
The Current Treatment Trends and Survival Patterns in Melanoma Patients with Positive Sentinel Lymph Node Biopsy (SLNB): A Multicenter Nationwide Study

 , , , , ,
, , , , ,  and
and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Characteristics of the Study Group
3.2. Treatment Trends
3.3. Relapse-Free Survival Analysis
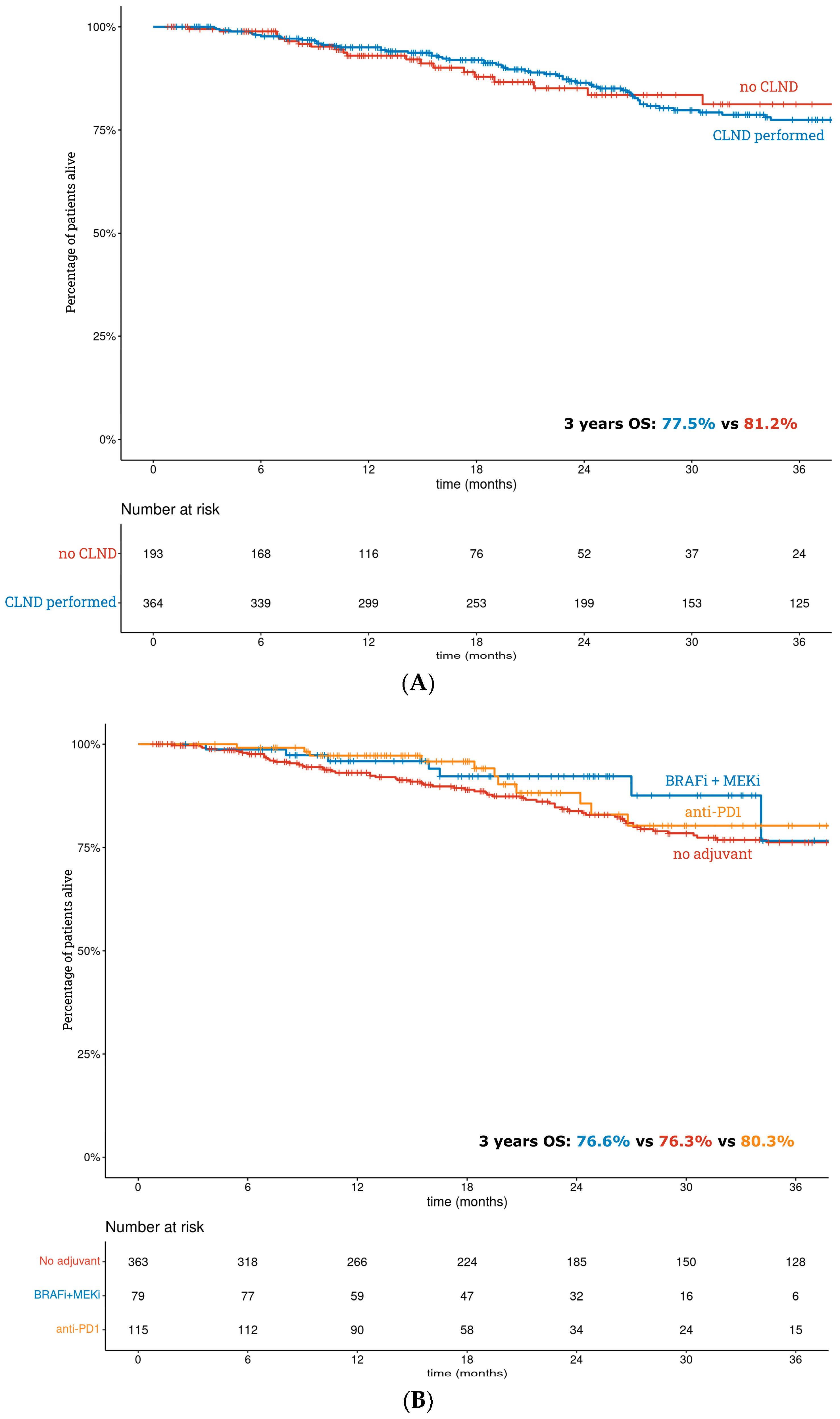
3.4. Overall Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scala, J.; Vojvodic, A.; Vojvodic, P.; Vlaskovic-Jovicevic, T.; Peric-Hajzler, Z.; Matovic, D.; Dimitrijevic, S.; Vojvodic, J.; Sijan, G.; Stepic, N.; et al. New Trends in Cutaneous Melanoma Surgery. Open Access Maced. J. Med. Sci. 2019, 7, 3090–3092. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Borgognoni, L.; Botti, G.; Guida, M.; Marchetti, P.; Mocellin, S.; Muto, P.; Palmieri, G.; Patuzzo, R.; Quaglino, P.; et al. New paradigm for stage III melanoma: From surgery to adjuvant treatment. J. Transl. Med. 2019, 17, 266. [Google Scholar] [CrossRef]
- Mott, N.M.; Duncan, Z.N.; Pesavento, C.M.; Vastardis, A.F.; Bredbeck, B.C.; Harter, C.A.; Dossett, L.A.; Broman, K.K.; Hughes, T.M. Implementation of melanoma guidelines in the multidisciplinary setting: A qualitative analysis. Am. J. Surg. 2022, 225, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Farrow, N.E.; Raman, V.; Williams, T.P.; Nguyen, K.Y.; Tyler, D.S.; Beasley, G.M. Adjuvant Therapy is Effective for Melanoma Patients with a Positive Sentinel Lymph Node Biopsy Who Forego Completion Lymphadenectomy. Ann. Surg. Oncol. 2020, 27, 5121–5125. [Google Scholar] [CrossRef] [PubMed]
- Morton, D.L.; Cochran, A.J.; Thompson, J.F.; Elashoff, R.; Essner, R.; Glass, E.C.; Mozzillo, N.; Nieweg, O.E.; Roses, D.F.; Hoekstra, H.J.; et al. Sentinel node biopsy for early-stage melanoma: Accuracy and morbidity in MSLT-I, an international multicenter trial. Ann. Surg. 2005, 242, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Morton, D.L.; Thompson, J.F.; Cochran, A.J.; Mozzillo, N.; Nieweg, O.E.; Roses, D.F.; Hoekstra, H.J.; Karakousis, C.P.; Puleo, C.A.; Coventry, B.J.; et al. Final trial report of sentinel-node biopsy versus nodal observation in melanoma. N. Engl. J. Med. 2014, 370, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Faries, M.B.; Thompson, J.F.; Cochran, A.J.; Andtbacka, R.H.; Mozzillo, N.; Zager, J.S.; Jahkola, T.; Bowles, T.L.; Testori, A.; Beitsch, P.D.; et al. Completion Dissection or Observation for Sentinel-Node Metastasis in Melanoma. N. Engl. J. Med. 2017, 376, 2211–2222. [Google Scholar] [CrossRef]
- Leiter, U.; Stadler, R.; Mauch, C.; Hohenberger, W.; Brockmeyer, N.; Berking, C.; Sunderkötter, C.; Kaatz, M.; Schulte, K.-W.; Lehmann, P.; et al. Complete lymph node dissection versus no dissection in patients with sentinel lymph node biopsy positive melanoma (DeCOG-SLT): A multicentre, randomised, phase 3 trial. Lancet Oncol. 2016, 17, 757–767. [Google Scholar] [CrossRef]
- Leiter, U.; Stadler, R.; Mauch, C.; Hohenberger, W.; Brockmeyer, N.H.; Berking, C.; Sunderkötter, C.; Kaatz, M.; Schatton, K.; Lehmann, P.; et al. Final Analysis of DeCOG-SLT Trial: No Survival Benefit for Complete Lymph Node Dissection in Patients with Melanoma with Positive Sentinel Node. J. Clin. Oncol. 2019, 37, 3000–3008. [Google Scholar] [CrossRef]
- Montgomery, K.B.; Correya, T.A.; Broman, K.K. Real-World Adherence to Nodal Surveillance for Sentinel Lymph Node-Positive Melanoma. Ann. Surg. Oncol. 2022, 29, 5961–5968. [Google Scholar] [CrossRef]
- Munkhammar, S.; Sars, C.; Schultz, I.; Gillgren, P.; Lindqvist, E.K. Complications after surgery for malignant melanoma do not delay further treatment. Eur. J. Plast. Surg. 2022, 45, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Ophuis, C.O.; Verhoef, C.; Rutkowski, P.; Powell, B.; van der Hage, J.; van Leeuwen, P.; Voit, C.; Testori, A.; Robert, C.; Hoekstra, H.; et al. The interval between primary melanoma excision and sentinel node biopsy is not associated with survival in sentinel node positive patients—An EORTC Melanoma Group study. Eur. J. Surg. Oncol. 2016, 42, 1906–1913. [Google Scholar] [CrossRef] [PubMed]
- Ziętek, M.; Zdzienicki, M.; Wierzbicki, J.; Cybulska-Stopa, B.; Krotewicz, M.; Łobaziewicz, W.; Wysocki, W.M.; Kamińska-Winciorek, G.; Turska-D’amico, M.; Rutkowski, P. Survival of patients with stage IIIC and IIID melanomas with nodal metastases in the light of new therapies. Adv. Dermatol. Allergol. 2022, 39, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Hauschild, A.; Santinami, M.; Atkinson, V.; Mandalà, M.; Sileni, V.C.; Larkin, J.; Nyakas, M.; Dutriaux, C.; Haydon, A.; et al. Adjuvant Dabrafenib plus Trametinib in Stage III BRAF-Mutated Melanoma. N. Engl. J. Med. 2017, 377, 1813–1823. [Google Scholar] [CrossRef]
- Eggermont, A.M.M.; Blank, C.U.; Mandalà, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.; Lichinitser, M.; Khattak, A.; Carlino, M.S.; et al. Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma. N. Engl. J. Med. 2018, 378, 1789–1801. [Google Scholar] [CrossRef]
- Michielin, O.; Van Akkooi, A.C.J.; Ascierto, P.A.; Dummer, R.; Keilholz, U.; ESMO Guidelines Committee. Electronic address: Clinicalguidelines@esmo.org. Cutaneous melanoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. 2019, 30, 1884–1901. [Google Scholar] [CrossRef]
- Weber, J.; Mandalà, M.; Del Vecchio, M.; Gogas, H.J.; Arance, A.M.; Cowey, C.L.; Dalle, S.; Schenker, M.; Chiarion-Sileni, V.; Marquez-Rodas, I.; et al. Adjuvant Nivolumab versus Ipilimumab in Resected Stage III or IV Melanoma. N. Engl. J. Med. 2017, 377, 1824–1835. [Google Scholar] [CrossRef]
- Garbe, C.; Amaral, T.; Peris, K.; Hauschild, A.; Arenberger, P.; Bastholt, L.; Bataille, V.; del Marmol, V.; Dréno, B.; Fargnoli, M.C.; et al. European consensus-based interdisciplinary guideline for melanoma. Part 2: Treatment—Update 2019. Eur. J. Cancer 2020, 126, 159–177. [Google Scholar] [CrossRef]
- Forsea, A.M. Melanoma Epidemiology and Early Detection in Europe: Diversity and Disparities. Dermatol. Pract. Concept. 2020, 10, e2020033. [Google Scholar] [CrossRef]
- dos Santos, F.L.C.; Wojciechowska, U.; Michalek, I.M.; Didkowska, J. Progress in cancer survival across last two decades: A nationwide study of over 1.2 million Polish patients diagnosed with the most common cancers. Cancer Epidemiol. 2022, 78, 102147. [Google Scholar] [CrossRef]
- Bello, D.M.; Faries, M.B. The Landmark Series: MSLT-1, MSLT-2 and DeCOG (Management of Lymph Nodes). Ann. Surg. Oncol. 2020, 27, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A. Sentinel Lymph Node Biopsy: Past and Present Implications for the Management of Cutaneous Melanoma with Nodal Metastasis. Am. J. Clin. Dermatol. 2018, 19 (Suppl. 1), 24–30. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Szydłowski, K.; Nowecki, Z.I.; Sałamacha, M.; Goryn, T.; Mitręga-Korab, B.; Pieñkowski, A.; Dziewirski, W.; Zdzienicki, M. The long-term results and prognostic significance of cutaneous melanoma surgery using sentinel node biopsy with triple technique. World J. Surg. Oncol. 2015, 13, 299. [Google Scholar] [CrossRef]
- Karlsson, A.K.; Saleh, S.N. Checkpoint inhibitors for malignant melanoma: A systematic review and meta-analysis. Clin. Cosmet. Investig. Dermatol. 2017, 10, 325–339. [Google Scholar] [CrossRef] [PubMed]
- Hauschild, A.; Dummer, R.; Schadendorf, D.; Santinami, M.; Atkinson, V.; Mandalà, M.; Chiarion-Sileni, V.; Larkin, J.; Nyakas, M.; Dutriaux, C.; et al. Longer Follow-Up Confirms Relapse-Free Survival Benefit with Adjuvant Dabrafenib Plus Trametinib in Patients with Resected BRAF V600-Mutant Stage III Melanoma. J. Clin. Oncol. 2018, 36, 3441–3449. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, A.M.M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.G.; Dalle, S.; Haydon, A.M.; Meshcheryakov, A.; Khattak, A.; Carlino, M.S.; et al. Longer Follow-Up Confirms Recurrence-Free Survival Benefit of Adjuvant Pembrolizumab in High-Risk Stage III Melanoma: Updated Results from the EORTC 1325-MG/KEYNOTE-054 Trial. J. Clin. Oncol. 2020, 38, 3925–3936. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, A.M.; Kicinski, M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.; Meshcheryakov, A.; Khattak, A.; et al. Five-Year Analysis of Adjuvant Pembrolizumab or Placebo in Stage III Melanoma. NEJM Evid. 2022, 1, EVIDoa2200214. [Google Scholar] [CrossRef]
- Sharon, C.E.; Straker, R.J., 3rd; Li, E.H.; Karakousis, G.C.; Miura, J.T. National Practice Patterns in the Management of the Regional Lymph Node Basin After Positive Sentinel Lymph Node Biopsy for Cutaneous Melanoma. Ann. Surg. Oncol. 2022, 29, 8456–8464. [Google Scholar] [CrossRef]
- Mandalà, M.; Rutkowski, P.; Galli, F.; Patuzzo, R.; De Giorgi, V.; Rulli, E.; Gianatti, A.; Valeri, B.; Merelli, B.; Szumera-Ciećkiewicz, A.; et al. Acral lentiginous melanoma histotype predicts outcome in clinical stage I-II melanoma patients: An International multicenter study. ESMO Open 2022, 7, 100469. [Google Scholar] [CrossRef]
- Morrison, S.; Han, D. Re-evaluation of Sentinel Lymph Node Biopsy for Melanoma. Curr. Treat. Options Oncol. 2021, 22, 22. [Google Scholar] [CrossRef]
- Castle, J.T.; Adatorwovor, R.; Levy, B.E.; Marcinkowski, E.F.; Merritt, A.; Stapleton, J.L.; Burke, E.E. Completion Lymph Node Dissection for Melanoma Before and After the Multicenter Selective Lymphadenectomy Trial-II in the United States. Ann. Surg. Oncol. 2023, 30, 1184–1193. [Google Scholar] [CrossRef] [PubMed]
- Nacchiero, E.; Maruccia, M.; Vestita, M.; Elia, R.; Marannino, P.; Giudice, G. Multiple lymphatic-venous anastomoses in reducing the risk of lymphedema in melanoma patients undergoing complete lymph node dissection. A retrospective case-control study. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Wysocki, P.J.; Nasierowska-Guttmejer, A.; Jeziorski, A.; Wysocki, W.M.; Kalinka, E.; Świtaj, T.; Kozak, K.; Kamińska-Winciorek, G.; Czarnecka, A.M.; et al. Cutaneous melanomas. Oncol. Clin. Pract. 2020, 16, 163–182. [Google Scholar] [CrossRef]
- Rutkowski, P.; Wysocki, P.; Kozak, K.; Nasierowska-Guttmejer, A.; Jeziorski, A.; Wysocki, W.M.; Kalinka, E.; Świtaj, T.; Kamińska-Winciorek, G.; Czarnecka, A.M.; et al. Expert recommendations on diagnostic-therapeutic management of melanoma patients. Oncol. Clin. Pract. 2022, 18, 357–392. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Number (n) | Percentage (%) | |
|---|---|---|---|
| Treatment group | CLND 1 alone | 248 | 44.5 |
| CLND 1 + adjuvant | 116 | 20.8 | |
| Adjuvant therapy alone | 79 | 14.2 | |
| Observation only after SLNB 2 | 114 | 20.5 | |
| Gender | male | 312 | 56.0 |
| female | 245 | 44.0 | |
| Age (mean ± SD, years) | 58.0 ± 15.9 | ||
| T stage | T1–T2 | 139 | 25.0 |
| T3 | 179 | 32.1 | |
| T4 or unknown | 239 | 42.9 | |
| Melanoma histologic subtype | NM 3 | 194 | 34.8 |
| SSM 4 | 107 | 19.2 | |
| unspecified and other | 256 | 46.0 | |
| Melanoma ulceration | yes | 343 | 61.6 |
| no | 202 | 36.3 | |
| unknown | 12 | 2.2 | |
| BRAF status | positive | 278 | 49.9 |
| negative | 162 | 29.1 | |
| unknown | 117 | 21.0 | |
| Surgery site of primary tumor | head and neck | 40 | 7.2 |
| upper limb | 100 | 18.0 | |
| trunk | 251 | 45.1 | |
| lower limb | 129 | 23.2 | |
| unknown | 37 | 6.6 | |
| SLN 5 positive count (mean ± SD) | 1.2 ± 0.7 | ||
| SLN 5 total number (mean ± SD) | 2.5 ± 2.0 | ||
| SLN 5 metastasis diameter | less or equal 1 mm | 112 | 20.1 |
| over 1 mm | 333 | 59.8 | |
| unknown | 112 | 20.1 | |
| CLND 1 performed | yes | 364 | 65.4 |
| no | 193 | 34.6 | |
| Adjuvant therapy | yes | 194 | 34.8 |
| no | 363 | 65.2 | |
| Systemic treatment regimen | BRAFi/MEKi 6 | 79 | 14.2 |
| PD1 7 | 115 | 20.6 | |
| Factors | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| T stage (ref. level: T1/T2) | T3 | 1.43 (0.89–2.28) | 0.136 | 1.12 (0.68–1.84) | 0.652 |
| T4 or unknown | 2.57 (1.68–3.93) | 0.001 | 1.82 (1.13–2.92) | 0.012 | |
| Melanoma histologic subtype (ref. level: = NM 1) | SSM 2 | 0.48 (0.30–0.77) | 0.003 | 0.72 (0.44–1.20) | 0.215 |
| unspecified and other | 0.71 (0.51–0.97) | 0.033 | 0.70 (0.50–0.98) | 0.036 | |
| Melanoma ulceration (ref. level: no) | present | 2.15 (1.51–3.05) | 0.001 | 1.69 (1.14–2.50) | 0.009 |
| CLND 3 (ref. level: = no) | yes | 1.22 (0.86–1.73) | 0.272 | 1.03 (0.71–1.49) | 0.871 |
| Systemic treatment regimen (ref. level: = none) | BRAFi 4: group on treatment * | 0.47 (0.27–0.84) | 0.011 | 0.20 (0.07–0.56) | 0.002 |
| BRAFi: group subsequently * | 0.83 (0.39–1.78) | 0.634 | |||
| PD1i 5: group on treatment * | 0.83 (0.56–1.23) | 0.357 | 0.50 (0.28–0.87) | 0.015 | |
| PD1i: group subsequently * | 1.09 (0.61–1.95) | 0.784 | |||
| Factors | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| Age (quantitative) (per 1 year change) | 1.04 (1.02–1.05) | 0.001 | 1.03 (1.01–1.05) | 0.001 | |
| T stage (ref. level: = T1/T2) | T3 | 1.99 (1.01–3.92) | 0.048 | 1.40 (0.69–2.84) | 0.345 |
| T4 or unknown | 2.81 (1.49–5.31) | 0.001 | 1.54 (0.78–3.07) | 0.218 | |
| Melanoma histologic subtype (ref. level: = NM 1) | SSM 2 | 0.42 (0.21–0.81) | 0.010 | 0.61 (0.30–1.22) | 0.163 |
| unspecified and other | 0.46 (0.29–0.72) | 0.001 | 0.55 (0.34–0.89) | 0.015 | |
| Melanoma ulceration (ref. level: = no) | present | 3.21 (1.81–5.70) | 0.001 | 2.37 (1.28–4.37) | 0.006 |
| BRAF status (ref. level: = negative) | positive | 0.44 (0.27–0.72) | 0.001 | 0.56 (0.33–0.97) | 0.040 |
| unknown | 0.84 (0.47–1.55) | 0.593 | |||
| CLND 3 (ref. level: = no) | yes | 0.94 (0.58–1.53) | 0.801 | 0.91 (0.56–1.51) | 0.739 |
| Systemic treatment regimen (ref. level: = none) | BRAFi 4 | 0.70 (0.33–1.46) | 0.343 | 1.16 (0.49–2.75) | 0.741 |
| PD1 5 | 0.74 (0.40–1.38) | 0.342 | 0.82 (0.42–1.60) | 0.562 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziętek, M.; Teterycz, P.; Wierzbicki, J.; Jankowski, M.; Las-Jankowska, M.; Zegarski, W.; Piekarski, J.; Nejc, D.; Drucis, K.; Cybulska-Stopa, B.; et al. The Current Treatment Trends and Survival Patterns in Melanoma Patients with Positive Sentinel Lymph Node Biopsy (SLNB): A Multicenter Nationwide Study. Cancers 2023, 15, 2667. https://doi.org/10.3390/cancers15102667
Ziętek M, Teterycz P, Wierzbicki J, Jankowski M, Las-Jankowska M, Zegarski W, Piekarski J, Nejc D, Drucis K, Cybulska-Stopa B, et al. The Current Treatment Trends and Survival Patterns in Melanoma Patients with Positive Sentinel Lymph Node Biopsy (SLNB): A Multicenter Nationwide Study. Cancers. 2023; 15(10):2667. https://doi.org/10.3390/cancers15102667
Chicago/Turabian StyleZiętek, Marcin, Paweł Teterycz, Jędrzej Wierzbicki, Michał Jankowski, Manuela Las-Jankowska, Wojciech Zegarski, Janusz Piekarski, Dariusz Nejc, Kamil Drucis, Bożena Cybulska-Stopa, and et al. 2023. "The Current Treatment Trends and Survival Patterns in Melanoma Patients with Positive Sentinel Lymph Node Biopsy (SLNB): A Multicenter Nationwide Study" Cancers 15, no. 10: 2667. https://doi.org/10.3390/cancers15102667
APA StyleZiętek, M., Teterycz, P., Wierzbicki, J., Jankowski, M., Las-Jankowska, M., Zegarski, W., Piekarski, J., Nejc, D., Drucis, K., Cybulska-Stopa, B., Łobaziewicz, W., Galwas, K., Kamińska-Winciorek, G., Zdzienicki, M., Sryukina, T., Ziobro, A., Kluz, A., Czarnecka, A. M., & Rutkowski, P. (2023). The Current Treatment Trends and Survival Patterns in Melanoma Patients with Positive Sentinel Lymph Node Biopsy (SLNB): A Multicenter Nationwide Study. Cancers, 15(10), 2667. https://doi.org/10.3390/cancers15102667