
Prognostic Factors in Patients Treated with Pembrolizumab as a Second-Line Treatment for Advanced Biliary Tract Cancer

 ,
,  , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
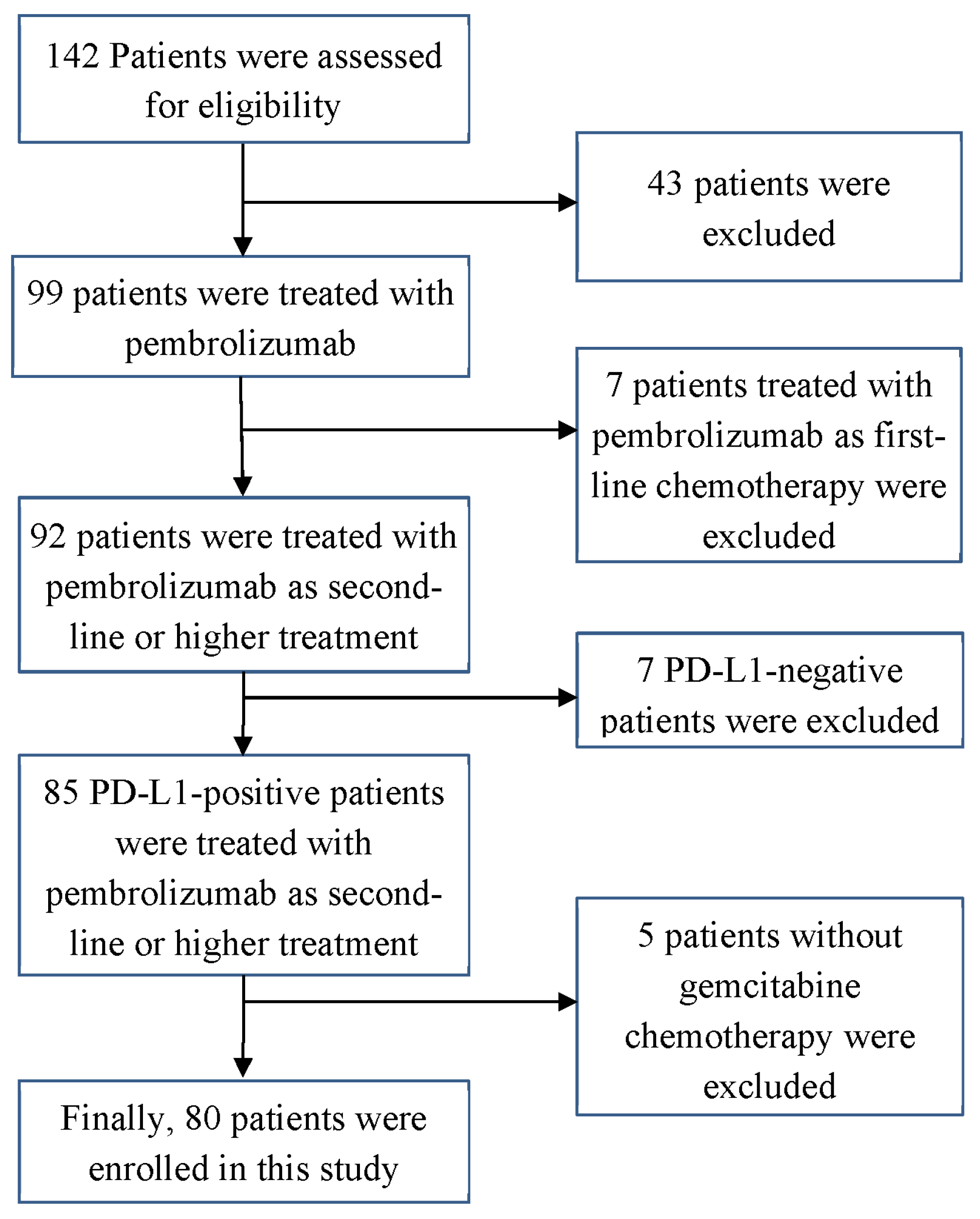
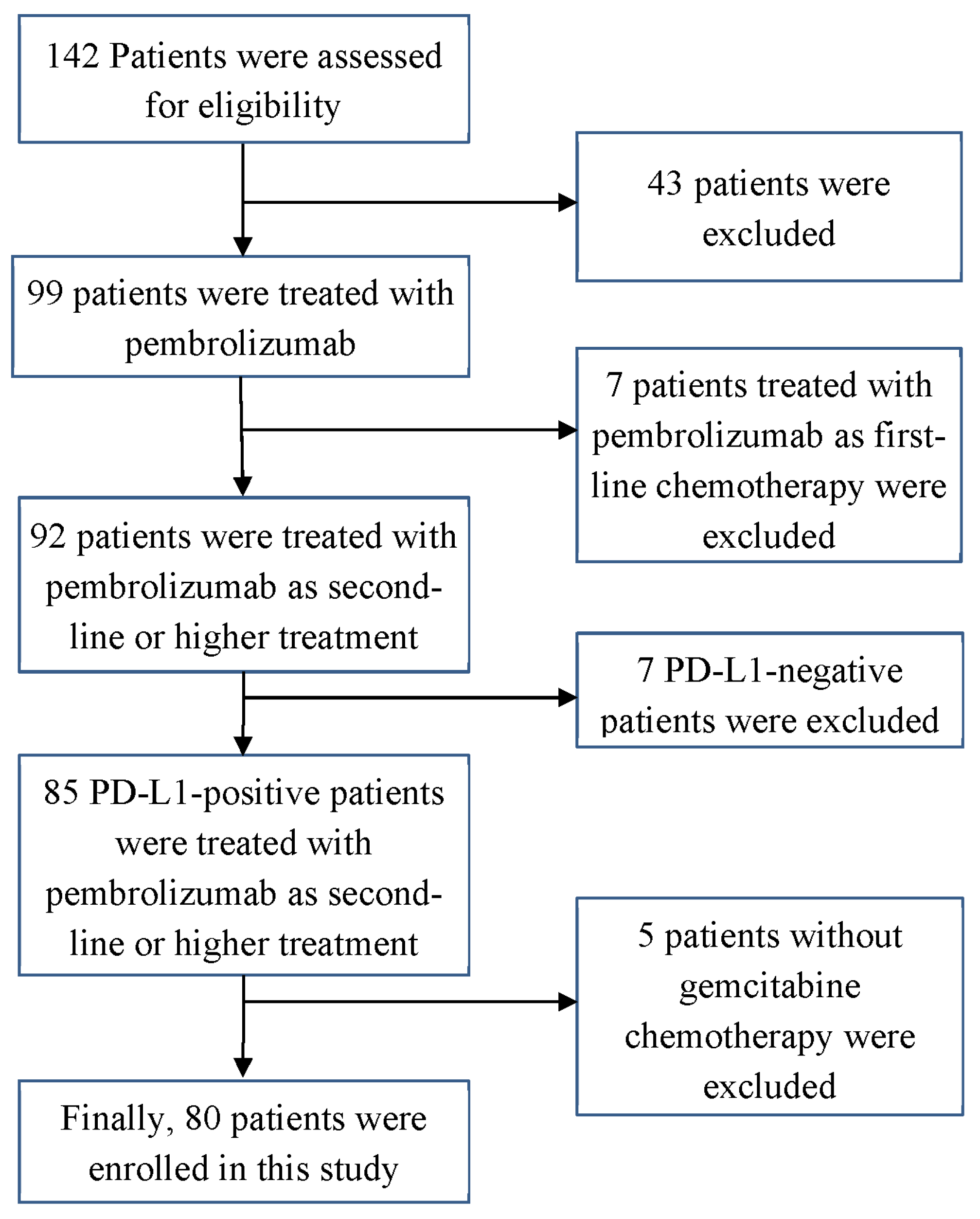
2.1. Patients
2.2. Histopathological Analysis
2.3. Treatment and Assessment
2.4. Outcomes
2.5. Assessment of Treatment-Related AEs
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
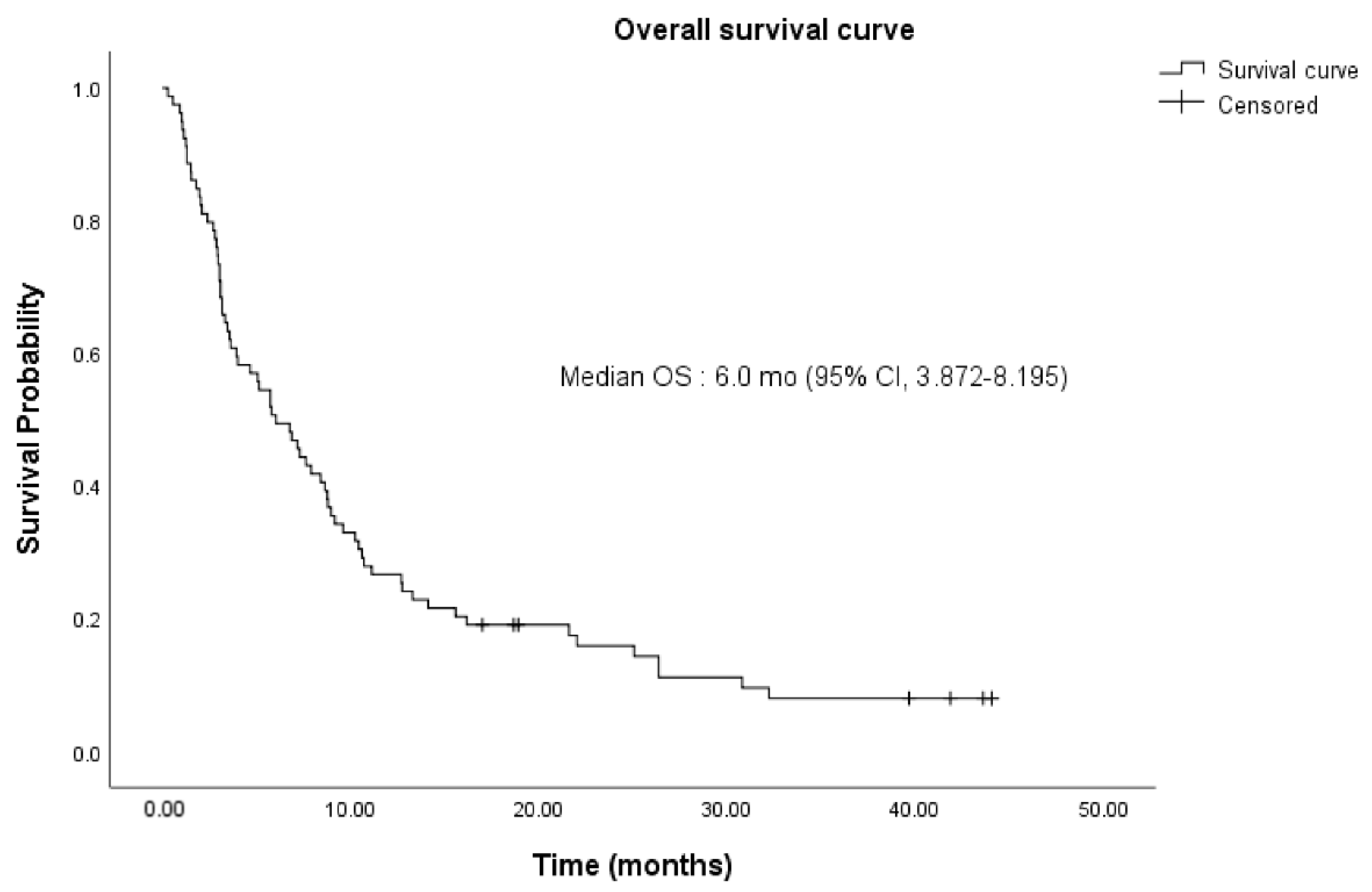
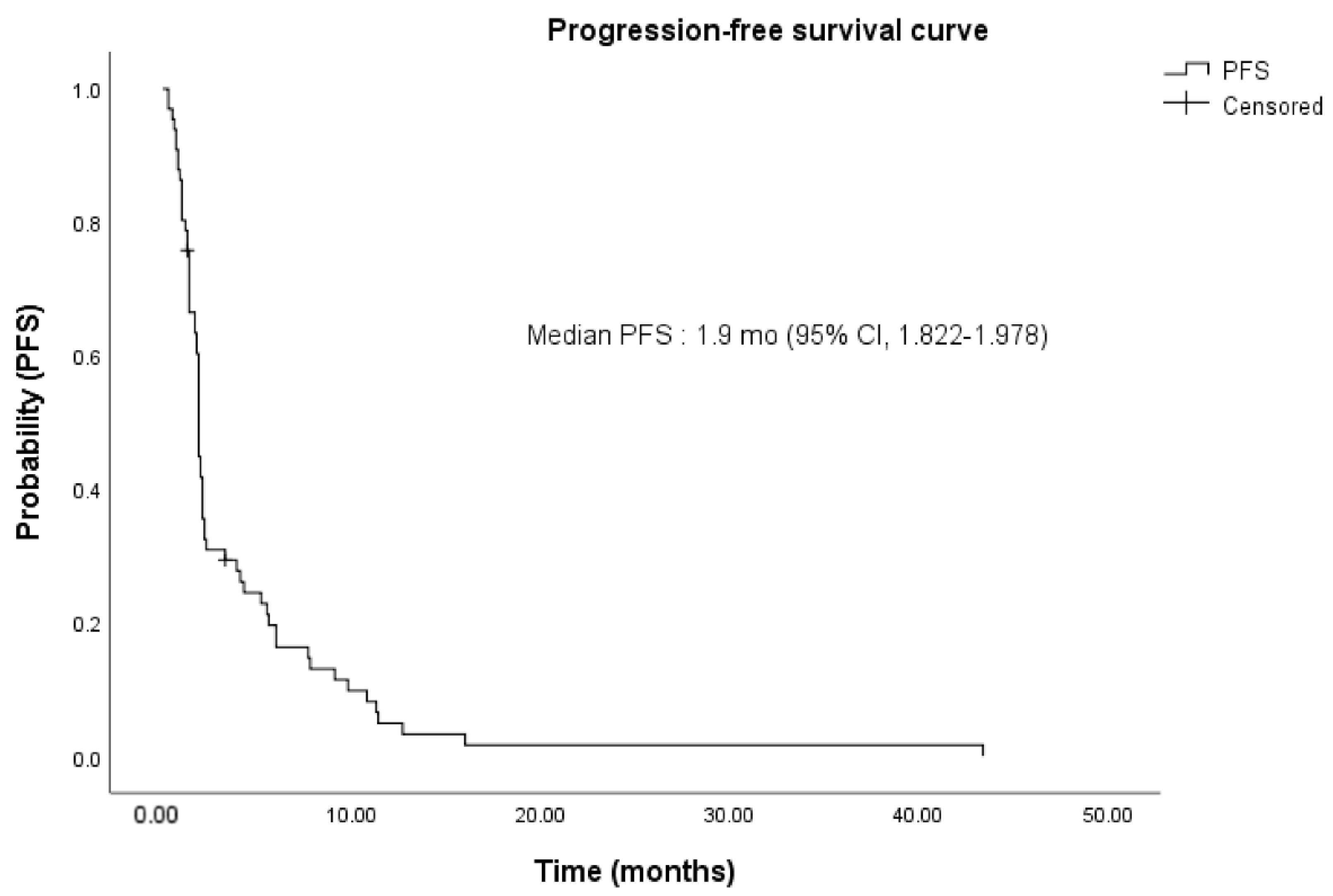
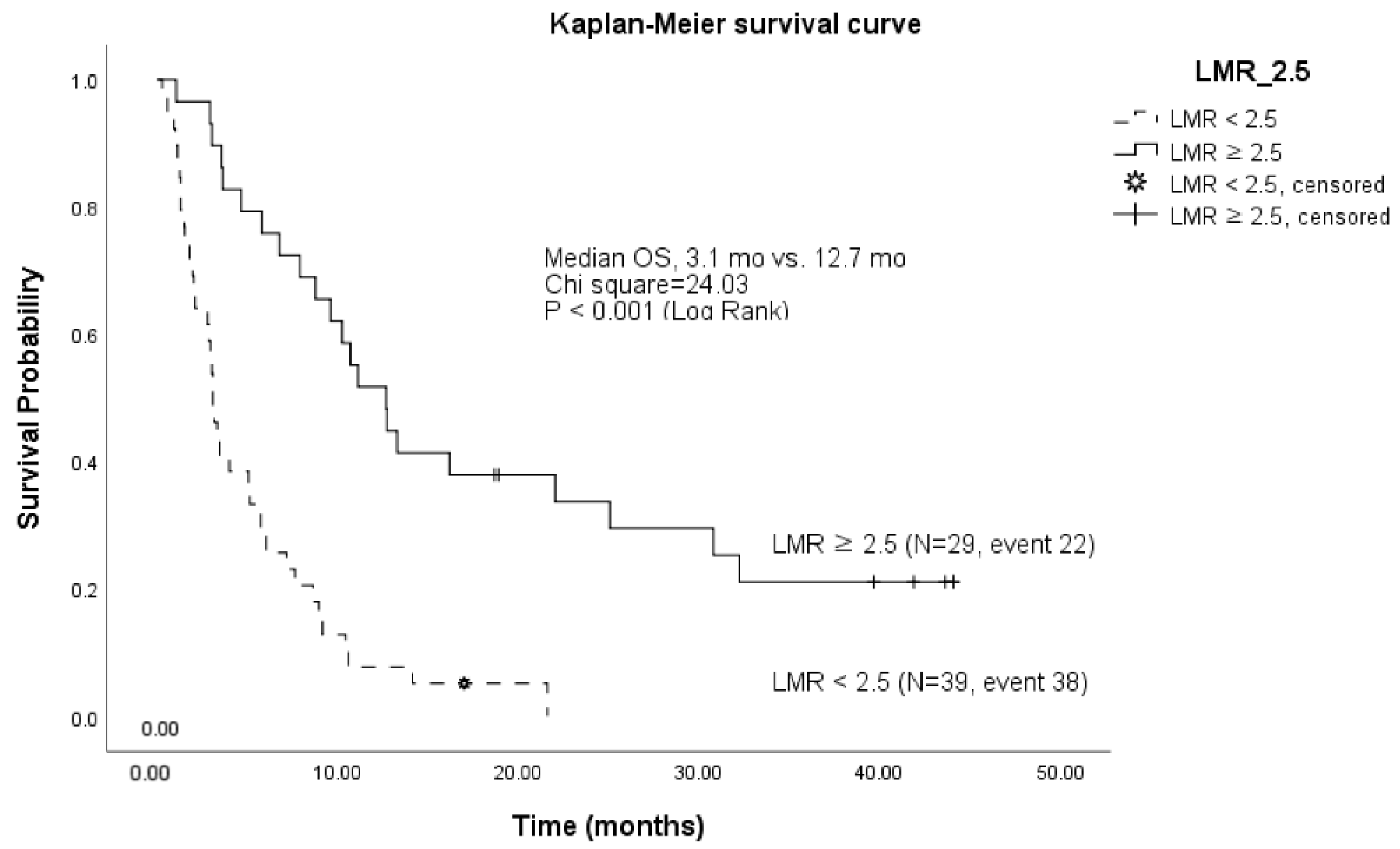
3.2. Treatment and Clinical Outcomes
3.3. Treatment-Related AEs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xie, C.; McGrath, N.A.; Monge Bonilla, C.; Fu, J. Systemic treatment options for advanced biliary tract carcinoma. J. Gastroenterol. 2020, 55, 944–957. [Google Scholar] [CrossRef] [PubMed]
- Piha-Paul, S.A.; Oh, D.Y.; Ueno, M.; Malka, D.; Chung, H.C.; Nagrial, A.; Kelley, R.K.; Ros, W.; Italiano, A.; Nakagawa, K.; et al. Efficacy and safety of pembrolizumab for the treatment of advanced biliary cancer: Results from the keynote-158 and keynote-028 studies. Int. J. Cancer 2020, 147, 2190–2198. [Google Scholar] [CrossRef] [PubMed]
- Hyung, J.; Kim, B.; Yoo, C.; Kim, K.P.; Jeong, J.H.; Chang, H.M.; Ryoo, B.Y. Clinical benefit of maintenance therapy for advanced biliary tract cancer patients showing no progression after first-line gemcitabine plus cisplatin. Cancer Res. Treat. 2019, 51, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Oneda, E.; Abu Hilal, M.; Zaniboni, A. Biliary tract cancer: Current medical treatment strategies. Cancers 2020, 12, 1237. [Google Scholar] [CrossRef] [PubMed]
- Modolell, I.; Guarner, L.; Malagelada, J.R. Vagaries of clinical presentation of pancreatic and biliary tract cancer. Ann. Oncol. 1999, 10 (Suppl 4), 82–84. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhang, H.; Zhou, Z.; Liu, R.; Liu, D.; Bai, M.; Fan, Q.; Li, J.; Zhu, K.; Li, H.; et al. Serum micrornas as biomarkers for the noninvasive early diagnosis of biliary tract cancer. Int. J. Gen. Med. 2021, 14, 1185–1195. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.F.; Hong, A.; Cioffi, G.; Alahmadi, A.; Tang, T.Y.; Ocuin, L.M.; Patil, N.; Bajor, D.L.; Saltzman, J.N.; Mohamed, A.; et al. Associations of racial and ethnic category, age, comorbidities, and socioeconomic factors on concordance to nccn guidelines for patients with high-risk biliary tract cancers after surgery. Front. Oncol. 2022, 12, 771688. [Google Scholar] [CrossRef]
- Lamarca, A.; Hubner, R.A.; David Ryder, W.; Valle, J.W. Second-line chemotherapy in advanced biliary cancer: A systematic review. Ann. Oncol. 2014, 25, 2328–2338. [Google Scholar] [CrossRef]
- Eggermont, A.M.M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.G.; Dalle, S.; Haydon, A.M.; Meshcheryakov, A.; Khattak, A.; Carlino, M.S.; et al. Adjuvant pembrolizumab versus placebo in resected stage iii melanoma (eortc 1325-mg/keynote-054): Distant metastasis-free survival results from a double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 643–654. [Google Scholar] [CrossRef]
- Muro, K.; Chung, H.C.; Shankaran, V.; Geva, R.; Catenacci, D.; Gupta, S.; Eder, J.P.; Golan, T.; Le, D.T.; Burtness, B.; et al. Pembrolizumab for patients with pd-l1-positive advanced gastric cancer (keynote-012): A multicentre, open-label, phase 1b trial. Lancet Oncol. 2016, 17, 717–726. [Google Scholar] [CrossRef]
- Muller, M.; Schouten, R.D.; De Gooijer, C.J.; Baas, P. Pembrolizumab for the treatment of non-small cell lung cancer. Expert Rev. Anticancer Ther. 2017, 17, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Rahman, O. Evaluation of efficacy and safety of different pembrolizumab dose/schedules in treatment of non-small-cell lung cancer and melanoma: A systematic review. Immunotherapy 2016, 8, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Soomin Ahn, J.-C.L.; Shin, D.W.; Kim, J.; Hwang, J. High pd-l1 expression is associated with therapeutic response to pembrolizumab in patients with advanced biliary tract cancer. Sci. Rep. 2020, 10, 8. [Google Scholar]
- Ahn, S.; Lee, Y.; Kim, J.W.; Lee, J.C.; Hwang, J.H.; Yoon, Y.S.; Cho, J.Y.; Han, H.S.; Choi, Y.; Kim, H. Programmed cell death ligand-1 (pd-l1) expression in extrahepatic biliary tract cancers: A comparative study using 22c3, sp263 and e1l3n anti-pd-l1 antibodies. Histopathology 2019, 75, 526–536. [Google Scholar] [CrossRef]
- Mody, K.; Starr, J.; Saul, M.; Poorman, K.; Weinberg, B.A.; Salem, M.E.; VanderWalde, A.; Shields, A.F. Patterns and genomic correlates of pd-l1 expression in patients with biliary tract cancers. J. Gastrointest. Oncol. 2019, 10, 1099–1109. [Google Scholar] [CrossRef]
- Kang, J.; Jeong, J.H.; Hwang, H.S.; Lee, S.S.; Park, D.H.; Oh, D.W.; Song, T.J.; Kim, K.H.; Hwang, S.; Hwang, D.W.; et al. Efficacy and safety of pembrolizumab in patients with refractory advanced biliary tract cancer: Tumor proportion score as a potential biomarker for response. Cancer Res. Treat. 2020, 52, 594–603. [Google Scholar] [CrossRef]
- Boileve, A.; Hilmi, M.; Smolenschi, C.; Ducreux, M.; Hollebecque, A.; Malka, D. Immunotherapy in advanced biliary tract cancers. Cancers 2021, 13, 1569. [Google Scholar] [CrossRef]
- Scheel, A.H.; Dietel, M.; Heukamp, L.C.; Johrens, K.; Kirchner, T.; Reu, S.; Ruschoff, J.; Schildhaus, H.U.; Schirmacher, P.; Tiemann, M.; et al. Harmonized pd-l1 immunohistochemistry for pulmonary squamous-cell and adenocarcinomas. Mod. Pathol. 2016, 29, 1165–1172. [Google Scholar] [CrossRef]
- Dolled-Filhart, M.; Roach, C.; Toland, G.; Stanforth, D.; Jansson, M.; Lubiniecki, G.M.; Ponto, G.; Emancipator, K. Development of a companion diagnostic for pembrolizumab in non-small cell lung cancer using immunohistochemistry for programmed death ligand-1. Arch. Pathol. Lab. Med. 2016, 140, 1243–1249. [Google Scholar] [CrossRef]
- Kulangara, K.; Zhang, N.; Corigliano, E.; Guerrero, L.; Waldroup, S.; Jaiswal, D.; Ms, M.J.; Shah, S.; Hanks, D.; Wang, J.; et al. Clinical utility of the combined positive score for programmed death ligand-1 expression and the approval of pembrolizumab for treatment of gastric cancer. Arch. Pathol. Lab. Med. 2019, 143, 330–337. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, M.; Bo, C.; Liu, X.; Zhang, J.; Li, Z.; Zhao, F.; Kong, L.; Yu, J. Prognostic significance of the lymphocyte-to-monocyte ratio and the tumor-infiltrating lymphocyte to tumor-associated macrophage ratio in patients with stage t3n0m0 esophageal squamous cell carcinoma. Cancer Immunol. Immunother. 2017, 66, 343–354. [Google Scholar] [CrossRef]
- Condeelis, J.; Pollard, J.W. Macrophages: Obligate partners for tumor cell migration, invasion, and metastasis. Cell 2006, 124, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Bai, R.; Lv, Z.; Xu, D.; Cui, J. Predictive biomarkers for cancer immunotherapy with immune checkpoint inhibitors. Biomark. Res. 2020, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, H.N.; Wang, L. Biomarkers for predicting the efficacy of immune checkpoint inhibitors. J. Cancer 2022, 13, 481–495. [Google Scholar] [CrossRef]
- Wu, X.; Qu, D.; Weygant, N.; Peng, J.; Houchen, C.W. Cancer stem cell marker dclk1 correlates with tumorigenic immune infiltrates in the colon and gastric adenocarcinoma microenvironments. Cancers 2020, 12, 274. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, Y.; Seno, H.; Fukuoka, A.; Ueo, T.; Yamaga, Y.; Maruno, T.; Nakanishi, N.; Kanda, K.; Komekado, H.; Kawada, M.; et al. Dclk1 distinguishes between tumor and normal stem cells in the intestine. Nat. Genet. 2013, 45, 98–103. [Google Scholar] [CrossRef]
- Cao, Z.; Weygant, N.; Chandrakesan, P.; Houchen, C.W.; Peng, J.; Qu, D. Tuft and cancer stem cell marker dclk1: A new target to enhance anti-tumor immunity in the tumor microenvironment. Cancers 2020, 12, 3801. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. (%) (Total n = 80) |
|---|---|
| Age, average (range, year) | 66.4 (43–85) |
| 65 | 29 (36.3%) |
| 65 | 51 (63.7%) |
| Sex | |
| Male | 51 (63.7%) |
| Female | 29 (36.3%) |
| Performance status | |
| ECOG 0/1/2 | 60/18/2 |
| Primary tumor location | |
| Intrahepatic/extrahepatic/gallbladder | 55/21/4 |
| Disease setting at presentation | |
| Locally advanced/metastatic | 10/70 |
| Site of metastasis | |
| Liver | 49 (61.3%) |
| Intra-abdominal lymph node | 40 (50.0%) |
| Peritoneum | 23 (28.8%) |
| Bone | 6 (7.5%) |
| Lung | 8 (10.0%) |
| Histological grading | |
| Well/moderate/poorly/unknown | 5/38/26/11 |
| PD-L1 positive %) | |
| 50 (TPS) | 43/13/11 |
| 50 (CPS) | 13/18/11 |
| MSI-High | 15 (18.8%) |
| Laboratory results | |
| Hemoglobin (g/dL) | 1.9 |
| Albumin (g/dL) | 0.6 |
| AST (IU/L) | 16.0 |
| ALT (IU/L) | 68.7 |
| ALP (IU/L) | 219.9 |
| Total bilirubin (mg/dL) | 0.6 |
| CA 19-9 (U/mL) | 3609.2 |
| Clinical information | |
| Number of prior therapies 3) | 61/12/7 |
| Cycles of pembrolizumab | 3.0 (1–30) |
| 44 (55.0%)/36 (45.0%) | |
| Combination treatment | 1 |
| Follow-up duration (months) | 6.4 (0.3–44.1) |
| Variable | RECIST v1.1 (n = 80) |
|---|---|
| Objective response | |
| CR | 1 (1.25%) |
| PR | 5 (6.25%) |
| SD | 26 (32.5%) |
| PD | 43 (53.75%) |
| Not evaluable | 5 (6.25%) |
| ORR (CR + PR) (%) | 6 (7.5%) |
| ORR by primary tumor site | |
| Intrahepatic cholangiocarcinoma | 6/56 (10.7%) |
| Extrahepatic cholangiocarcinoma | 0/21(0%) |
| Gallbladder cancer | 0/4 (0%) |
| DCR (SD + CR + PR) (%) | 32 (40%) |
| DCR by primary tumor site | |
| Intrahepatic cholangiocarcinoma | 26/56 (46.4%) |
| Extrahepatic cholangiocarcinoma | 5/21 (23.8%) |
| Gallbladder cancer | 1/4 (25%) |
| Progression-free survival (95% CI, month) | 1.9 (0.3–43.4) |
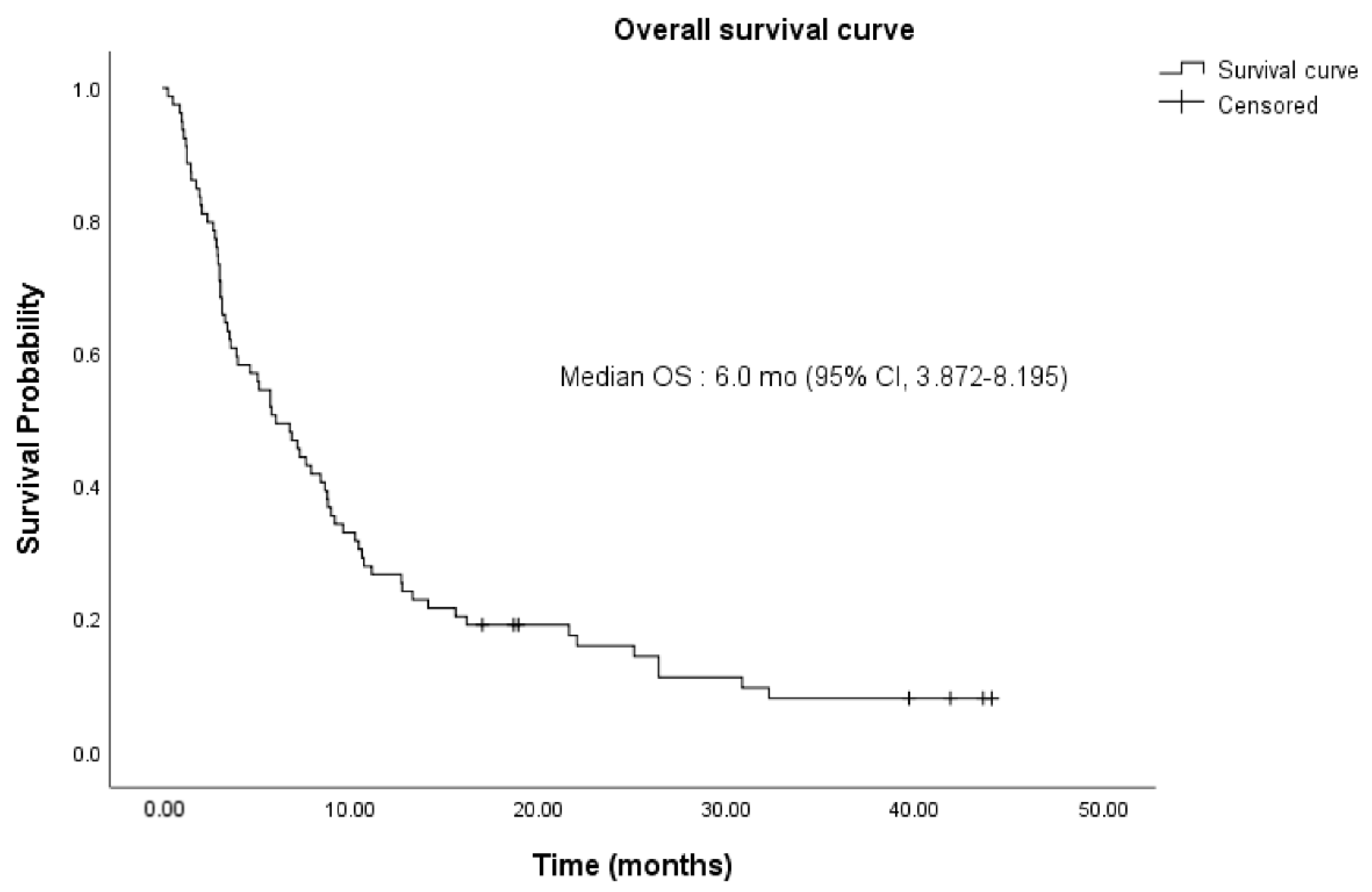
| Overall survival (95% CI, month) | 6.0 (0.3–44.1) |
| Variable (Cut-Off) | Univariate | Multivariate | ||
|---|---|---|---|---|
| p-Value | HR (95% CI) | p-Value | HR (95% CI) | |
| TPS | 0.995 | 1.000 (0.992–1.008) | ||
| CPS | 0.237 | 0.994 (0.985–1.004) | ||
| TB base (10 mm) | 0.010 | 1.101 (1.023–1.184) | 0.015 | 2.286 (1.177–4.440) |
| MSI-H | 0.162 | 1.652 (0.817–3.339) | ||
| Albumin (3.5 g/dL) | <0.001 | 0.346 (0.216–0.553) | 0.003 | 0.392 (0.211–0.725) |
| ALP (151 IU/L) | 0.066 | 1.001 (1.000–1.002) | 0.021 | 1.938 (1.105–3.400) |
| AST | 0.108 | 0.987 (0.970–1.003) | ||
| ALT | 0.859 | 1.000 (0.997–1.004) | ||
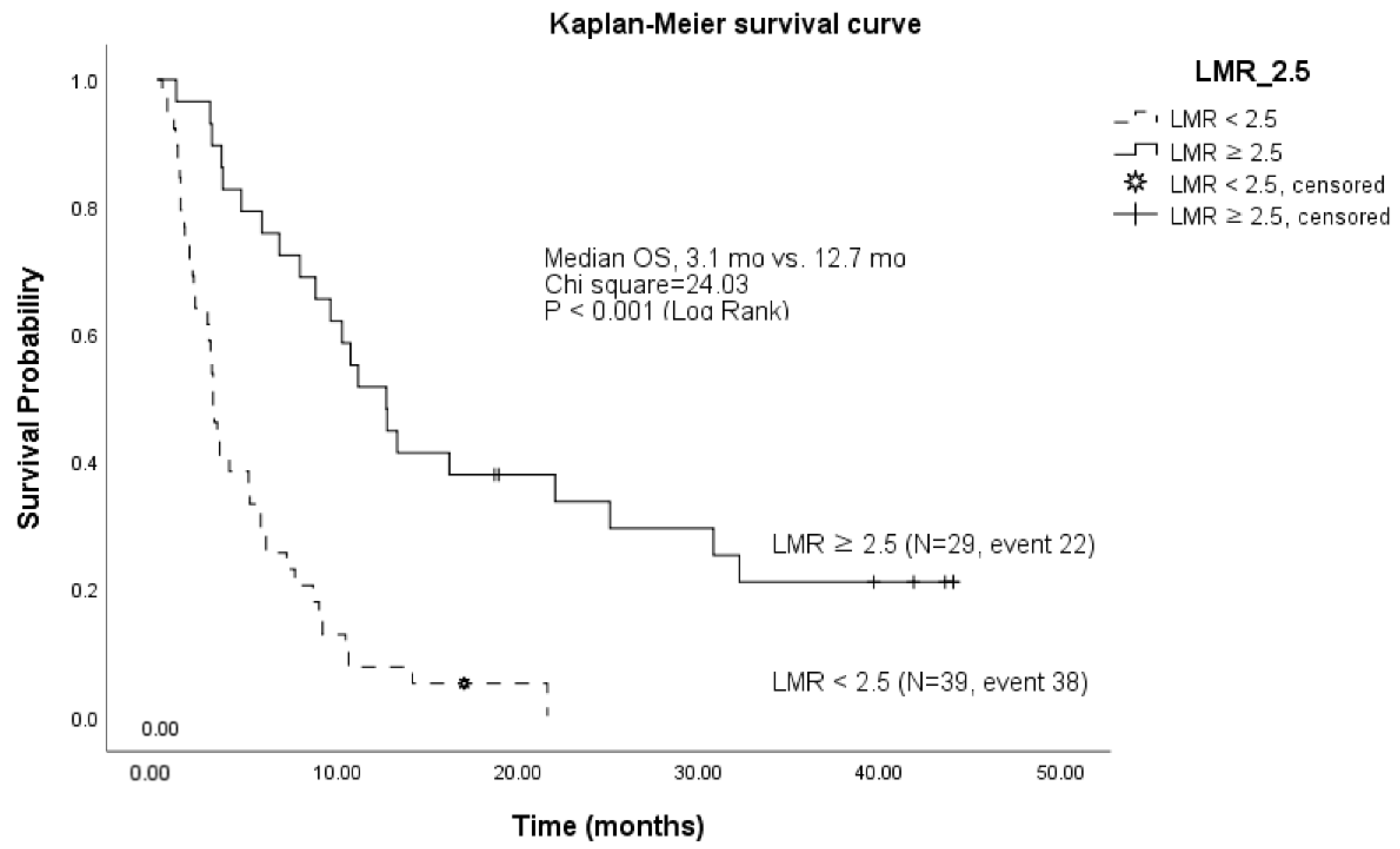
| LMR (2.5) | 0.003 | 0.721 (0.579–0.896) | <0.001 | 0.325 (0.173–0.609) |
| NLR | <0.001 | 1.277 (1.177–1.387) | ||
| PLR | <0.001 | 1.005 (1.002–1.007) | ||
| CA19-9 | 0.022 | 1.000 (1.000–1.000) | ||
| BMI | 0.687 | 0.985 (0.915–1.060) | ||
| Adverse Events | Grade 1/2 (n = 30) | Grade 3/4 (n = 2) |
|---|---|---|
| No. (%) | No. (%) | |
| General weakness | 8 (10.0%) | 0 |
| Anemia | 1 (1.3%) | 0 |
| Acute kidney injury | 2 (2.5%) | 2 (2.5%) |
| Diarrhea | 2 (2.5%) | 0 |
| Facial edema | 1 (1.3%) | 0 |
| Fatigue | 2 (2.5%) | 0 |
| Hypothyroidism | 3 (3.8%) | 0 |
| Skin rash | 2 (2.5%) | 0 |
| Itching sensation | 3 (3.8%) | 0 |
| Thrombocytopenia | 1 (1.3%) | 0 |
| Peripheral neuropathy | 2 (2.5%) | 0 |
| AST/ALT elevation | 1 (1.3%) | 0 |
| Drug-induced pneumonitis | 2 (2.5%) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, C.S.; Sung, M.J.; Kim, S.J.; Jo, J.H.; Lee, H.S.; Chung, M.J.; Bang, S.; Park, S.W.; Song, S.Y.; Park, J.Y. Prognostic Factors in Patients Treated with Pembrolizumab as a Second-Line Treatment for Advanced Biliary Tract Cancer. Cancers 2022, 14, 4323. https://doi.org/10.3390/cancers14174323
Park CS, Sung MJ, Kim SJ, Jo JH, Lee HS, Chung MJ, Bang S, Park SW, Song SY, Park JY. Prognostic Factors in Patients Treated with Pembrolizumab as a Second-Line Treatment for Advanced Biliary Tract Cancer. Cancers. 2022; 14(17):4323. https://doi.org/10.3390/cancers14174323
Chicago/Turabian StylePark, Chan Su, Min Je Sung, So Jeong Kim, Jung Hyun Jo, Hee Seung Lee, Moon Jae Chung, Seungmin Bang, Seung Woo Park, Si Young Song, and Jeong Youp Park. 2022. "Prognostic Factors in Patients Treated with Pembrolizumab as a Second-Line Treatment for Advanced Biliary Tract Cancer" Cancers 14, no. 17: 4323. https://doi.org/10.3390/cancers14174323
APA StylePark, C. S., Sung, M. J., Kim, S. J., Jo, J. H., Lee, H. S., Chung, M. J., Bang, S., Park, S. W., Song, S. Y., & Park, J. Y. (2022). Prognostic Factors in Patients Treated with Pembrolizumab as a Second-Line Treatment for Advanced Biliary Tract Cancer. Cancers, 14(17), 4323. https://doi.org/10.3390/cancers14174323