
A Systematic Review of High-Dose Methotrexate for Adults with Primary Central Nervous System Lymphoma

 , , , , ,
, , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
3.1. Characteristics of the Analytic Cohorts
3.2. High-Dose Methotrexate Induction Regimens
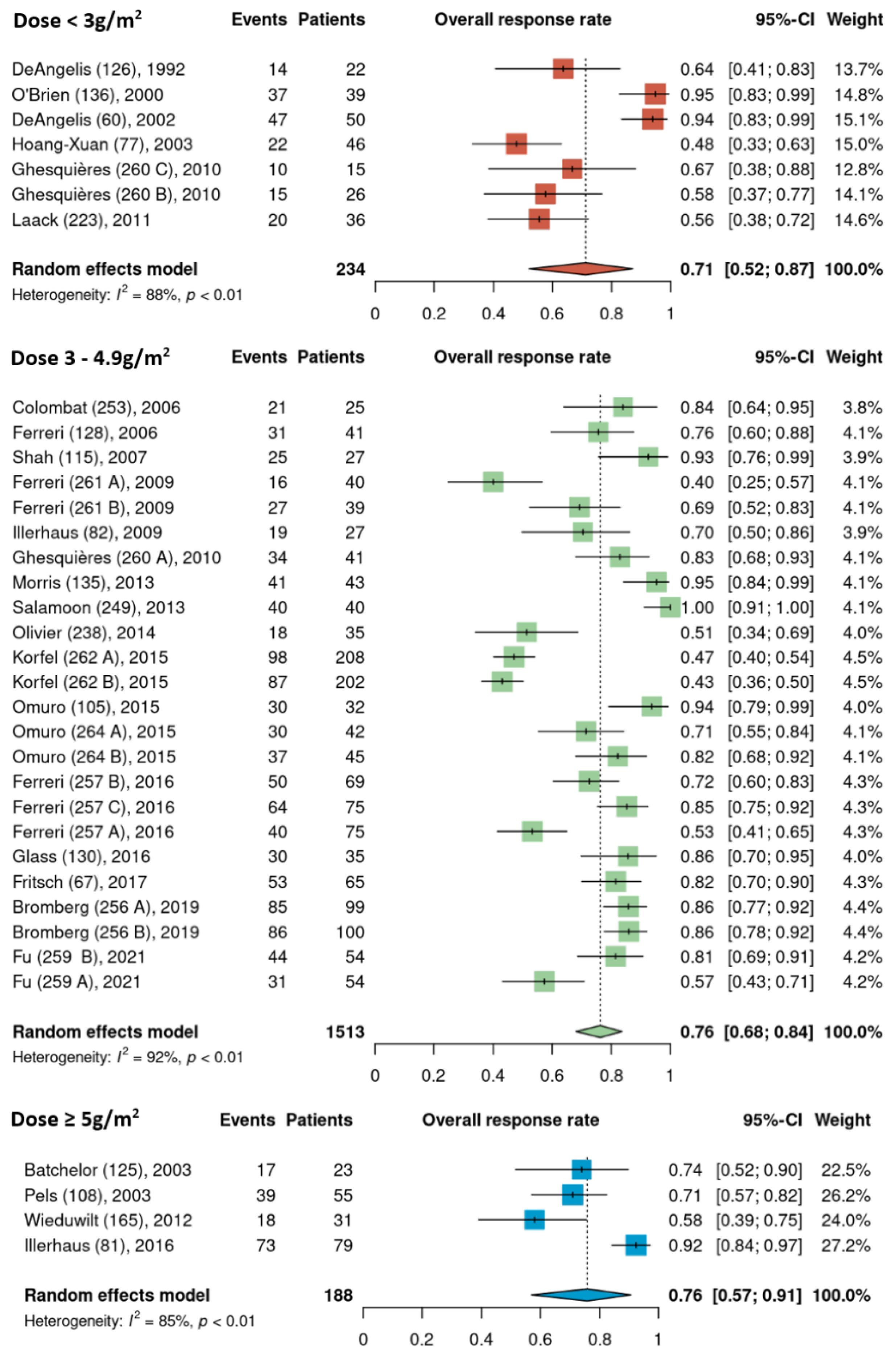
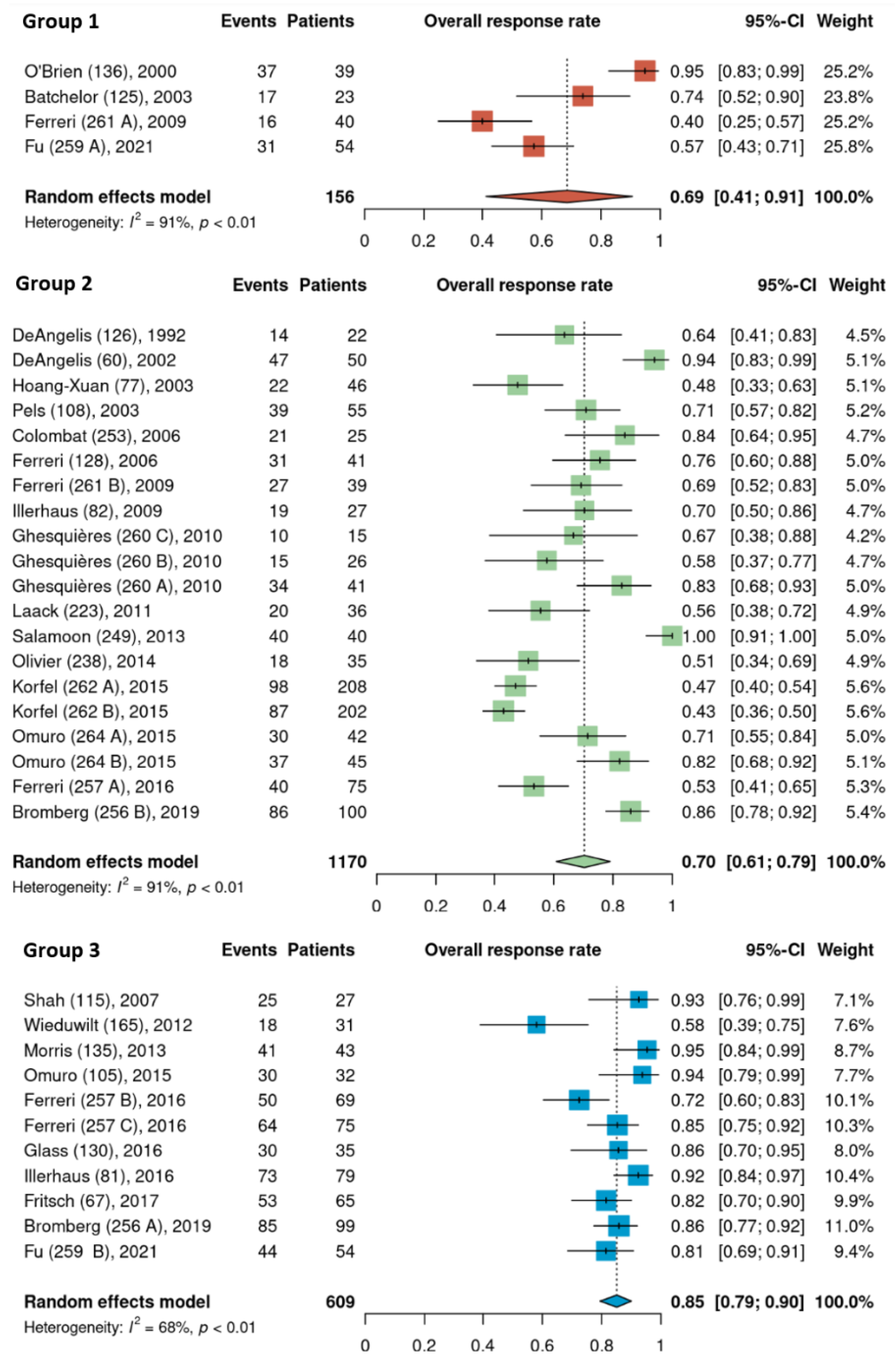
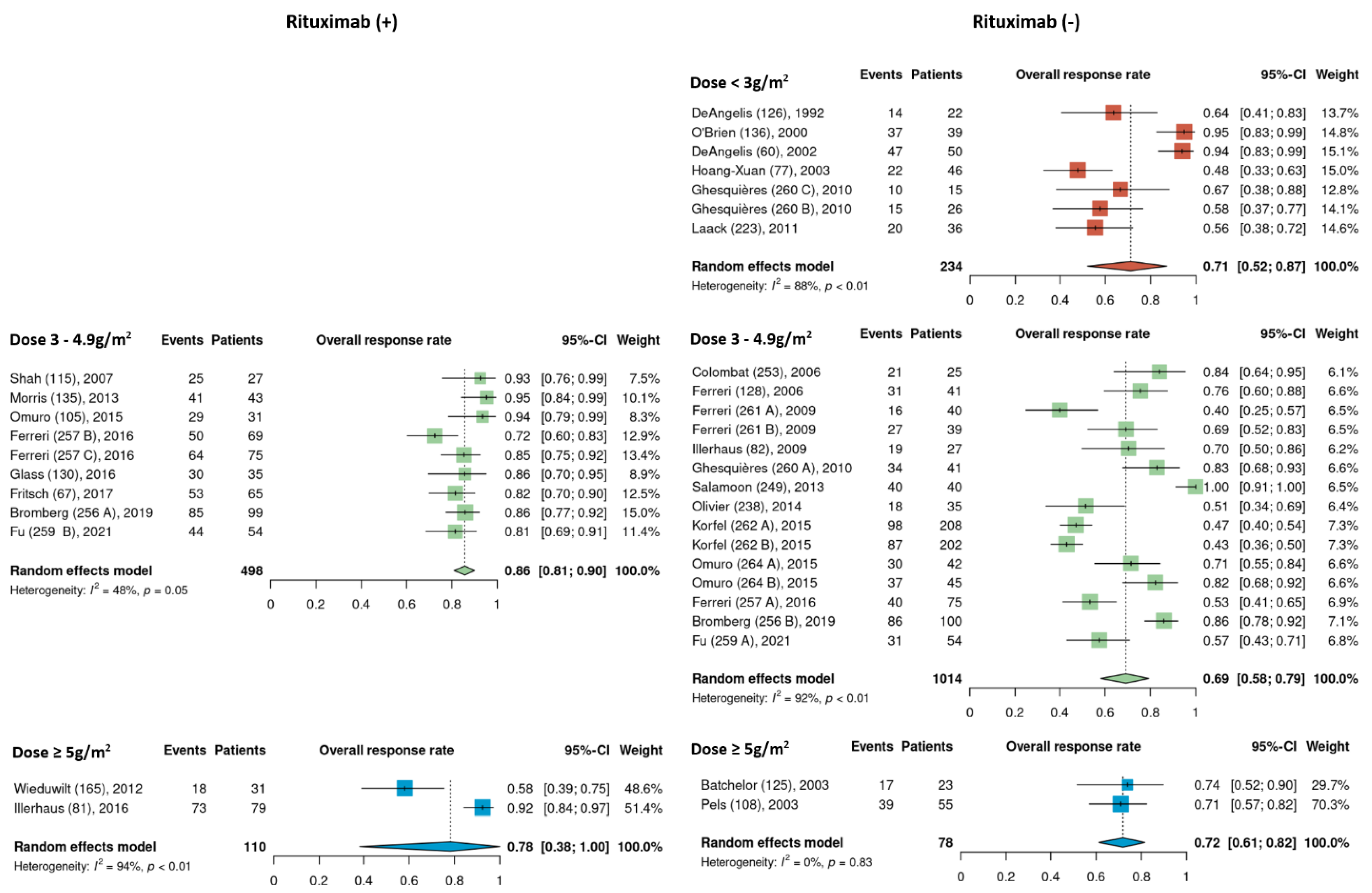
3.3. Overall Response Rates


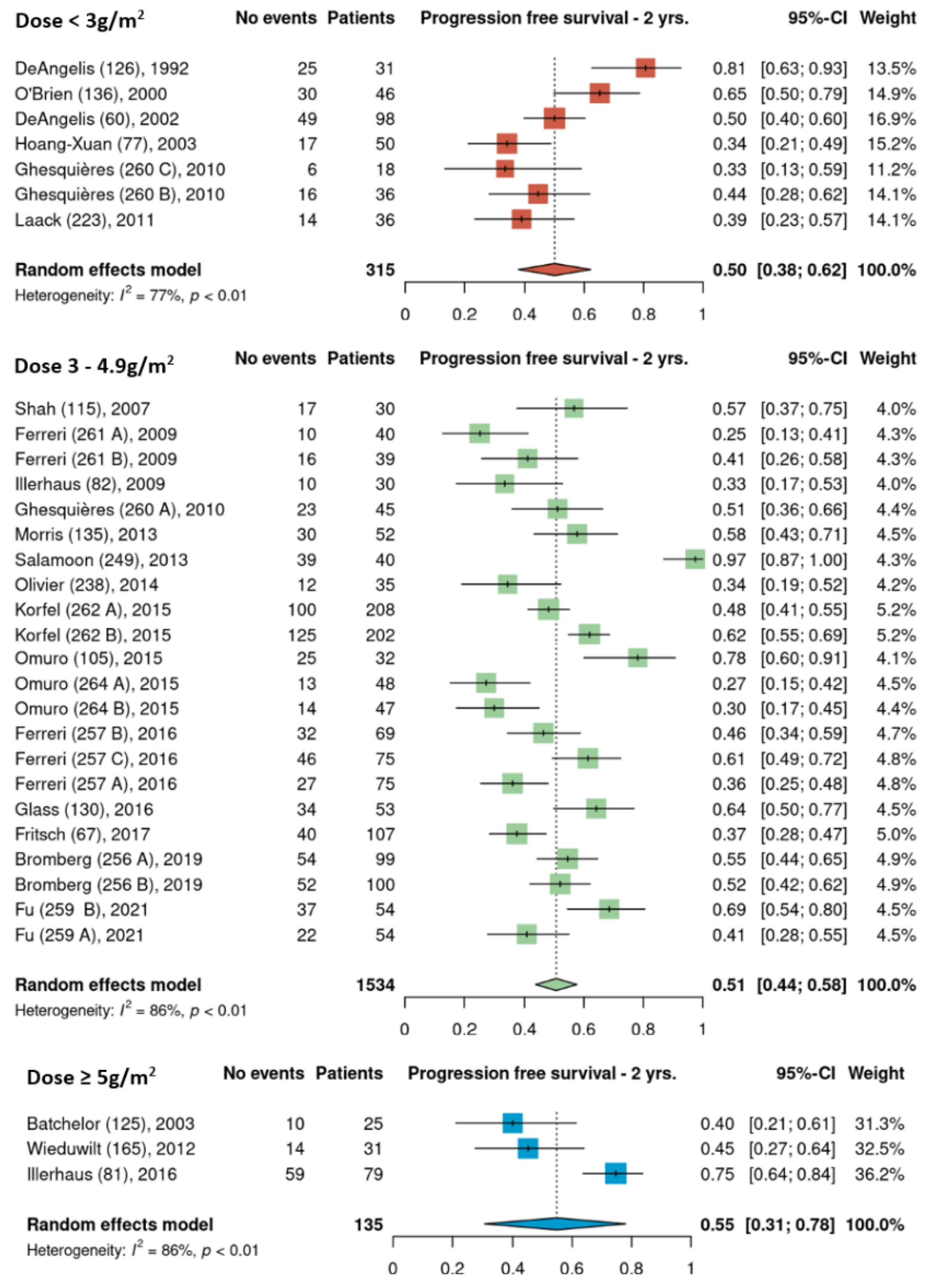
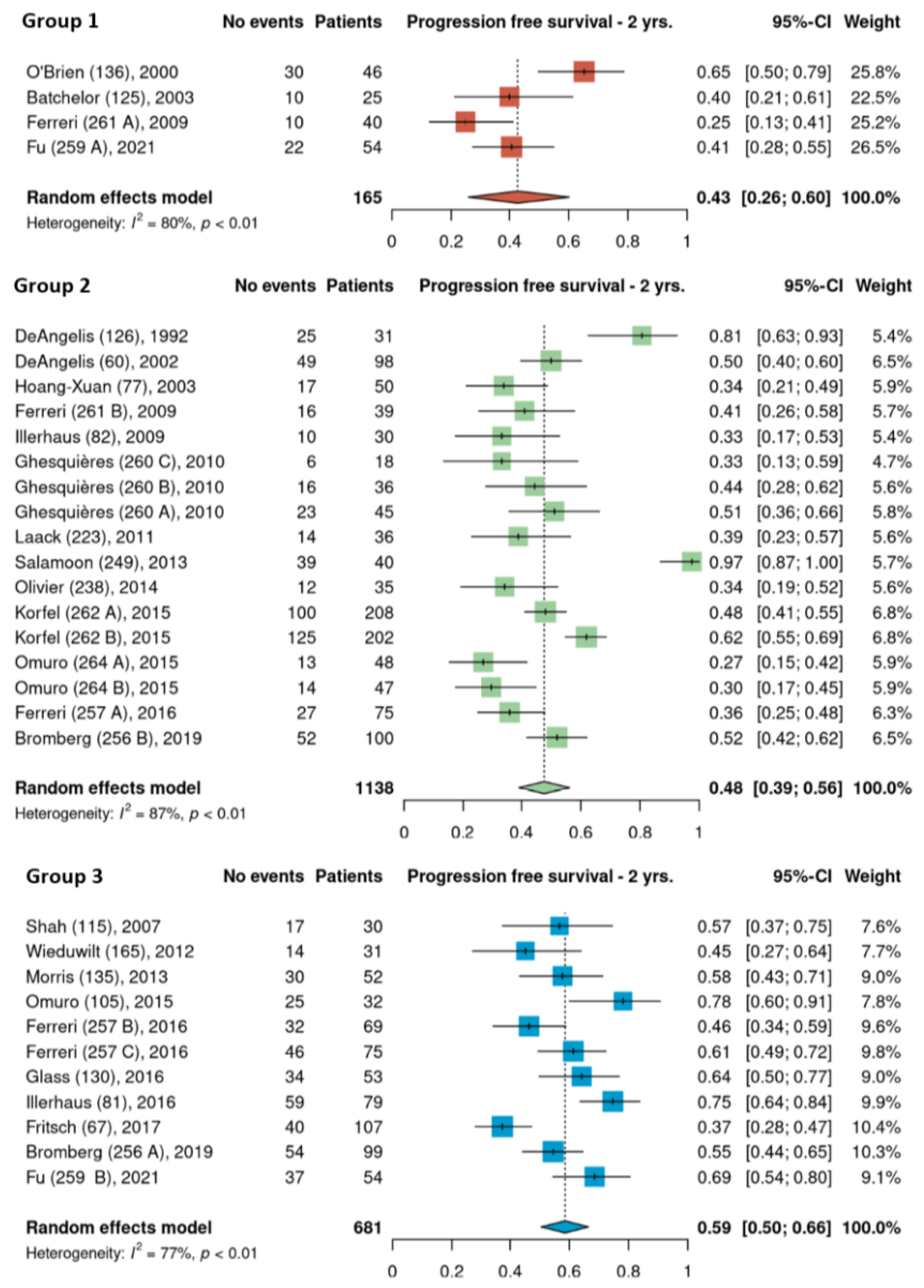
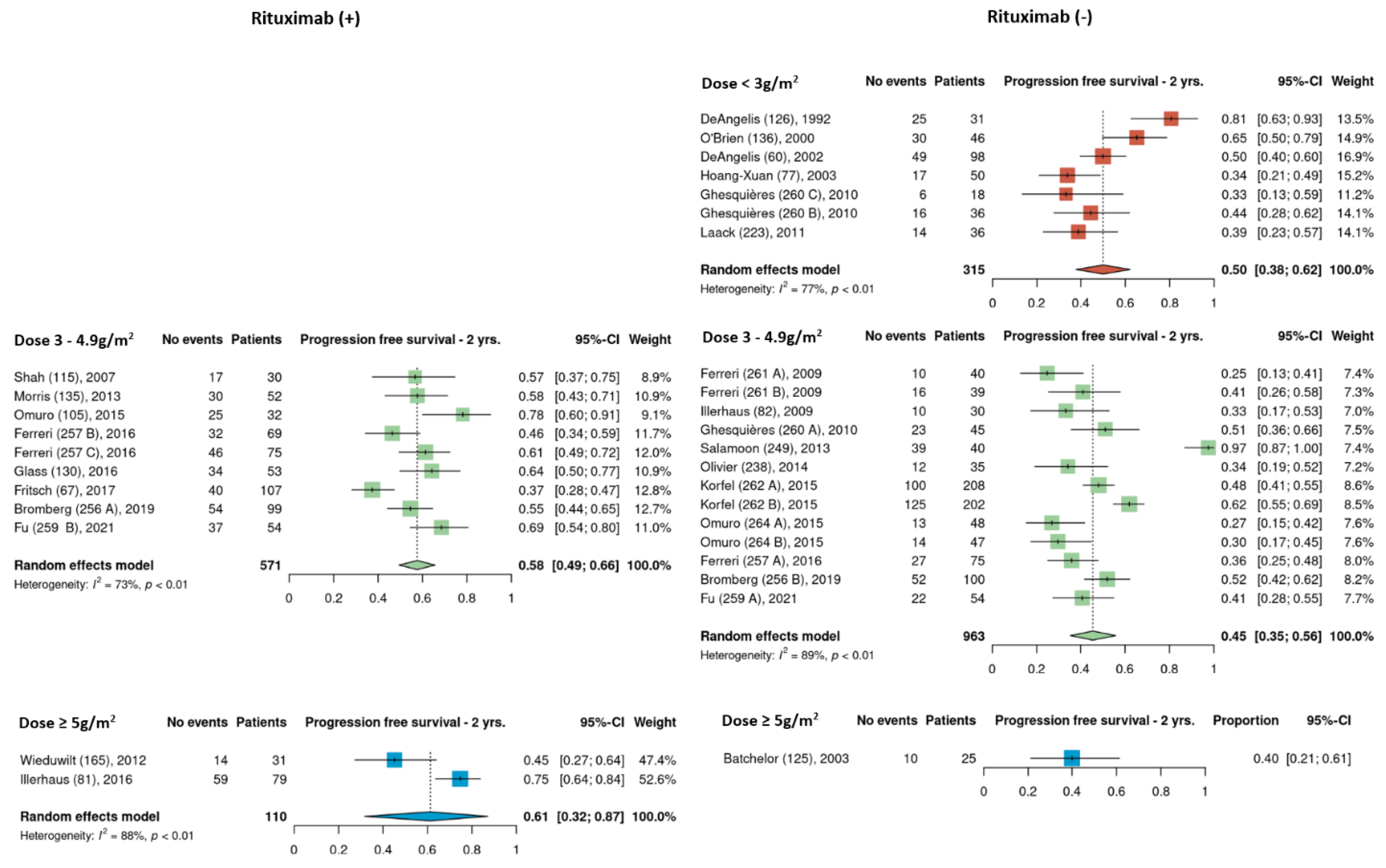
3.4. Progression-Free Survival


3.5. Consolidation Therapy
3.6. Toxicities
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Villano, J.L.; Koshy, M.; Shaikh, H.; Dolecek, T.A.; McCarthy, B.J. Age, gender, and racial differences in incidence and survival in primary CNS lymphoma. Br. J. Cancer 2011, 105, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Grommes, C.; De Angelis, L.M. Primary CNS Lymphoma. J. Clin. Oncol. 2017, 35, 2410–2418. [Google Scholar] [CrossRef] [PubMed]
- Camilleri-Broet, S.; Martin, A.; Moreau, A.; Angonin, R.; Henin, D.; Gontier, M.F.; Rousselet, M.C.; Caulet-Maugendre, S.; Cuilliere, P.; Lefrancq, T.; et al. Primary central nervous system lymphomas in 72 immunocompetent patients: Pathologic findings and clinical correlations. Groupe Ouest Est d’etude des Leucenies et Autres Maladies du Sang (GOELAMS). Am. J. Clin. Pathol. 1998, 110, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Calimeri, T.; Steffanoni, S.; Gagliardi, F.; Chiara, A.; Ferreri, A.J.M. How we treat primary central nervous system lymphoma. ESMO Open 2021, 6, 100213. [Google Scholar] [CrossRef]
- van der Meulen, M.; Dinmohamed, A.G.; Visser, O.; Doorduijn, J.K.; Bromberg, J.E.C. Improved survival in primary central nervous system lymphoma up to age 70 only: A population-based study on incidence, primary treatment and survival in the Netherlands, 1989–2015. Leukemia 2017, 31, 1822–1825. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Patil, N.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2013-2017. Neuro Oncol. 2020, 22 (Suppl. 1), iv1–iv96. [Google Scholar] [CrossRef]
- Mendez, J.S.; Ostrom, Q.T.; Gittleman, H.; Kruchko, C.; DeAngelis, L.M.; Barnholtz-Sloan, J.S.; Grommes, C. The elderly left behind-changes in survival trends of primary central nervous system lymphoma over the past 4 decades. Neuro Oncol. 2018, 20, 687–694. [Google Scholar] [CrossRef]
- Jahnke, K.; Thiel, E.; Martus, P.; Herrlinger, U.; Weller, M.; Fischer, L.; Korfel, A. The German Primary Central Nervous System Lymphoma Study Group.. Relapse of primary central nervous system lymphoma: Clinical features, outcome and prognostic factors. J. Neurooncol. 2006, 80, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Nayak, L.; Hedvat, C.; Rosenblum, M.K.; Abrey, L.E.; DeAngelis, L.M. Late relapse in primary central nervous system lymphoma: Clonal persistence. Neuro Oncol. 2011, 13, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Grommes, C.; Rubenstein, J.L.; DeAngelis, L.M.; Ferreri, A.J.M.; Batchelor, T.T. Comprehensive approach to diagnosis and treatment of newly diagnosed primary CNS lymphoma. Neuro Oncol. 2019, 21, 296–305. [Google Scholar] [CrossRef]
- Bromberg, J.E.C.; van der Meulen, M.; Doorduijn, J.K. The Role of Rituximab in Primary Central Nervous System Lymphoma. Curr. Oncol. Rep. 2020, 22, 78. [Google Scholar] [CrossRef]
- Morris, P.G.; Correa, D.D.; Yahalom, J.; Raizer, J.J.; Schiff, D.; Grant, B.; Grimm, S.; Lai, R.K.; Reiner, A.S.; Panageas, K.; et al. Rituximab, methotrexate, procarbazine, and vincristine followed by consolidation reduced-dose whole-brain radiotherapy and cytarabine in newly diagnosed primary CNS lymphoma: Final results and long-term outcome. J. Clin. Oncol. 2013, 31, 3971–3979. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, J.L.; Hsi, E.D.; Johnson, J.L.; Jung, S.H.; Nakashima, M.O.; Grant, B.; Cheson, B.D.; Kaplan, L.D. Intensive chemotherapy and immunotherapy in patients with newly diagnosed primary CNS lymphoma: CALGB 50202 (Alliance 50202). J. Clin. Oncol. 2013, 31, 3061–3068. [Google Scholar] [CrossRef]
- Bromberg, J.E.C.; Issa, S.; Bakunina, K.; Minnema, M.C.; Seute, T.; Durian, M.; Cull, G.; Schouten, H.C.; Stevens, W.B.C.; Zijlstra, J.M.; et al. Rituximab in patients with primary CNS lymphoma (HOVON 105/ALLG NHL 24): A randomised, open-label, phase 3 intergroup study. Lancet Oncol. 2019, 20, 216–228. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, A.J.; Cwynarski, K.; Pulczynski, E.; Ponzoni, M.; Deckert, M.; Politi, L.S.; Torri, V.; Fox, C.P.; Rosee, P.L.; Schorb, E.; et al. Chemoimmunotherapy with methotrexate, cytarabine, thiotepa, and rituximab (MATRix regimen) in patients with primary CNS lymphoma: Results of the first randomisation of the International Extranodal Lymphoma Study Group-32 (IELSG32) phase 2 trial. Lancet Haematol. 2016, 3, e217–e227. [Google Scholar] [CrossRef]
- Rubenstein, J.L.; Combs, D.; Rosenberg, J.; Levy, A.; McDermott, M.; Damon, L.; Ignoffo, R.; Aldape, K.; Shen, A.; Lee, D.; et al. Rituximab therapy for CNS lymphomas: Targeting the leptomeningeal compartment. Blood 2003, 101, 466–468. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, T.T.; Grossman, S.A.; Mikkelsen, T.; Ye, X.; Desideri, S.; Lesser, G.J. Rituximab monotherapy for patients with recurrent primary CNS lymphoma. Neurology 2011, 76, 929–930. [Google Scholar] [CrossRef]
- Shah, G.D.; Yahalom, J.; Correa, D.D.; Lai, R.K.; Raizer, J.J.; Schiff, D.; LaRocca, R.; Grant, B.; DeAngelis, L.M.; Abrey, L.E. Combined immunochemotherapy with reduced whole-brain radiotherapy for newly diagnosed primary CNS lymphoma. J. Clin. Oncol. 2007, 25, 4730–4735. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Batchelor, T.; Carson, K.; O’Neill, A.; Grossman, S.A.; Alavi, J.; New, P.; Hochberg, F.; Priet, R. Treatment of primary CNS lymphoma with methotrexate and deferred radiotherapy: A report of NABTT 96-07. J. Clin. Oncol. 2003, 21, 1044–1049. [Google Scholar] [CrossRef]
- Colombat, P.; Lemevel, A.; Bertrand, P.; Delwail, V.; Rachieru, P.; Brion, A.; Berthou, C.; Bay, J.O.; Delepine, R.; Desablens, B.; et al. High-dose chemotherapy with autologous stem cell transplantation as first-line therapy for primary CNS lymphoma in patients younger than 60 years: A multicenter phase II study of the GOELAMS group. Bone Marrow Transplant. 2006, 38, 417–420. [Google Scholar] [CrossRef] [PubMed]
- DeAngelis, L.M.; Yahalom, J.; Thaler, H.T.; Kher, U. Combined modality therapy for primary CNS lymphoma. J. Clin. Oncol. 1992, 10, 635–643. [Google Scholar] [CrossRef] [PubMed]
- DeAngelis, L.M.; Seiferheld, W.; Schold, S.C.; Fisher, B.; Schultz, C.J.; Radiation Therapy Oncology Group. Combination chemotherapy and radiotherapy for primary central nervous system lymphoma: Radiation Therapy Oncology Group Study 93-10. J. Clin. Oncol. 2002, 20, 4643–4648. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, A.J.; Dell’Oro, S.; Foppoli, M.; Bernardi, M.; Brandes, A.A.; Tosoni, A.; Montanari, M.; Balzarotti, M.; Spina, M.; Ilariucci, F.; et al. MATILDE regimen followed by radiotherapy is an active strategy against primary CNS lymphomas. Neurology 2006, 66, 1435–1438. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, A.J.; Reni, M.; Foppoli, M.; Martelli, M.; Pangalis, G.A.; Frezzato, M.; Cabras, M.G.; Fabbri, A.; Corazzelli, G.; Ilariucci, F.; et al. High-dose cytarabine plus high-dose methotrexate versus high-dose methotrexate alone in patients with primary CNS lymphoma: A randomised phase 2 trial. Lancet 2009, 374, 1512–1520. [Google Scholar] [CrossRef]
- Fritsch, K.; Kasenda, B.; Schorb, E.; Hau, P.; Bloehdorn, J.; Mohle, R.; Low, S.; Binder, M.; Atta, J.; Keller, U.; et al. High-dose methotrexate-based immuno-chemotherapy for elderly primary CNS lymphoma patients (PRIMAIN study). Leukemia 2017, 31, 846–852. [Google Scholar] [CrossRef]
- Fu, J.; Ma, X. High-dose methotrexate combined with rituximab improves the survival rate of patients with primary central nervous system lymphoma. J. BUON 2021, 26, 366–372. [Google Scholar]
- Ghesquieres, H.; Ferlay, C.; Sebban, C.; Perol, D.; Bosly, A.; Casasnovas, O.; Reman, O.; Coiffier, B.; Tilly, H.; Morel, P.; et al. Long-term follow-up of an age-adapted C5R protocol followed by radiotherapy in 99 newly diagnosed primary CNS lymphomas: A prospective multicentric phase II study of the Groupe d’Etude des Lymphomes de l’Adulte (GELA). Ann. Oncol. 2010, 21, 842–850. [Google Scholar] [CrossRef]
- Glass, J.; Won, M.; Schultz, C.J.; Brat, D.; Bartlett, N.L.; Suh, J.H.; Werner-Wasik, M.; Fisher, B.J.; Liepman, M.K.; Augspurger, M.; et al. Phase I and II Study of Induction Chemotherapy With Methotrexate, Rituximab, and Temozolomide, Followed By Whole-Brain Radiotherapy and Postirradiation Temozolomide for Primary CNS Lymphoma: NRG Oncology RTOG 0227. J. Clin. Oncol. 2016, 34, 1620–1625. [Google Scholar] [CrossRef]
- Hoang-Xuan, K.; Taillandier, L.; Chinot, O.; Soubeyran, P.; Bogdhan, U.; Hildebrand, J.; Frenay, M.; De Beule, N.; Delattre, J.Y.; Baron, B. European Organization for Research and Treatment of Cancer Brain Tumor Group Chemotherapy alone as initial treatment for primary CNS lymphoma in patients older than 60 years: A multicenter phase II study (26952) of the European Organization for Research and Treatment of Cancer Brain Tumor Group. J. Clin. Oncol. 2003, 21, 2726–2731. [Google Scholar] [PubMed]
- Illerhaus, G.; Marks, R.; Muller, F.; Ihorst, G.; Feuerhake, F.; Deckert, M.; Ostertag, C.; Finke, J. High-dose methotrexate combined with procarbazine and CCNU for primary CNS lymphoma in the elderly: Results of a prospective pilot and phase II study. Ann. Oncol. 2009, 20, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Illerhaus, G.; Kasenda, B.; Ihorst, G.; Egerer, G.; Lamprecht, M.; Keller, U.; Wolf, H.H.; Hirt, C.; Stilgenbauer, S.; Binder, M.; et al. High-dose chemotherapy with autologous haemopoietic stem cell transplantation for newly diagnosed primary CNS lymphoma: A prospective, single-arm, phase 2 trial. Lancet Haematol. 2016, 3, e388–e397. [Google Scholar] [CrossRef]
- Korfel, A.; Thiel, E.; Martus, P.; Mohle, R.; Griesinger, F.; Rauch, M.; Roth, A.; Hertenstein, B.; Fischer, T.; Hundsberger, T.; et al. Randomized phase III study of whole-brain radiotherapy for primary CNS lymphoma. Neurology 2015, 84, 1242–1248. [Google Scholar] [CrossRef]
- Laack, N.N.; O’Neill, B.P.; Ballman, K.V.; O’Fallon, J.R.; Carrero, X.W.; Kurtin, P.J.; Scheithauer, B.W.; Brown, P.D.; Habermann, T.M.; Colgan, J.P.; et al. CHOD/BVAM chemotherapy and whole-brain radiotherapy for newly diagnosed primary central nervous system lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 476–482. [Google Scholar] [CrossRef]
- O’Brien, P.; Roos, D.; Pratt, G.; Liew, K.; Barton, M.; Poulsen, M.; Olver, I.; Trotter, G. Phase II multicenter study of brief single-agent methotrexate followed by irradiation in primary CNS lymphoma. J. Clin. Oncol. 2000, 18, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Olivier, G.; Clavert, A.; Lacotte-Thierry, L.; Gardembas, M.; Escoffre-Barbe, M.; Brion, A.; Cumin, I.; Legouffe, E.; Solal-Celigny, P.; Chabin, M.; et al. A phase 1 dose escalation study of idarubicin combined with methotrexate, vindesine, and prednisolone for untreated elderly patients with primary central nervous system lymphoma. The GOELAMS LCP 99 trial. Am. J. Hematol. 2014, 89, 1024–1029. [Google Scholar] [CrossRef]
- Omuro, A.; Correa, D.D.; DeAngelis, L.M.; Moskowitz, C.H.; Matasar, M.J.; Kaley, T.J.; Gavrilovic, I.T.; Nolan, C.; Pentsova, E.; Grommes, C.C.; et al. R-MPV followed by high-dose chemotherapy with TBC and autologous stem-cell transplant for newly diagnosed primary CNS lymphoma. Blood 2015, 125, 1403–1410. [Google Scholar] [CrossRef]
- Omuro, A.; Chinot, O.; Taillandier, L.; Ghesquieres, H.; Soussain, C.; Delwail, V.; Lamy, T.; Gressin, R.; Choquet, S.; Soubeyran, P.; et al. Methotrexate and temozolomide versus methotrexate, procarbazine, vincristine, and cytarabine for primary CNS lymphoma in an elderly population: An intergroup ANOCEF-GOELAMS randomised phase 2 trial. Lancet Haematol. 2015, 2, e251–e259. [Google Scholar] [CrossRef]
- Pels, H.; Schmidt-Wolf, I.G.; Glasmacher, A.; Schulz, H.; Engert, A.; Diehl, V.; Zellner, A.; Schackert, G.; Reichmann, H.; Kroschinsky, F.; et al. Primary central nervous system lymphoma: Results of a pilot and phase II study of systemic and intraventricular chemotherapy with deferred radiotherapy. J. Clin. Oncol. 2003, 21, 4489–4495. [Google Scholar] [CrossRef]
- Salamoon, M.; Hussein, T.; Kenj, M.; Bachour, M. High-dose methotrexate, high-dose cytarabine and temozolomide for the treatment of primary central nervous system lymphoma (PCNSL). Med. Oncol. 2013, 30, 690. [Google Scholar] [CrossRef] [PubMed]
- Wieduwilt, M.J.; Valles, F.; Issa, S.; Behler, C.M.; Hwang, J.; McDermott, M.; Treseler, P.; O’Brien, J.; Shuman, M.A.; Cha, S.; et al. Immunochemotherapy with intensive consolidation for primary CNS lymphoma: A pilot study and prognostic assessment by diffusion-weighted MRI. Clin. Cancer Res. 2012, 18, 1146–1155. [Google Scholar] [CrossRef] [PubMed]
- Borsi, J.D.; Moe, P.J. A comparative study on the pharmacokinetics of methotrexate in a dose range of 0.5 g to 33.6 g/m2 in children with acute lymphoblastic leukemia. Cancer 1987, 60, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Howard, S.C.; McCormick, J.; Pui, C.H.; Buddington, R.K.; Harvey, R.D. Preventing and Managing Toxicities of High-Dose Methotrexate. Oncologist 2016, 21, 1471–1482. [Google Scholar] [CrossRef] [PubMed]
- Hamed, K.M.; Dighriri, I.M.; Baomar, A.F.; Alharthy, B.T.; Alenazi, F.E.; Alali, G.H.; Alenazy, R.H.; Alhumaidi, N.T.; Alhulayfi, D.H.; Alotaibi, Y.B.; et al. Overview of Methotrexate Toxicity: A Comprehensive Literature Review. Cureus 2022, 14, e29518. [Google Scholar] [CrossRef]
- Dalia, S.; Price, S.; Forsyth, P.; Sokol, L.; Jaglal, M. What is the optimal dose of high-dose methotrexate in the initial treatment of primary central nervous system lymphoma? Leuk. Lymphoma 2015, 56, 500–502. [Google Scholar] [CrossRef]
- Li, Q.; Ma, J.; Ma, Y.; Lin, Z.; Kang, H.; Chen, B. Improvement of outcomes of an escalated high-dose methotrexate-based regimen for patients with newly diagnosed primary central nervous system lymphoma: A real-world cohort study. Cancer Manag. Res. 2021, 13, 6115–6122. [Google Scholar] [CrossRef]
- Han, C.H.; Batchelor, T.T. Diagnosis and management of primary central nervous system lymphoma. Cancer 2017, 123, 4314–4324. [Google Scholar] [CrossRef]
- Schmitt, A.M.; Herbrand, A.K.; Fox, C.P.; Bakunina, K.; Bromberg, J.E.C.; Cwynarski, K.; Doorduijn, J.K.; Ferreri, A.J.M.; Illerhaus, G.; Issa, S.; et al. Rituximab in primary central nervous system lymphoma-A systematic review and meta-analysis. Hematol. Oncol. 2019, 37, 548–557. [Google Scholar] [CrossRef]
- Fritsch, K.; Kasenda, B.; Hader, C.; Nikkhah, G.; Prinz, M.; Haug, V.; Haug, S.; Ihorst, G.; Finke, J.; Illerhaus, G. Immunochemotherapy with rituximab, methotrexate, procarbazine, and lomustine for primary CNS lymphoma (PCNSL) in the elderly. Ann. Oncol. 2011, 22, 2080–2085. [Google Scholar] [CrossRef]
- Roth, P.; Martus, P.; Kiewe, P.; Mohle, R.; Klasen, H.; Rauch, M.; Roth, A.; Kaun, S.; Thiel, E.; Korfel, A.; et al. Outcome of elderly patients with primary CNS lymphoma in the G-PCNSL-SG-1 trial. Neurology 2012, 79, 890–896. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Cohort Number † | Study Type | Total N0 Treated with HDMTX | HDMTX Dose (g/m2) | N0 of HDMTX Cycles | Rituximab (Y/N) | Other Chemotherapeutic Agents | CNS Delivery | Consolidation Therapy | ORR (CR + PR) | 1-Year PFS | 2-Year PFS | 3-Year PFS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Batchelor et al., (2003) [21] | 125 | Multicenter, Phase II | 25 | 8 | Up to 8 | N | - | - | HDCT (MTX) | 74% | 50% | 38% | 38% |
| Bromberg et al., (2019) [14] | 256A | Randomized Phase III | 99 | 3 | 2 | Y | Carmustine, teniposide, prednisone | IT a | HDCT (ARA-C) ± RT | 86% | 65% | 55% | 55% |
| Bromberg et al., (2019) [14] | 256B | Randomized Phase III | 100 | 3 | 2 | N | Carmustine, teniposide, prednisone | IT a | HDCT (ARA-C) ± RT | 86% | 58% | 52% | 40% |
| Columbat et al., (2006) [22] | 253 | Multicenter, Phase II | 25 | 3 | 2 | N | Etoposide, carmustine, MPD | IT b | SCT | 84% | - | - | - |
| DeAngelis et al., (1992) [23] | 126 | Single center | 31 | 1 | 1 | N | Dexamethasone | ICV a | RT + HDCT (ARA-C) | 64% | 90% # | 80% # | 66% # |
| DeAngelis et al., (2002) [24] | 60 | Single-arm | 98 | 2.5 | 5 | N | Vincristine, procarbazine | ICV a | RT + HDCT (ARA-C) | 94% | 64% | 50% | 41% |
| Ferrari et al., (2016) [15] | 257A | Randomized Phase II | 75 | 3.5 | 4 | N | Cytarabine | - | SCT or RT * | 54% | 40% | 36% | 31% |
| Ferrari et al., (2016) [15] | 257B | Randomized Phase II | 69 | 3.5 | 4 | Y | Cytarabine | - | SCT or RT * | 73% | 57% | 46% | 40% |
| Ferrari et al., (2016) [15] | 257C | Randomized Phase II | 75 | 3.5 | 4 | Y | Cytarabine, thiotepa | - | SCT or RT * | 86% | 65% | 61% | 52% |
| Ferrari et al., (2006) [25] | 128 | Phase II | 41 | 3.5 | 3 | N | Idarubicin, cytarabine, thiotepa | - | RT | 76% | - | - | 43% |
| Ferrari et al., (2009) [26] | 261A | Randomized Phase II | 40 | 3.5 | 4 | N | - | - | RT | 41% | 30% ¶ | 25% ¶ | 21% ¶ |
| Ferrari et al., (2009) [26] | 261B | Randomized Phase II | 39 | 3.5 | 4 | N | Cytarabine | - | RT | 69% | 50% ¶ | 40% ¶ | 38% ¶ |
| Fritsch et al., (2017) [27] | 67 | Multicenter Single-arm | 107 | 3 | 3 | Y | Procarbazine, lomustine | - | - | 81% ǁ | 46% | 37% | 37% |
| Fu et al., (2021) [28] | 259A | Randomized | 54 | 3 | 4 | N | - | - | RT | 57% | 46% | 40% | 15% |
| Fu et al.,(2021) [28] | 259B | Randomized | 54 | 3 | 4 | Y | - | - | RT | 81% | 70% | 68% | 28% |
| Ghesquières et al., (2010) [29] | 260A | Multicenter Phase II | 45 | 3 | 4 | N | Cyclophosphamide, doxorubicin, vincristine, prednisone, cytarabine | IT c | RT | 82% | 68% | 51% | 45% |
| Ghesquières et al., (2010) [29] | 260B | Multicenter Phase II | 36 | 1.5 | 4 | N | Cyclophosphamide, doxorubicin, vincristine, prednisone, cytarabine | IT c | RT | 58% | 54% | 45% | 38% |
| Ghesquières et al., (2010) [29] | 260C | Multicenter Phase II | 18 | 1.5 | 4 | N | Cyclophosphamide, etoposide | IT c | RT | 66% | 50% | 35% | 18% |
| Glass et al.,(2016) [30] | 130 | Phase I and II | 53 | 3.5 | 5 | Y | Temozolamide | - | RT + HDCT (TMZ) | 85% | 80% | 64% | 57% |
| Hoang-Xuan et al., (2003) [31] | 77 | Multicenter Phase II | 50 | 1 | 1 | N | Procarbazine, lomustine, MPD | ITd | - | 48% | 40% | 34% | 30% |
| Illerhaus et al., (2009) [32] | 82 | Pilot & Phase II | 30 | 3 | 3 | N | Procarbazine, lomustine | - | - | 70% | 45% | 35% | 32% |
| Illerhaus et al., (2016) [33] | 81 | Single-arm Phase II | 79 | 8 | 1 | Y | Cytarabine, thiotepa | - | SCT | 92% | 79% | 75% | 67% |
| Korfel et al., (2015) [34] | 262A | Randomized Phase III | 208 | 4 | 6 | N | Ifosfamide | - | - | 47% ‡ | 72% ‡ | 48% ‡ | 39% ‡ |
| Korfel et al., (2015) [34] | 262B | Randomized Phase III | 202 | 4 | 6 | N | Ifosfamide | - | RT | 43% ‡ | 85% ‡ | 62% ‡ | 49% ‡ |
| Laack et al., (2011) [35] | 223 | Phase II | 36 | 1.5 | 6 | N | Cyclophosphamide, doxorubicin, vincristine, dexamethasone, carmustine, cytarabine | - | RT | 56% | 50% | 38% | 31% |
| Morris et al., (2013) [12] | 135 | Multicenter Phase II | 52 | 3.5 | 5 | Y | Procarbazine, vincristine | ICV a | RT + HDCT (ARA-C) | 95% | 65% | 57% | 51% |
| O’Brien et al., (2000) [36] | 136 | Multicenter Phase II | 46 | 1 | 1 | N | - | IT e | RT | 95% | 79% | 65% | 55% |
| Olivier et al., (2014) [37] | 238 | Multicenter Phase I | 35 | 3 | 3 | N | Idarubicin, vindesine, prednisolone | IT c | RT | 51% | 55% | 33% | 28% |
| Omuro et al., (2015) [38] | 105 | Phase II | 32 | 3.5 | 5 to 7 | Y | Procarbazine, vincristine | - | SCT | 94% | 82% | 79% | 79% |
| Omuro et al., (2015) [39] | 264A | Randomized Phase II | 48 | 3.5 | 3 | N | Temozolomide | - | HDCT (ARA-C) | 71% | 36% | 28% | 22% |
| Omuro et al., (2015) [39] | 264B | Randomized Phase II | 47 | 3.5 | 3 | N | Procarbazine, vincristine, cytarabine | - | HDCT (ARA-C) | 82% | 36% | 30% | 20% |
| Pels et al., (2003) [40] | 108 | Pilot and Phase II | 65 | 5 | 4 | N | Vincristine, ifosfamide, dexamethasone, cyclophosphamide, cytarabine, vindesine | ICV a | - | 71% | - | - | - |
| Salamoon et al., (2013) [41] | 249 | Single-arm | 40 | 3 | 6 | N | Cytarabine, temozolamide | - | - | 100% | 100% | 97% | 95% |
| Shah et al., (2007) [18] | 115 | Single-arm | 30 | 3.5 | 5 to 7 cycles | Y | Procarbazine, vincristine | IT a | RT + HDCT (ARA-C) | 92% | 69% | 57% | 57% |
| Wieduwilt et al., (2012) [42] | 165 | Single-arm | 31 | 8 | Up to 8 | Y | Temozolamide | - | HDCT(ARA-C, VP-16) | 58% | 53% | 45% | 45% |
| Total (N) | 35 | 2115 | Y = 11 | 14 | 29 |
| ORR (95% C.I.) | 2-Year PFS (95% C.I.) | ||
|---|---|---|---|
| N0 of planned HDMTX courses (induction) | <5 (n = 20) | 73% (65–80%) | 50% (43–58%) |
| ≥5 (n = 15) | 79% (66–89%) | 52% (43–61%) | |
| Chemotherapy to CNS compartment (induction) | No (n = 21) | 73% (64–81%) | 51% (42–59%) |
| Yes (n = 14) | 79% (70–81%) | 52% (45–58%) | |
| Radiation therapy (consolidation) | No (n = 13) | 77% (65–87%) | 52% (39–65%) |
| Yes (N = 22) | 74% (65–82%) | 50% (45–56%) | |
| Stem cell transplant (consolidation) | No (n = 29) | 81% (68–92%) | 59% (43–74%) |
| Yes (n = 6) | 74% (66–81%) | 49% (43–56%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villanueva, G.; Guscott, M.; Schaiquevich, P.; Sampor, C.; Combs, R.; Tentoni, N.; Hwang, M.; Lowe, J.; Howard, S. A Systematic Review of High-Dose Methotrexate for Adults with Primary Central Nervous System Lymphoma. Cancers 2023, 15, 1459. https://doi.org/10.3390/cancers15051459
Villanueva G, Guscott M, Schaiquevich P, Sampor C, Combs R, Tentoni N, Hwang M, Lowe J, Howard S. A Systematic Review of High-Dose Methotrexate for Adults with Primary Central Nervous System Lymphoma. Cancers. 2023; 15(5):1459. https://doi.org/10.3390/cancers15051459
Chicago/Turabian StyleVillanueva, Gabriela, Martin Guscott, Paula Schaiquevich, Claudia Sampor, Ryan Combs, Nicolás Tentoni, Miriam Hwang, Jennifer Lowe, and Scott Howard. 2023. "A Systematic Review of High-Dose Methotrexate for Adults with Primary Central Nervous System Lymphoma" Cancers 15, no. 5: 1459. https://doi.org/10.3390/cancers15051459
APA StyleVillanueva, G., Guscott, M., Schaiquevich, P., Sampor, C., Combs, R., Tentoni, N., Hwang, M., Lowe, J., & Howard, S. (2023). A Systematic Review of High-Dose Methotrexate for Adults with Primary Central Nervous System Lymphoma. Cancers, 15(5), 1459. https://doi.org/10.3390/cancers15051459