | Care process Treatment | Number of consultations with a psychologist or psychiatrist (SF-12 mental, HAD, EORTC) | Number of patients treated for HCC | Age > 18, justifying psychological, psychiatric, or psychiatric care | _ | EHR | Added by the bibliographic panel |
| Indicator Title | Type of Indicator | Numerator | Demoninator | Inclusion Criteria | Exclusion Criteria | Data Sources | Bibliographic References |
|---|---|---|---|---|---|---|---|
| Time between the date of surgery and the date of the first radiotherapy session | Care process Therapeutic delay | Time between surgery and adjuvant radiotherapy | Number of patients with gynecological cancer who underwent surgery and received adjuvant radiotherapy during the given period | Woman with gynecological cancer (excluding ovarian cancer) | _ | SNDS | [43] |
| Annual percentage of women treated with radiotherapy or radiochemotherapy as first-line treatment for cervical cancer | Care process Treatment | Annual number of women with cervical cancer receiving radiotherapy or radiochemotherapy | Annual number of women diagnosed with cervical cancer | Woman with with cervical cancer in the first-line treatment | _ | SNDS | [44] |
| Time between first consultation and date of biopsy | Care process Diagnosis | Time between first consultation and date of biopsy | Number of women diagnosed with gynecological cancer during the given period | Age > 18, requiring diagnostic biopsy | Biopsy available at the first consultation | EHR | Added by the expert panel. |
| Time between diagnosis and surgery for cervical cancer | Care process Therapeutic delay | Time between diagnosis and surgery | Number of women diagnosed with cervical cancer and treated with upfront surgery during the given period | Hysterectomy or trachelectomy for stage Ia-IIa cervical cancer | Pre-cancerous cells Surgery other than hysterectomy or trachelectomy | EHR SNDS | [45,46] |
| Percentage of patients for whom surgery is indicated who have received neoadjuvant treatment | Care process Treatment | Number of patients receiving neoadjuvant treatment (radiotherapy, chemotherapy, hormone therapy) | Number of patients with a surgical indication during the given period | Woman with gynecological cancer (excluding ovarian cancer) | Patient with no indication for surgery | EHR | [47] |
| Time between the first symptom reported by the patient and the first consultation | Care process Diagnosis | Time between first symptom and first consultation in gynecology | Number of women diagnosed with gynecologic cancer and with at least one reported symptom at the time of diagnosis during the given period | Woman with gynecological cancer (excluding ovarian cancer) | _ | EHR | Added by the expert panel. |
| Number of new files presented to specialist MDTMs | Care process Diagnosis | Number of new files presented to specialist MDTMs | Number of newly diagnosed cancer patients | All new women presented to specialist MDTMs | _ | EHR | [48] |
| Number of consultations with a psychologist or psychiatrist | Care process Treatment | Number of consultations with a psychologist or psychiatrist (SF-12 mental, HAD, EORTC) | Number of patients treated for cancer | Age > 18, justifying psychological, psychiatric, or psychiatric care | _ | EHR | [48] |
| Indicator Title | Type of Indicator | Numerator | Denominator | Inclusion Criteria | Exclusion Criteria | Data Sources | Bibliographic References |
|---|---|---|---|---|---|---|---|
| Time between consultation for curative indication and CRS +/− HIPEC | Care process Therapeutic delay | Time between consultation for curative indication and CRS ± HIPEC | Number of patients who had a consultation for curative intent and underwent CRS ± HIPEC during the given period | Age > 18 Resectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | EHR SNDS | Added by the bibliographic panel. |
| Time between MDTM decision and CRS +/− HIPEC | Care process Therapeutic delay | Time between MDTM decision and CRS ± HIPEC | Number of patients for whom CRS ± HIPEC was decided at an MDTM and performed during the given period | Age > 18 Resectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | EHR SNDS | Added by the bibliographic panel. |
| Time without treatment (chemotherapy or CRS +/− HIPEC) | Care process Therapeutic delay | Time without treatment (chemotherapy or CRS +/− HIPEC) | Number of patients who had a documented treatment interruption or treatment delay during the given period | Age > 18 Resectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | EHR SNDS | Added by the bibliographic panel. |
| Proportion of interventions (CRS +/− HIPEC) postponed | Care process Treatment | Number of patients operated on | Total number of patients planned for CRS +/− HIPEC | Age > 18 Resectable peritoneal carcinosis of digestive or gynecological origin with CRS +/− HIPEC postponed | Age < 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | EHR SNDS | Added by the bibliographic panel. |
| Proportion of conversions to non-resectability | Care process Treatment | Number of exploratory laparotomies without CRS +/− HIPEC | Total number of patients planned for CRS +/− HIPEC | Age > 18 Peritoneal carcinosis of digestive or gynecological origin, which has become unresectable due to waiting times | Age < 18 Resectable peritoneal carcinosis of digestive or gynecological origin | EHR | [49,50] |
| Proportion of patients progressing after deferral or cancellation (morphological assessment/markers) | Quality impact | Number of patients with clinical, biological, or morphological progression | Total number of patients planned for CRS +/− HIPEC | Age > 18 Peritoneal carcinosis of digestive or gynecological origin with clinical, biological, or morphological progression due to waiting time | Age < 18 | EHR | [51,52] |
| Total duration of chemotherapy (weeks) or number of cycles of chemotherapy | Care process Treatment | Number of chemotherapy cycles administered per patient | Number of patients who received chemotherapy during the given period | Age > 18 Resectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | SNDS | [53] |
| Rate of additional cycles of chemotherapy compared with the initial number | Care process Treatment | Number of additional chemotherapies | Number of chemotherapy treatments initially planned | Age > 18 Resectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | EHR SNDS | Added by the bibliographic panel. |
| Proportion of patients cancelled on the same day | Care process Treatment | Number of patients cancelled on the same day | Number of chemotherapy treatments initially planned | Age > 18 Resectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | EHR | [54,55] |
| Proportion of patients with shortened prehabilitation (<3 weeks) | Care process Treatment | Number of patients planned for CRS +/− HIPEC with prehabilitation < 3 weeks | Number of chemotherapy treatments initially planned | Age > 18 Resectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | EHR | [50] |
| Morbidity–mortality rate within 30 days of surgery after CRS +/− HIPEC | Quality impact | Number of patients who experienced severe post-operative complications or died within 30 days after CRS ± HIPEC | Number of patients who underwent CRS ± HIPEC during the given period | Age > 18 Resectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | SNDS | [56] |
| Time between consultation for indication of PIPAC and first PIPAC | Care process Therapeutic delay | Time between consultation for indication of PIPAC and first PIPAC | Number of patients for whom PIPAC was indicated and performed during the given period | Age > 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Resectable peritoneal carcinosis of digestive or gynecological origin | EHR SNDS | Added by the bibliographic panel. |
| Time between MDTM decision (indication given) and first PIPAC | Care process Therapeutic delay | Time between MDTM decision (indication given) and first PIPAC | Number of patients for whom a PIPAC was indicated in an MDTM and performed during the given period | Age > 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Resectable peritoneal carcinosis of digestive or gynecological origin | EHR SNDS | Added by the bibliographic panel. |
| Time without active treatment (chemotherapy or surgery) during the therapeutic pathway | Care process Therapeutic delay | Time without active treatment (chemotherapy or surgery) during the therapeutic pathway | Number of patients treated during the given period | Age > 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Resectable peritoneal carcinosis of digestive or gynecological origin | EHR | [53] |
| Proportion of interventions (PIPACs) reported | Care process Treatment | Actual number of patients operated on | Total number of patients included in the PIPAC pathway | Age > 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Resectable peritoneal carcinosis of digestive or gynecological origin | EHR | Added by the bibliographic panel. |
| Proportion of patients treated with PIPAC alone | Care process Treatment | Number of patients treated by PIPAC alone | Total number of patients included in the PIPAC pathway | Age > 18 Unresectable peritoneal carcinosis of digestive or gynecological origin | Age < 18 Resectable peritoneal carcinosis of digestive or gynecological origin | SNDS | Added by the bibliographic panel. |
| Number of new files presented to specialist MDTMs | Care process Diagnosis | Number of new files presented to specialist MDTMs | Number of new patients diagnosed | All new patients presented to specialist MDTMs | _ | EHR | [48] |
| Number of consultations with a psychologist or psychiatrist | Care process Treatment | Number of consultations with a psychologist or psychiatrist (SF-12 mental, HAD, EORTC) | Number of patients treated for cancer | Age > 18, justifying psychological, psychiatric, or psychiatric care | _ | EHR | [48,50] |
References
- Milon, A.; Deroche, C.; Jomier, B.; Vermeillet, S. Santé Publique: Pour un Nouveau Eépart–Leçons de L’épidémie de COVID-19; Sénat: Paris, France, 2020; Rapport d’information No. 199 (2020–2021); Available online: https://www.senat.fr/rap/r20-199-1/r20-199-110.html#toc645 (accessed on 25 December 2023).
- French National Cancer Institute. Préconisations Pour L’adaptation de L’offre de Soins des Établissements Accueillant les Patients Atteints de Cancer Dans le Contexte de L’épidémie de COVID-19; Réseau de Prévention des Infections Associées aux Soins (REPIAS): Saint-Maurice, France, 2020; Available online: https://www.preventioninfection.fr/document/preconisations-pour-ladaptation-de-loffre-de-soins-des-etablissements-accueillant-les-patients-atteints-de-cancer-dans-le-contexte-de-lepidemie-de-covid-19/ (accessed on 25 December 2023).
- You, B.; Ravaud, A.; Canivet, A.; Ganem, G.; Giraud, P.; Guimbaud, R.; Kaluzinski, L.; Krakowski, I.; Mayeur, D.; Grellety, T.; et al. The official French guidelines to protect patients with cancer against SARS-CoV-2 infection. Lancet Oncol. 2020, 21, 619–621. [Google Scholar] [CrossRef] [PubMed]
- Worthington, J.; van Wifferen, F.; Sun, Z.; de Jonge, L.; Lew, J.-B.; Greuter, M.J.; Puttelaar, R.v.D.; Feletto, E.; Lansdorp-Vogelaar, I.; Coupé, V.M.; et al. Potential global loss of life expected due to COVID-19 disruptions to organised colorectal cancer screening. eClinicalMedicine 2023, 62, 102081. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative. Effect of COVID-19 pandemic lockdowns on planned cancer surgery for 15 tumour types in 61 countries: An international, prospective, cohort study. Lancet Oncol. 2021, 22, 1507–1517. [Google Scholar] [CrossRef]
- De Vincentiis, L.; Carr, R.A.; Mariani, M.P.; Ferrara, G. Cancer diagnostic rates during the 2020 ‘lockdown’, due to COVID-19 pandemic, compared with the 2018–2019: An audit study from cellular pathology. J. Clin. Pathol. 2021, 74, 187–189. [Google Scholar] [CrossRef]
- Le Bihan-Benjamin, C.; Rocchi, M.; Putton, M.; Méric, J.-B.; Bousquet, P.J. Estimation of Oncologic Surgery Case Volume Before and After the COVID-19 Pandemic in France. JAMA Netw. Open 2023, 6, e2253204. [Google Scholar] [CrossRef]
- Walker, M.J.; Wang, J.; Mazuryk, J.; Skinner, S.-M.; Meggetto, O.; Ashu, E.; Habbous, S.; Rad, N.N.; Espino-Hernández, G.; Wood, R.; et al. Delivery of Cancer Care in Ontario, Canada, During the First Year of the COVID-19 Pandemic. JAMA Netw. Open 2022, 5, e228855. [Google Scholar] [CrossRef]
- Belmont, A.-S.; Sajous, C.; Bruyas, A.; Calattini, S.; Cartalat, S.; Chauvenet, M.; Colombel, M.; Dalle, S.; Dagonneau, T.; Darrason, M.; et al. Impact of the First Wave of the COVID-19 Pandemic on the Lyon University Hospital Cancer Institute (IC-HCL). Cancers 2021, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, C.L.B.; Simonnet, J.-A.; Rocchi, M.; Khati, I.; Ménard, E.; Houas-Bernat, E.; Méric, J.-B.; Bousquet, P.-J. Monitoring the impact of COVID-19 in France on cancer care: A differentiated impact. Sci. Rep. 2022, 12, 4207. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, M.A.; Koul, S.; Olivecrona, G.K.; Götberg, M.; Tydén, P.; Rydberg, E.; Scherstén, F.; Alfredsson, J.; Vasko, P.; Omerovic, E.; et al. Incidence and outcome of myocardial infarction treated with percutaneous coronary intervention during COVID-19 pandemic. Heart 2020, 106, 1812–1818. [Google Scholar] [CrossRef]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Bray, M.; Hollings, S.; Roebuck, C.; Gale, C.P.; A Mamas, M.; et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Carinci, F.; Van Gool, K.; Mainz, J.; Veillard, J.; Pichora, E.C.; Januel, J.M.; Arispe, I.; Kim, S.M.; Klazinga, N.; Haelterman, M.; et al. Towards actionable international comparisons of health system performance: Expert revision of the OECD framework and quality indicators. Int. J. Qual. Health Care 2015, 27, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; McCartney, A.; Ponti, A.; Marotti, L.; Vrieling, C.; Eniu, A.; Sousa, B.; Ripamonti, C.; Travado, L.; Spitz, S.; et al. European Society of Breast Cancer Specialists/Advanced Breast Cancer Global Alliance quality indicators for metastatic breast cancer care. Eur. J. Cancer 2023, 187, 105–113. [Google Scholar] [CrossRef] [PubMed]
- La Torre, G.; Mannocci, A.; Cocchiara, R.A.; D’Egidio, V.; Sestili, C.; Lia, L.; Cianfanelli, S.; Backhaus, I.; Dorelli, B.; Ricciardi, M. Systematic Review of the Quality Indicators (Qis) to Evaluate the CCCN Approach in the Management of Oncologic Patients. 2019. Available online: https://www.ipaac.eu/res/file/outputs/wp10/quality-indicators-systematic-review-evaluation-comprehensive-cancer-care-network.pdf (accessed on 16 April 2025).
- Linck, P.-A.; Garnier, C.; Depetiteville, M.-P.; MacGrogan, G.; Mathoulin-Pélissier, S.; Quénel-Tueux, N.; Charitansky, H.; Boisserie-Lacroix, M.; Chamming’s, F. Impact of the COVID-19 lockdown in France on the diagnosis and staging of breast cancers in a tertiary cancer centre. Eur. Radiol. 2021, 32, 1644–1651. [Google Scholar] [CrossRef]
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S.; Adeyi, O.; Barker, P.; Daelmans, B.; Doubova, S.V.; et al. High-Quality Health Systems in the Sustainable Development Goals Era: Time for a Revolution. Lancet Glob. Health 2018, 6, e1196–e1252. [Google Scholar] [CrossRef]
- Carvalho, A.S.; Fernandes, Ó.B.; de Lange, M.; Lingsma, H.; Klazinga, N.; Kringos, D. Changes in the quality of cancer care as assessed through performance indicators during the first wave of the COVID-19 pandemic in 2020: A scoping review. BMC Health Serv. Res. 2022, 22, 786. [Google Scholar] [CrossRef] [PubMed]
- Dudley, L.; Mamdoo, P.; Naidoo, S.; Muzigaba, M. Towards a harmonised framework for developing quality of care indicators for global health: A scoping review of existing conceptual and methodological practices. BMJ Health Care Inform. 2022, 29, e100469. [Google Scholar] [CrossRef]
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D.; Burnand, B.; LaCalle, J.R.; Lazaro, P.; van het Loo, M.; McDonnell, J.; Vader, J.; Kahan, J.P. The RAND/UCLA Appropriateness Method User’s Manual; RAND Corporation: Santa Monica, CA, USA, 2001. [Google Scholar]
- Biganzoli, L.; Marotti, L.; Hart, C.D.; Cataliotti, L.; Cutuli, B.; Kühn, T.; Mansel, R.E.; Ponti, A.; Poortmans, P.; Regitnig, P.; et al. Quality indicators in breast cancer care: An update from the EUSOMA working group. Eur. J. Cancer 2017, 86, 59–81. [Google Scholar] [CrossRef]
- Maes-Carballo, M.; Gómez-Fandiño, Y.; Hermida, A.R.; Estrada-López, C.R.; Martín-Díaz, M.; Khan, K.S.; Bueno-Cavanillas, A. Quality indicators for breast cancer care: A systematic review. Breast 2021, 59, 221–231. [Google Scholar] [CrossRef]
- Houzard, S.; Courtois, E.; Benjamin, C.L.B.; Erbault, M.; Arnould, L.; Barranger, E.; Coussy, F.; Couturaud, B.; Cutuli, B.; de Cremoux, P.; et al. Monitoring Breast Cancer Care Quality at National and Local Level Using the French National Cancer Cohort. Clin. Breast Cancer 2022, 22, e832–e841. [Google Scholar] [CrossRef]
- French Health Ministry. National Health Strategy 2018–2022. Published 17 December 2017. Available online: https://sante.gouv.fr/systeme-de-sante/strategie-nationale-de-sante/article/la-strategie-nationale-de-sante-2018-2022 (accessed on 25 December 2023).
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef]
- Westby, M.D.; Marshall, D.; Jones, C. Development of quality indicators for hip and knee arthroplasty rehabilitation. Osteoarthr. Cartil. 2018, 26, 370–382. [Google Scholar] [CrossRef] [PubMed]
- Bombard, Y.; Baker, G.R.; Orlando, E.; Fancott, C.; Bhatia, P.; Casalino, S.; Onate, K.; Denis, J.-L.; Pomey, M.-P. Engaging Patients to Improve Quality of Care: A Systematic Review. Implement. Sci. 2018, 13, 98. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth Edition of the AJCC Cancer Staging Manual: Breast Cancer. Ann. Surg. Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Wiley Blackwell: Oxford, UK, 2017. [Google Scholar]
- Institut National du Cancer. Cancer du Sein: Indicateurs de Qualité et de Sécurité des Soins. Collection les Données [Internet]. 2019. Available online: https://www.e-cancer.fr/Expertises-et-publications/Catalogue-des-publications/Cancer-du-sein-indicateurs-de-qualite-et-de-securite-des-soins (accessed on 25 March 2025).
- Perry, N.; Broeders, M.; de Wolf, C. European guidelines for quality assurance in breast cancer screening and diagnosis. Fourth edition summary document. Ann. Oncol. 2008, 19, 614–622. [Google Scholar] [CrossRef]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef] [PubMed]
- Ferrua, M. Development and feasibility of a set of quality indicators relative to the timeliness and organisation of care for new breast cancer patients undergoing surgery. BMC Health Serv. Res. 2012, 12, 167. [Google Scholar] [CrossRef]
- Andreano, A.; Anghinoni, E.; Autelitano, M. Indicators based on registers and administrative data for breast cancer: Routine evaluation of oncologic care pathway can be implemented. J. Eval. Clin. Pract. 2016, 22, 62–70. [Google Scholar] [CrossRef]
- Bleicher, R.J. Timing and Delays in Breast Cancer Evaluation and Treatment. Ann. Surg. Oncol. 2018, 25, 2829–2838. [Google Scholar] [CrossRef]
- Blanc, J.; Barbare, J.C.; Baumann, A.S. «Carcinome hépatocellulaire». [Internet]. Thésaurus National de Cancérologie Digestive. 2019. Available online: http://www.tncd.org (accessed on 25 March 2025).
- Inca HAS. Guide–Affection de Longue Durée. ALD 30-Tumeur Maligne, Affection Maligne du Tissu Lymphatique ou Hématopoïétique. Cancer Primitif du Foie. 2010. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2010-02/ald_30_lap_ksein_vd.pdf (accessed on 25 March 2025).
- Dhanasekaran, R.; Talwalkar, J.A. Quality of Cancer Care in Patients with Cirrhosis and Hepatocellular Carcinoma. Curr. Gastroenterol. Rep. 2015, 17, 34. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Berenguer, M.; Burra, P.; Ghobrial, M. Posttransplant Management of Recipients Undergoing Liver Transplantation for Hepatocellular Carcinoma. Working Group Report From the ILTS Transplant Oncology Consensus Conference. Transplantation 2020, 104, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Amaddeo, G.; Brustia, R.; Allaire, M. Impact of COVID-19 on the management of hepatocellular carcinoma in a high-prevalence area. JHEP Rep. 2021, 3, 100199. [Google Scholar] [CrossRef]
- Plan Cancer 2014–2019 [Internet]. p. 27. Available online: https://www.iccp-portal.org/sites/default/files/plans/Summary-plan-cancer-2014-2019-Anglais.pdf (accessed on 25 March 2025).
- Wang, Y.; Zhang, S.; Wei, L. Recommendations on management of gynecological malignancies during the COVID-19 pandemic: Perspectives from Chinese gynecological oncologists. J. Gynecol. Oncol. 2020, 31, e68. [Google Scholar] [CrossRef]
- Akladios, C.; Azais, H.; Ballester, M.; Bendifallah, S.; Bolze, P.A.; Bourdel, N.; Bricou, A.; Canlorbe, G.; Carcopino, X.; Chauvet, P.; et al. Recommendations for the surgical management of gynecological cancers during the COVID-19 pandemic-FRANCOGYN group for the CNGOF. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101729. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Novatt, H.; Matsuzaki, S.; Hom, M.S.; Castaneda, A.V.; Licon, E.; Nusbaum, D.J.; Roman, L.D. Wait-time for hysterectomy and survival of women with early-stage cervical cancer: A clinical implication during the coronavirus pandemic. Gynecol. Oncol. 2020, 158, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Lamblin, G.; Golfier, F.; Peron, J.; Moret, S.; Chene, G.; Nohuz, E.; Lebon, M.; Dubernard, G.; Cortet, M. Impact de la pandémie de COVID-19 sur les modifications thérapeutiques des patientes atteintes de cancers gynécologiques [Impact of the COVID-19 Outbreak on the management of patients with gynecological cancers]. Gynecol. Obstet. Fertil. Senol. 2020, 48, 777–783. [Google Scholar]
- Raymond, E.; Thieblemont, C.; Alran, S.; Faivre, S. Impact of the COVID-19 Outbreak on the Management of Patients with Cancer. Target. Oncol. 2020, 15, 249–259. [Google Scholar] [CrossRef]
- Fadavi, P.; Houshyari, M.; Yousefi Kashi, A.S.; Jarrahi, A.M.; Roshanmehr, F.; Broomand, M.A.; Sandoughdaran, S.; Taghizadeh-Hesary, F. Review on the Oncology Practice in the Midst of COVID-19 Crisis: The Challenges and Solutions. Asian Pac. J. Cancer Prev. 2021, 22, 19–24. [Google Scholar] [CrossRef]
- Birgisson, H.; Enblad, M.; Artursson, S.; Ghanipour, L.; Cashin, P.; Graf, W. Patients with colorectal peritoneal metastases and high peritoneal cancer index may benefit from cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Eur. J. Surg. Oncol. 2020, 46, 2283–2291. [Google Scholar] [CrossRef]
- Fotopoulou, C.; Concin, N.; Planchamp, F.; Morice, P.; Vergote, I.; du Bois, A.; Querleu, D. Quality indicators for advanced ovarian cancer surgery from the European Society of Gynaecological Oncology (ESGO): 2020 update. Int. J. Gynecol. Cancer 2020, 30, 436–440. [Google Scholar] [CrossRef]
- Glehen, O.; Kepenekian, V.; Bouché, O.; Gladieff, L.; Honore, C.; RENAPE-BIG-RENAPE. Treatment of primary and metastatic peritoneal tumors in the COVID-19 pandemic. Proposals for prioritization from the RENAPE and BIG-RENAPE groups. J. Visc. Surg. 2020, 157, S25–S31. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, C.D.; Tran Cao, H.S.; Roland, C.L.; Teshome, M.; Bednarski, B.K.; Ikoma, N.; Graham, P.H.; Keung, E.Z.; Scally, C.P.; Katz, M.H.G.; et al. Surgical decision-making and prioritization for cancer patients at the onset of the COVID-19 pandemic: A multidisciplinary approach. Surg. Oncol. 2020, 34, 182–185. [Google Scholar] [CrossRef]
- Cavaliere, D.; Parini, D.; Marano, L.; Cipriani, F.; Di Marzo, F.; Macrì, A.; D’Ugo, D.; Roviello, F.; Gronchi, A.; SICO (Italian Society of Surgical Oncology). Surgical management of oncologic patient during and after the COVID-19 outbreak: Practical recommendations from the Italian society of Surgical Oncology. Updates Surg. 2021, 73, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Classe, J.M.; Dolivet, G.; Evrard, S.; Ferron, G.; Lécuru, F.; Leufflen, L.; Rivoire, M.; Sgarbura, O. Recommandations de la Société française de chirurgie oncologique (SFCO) pour l’organisation de la chirurgie oncologique durant l’épidémie de COVID-19 [French Society for Surgical Oncology (SFCO) guidelines for the management of surgical oncology in the pandemic context of COVID 19]. Bull. Cancer 2020, 107, 524–527. [Google Scholar] [PubMed]
- Shariff, F.; Bischof, D.; Govindarajan, A.; Prince, R.; Burkes, R.; Haase, E.; Mack, L.; Temple, W.; Hebbard, P.; Boulanger-Gobeil, C.; et al. Evidence-Based Strategies for the Treatment of Peritoneal Malignancies during Health Care Resource Restriction: The COVID-19 Pandemic. Curr. Oncol. 2020, 28, 40–51. [Google Scholar] [CrossRef]
- Alyami, M.; Kim, B.J.; Villeneuve, L.; Vaudoyer, D.; Képénékian, V.; Bakrin, N.; Gilly, F.N.; Cotte, E.; Glehen, O.; Passot, G. Ninety-day post-operative morbidity and mortality using the National Cancer Institute’s common terminology criteria for adverse events better describe post-operative outcome after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Int. J. Hyperth. 2018, 34, 532–537. [Google Scholar] [CrossRef]
| Breast Cancer | Hepatocellular Carcinomatosis | Gynecologic Cancer | Peritoneal Carcinomatosis | |
|---|---|---|---|---|
| Bibliographic panel composition | Medical oncologist, n = 1 Surgeons, n = 2 | Gastroenterologist, n = 3 | Medical oncologist, n = 1 Surgeons, n = 2 | Surgeons, n = 2 |
| Years of experience <10, n = 3 10–20, n = 0 >20, n = 0 | Years of experience <10, n = 2 10–20, n = 1 >20, n = 0 | Years of experience <10, n = 2 10–20, n = 1 >20, n = 0 | Years of experience <10, n = 1 10–20, n = 0 >20, n = 1 | |
| Expert panel composition | Medical oncologist, n = 2 Surgeons, n = 3 Radiation therapist, n = 1 | Medical oncologist, n = 1 Gastroenterologist, n = 6 | Medical oncologist, n = 1 Surgeons, n = 3 Radiation therapist, n = 2 | Surgeons, n = 5 |
| Years of experience <10, n = 0 10–20, n = 3 >20, n = 3 | Years of experience <10, n = 0 10–20, n = 1 >20, n = 6 | Years of experience <10, n = 1 10–20, n = 2 >20, n = 3 | Years of experience <10, n = 1 10–20, n = 2 >20, n = 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piazzon, N.; Haesebaert, J.; Michel, P.; Belmont, A.S.; Kepenekian, V.; Lamblin, G.; Costentin, C.; Péron, J. Developing Cancer Quality of Care Indicators to Quantify the Impact of a Global Destabilization of the Care System (COLLAT-COVID). Cancers 2025, 17, 1680. https://doi.org/10.3390/cancers17101680
Piazzon N, Haesebaert J, Michel P, Belmont AS, Kepenekian V, Lamblin G, Costentin C, Péron J. Developing Cancer Quality of Care Indicators to Quantify the Impact of a Global Destabilization of the Care System (COLLAT-COVID). Cancers. 2025; 17(10):1680. https://doi.org/10.3390/cancers17101680
Chicago/Turabian StylePiazzon, Nathalie, Julie Haesebaert, Philippe Michel, Anne Sophie Belmont, Vahan Kepenekian, Gery Lamblin, Charlotte Costentin, and Julien Péron. 2025. "Developing Cancer Quality of Care Indicators to Quantify the Impact of a Global Destabilization of the Care System (COLLAT-COVID)" Cancers 17, no. 10: 1680. https://doi.org/10.3390/cancers17101680
APA StylePiazzon, N., Haesebaert, J., Michel, P., Belmont, A. S., Kepenekian, V., Lamblin, G., Costentin, C., & Péron, J. (2025). Developing Cancer Quality of Care Indicators to Quantify the Impact of a Global Destabilization of the Care System (COLLAT-COVID). Cancers, 17(10), 1680. https://doi.org/10.3390/cancers17101680