
High HER2 Intratumoral Heterogeneity Is a Predictive Factor for Poor Prognosis in Early-Stage and Locally Advanced HER2-Positive Breast Cancer

 , , , , and
, , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection and Breast Tumor Samples
2.2. HER2 FISH Assay
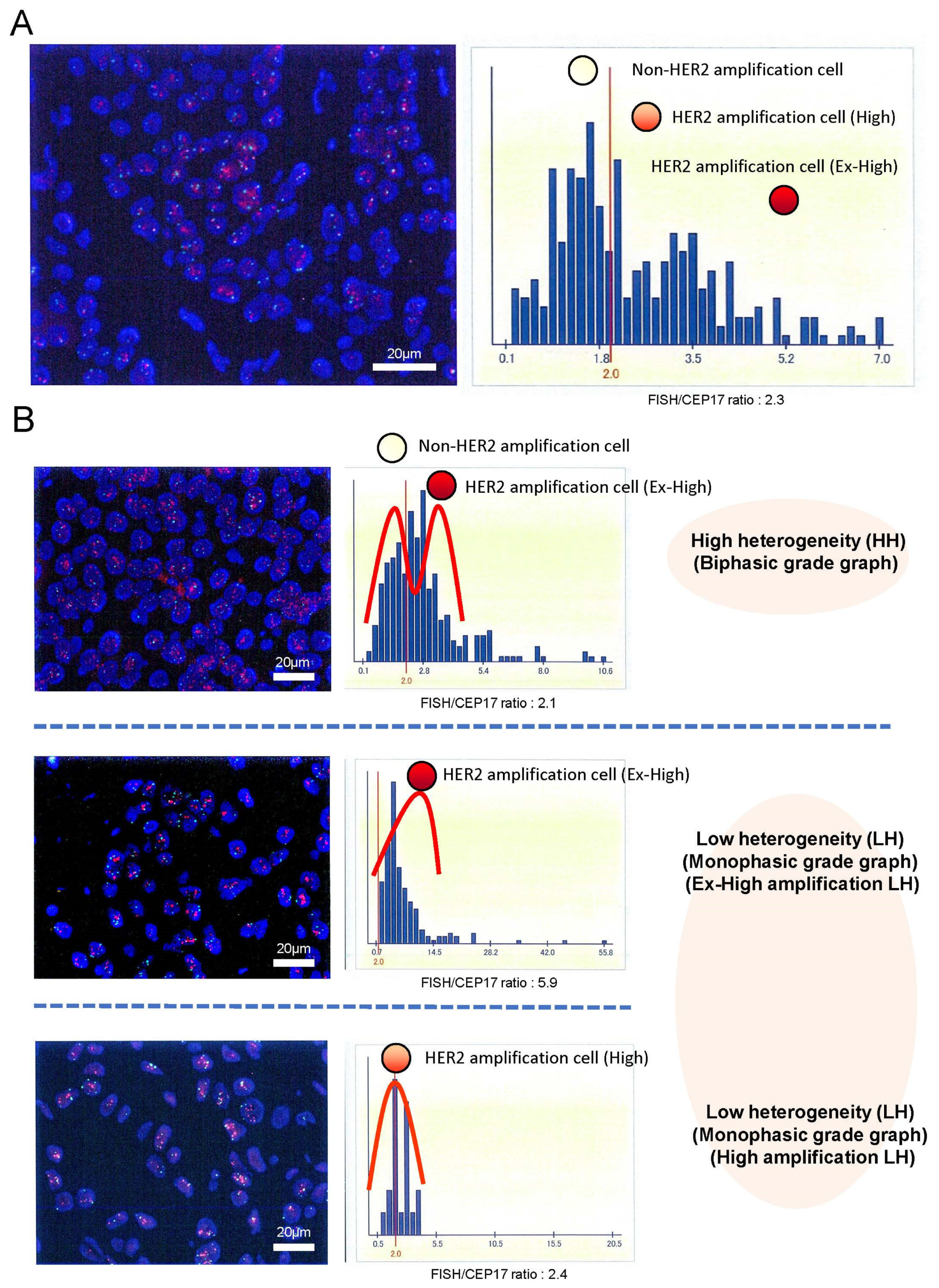
2.3. Assessment of HER2 Intratumoral Heterogeneity
2.4. Statistical Analysis
2.5. Data Availability
3. Results
3.1. Association between HER2 Intratumoral Heterogeneity and Patient Characteristics
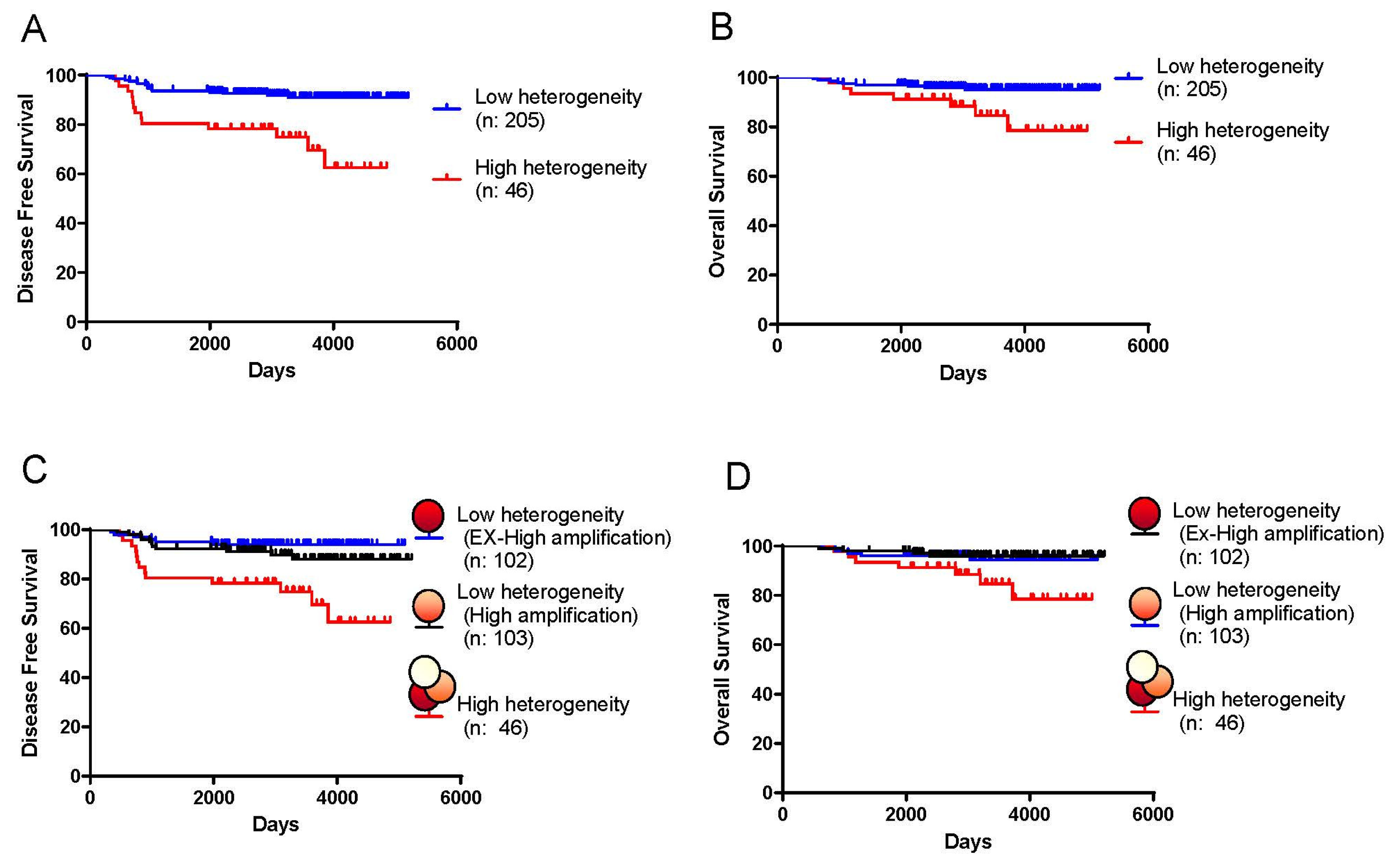
3.2. HER2 Intratumoral Heterogeneity and Patient Prognosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- IJzerman, M.J.; Berghuis, A.S.; de Bono, J.S.; Terstappen, L.W. Health Economic Impact of Liquid Biopsies in Cancer Management. Expert Rev. Pharmacoeconomics Outcomes Res. 2018, 18, 593–599. [Google Scholar] [CrossRef]
- Dagogo-Jack, I.; Shaw, A.T. Tumour Heterogeneity and Resistance to Cancer Therapies. Nat. Rev. Clin. Oncol. 2018, 15, 81–94. [Google Scholar] [CrossRef]
- Ramón y Cajal, S.; Sesé, M.; Capdevila, C.; Aasen, T.; De Mattos-Arruda, L.; Diaz-Cano, S.J.; Hernández-Losa, J.; Castellvί, J. Clinical Implications of Intratumor Het- erogeneity: Challenges and Opportunities. J. Mol. Med. 2020, 98, 161–177. [Google Scholar] [CrossRef]
- Beca, F.; Polyak, K. Intratumor Heterogeneity in Breast Cancer. Nov. Biomark. Contin. Breast Cancer 2016, 882, 169–189. [Google Scholar]
- Marusyk, A.; Polyak, K. Tumor Heterogeneity: Causes and Consequences. Biochim. Biophys. Acta (BBA)-Rev. Cancer 2010, 1805, 105–117. [Google Scholar] [CrossRef]
- Marusyk, A.; Janiszewska, M.; Polyak, K. Intratumor Heterogeneity: The Rosetta Stone of Therapy Resistance. Cancer Cell 2020, 37, 471–484. [Google Scholar] [CrossRef]
- Hayes, D.F. HER2 and Breast Cancer—A Phenomenal Success Story. N. Engl. J. Med. 2019, 381, 1284–1286. [Google Scholar] [CrossRef]
- Hanna, W.M.; Rüschoff, J.; Bilous, M.; Coudry, R.A.; Dowsett, M.; Osamura, R.Y.; Penault-Llorca, F.; Van De Vijver, M.; Viale, G. HER2 in Situ Hybridization in Breast Cancer: Clinical Implications of Polysomy 17 and Genetic Heterogeneity. Mod. Pathol. 2014, 27, 4–18. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Procter, M.; de Azambuja, E.; Zardavas, D.; Benyunes, M.; Viale, G.; Suter, T.; Arahmani, A.; Rouchet, N.; Clark, E.; et al. Adjuvant Pertuzumab and Trastuzumab in Early HER2-Positive Breast Cancer. N. Engl. J. Med. 2017, 377, 122–131. [Google Scholar] [CrossRef]
- Cameron, D.; Piccart-Gebhart, M.J.; Gelber, R.D.; Procter, M.; Goldhirsch, A.; de Azambuja, E.; Castro, G.; Untch, M.; Smith, I.; Gianni, L.; et al. 11 Years’ Follow-up of Trastuzumab After Adjuvant Chemotherapy in HER2-Positive Early Breast Cancer: Final Analysis of the HERceptin Adjuvant (HERA) Trial. Lancet 2017, 389, 1195–1205. [Google Scholar] [CrossRef]
- Marchiò, C.; Annaratone, L.; Marques, A.; Casorzo, L.; Berrino, E.; Sapino, A. Evolving Concepts in HER2 Evaluation in Breast Cancer: Heterogeneity, HER2-Low Carcinomas and Beyond. In Seminars in Cancer Biology; Elsevier: Amsterdam, The Netherlands, 2021; Volume 72, pp. 123–135. [Google Scholar]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. Arch. Pathol. Lab. Med. 2018, 142, 1364–1382. [Google Scholar] [CrossRef]
- Zardavas, D.; Irrthum, A.; Swanton, C.; Piccart, M. Clinical Management of Breast Cancer Heterogeneity. Nat. Rev. Clin. Oncol. 2015, 12, 381–394. [Google Scholar] [CrossRef]
- Assenov, Y.; Brocks, D.; Gerhäuser, C. Intratumor Heterogeneity in Epigenetic Patterns. In Seminars in Cancer Biology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 51, pp. 12–21. [Google Scholar]
- Wolff, A.C.; Hammond, M.E.H.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; Dowsett, M.; Fitzgibbons, P.L.; Hanna, W.M.; Langer, A.; et al. American Society of Clinical Oncology/College of American Pathologists Guideline Recommen- dations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer. Arch. Pathol. Lab. Med. 2007, 131, 18–43. [Google Scholar] [CrossRef]
- Allison, K.H.; Dintzis, S.M.; Schmidt, R.A. Frequency of HER2 Heterogeneity by Fluorescence in Situ Hybridization According to CAP Expert Panel Recommendations: Time for a New Look at How to Report Heterogeneity. Am. J. Clin. Pathol. 2011, 136, 864–871. [Google Scholar] [CrossRef]
- Chang, M.C.; Malowany, J.I.; Mazurkiewicz, J.; Wood, M. ‘Genetic Heterogeneity’ in HER2/Neu Testing by Fluorescence In Situ Hybridization: A Study of 2522 Cases. Mod. Pathol. 2012, 25, 683–688. [Google Scholar] [CrossRef]
- Miglietta, F.; Griguolo, G.; Bottosso, M.; Giarratano, T.; Lo Mele, M.; Fassan, M.; Cacciatore, M.; Genovesi, E.; De Bartolo, D.; Vernaci, G.; et al. Evolution of HER2-Low Expression from Primary to Recurrent Breast Cancer. NPJ Breast Cancer 2021, 7, 137. [Google Scholar] [CrossRef]
- Sapino, A.; Goia, M.; Recupero, D.; Marchiò, C. Current Challenges for HER2 Testing in Diagnostic Pathology: State of the Art and Controversial Issues. Front. Oncol. 2013, 3, 129. [Google Scholar] [CrossRef]
- Denkert, C.; Seither, F.; Schneeweiss, A.; Link, T.; Blohmer, J.-U.; Just, M.; Wimberger, P.; Forberger, A.; Tesch, H.; Jackisch, C.; et al. Clinical and Molecular Characteristics of HER2-Low-Positive Breast Cancer: Pooled Analysis of Individual Patient Data from Four Prospective, Neoadjuvant Clinical Trials. Lancet Oncol. 2021, 22, 1151–1161. [Google Scholar] [CrossRef]
- Hou, Y.; Nitta, H.; Li, Z. HER2 Intratumoral Heterogeneity in Breast Cancer, an Evolving Concept. Cancers 2023, 15, 2664. [Google Scholar] [CrossRef]
- Hamilton, E.; Shastry, M.; Shiller, S.M.; Ren, R. Targeting HER2 Heterogeneity in Breast Cancer. Cancer Treat. Rev. 2021, 100, 102286. [Google Scholar] [CrossRef]
- Mansfield, A.S.; Sukov, W.R.; Eckel-Passow, J.E.; Sakai, Y.; Walsh, F.J.; Lonzo, M.; Wiktor, A.E.; Dogan, A.; Jenkins, R.B. Comparison of Fluorescence in Situ Hybridization (FISH) and Dual-ISH (DISH) in the Determination of HER2 Status in Breast Cancer. Am. J. Clin. Pathol. 2013, 139, 144–150. [Google Scholar] [CrossRef]
- Schiavon, B.N.; Jasani, B.; De Brot, L.; Vassallo, J.; Damascena, A.; Cirullo-Neto, J.; Neves, J.I.; Soares, F.A.; Gobbi, H.; Rocha, R.M. Evaluation of Reliability of FISH Versus Brightfield Dual-Probe in Situ Hy-Bridization (BDISH) for Frontline Assessment of HER2 Status in Breast Cancer Samples in a Community Setting: Influence of Poor Tissue Preservation. Am. J. Surg. Pathol. 2012, 36, 1489–1496. [Google Scholar] [CrossRef]
- Babic, A.; Loftin, I.R.; Stanislaw, S.; Wang, M.; Miller, R.; Warren, S.M.; Zhang, W.; Lau, A.; Miller, M.; Wu, P.; et al. The Impact of Pre-Analytical Processing on Staining Quality for h&e, Dual Hapten, Dual Color in Situ Hybridization and Fluorescent in Situ Hybridization Assays. Methods 2010, 52, 287–300. [Google Scholar]
- Seol, H.; Lee, H.J.; Choi, Y.; Lee, H.E.; Kim, Y.J.; Kim, J.H.; Kang, E.; Kim, S.-W.; Park, S.Y. Intratumoral Heterogeneity of HER2 Gene Amplification in Breast Cancer: Its Clinicopathological Significance. Mod. Pathol. 2012, 25, 938–948. [Google Scholar] [CrossRef]
- Shen, T.; Nitta, H.; Wei, L.; Parwani, A.V.; Li, Z. HER2 Intratumoral Heterogeneity Is Independently Associated with Distal Metastasis and Overall Survival in HER2-Positive Breast Carcinomas. Breast Cancer Res. Treat. 2020, 181, 519–527. [Google Scholar] [CrossRef]
- Furrer, D.; Sanschagrin, F.; Jacob, S.; Diorio, C. Advantages and Disadvantages of Technologies for HER2 Testing in Breast Cancer Specimens. Am. J. Clin. Pathol. 2015, 144, 686–703. [Google Scholar] [CrossRef]
- de Torrenté, L.; Zimmerman, S.; Suzuki, M.; Christopeit, M.; Greally, J.M.; Mar, J.C. The Shape of Gene Expression Distributions Matter: How Incorporating Distribution Shape Improves the Interpretation of Cancer Transcriptomic Data. BMC Bioinform. 2020, 21, 562. [Google Scholar] [CrossRef]
- Patkulkar, P.A.; Subbalakshmi, A.R.; Jolly, M.K.; Sinharay, S. Mapping Spatiotemporal Heterogeneity in Tumor Profiles by Integrating High-Throughput Imaging and Omics Analysis. ACS Omega 2023, 8, 6126–6138. [Google Scholar] [CrossRef]
- Radziuviene, G.; Rasmusson, A.; Augulis, R.; Lesciute-Krilaviciene, D.; Laurinaviciene, A.; Clim, E.; Laurinavicius, A. Automated Image Analysis of HER2 Fluores- cence In Situ Hybridization to Refine Definitions of Genetic Heterogeneity in Breast Cancer Tissue. BioMed Res. Int. 2017, 2017, 2321916. [Google Scholar] [CrossRef]
- Prabakaran, I.; Wu, Z.; Lee, C.; Tong, B.; Steeman, S.; Koo, G.; Zhang, P.J.; Guvakova, M.A. Gaussian Mixture Models for Probabilistic Classification of Breast Cancer. Cancer Res. 2019, 79, 3492–3502. [Google Scholar] [CrossRef]
- Skibinski, A.; Kuperwasser, C. The Origin of Breast Tumor Heterogeneity. Oncogene 2015, 34, 5309–5316. [Google Scholar] [CrossRef]
- Horii, R.; Nitta, H.; Nojima, M.; Maruyama, R.; Ueno, T.; Ito, Y.; Ohno, S.; Banks, P.; Kanda, H.; Akiyama, F. Predictive Significance of HER2 Intratumoral Heterogeneity, Determined by Simultaneous Gene and Protein Analysis, for Resistance to Trastuzumab-Based Treatments for HER2-Positive Breast Cancer. Virchows Arch. 2021, 479, 13–21. [Google Scholar] [CrossRef]
- Hou, Y.; Nitta, H.; Wei, L.; Banks, P.M.; Portier, B.; Parwani, A.V.; Li, Z. HER2 Intratumoral Heterogeneity Is Independently Associated with Incomplete Response to Anti-HER2 Neoadjuvant Chemotherapy in HER2-Positive Breast Carcinoma. Breast Cancer Res. Treat. 2017, 166, 447–457. [Google Scholar] [CrossRef]
- Jiang, G.; Zhang, S.; Yazdanparast, A.; Li, M.; Pawar, A.V.; Liu, Y.; Inavolu, S.M.; Cheng, L. Comprehensive Comparison of Molecular Portraits Between Cell Lines and Tumors in Breast Cancer. BMC Genom. 2016, 17, 281–301. [Google Scholar] [CrossRef]
- Bui, M.M.; Riben, M.W.; Allison, K.H.; Chlipala, E.; Colasacco, C.; Kahn, A.G.; Lacchetti, C.; Madabhushi, A.; Pantanowitz, L.; Salama, M.E.; et al. Quantitative Image Analysis of Human Epidermal Growth Factor Receptor 2 Immunohistochemistry for Breast Cancer: Guideline from the College of American Pathologists. Arch. Pathol. Lab. Med. 2019, 143, 1180–1195. [Google Scholar] [CrossRef]
- Yousif, M.; Huang, Y.; Sciallis, A.; Kleer, C.G.; Pang, J.; Smola, B.; Naik, K.; McClintock, D.S.; Zhao, L.; Kunju, L.P.; et al. Quantitative Image Analysis as an Adjunct to Manual Scoring of ER, PgR, and HER2 in Invasive Breast Carcinoma. Am. J. Clin. Pathol. 2022, 157, 899–907. [Google Scholar] [CrossRef]
- Farahmand, S.; Fernandez, A.I.; Ahmed, F.S.; Rimm, D.L.; Chuang, J.H.; Reisenbichler, E.; Zarringhalam, K. Deep Learning Trained on Hematoxylin and Eosin Tumor Region of Interest Predicts HER2 Status and Trastuzumab Treatment Response in HER2+ Breast Cancer. Mod. Pathol. 2022, 35, 44–51. [Google Scholar] [CrossRef]
- Helin, H.O.; Tuominen, V.J.; Ylinen, O.; Helin, H.J.; Isola, J. Free Digital Image Analysis Software Helps to Resolve Equivocal Scores in HER2 Immunohistochemistry. Virchows Arch. 2016, 468, 191–198. [Google Scholar] [CrossRef]
- Tarantino, P.; Hamilton, E.; Tolaney, S.M.; Cortes, J.; Morganti, S.; Ferraro, E.; Marra, A.; Viale, G.; Trapani, D.; Cardoso, F.; et al. HER2-Low Breast Cancer: Pathological and Clinical Landscape. J. Clin. Oncol. 2020, 38, 1951–1962. [Google Scholar] [CrossRef]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef]
- Ogitani, Y.; Aida, T.; Hagihara, K.; Yamaguchi, J.; Ishii, C.; Harada, N.; Soma, M.; Okamoto, H.; Oitate, M.; Arakawa, S.; et al. DS-8201a, a Novel HER2-Targeting ADC with a Novel DNA Topoisomerase i Inhibitor, Demonstrates a Promising Antitumor Efficacy with Differentiation from t-DM1Preclinical Efficacy of DS-8201a, a Novel HER2-Targeting ADC. Clin. Cancer Res. 2016, 22, 5097–5108. [Google Scholar] [CrossRef]
- Ogitani, Y.; Hagihara, K.; Oitate, M.; Naito, H.; Agatsuma, T. Bystander Killing Effect of DS-8201a, a Novel Anti-Human Epidermal Growth Factor Receptor 2 Antibody–Drug Conjugate, in Tumors with Human Epidermal Growth Factor Receptor 2 Heterogeneity. Cancer Sci. 2016, 107, 1039–1046. [Google Scholar] [CrossRef]
- Mosele, F.; Deluche, E.; Lusque, A.; Le Bescond, L.; Filleron, T.; Pradat, Y.; Ducoulombier, A.; Pistilli, B.; Bachelot, T.; Viret, F.; et al. Trastuzumab Deruxtecan in Metastatic Breast Cancer with Variable HER2 Expression: The Phase 2 DAISY Trial. Nat. Med. 2023, 29, 2110–2120. [Google Scholar] [CrossRef]
- Bang, Y.-J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in Combination with Chemotherapy Versus Chemotherapy Alone for Treatment of HER2-Positive Advanced Gastric or Gastro-Oesophageal Junction Cancer (ToGA): A Phase 3, Open-Label, Randomised Controlled Trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Johnson, A.M.; Dumbrava, E.E.I.; Raghav, K.; Balaji, K.; Bhatt, M.; Murthy, R.K.; Rodon, J.; Piha-Paul, S.A. Advances in HER2-Targeted Therapy: Novel Agents and Opportunities Beyond Breast and Gastric Cancer. Clin. Cancer Res. 2019, 25, 2033–2041. [Google Scholar] [CrossRef]
- Jørgensen, J.T.; Winther, H.; Askaa, J.; Andresen, L.; Olsen, D.; Mollerup, J. A Companion Diagnostic with Significant Clinical Impact in Treatment of Breast and Gastric Cancer. Front. Oncol. 2021, 11, 676939. [Google Scholar] [CrossRef]
- Grillo, F.; Fassan, M.; Sarocchi, F.; Fiocca, R.; Mastracci, L. HER2 Heterogeneity in Gastric/Gastroesophageal Cancers: From Benchside to Practice. World J. Gastroenterol. 2016, 22, 5879. [Google Scholar] [CrossRef]
- Bang, K.; Cheon, J.; Park, Y.S.; Kim, H.-D.; Ryu, M.-H.; Park, Y.; Moon, M.; Lee, H.; Kang, Y.-K. Association Between HER2 Heterogeneity and Clinical Outcomes of HER2-Positive Gastric Cancer Patients Treated with Trastuzumab. Gastric Cancer 2022, 25, 794–803. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Number | (%) | Number | (%) | ||
|---|---|---|---|---|---|
| Menopause | ER | ||||
| Pre- | 96 | (38.2) | Positive | 167 | (66.5) |
| Post- | 155 | (61.8) | Negative | 84 | (33.5) |
| Histological type | PgR | ||||
| IDC | 244 | (97.2) | Positive | 99 | (39.4) |
| ILC | 7 | (2.8) | Negative | 152 | (60.6) |
| Histological type | HER2 IHC | ||||
| 1 | 26 | (10.4) | 3+ | 232 | (92.4) |
| 2 | 91 | (36.3) | 2+ | 19 | (7.6) |
| 3 | 134 | (53.4) | HER2 ratio | ||
| Tumor size | Mean | 4.8 ± 2.5 | |||
| T1 | 86 | (34.3) | HER2 heterogeneity | ||
| T2 | 139 | (55.4) | High (HH) | 46 | (18.3) |
| T3 or T4 | 26 | (10.4) | Low (LH) | 205 | (81.7) |
| Pretreatment LN metastasis | (Ex-High-Amplification LH) | 102 | (49.8) | ||
| Negative | 134 | (53.4) | (High-Amplification LH) | 103 | (50.2) |
| Positive | 117 | (46.6) | Stage | ||
| Resected LN metastasis | I | 68 | (27.1) | ||
| Yes | 116 | (46.2) | II | 161 | (64.1) |
| No | 135 | (53.8) | III | 22 | (8.8) |
| Neoadjuvant chemotherapy | |||||
| Negative | 185 | (73.7) | |||
| Positive | 66 | (26.3) | |||
| HER-2 Heterogeneity | ||||
|---|---|---|---|---|
| Total | High (HH) | Low (LH) | p-Value | |
| n = 251, % | n = 46, % | n = 205, % | ||
| Menopause | ||||
| Pre- | 96 (38.2%) | 23 (50.0%) | 73 (35.6%) | 0.1 |
| Post- | 155 (61.8%) | 23 (50.0%) | 132 (64.4%) | |
| Histological type | ||||
| IDC | 244 (97.2%) | 43 (93.5%) | 201 (98.0%) | 0.118 |
| ILC | 7 (2.8%) | 3 (6.5%) | 4 (2.0%) | |
| Histological grade | ||||
| 1 | 26 (10.4%) | 3 (6.5%) | 23 (11.2%) | 0.421 |
| 2 | 91 (36.3%) | 20 (43.5%) | 71 (34.6%) | |
| 3 | 134 (53.4%) | 23 (50.0%) | 111 (54.1%) | |
| Tumor size | ||||
| T1 | 86 (34.3%) | 14 (30.4%) | 72 (35.1%) | 0.665 |
| T2–T4 | 165 (65.7%) | 32 (69.6%) | 133 (64.9%) | |
| Pretreatment LN metastasis | ||||
| Negative | 134 (53.4%) | 19 (41.3%) | 115 (56.1%) | 0.098 |
| Positive | 117 (46.6%) | 27 (58.7%) | 90 (43.9%) | |
| Resected LN metastasis | ||||
| Negative | 185 (73.7%) | 31 (67.4%) | 154 (75.1%) | 0.373 |
| Positive | 66 (26.3%) | 15 (32.6%) | 51 (24.9%) | |
| ER | ||||
| Positive | 167 (66.5%) | 40 (87.0%) | 127 (62.0%) | 0.002 |
| Negative | 84 (33.5%) | 6 (13.0%) | 78 (38.0%) | |
| PgR | ||||
| Positive | 99 (39.4%) | 29 (63.0%) | 70 (34.1%) | 5.46 × 10−4 |
| Negative | 152 (60.6%) | 17 (37.0%) | 135 (65.9%) | |
| HER2 IHC | ||||
| 3+ | 232 (92.4%) | 40 (87.0%) | 192 (93.7%) | 0.128 |
| 2+ | 19 (7.6%) | 6 (13.0%) | 13 (6.3%) | |
| HER2 ratio | ||||
| Mean | 4.8 ± 2.5 | 2.3 ± 0.4 | 5.4 ± 2.4 | 1.03 × 10−43 |
| Neoadjuvant chemotherapy | ||||
| Yes | 116 (46.2%) | 27 (58.7%) | 89 (43.4%) | 0.086 |
| No | 135 (53.8%) | 19 (41.3%) | 116 (56.6%) | |
| Stage | ||||
| I | 68 (27.1%) | 8 (17.4%) | 60 (29.3%) | 0.094 |
| II | 161 (64.1%) | 31 (67.4%) | 130 (63.4%) | |
| III | 22 (8.8%) | 7 (15.2%) | 15 (7.3%) | |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | N | Event (N) | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| cT | ||||||||
| T1 | 86 | 8 | 1 | 1 | ||||
| T2–T4 | 165 | 22 | 1.41 | 0.63–3.16 | 0.41 | 1.04 | 0.45–2.40 | 0.932 |
| ER | ||||||||
| Positive | 167 | 20 | 1 | 1 | ||||
| Negative | 84 | 10 | 0.99 | 0.46–2.12 | 0.985 | 1.63 | 0.62–4.29 | 0.326 |
| PgR | ||||||||
| Positive | 99 | 14 | 1 | 1 | ||||
| Negative | 152 | 16 | 0.76 | 0.37–1.56 | 0.452 | 0.95 | 0.39–2.33 | 0.918 |
| Pretreatment LN metastasis | ||||||||
| Negative | 134 | 10 | 1 | 1 | ||||
| Positive | 117 | 20 | 2.33 | 1.09–4.98 | 0.029 | 1.23 | 0.43–3.52 | 0.696 |
| Resected LN metastasis | ||||||||
| Negative | 185 | 16 | 1 | 1 | ||||
| Positive | 66 | 14 | 2.6 | 1.27–5.32 | 0.009 | 2.26 | 0.81–6.30 | 0.12 |
| HG | ||||||||
| 1 or 2 | 117 | 14 | 1 | 1 | ||||
| 3 | 134 | 16 | 1.04 | 0.51–2.13 | 0.919 | 1.24 | 0.59–2.63 | 0.57 |
| HER2 heterogeneity | ||||||||
| Low (LH) | 205 | 17 | 1 | 1 | ||||
| High (HH) | 46 | 13 | 3.8 | 1.84–7.83 | 2.95 × 10−4 | 4.03 | 1.83–8.87 | 5.51 × 10−4 |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | N | Event (N) | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| cT | ||||||||
| T1 | 86 | 8 | 1 | 1 | ||||
| T2–T4 | 165 | 22 | 2.22 | 0.63–7.78 | 0.214 | 1.44 | 0.39–5.24 | 0.584 |
| ER | ||||||||
| Positive | 167 | 20 | 1 | 1 | ||||
| Negative | 84 | 10 | 0.67 | 0.22–2.07 | 0.485 | 0.78 | 0.21–2.94 | 0.715 |
| PgR | ||||||||
| Positive | 99 | 14 | 1 | 1 | ||||
| Negative | 152 | 16 | 0.88 | 0.33–2.36 | 0.797 | 1.67 | 0.53–5.26 | 0.382 |
| Pretreatment LN metastasis | ||||||||
| Negative | 134 | 10 | 1 | 1 | ||||
| Positive | 117 | 20 | 4.84 | 1.38–16.99 | 0.014 | 2.79 | 0.61–12.90 | 0.188 |
| Resected LN metastasis | ||||||||
| Negative | 185 | 16 | 1 | 1 | ||||
| Positive | 66 | 14 | 3.71 | 1.38–9.96 | 0.009 | 1.83 | 0.53–6.26 | 0.336 |
| HG | ||||||||
| 1 or 2 | 117 | 14 | 1 | 1 | ||||
| 3 | 134 | 16 | 0.7 | 0.26–1.88 | 0.482 | 0.84 | 0.31–2.33 | 0.745 |
| HER2 heterogeneity | ||||||||
| Low (LH) | 205 | 17 | 1 | 1 | ||||
| High (HH) | 46 | 13 | 3.55 | 1.32–9.54 | 0.012 | 3.1 | 1.06–9.08 | 0.039 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanei, T.; Seno, S.; Sota, Y.; Hatano, T.; Kitahara, Y.; Abe, K.; Masunaga, N.; Tsukabe, M.; Yoshinami, T.; Miyake, T.; et al. High HER2 Intratumoral Heterogeneity Is a Predictive Factor for Poor Prognosis in Early-Stage and Locally Advanced HER2-Positive Breast Cancer. Cancers 2024, 16, 1062. https://doi.org/10.3390/cancers16051062
Tanei T, Seno S, Sota Y, Hatano T, Kitahara Y, Abe K, Masunaga N, Tsukabe M, Yoshinami T, Miyake T, et al. High HER2 Intratumoral Heterogeneity Is a Predictive Factor for Poor Prognosis in Early-Stage and Locally Advanced HER2-Positive Breast Cancer. Cancers. 2024; 16(5):1062. https://doi.org/10.3390/cancers16051062
Chicago/Turabian StyleTanei, Tomonori, Shigeto Seno, Yoshiaki Sota, Takaaki Hatano, Yuri Kitahara, Kaori Abe, Nanae Masunaga, Masami Tsukabe, Tetsuhiro Yoshinami, Tomohiro Miyake, and et al. 2024. "High HER2 Intratumoral Heterogeneity Is a Predictive Factor for Poor Prognosis in Early-Stage and Locally Advanced HER2-Positive Breast Cancer" Cancers 16, no. 5: 1062. https://doi.org/10.3390/cancers16051062
APA StyleTanei, T., Seno, S., Sota, Y., Hatano, T., Kitahara, Y., Abe, K., Masunaga, N., Tsukabe, M., Yoshinami, T., Miyake, T., Shimoda, M., Matsuda, H., & Shimazu, K. (2024). High HER2 Intratumoral Heterogeneity Is a Predictive Factor for Poor Prognosis in Early-Stage and Locally Advanced HER2-Positive Breast Cancer. Cancers, 16(5), 1062. https://doi.org/10.3390/cancers16051062