
The Role of HPV in Determining Treatment, Survival, and Prognosis of Head and Neck Squamous Cell Carcinoma

 , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Specimen Collection
2.2. Preparation of the Tissue Sections
2.3. Histological Analysis
2.4. HPV DNA Genotyping
2.5. Statistical Analysis
3. Results
3.1. Summary of the Study Population
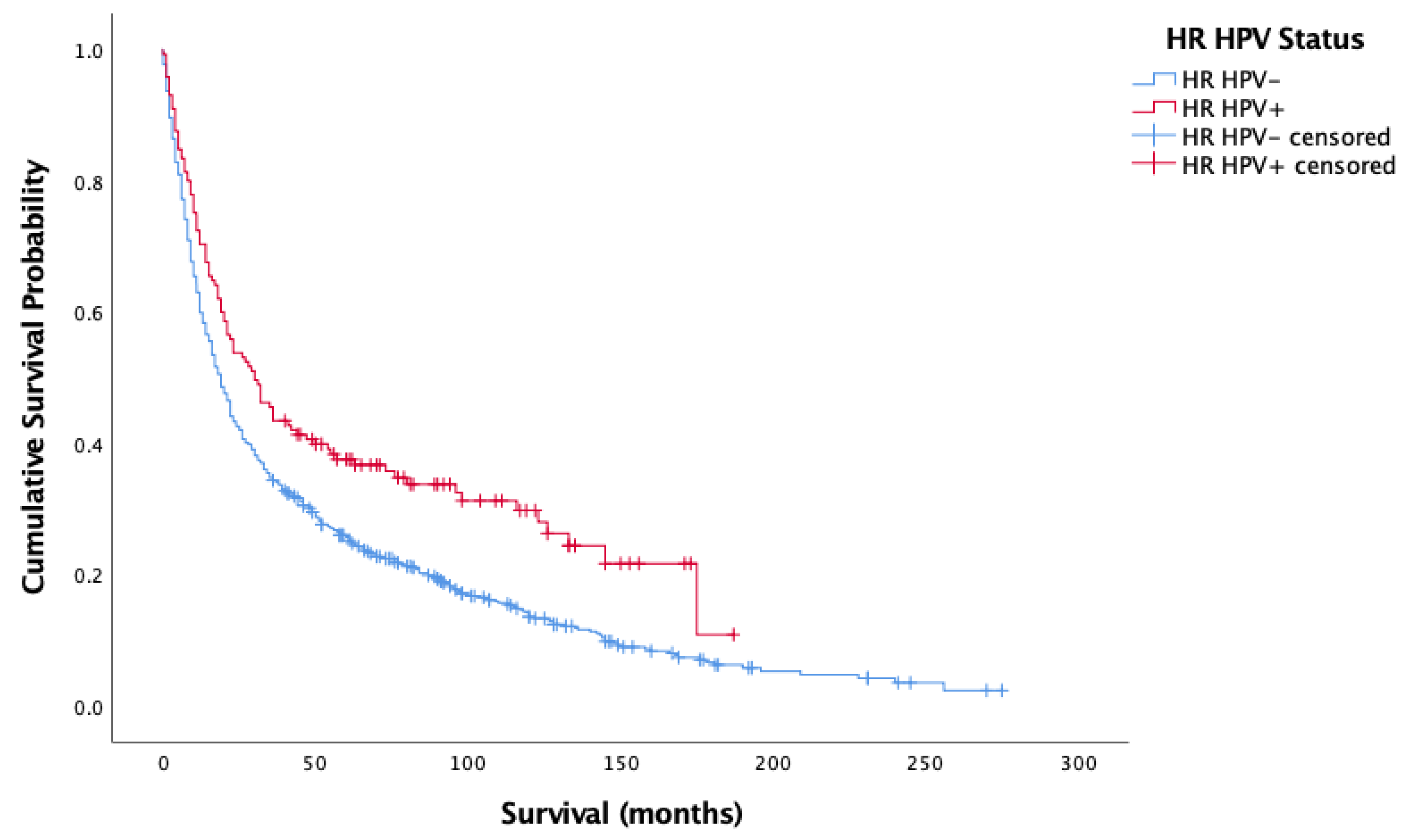
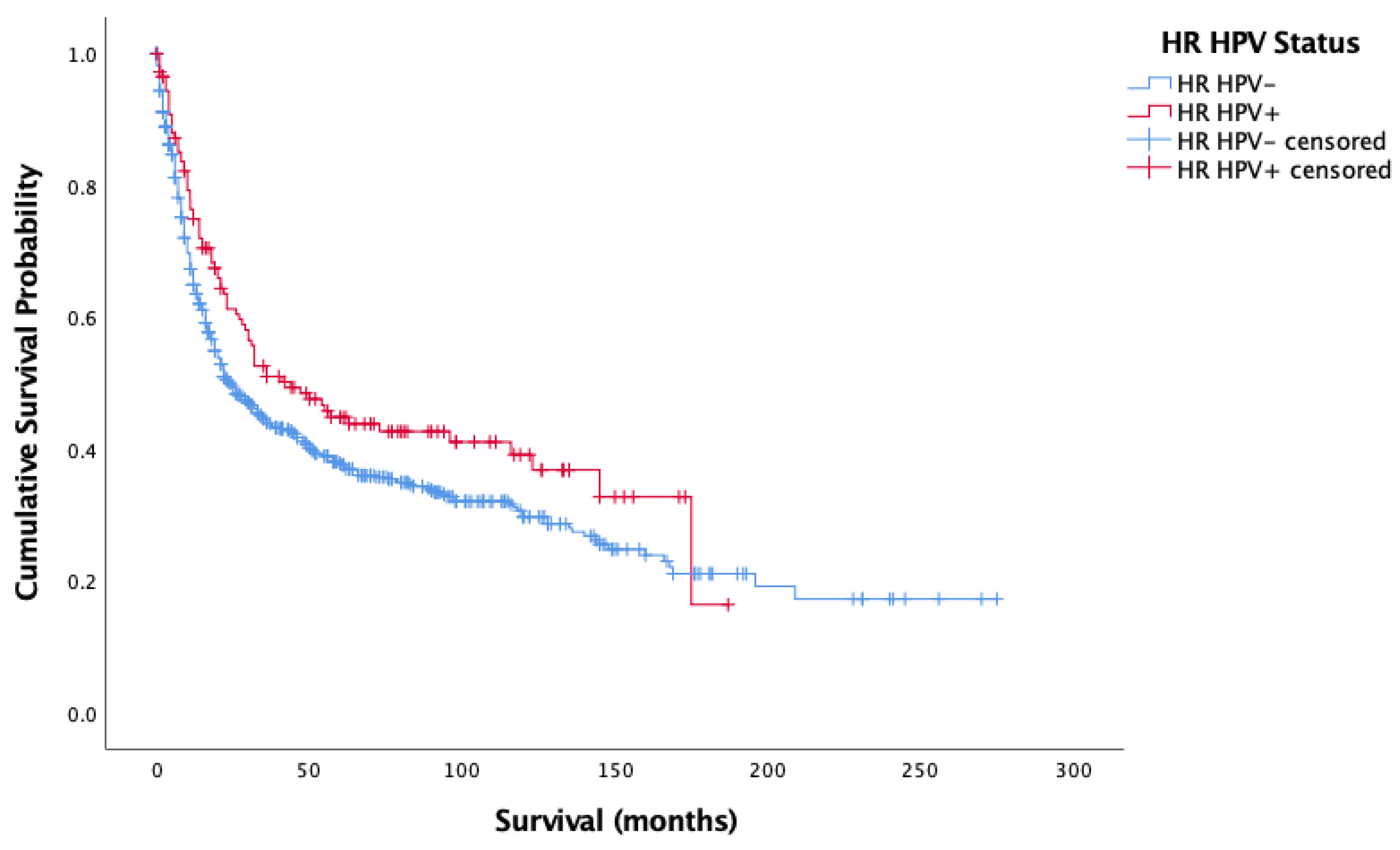
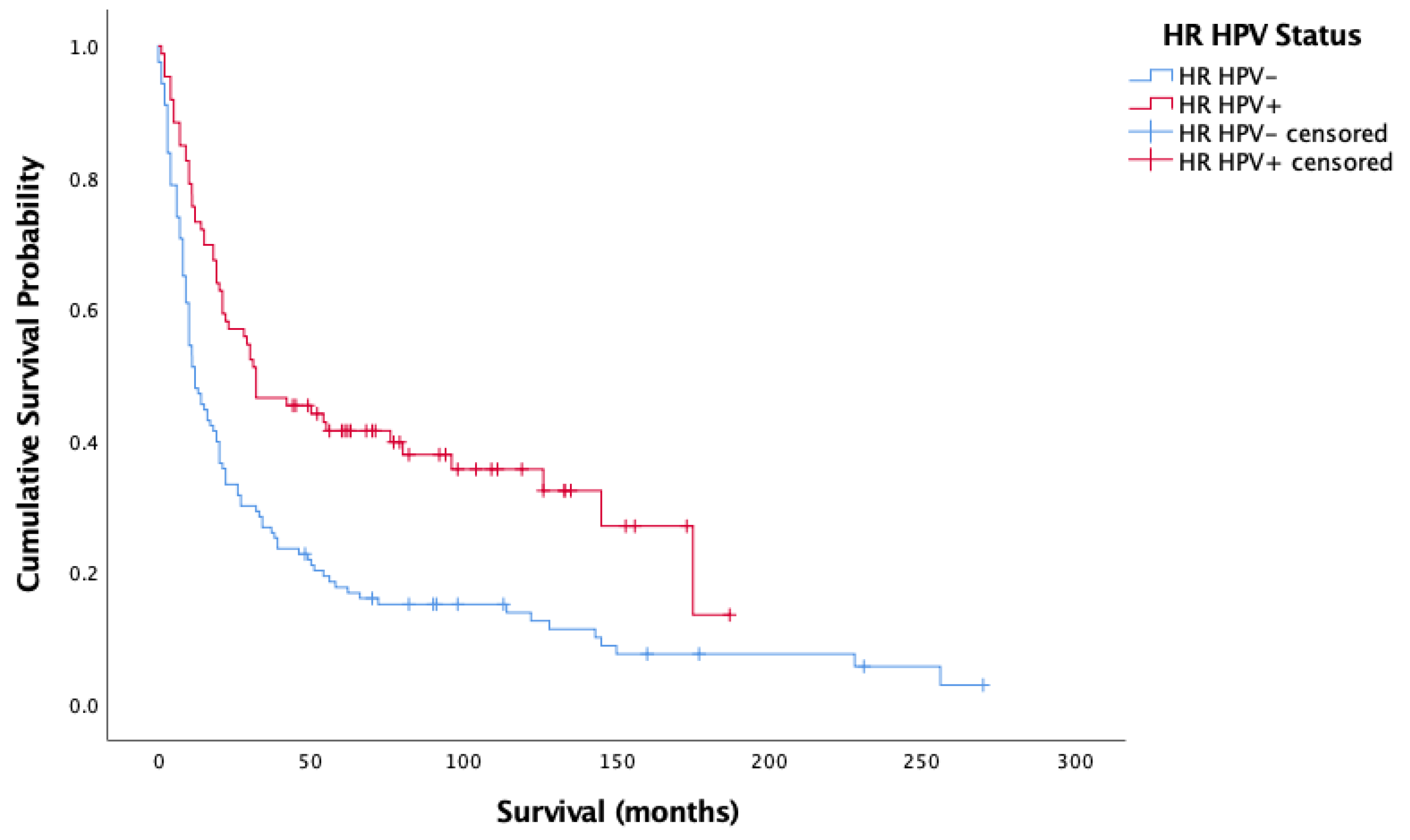
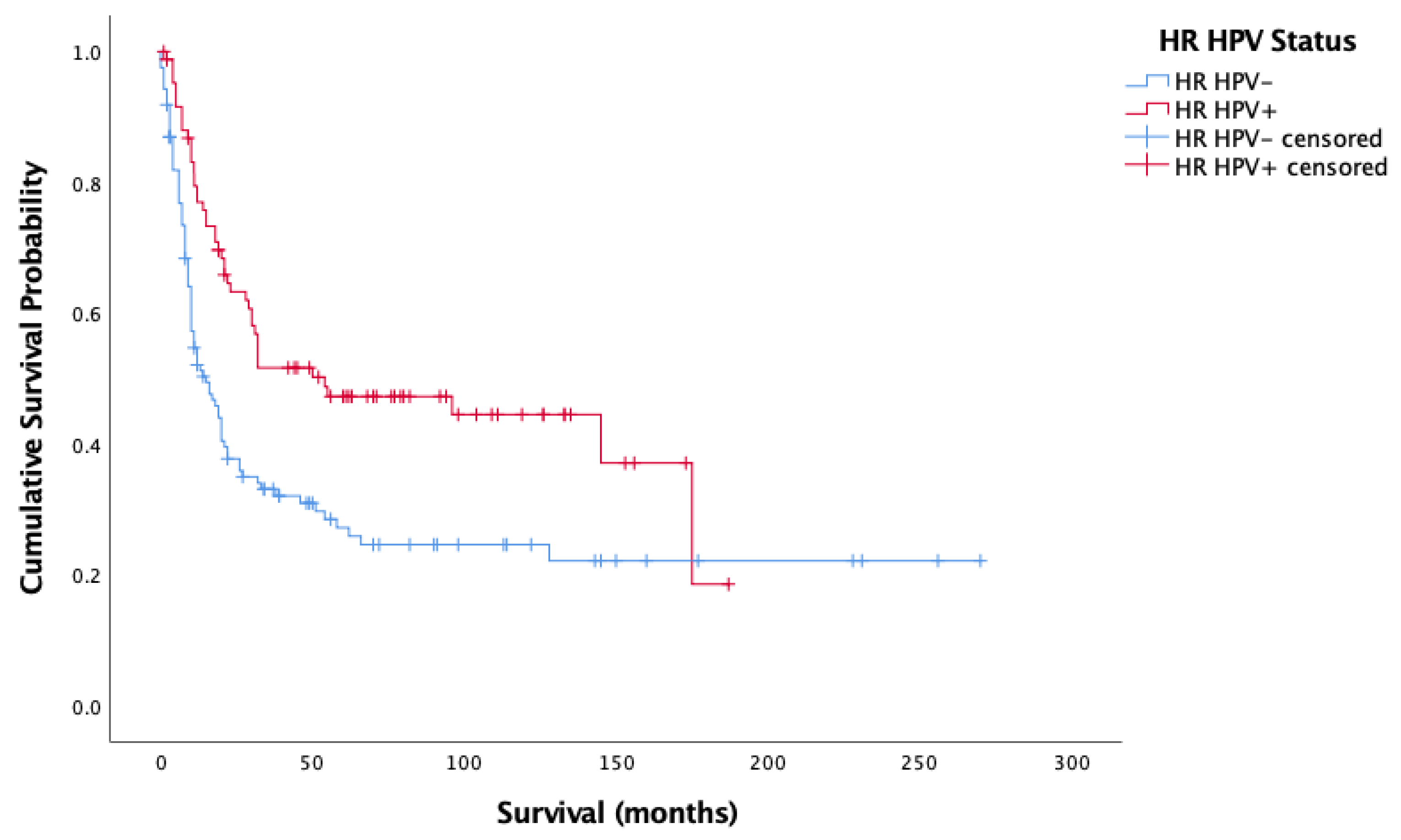
3.2. Survival by HPV DNA Status
3.3. The Relationship between Treatment Modality and HPV Status
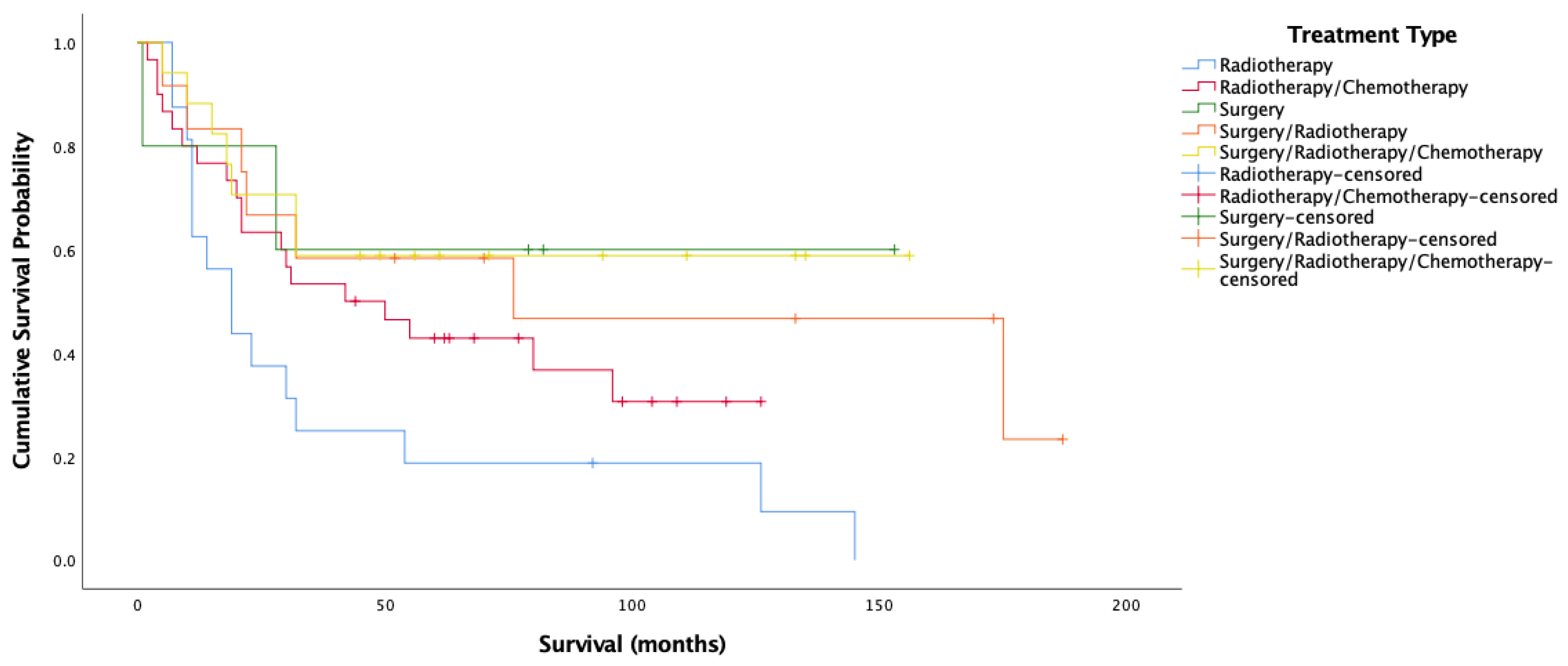
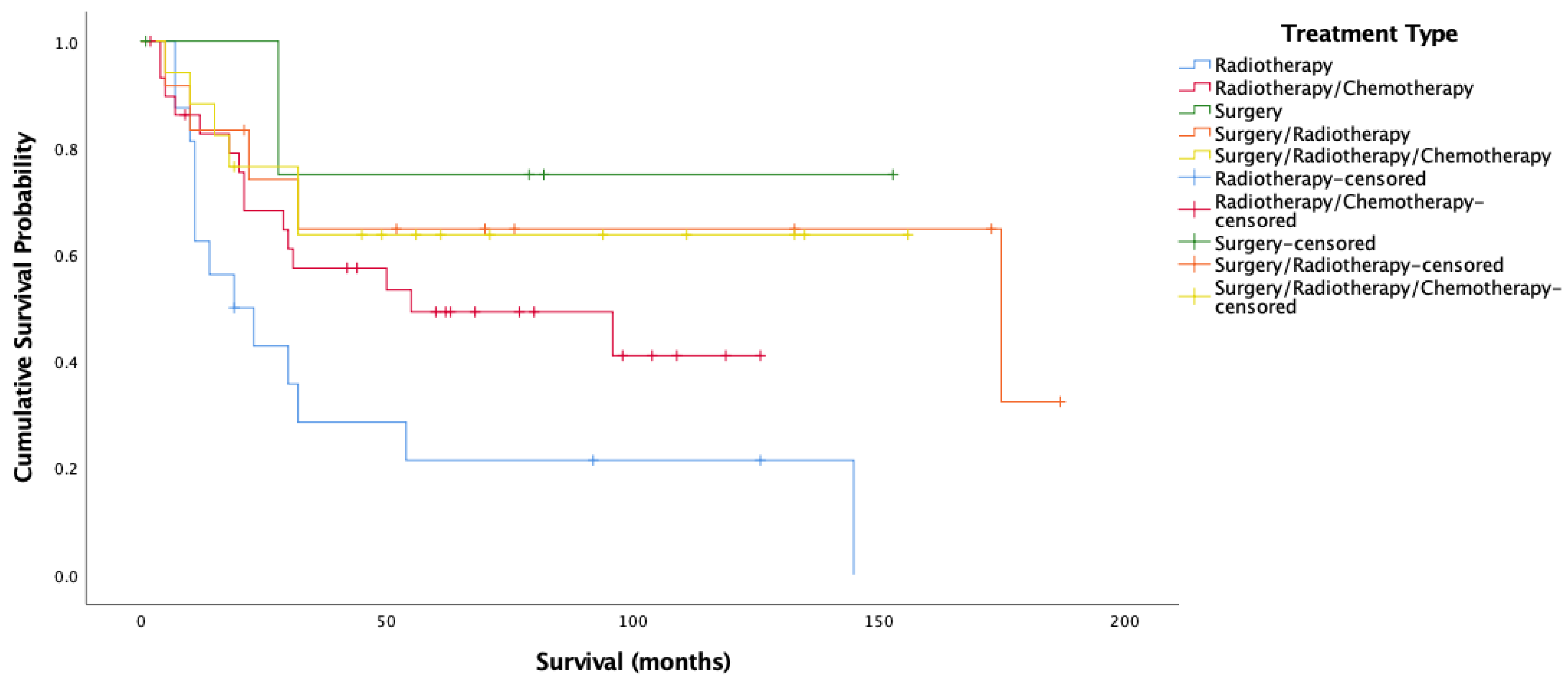
3.4. The Relationship between HPV Status, Treatment Modality, and Survival
3.5. Modeling Predictors of Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Goldberg, H.I.; Lockwood, S.A.; Crossett, L.S.; Wyatt, S.W. Trends and differentials in mortality from cancers of the oral cavity and pharynx in the United States, 1973–1987. Cancer 1994, 74, 565–572. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8033034 (accessed on 7 February 2017). [CrossRef]
- Thomas, G.R.; Nadiminti, H.; Regalado, J. Molecular predictors of clinical outcome in patients with head and neck squamous cell carcinoma. Int. J. Exp. Pathol. 2005, 86, 347–363. [Google Scholar] [CrossRef] [PubMed]
- Hafkamp, H.C.; Manni, J.; Haesevoets, A.; Voogd, A.; Schepers, M.; Bot, F.; Hopman, A.; Ramaekers, F.; Speel, E.-J.M. Marked differences in survival rate between smokers and nonsmokers with HPV 16-associated tonsillar carcinomas. Int. J. Cancer 2008, 122, 2656–2664. [Google Scholar] [CrossRef] [PubMed]
- Krane, J.F. Role of cytology in the diagnosis and management of HPV-associated head and neck carcinoma. Acta Cytol. 2013, 57, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. JNCI J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Mroz, E.A.; Forastiere, A.A.; Rocco, J.W. Implications of the oropharyngeal cancer epidemic. J. Clin. Oncol. 2011, 29, 4222–4223. [Google Scholar] [CrossRef]
- Thompson, L.D.; Heffner, D.K. The clinical importance of cystic squamous cell carcinomas in the neck: A study of 136 cases. Cancer 1998, 82, 944–956. Available online: http://www.ncbi.nlm.nih.gov/pubmed/9486586 (accessed on 7 February 2017). [CrossRef]
- Joo, Y.-H.; Jung, C.-K.; Sun, D.-I.; Park, J.-O.; Cho, K.-J.; Kim, M.-S. High-risk human papillomavirus and cervical lymph node metastasis in patients with oropharyngeal cancer. Head Neck 2011, 34, 10–14. [Google Scholar] [CrossRef]
- Psyrri, A.; Sasaki, C.; Vassilakopoulou, M.; Dimitriadis, G.; Rampias, T. Future directions in research, treatment and prevention of HPV-related squamous cell carcinoma of the head and neck. Head Neck Pathol. 2012, 6 (Suppl. S1), 121–128. [Google Scholar] [CrossRef]
- Chien, C.-Y.; Su, C.-Y.; Fang, F.-M.; Huang, H.-Y.; Chuang, H.-C.; Chen, C.-M. Lower prevalence but favorable survival for human papillomavirus-related squamous cell carcinoma of tonsil in Taiwan. Oral Oncol. 2008, 44, 174–179. [Google Scholar] [CrossRef]
- Fischer, C.A.; Kampmann, M.; Zlobec, I.; Green, E.; Tornillo, L.; Lugli, A.; Wolfensberger, M.; Terracciano, L.M. p16 expression in oropharyngeal cancer: Its impact on staging and prognosis compared with the conventional clinical staging parameters. Ann. Oncol. 2010, 21, 1961–1966. [Google Scholar] [CrossRef] [PubMed]
- Marur, S.; Forastiere, A.A. Head and neck cancer: Changing epidemiology, diagnosis, and treatment. Mayo Clin. Proc. 2008, 83, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Kimple, R.J.; Harari, P.M. The prognostic value of HPV in head and neck cancer patients undergoing postoperative chemoradiotherapy. Ann. Transl. Med. 2015, 3 (Suppl. S1), S14. [Google Scholar] [CrossRef]
- Nichols, A.C.; Dhaliwal, S.S.; Palma, D.A.; Basmaji, J.; Chapeskie, C.; Dowthwaite, S.; Franklin, J.H.; Fung, K.; Kwan, K.; Wehrli, B.; et al. Does HPV type affect outcome in oropharyngeal cancer? J. Otolaryngol. Head Neck Surg. 2013, 42, 9. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef]
- Gillison, M.L. HPV and prognosis for patients with oropharynx cancer. Eur. J. Cancer 2009, 45, 383–385. [Google Scholar] [CrossRef]
- Lassen, P.; Eriksen, J.G.; Krogdahl, A.; Therkildsen, M.H.; Ulhøi, B.P.; Overgaard, M.; Specht, L.; Andersen, E.; Johansen, J.; Neck Cancer Group (DAHANCA); et al. The influence of HPV-associated p16-expression on accelerated fractionated radiotherapy in head and neck cancer: Evaluation of the randomised DAHANCA 6 & 7 trial. Radiother. Oncol. 2011, 100, 49–55. [Google Scholar] [CrossRef]
- Posner, M.R.; Lorch, J.H.; Goloubeva, O.; Tan, M.; Schumaker, L.M.; Sarlis, N.J.; Haddad, R.I.; Cullen, K.J. Survival and human papillomavirus in oropharynx cancer in TAX 324: A subset analysis from an international phase III trial. Ann. Oncol. 2011, 22, 1071–1077. [Google Scholar] [CrossRef]
- Rischin, D.; Young, R.J.; Fisher, R.; Fox, S.B.; Le, Q.-T.; Peters, L.J.; Solomon, B.; Choi, J.; O’Sullivan, B.; Kenny, L.M.; et al. Prognostic significance of p16INK4A and human papillomavirus in patients with oropharyngeal cancer treated on TROG 02.02 phase III Trial. J. Clin. Oncol. 2010, 28, 4142–4148. [Google Scholar] [CrossRef]
- Shaw, R.; Robinson, M. The increasing clinical relevance of human papillomavirus type 16 (HPV-16) infection in oropharyngeal cancer. Br. J. Oral Maxillofac. Surg. 2011, 49, 423–429. [Google Scholar] [CrossRef]
- Albers, A.E.; Qian, X.; Kaufmann, A.M.; Coordes, A. Meta analysis: HPV and p16 pattern determines survival in patients with HNSCC and identifies potential new biologic subtype. Sci. Rep. 2017, 7, 16715. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.; Cordell, K.G.; Lee, J.S.; Worden, F.P.; Prince, M.E.; Tran, H.H.; Wolf, G.T.; Urba, S.G.; Chepeha, D.B.; Teknos, T.N.; et al. EGFR, p16, HPV Titer, Bcl-xL and p53, sex, and smoking as indicators of response to therapy and survival in oropharyngeal cancer. J. Clin. Oncol. 2008, 26, 3128–3137. [Google Scholar] [CrossRef]
- Dahlstrom, K.R.; Anderson, K.S.; Cheng, J.N.; Chowell, D.; Li, G.; Posner, M.; Sturgis, E.M. HPV serum antibodies as predictors of survival and disease progression in patients with HPV-positive squamous cell carcinoma of the oropharynx. Clin. Cancer Res. 2015, 21, 2861–2869. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicka, M.; Szyfter, K.; Milecki, P.; Składowski, K.; Ramlau, R. The rationale for HPV-related oropharyngeal cancer de-escalation treatment strategies. Contemp. Oncol. 2015, 4, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Geiger, J.L.; Lazim, A.F.; Walsh, F.J.; Foote, R.L.; Moore, E.J.; Okuno, S.H.; Olsen, K.D.; Kasperbauer, J.L.; Price, D.L.; Garces, Y.I.; et al. Adjuvant chemoradiation therapy with high-dose versus weekly cisplatin for resected, locally-advanced HPV/p16-positive and negative head and neck squamous cell carcinoma. Oral Oncol. 2014, 50, 311–318. [Google Scholar] [CrossRef]
- Gillison, M.L.; Koch, W.M.; Capone, R.B.; Spafford, M.; Westra, W.H.; Wu, L.; Zahurak, M.L.; Daniel, R.W.; Viglione, M.; Symer, D.E.; et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. JNCI J. Natl. Cancer Inst. 2000, 92, 709–720. Available online: http://www.ncbi.nlm.nih.gov/pubmed/10793107 (accessed on 7 February 2017). [CrossRef]
- Kimple, R.J.; Smith, M.A.; Blitzer, G.C.; Torres, A.D.; Martin, J.A.; Yang, R.Z.; Peet, C.R.; Lorenz, L.D.; Nickel, K.P.; Klingelhutz, A.J.; et al. Enhanced Radiation Sensitivity in HPV-Positive Head and Neck Cancer. Cancer Res. 2013, 73, 4791–4800. [Google Scholar] [CrossRef]
- Rieckmann, T.; Tribius, S.; Grob, T.J.; Meyer, F.; Busch, C.-J.; Petersen, C.; Dikomey, E.; Kriegs, M. HNSCC cell lines positive for HPV and p16 possess higher cellular radiosensitivity due to an impaired DSB repair capacity. Radiother. Oncol. 2013, 107, 242–246. [Google Scholar] [CrossRef]
- Vu, H.L.; Sikora, A.G.; Fu, S.; Kao, J. HPV-induced oropharyngeal cancer, immune response and response to therapy. Cancer Lett. 2010, 288, 149–155. [Google Scholar] [CrossRef]
- Woods, R. Human Papillomavirus-Related Oropharyngeal Squamous Cell Carcinoma—Prevalence and Incidence in a Defined Population and Analysis of the Expression of Specific Cellular Biomarkers. Ph.D. Thesis, Trinity College Dublin, Dublin, Ireland, 2016. [Google Scholar]
- World Health Organization. ICD-10 Code Descriptions for All Disease Types; World Health Organization: Geneva, Switzerland, 2016; Available online: https://icd.who.int/browse10/2016/en (accessed on 27 May 2019).
- Gheit, T.; Anantharaman, D.; Holzinger, D.; Alemany, L.; Tous, S.; Lucas, E.; Prabhu, P.R.; Pawlita, M.; Ridder, R.; Rehm, S.; et al. Role of mucosal high-risk human papillomavirus types in head and neck cancers in central India. Int. J. Cancer 2017, 141, 143–151. [Google Scholar] [CrossRef]
- Leica Biosystems. 2019. Available online: https://www.leicabiosystems.com/ (accessed on 28 May 2019).
- Leica Biosystems. Leica Microsystems BOND Plus Slides. 2019. Available online: https://www.leicabiosystems.com/ihc-ish-fish/bond-ancillary-ihc-ish-reagents/consumables/products/leica-microsystems-plus-slides/ (accessed on 27 May 2019).
- Life Technologies. Life Technologies: ThermoFisher Scientific. 2019. Available online: https://www.thermofisher.com/ie/en/home/brands/life-technologies.html (accessed on 27 May 2019).
- ThermoFisher Scientific. DNAZap PCR DNA Degradation Solutions. 2019. Available online: https://www.thermofisher.com/order/catalog/product/AM9890?SID=srch-srp-AM9890 (accessed on 28 May 2019).
- Gheit, T.; Landi, S.; Gemignani, F.; Snijders, P.J.F.; Vaccarella, S.; Franceschi, S.; Canzian, F.; Tommasino, M. Development of a sensitive and specific assay combining multiplex PCR and DNA microarray primer extension to detect high-risk mucosal human papillomavirus types. J. Clin. Microbiol. 2006, 44, 2025–2031. [Google Scholar] [CrossRef] [PubMed][Green Version]
- xMAP® Technology for Research & Applied Markets. 2017. Available online: https://www.luminexcorp.com/research/our-technology/xmap-technology/ (accessed on 22 August 2017).
- Affymetrix Panomics. Luminex Assays: How it Works. 2014. Available online: http://cdn.panomics.com/products/luninex-assays/technical-overview/how-it-works (accessed on 15 November 2017).
- Mena, M.; Lloveras, B.; Tous, S.; Bogers, J.; Maffini, F.; Gangane, N.; Kumar, R.V.; Somanathan, T.; Lucas, D.; H.-A. Study Group; et al. Development and validation of a protocol for optimizing the use of paraffin blocks in molecular epidemiological studies: The example from the HPV-AHEAD study. PLoS ONE 2017, 12, e0184520. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, M.; Bravo, I.G.; Snijders, P.J.F.; Gissmann, L.; Pawlita, M.; Waterboer, T. Bead-based multiplex genotyping of human papillomaviruses. J. Clin. Microbiol. 2006, 44, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, M.; Dondog, B.; Waterboer, T.; Pawlita, M.; Tommasino, M.; Gheit, T. Abundance of multiple high-risk Human Papillomavirus (HPV) infections found in cervical cells analyzed by use of an ultrasensitive HPV genotyping assay. J. Clin. Microbiol. 2010, 48, 143–149. [Google Scholar] [CrossRef]
- Woods, E.M.O.R.S.; Regan, S.K.; Kennedy, S.; Martin, C.; Leary, C.T.; Timon, C. Role of human papillomavirus in oropharyngeal squamous cell carcinoma: A review. World J. Clin. Cases 2014, 2, 172–193. [Google Scholar] [CrossRef]
- Balermpas, P.; Michel, Y.; Wagenblast, J.; Seitz, O.; Weiss, C.; Rödel, F.; Rödel, C.; Fokas, E. Tumour-infiltrating lymphocytes predict response to definitive chemoradiotherapy in head and neck cancer. Br. J. Cancer 2013, 110, 501–509. [Google Scholar] [CrossRef]
- Jung, A.C.; Guihard, S.; Krugell, S.; Ledrappier, S.; Brochot, A.; Dalstein, V.; Job, S.; de Reynies, A.; Noël, G.; Wasylyk, B.; et al. CD8-alpha T-cell infiltration in human papillomavirus-related oropharyngeal carcinoma correlates with improved patient prognosis. Int. J. Cancer 2012, 132, E26–E36. [Google Scholar] [CrossRef]
- Cancer.Net. Side Effects of Radiation Therapy. ASCO. 2019. Available online: https://www.cancer.net/navigating-cancer-care/how-cancer-treated/radiation-therapy/side-effects-radiation-therapy (accessed on 4 July 2019).
- Tolentino, E.; Centurion, B.S.; Ferreira, L.H.C.; De Souza, A.P.; Damante, J.H.; Rubira-Bullen, I.R. Oral adverse effects of head and neck radiotherapy: Literature review and suggestion of a clinical oral care guideline for irradiated patients. J. Appl. Oral Sci. 2011, 19, 448–454. [Google Scholar] [CrossRef]
- Lyon, A.R. Heart failure resulting from cancer treatment: Still serious but an opportunity for prevention. Heart 2018, 105, 6–8. [Google Scholar] [CrossRef]
- Aleman, B.M.P.; Moser, E.C.; Nuver, J.; Suter, T.M.; Maraldo, M.V.; Specht, L.; Vrieling, C.; Darby, S.C. Cardiovascular disease after cancer therapy. Eur. J. Cancer Suppl. 2014, 12, 18–28. [Google Scholar] [CrossRef]
- Atienza, J.A.S.; Dasanu, C.A. Incidence of second primary malignancies in patients with treated head and neck cancer: A comprehensive review of literature. Curr. Med. Res. Opin. 2012, 28, 1899–1909. [Google Scholar] [CrossRef] [PubMed]
- Chuang, S.-C.; Scelo, G.; Tonita, J.M.; Tamaro, S.; Jonasson, J.G.; Kliewer, E.V.; Hemminki, K.; Weiderpass, E.; Pukkala, E.; Tracey, E.; et al. Risk of second primary cancer among patients with head and neck cancers: A pooled analysis of 13 cancer registries. Int. J. Cancer 2008, 123, 2390–2396. [Google Scholar] [CrossRef] [PubMed]
- Elicin, O.; Sermaxhaj, B.; Bojaxhiu, B.; Shelan, M.; Giger, R.; Rauch, D.; Aebersold, D.M. Incidence of second primary cancers after radiotherapy combined with platinum and/or cetuximab in head and neck cancer patients. Strahlenther. Onkol. 2018, 195, 468–474. [Google Scholar] [CrossRef]
- Wong, S.J.; Heron, D.E.; Stenson, K.; Ling, D.C.; Vargo, J.A. Locoregional recurrent or second primary head and neck cancer: Management strategies and challenges. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e284–e292. [Google Scholar] [CrossRef] [PubMed]
- White, H.N.; Moore, E.J.; Rosenthal, E.L.; Carroll, W.R.; Olsen, K.D.; Desmond, R.A.; Magnuson, J.S. Transoral robotic-assisted surgery for head and neck squamous cell carcinoma. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 1248–1252. [Google Scholar] [CrossRef][Green Version]
- Iseli, T.; Kulbersh, B.D.; Iseli, C.E.; Carroll, W.R.; Rosenthal, E.L.; Magnuson, J.S. Functional outcomes after transoral robotic surgery for head and neck cancer. Otolaryngol. Neck Surg. 2009, 141, 166–171. [Google Scholar] [CrossRef]
- Genden, E.M. The role for surgical management of HPV-related oropharyngeal carcinoma. Head Neck Pathol. 2012, 6, 98–103. [Google Scholar] [CrossRef]
- Golusiński, W. Functional organ preservation surgery in head and neck cancer: Transoral robotic surgery and beyond. Front. Oncol. 2019, 9, 293. [Google Scholar] [CrossRef]
- Mahmoud, O.; Sung, K.; Civantos, F.J.; Thomas, G.R.; Samuels, M.A. Transoral robotic surgery for oropharyngeal squamous cell carcinoma in the era of human papillomavirus. Head Neck 2017, 40, 710–721. [Google Scholar] [CrossRef]
- Weinstein, G.S.; Quon, H.; Newman, H.J.; Chalian, J.A.; Malloy, K.; Lin, A.; Desai, A.; Livolsi, V.A.; Montone, K.T.; Cohen, K.R.; et al. Transoral robotic surgery alone for oropharyngeal cancer. Arch. Otolaryngol. Head Neck Surg. 2012, 138, 628–634. [Google Scholar] [CrossRef]
- Genden, E.M.; Kotz, T.; Ms, C.C.L.T.; Smith, C.; Sikora, A.G.; Teng, M.S.; Packer, S.H.; Lawson, W.L.; Kao, J. Transoral robotic resection and reconstruction for head and neck cancer. Laryngoscope 2011, 121, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Brotherston, D.C.; Poon, I.; Le, T.; Leung, M.; Kiss, A.; Ringash, J.; Balogh, J.; Lee, J.; Wright, J.R. Patient preferences for oropharyngeal cancer treatment de-escalation. Head Neck 2012, 35, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Felix, C.; Wang, P.-C.; Hsu, S.; Basehart, V.; Garst, J.; Beron, P.; Wong, D.; Rosove, M.H.; Rao, S.; et al. Reduced-dose radiotherapy for human papillomavirus-associated squamous-cell carcinoma of the oropharynx: A single-arm, phase 2 study. Lancet Oncol. 2017, 18, 803–811. [Google Scholar] [CrossRef]
- Villaflor, V.; Melotek, J.; Karrison, T.; Brisson, R.; Blair, E.; Portugal, L.; De Souza, J.; Ginat, D.; Stenson, K.; Langerman, A.; et al. Response-adapted volume de-escalation (RAVD) in locally advanced head and neck cancer. Ann. Oncol. 2016, 27, 908–913. [Google Scholar] [CrossRef]
- Mirghani, H.; Blanchard, P. Treatment de-escalation for HPV-driven oropharyngeal cancer: Where do we stand? Clin. Transl. Radiat. Oncol. 2017, 8, 4–11. [Google Scholar] [CrossRef]
- Smith, E.M.; Ritchie, J.M.; Summersgill, K.F.; Klussmann, J.P.; Lee, J.H.; Wang, D.; Haugen, T.H.; Turek, L.P. Age, sexual behavior and human papillomavirus infection in oral cavity and oropharyngeal cancers. Int. J. Cancer 2003, 108, 766–772. [Google Scholar] [CrossRef]
- Husain, N.; Neyaz, A. Human papillomavirus associated head and neck squamous cell carcinoma: Controversies and new concepts. J. Oral Biol. Craniofacial Res. 2017, 7, 198–205. [Google Scholar] [CrossRef]
- American Joint Committee on Cancer and American Cancer Society. Head and neck sites. In AJCC Cancer Staging Manual, 5th ed.; Lippincott-Raven Publishers: Philadelphia, PA, USA, 1997; pp. 24–59. Available online: https://cancerstaging.org/references-tools/deskreferences/Documents/AJCC5thEdCancerStagingManual.pdf (accessed on 14 April 2019).
- American Joint Committee on Cancer and American Cancer Society. AJCC Cancer Staging Manual, 8th ed.; Springer Publishing: New York, NY, USA, 2016; Available online: https://cancerstaging.org/references-tools/deskreferences/pages/default.aspx (accessed on 14 April 2019).
- Boscolo-Rizzo, P.; Del Mistro, A.; Bussu, F.; Lupato, V.; Baboci, L.; Almadori, G.; Da Mosto, M.; Paludetti, G. New insights into human papillomavirus-associated head and neck squamous cell carcinoma. Acta Otorhinolaryngol. Ital. 2013, 33, 77–87. Available online: http://www.ncbi.nlm.nih.gov/pubmed/23853396 (accessed on 3 February 2017).
- D’Souza, G.; McNeel, T.; Fakhry, C. Understanding personal risk of oropharyngeal cancer: Risk-groups for oncogenic oral HPV infection and oropharyngeal cancer. Ann. Oncol. 2017, 28, 3065–3069. [Google Scholar] [CrossRef]
- Brisson, R.J.; Kochanny, S.; Foster, C.C.; Vokes, E.E.; Haraf, D.J.; Seiwert, T.Y. De-escalation in HPV-negative locally advanced head and neck squamous cell cancer (LA-HNSCC) in patients after induction chemotherapy: A retrospective case series. J. Clin. Oncol. 2018, 36 (Suppl. S15), e18090. [Google Scholar] [CrossRef]
- Mehanna, H.; Rischin, D.; Wong, S.J.; Gregoire, V.; Ferris, R.; Waldron, J.; Le, Q.-T.; Forster, M.; Gillison, M.; Laskar, S.; et al. De-escalation after De-ESCALATE and RTOG 1016: A head and neck cancer InterGroup framework for future de-escalation studies. J. Clin. Oncol. 2020, 38, 2552–2557. [Google Scholar] [CrossRef] [PubMed]
- Marur, S.; Li, S.; Cmelak, A.J.; Gillison, M.L.; Zhao, W.J.; Ferris, R.L.; Westra, W.H.; Gilbert, J.; Bauman, J.E.; Wagner, L.I.; et al. E1308: Phase II trial of induction chemotherapy followed by reduced-dose radiation and weekly cetuximab in patients with HPV-associated resectable squamous cell carcinoma of the oropharynx—ECOG-ACRIN cancer research group. J. Clin. Oncol. 2017, 35, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Seiwert, T.; Foster, C.; Blair, E.; Karrison, T.; Agrawal, N.; Melotek, J.; Portugal, L.; Brisson, R.; Dekker, A.; Kochanny, S.; et al. OPTIMA: A phase II dose and volume de-escalation trial for human papillomavirus-positive oropharyngeal cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Vermorken, J.B.; Psyrri, A.; Mesía, R.; Peyrade, F.; Beier, F.; de Blas, B.; Celik, I.; Licitra, L. Impact of tumor HPV status on outcome in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck receiving chemotherapy with or without cetuximab: Retrospective analysis of the phase III EXTREME trial. Ann. Oncol. 2014, 25, 801–807. [Google Scholar] [CrossRef]
- Jung, A.C.; Briolat, J.; Millon, R.; de Reyniès, A.; Rickman, D.; Thomas, E.; Abecassis, J.; Clavel, C.; Wasylyk, B. Biological and clinical relevance of transcriptionally active human papillomavirus (HPV) infection in oropharynx squamous cell carcinoma. Int. J. Cancer 2009, 126, 1882–1894. [Google Scholar] [CrossRef]
- Guo, T.; Eisele, D.W.; Fakhry, C. The potential impact of prophylactic human papillomavirus vaccination on oropharyngeal cancer. Cancer 2016, 122, 2313–2323. [Google Scholar] [CrossRef]
- Herrero, R.; Quint, W.; Hildesheim, A.; Gonzalez, P.; Struijk, L.; Katki, H.A.; Porras, C.; Schiffman, M.; Rodriguez, A.C.; CVT Vaccine Group; et al. Reduced prevalence of oral Human Papillomavirus (HPV) 4 years after bivalent HPV vaccination in a randomized clinical trial in costa Rica. PLoS ONE 2013, 8, e68329. [Google Scholar] [CrossRef]
- Graham, D.M.; Isaranuwatchai, W.; Habbous, S.; de Oliveira, C.; Liu, G.; Siu, L.L.; Ma, J.S.H. A cost-effectiveness analysis of human papillomavirus vaccination of boys for the prevention of oropharyngeal cancer. Cancer 2015, 121, 1785–1792. [Google Scholar] [CrossRef]
- Fakhry, C.; Rosenthal, B.T.; Clark, D.P.; Gillison, M.L. Associations between oral HPV16 infection and cytopathology: Evaluation of an oropharyngeal “pap-test equivalent” in high-risk populations. Cancer Prev. Res. 2011, 4, 1378–1384. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Chaturvedi, A.K. HPV-associated oropharyngeal cancers—Are they preventable? Cancer Prev. Res. 2011, 4, 1346–1349. [Google Scholar] [CrossRef]
- Skandarajah, A.; Sunny, S.P.; Gurpur, P.; Reber, C.D.; D’Ambrosio, M.V.; Raghavan, N.; James, B.L.; Ramanjinappa, R.D.; Suresh, A.; Kandasarma, U.; et al. Mobile microscopy as a screening tool for oral cancer in India: A pilot study. PLoS ONE 2017, 12, e0188440. [Google Scholar] [CrossRef] [PubMed]
- Health Service Executive. Cervical Check. 2019. Available online: https://www.hse.ie/eng/cervicalcheck/ (accessed on 19 May 2019).
- Wentzensen, N.; Schiffman, M.; Palmer, T.; Arbyn, M. Triage of HPV positive women in cervical cancer screening. J. Clin. Virol. 2015, 76, S49–S55. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable Code | Meaning | Variable Definition | Notes on Adjustments |
|---|---|---|---|
| SEX | Sex of patient | Sex of patient | N/A |
| AGE | Integer age at date of diagnosis | Integer age at date of diagnosis | Age was assessed both continuously and based on age younger than or equal to, and older than age 50. Only continuous age was brought forward for multivariable analysis where relevant. |
| SMOKER_ ID | Smoking status | Indication of current, ex-, or never-smoked behavior | N/A |
| GRADE | Grade of primary tumor | Poorly, moderately, well-, or un-differentiated grade of tumor | Only 2 undifferentiated cases were detected in the population. These were excluded after distribution was determined for all grade statistics generated to avoid skew in results. |
| T5 | T stage | T category of stage (5th edition for cases diagnosed up to 2013) derived from best available clinical or pathological T data | Due to low frequencies for sub-stages, these were combined to yield the following T stage categories: T1, T2, T3, T4. |
| N5 | N Stage | N category of stage (5th edition for cases diagnosed up to 2013) derived from best available clinical or pathological N data | Due to low frequencies for sub-stages, these were combined to yield the following N stage categories: N0, N1, N2, N3. N2 and N3 were also combined due to extremely low numbers of N3 patients. |
| M5 | M Stage | M category of stage (5th edition for cases diagnosed up to 2013) derived from best available clinical or pathological M data | N/A |
| TNM5 | TNM Stage | TNM stage (5th edition for cases diagnosed up to 2013) derived from best available clinical or pathological data | Due to low frequencies for sub-stages of Stage IV, TNM stages were combined to yield the following categories: Stage I, II, III, IV. |
| COUNTY_ RES | County of residence | County of residence of patient at time of diagnosis | Due to low frequencies for many counties, county was assessed based on both residence in counties with large urban centers (Dublin/Limerick/Cork) and residence in or outside Dublin. |
| DEPRIV_ POBAL_ 2011 | Socio-economic status/Social Deprivation Score | Pobal index of deprivation from 1 to 5 for 2011 patient’s Electoral Division (ED) of residence at diagnosis re-expressed as quintiles of 2011 population | Social deprivation score was categorical on a scale of 1 to 5, with 5 being the most deprived. It was assessed both categorically and as a continuous variable. |
| MARITAL | Marital status | Indication of single, separated, widowed, or divorced status of patient | Divorced and separated individuals were grouped together due to similarity in status and low numbers of divorced patients. |
| Variable Code | Meaning | Definition |
|---|---|---|
| Chemo_1y | Chemotherapy | Binary indication of whether or not patient was treated with chemotherapy targeting the cancer within 1 year of diagnosis. |
| Radio_1y | Radiotherapy | Binary indication of whether or not patient was treated with radiotherapy targeting the cancer within 1 year of diagnosis. |
| Surg_1y | Surgery | Binary indication of whether or not patient was treated with surgery targeting the cancer within 1 year of diagnosis |
| Variable Code | Meaning | Variable Definition |
|---|---|---|
| VITAL_STAT | Overall survival | All-cause vital status of patient (0 alive or 1 dead) at common censoring date based mainly on death-certificate matching. |
| VITAL_CAN | Disease-specific (cancer-specific) survival | Cause-specific vital status (0 alive or died of other cause or different cancer or 1 died from the cancer of interest) at common censoring date. |
| SURVIVAL_MONTHS | Survival in months | Number of complete months from diagnosis of a specific tumor to common censoring date. |
| Variable/Characteristic | Sub-Set of Variable | Proportion/Mean/Median |
|---|---|---|
| Sex | Male | (661/861) = 76.8% |
| Female | (200/861) = 23.2% | |
| Age (Continuous) | Mean = 63.30 (CI: 62.52, 64.08) Median = 63.00 | |
| 50 | 50 | (121/861) = 14.1% |
| >50 | (740/861) = 86.9% | |
| Smoking Status | Current smoker | (479/861) = 55.6% |
| Ex-smoker | (110/861) = 12.8% | |
| Never smoked | (156/861) = 18.1% | |
| Unknown | (116/861) = 13.5% | |
| Sub-site | Oropharynx | (209/861) = 24.3% |
| Oral Cavity | (331/861) = 38.4% | |
| Larynx | (321/861) = 37.3% | |
| Grade | Well-differentiated | (88/861) = 10.2% |
| Moderately differentiated | (475/861) = 55.2% | |
| Poorly differentiated | (187/861) = 21.7% | |
| Un-differentiated | (2/861) = 0.2% | |
| Unknown | (109/861) = 12.7% | |
| TNM Stage | Stage I | (119/861) = 13.8% |
| Stage II | (126/861) = 14.6% | |
| Stage III | (133/861) = 15.4% | |
| Stage IV | (376/861) = 43.8% | |
| Unknown | (107/861) = 12.4% |
| Sub-Site | Fraction | Prevalence |
|---|---|---|
| Oropharynx | 86/209 | 41.1% |
| Oral Cavity | 36/331 | 10.9% |
| Larynx | 25/321 | 7.8% |
| All | 147/861 | 17.1% |
| Variable/Factor | Statistic | Increased Risk of Death |
|---|---|---|
| Age (Continuous) | HR = 0.020 SE = 0.009 p = 0.029 | Older age |
| HR HPV Status | HR = 0.737 SE = 0.190 p < 0.0001 | HPV negativity |
| T Stage | Base comparison to: T4 (vs. T3, T2, T1, Missing) HR = −0.709, −1.548, −0.604, −0.593 SE = 0.273, 0.273, 0.221, 0.247 p < 0.0001, 0.009, 0.0001, 0.006, 0.016 | T4 > T3, T2, Missing > T1 |
| M Stage | Base comparison to: M1 (vs. M0, Missing) HR = −1.049, −1.198 SE-0.316, 0.313 p = 0.001, 0.001, 0.0001 | M1 > M0, Missing |
| Variable/Factor | Statistic | Increased Risk of Death |
|---|---|---|
| Age (Continuous) | HR = 0.039 SE = 0.012 p = 0.002 | Older age |
| HR HPV Status | HR = 0.937 SE = 0.247 p < 0.0001 | HPV negativity |
| Deprivation Score | HR = 0.165 SE = 0.064 p = 0.010 | More deprived |
| TNM Stage | Base comparison to: T4 (vs. T3, T2, T1, Missing) HR = −0.694, −1.615, −0.564, −0.540 SE = 0.327, 0.598, 0.305, 0.292 p = 0.006, 0.034, 0.007, 0.065, 0.065 | T4 > T3, T2, Missing > T1 |
| Variable/Factor | Statistic | Increased Risk of Death |
|---|---|---|
| Age (Continuous) | HR = 0.039 SE = 0.007 p < 0.0001 | Older age |
| Sex | HR = −0.514 SE = 0.153 p = 0.001 | Male > Female |
| Smoking Status | Base comparison to: Current smoker (vs. ex, never, Missing) HR = −0.634, −0.371, −0.246 SE = 0.196, 0.196, 0.219 p = 0.007, 0.001, 0.058, 0.260 | Current smoker, Missing > Ex-smoker |
| Treatment | Base comparison to: all three modalities HR = 0.577, 0.222, −0.638, −0.126 SE = 0.272, 0.292, 0.256, 0.246 p < 0.0001, 0.034, 0.447, 0.013, 0.608 | Radiotherapy > Surgery/Radiotherapy/Chemotherapy, Surgery |
| Variable/Factor | Statistic | Increased Risk of Death |
|---|---|---|
| Sex | HR = −0.459 SE = 0.179 p = 0.010 | Male > Female |
| Age (Continuous) | HR = 0.028 SE = 0.008 p < 0.0001 | Older age |
| Smoking Status | Base comparison to: Current smoker (vs. ex, never, Missing) HR = −0.880, −0.247, −0.086 SE = 0.255, 0.226, 0.243 p = 0.005, 0.001, 0.125, 0.725 | Current smoker, Never smoker, Missing > Ex-smoker |
| Treatment Type | Base comparison to: all three modalities HR = 0.840, 0.274, −0.458, −0.051 SE = 0.312, 0.341, 0.303, 0.292 p < 0.0001, 0.007, 0.422, 0.131, 0.860 | Radiotherapy > Radiotherapy/Chemotherapy, Surgery/Radiotherapy, Surgery/Radiotherapy/Chemotherapy > Surgery |
| Variable/Factor | Statistic | Increased Risk of Death |
|---|---|---|
| Age (Continuous) | HR = 0.030 SE = 0.007 p < 0.0001 | Older age |
| TNM Stage | Base comparison to: IV (vs. III, II, I, Missing) HR = −0.704, −1.260, −0.790, −0.653 SE = 0.190, 0.197, 0.189, 0.188 p < 0.0001, 0.001, 0.0001, 0.0001, 0.001 | IV > II, II, Missing > I |
| Marital Status | Base comparison to: Single (vs. separated, divorced, married) HR = 0.341, −0.171, 0.340 SE = 0.294, 0.172, 0.200 p = 0.008, 0.246, 0.318, 0.090 | Single > Married |
| Variable/Factor | Statistic | Increased Risk of Death |
|---|---|---|
| TNM Stage | Base comparison to: IV (vs. III, II, I, Missing) HR = −0.717, −1.423, −0.818, −0.757 SE = 0.264, 0.276, 0.248, 0.248 p < 0.0001, 0.007, 0.0001, 0.001, 0.002 | Stage IV> Stage III, II, Missing > Stage I |
| Characteristic |
|---|
| HR HPV Positive |
| Oropharyngeal sub-site |
| Never- or ex-smoker |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharkey Ochoa, I.; O’Regan, E.; Toner, M.; Kay, E.; Faul, P.; O’Keane, C.; O’Connor, R.; Mullen, D.; Nur, M.; O’Murchu, E.; et al. The Role of HPV in Determining Treatment, Survival, and Prognosis of Head and Neck Squamous Cell Carcinoma. Cancers 2022, 14, 4321. https://doi.org/10.3390/cancers14174321
Sharkey Ochoa I, O’Regan E, Toner M, Kay E, Faul P, O’Keane C, O’Connor R, Mullen D, Nur M, O’Murchu E, et al. The Role of HPV in Determining Treatment, Survival, and Prognosis of Head and Neck Squamous Cell Carcinoma. Cancers. 2022; 14(17):4321. https://doi.org/10.3390/cancers14174321
Chicago/Turabian StyleSharkey Ochoa, Imogen, Esther O’Regan, Mary Toner, Elaine Kay, Peter Faul, Connor O’Keane, Roisin O’Connor, Dorinda Mullen, Mataz Nur, Eamon O’Murchu, and et al. 2022. "The Role of HPV in Determining Treatment, Survival, and Prognosis of Head and Neck Squamous Cell Carcinoma" Cancers 14, no. 17: 4321. https://doi.org/10.3390/cancers14174321
APA StyleSharkey Ochoa, I., O’Regan, E., Toner, M., Kay, E., Faul, P., O’Keane, C., O’Connor, R., Mullen, D., Nur, M., O’Murchu, E., Barry-O’Crowley, J., Kernan, N., Tewari, P., Keegan, H., O’Toole, S., Woods, R., Kennedy, S., Feeley, K., Sharp, L., ... Martin, C. M. (2022). The Role of HPV in Determining Treatment, Survival, and Prognosis of Head and Neck Squamous Cell Carcinoma. Cancers, 14(17), 4321. https://doi.org/10.3390/cancers14174321