
Trap-Door Thoracotomy and Clamshell Thoracotomy as Surgical Approaches for Neuroblastoma and Other Thoracic Tumors in Children

 , , , , and
, , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
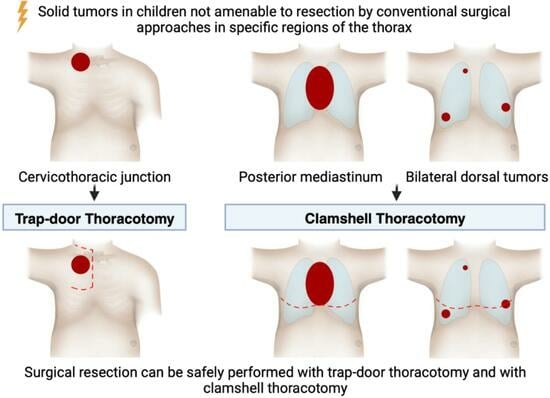
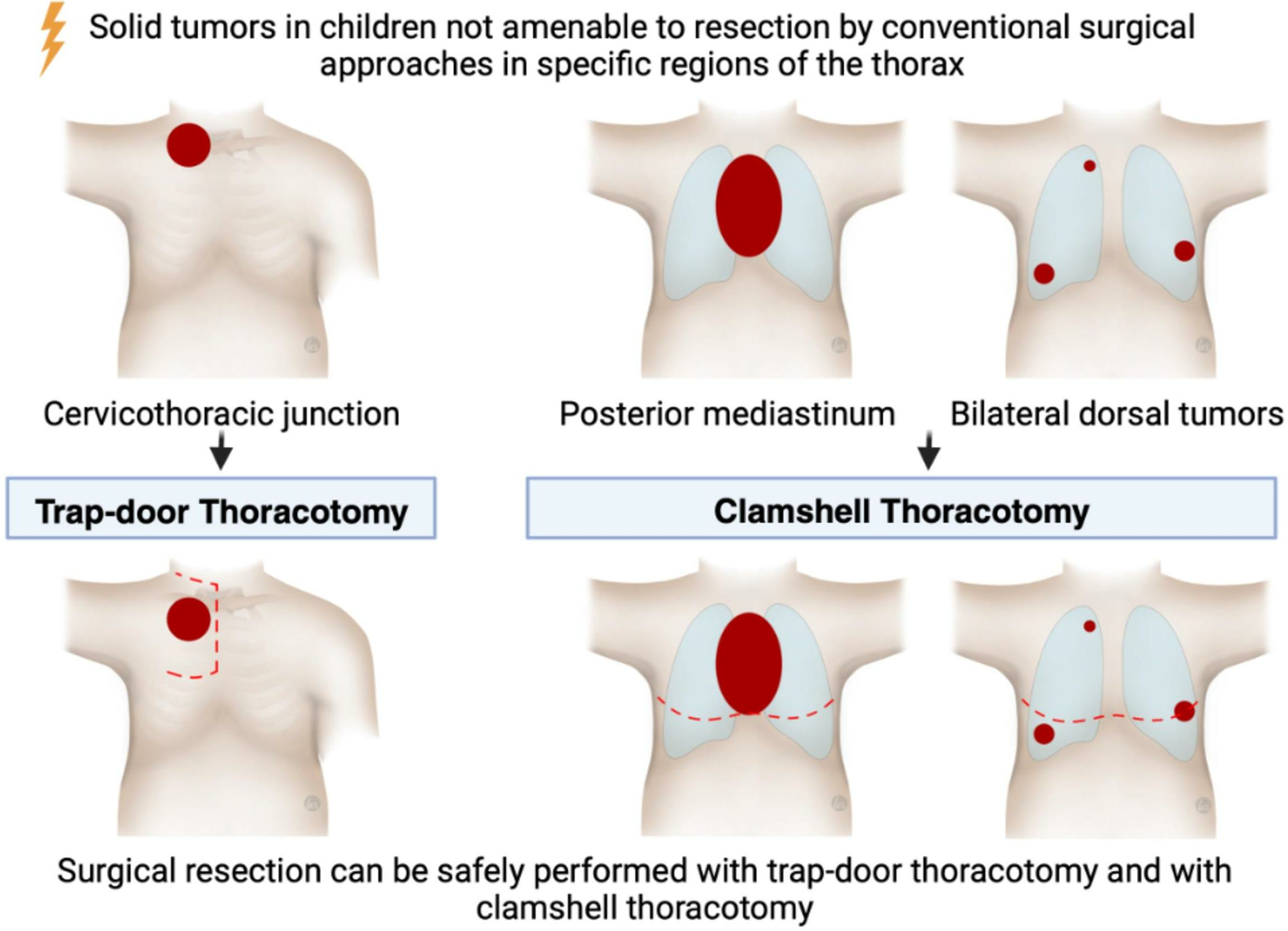
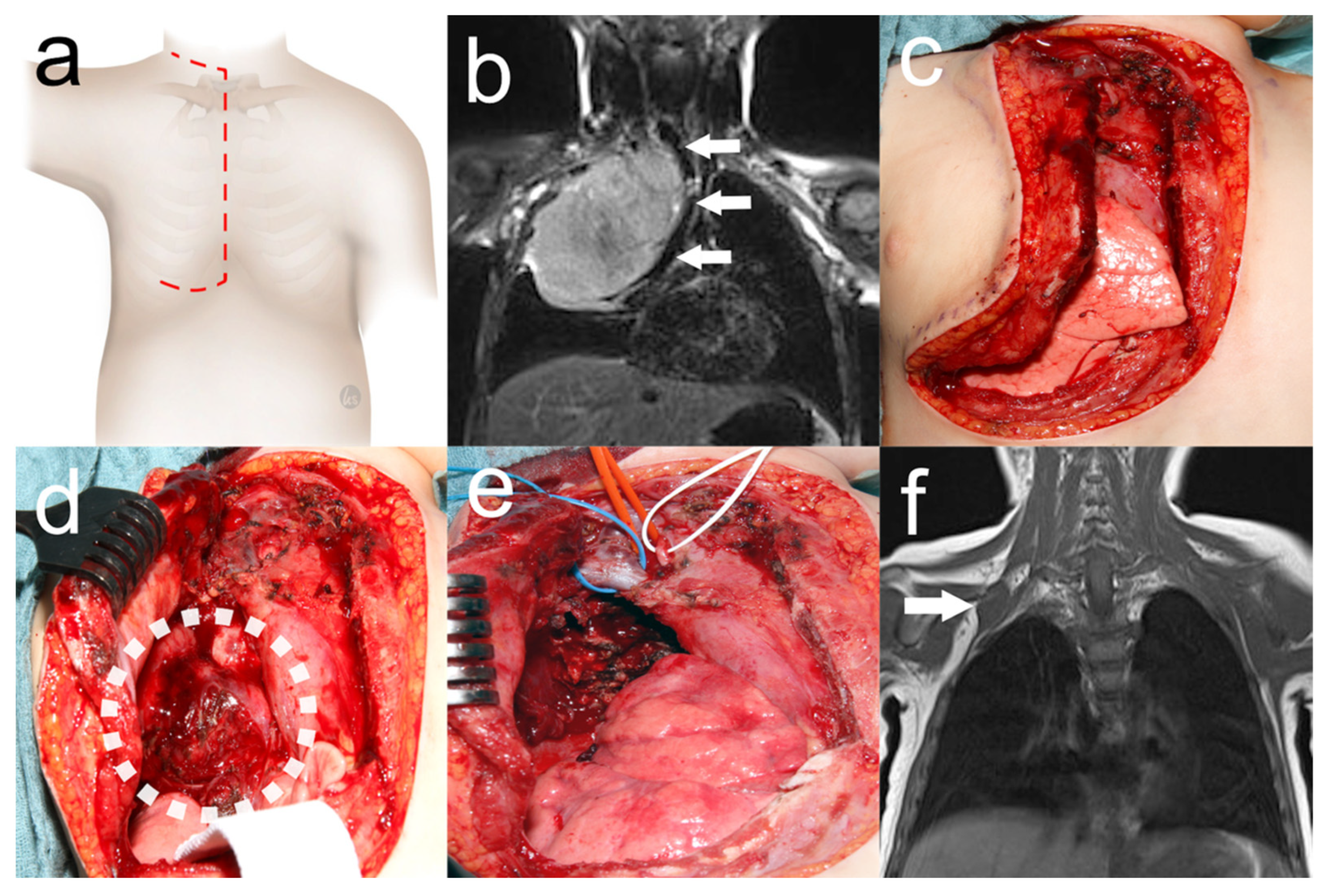
2.2. Trap-Door Thoracotomy
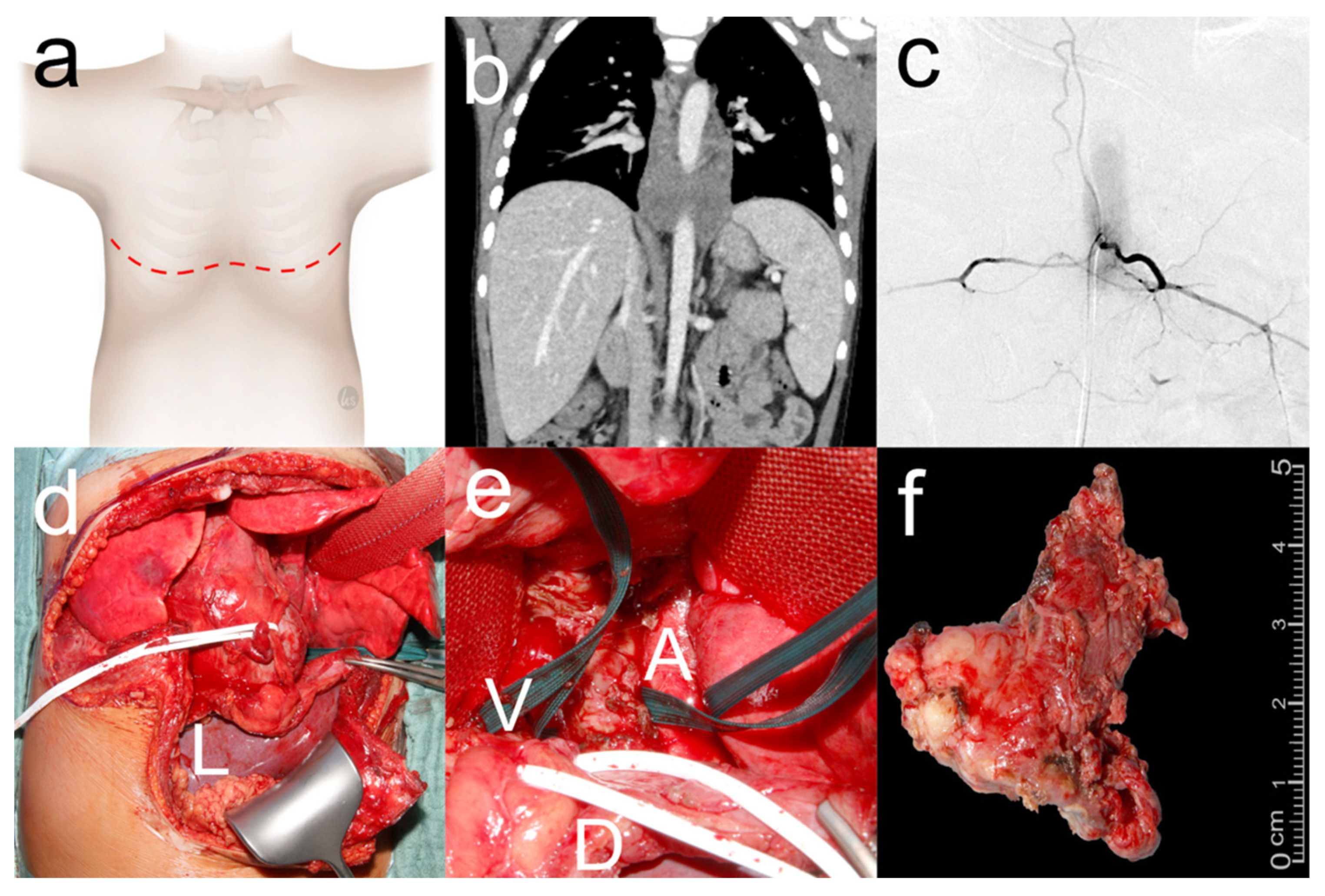
2.3. Clamshell Thoracotomy
2.4. Demographic and Clinical Characteristics
2.5. Surgical and Oncological Data
2.6. Statistical Analysis
3. Results
3.1. Trap-Door Thoracotomy
3.2. Clamshell Thoracotomy

{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 26) | Trap-Door (n = 14) | Clamshell (n = 12) |
|---|---|---|---|
| Operative time [minutes] * | 197 (104–424) | 207 (122–424) | 179 (104–381) |
| Resection with neurosurgery [n] | 7 (26.9%) | 7 (26.9%) | 0 |
| Intermittent neuromonitoring [n] | 8 (30.8%) | 8 (30.8%) | 0 |
| Resection status | |||
| MCE (neuroblastoma) ** | 11 (42.3%) | 7 (26.9%) | 4 (15.4%) |
| R0 resection (other tumors) | 14 (53.9%) | 7 (26.9%) | 7 (26.9%) |
| MCE (all tumor entities) ** | 25 (96.2%) | 14 (53.8%) | 11 (42.3%) |
| Biopsy | 1 (3.9%) | 0 | 1 (3.9%) |
| Duration of ventilation [days] * | 1 (0–6) | 1 (0–5) | 1 (0–6) |
| Duration of chest tube [days] * | 6 (1–14) | 6 (3–11) | 6 (1–14) |
| Length of ICU stay [days] * | 2 (1–12) | 3 (1–12) | 2 (1–8) |
| Length of hospital stay [days] * | 10 (6–35) | 9 (6–22) | 14 (7–35) |
| Complications [n] *** | 17 (54.2%) | 9 (25%) | 8 (29.2%) |
| 7 (26.9%) | 7 (26.9%) | 0 |
| Diaphragm paresis | 6 (23.1%) | 5 (19.2%) | 1 (3.9%) |
| Pleural effusion | 3 (11.5%) | 2 (7.7%) | 1 (3.9%) |
| Paresis after nerve resection | 3 (11.5%) | 3 (11.5%) | 0 |
| 2 (7.7%) | 2 (7.7%) | 0 |
| 2 (7.7%) | 0 | 2 (7.7%) |
| Pleural effusion | 1 (3.9%) | 0 | 1 (3.9%) |
| Chest wall hematoma | 1 (3.9%) | 1 (3.9%) | 0 |
| Pathology result differs from biopsy [n] | 8 (30.8%) | 6 (23.1%) | 2 (7.7%) |
| Adjuvant chemotherapy [n] | 18 (69.2%) | 8 (30.8%) | 10 (38.5%) |
| Adjuvant radiotherapy [n] | 5 (19.2%) | 3 (11.5%) | 2 (7.7%) |
| Follow-up [months] * | 8 (0–60) | 10 (5–21) | 7 (0–60) |
| Lost to follow-up | 9 (34.6%) | 4 (15.4%) | 4 (15.5%) |
| Tumor recurrence [n] | 7 (38.8%) | 4 (22.2%) | 3 (16.7%) |
| Oncological outcome [n] | |||
| Complete remission | 6 (33.3%) | 4 (22.2%) | 3 (16.7%) |
| Local control | 5 (27.8%) | 4 (22.2%) | 1 (5.6%) |
| Progress | 2 (11.1%) | 1 (5.6%) | 1 (5.6%) |
| Death | 4 (22.2%) | 1 (5.6%) | 3 (16.7%) |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Häcker, F.-M.; Schweinitz, D.V.; Gambazzi, F. The Relevance of Surgical Therapy for Bilateral and/or Multiple Pulmonary Metastases in Children. Eur. J. Pediatr. Surg. 2007, 17, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Zarroug, A.E.; Hamner, C.E.; Pham, T.H.; Houghton, S.G.; Stavlo, P.; Moir, C.R.; Rodeberg, D.A. Bilateral Staged versus Bilateral Simultaneous Thoracotomy in the Pediatric Population. J. Pediatr. Surg. 2006, 41, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Kiely, E. A Technique for Excision of Abdominal and Pelvic Neuroblastomas. Annals 2007, 89, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, J.; Urla, C.; Sparber-Sauer, M.; Schuck, A.; Leuschner, I.; Klingebiel, T.; Blumenstock, G.; Seitz, G.; Koscielniak, E. Treatment and Outcome of Patients with Localized Intrathoracic and Chest Wall Rhabdomyosarcoma: A Report of the Cooperative Weichteilsarkom Studiengruppe (CWS). J. Cancer Res. Clin. Oncol. 2018, 144, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Briccoli, A.; Rocca, M.; Salone, M.; Guzzardella, G.A.; Balladelli, A.; Bacci, G. High Grade Osteosarcoma of the Extremities Metastatic to the Lung: Long-Term Results in 323 Patients Treated Combining Surgery and Chemotherapy, 1985–2005. Surg. Oncol. 2010, 19, 193–199. [Google Scholar] [CrossRef]
- Morgan, K.M.; Siow, V.S.; Strotmeyer, S.; Gow, K.W.; Malek, M.M. Characteristics and Outcomes in Pediatric Non-Central Nervous System Malignant Rhabdoid Tumors: A Report from the National Cancer Database. Ann. Surg. Oncol. 2022, 29, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Tronc, F.; Conter, C.; Marec-Berard, P.; Bossard, N.; Remontet, L.; Orsini, A.; Gamondes, J.-P.; Louis, D. Prognostic Factors and Long-Term Results of Pulmonary Metastasectomy for Pediatric Histologies. Eur. J. Cardio-Thorac. Surg. 2008, 34, 1240–1246. [Google Scholar] [CrossRef]
- Masaoka, A.; Ito, Y.; Yasumitsu, T. Anterior Approach for Tumor of the Superior Sulcus. J. Thorac. Cardiovasc. Surg. 1979, 78, 413–415. [Google Scholar] [CrossRef] [PubMed]
- Lebreton, G.; Baste, J.-M.; Thumerel, M.; Delcambre, F.; Velly, J.-F.; Jougon, J. The Hemiclamshell Approach in Thoracic Surgery: Indications and Associated Morbidity in 50 Patients. Interact. Cardiovasc. Thorac. Surg. 2009, 9, 965–969. [Google Scholar] [CrossRef]
- Dartevelle, P.G.; Chapelier, A.R.; Macchiarini, P.; Lenot, B.; Cerrina, J.; Roy Ladurie, F.L.; Parquin, F.J.F.; Lafont, D.; Deslauriers, J. Anterior Transcervical-Thoracic Approach for Radical Resection of Lung Tumors Invading the Thoracic Inlet. J. Thorac. Cardiovasc. Surg. 1993, 105, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Bains, M.S.; Ginsberg, R.J.; Jones, W.G.; McCormack, P.M.; Rusch, V.W.; Burt, M.E.; Martini, N. The Clamshell Incision: An Improved Approach to Bilateral Pulmonary and Mediastinal Tumor. Ann. Thorac. Surg. 1994, 58, 30–33. [Google Scholar] [CrossRef]
- Abbo, O.; Guatta, R.; Pinnagoda, K.; Joseph, J.-M. Bilateral Anterior Sternothoracotomy (Clamshell Incision): A Suitable Alternative for Bilateral Lung Sarcoma Metastasis in Children. World J. Surg. Onc. 2014, 12, 233. [Google Scholar] [CrossRef]
- Chui, C.H.; Thirugnanam, A. Trapdoor Anterior Thoracotomy for Cervicothoracic and Apical Thoracic Neuroblastoma in Children. Pediatr. Surg. Int. 2020, 36, 891–895. [Google Scholar] [CrossRef] [PubMed]
- De Corti, F.; Avanzini, S.; Cecchetto, G.; Buffa, P.; Guida, E.; Zanon, G.F.; Jasonni, V. The Surgical Approach for Cervicothoracic Masses in Children. J. Pediatr. Surg. 2012, 47, 1662–1668. [Google Scholar] [CrossRef]
- Christison-Lagay, E.R.; Darcy, D.G.; Stanelle, E.J.; DaSilva, S.; Avila, E.; La Quaglia, M.P. “Trap-Door” and “Clamshell” Surgical Approaches for the Management of Pediatric Tumors of the Cervicothoracic Junction and Mediastinum. J. Pediatr. Surg. 2014, 49, 172–177. [Google Scholar] [CrossRef]
- Schmidt, A.; Hempel, J.-M.; Ellerkamp, V.; Warmann, S.W.; Ernemann, U.; Fuchs, J. The Relevance of Preoperative Identification of the Adamkiewicz Artery in Posterior Mediastinal Pediatric Tumors. Ann. Surg. Oncol. 2022, 29, 493–499. [Google Scholar] [CrossRef]
- Brisse, H.J.; McCarville, M.B.; Granata, C.; Krug, K.B.; Wootton-Gorges, S.L.; Kanegawa, K.; Giammarile, F.; Schmidt, M.; Shulkin, B.L.; Matthay, K.K.; et al. Guidelines for Imaging and Staging of Neuroblastic Tumors: Consensus Report from the International Neuroblastoma Risk Group Project. Radiology 2011, 261, 243–257. [Google Scholar] [CrossRef]
- Kiely, E.M. Radical Surgery for Abdominal Neuroblastoma. Semin. Surg. Oncol. 1993, 9, 489–492. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A New Proposal With Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205. [Google Scholar] [CrossRef]
- La Quaglia, M.P.; Kushner, B.H.; Su, W.; Heller, G.; Kramer, K.; Abramson, S.; Rosen, N.; Wolden, S.; Cheung, N.-K.V. The Impact of Gross Total Resection on Local Control and Survival in High-Risk Neuroblastoma. J. Pediatr. Surg. 2004, 39, 412–417; discussion 412–417. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.; Pohl, A.; Volland, R.; Hero, B.; Dübbers, M.; Cernaianu, G.; Berthold, F.; von Schweinitz, D.; Simon, T. Complete Surgical Resection Improves Outcome in INRG High-Risk Patients with Localized Neuroblastoma Older than 18 Months. BMC Cancer 2017, 17, 520. [Google Scholar] [CrossRef]
- Holmes, K.; Pötschger, U.; Pearson, A.D.J.; Sarnacki, S.; Cecchetto, G.; Gomez-Chacon, J.; Squire, R.; Freud, E.; Bysiek, A.; Matthyssens, L.E.; et al. Influence of Surgical Excision on the Survival of Patients with Stage 4 High-Risk Neuroblastoma: A Report from the HR-NBL1/SIOPEN Study. J. Clin. Oncol. 2020, 38, 2902–2915. [Google Scholar] [CrossRef]
- Urla, C.; Warmann, S.W.; Schmidt, A.; Mayer, B.; Handgretinger, R.; Neunhoeffer, F.; Schäfer, J.; Fuchs, J. Two-Cavities Approach for Resection of Pediatric Abdominal Neuroblastic Tumors: Experience of a National Reference Pediatric Onco-Surgical Center. J. Cancer Res. Clin. Oncol. 2023, 149, 1485–1493. [Google Scholar] [CrossRef]
- Weber, T.; Mätzl, J.; Rokitansky, A.; Klimscha, W.; Neumann, K.; Deusch, E. Superior Postoperative Pain Relief with Thoracic Epidural Analgesia versus Intravenous Patient-Controlled Analgesia after Minimally Invasive Pectus Excavatum Repair. J. Thorac. Cardiovasc. Surg. 2007, 134, 865–870. [Google Scholar] [CrossRef] [PubMed]
- El Madi, A.; Irtan, S.; Sauvat, F.; Zérah, M.; Schleiermacher, G.; Galmiche-Roland, L.; Minard-Colin, V.; Brisse, H.; Sarnacki, S. Long-Term Results of the Transmanubrial Osteomuscular-Sparing Approach for Pediatric Tumors. Pediatr. Blood Cancer 2017, 64, e26527. [Google Scholar] [CrossRef]
- Schubert, C.; Grimm, A.-S.; Stahl, J.-H.; Küpper, H.; Kegele, J.; Wittlinger, J.; Serna-Higuita, L.; Winter, N.; Groeschel, S.; Grimm, A. Nerve Ultrasound Reference Data in Children from Two to Seven Years. Clin. Neurophysiol. 2020, 131, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Sala, F.; Kržan, M.J.; Deletis, V. Intraoperative Neurophysiological Monitoring in Pediatric Neurosurgery: Why, When, How? Childs Nerv. Syst. 2002, 18, 264–287. [Google Scholar] [CrossRef] [PubMed]
- Li, W.W.L.; Lee, T.W.; Yim, A.P.C. Shoulder Function after Thoracic Surgery. Thorac. Surg. Clin. 2004, 14, 331–343. [Google Scholar] [CrossRef]
- Sauvat, F.; Brisse, H.; Magdeleinat, P.; Lopez, M.; Philippe-Chomette, P.; Orbach, D.; Aerts, I.; Brugieres, L.; Revillon, Y.; Sarnacki, S. The Transmanubrial Approach: A New Operative Approach to Cervicothoracic Neuroblastoma in Children. Surgery 2006, 139, 109–114. [Google Scholar] [CrossRef]
- Ferrari, A.; Brecht, I.B.; Koscielniak, E.; Casanova, M.; Scagnellato, A.; Bisogno, G.; Alaggio, R.; Cecchetto, G.; Catania, S.; Meazza, C.; et al. The Role of Adjuvant Chemotherapy in Children and Adolescents with Surgically Resected, High-Risk Adult-Type Soft Tissue Sarcomas. Pediatr. Blood Cancer 2005, 45, 128–134. [Google Scholar] [CrossRef]


| Variable | All (n = 26) | Trap-Door (n = 14) | Clamshell (n = 12) |
|---|---|---|---|
| Sex [n] | |||
| Female | 17 (65.4%) | 8 (30.8%) | 9 (34.6%) |
| Male | 9 (34.6%) | 6 (23%) | 3 (11.5%) |
| Median age at diagnosis [months] (range) | 51 (4–205) | 50 (4–151) | 42 (11–205) |
| Tumor entity [n] | |||
| Neuroblastoma | 12 (46.2%) | 6 (23.1%) | 6 (23.1%) |
| Malignant rhabdoid tumor | 4 (15.4%) | 4 (15.4%) | 0 |
| Ewing sarcoma | 1 (3.9%) | 1 (3.9%) | 0 |
| Rhabdomyosarcoma | 1 (3.9%) | 0 | 1 (3.9%) |
| Inflammatory myofibroblastic tumor | 1 (3.9%) | 1 (3.9%) | 0 |
| Metastatic disease | 7 (26.9%) | 1 (3.9%) | 6 (23.1%) |
| Osteosarcoma | 3 (11.5%) | 1 (3.9%) | 2 (7.7%) |
| Neuroblastoma | 1 (3.9%) | 0 | 1 (3.9%) |
| Malignant rhabdoid tumor | 1 (3.9%) | 0 | 1 (3.9%) |
| Hepatoblastoma | 1 (3.9%) | 0 | 1 (3.9%) |
| Renal clear cell sarcoma | 1 (3.9%) | 0 | 1 (3.9%) |
| Tumor localization [n] | |||
| Mediastinum | 12 (46.2%) | 4 (15.4%) | 8 (29.2%) |
| Cervicothoracic junction | 6 (23.1%) | 6 (23.1%) | 0 |
| Thoracic inlet | 4 (15.4%) | 4 (15.4%) | 0 |
| Bilateral dorsal thorax | 4 (15.4%) | 0 | 4 (15.4%) |
| Affected structures [n] | |||
| Major vessels encased | 21 (80.8%) | 12 (46.2%) | 9 (34.6%) |
| Nerves and neuroforamina | 16 (61.5%) | 12 (46.2%) | 4 (15.4%) |
| Trachea and bronchi | 7 (26.9%) | 3 (11.5%) | 4 (15.4%) |
| Esophagus | 7 (26.9%) | 2 (7.7%) | 5 (19.2%) |
| Pericardium | 5 (19.2%) | 1 (3.9%) | 4 (15.4%) |
| Preoperative symptoms [n] | 11 (42.3%) | 8 (30.8%) | 3 (11.5%) |
| Horner syndrome | 3 (11.5%) | 3 (11.5%) | 0 |
| Respiratory insufficiency | 3 (11.5%) | 1 (3.9%) | 2 (8.3%) |
| Paresis upper limb | 2 (7.7%) | 2 (7.7%) | 0 |
| Pain upper limb | 2 (7.7%) | 2 (7.7%) | 0 |
| Upper inflow congestion | 2 (7.7%) | 1 (3.9%) | 1 (3.9%) |
| Lymph edema upper limb | 1 (3.9%) | 1 (3.9%) | 0 |
| Neoadjuvant chemotherapy [n] | 24 (92.3%) | 13 (50%) | 11 (42.3%) |
| Preoperative imaging [n] | |||
| Magnetic resonance imaging | 21 (80.8%) | 13 (50%) | 8 (30.8%) |
| Computed tomography | 12 (46.2%) | 3 (11.5%) | 9 (34.6%) |
| Spinal angiography | 7 (26.9%) | 2 (7.7%) | 5 (19.2%) |
| Ultrasound of peripheral nerve | 3 (11.5%) | 3 (11.5%) | 0 |
| Cerebral angiography | 1 (3.9%) | 1 (3.9%) | 0 |
| Median age at surgery [months] (range) | 54 (8–229) | 54 (8–176) | 53 (18–229) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mayer, B.F.B.; Schunn, M.C.; Urla, C.; Schäfer, J.F.; Fideler, F.; Neunhoeffer, F.; Schuhmann, M.U.; Warmann, S.W.; Fuchs, J. Trap-Door Thoracotomy and Clamshell Thoracotomy as Surgical Approaches for Neuroblastoma and Other Thoracic Tumors in Children. Cancers 2024, 16, 373. https://doi.org/10.3390/cancers16020373
Mayer BFB, Schunn MC, Urla C, Schäfer JF, Fideler F, Neunhoeffer F, Schuhmann MU, Warmann SW, Fuchs J. Trap-Door Thoracotomy and Clamshell Thoracotomy as Surgical Approaches for Neuroblastoma and Other Thoracic Tumors in Children. Cancers. 2024; 16(2):373. https://doi.org/10.3390/cancers16020373
Chicago/Turabian StyleMayer, Benjamin F. B., Matthias C. Schunn, Cristian Urla, Jürgen F. Schäfer, Frank Fideler, Felix Neunhoeffer, Martin U. Schuhmann, Steven W. Warmann, and Jörg Fuchs. 2024. "Trap-Door Thoracotomy and Clamshell Thoracotomy as Surgical Approaches for Neuroblastoma and Other Thoracic Tumors in Children" Cancers 16, no. 2: 373. https://doi.org/10.3390/cancers16020373
APA StyleMayer, B. F. B., Schunn, M. C., Urla, C., Schäfer, J. F., Fideler, F., Neunhoeffer, F., Schuhmann, M. U., Warmann, S. W., & Fuchs, J. (2024). Trap-Door Thoracotomy and Clamshell Thoracotomy as Surgical Approaches for Neuroblastoma and Other Thoracic Tumors in Children. Cancers, 16(2), 373. https://doi.org/10.3390/cancers16020373