
Safety of the Breast Cancer Adjuvant Radiotherapy in Ataxia–Telangiectasia Mutated Variant Carriers
 , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. ATM Variants Identification and Classification
2.3. Radiation Therapy Treatment Characteristics and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Characteristics of Genetic Variants
3.3. Treatment Details
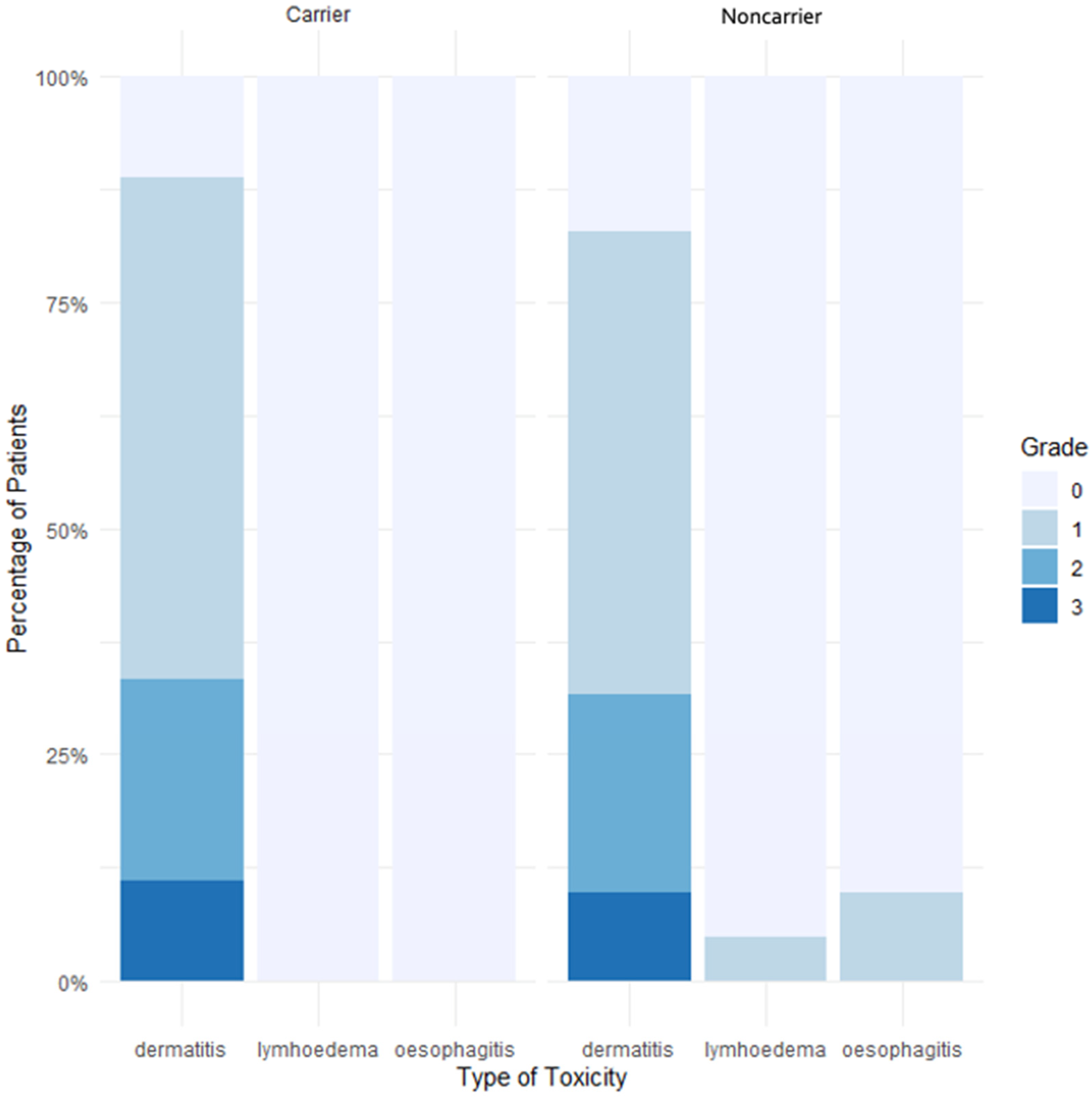
3.4. Acute Toxicities
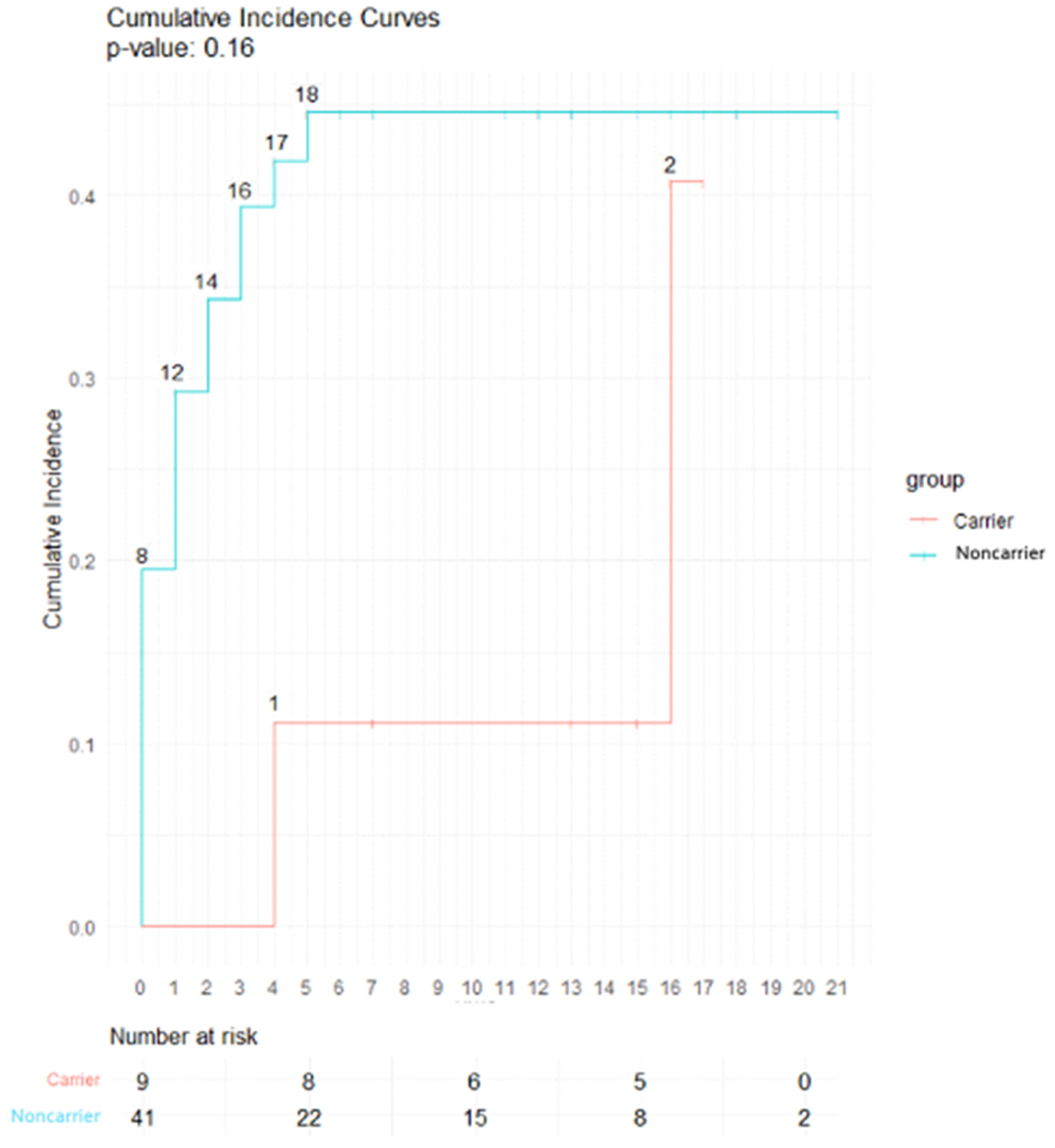
3.5. Late Toxicities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer Statistics for the Year 2020: An Overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Coates, A.S.; Winer, E.P.; Goldhirsch, A.; Gelber, R.D.; Gnant, M.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J.; André, F.; Baselga, J.; et al. Tailoring Therapies—Improving the Management of Early Breast Cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann. Oncol. 2015, 26, 1533–1546. [Google Scholar] [CrossRef] [PubMed]
- Effect of Radiotherapy after Breast-Conserving Surgery on 10-Year Recurrence and 15-Year Breast Cancer Death: Meta-Analysis of Individual Patient Data for 10 801 Women in 17 Randomised Trials. Lancet 2011, 378, 1707–1716. [CrossRef] [PubMed]
- Hamdan, D.; Nguyen, T.T.; Leboeuf, C.; Meles, S.; Janin, A.; Bousquet, G. Genomics Applied to the Treatment of Breast Cancer. Oncotarget 2019, 10, 4786–4801. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Paull, T.T. ATM Activation by DNA Double-Strand Breaks through the Mre11-Rad50-Nbs1 Complex. Science 2005, 308, 551–554. [Google Scholar] [CrossRef] [PubMed]
- Shiloh, Y. ATM and Related Protein Kinases: Safeguarding Genome Integrity. Nat. Rev. Cancer 2003, 3, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Rothblum-Oviatt, C.; Wright, J.; Lefton-Greif, M.A.; McGrath-Morrow, S.A.; Crawford, T.O.; Lederman, H.M. Ataxia Telangiectasia: A Review. Orphanet J. Rare Dis. 2016, 11, 159. [Google Scholar] [CrossRef] [PubMed]
- Hecht, F.; Hecht, B.K. Cancer in Ataxia-Telangiectasia Patients. Cancer Genet. Cytogenet. 1990, 46, 9–19. [Google Scholar] [CrossRef]
- Angèle, S.; Romestaing, P.; Moullan, N.; Vuillaume, M.; Chapot, B.; Friesen, M.; Jongmans, W.; Cox, D.G.; Pisani, P.; Gérard, J.-P.; et al. ATM Haplotypes and Cellular Response to DNA Damage: Association with Breast Cancer Risk and Clinical Radiosensitivity. Cancer Res. 2003, 63, 8717–8725. [Google Scholar]
- Thorstenson, Y.R.; Roxas, A.; Kroiss, R.; Jenkins, M.A.; Yu, K.M.; Bachrich, T.; Muhr, D.; Wayne, T.L.; Chu, G.; Davis, R.W.; et al. Contributions of ATM Mutations to Familial Breast and Ovarian Cancer. Cancer Res. 2003, 63, 3325–3333. [Google Scholar]
- Renwick, A.; Thompson, D.; Seal, S.; Kelly, P.; Chagtai, T.; Ahmed, M.; North, B.; Jayatilake, H.; Barfoot, R.; Spanova, K.; et al. ATM Mutations That Cause Ataxia-Telangiectasia Are Breast Cancer Susceptibility Alleles. Nat. Genet. 2006, 38, 873–875. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, J.; Birrell, G.; Lavin, M. Testing for Mutations of the Ataxia Telangiectasia Gene in Radiosensitive Breast Cancer Patients. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 1998, 47, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, S.; Arutyunyan, R.; Stumm, M.; Dörk, T.; Bendix, R.; Bremer, M.; Varon, R.; Sauer, R.; Gebhart, E. Radiosensitivity of Ataxia Telangiectasia and Nijmegen Breakage Syndrome Homozygotes and Heterozygotes as Determined by Three-Color FISH Chromosome Painting. Radiat. Res. 2002, 157, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Weil, M.M.; Kittrell, F.S.; Yu, Y.; McCarthy, M.; Zabriskie, R.C.; Ullrich, R.L. Radiation Induces Genomic Instability and Mammary Ductal Dysplasia in Atm Heterozygous Mice. Oncogene 2001, 20, 4409–4411. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhou, Q.; Howard, M.E.; Tu, X.; Zhu, Q.; Denbeigh, J.M.; Remmes, N.B.; Herman, M.G.; Beltran, C.J.; Yuan, J.; Greipp, P.T.; et al. Inhibition of ATM Induces Hypersensitivity to Proton Irradiation by Upregulating Toxic End Joining. Cancer Res. 2021, 81, 3333–3346. [Google Scholar] [CrossRef] [PubMed]
- McDuff, S.G.R.; Bellon, J.R.; Shannon, K.M.; Gadd, M.A.; Dunn, S.; Rosenstein, B.S.; Ho, A.Y. ATM Variants in Breast Cancer: Implications for Breast Radiation Therapy Treatment Recommendations. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 1373–1382. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Cui, J.; Tang, F.; Cong, X.; Han, F. Ataxia Telangiectasia-Mutated Gene Polymorphisms and Acute Normal Tissue Injuries in Cancer Patients after Radiation Therapy: A Systematic Review and Meta-Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 1090–1098. [Google Scholar] [CrossRef]
- Terrazzino, S.; Cargnin, S.; Deantonio, L.; Pisani, C.; Masini, L.; Canonico, P.L.; Genazzani, A.A.; Krengli, M. Impact of ATM Rs1801516 on Late Skin Reactions of Radiotherapy for Breast Cancer: Evidences from a Cohort Study and a Trial Sequential Meta-Analysis. PLoS ONE 2019, 14, e0225685. [Google Scholar] [CrossRef]
- Andreassen, C.N.; Overgaard, J.; Alsner, J.; Overgaard, M.; Herskind, C.; Cesaretti, J.A.; Atencio, D.P.; Green, S.; Formenti, S.C.; Stock, R.G.; et al. ATM Sequence Variants and Risk of Radiation-Induced Subcutaneous Fibrosis after Postmastectomy Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 776–783. [Google Scholar] [CrossRef]
- Bremer, M.; Klöpper, K.; Yamini, P.; Bendix-Waltes, R.; Dörk, T.; Karstens, J.H. Clinical Radiosensitivity in Breast Cancer Patients Carrying Pathogenic ATM Gene Mutations: No Observation of Increased Radiation-Induced Acute or Late Effects. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2003, 69, 155–160. [Google Scholar] [CrossRef]
- Iannuzzi, C.M.; Atencio, D.P.; Green, S.; Stock, R.G.; Rosenstein, B.S. ATM Mutations in Female Breast Cancer Patients Predict for an Increase in Radiation-Induced Late Effects. Int. J. Radiat. Oncol. Biol. Phys. 2002, 52, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.Y.; Fan, G.; Atencio, D.P.; Green, S.; Formenti, S.C.; Haffty, B.G.; Iyengar, P.; Bernstein, J.L.; Stock, R.G.; Cesaretti, J.A.; et al. Possession of ATM Sequence Variants as Predictor for Late Normal Tissue Responses in Breast Cancer Patients Treated with Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Sinilnikova, O.M.; Dondon, M.-G.; Eon-Marchais, S.; Damiola, F.; Barjhoux, L.; Marcou, M.; Verny-Pierre, C.; Sornin, V.; Toulemonde, L.; Beauvallet, J.; et al. GENESIS: A French National Resource to Study the Missing Heritability of Breast Cancer. BMC Cancer 2016, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Janin, N.; Andrieu, N.; Ossian, K.; Laugé, A.; Croquette, M.F.; Griscelli, C.; Debré, M.; Bressac-de-Paillerets, B.; Aurias, A.; Stoppa-Lyonnet, D. Breast Cancer Risk in Ataxia Telangiectasia (AT) Heterozygotes: Haplotype Study in French AT Families. Br. J. Cancer 1999, 80, 1042–1045. [Google Scholar] [CrossRef][Green Version]
- Girard, E.; Eon-Marchais, S.; Olaso, R.; Renault, A.-L.; Damiola, F.; Dondon, M.-G.; Barjhoux, L.; Goidin, D.; Meyer, V.; Le Gal, D.; et al. Familial Breast Cancer and DNA Repair Genes: Insights into Known and Novel Susceptibility Genes from the GENESIS Study, and Implications for Multigene Panel Testing. Int. J. Cancer 2019, 144, 1962–1974. [Google Scholar] [CrossRef] [PubMed]
- Kircher, M.; Witten, D.M.; Jain, P.; O’Roak, B.J.; Cooper, G.M.; Shendure, J. A General Framework for Estimating the Relative Pathogenicity of Human Genetic Variants. Nat. Genet. 2014, 46, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Rentzsch, P.; Witten, D.; Cooper, G.M.; Shendure, J.; Kircher, M. CADD: Predicting the Deleteriousness of Variants throughout the Human Genome. Nucleic Acids Res. 2019, 47, D886–D894. [Google Scholar] [CrossRef] [PubMed]
- Tavtigian, S.V.; Byrnes, G.B.; Goldgar, D.E.; Thomas, A. Classification of Rare Missense Substitutions, Using Risk Surfaces, with Genetic- and Molecular-Epidemiology Applications. Hum. Mutat. 2008, 29, 1342–1354. [Google Scholar] [CrossRef]
- Tavtigian, S.V.; Oefner, P.J.; Babikyan, D.; Hartmann, A.; Healey, S.; Le Calvez-Kelm, F.; Lesueur, F.; Byrnes, G.B.; Chuang, S.-C.; Forey, N.; et al. Rare, Evolutionarily Unlikely Missense Substitutions in ATM Confer Increased Risk of Breast Cancer. Am. J. Hum. Genet. 2009, 85, 427–446. [Google Scholar] [CrossRef]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. Using the Common Terminology Criteria for Adverse Events (CTCAE—Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. Actas Dermosifiliogr. 2021, 112, 90–92. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to Build a Bridge from a Population-Based to a More “Personalized” Approach to Cancer Staging. CA. Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.B.; Pilarski, R.; Berry, M.; Buys, S.S.; Farmer, M.; Friedman, S.; Garber, J.E.; Kauff, N.D.; Khan, S.; Klein, C.; et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Breast and Ovarian, Version 2.2017. J. Natl. Compr. Cancer Netw. JNCCN 2017, 15, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Lesueur, F.; Easton, D.F.; Renault, A.-L.; Tavtigian, S.V.; Bernstein, J.L.; Kote-Jarai, Z.; Eeles, R.A.; Plaseska-Karanfia, D.; Feliubadaló, L.; Spanish ATM Working Group; et al. First International Workshop of the ATM and Cancer Risk Group (4–5 December 2019). Fam. Cancer 2022, 21, 211–227. [Google Scholar] [CrossRef] [PubMed]
- Lesueur, F.; Eon-Marchais, S.; Bonnet-Boissinot, S.; Beauvallet, J.; Dondon, M.-G.; Golmard, L.; Rouleau, E.; Garrec, C.; Martinez, M.; Toulas, C.; et al. TUMOSPEC: A Nation-Wide Study of Hereditary Breast and Ovarian Cancer Families with a Predicted Pathogenic Variant Identified through Multigene Panel Testing. Cancers 2021, 13, 3659. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.M.; Eccles, D.M.; Romero, I.L.; Al-Mulla, F.; Balmaña, J.; Biancolella, M.; Bslok, R.; Caligo, M.A.; Calvello, M.; Capone, G.L.; et al. Genetic Testing and Clinical Management Practices for Variants in Non-BRCA1/2 Breast (and Breast/Ovarian) Cancer Susceptibility Genes: An International Survey by the Evidence-Based Network for the Interpretation of Germline Mutant Alleles (ENIGMA) Clinical Working Group. JCO Precis. Oncol. 2018, 2, PO.18.00091. [Google Scholar] [CrossRef]
- Porras, L.-M.; Padilla, N.; Moles-Fernández, A.; Feliubadaló, L.; Santamariña-Pena, M.; Sánchez, A.T.; López-Novo, A.; Blanco, A.; de la Hoya, M.; Molina, I.J.; et al. A New Set of in Silico Tools to Support the Interpretation of ATM Missense Variants Using Graphical Analysis. J. Mol. Diagn. JMD 2024, 26, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Abdulrahman, A.A.; Heintzelman, R.C.; Corbman, M.; Garcia, F.U. Invasive Breast Carcinomas with ATM Gene Variants of Uncertain Significance Share Distinct Histopathologic Features. Breast J. 2018, 24, 291–297. [Google Scholar] [CrossRef]
- Renault, A.-L.; Mebirouk, N.; Fuhrmann, L.; Bataillon, G.; Cavaciuti, E.; Le Gal, D.; Girard, E.; Popova, T.; La Rosa, P.; Beauvallet, J.; et al. Morphology and Genomic Hallmarks of Breast Tumours Developed by ATM Deleterious Variant Carriers. Breast Cancer Res. BCR 2018, 20, 28. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total Number n = 50 | Rare ATM Variant Carriers * n = 9 | Noncarriers n = 41 | p-Value |
|---|---|---|---|---|
| Median age at diagnosis (years, [median, range]) | 53 (35–77) | 52 (36–77) | 53 (35–75) | 0.48 |
| Mean follow up (years, range) | 13.1 (1.6–21.9) | 14.3 (7–18.2) | 12.9 (1.6–21.9) | 0.53 |
| BMI (kg/m2, [median, range]) | 24.6 (18.2–34.9) | 23.4 (18.2–28.9) | 22.9 (18.2–34.9) | 0.48 |
| Smoking status | ||||
| Ever (30%) | 15 | 2 | 13 | |
| Never (70%) | 35 | 7 | 28 | 0.87 |
| Histopathology (WHO classification) | ||||
| In situ carcinoma (4%) | 2 | 0 | 4 | |
| Invasive ductal carcinoma (82%) | 41 | 9 | 32 | |
| Invasive lobular carcinoma (14%) | 7 | 0 | 7 | 0.29 |
| Immunochemistry | ||||
| Grade | ||||
| 1 (26%) | 13 | 1 | 12 | |
| 2 (44%) | 22 | 5 | 17 | |
| 3 (26%) | 13 | 3 | 10 | |
| Unknown (4%) | 2 | 0 | 2 | 0.58 |
| Mitotic index (%) | ||||
| <4 (20%) | 10 | 2 | 8 | |
| 4–12 (44%) | 22 | 5 | 17 | |
| >12 (30%) | 15 | 2 | 13 | |
| Unknown (6%) | 3 | 0 | 3 | 0.65 |
| Embolus | ||||
| Yes (26%) | 13 | 4 | 9 | |
| No (68%) | 34 | 5 | 29 | |
| Unknown (6%) | 3 | 0 | 3 | 0.30 |
| ER expression | ||||
| Positive (80%) | 40 | 8 | 32 | |
| Negative (16%) | 8 | 1 | 7 | |
| Unknown (4%) | 2 | 0 | 2 | 0.70 |
| HER 2 expression | ||||
| 0 (40%) | 20 | 3 | 17 | |
| + (18%) | 9 | 2 | 7 | |
| ++ and FISH negative (6%) | 3 | 1 | 2 | |
| +++ (12%) | 6 | 1 | 5 | |
| Unknown (24%) | 12 | 2 | 10 | 0.70 |
| Clinical stage (AJCC 2017 v8) | ||||
| 0 (4%) | 2 | 0 | 2 | |
| I (40%) | 20 | 4 | 16 | |
| IIA (24%) | 12 | 1 | 11 | |
| IIB (20%) | 10 | 3 | 7 | |
| IIIA (6%) | 3 | 0 | 3 | |
| IIIB (2%) | 1 | 1 | 0 | |
| Unknown (4%) | 2 | 0 | 2 | 0.16 |
| Patient | Study | ATM Rare Variant | MAF in GnomAD a | In Silico Predictions | Our Classification for This Study | ClinVar Classification | Genotype for rs1801516 (c.5557G>A; p.Asp1853Asn) d | |
|---|---|---|---|---|---|---|---|---|
| CADD Phred Score b | Align-GVGD c | |||||||
| Pt 1 | GENESIS | c.8494C>T; p.Arg2832Cys | 0.0004 | 32 | C45 | PV | PV | GG |
| Pt 2 | CoF-AT2 | c.3894dupT; p.Ala1299CysfsX3 | 0.000007 | n/a | n/a | PV | PV | Unknown |
| Pt 3 | CoF-AT2 | c.5644C>T; p.Arg1882X | Not reported | 36 | n/a | PV | PV | Unknown |
| Pt 4 | GENESIS | c.4709T>C; p.Val1570Ala | 0.0007 | 17.66 | C0 | PPV | VUS | GG |
| Pt 5 | GENESIS | c.2T>G; p.Met1Arg (START loss) | Not reported | 23.4 | C65 | PPV | VUS | GG |
| Pt 6 | GENESIS | c.6059G>T; p.Gly2020Val | Not reported | 27.3 | C65 | PPV | VUS | GG |
| Pt 7 | GENESIS | c.4853G>A; p.Arg1618Gln | 0.00003 | 22.6 | C0 | PPV | VUS | GA |
| Pt 8 | GENESIS | c.6067G>A; p.Gly2023Arg | 0.0024 | 28.9 | C25 | PPV | VUS | GG |
| Pt 9 | GENESIS | c.1073A>G; p.Asn358Ser | 0.00001 | 14.04 | C0 | PPV | Benign | Unknown |
| Pt 10 | GENESIS | - | - | - | - | - | - | GA |
| Pt 11 | GENESIS | - | - | - | - | - | - | GA |
| Pt 12 | GENESIS | - | - | - | - | - | - | GA |
| Pt 13 | GENESIS | - | - | - | - | - | - | GA |
| Pt 14 | GENESIS | - | - | - | - | - | - | GA |
| Pt 15 | GENESIS | - | - | - | - | - | - | GA |
| Pt 16 | GENESIS | - | - | - | - | - | - | GA |
| Treatment Characteristics | Number of Treated Patients | % of Total | Rare ATM Variant Carriers | Noncarriers | p-Value |
|---|---|---|---|---|---|
| Type of surgery before RT | |||||
| Breast conserving | 40 | 80 | 6 | 34 | |
| Mastectomy | 10 | 20 | 3 | 7 | |
| Sentinel lymph node | 12 | 24 | 2 | 10 | |
| ALND | 34 | 68 | 6 | 28 | 0.51 |
| Chemotherapy | |||||
| NAC | 9 | 18 | 3 | 6 | 0.39 |
| Adjuvant chemotherapy | 18 | 36 | 4 | 14 | 0.84 |
| Targeted adjuvant therapy | 4 | 8 | 0 | 4 | 0.76 |
| Hormonotherapy | |||||
| AI | 10 | 20 | 0 | 10 | |
| Tamoxifen | 22 | 44 | 5 | 17 | 0.37 |
| Median duration of HT (years, range) | 5 (1–11) | NA | 5 (4–11) | 5 (1–10) | |
| Technique of radiation therapy | |||||
| 3D-CRT | 35 | 70 | 5 | 30 | |
| ILD | 15 | 30 | 4 | 11 | 0.52 |
| Mean dose of radiation therapy (Gy, range) | 56 (45–71) | NA | 57 (45–66) | 56 (45–71) | 0.64 |
| Mean RT duration (days, range) | 42.7 (28–81) | NA | 42 (32–52) | 43 (28–81) | 0.73 |
| Irradiated volume | |||||
| Only breast | 22 | 44 | 3 | 19 | |
| Breast and lymph nodes | 28 | 56 | 6 | 22 | |
| Associated boost | 22 | 44 | 4 | 18 | 0.73 |
| Number of Patients with Toxicities (%) | p-Value | |||||
|---|---|---|---|---|---|---|
| Acute toxicities | ||||||
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | |||
| Dermatitis | Noncarriers | 7 (14%) | 21(42%) | 9 (18%) | 4 (8%) | |
| Carriers | 1 (2%) | 5 (10%) | 2 (4%) | 1 (2%) | ||
| Total | 8 (16%) | 26 (52%) | 11 (22%) | 5 (10%) | 0.98 (Chi 2) | |
| Dysphagia | Noncarriers | 37 (74%) | 4 (8%) | 0 | 0 | |
| Carriers | 9 (18%) | 0 | 0 | 0 | ||
| Total | 46 (92%) | 4 (8%) | 0 | 0 | 1 (Chi 2) | |
| Lymphoedema | Noncarriers | 39 (78%) | 2 (4%) | 0 | 0 | |
| Carriers | 9 (18%) | 0 | 0 | 0 | ||
| Total | 48 (96%) | 2 (4%) | 0 | 0 | 1 (Chi 2) | |
| Late toxicities | ||||||
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | |||
| Subcutaneous fibrosis | Noncarriers | 23 (46%) | 16 (32%) | 2 (4%) | ||
| Carriers | 7 (14%) | 2 (4%) | 0 | |||
| Total | 30 (60%) | 18 (36%) | 2 (4%) | 0.16 (Gray) | ||
| Telangiectasia | Noncarriers | 37 (74%) | 4 (8%) | 0 | ||
| Carriers | 9 (18%) | 0 | 0 | |||
| Total | 46 (92%) | 4 (8%) | 0 | 0.33 (Gray) | ||
| Lymphoedema | Noncarriers | 38 (76%) | 0 | 3 (6%) | ||
| Carriers | 8 (16%) | 1 (2%) | 0 | |||
| Total | 46 (92%) | 1 (2%) | 3 (6%) | 0.72 (Gray) | ||
| Heart disease | Noncarriers | 40 (80%) | 1 (2%) | 0 | ||
| Carriers | 9 (18%) | 0 | 0 | |||
| Total | 49 (98%) | 1 (2%) | 0 | 1 (Gray) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bensenane, R.; Beddok, A.; Lesueur, F.; Fourquet, A.; Warcoin, M.; Le Mentec, M.; Cavaciuti, E.; Le Gal, D.; Eon-Marchais, S.; Andrieu, N.; et al. Safety of the Breast Cancer Adjuvant Radiotherapy in Ataxia–Telangiectasia Mutated Variant Carriers. Cancers 2024, 16, 1417. https://doi.org/10.3390/cancers16071417
Bensenane R, Beddok A, Lesueur F, Fourquet A, Warcoin M, Le Mentec M, Cavaciuti E, Le Gal D, Eon-Marchais S, Andrieu N, et al. Safety of the Breast Cancer Adjuvant Radiotherapy in Ataxia–Telangiectasia Mutated Variant Carriers. Cancers. 2024; 16(7):1417. https://doi.org/10.3390/cancers16071417
Chicago/Turabian StyleBensenane, Rayan, Arnaud Beddok, Fabienne Lesueur, Alain Fourquet, Mathilde Warcoin, Marine Le Mentec, Eve Cavaciuti, Dorothée Le Gal, Séverine Eon-Marchais, Nadine Andrieu, and et al. 2024. "Safety of the Breast Cancer Adjuvant Radiotherapy in Ataxia–Telangiectasia Mutated Variant Carriers" Cancers 16, no. 7: 1417. https://doi.org/10.3390/cancers16071417
APA StyleBensenane, R., Beddok, A., Lesueur, F., Fourquet, A., Warcoin, M., Le Mentec, M., Cavaciuti, E., Le Gal, D., Eon-Marchais, S., Andrieu, N., Stoppa-Lyonnet, D., & Kirova, Y. (2024). Safety of the Breast Cancer Adjuvant Radiotherapy in Ataxia–Telangiectasia Mutated Variant Carriers. Cancers, 16(7), 1417. https://doi.org/10.3390/cancers16071417