
A Preparatory Virtual Reality Experience Reduces Anxiety before Surgery in Gynecologic Oncology Patients: A Randomized Controlled Trial


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Procedure
2.4. Virtual Reality Intervention
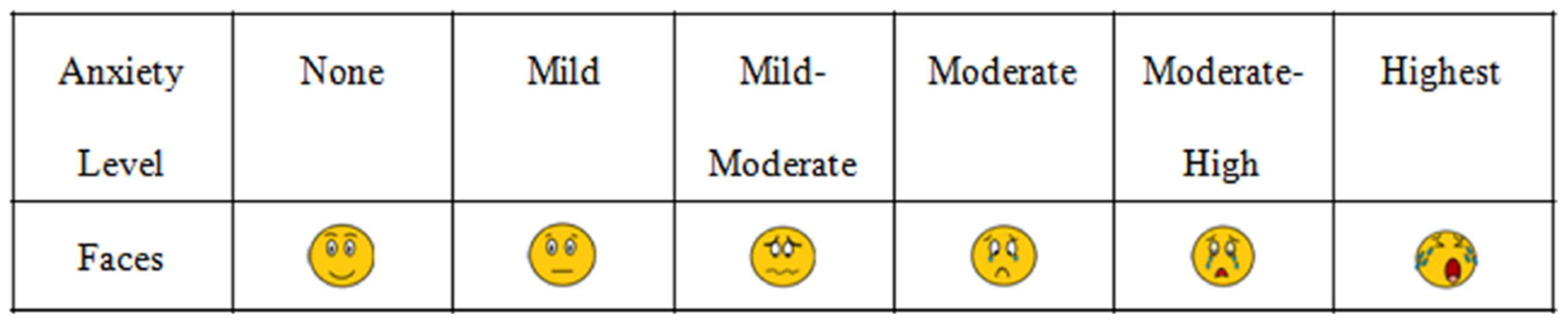
2.5. Assessment Tool
2.6. Statistics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eberhart, L.; Aust, H.; Schuster, M.; Sturm, T.; Gehling, M.; Euteneuer, F.; Rusch, D. Preoperative anxiety in adults—A cross-sectional study on specific fears and risk factors. BMC Psychiatry 2020, 20, 140. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.M.K.; Bell, M.; Cook, T.M.; Grocott, M.P.W.; Moonesinghe, S.R.; Central, S.-O.; National Study, G. Patient reported outcome of adult perioperative anaesthesia in the United Kingdom: A cross-sectional observational study. Br. J. Anaesth. 2016, 117, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Norris, W.; Baird, W.L. Pre-operative anxiety: A study of the incidence and aetiology. Br. J. Anaesth. 1967, 39, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, Y.; Baba, S.; Koh, H.; Takagi, H.; Ishihara, H.; Matsuki, A. Anxiolytic effect of preoperative showing of “anesthesia video” for surgical patients. Masui 1993, 42, 611–616. [Google Scholar] [PubMed]
- Matthias, A.T.; Samarasekera, D.N. Preoperative anxiety in surgical patients–experience of a single unit. Acta Anaesthesiol. Taiwan. 2012, 50, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Mohan, B.; Kumar, R.; Attri, J.P.; Chatrath, V.; Bala, N. Anesthesiologist’s Role in Relieving Patient’s Anxiety. Anesth. Essays Res. 2017, 11, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Schmid, B.C.; Yuan, R.; Watterson, L.; Yu, J.; Hacker, N. Two case studies of cardiac arrest occurring in medically fit patients undergoing radical hysterectomy for cervical cancer. Gynecol. Oncol. Rep. 2021, 37, 100823. [Google Scholar] [CrossRef] [PubMed]
- Kindler, C.H.; Harms, C.; Amsler, F.; Ihde-Scholl, T.; Scheidegger, D. The visual analog scale allows effective measurement of preoperative anxiety and detection of patients’ anesthetic concerns. Anesth. Analg. 2000, 90, 706–712. [Google Scholar] [CrossRef]
- Wechsler, T.F.; Kumpers, F.; Muhlberger, A. Inferiority or Even Superiority of Virtual Reality Exposure Therapy in Phobias?-A Systematic Review and Quantitative Meta-Analysis on Randomized Controlled Trials Specifically Comparing the Efficacy of Virtual Reality Exposure to Gold Standard in vivo Exposure in Agoraphobia, Specific Phobia, and Social Phobia. Front. Psychol. 2019, 10, 1758. [Google Scholar] [CrossRef]
- Maskey, M.; Lowry, J.; Rodgers, J.; McConachie, H.; Parr, J.R. Reducing specific phobia/fear in young people with autism spectrum disorders (ASDs) through a virtual reality environment intervention. PLoS ONE 2014, 9, e100374. [Google Scholar] [CrossRef]
- Tas, F.Q.; van Eijk, C.A.M.; Staals, L.M.; Legerstee, J.S.; Dierckx, B. Virtual reality in pediatrics, effects on pain and anxiety: A systematic review and meta-analysis update. Paediatr. Anaesth. 2022, 32, 1292–1304. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.H.; Park, S.J.; Park, J.W.; Kim, J.W.; Yoo, H.J.; Kim, T.W.; Hong, J.S.; Han, S.H. Randomized clinical trial of immersive virtual reality tour of the operating theatre in children before anaesthesia. Br. J. Surg. 2017, 104, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Eijlers, R.; Dierckx, B.; Staals, L.M.; Berghmans, J.M.; van der Schroeff, M.P.; Strabbing, E.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Legerstee, J.S.; Utens, E. Virtual reality exposure before elective day care surgery to reduce anxiety and pain in children: A randomised controlled trial. Eur. J. Anaesthesiol. 2019, 36, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Chow, H.; Hon, J.; Chua, W.; Chuan, A. Effect of Virtual Reality Therapy in Reducing Pain and Anxiety for Cancer-Related Medical Procedures: A Systematic Narrative Review. J. Pain Symptom Manag. 2021, 61, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Yumul, R.; Elvir Lazo, O.L.; Friedman, J.; Durra, O.; Zhang, X.; White, P.F. A novel visual facial anxiety scale for assessing preoperative anxiety. PLoS ONE 2017, 12, e0171233. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Turrado, V.; Guzmán, Y.; Jiménez-Lillo, J.; Villegas, E.; de Lacy, F.B.; Blanch, J.; Balibrea, J.M.; Lacy, A. Exposure to virtual reality as a tool to reduce peri-operative anxiety in patients undergoing colorectal cancer surgery: A single-center prospective randomized clinical trial. Surg. Endosc. 2021, 35, 4042–4047. [Google Scholar] [CrossRef]
- Chiu, P.L.; Li, H.; Yap, K.Y.; Lam, K.C.; Yip, P.R.; Wong, C.L. Virtual Reality-Based Intervention to Reduce Preoperative Anxiety in Adults Undergoing Elective Surgery: A Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e2340588. [Google Scholar] [CrossRef]
- Tennant, M.; Anderson, N.; Youssef, G.J.; McMillan, L.; Thorson, R.; Wheeler, G.; McCarthy, M.C. Effects of immersive virtual reality exposure in preparing pediatric oncology patients for radiation therapy. Tech. Innov. Patient Support Radiat. Oncol. 2021, 19, 18–25. [Google Scholar] [CrossRef]
- Varma, A.; Naqvi, W.M.; Mulla, S.; Syed, S.; Thakur, S.; Arora, S.P.; Varma, A.R.; Besekar, S. A Systematic Review of Randomized Controlled Trials on Virtual Reality Application in Pediatric Patients. Cureus 2022, 14, e30543. [Google Scholar] [CrossRef] [PubMed]
- Garrett, B.; Taverner, T.; Masinde, W.; Gromala, D.; Shaw, C.; Negraeff, M. A rapid evidence assessment of immersive virtual reality as an adjunct therapy in acute pain management in clinical practice. Clin. J. Pain 2014, 30, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Gold, J.I.; Belmont, K.A.; Thomas, D.A. The neurobiology of virtual reality pain attenuation. Cyberpsychol. Behav. 2007, 10, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Hecken, J.M.; Halagiera, P.; Rehman, S.; Tempfer, C.B.; Rezniczek, G.A. Virtual Reality for Anxiety Reduction in Women Undergoing Colposcopy: A Randomized Controlled Trial. J. Low. Genit. Tract. Dis. 2023, 27, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Indovina, P.; Barone, D.; Gallo, L.; Chirico, A.; De Pietro, G.; Giordano, A. Virtual Reality as a Distraction Intervention to Relieve Pain and Distress During Medical Procedures: A Comprehensive Literature Review. Clin. J. Pain 2018, 34, 858–877. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, H.G.; Chambers, G.T.; Meyer, W.J.; Arceneaux, L.L.; Russell, W.J.; Seibel, E.J.; Richards, T.L.; Sharar, S.R.; Patterson, D.R. Virtual reality as an adjunctive non-pharmacologic analgesic for acute burn pain during medical procedures. Ann. Behav. Med. 2011, 41, 183–191. [Google Scholar] [CrossRef]
- Triberti, S.; Repetto, C.; Riva, G. Psychological factors influencing the effectiveness of virtual reality-based analgesia: A systematic review. Cyberpsychol. Behav. Social Netw. 2014, 17, 335–345. [Google Scholar] [CrossRef]
- Souchet, A.D.; Lourdeaux, D.; Burkhardt, J.-M.; Hancock, P.A. Design guidelines for limiting and eliminating virtual reality-induced symptoms and effects at work: A comprehensive, factor-oriented review. Front. Psychol. 2023, 14, 1161932. [Google Scholar] [CrossRef]
- Drazich, B.F.; McPherson, R.; Gorman, E.F.; Chan, T.; Teleb, J.; Galik, E.; Resnick, B. In too deep? A systematic literature review of fully-immersive virtual reality and cybersickness among older adults. J. Am. Geriatr. Soc. 2023, 71, 3906–3915. [Google Scholar] [CrossRef]
- Suissa, A.J. Cyber addictions: Toward a psychosocial perspective. Addict. Behav. 2015, 43, 28–32. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall | VR Intervention Group 1 | Care as Usual Group 2 |
|---|---|---|---|
| Number of patients | 67 | 34 (50.7%) 1 | 33 (49.3%) 1 |
| Age, y | 57.0 ± 13.9 [5] | 54.0 ± 15.4 [3] | 60.0 ± 11.7 [2] |
| Suspected cancer | [4] | [2] | [2] |
| Ovarian | 26 (41.3%) | 14 (43.8%) | 12 (38.7%) |
| Uterine | 26 (41.3%) | 12 (37.5%) | 14 (45.2%) |
| Vulva | 6 (9.5%) | 2 (6.3%) | 4 (12.9%) |
| Cervical | 2 (3.2%) | 1 (3.1%) | 1 (3.2%) |
| Benign | 3 (4.8%) | 3 (9.4%) | 0 |
| Procedure type | [5] | [2] | [3] |
| Laparoscopy | 37 (59.7%) | 17 (53.1%) | 20 (66.7%) |
| Laparotomy | 16 (25.8%) | 11 (34.4%) | 5 (16.7%) |
| Other | 9 (14.5%) | 4 (12.5%) | 5 (16.7%) |
| Outcome | Overall (n = 67) | VR Intervention Group 1 (n = 34) | Care as Usual Group 2 (n = 33) | p 3 |
|---|---|---|---|---|
| Outpatient visit | ||||
| Baseline anxiety 1 (T0) | 4 (2–5) | 3 (2–5) | 4 (2–5) | 0.783 |
| Anxiety 1 after VR/CAU (T1) | 3 (2–4) | 2.5 (2–4) | 4 (2–5) | 0.043 |
| p 2 T1 vs. T0 | 0.002 | <0.001 | >0.999 | |
| ΔT1 − T0 | 0 (0–0) | 0 (−1–0) | 0 (0–0) | <0.001 |
| Time interval | ||||
| Time until procedure, d | 35 (15–53) | 34 (14–65.75) | 35 (16.5–45.5) | 0.758 |
| Day of surgery | ||||
| Anxiety 1 before surgery (T2) | 3 (2–4) | 2 (2–3) | 4 (3–5) | <0.001 |
| p 2 T2 vs. T0 | 0.085 | <0.001 | 0.064 | |
| p 2 T2 vs. T1 | 0.763 | 0.026 | 0.076 | |
| ΔT2 − T0 | 0 (−1–1) | −1 (−2–0) | 0 (0–1) | <0.001 |
| ΔT2 − T1 | 0 (−1–1) | 0 (−1–0) | 0 (0–1) | 0.004 |
| Independent Variables | Dependent Variable: ΔT2 − T0 [8] p |
|---|---|
| Age [5] | 0.185 |
| Time until surgical procedure | 0.438 |
| Type of procedure [5] | 0.335 |
| Virtual reality intervention | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmid, B.C.; Marsland, D.; Jacobs, E.; Rezniczek, G.A. A Preparatory Virtual Reality Experience Reduces Anxiety before Surgery in Gynecologic Oncology Patients: A Randomized Controlled Trial. Cancers 2024, 16, 1913. https://doi.org/10.3390/cancers16101913
Schmid BC, Marsland D, Jacobs E, Rezniczek GA. A Preparatory Virtual Reality Experience Reduces Anxiety before Surgery in Gynecologic Oncology Patients: A Randomized Controlled Trial. Cancers. 2024; 16(10):1913. https://doi.org/10.3390/cancers16101913
Chicago/Turabian StyleSchmid, Bernd C., Dominic Marsland, Eilish Jacobs, and Günther A. Rezniczek. 2024. "A Preparatory Virtual Reality Experience Reduces Anxiety before Surgery in Gynecologic Oncology Patients: A Randomized Controlled Trial" Cancers 16, no. 10: 1913. https://doi.org/10.3390/cancers16101913
APA StyleSchmid, B. C., Marsland, D., Jacobs, E., & Rezniczek, G. A. (2024). A Preparatory Virtual Reality Experience Reduces Anxiety before Surgery in Gynecologic Oncology Patients: A Randomized Controlled Trial. Cancers, 16(10), 1913. https://doi.org/10.3390/cancers16101913