

Artificial-Intelligence-Assisted Detection of Metastatic Colorectal Cancer Cells in Ascitic Fluid
 , ,
, ,  , , , , and
, , , , and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
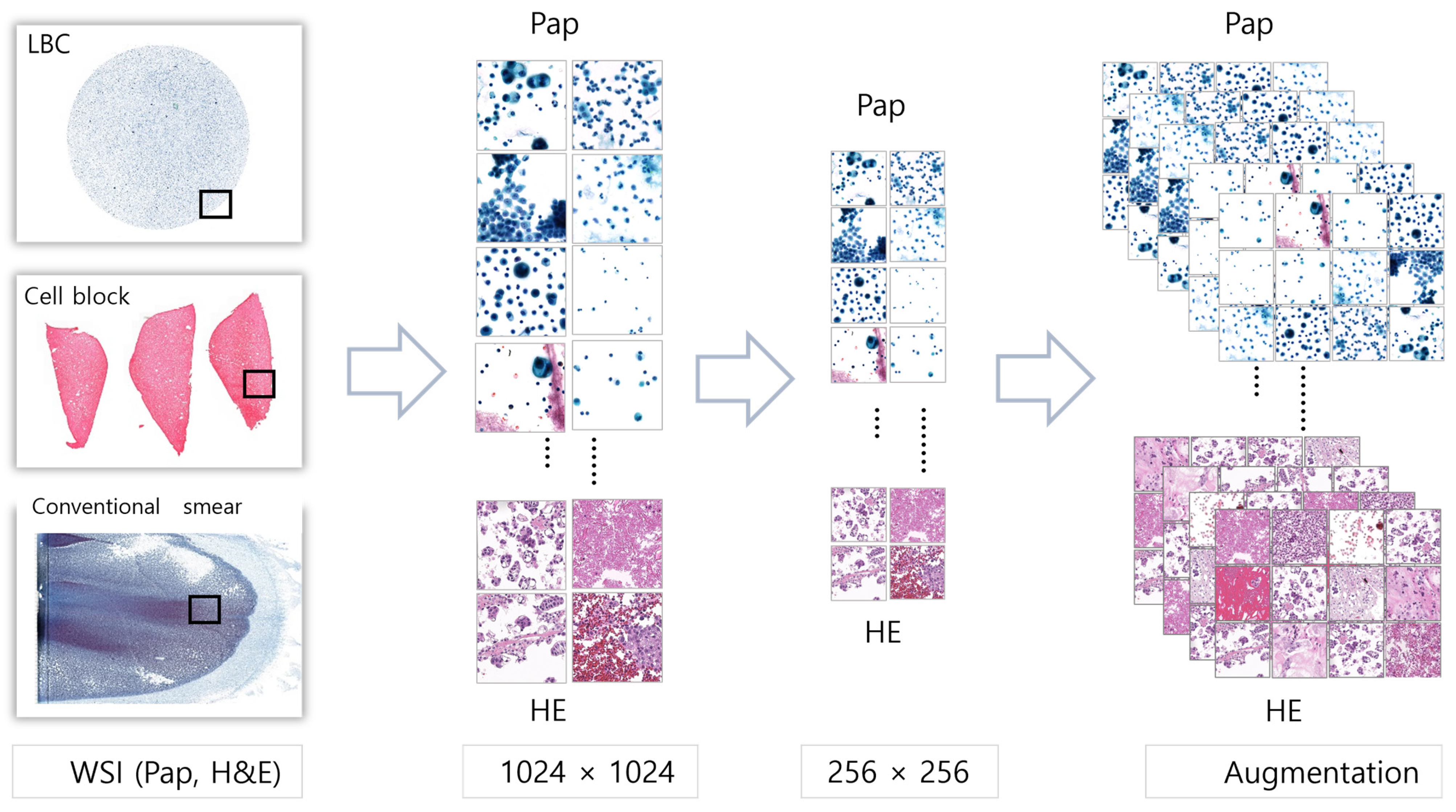
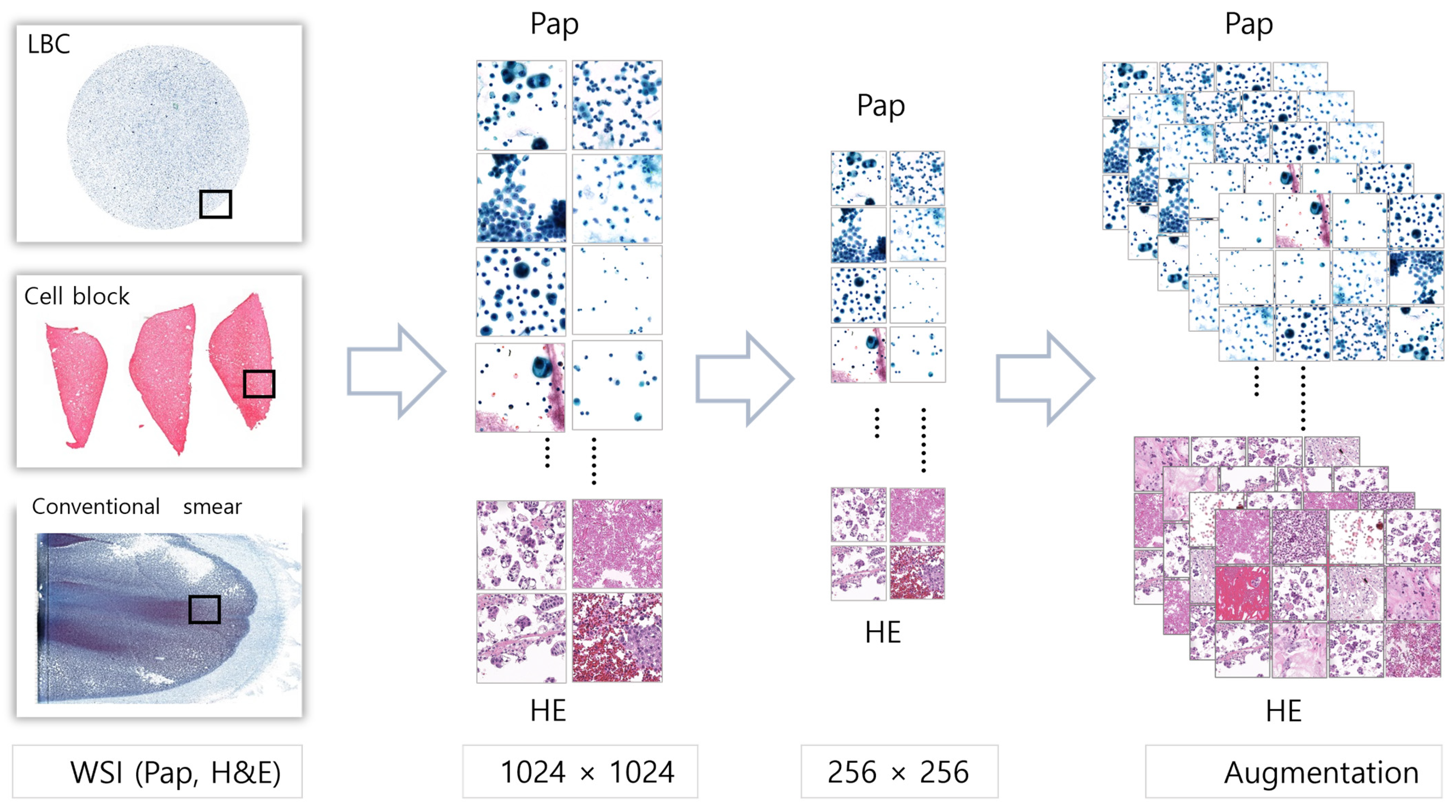
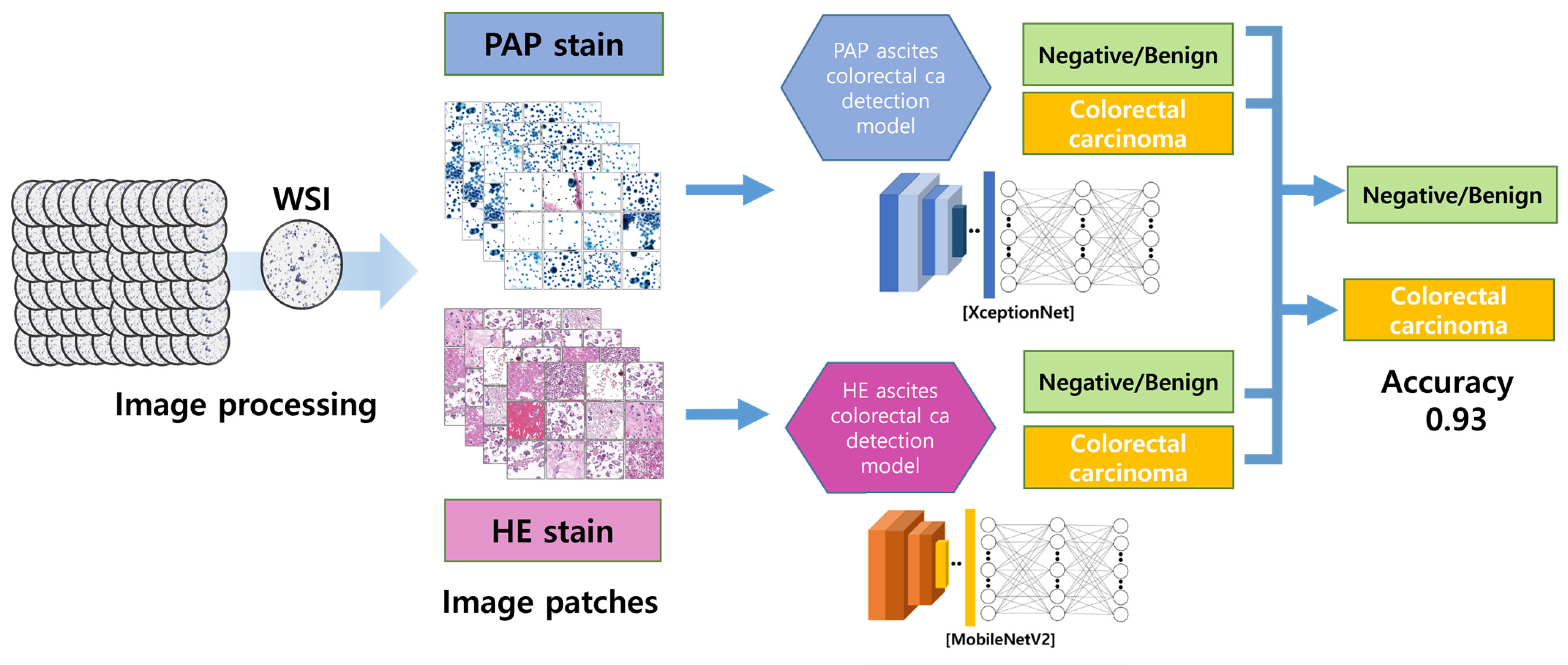
2.1. Image Processing
2.2. Data Distributions
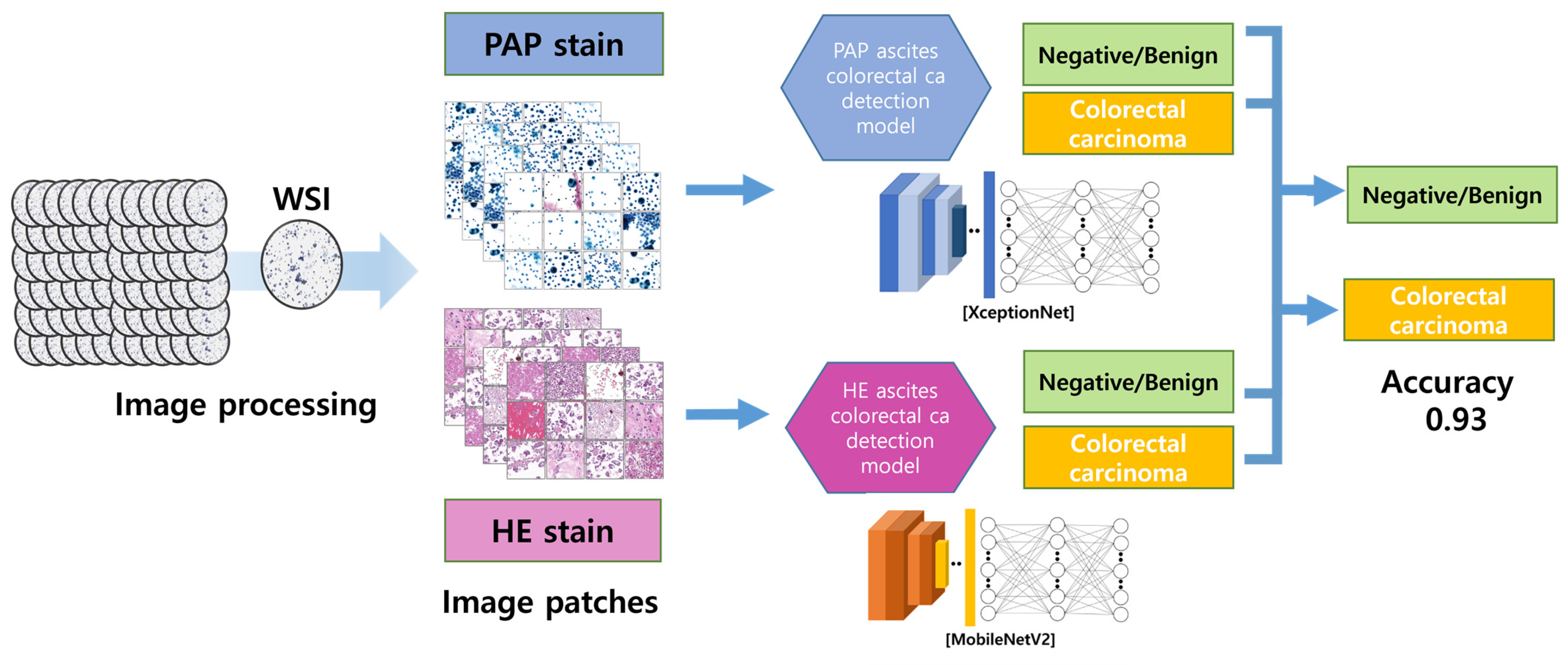
2.3. Deep Convolutional Neural Networking (DCNN) Model Training
2.4. Random Patch Image Comparison between Pathologists and the AI Model
2.5. Statistical Analysis
3. Results
3.1. Pretest for AI Model Selection
3.2. AI Model Results
3.3. Random Patch Image Comparison between Pathologists and the AI Model
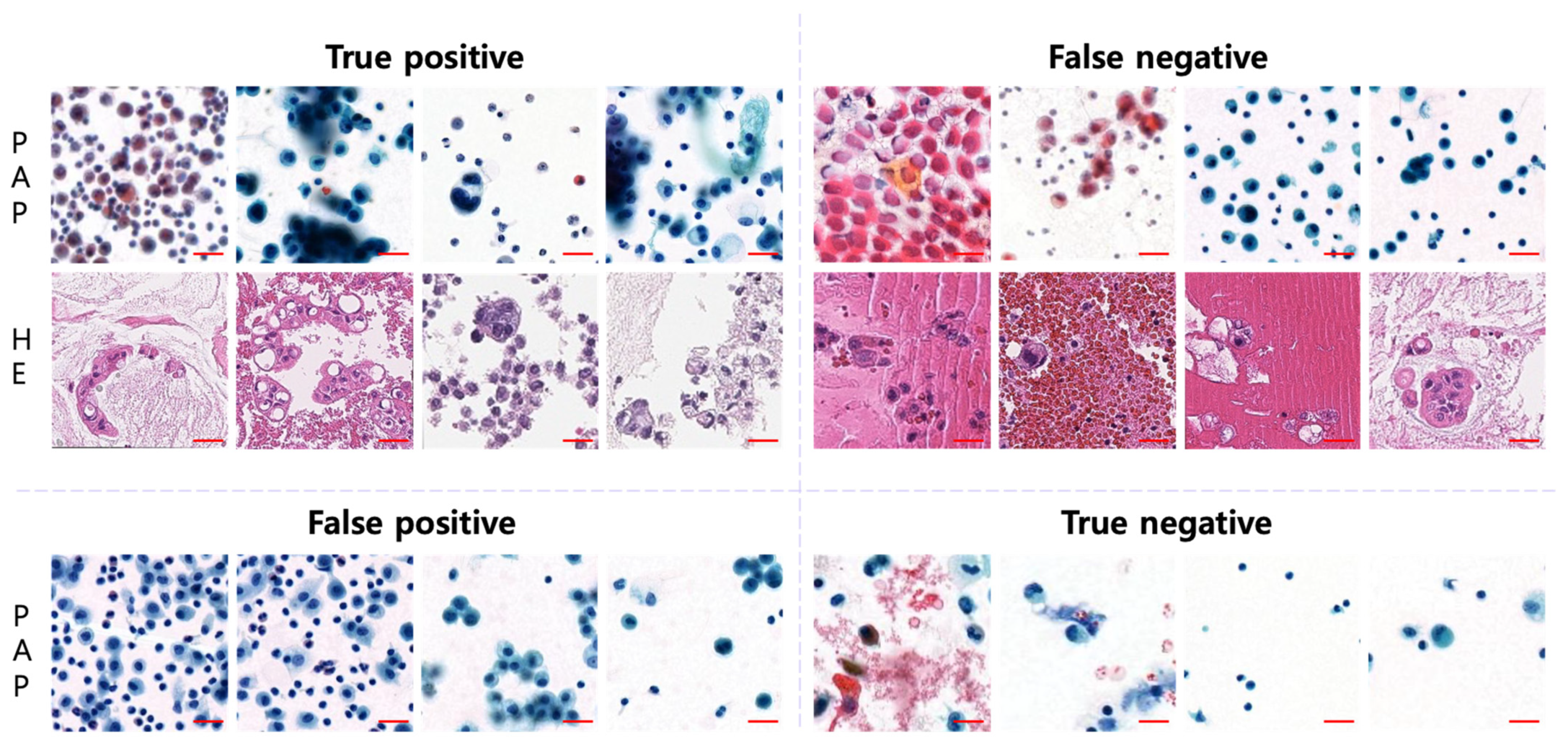
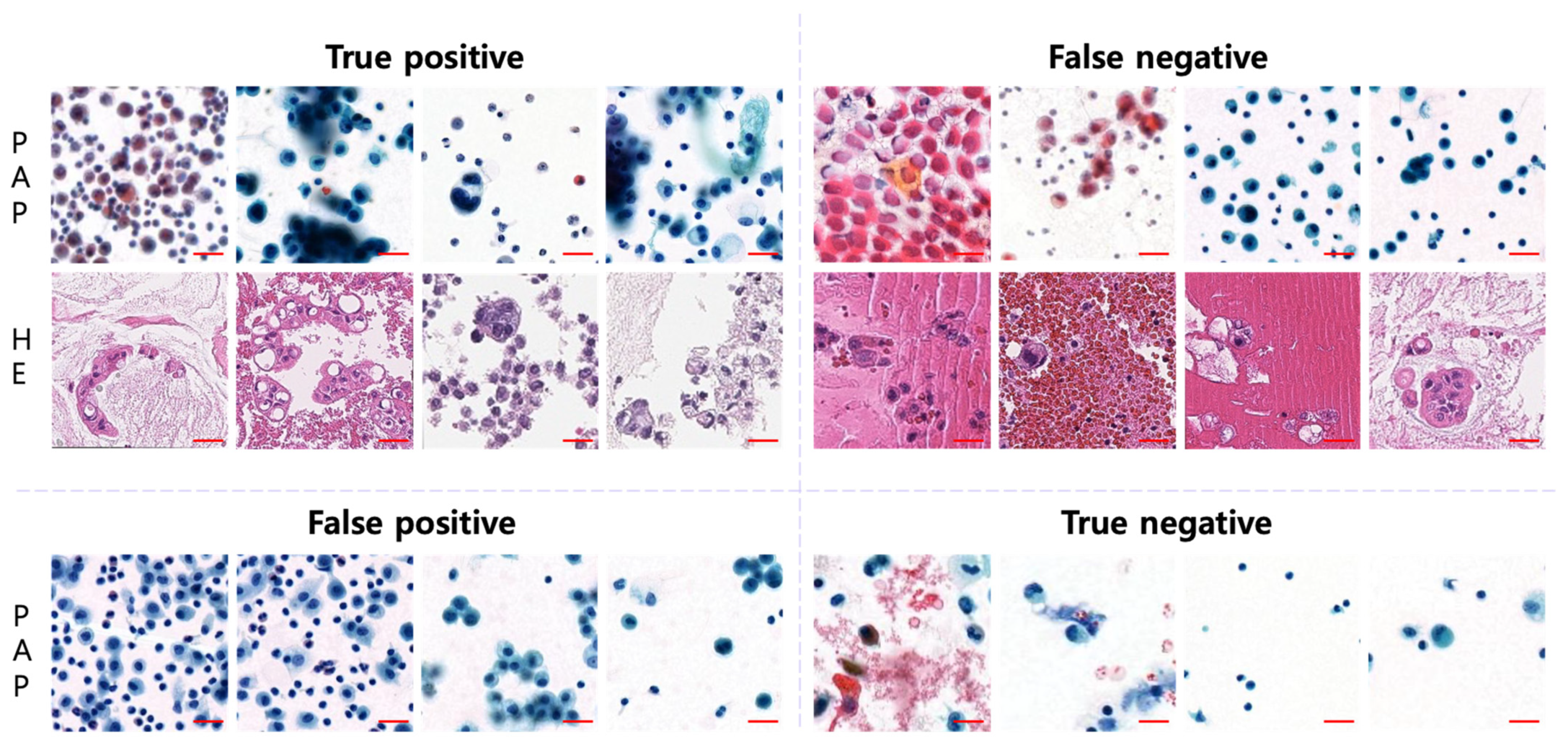
3.4. AI-Diagnosed Patch Images
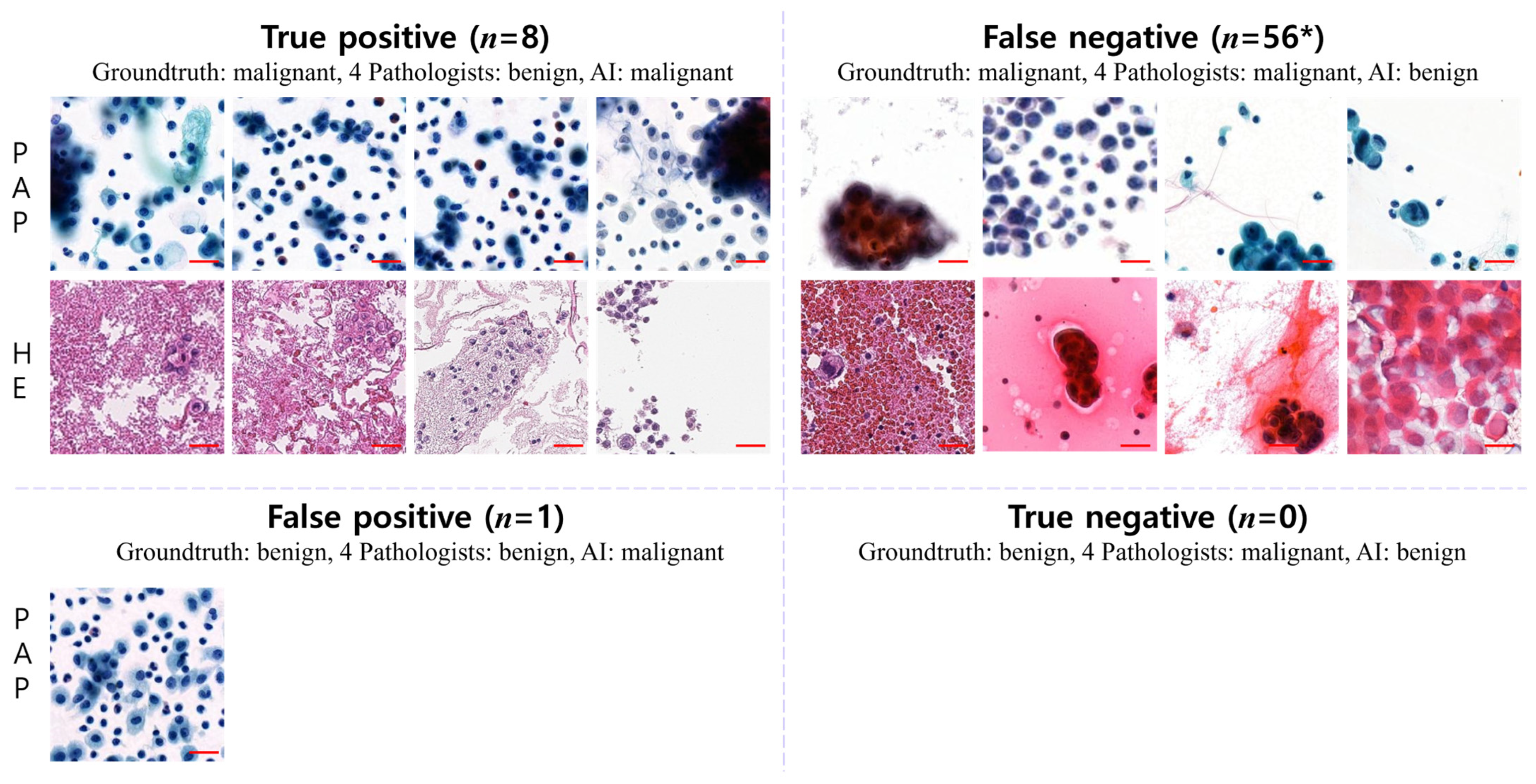
3.5. Disagreement between Pathologists and AI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kranenburg, O.; van der Speeten, K.; de Hingh, I. Peritoneal metastases from colorectal cancer: Defining and addressing the challenges. Front. Oncol. 2021, 11, 650098. [Google Scholar] [CrossRef]
- Daskalakis, A.; Kostopoulos, S.; Spyridonos, P.; Glotsos, D.; Ravazoula, P.; Kardari, M.; Kalatzis, I.; Cavouras, D.; Nikiforidis, G. Design of a multi-classifier system for discriminating benign from malignant thyroid nodules using routinely H&E-stained cytological images. Comput. Biol. Med. 2008, 38, 196–203. [Google Scholar]
- Poloz, T.; Shkurupiĭ, V.; Poloz, V.; Demin, A. The results of quantitative cytological analysis of the structure of follicular thyroid tumors using computer and neural network technologies. Vestn. Ross. Akad. Meditsinskikh Nauk 2006, 8, 7–10. [Google Scholar]
- Thakur, N.; Alam, M.R.; Abdul-Ghafar, J.; Chong, Y. Recent application of artificial intelligence in non-gynecological cancer cytopathology: A systematic review. Cancers 2022, 14, 3529. [Google Scholar] [CrossRef]
- Alam, M.R.; Abdul-Ghafar, J.; Yim, K.; Thakur, N.; Lee, S.H.; Jang, H.-J.; Jung, C.K.; Chong, Y. Recent applications of artificial intelligence from histopathologic image-based prediction of microsatellite instability in solid cancers: A systematic review. Cancers 2022, 14, 2590. [Google Scholar] [CrossRef]
- Feng, H.; Yang, B.; Wang, J.; Liu, M.; Yin, L.; Zheng, W.; Yin, Z.; Liu, C. Identifying malignant breast ultrasound images using ViT-patch. Appl. Sci. 2023, 13, 3489. [Google Scholar] [CrossRef]
- Zhuang, Y.; Chen, S.; Jiang, N.; Hu, H. An Effective WSSENet-Based Similarity Retrieval Method of Large Lung CT Image Databases. KSII Trans. Internet Inf. Syst. 2022, 16, p2359. [Google Scholar]
- Alam, M.R.; Seo, K.J.; Abdul-Ghafar, J.; Yim, K.; Lee, S.H.; Jang, H.-J.; Jung, C.K.; Chong, Y. Recent application of artificial intelligence on histopathologic image-based prediction of gene mutation in solid cancers. Brief. Bioinform. 2023, 24, bbad151. [Google Scholar] [CrossRef]
- Xie, X.; Fu, C.-C.; Lv, L.; Ye, Q.; Yu, Y.; Fang, Q.; Zhang, L.; Hou, L.; Wu, C. Deep convolutional neural network-based classification of cancer cells on cytological pleural effusion images. Mod. Pathol. 2022, 35, 609–614. [Google Scholar] [CrossRef]
- Park, H.S.; Chong, Y.; Lee, Y.; Yim, K.; Seo, K.J.; Hwang, G.; Kim, D.; Gong, G.; Cho, N.H.; Yoo, C.W. Deep learning-based computational cytopathologic diagnosis of metastatic breast carcinoma in pleural fluid. Cells 2023, 12, 1847. [Google Scholar] [CrossRef]
- Subbaiah, R.; Dey, P.; Nijhawan, R. Artificial neural network in breast lesions from fine-needle aspiration cytology smear. Diagn. Cytopathol. 2014, 42, 218–224. [Google Scholar] [CrossRef]
- Sanyal, P.; Mukherjee, T.; Barui, S.; Das, A.; Gangopadhyay, P. Artificial intelligence in cytopathology: A neural network to identify papillary carcinoma on thyroid fine-needle aspiration cytology smears. J. Pathol. Inform. 2018, 9, 43. [Google Scholar] [CrossRef]
- Elliott Range, D.D.; Dov, D.; Kovalsky, S.Z.; Henao, R.; Carin, L.; Cohen, J. Application of a machine learning algorithm to predict malignancy in thyroid cytopathology. Cancer Cytopathol. 2020, 128, 287–295. [Google Scholar] [CrossRef]
- Girolami, I.; Marletta, S.; Pantanowitz, L.; Torresani, E.; Ghimenton, C.; Barbareschi, M.; Scarpa, A.; Brunelli, M.; Barresi, V.; Trimboli, P. Impact of image analysis and artificial intelligence in thyroid pathology, with particular reference to cytological aspects. Cytopathology 2020, 31, 432–444. [Google Scholar] [CrossRef]
- Fragopoulos, C.; Pouliakis, A.; Meristoudis, C.; Mastorakis, E.; Margari, N.; Chroniaris, N.; Koufopoulos, N.; Delides, A.G.; Machairas, N.; Ntomi, V. Radial basis function artificial neural network for the investigation of thyroid cytological lesions. J. Thyroid Res. 2020, 2020, 5464787. [Google Scholar] [CrossRef]
- Kezlarian, B.; Lin, O. Artificial intelligence in thyroid fine needle aspiration biopsies. Acta Cytol. 2021, 65, 324–329. [Google Scholar] [CrossRef]
- Ye, M.; Chen, W.; Cai, B.; Jin, C.; He, X. A convolutional neural network based model for assisting pathological diagnoses on thyroid liquid-based cytology. Zhonghua Bing Li Xue Za Zhi Chin. J. Pathol. 2021, 50, 358–362. [Google Scholar]
- Youn, I.; Lee, E.; Yoon, J.H.; Lee, H.S.; Kwon, M.-R.; Moon, J.; Kang, S.; Kwon, S.K.; Jung, K.Y.; Park, Y.J. Diagnosing thyroid nodules with atypia of undetermined significance/follicular lesion of undetermined significance cytology with the deep convolutional neural network. Sci. Rep. 2021, 11, 20048. [Google Scholar] [CrossRef]
- Patel, K.A.; Anandani, G.; Sharma, B.S.; Parmar, R.A.; Parmar, R. Study of Fine Needle Aspiration Cytology (FNAC) of Thyroid Gland According to the Bethesda System. Cureus 2023, 15, e37371. [Google Scholar] [CrossRef]
- Muralidaran, C.; Dey, P.; Nijhawan, R.; Kakkar, N. Artificial neural network in diagnosis of urothelial cell carcinoma in urine cytology. Diagn. Cytopathol. 2015, 43, 443–449. [Google Scholar] [CrossRef]
- Sanghvi, A.B.; Allen, E.Z.; Callenberg, K.M.; Pantanowitz, L. Performance of an artificial intelligence algorithm for reporting urine cytopathology. Cancer Cytopathol. 2019, 127, 658–666. [Google Scholar] [CrossRef]
- Vaickus, L.J.; Suriawinata, A.A.; Wei, J.W.; Liu, X. Automating the Paris System for urine cytopathology—A hybrid deep-learning and morphometric approach. Cancer Cytopathol. 2019, 127, 98–115. [Google Scholar] [CrossRef]
- Awan, R.; Benes, K.; Azam, A.; Song, T.H.; Shaban, M.; Verrill, C.; Tsang, Y.W.; Snead, D.; Minhas, F.; Rajpoot, N. Deep learning based digital cell profiles for risk stratification of urine cytology images. Cytom. Part A 2021, 99, 732–742. [Google Scholar] [CrossRef]
- Zhang, Z.; Fu, X.; Liu, J.; Huang, Z.; Liu, N.; Fang, F.; Rao, J. Developing a machine learning algorithm for identifying abnormal urothelial cells: A feasibility study. Acta Cytol. 2021, 65, 335–341. [Google Scholar] [CrossRef]
- Lin, Y.-J.; Chao, T.-K.; Khalil, M.-A.; Lee, Y.-C.; Hong, D.-Z.; Wu, J.-J.; Wang, C.-W. Deep learning fast screening approach on cytological whole slides for thyroid cancer diagnosis. Cancers 2021, 13, 3891. [Google Scholar] [CrossRef]
- Barwad, A.; Dey, P.; Susheilia, S. Artificial neural network in diagnosis of metastatic carcinoma in effusion cytology. Cytom. Part B Clin. Cytom. 2012, 82, 107–111. [Google Scholar] [CrossRef]
- Su, F.; Sun, Y.; Hu, Y.; Yuan, P.; Wang, X.; Wang, Q.; Li, J.; Ji, J.-F. Development and validation of a deep learning system for ascites cytopathology interpretation. Gastric Cancer 2020, 23, 1041–1050. [Google Scholar] [CrossRef]
- Tizhoosh, H.R.; Pantanowitz, L. Artificial intelligence and digital pathology: Challenges and opportunities. J. Pathol. Inform. 2018, 9, 38. [Google Scholar] [CrossRef]
- Thakur, N.; Yoon, H.; Chong, Y. Current trends of artificial intelligence for colorectal cancer pathology image analysis: A systematic review. Cancers 2020, 12, 1884. [Google Scholar] [CrossRef]
- Kim, H.; Yoon, H.; Thakur, N.; Hwang, G.; Lee, E.J.; Kim, C.; Chong, Y. Deep learning-based histopathological segmentation for whole slide images of colorectal cancer in a compressed domain. Sci. Rep. 2021, 11, 22520. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training | Validation | Testing | Total | ||
|---|---|---|---|---|---|
| PAP | Negative | 281 (10,828) | 35 (1353) | 35 (1355) | 351 (13,536) |
| Positive | 33 (10,828) | 4 (1353) | 4 (1332) | 41 (13,513) | |
| Total | 314 (21,656) | 49 (2706) | 39 (2687) | 392 (27,049) | |
| H&E | Negative | 120 (17,452) | 15 (2181) | 15 (1903) | 150 (21,536) |
| Positive | 31 (17,452) | 4 (2181) | 4 (1944) | 39 (21,577) | |
| Total | 151 (34,904) | 19 (4362) | 19 (3847) | 189 (43,113) |
| PAP (xceptionNet) | H&E (mobilenetv2) | |||||
|---|---|---|---|---|---|---|
| Accuracy | Sensitivity | Specificity | Accuracy | Sensitivity | Specificity | |
| Training | 1.0000 | - | - | 1.0000 | - | - |
| Validation | 0.9424 | 0.8973 | 0.9874 | 0.9603 | 0.9207 | 1.0000 |
| Test | 0.8954 | 0.7890 | 1.0000 | 0.9667 | 0.9383 | 0.9958 |
| PAP and HE | ||||||
| Accuracy | Sensitivity | Specificity | ||||
| Training | - | - | - | |||
| Validation | 0.9535 | 0.9117 | 0.9952 | |||
| Test | 0.9374 | 0.8776 | 0.9975 | |||
| Pathologist | Pathologist with AI | AI | |||||
|---|---|---|---|---|---|---|---|
| A | B | C | D | Average | |||
| Sensitivity | 70.5% | 53.9% | 77.1% | 91.7% | 73.3% | 79.3% | 68.6% |
| Specificity | 96.3% | 99.8% | 94.7% | 84.0% | 93.7% | 94.8% | 97.5% |
| Accuracy | 86.6% | 79.6% | 89.3% | 91.5% | 86.8% | 90.5% | 86.2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.K.; Han, E.; Lee, J.; Yim, K.; Abdul-Ghafar, J.; Seo, K.J.; Seo, J.W.; Gong, G.; Cho, N.H.; Kim, M.; et al. Artificial-Intelligence-Assisted Detection of Metastatic Colorectal Cancer Cells in Ascitic Fluid. Cancers 2024, 16, 1064. https://doi.org/10.3390/cancers16051064
Kim HK, Han E, Lee J, Yim K, Abdul-Ghafar J, Seo KJ, Seo JW, Gong G, Cho NH, Kim M, et al. Artificial-Intelligence-Assisted Detection of Metastatic Colorectal Cancer Cells in Ascitic Fluid. Cancers. 2024; 16(5):1064. https://doi.org/10.3390/cancers16051064
Chicago/Turabian StyleKim, Hyung Kyung, Eunkyung Han, Jeonghyo Lee, Kwangil Yim, Jamshid Abdul-Ghafar, Kyung Jin Seo, Jang Won Seo, Gyungyub Gong, Nam Hoon Cho, Milim Kim, and et al. 2024. "Artificial-Intelligence-Assisted Detection of Metastatic Colorectal Cancer Cells in Ascitic Fluid" Cancers 16, no. 5: 1064. https://doi.org/10.3390/cancers16051064
APA StyleKim, H. K., Han, E., Lee, J., Yim, K., Abdul-Ghafar, J., Seo, K. J., Seo, J. W., Gong, G., Cho, N. H., Kim, M., Yoo, C. W., & Chong, Y. (2024). Artificial-Intelligence-Assisted Detection of Metastatic Colorectal Cancer Cells in Ascitic Fluid. Cancers, 16(5), 1064. https://doi.org/10.3390/cancers16051064