
Clinical Application of ImmunoPET Targeting Checkpoint Inhibitors
 , , , and
, , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
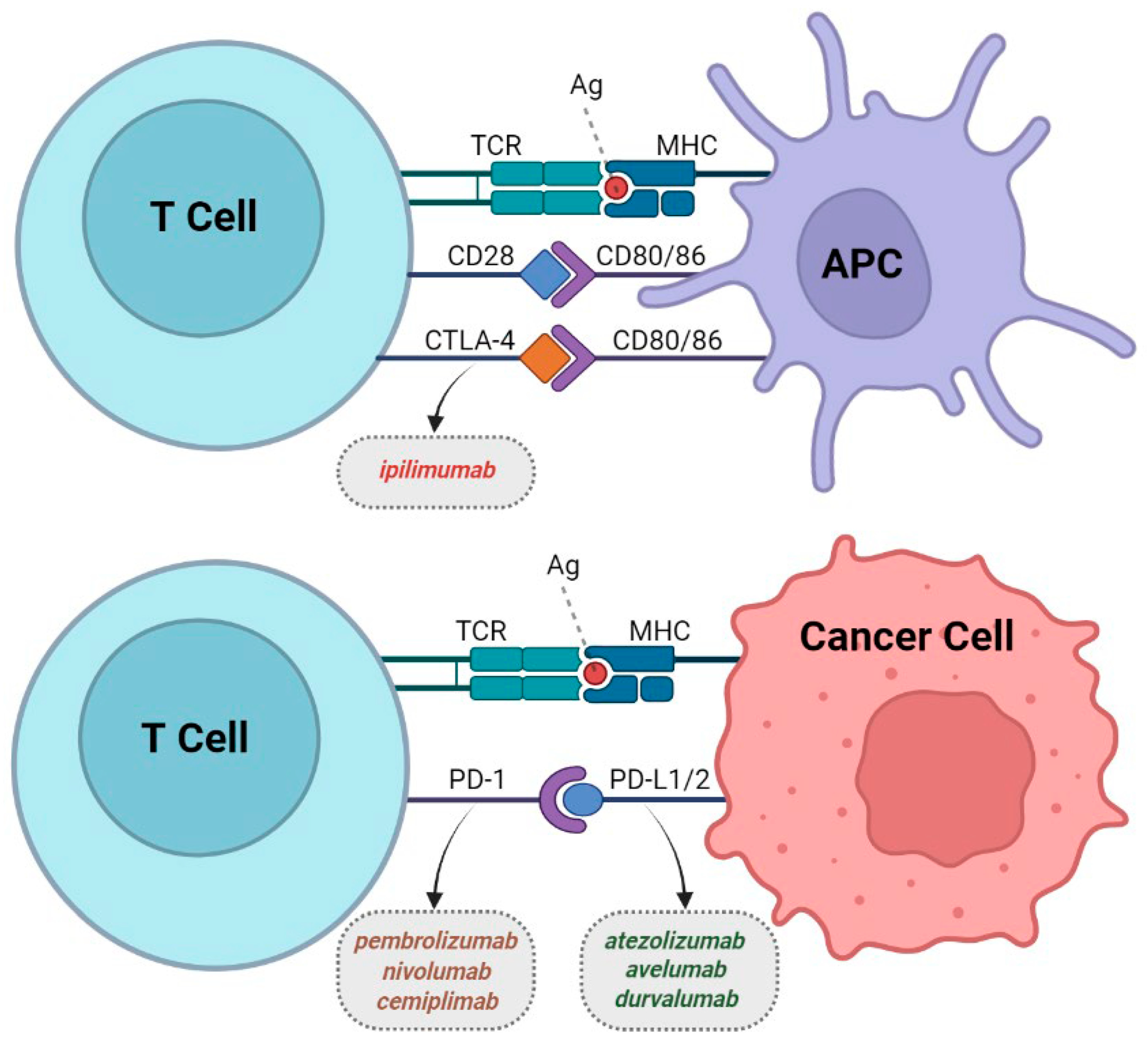
2. CTLA-4
3. PD-1/PD-L1
4. Tumor-Infiltrating Lymphocytes
5. Conclusions and Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Beatty, G.L.; Gladney, W.L. Immune escape mechanisms as a guide for cancer immunotherapy. Clin. Cancer Res. 2015, 21, 687–692. [Google Scholar] [CrossRef]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Naimi, A.; Mohammed, R.N.; Raji, A.; Chupradit, S.; Yumashev, A.V.; Suksatan, W.; Shalaby, M.N.; Thangavelu, L.; Kamrava, S.; Shomali, N.; et al. Tumor immunotherapies by immune checkpoint inhibitors (ICIs); the pros and cons. Cell Commun. Signal. 2022, 20, 44. [Google Scholar] [CrossRef]
- Shiravand, Y.; Khodadadi, F.; Kashani, S.M.A.; Hosseini-Fard, S.R.; Hosseini, S.; Sadeghirad, H.; Ladwa, R.; O’Byrne, K.; Kulasinghe, A. Immune Checkpoint Inhibitors in Cancer Therapy. Curr. Oncol. 2022, 29, 3044–3060. [Google Scholar] [CrossRef]
- Vaddepally, R.K.; Kharel, P.; Pandey, R.; Garje, R.; Chandra, A.B. Review of Indications of FDA-Approved Immune Checkpoint Inhibitors per NCCN Guidelines with the Level of Evidence. Cancers 2020, 12, 738. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Chen, Y.P.; Du, X.J.; Liu, J.Q.; Huang, C.L.; Chen, L.; Zhou, G.Q.; Li, W.F.; Mao, Y.P.; Hsu, C.; et al. Comparative safety of immune checkpoint inhibitors in cancer: Systematic review and network meta-analysis. Br. Med. J. 2018, 363, k4226. [Google Scholar] [CrossRef] [PubMed]
- Borgeaud, M.; Sandoval, J.; Obeid, M.; Banna, G.; Michielin, O.; Addeo, A.; Friedlaender, A. Novel targets for immune-checkpoint inhibition in cancer. Cancer Treat. Rev. 2023, 120, 102614. [Google Scholar] [CrossRef]
- Lopci, E.; Hicks, R.J.; Dimitrakopoulou-Strauss, A.; Dercle, L.; Iravani, A.; Seban, R.D.; Sachpekidis, C.; Humbert, O.; Gheysens, O.; Glaudemans, A.W.J.M.; et al. Joint EANM/SNMMI/ANZSNM practice guidelines/procedure standards on recommended use of [18F]FDG PET/CT imaging during immunomodulatory treatments in patients with solid tumors version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 2323–2341. [Google Scholar] [CrossRef]
- Mangas Losada, M.; Romero Robles, L.; Mendoza Melero, A.; García Megías, I.; Villanueva Torres, A.; Garrastachu Zumarán, P.; Boulvard Chollet, X.; Lopci, E.; Ramírez Lasanta, R.; Delgado Bolton, R.C. [18F]FDG PET/CT in the Evaluation of Melanoma Patients Treated with Immunotherapy. Diagnostics 2023, 13, 978. [Google Scholar] [CrossRef]
- Dercle, L.; Sun, S.; Seban, R.D.; Mekki, A.; Sun, R.; Tselikas, L.; Hans, S.; Bernard-Tessier, A.; Mihoubi Bouvier, F.; Aide, N.; et al. Emerging and Evolving Concepts in Cancer Immunotherapy Imaging. Radiology 2023, 306, 32–46. [Google Scholar] [CrossRef]
- Wei, W.; Rosenkrans, Z.T.; Liu, J.; Huang, G.; Luo, Q.Y.; Cai, W. ImmunoPET: Concept, Design, and Applications. Chem. Rev. 2020, 120, 3787–3851. [Google Scholar] [CrossRef] [PubMed]
- Basudan, A.M. The Role of Immune Checkpoint Inhibitors in Cancer Therapy. Clin. Pract. 2023, 13, 22–40. [Google Scholar] [CrossRef] [PubMed]
- Fallarino, F.; Fields, P.E.; Gajewski, T.F. B7-1 engagement of cytotoxic T lymphocyte antigen 4 inhibits T cell activation in the absence of CD28. J. Exp. Med. 1998, 188, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Walunas, T.L.; Lenschow, D.J.; Bakker, C.Y.; Linsley, P.S.; Freeman, G.J.; Green, J.M.; Thompson, C.B.; Bluestone, J.A. CTLA-4 can function as a negative regulator of T cell activation. Immunity 1994, 1, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/yervoy (accessed on 22 August 2023).
- Miedema, I.H.; Zwezerijnen, G.J.; van Dongen, G.A. Tumor uptake and biodistribution of 89Zirconium-labeled ipilimumab in patients with metastatic melanoma during ipilimumab treatment. Clin. Cancer Res. 2019, 79, 1136. [Google Scholar]
- Higashikawa, K.; Yagi, K.; Watanabe, K.; Kamino, S.; Ueda, M.; Hiromura, M.; Enomoto, S. 64Cu-DOTA-anti-CTLA-4 mAb enabled PET visualization of CTLA-4 on the T-cell infiltrating tumor tissues. PLoS ONE 2014, 9, e109866. [Google Scholar] [CrossRef] [PubMed]
- Ehlerding, E.B.; England, C.G.; Majewski, R.L.; Valdovinos, H.F.; Jiang, D.; Liu, G.; McNeel, D.G.; Nickles, R.J.; Cai, W. ImmunoPET Imaging of CTLA-4 Expression in Mouse Models of Non-small Cell Lung Cancer. Mol. Pharm. 2017, 14, 1782–1789. [Google Scholar] [CrossRef]
- Ehlerding, E.B.; Lee, H.J.; Jiang, D.; Ferreira, C.A.; Zahm, C.D.; Huang, P.; Engle, J.W.; McNeel, D.G.; Cai, W. Antibody and fragment-based PET imaging of CTLA-4+ T-cells in humanized mouse models. Am. J. Cancer Res. 2019, 9, 53–63. [Google Scholar]
- Riley, J.L. PD-1 signaling in primary T cells. Immunol. Rev. 2009, 229, 114–125. [Google Scholar] [CrossRef]
- Sznol, M.; Chen, L. Antagonist antibodies to PD-1 and B7-H1 (PD-L1) in the treatment of advanced human cancer. Clin. Cancer Res. 2013, 19, 1021–1034. [Google Scholar] [CrossRef] [PubMed]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. Pd-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/opdivo (accessed on 22 August 2023).
- Niemeijer, A.N.; Leung, D.; Huisman, M.C.; Bahce, I.; Hoekstra, O.S.; van Dongen, G.A.M.S.; Boellaard, R.; Du, S.; Hayes, W.; Smith, R.; et al. Whole body PD-1 and PD-L1 positron emission tomography in patients with non-small-cell lung cancer. Nat. Commun. 2018, 9, 4664. [Google Scholar] [CrossRef] [PubMed]
- Kok, I.C.; Hooiveld, J.S.; van de Donk, P.P.; Giesen, D.; van der Veen, E.L.; Lub-de Hooge, M.N.; Brouwers, A.H.; Hiltermann, T.J.N.; van der Wekken, A.J.; Hijmering-Kappelle, L.B.M.; et al. 89Zr-pembrolizumab imaging as a non-invasive approach to assess clinical response to PD-1 blockade in cancer. Ann. Oncol. 2022, 33, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Niemeijer, A.N.; Oprea-Lager, D.E.; Huisman, M.C.; Hoekstra, O.S.; Boellaard, R.; de Wit-van der Veen, B.J.; Bahce, I.; Vugts, D.J.; van Dongen, G.A.M.S.; Thunnissen, E.; et al. Study of 89Zr-Pembrolizumab PET/CT in Patients with Advanced-Stage Non-Small Cell Lung Cancer. J. Nucl. Med. 2022, 63, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Bensch, F.; van der Veen, E.L.; Lub-de Hooge, M.N.; Jorritsma-Smit, A.; Boellaard, R.; Kok, I.C.; Oosting, S.F.; Schröder, C.P.; Hiltermann, T.J.N.; van der Wekken, A.J.; et al. 89Zr-atezolizumab imaging as a non-invasive approach to assess clinical response to PD-L1 blockade in cancer. Nat. Med. 2018, 24, 1852–1858. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Smit, J.; Borm, F.J.; Niemeijer, A.N.; Huisman, M.C.; Hoekstra, O.S.; Boellaard, R.; Oprea-Lager, D.E.; Vugts, D.J.; van Dongen, G.A.M.S.; de Wit-van der Veen, B.J.; et al. PD-L1 PET/CT Imaging with Radiolabeled Durvalumab in Patients with Advanced-Stage Non-Small Cell Lung Cancer. J. Nucl. Med. 2022, 63, 686–693. [Google Scholar] [CrossRef]
- Verhoeff, S.R.; van de Donk, P.P.; Aarntzen, E.H.J.G.; Oosting, S.F.; Brouwers, A.H.; Miedema, I.H.C.; Voortman, J.; Menke-van der Houven van Oordt, W.C.; Boellaard, R.; Vriens, D.; et al. 89Zr-DFO-Durvalumab PET/CT Before Durvalumab Treatment in Patients with Recurrent or Metastatic Head and Neck Cancer. J. Nucl. Med. 2022, 63, 1523–1530. [Google Scholar] [CrossRef]
- Hegi-Johnson, F.; Rudd, S.E.; Wichmann, C.; Akhurst, T.; Roselt, P.; Trinh, J.; John, T.; Devereux, L.; Donnelly, P.S.; Hicks, R.; et al. ImmunoPET: IMaging of cancer imMUNOtherapy targets with positron Emission Tomography: A phase 0/1 study characterising PD-L1 with 89Zr-durvalumab (MEDI4736) PET/CT in stage III NSCLC patients receiving chemoradiation study protocol. BMJ Open. 2022, 12, e056708. [Google Scholar] [CrossRef]
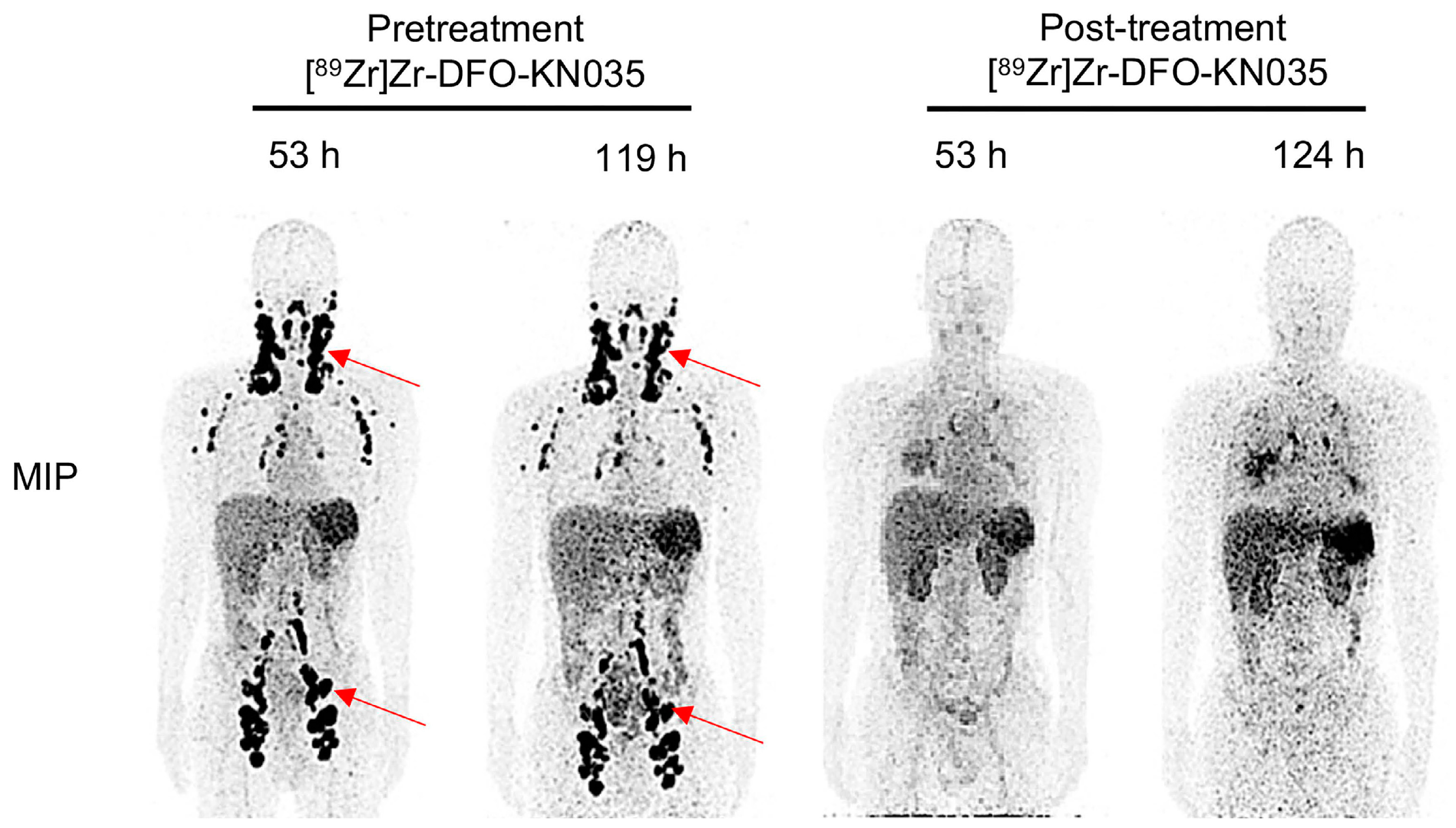
- He, H.; Qi, X.; Fu, H.; Xu, J.; Zheng, Q.; Chen, L.; Zhang, Y.; Hua, H.; Xu, W.; Xu, Z.; et al. Imaging diagnosis and efficacy monitoring by [89Zr]Zr-DFO-KN035 immunoPET in patients with PD-L1-positive solid malignancies. Theranostics 2024, 14, 392–405. [Google Scholar]
- Papadopoulos, K.P.; Harb, W.; Peer, C.J.; Hua, Q.; Xu, S.; Lu, H.; Lu, N.; He, Y.; Xu, T.; Dong, R.; et al. First-in-human phase I study of envafolimab, a novel subcutaneous single-domain anti-PD-L1 antibody, in patients with advanced solid tumors. Oncologist 2021, 26, e1514–e1525. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Deng, Y.; Zhang, W.; Zhou, A.P.; Guo, W.; Yang, J.; Yuan, Y.; Zhu, L.; Qin, S.; Xiang, S.; et al. Subcutaneous envafolimab monotherapy in patients with advanced defective mismatch repair/microsatellite instability high solid tumors. J. Hematol. Oncol. 2021, 14, 95. [Google Scholar] [CrossRef] [PubMed]
- Fu, R.; Carroll, L.; Yahioglu, G.; Aboagye, E.O.; Miller, P.W. Antibody Fragment and Affibody ImmunoPET Imaging Agents: Radiolabelling Strategies and Applications. ChemMedChem 2018, 13, 2466–2478. [Google Scholar] [CrossRef] [PubMed]
- Huisman, M.C.; Niemeijer, A.N.; Windhorst, A.D.; Schuit, R.C.; Leung, D.; Hayes, W.; Poot, A.; Bahce, I.; Radonic, T.; Oprea-Lager, D.E.; et al. Quantification of PD-L1 Expression with 18F-BMS-986192 PET/CT in Patients with Advanced-Stage Non-Small Cell Lung Cancer. J. Nucl. Med. 2020, 61, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Jiang, J.; Yang, X.; Liu, T.; Ding, J.; Nimmagadda, S.; Pomper, M.G.; Zhu, H.; Zhao, J.; Yang, Z.; et al. First-in-Humans Evaluation of a PD-L1-Binding Peptide PET Radiotracer in Non-Small Cell Lung Cancer Patients. J. Nucl. Med. 2022, 63, 536–542. [Google Scholar] [CrossRef]
- Kumar, D.; Lisok, A.; Dahmane, E.; McCoy, M.; Shelake, S.; Chatterjee, S.; Allaj, V.; Sysa-Shah, P.; Wharram, B.; Lesniak, W.G.; et al. Peptide-based PET quantifies target engagement of PD-L1 therapeutics. J. Clin. Investig. 2019, 129, 616–630. [Google Scholar] [CrossRef]
- Park, K.; Veena, M.S.; Shin, D.S. Key Players of the Immunosuppressive Tumor Microenvironment and Emerging Therapeutic Strategies. Front. Cell Dev. Biol. 2022, 10, 830208. [Google Scholar] [CrossRef]
- Mushtaq, M.U.; Papadas, A.; Pagenkopf, A.; Flietner, E.; Morrow, Z.; Chaudhary, S.G.; Asimakopoulos, F. Tumor matrix remodeling and novel immunotherapies: The promise of matrix-derived immune biomarkers. J. Immunother. Cancer 2018, 6, 65. [Google Scholar] [CrossRef]
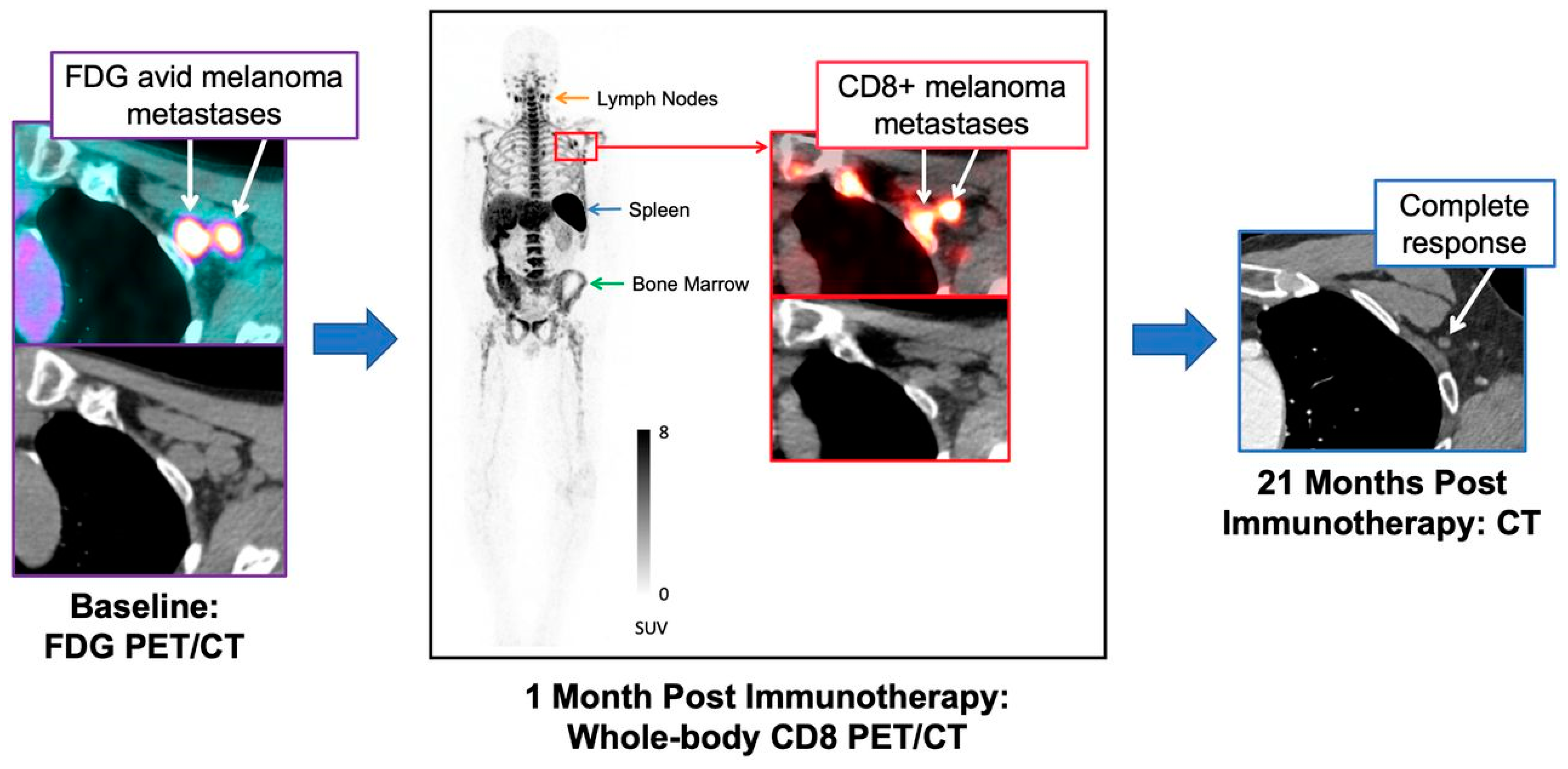
- Farwell, M.D.; Gamache, R.F.; Babazada, H.; Hellmann, M.D.; Harding, J.J.; Korn, R.; Mascioni, A.; Le, W.; Wilson, I.; Gordon, M.S.; et al. CD8-Targeted PET Imaging of Tumor-Infiltrating T Cells in Patients with Cancer: A Phase I First-in-Humans Study of 89Zr-Df-IAB22M2C, a Radiolabeled Anti-CD8 Minibody. J. Nucl. Med. 2022, 63, 720–726. [Google Scholar] [CrossRef]
- Pandit-Taskar, N.; Postow, M.A.; Hellmann, M.D.; Harding, J.J.; Barker, C.A.; O’Donoghue, J.A.; Ziolkowska, M.; Ruan, S.; Lyashchenko, S.K.; Tsai, F.; et al. First-in-Humans Imaging with 89Zr-Df-IAB22M2C Anti-CD8 Minibody in Patients with Solid Malignancies: Preliminary Pharmacokinetics, Biodistribution, and Lesion Targeting. J. Nucl. Med. 2020, 61, 512–519. [Google Scholar] [CrossRef]
- Kist de Ruijter, L.; van de Donk, P.P.; Hooiveld-Noeken, J.S.; Giesen, D.; Elias, S.G.; Lub-de Hooge, M.N.; Oosting, S.F.; Jalving, M.; Timens, W.; Brouwers, A.H.; et al. Whole-body CD8+ T cell visualization before and during cancer immunotherapy: A phase 1/2 trial. Nat. Med. 2022, 28, 2601–2610. [Google Scholar] [CrossRef] [PubMed]
- Nagle, V.L.; Henry, K.E.; Hertz, C.A.J.; Graham, M.S.; Campos, C.; Parada, L.F.; Pandit-Taskar, N.; Schietinger, A.; Mellinghoff, I.K.; Lewis, J.S. Imaging Tumor-Infiltrating Lymphocytes in Brain Tumors with [64Cu]Cu-NOTA-anti-CD8 PET. Clin. Cancer Res. 2021, 27, 1958–1966. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, C.; Huang, M.; Qin, S.; Zhao, J.; Sang, S.; Zheng, M.; Bian, Y.; Huang, C.; Zhang, H.; et al. Pilot study of a novel nanobody 68 Ga-NODAGA-SNA006 for instant PET imaging of CD8+ T cells. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4394–4405. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Wang, Y.; Xu, H.; Shen, X.; Zhang, T.; Zhou, X.; Zeng, Y.; Li, K.; Zhang, L.; Zhu, H.; et al. Noninvasive interrogation of CD8+ T cell effector function for monitoring early tumor responses to immunotherapy. J. Clin. Investig. 2022, 132, e161065. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Bardine, C.; Lourenço, A.L.; Wang, Y.H.; Huang, Y.; Cleary, S.J.; Wilson, D.M.; Oh, D.Y.; Fong, L.; Looney, M.R.; et al. In Vivo Measurement of Granzyme Proteolysis from Activated Immune Cells with PET. ACS Cent. Sci. 2021, 7, 1638–1649. [Google Scholar] [CrossRef] [PubMed]
- Larimer, B.M.; Bloch, E.; Nesti, S.; Austin, E.E.; Wehrenberg-Klee, E.; Boland, G.; Mahmood, U. The Effectiveness of Checkpoint Inhibitor Combinations and Administration Timing Can Be Measured by Granzyme B PET Imaging. Clin. Cancer Res. 2019, 25, 1196–1205. [Google Scholar] [CrossRef]
- Larimer, B.M.; Wehrenberg-Klee, E.; Dubois, F.; Mehta, A.; Kalomeris, T.; Flaherty, K.; Boland, G.; Mahmood, U. Granzyme B PET Imaging as a Predictive Biomarker of Immunotherapy Response. Cancer Res. 2017, 77, 2318–2327. [Google Scholar] [CrossRef]
- Levi, J.; Perk, T.; Huynh, L.; Juliet Packiasamy Cheng, S.; Sunwoo, J.; Dimitrios Colevas, A. AI-assisted whole-body assessment of immunotherapy response using [18F]F-AraG, a PET agent for activated T cells. J. Immuno Ther. Cancer 2021, 9, A52. [Google Scholar] [CrossRef]
- Ribas, A.; Benz, M.R.; Allen-Auerbach, M.S.; Radu, C.; Chmielowski, B.; Seja, E.; Williams, J.L.; Gomez-Navarro, J.; McCarthy, T.; Czernin, J. Imaging of CTLA4 blockade-induced cell replication with (18)F-FLT PET in patients with advanced melanoma treated with tremelimumab. J. Nucl. Med. 2010, 51, 340–346. [Google Scholar] [CrossRef]
- Prendergast, C.M.; Lopci, E.; Seban, R.D.; De Jong, D.; Ammari, S.; Aneja, S.; Lévy, A.; Sajan, A.; Salvatore, M.M.; Cappacione, K.M.; et al. Integrating [18F]-Fluorodeoxyglucose Positron Emission Tomography with Computed Tomography with Radiation Therapy and Immunomodulation in Precision Therapy for Solid Tumors. Cancers 2023, 15, 5179. [Google Scholar] [CrossRef]
- McGale, J.; Hama, J.; Yeh, R.; Vercellino, L.; Sun, R.; Lopci, E.; Ammari, S.; Dercle, L. Artificial Intelligence and Radiomics: Clinical Applications for Patients with Advanced Melanoma Treated with Immunotherapy. Diagnostics 2023, 13, 3065. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Identifier Number | Phase | Study Type | Status | Radiotracer | Study Title | Conditions | Country | Last Update |
|---|---|---|---|---|---|---|---|---|
| NCT04271436 | II | Interventional | Recruiting | [18F]F-FLT | Immune Checkpoint Blockade Therapy Using [18F]F-FLT PET/CT | Cancer | USA | 2023-05 |
| NCT05471271 | NA | Interventional | Recruiting | [18F]F-AlF-RESCA-IL2 | IL-2 PET Imaging in Advanced Solid Tumours | Metastatic solid tumors | The Netherlands | 2023-10 |
| NCT04721756 | Early Phase I | Interventional | Recruiting | [18F]F-LY3546117 | Early Clinical Evaluation of [18F]F-LY3546117 in Tumor Imaging | Malignant neoplasms | Australia | 2022-04 |
| NCT04706715 | I; II | Interventional | Recruiting | [89Zr]Zr-DFO-REGN3767 | LAG3 PET Imaging in Advanced Solid Tumors | Metastatic solid tumors | The Netherlands | 2023-02 |
| NCT04029181 | I; II | Interventional | Active; not recruiting | Anti-CD8 agent (ZED88082A) | ImmunoPET with an Anti-CD8 Imaging Agent | Metastatic cancer; unresectable malignant neoplasms | The Netherlands | 2023-05 |
| NCT04006522 | II | Interventional | Recruiting | [89Zr]Zr-DFO-Atezolizumab | [89Zr]Zr-DFO-Atezolizumab ImmunoPET/CT in Patients with Locally Advanced or Metastatic Renal Cell Carcinoma | Renal cell carcinoma | USA | 2023-06 |
| NCT05000372 | NA | Observational | Recruiting | [68Ga]Ga-grazytracer | [68Ga]Ga-grazytracer PET/CT in Subjects with Non-small Cell Lung Cancer or Melanoma | Non-small cell lung cancer; melanoma | China | 2023-03 |
| NCT05888532 | I; II | Interventional | Recruiting | [64Cu]Cu-GRIP B | [64Cu]Cu-GRIP B in Patients with Advanced Genitourinary Malignancies | Prostate cancer, renal cancer, and urethral cancer | USA | 2023-06 |
| NCT05629689 | I | Interventional | Recruiting | [18F]F-GEH200521 | A Study to Evaluate GEH200520/GEH200521 (18F) Safety and Tolerability When Used for PET Scans in Patients with Solid Tumour Malignancies | Irresectable or metastatic solid tumors or local and resectable head and neck squamous cell carcinomas | The Netherlands | 2023-09 |
| NCT04726215 | II | Interventional | Recruiting | [18F]F AraG | Imaging of T-cell Activation with [18F]F-AraG in Advanced Non-Small Cell Lung Cancer | Non-small cell lung cancer | USA | 2023-09 |
| NCT04260256 | II | Interventional | Recruiting | [18F]F AraG | A Study Using [18F]F AraG PET to Evaluate Response to Checkpoint Inhibitor Therapy(CkIT) in Patients with Solid Tumors | Advanced solid tumors | USA | 2023-10 |
| NCT04524195 | I | Interventional | Recruiting | [18F]F AraG | PET Imaging with [18F]F-AraG in Advanced Non-small Cell Lung Cancer (NSCLC) | Non-small cell lung cancer | USA | 2023-01 |
| NCT05157659 | NA | Interventional | Recruiting | [18F]F AraG | [18F]F-AraG PET Imaging to Visualize Tumor Infiltrating T-cell Activation in Non-small Cell Lung Cancer (ATTAIN) | Non-small cell lung cancer | The Netherlands | 2023-04 |
| NCT05701176 | NA | Interventional | Recruiting | [18F]F AraG | A Clinical Imaging Study of the Changes in [18F]F-AraG Uptake Following Anti-PD-1 Therapy in Non-small Cell Lung Cancer (SHARP) | Advanced stage non-small cell lung cancer | The Netherlands | 2023-01 |
| NCT05533086 | NA | Observational | Recruiting | [68Ga]Ga-BMS986192 | PD-L1 PET Imaging in Patients with Immunotherapy for Non-small Cell Lung Cancer | NSCLC stage IV; PD-L1 gene amplification | China | 2023-02 |
| NCT02453984 | NA | Interventional | Active; not recruiting | [89Zr]Zr-MPDL3280A | MPDL3280A-imaging-IST-UMCG | Locally advanced or metastatic solid tumors irrespective of PD-L1 expression | The Netherlands | 2023-01 |
| NCT04401995 | II | Interventional | Recruiting | [18F]F-AraG | Study of TLR9 Agonist Vidutolimod (CMP-001) in Combination with Nivolumab vs. Nivolumab | Melanoma | USA | 2023-02 |
| NCT05289193 | II | Interventional | Recruiting | [89Zr]Zr-Df-Crefmirlimab | CD8+ T Cell Imaging During Pre-surgery Immunotherapy in People with Melanoma | Melanoma stage III | USA | 2023-04 |
| NCT03843515 | I | Interventional | Unknown status | [18F]FBMS-986192/2-[18F]FDG PET | Neoadjuvant Nivolumab for Oral Cancer Combined with FDG and Anti-PD-L1 PET/CT Imaging for Response Prediction (NeoNivo) | Oral cavity squamous cell carcinoma | The Netherlands | 2021-10 |
| NCT05742269 | NA | Observational | Recruiting | [89Zr]Zr-atezolizumab | Molecular PD-L1 PET/CT Imaging with [89Zr]Zr-atezolizumab in Metastatic Triple Negative Breast Cancer (MIMIR-mTNBC) | Metastatic triple-negative breast carcinoma | Sweden | 2023-10 |
| NCT03313323 | II | Interventional | Unknown status | [89Zr]Zr-ipilimumab | Uptake and Biodistribution of 89Zirconium-labeled Ipilimumab in Ipilimumab Treated Patients with Metastatic Melanoma (Zirconipi) | Melanoma | The Netherlands | 2021-04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abenavoli, E.M.; Linguanti, F.; Calabretta, R.; Delgado Bolton, R.C.; Berti, V.; Lopci, E. Clinical Application of ImmunoPET Targeting Checkpoint Inhibitors. Cancers 2023, 15, 5675. https://doi.org/10.3390/cancers15235675
Abenavoli EM, Linguanti F, Calabretta R, Delgado Bolton RC, Berti V, Lopci E. Clinical Application of ImmunoPET Targeting Checkpoint Inhibitors. Cancers. 2023; 15(23):5675. https://doi.org/10.3390/cancers15235675
Chicago/Turabian StyleAbenavoli, Elisabetta Maria, Flavia Linguanti, Raffaella Calabretta, Roberto C. Delgado Bolton, Valentina Berti, and Egesta Lopci. 2023. "Clinical Application of ImmunoPET Targeting Checkpoint Inhibitors" Cancers 15, no. 23: 5675. https://doi.org/10.3390/cancers15235675
APA StyleAbenavoli, E. M., Linguanti, F., Calabretta, R., Delgado Bolton, R. C., Berti, V., & Lopci, E. (2023). Clinical Application of ImmunoPET Targeting Checkpoint Inhibitors. Cancers, 15(23), 5675. https://doi.org/10.3390/cancers15235675