
Real-World Electronic Medical Records Data Identify Risk Factors for Myelofibrosis and Can Be Used to Validate Established Prognostic Scores


Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Source
2.2. Study Design
2.3. Statistical Analysis
3. Results
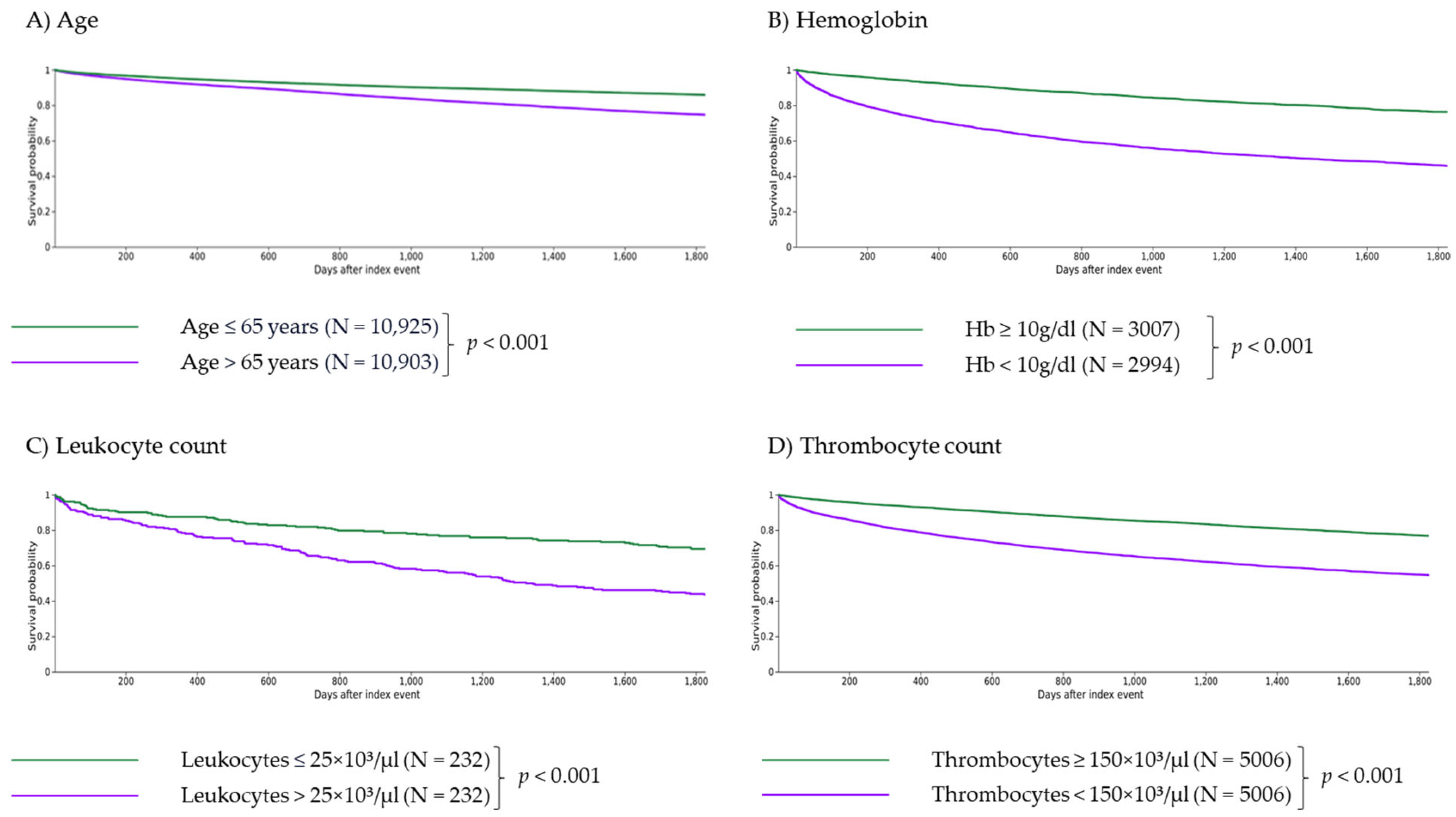
3.1. Independent Impact of Parameters
3.1.1. Impact of Age
3.1.2. Impact of Anemia
3.1.3. Impact of Leukocytosis
3.1.4. Impact of Thrombocytopenia
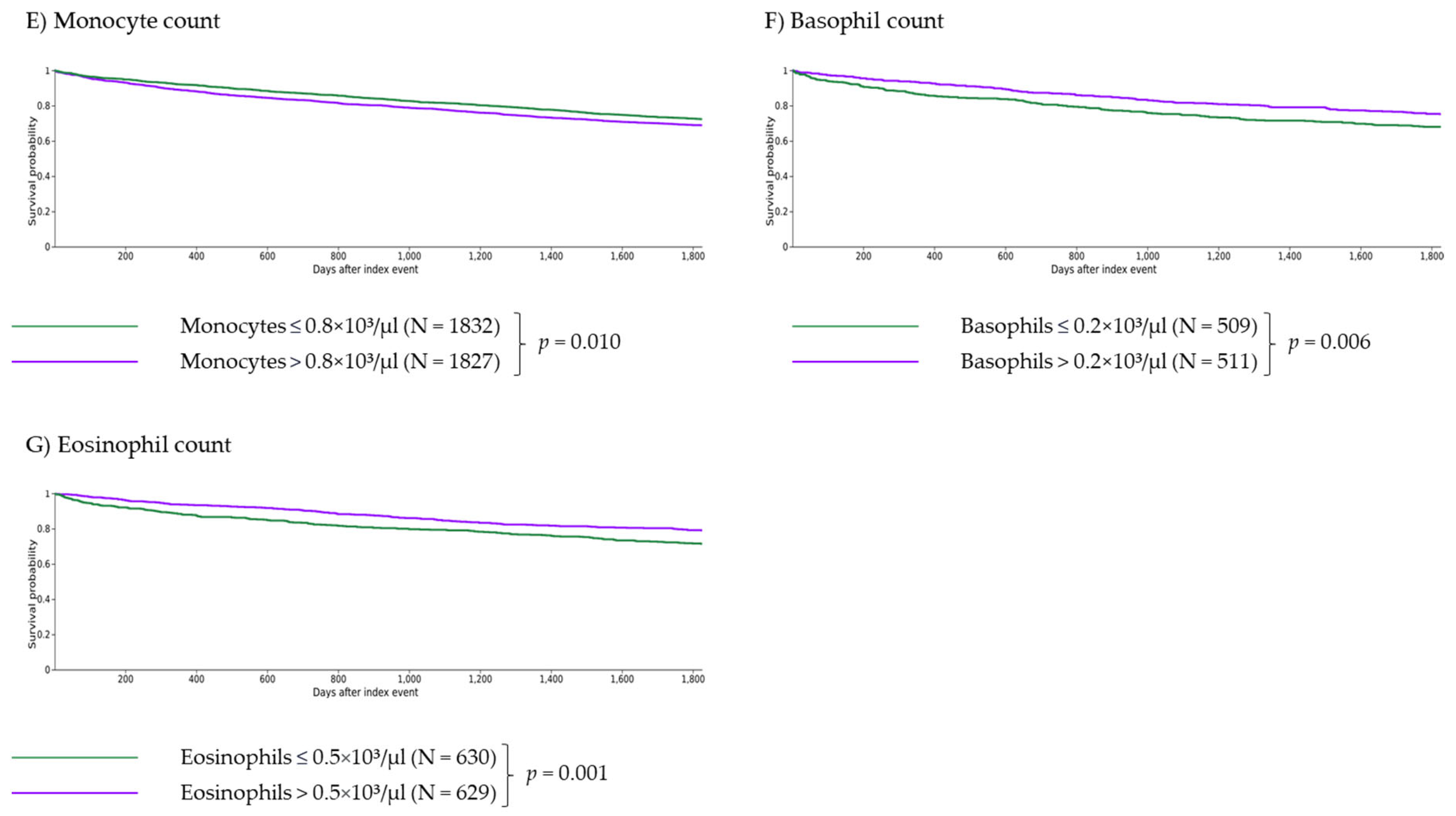
3.1.5. Impact of Monocytosis
3.1.6. Impact of Basophilia
3.1.7. Impact of Eosinophilia
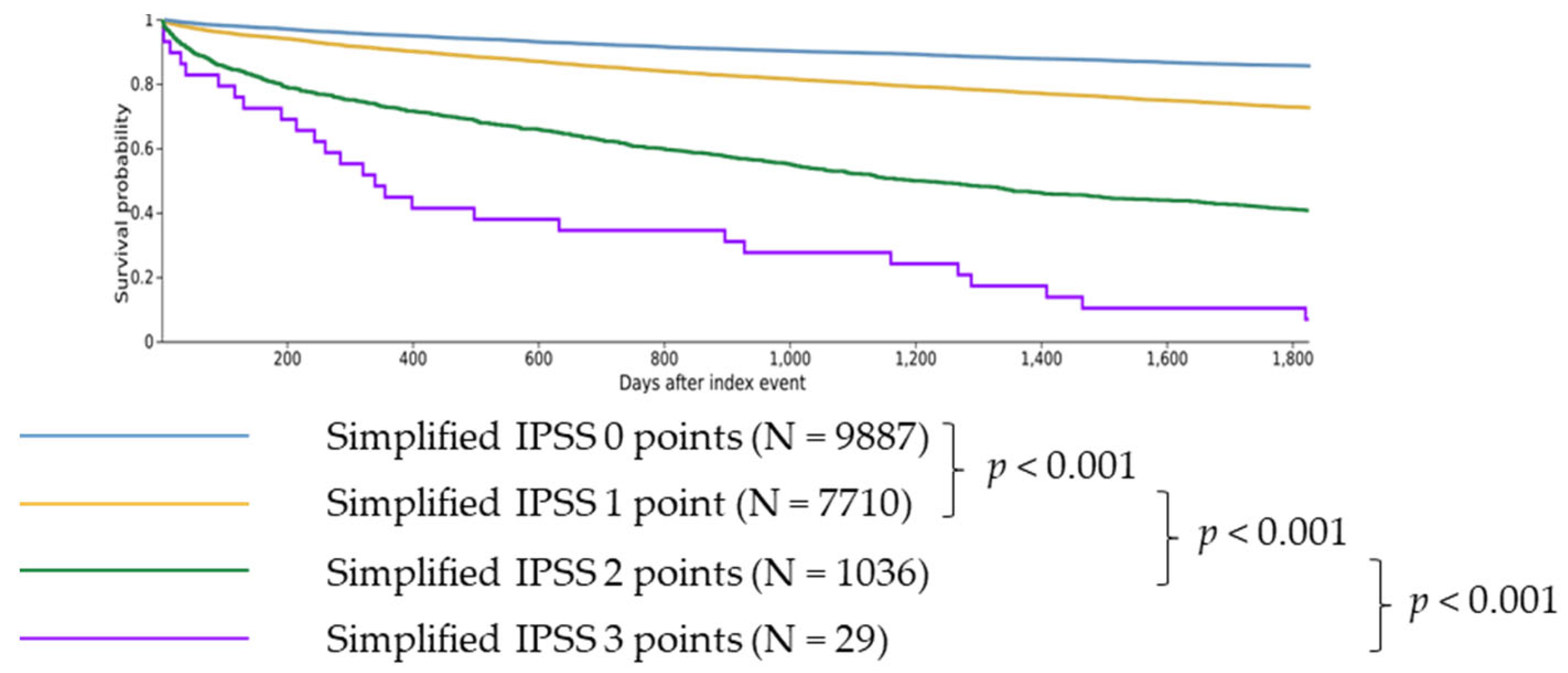
3.2. Impact of the Simplified IPSS Score
3.2.1. Comparison of 0 vs. 1 Point
3.2.2. Comparison of 1 vs. 2 Points
3.2.3. Comparison of 2 vs. 3 Points
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arber, D.A.; Orazi, A.; Hasserjian, R.P.; Borowitz, M.J.; Calvo, K.R.; Kvasnicka, H.-M.; Wang, S.A.; Bagg, A.; Barbui, T.; Branford, S.; et al. International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: Integrating morphologic, clinical, and genomic data. Blood 2022, 140, 1200–1228. [Google Scholar] [CrossRef]
- Tefferi, A. Primary myelofibrosis: 2023 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2023, 98, 801–821. [Google Scholar] [CrossRef]
- Verstovsek, S.; Mesa, R.A.; Gotlib, J.; Levy, R.S.; Gupta, V.; Di Persio, J.F.; Catalano, J.V.; Deininger, M.; Miller, C.; Silver, R.T.; et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N. Engl. J. Med. 2012, 366, 799–807. [Google Scholar] [CrossRef]
- Harrison, C.N.; Schaap, N.; Vannucchi, A.M.; Kiladjian, J.-J.; Jourdan, E.; Silver, R.T.; Schouten, H.C.; Passamonti, F.; Zweegman, S.; Talpaz, M.; et al. Fedratinib in patients with myelofibrosis previously treated with ruxolitinib: An updated analysis of the JAKARTA2 study using stringent criteria for ruxolitinib failure. Am. J. Hematol. 2020, 95, 594–603. [Google Scholar] [CrossRef]
- Pardanani, A.; Tefferi, A.; Masszi, T.; Mishchenko, E.; Drummond, M.; Jourdan, E.; Vannucchi, A.; Jurgutis, M.; Ribrag, V.; Rambaldi, A.; et al. Updated results of the placebo-controlled, phase III JAKARTA trial of fedratinib in patients with intermediate-2 or high-risk myelofibrosis. Br. J. Haematol. 2021, 195, 244–248. [Google Scholar] [CrossRef]
- Takenaka, K.; Shimoda, K.; Akashi, K. Recent advances in the diagnosis and management of primary myelofibrosis. Korean J. Intern. Med. 2018, 33, 679–690. [Google Scholar] [CrossRef]
- Amé, S.; Barraco, F.; Ianotto, J.-C.; Jourdan, E.; Rey, J.; Viallard, J.-F.; Wémeau, M.; Kiladjian, J.-J. Advances in management of primary myelofibrosis and polycythaemia vera: Implications in clinical practice. EJHaem 2023, 4, 779–791. [Google Scholar] [CrossRef]
- Cervantes, F.; Dupriez, B.; Pereira, A.; Passamonti, F.; Reilly, J.T.; Morra, E.; Vannucchi, A.M.; Mesa, R.A.; Demory, J.-L.; Barosi, G.; et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for Myelofibrosis Research and Treatment. Blood 2009, 113, 2895–2901. [Google Scholar] [CrossRef]
- Passamonti, F.; Cervantes, F.; Vannucchi, A.M.; Morra, E.; Rumi, E.; Pereira, A.; Guglielmelli, P.; Pungolino, E.; Caramella, M.; Maffioli, M.; et al. A dynamic prognostic model to predict survival in primary myelofibrosis: A study by the IWG-MRT (International Working Group for Myeloproliferative Neoplasms Research and Treatment). Blood 2010, 115, 1703–1708. [Google Scholar] [CrossRef]
- Gangat, N.; Caramazza, D.; Vaidya, R.; George, G.; Begna, K.; Schwager, S.; van Dyke, D.; Hanson, C.; Wu, W.; Pardanani, A.; et al. DIPSS plus: A refined Dynamic International Prognostic Scoring System for primary myelofibrosis that incorporates prognostic information from karyotype, platelet count, and transfusion status. J. Clin. Oncol. 2011, 29, 392–397. [Google Scholar] [CrossRef]
- Gowin, K.; Coakley, M.; Kosiorek, H.; Mesa, R. Discrepancies of applying primary myelofibrosis prognostic scores for patients with post polycythemia vera/essential thrombocytosis myelofibrosis. Haematologica 2016, 101, e405–e406. [Google Scholar] [CrossRef]
- Passamonti, F.; Giorgino, T.; Mora, B.; Guglielmelli, P.; Rumi, E.; Maffioli, M.; Rambaldi, A.; Caramella, M.; Komrokji, R.; Gotlib, J.; et al. A clinical-molecular prognostic model to predict survival in patients with post polycythemia vera and post essential thrombocythemia myelofibrosis. Leukemia 2017, 31, 2726–2731. [Google Scholar] [CrossRef]
- Guglielmelli, P.; Lasho, T.L.; Rotunno, G.; Mudireddy, M.; Mannarelli, C.; Nicolosi, M.; Pacilli, A.; Pardanani, A.; Rumi, E.; Rosti, V.; et al. MIPSS70: Mutation-Enhanced International Prognostic Score System for Transplantation-Age Patients with Primary Myelofibrosis. J. Clin. Oncol. 2018, 36, 310–318. [Google Scholar] [CrossRef]
- Titmarsh, G.J.; Duncombe, A.S.; McMullin, M.F.; O’Rorke, M.; Mesa, R.; de Vocht, F.; Horan, S.; Fritschi, L.; Clarke, M.; Anderson, L.A. How common are myeloproliferative neoplasms? A systematic review and meta-analysis. Am. J. Hematol. 2014, 89, 581–587. [Google Scholar] [CrossRef]
- Anderson, L.A.; McMullin, M.F. Epidemiology of MPN: What do we know? Curr. Hematol. Malig. Rep. 2014, 9, 340–349. [Google Scholar] [CrossRef]
- Shallis, R.M.; Wang, R.; Davidoff, A.; Ma, X.; Podoltsev, N.A.; Zeidan, A.M. Epidemiology of the classical myeloproliferative neoplasms: The four corners of an expansive and complex map. Blood Rev. 2020, 42, 100706. [Google Scholar] [CrossRef]
- Stapff, M.P. Using real world data to assess cardiovascular outcomes of two antidiabetic treatment classes. World J. Diabetes 2018, 9, 252–257. [Google Scholar] [CrossRef]
- Singh, S.; Khan, A. Clinical Characteristics and Outcomes of Coronavirus Disease 2019 Among Patients with Preexisting Liver Disease in the United States: A Multicenter Research Network Study. Gastroenterology 2020, 159, 768–771.e3. [Google Scholar] [CrossRef]
- Taquet, M.; Luciano, S.; Geddes, J.R.; Harrison, P.J. Bidirectional associations between COVID-19 and psychiatric disorder: Retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry 2021, 8, 130–140. [Google Scholar] [CrossRef]
- Zhu, J.; Wei, Z.; Suryavanshi, M.; Chen, X.; Xia, Q.; Jiang, J.; Ayodele, O.; Bradbury, B.D.; Brooks, C.; Brown, C.A.; et al. Characteristics and outcomes of hospitalised adults with COVID-19 in a Global Health Research Network: A cohort study. BMJ Open 2021, 11, e051588. [Google Scholar] [CrossRef]
- Sokal, J.E.; Cox, E.B.; Baccarani, M.; Tura, S.; Gomez, G.A.; Robertson, J.E.; Tso, C.Y.; Braun, T.J.; Clarkson, B.D.; Cervantes, F. Prognostic discrimination in “good-risk” chronic granulocytic leukemia. Blood 1984, 63, 789–799. [Google Scholar] [CrossRef]
- Hasford, J.; Pfirrmann, M.; Hehlmann, R.; Allan, N.C.; Baccarani, M.; Kluin-Nelemans, J.C.; Alimena, G.; Steegmann, J.L.; Ansari, H. A new prognostic score for survival of patients with chronic myeloid leukemia treated with interferon alfa. Writing Committee for the Collaborative CML Prognostic Factors Project Group. J. Natl. Cancer Inst. 1998, 90, 850–858. [Google Scholar] [CrossRef]
- Valent, P.; Horny, H.-P.; Arock, M. The underestimated role of basophils in Ph+ chronic myeloid leukaemia. Eur. J. Clin. Investig. 2018, 48, e13000. [Google Scholar] [CrossRef]
- Sperr, W.R.; Kundi, M.; Alvarez-Twose, I.; van Anrooij, B.; Oude Elberink, J.N.G.; Gorska, A.; Niedoszytko, M.; Gleixner, K.V.; Hadzijusufovic, E.; Zanotti, R.; et al. International prognostic scoring system for mastocytosis (IPSM): A retrospective cohort study. Lancet Haematol. 2019, 6, e638–e649. [Google Scholar] [CrossRef]
- Hintzke, M.; Hosking, P.; Olteanu, H.; Harrington, A.; Kroft, S.H. Bone Marrow Monocytosis: A Survey of 150 Cases. Am. J. Clin. Pathol. 2015, 144, A150. [Google Scholar] [CrossRef][Green Version]
- Kovalszki, A.; Weller, P.F. Eosinophilia. Prim. Care 2016, 43, 607–617. [Google Scholar] [CrossRef]
- Sticco, K.L.; Pandya, N.K.; Lynch, D.T. StatPearls: Basophilia; StatPearls: Treasure Island, FL, USA, 2024. [Google Scholar]
- Hadi, Y.B.; Lakhani, D.A.; Naqvi, S.F.; Fatima, N.U.; Sarwari, A.R. Outcomes of SARS-CoV-2 infection in patients with cystic fibrosis: A multicenter retrospective research network study. Respir. Med. 2021, 188, 106606. [Google Scholar] [CrossRef]
- Mughal, T.I.; Vaddi, K.; Sarlis, N.J.; Verstovsek, S. Myelofibrosis-associated complications: Pathogenesis, clinical manifestations, and effects on outcomes. Int. J. Gen. Med. 2014, 7, 89–101. [Google Scholar] [CrossRef]
- Kc, D.; Falchi, L.; Verstovsek, S. The underappreciated risk of thrombosis and bleeding in patients with myelofibrosis: A review. Ann. Hematol. 2017, 96, 1595–1604. [Google Scholar] [CrossRef]
- Savona, M.R. Are we altering the natural history of primary myelofibrosis? Leuk. Res. 2014, 38, 1004–1012. [Google Scholar] [CrossRef]
- Meckstroth, S.; Wang, R.; Ma, X.; Podoltsev, N. Patterns of Care for Older Patients with Myelofibrosis: A Population-based Study. Clin. Lymphoma Myeloma Leuk. 2021, 21, e551–e558. [Google Scholar] [CrossRef] [PubMed]
- Bose, P.; Verstovsek, S. Management of Myelofibrosis-Related Cytopenias. Curr. Hematol. Malig. Rep. 2018, 13, 164–172. [Google Scholar] [CrossRef]
- Santoshi, R.K.; Patel, R.; Patel, N.S.; Bansro, V.; Chhabra, G. A Comprehensive Review of Thrombocytopenia with a Spotlight on Intensive Care Patients. Cureus 2022, 14, e27718. [Google Scholar] [CrossRef]
- Lucijanic, M.; Krecak, I.; Soric, E.; Sabljic, A.; Galusic, D.; Holik, H.; Perisa, V.; Moric Peric, M.; Zekanovic, I.; Kusec, R. Patients with post polycythemia vera myelofibrosis might experience increased thrombotic risk in comparison to primary and post essential thrombocythemia myelofibrosis. Leuk. Res. 2022, 119, 106905. [Google Scholar] [CrossRef]
- Guglielmelli, P.; Carobbio, A.; Rumi, E.; de Stefano, V.; Mannelli, L.; Mannelli, F.; Rotunno, G.; Coltro, G.; Betti, S.; Cavalloni, C.; et al. Validation of the IPSET score for thrombosis in patients with prefibrotic myelofibrosis. Blood Cancer J. 2020, 10, 21. [Google Scholar] [CrossRef]
- Barbui, T.; Ghirardi, A.; Carobbio, A.; Masciulli, A.; Carioli, G.; Rambaldi, A.; Finazzi, M.C.; Bellini, M.; Rumi, E.; Vanni, D.; et al. Increased risk of thrombosis in JAK2 V617F-positive patients with primary myelofibrosis and interaction of the mutation with the IPSS score. Blood Cancer J. 2022, 12, 156. [Google Scholar] [CrossRef]
- Voigtlaender, M.; Langer, F. Management of Vascular Thrombosis in Patients with Thrombocytopenia. Hamostaseologie 2022, 42, 19–28. [Google Scholar] [CrossRef]
- Boiocchi, L.; Espinal-Witter, R.; Geyer, J.T.; Steinhilber, J.; Bonzheim, I.; Knowles, D.M.; Fend, F.; Orazi, A. Development of monocytosis in patients with primary myelofibrosis indicates an accelerated phase of the disease. Mod. Pathol. 2013, 26, 204–212. [Google Scholar] [CrossRef]
- Thomsen, G.N.; Christoffersen, M.N.; Lindegaard, H.M.; Davidsen, J.R.; Hartmeyer, G.N.; Assing, K.; Mortz, C.G.; Martin-Iguacel, R.; Møller, M.B.; Kjeldsen, A.D.; et al. The multidisciplinary approach to eosinophilia. Front. Oncol. 2023, 13, 1193730. [Google Scholar] [CrossRef]
- Lucijanic, M.; Livun, A.; Stoos-Veic, T.; Pejsa, V.; Jaksic, O.; Cicic, D.; Lucijanic, J.; Romic, Z.; Orehovec, B.; Aralica, G.; et al. High absolute basophil count is a powerful independent predictor of inferior overall survival in patients with primary myelofibrosis. Hematology 2018, 23, 201–207. [Google Scholar] [CrossRef]
- Dobrowolski, J.; Pasca, S.; Teodorescu, P.; Selicean, C.; Rus, I.; Zdrenghea, M.; Bojan, A.; Trifa, A.; Fetica, B.; Petrushev, B.; et al. Persistent Basophilia May Suggest an “Accelerated Phase” in the Evolution of CALR-Positive Primary Myelofibrosis Toward Acute Myeloid Leukemia. Front. Oncol. 2019, 9, 872. [Google Scholar] [CrossRef] [PubMed]
- Pieri, L.; Bogani, C.; Guglielmelli, P.; Zingariello, M.; Rana, R.A.; Bartalucci, N.; Bosi, A.; Vannucchi, A.M. The JAK2V617 mutation induces constitutive activation and agonist hypersensitivity in basophils from patients with polycythemia vera. Haematologica 2009, 94, 1537–1545. [Google Scholar] [CrossRef] [PubMed]
- Rozovski, U.; Verstovsek, S.; Manshouri, T.; Dembitz, V.; Bozinovic, K.; Newberry, K.; Zhang, Y.; Bove, J.E.; Pierce, S.; Kantarjian, H.; et al. An accurate, simple prognostic model consisting of age, JAK2, CALR, and MPL mutation status for patients with primary myelofibrosis. Haematologica 2017, 102, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A.; Guglielmelli, P.; Larson, D.R.; Finke, C.; Wassie, E.A.; Pieri, L.; Gangat, N.; Fjerza, R.; Belachew, A.A.; Lasho, T.L.; et al. Long-term survival and blast transformation in molecularly annotated essential thrombocythemia, polycythemia vera, and myelofibrosis. Blood 2014, 124, 2507–2513; quiz 2615. [Google Scholar] [CrossRef] [PubMed]
- Masarova, L.; Bose, P.; Pemmaraju, N.; Daver, N.G.; Sasaki, K.; Chifotides, H.T.; Zhou, L.; Kantarjian, H.M.; Estrov, Z.; Verstovsek, S. Improved survival of patients with myelofibrosis in the last decade: Single-center experience. Cancer 2022, 128, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Ersal, T.; Özkocaman, V.; Pınar, İ.E.; Yalçın, C.; Orhan, B.; Candar, Ö.; Çubukçu, S.; Koca, T.G.; Hunutlu, F.Ç.; Yavuz, Ş.; et al. Systemic inflammatory indices for predicting prognosis of myelofibrosis. Sci. Rep. 2023, 13, 12539. [Google Scholar] [CrossRef] [PubMed]
- Hilarius, D.L.; Kloeg, P.H.A.M.; Detmar, S.B.; Muller, M.J.; Aaronson, N.K. Level of agreement between patient self-report and observer ratings of health-related quality of life communication in oncology. Patient Educ. Couns. 2007, 65, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Fuentes-Arderiu, X.; García-Panyella, M.; Dot-Bach, D. Between-examiner reproducibility in manual differential leukocyte counting. Accredit. Qual. Assur. 2007, 12, 643–645. [Google Scholar] [CrossRef]
- Quinten, C.; Maringwa, J.; Gotay, C.C.; Martinelli, F.; Coens, C.; Reeve, B.B.; Flechtner, H.; Greimel, E.; King, M.; Osoba, D.; et al. Patient self-reports of symptoms and clinician ratings as predictors of overall cancer survival. J. Natl. Cancer Inst. 2011, 103, 1851–1858. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cohort 1 | Cohort 2 | |
|---|---|---|
| Age | >65 years | ≤65 years |
| Hemoglobin (Hb) | <10 g/dL | ≥10 g/dL |
| Leukocytes | >25 × 103/µL | ≤25 × 103/µL |
| Platelets | <150 × 103/µL | ≥150 × 103/µL |
| Monocytes | >0.8 × 103/µL | ≤0.8 × 103/µL |
| Basophiles | >0.2 × 103/µL | ≤0.2 × 103/µL |
| Eosinophiles | >0.5 × 103/µL | ≤0.5 × 103/µL |
| Attribute | |
|---|---|
| Total cohort, n (%) | 37,513 (100%) |
| Sex, n (%) | |
| Female | 19,976 (53.3%) |
| Male | 15,394 (41.0%) |
| Unkown | 2143 (5.7%) |
| Age at diagnosis | |
| Mean ± SD | 60.3 + 17.5 |
| Race | |
| White | 25,963 (69.2%) |
| Unknown | 6806 (18.1%) |
| Black or African American | 2907 (7.7%) |
| Asian | 802 (2.1%) |
| Other | 1035 (2.8%) |
| Laboratory (mean ± SD) | |
| Hemoglobin (in g/dL) in Blood | 13.1 ± 2.0 |
| Leukocytes (in ×103/µL) in Blood | 12.3 ± 146 |
| Platelets (in ×103/µL) in Blood | 230 ± 100 |
| Monocytes (in ×103/µL) in Blood | 8.4 ± 3.6 |
| Basophiles (in ×103/µL) in Blood | 0.6 ± 0.8 |
| Eosinophiles (in ×103/µL) in Blood | 2.5 ± 2.5 |
| Outcome | |
| Five-year survival rate (in %) | 78.4% |
| Documented five-year AML progression (in %) | 1.3% |
| Documented five-year cachexia rate (in %) | 1.6% |
| Documented five-year SIRS rate (in %) | 4.9% |
| Documented five-year hemorrhage rate (in %) | 8.0% |
| Documented five-year thrombosis rate (in %) | 5.2% |
| Death | AML Transformation | Cachexia | SIRS | Hemorrhage | Thrombosis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Risk Factor | RR | (95% CI) | RR | (95% CI) | RR | (95% CI) | RR | (95% CI) | RR | (95% CI) | RR | (95% CI) |
| Age | 1.798 | (1.700, 1.903) | 1.548 | (1.251, 1.915) | 1.189 | (0.967, 1.461) | 1.093 | (0.974, 1.226) | 1.280 | (1.171, 1.400) | 1.305 | (1.166, 1.461) |
| Anemia | 2.278 | (2.120, 2.448) | 6.096 | (4.124, 9.010) | 3.052 | (2.264, 4.114) | 2.970 | (2.485, 3.550) | 1.406 | (1.206, 1.641) | 1.919 | (1.587, 2.320) |
| Leuko-cytosis | 1.845 | (1.474, 2.309) | 3.377 | (1.702, 6.702) | 1.917 | (0.911, 4.032) | 1.130 | (0.625, 2.044) | 1.443 | (0.882, 2.360) | 1.505 | (0.808, 2.802) |
| Thrombo-cytopenia | 2.032 | (1.910, 2.162) | 5.632 | (4.365, 7.268) | 1.799 | (1.397, 2.315) | 2.150 | (1.858, 2.487) | 1.421 | (1.257, 1.605) | 1.579 | (1.357, 1.837) |
| Monocytosis | 1.126 | (1.018, 1.245) | 1.122 | (0.714, 1.763) | 0.941 | (0.583, 1.519) | 1.407 | (1.092, 1.811) | 1.046 | (0.850, 1.288) | 1.428 | (1.101, 1.853) |
| Basophilia | 0.776 | (0.637, 0.945) | 1.640 | (0.875, 3.074) | 1.482 | (0.672, 3.268) | 1.022 | (0.636, 1.642) | 1.165 | (0.790, 1.717) | 1.106 | (0.717, 1.704) |
| Eosinophilia | 0.734 | (0.604, 0.893) | 0.662 | (0.322, 1.363) | 0.836 | (0.364, 1.921) | 0.920 | (0.593, 1.427) | 0.966 | (0.688, 1.356) | 1.161 | (0.731, 1.844) |
| Death | AML Transformation | Cachexia | SIRS | Hemorrhage | Thrombosis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Simplified IPSS | RR | (95% CI) | RR | (95% CI) | RR | (95% CI) | RR | (95% CI) | RR | (95% CI) | RR | (95% CI) |
| 0 vs. 1 | 1.932 | (1.815, 2.056) | 2.515 | (1.934, 3.271) | 1.837 | (1.470, 2.296) | 1.609 | (1.429, 1.812) | 1.370 | (1.242, 1.512) | 1.429 | (1.265, 1.614) |
| 1 vs. 2 | 2.255 | (2.118, 2.402) | 4.609 | (3.616, 5.875) | 2.165 | (1.607, 2.918) | 1.858 | (1.560, 2.213) | 1.287 | (1.077, 1.537) | 1.497 | (1.221, 1.836) |
| 2 vs. 3 | 1.571 | (1.406, 1.756) | 3.623 | (2.129, 6.165) | 6.604 | (3.749, 11.631) | 2.489 | (1.479, 4.191) | 3.015 | (1.827, 4.976) | 3.312 | (1.948, 5.630) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kappenstein, M.; von Bubnoff, N. Real-World Electronic Medical Records Data Identify Risk Factors for Myelofibrosis and Can Be Used to Validate Established Prognostic Scores. Cancers 2024, 16, 1416. https://doi.org/10.3390/cancers16071416
Kappenstein M, von Bubnoff N. Real-World Electronic Medical Records Data Identify Risk Factors for Myelofibrosis and Can Be Used to Validate Established Prognostic Scores. Cancers. 2024; 16(7):1416. https://doi.org/10.3390/cancers16071416
Chicago/Turabian StyleKappenstein, Max, and Nikolas von Bubnoff. 2024. "Real-World Electronic Medical Records Data Identify Risk Factors for Myelofibrosis and Can Be Used to Validate Established Prognostic Scores" Cancers 16, no. 7: 1416. https://doi.org/10.3390/cancers16071416
APA StyleKappenstein, M., & von Bubnoff, N. (2024). Real-World Electronic Medical Records Data Identify Risk Factors for Myelofibrosis and Can Be Used to Validate Established Prognostic Scores. Cancers, 16(7), 1416. https://doi.org/10.3390/cancers16071416