
The Impact of DNMT3A Status on NPM1 MRD Predictive Value and Survival in Elderly AML Patients Treated Intensively


 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Treatments
2.3. Clinical and Molecular Markers
2.4. Outcome Parameters
2.5. Statistical Analyses
3. Results
3.1. Initial Patient Characteristics
3.2. General Outcome According to DNMT3A and FLT3-ITD Status
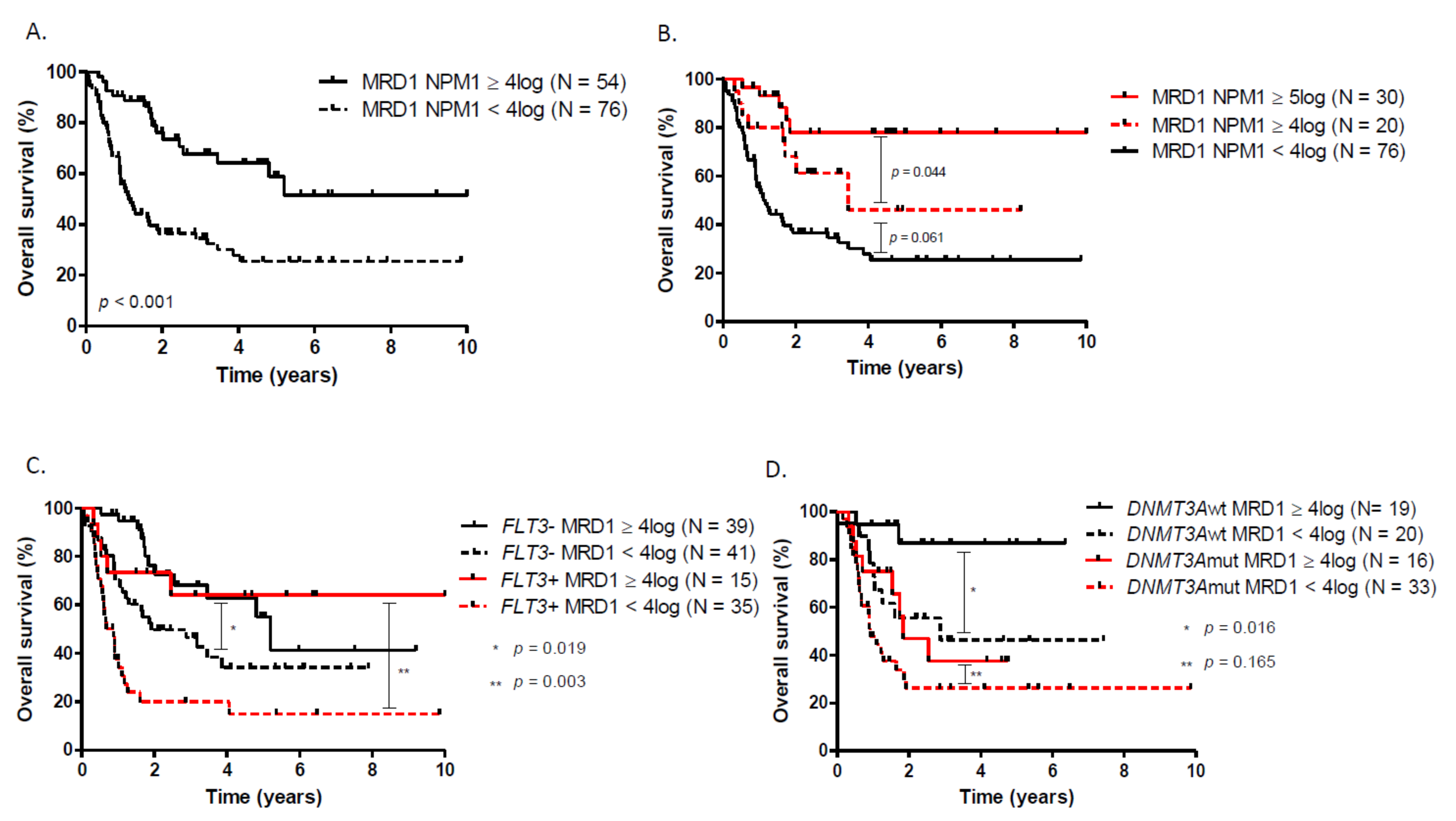
3.3. Prognostic Impact of Postinduction NPM1 BM-MRD Log Reduction
3.4. Multivariate Analysis and Prognosis Model
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Appelbaum, F.R.; Gundacker, H.; Head, D.R.; Slovak, M.L.; Willman, C.L.; Godwin, J.E.; Anderson, J.E.; Petersdorf, S.H. Age and acute myeloid leukemia. Blood 2006, 107, 3481–3485. [Google Scholar] [CrossRef]
- Herold, T.; Rothenberg-Thurley, M.; Grunwald, V.V.; Janke, H.; Goerlich, D.; Sauerland, M.C.; Konstandin, N.P.; Dufour, A.; Schneider, S.; Neusser, M.; et al. Validation and refinement of the revised 2017 European LeukemiaNet genetic risk stratification of acute myeloid leukemia. Leukemia 2020, 34, 3161–3172. [Google Scholar] [CrossRef] [PubMed]
- Nagel, G.; Weber, D.; Fromm, E.; Erhardt, S.; Lübbert, M.; Fiedler, W.; Kindler, T.; Krauter, J.; Brossart, P.; Kündgen, A.; et al. Epidemiological, genetic, and clinical characterization by age of newly diagnosed acute myeloid leukemia based on an academic population-based registry study (AMLSG BiO). Ann. Hematol. 2017, 96, 1993–2003. [Google Scholar] [CrossRef]
- Devillier, R.; Forcade, E.; Garnier, A.; Thepot, S.; Guillerm, G.; Hicheri, Y.; Bulabois, C.-E.; Lioure, B.; Roth Guepin, G.; Dumas, P.-Y.; et al. Allogeneic Hematopoietic Stem Cell Transplantation Improves Outcome of Elderly Patients with Acute Myeloid Leukemia in First Complete Remission: A Time-Dependent and Multistate Analysis from the French Innovative Leukemia Organization. Blood 2018, 132, 209. [Google Scholar] [CrossRef]
- Von dem Borne, P.A.; de Wreede, L.C.; Halkes, C.J.M.; Marijt, W.A.F.; Falkenburg, J.H.F.; Veelken, H. Effectivity of a strategy in elderly AML patients to reach allogeneic stem cell transplantation using intensive chemotherapy: Long-term survival is dependent on complete remission after first induction therapy. Leuk. Res. 2016, 46, 45–50. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Jonas, B.A.; Pullarkat, V.; Thirman, M.J.; Garcia, J.S.; Wei, A.H.; Konopleva, M.; Döhner, H.; Letai, A.; Fenaux, P.; et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N. Engl. J. Med. 2020, 383, 617–629. [Google Scholar] [CrossRef]
- Balsat, M.; Renneville, A.; Thomas, X.; De Botton, S.; Caillot, D.; Marceau, A.; Lemasle, E.; Marolleau, J.P.; Nibourel, O.; Berthon, C.; et al. Postinduction minimal residual disease predicts outcome and benefit from allogeneic stem cell transplantation in acute myeloid leukemia with NPM1 mutation: A study by the acute leukemia French association group. J. Clin. Oncol. 2017, 35, 185–193. [Google Scholar] [CrossRef]
- Krönke, J.; Schlenk, R.F.; Jensen, K.O.; Tschürtz, F.; Corbacioglu, A.; Gaidzik, V.I.; Paschka, P.; Onken, S.; Eiwen, K.; Habdank, M.; et al. Monitoring of minimal residual disease in NPM1-mutated acute myeloid leukemia: A study from the German-Austrian acute myeloid leukemia study group. Proc. J. Clin. Oncol. 2011, 29, 2709–2716. [Google Scholar] [CrossRef] [PubMed]
- Heiblig, M.; Labussière-Wallet, H.; Nicolini, F.E.; Michallet, M.; Hayette, S.; Sujobert, P.; Plesa, A.; Balsat, M.; Paubelle, E.; Barraco, F.; et al. Prognostic value of genetic alterations in elderly patients with acute myeloid leukemia: A single institution experience. Cancers 2019, 11, 570. [Google Scholar] [CrossRef]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic classification and prognosis in acute myeloid leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar]
- Renneville, A.; Boissel, N.; Nibourel, O.; Berthon, C.; Helevaut, N.; Gardin, C.; Cayuela, J.M.; Hayette, S.; Reman, O.; Contentin, N.; et al. Prognostic significance of DNA methyltransferase 3A mutations in cytogenetically normal acute myeloid leukemia: A study by the Acute Leukemia French Association. Leukemia 2012, 26, 1247–1254. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef]
- Gardin, C.; Pautas, C.; Fournier, E.; Itzykson, R.; Lemasle, E.; Bourhis, J.H.; Adès, L.; Marolleau, J.P.; Malfuson, J.V.; Gastaud, L.; et al. Added prognostic value of secondary AML-like gene mutations in ELN intermediate-risk older AML: ALFA-1200 study results. Blood Adv. 2020, 4, 1942–1949. [Google Scholar] [CrossRef]
- Lambert, J.; Pautas, C.; Terré, C.; Raffoux, E.; Turlure, P.; Caillot, D.; Legrand, O.; Thomas, X.; Gardin, C.; Gogat-Marchant, K.; et al. Gemtuzumab ozogamicin for de novo acute myeloid leukemia: Final efficacy and safety updates from the open-label, phase III ALFA-0701 trial. Haematologica 2019, 104, 113–119. [Google Scholar] [CrossRef]
- Fenwarth, L.; Duployez, N.; Thomas, X.; Boissel, N.; Geffroy, S.; Marceau-Renaut, A.; Caillot, D.; Raffoux, E.; Lemasle, E.; Marolleau, J.P.; et al. Clofarabine improves relapse-free survival of acute myeloid leukemia in younger adults with micro-complex karyotype. Cancers 2020, 12, 88. [Google Scholar] [CrossRef]
- Simons, A.; Shaffer, L.G.; Hastings, R.J. Cytogenetic nomenclature: Changes in the ISCN 2013 compared to the 2009 edition. Cytogenet. Genome Res. 2013, 141, 1–6. [Google Scholar] [CrossRef]
- Huet, S.; Jallades, L.; Charlot, C.; Chabane, K.; Nicolini, F.E.; Michallet, M.; Magaud, J.-P.; Hayette, S. New Quantitative Method to Identify NPM1 Mutations in Acute Myeloid Leukaemia. Leuk. Res. Treatment 2013, 2013, 756703. [Google Scholar] [CrossRef]
- Meshinchi, S.; Woods, W.G.; Stirewalt, D.L.; Sweetser, D.A.; Buckley, J.D.; Tjoa, T.K.; Bernstein, I.D.; Radich, J.P. Prevalence and prognostic significance of Flt3 internal tandem duplication in pediatric acute myeloid leukemia. Blood 2001, 97, 89–94. [Google Scholar] [CrossRef]
- Silva, P.; Neumann, M.; Schroeder, M.P.; Vosberg, S.; Schlee, C.; Isaakidis, K.; Ortiz-Tanchez, J.; Fransecky, L.R.; Hartung, T.; Türkmen, S.; et al. Acute myeloid leukemia in the elderly is characterized by a distinct genetic and epigenetic landscape. Leukemia 2017, 31, 1640–1644. [Google Scholar] [CrossRef]
- Rao, A.V.; Valk, P.J.M.; Metzeler, K.H.; Acharya, C.R.; Tuchman, S.A.; Stevenson, M.M.; Rizzieri, D.A.; Delwel, R.; Buske, C.; Bohlander, S.K.; et al. Age-specific differences in oncogenic pathway dysregulation and anthracycline sensitivity in patients with acute myeloid leukemia. J. Clin. Oncol. 2009, 27, 5580–5586. [Google Scholar] [CrossRef]
- Gorello, P.; Cazzaniga, G.; Alberti, F.; Dell’Oro, M.G.; Gottardi, E.; Specchia, G.; Roti, G.; Rosati, R.; Martelli, M.F.; Diverio, D.; et al. Quantitative assessment of minimal residual disease in acute myeloid leukemia carrying nucleophosmin (NPM1) gene mutations. Leukemia 2006, 20, 1103–1108. [Google Scholar] [CrossRef]
- Schnittger, S.; Schoch, C.; Kern, W.; Mecucci, C.; Tschulik, C.; Martelli, M.F.; Haferlach, T.; Hiddemann, W.; Falini, B. Nucleophosmin gene mutations are predictors of favorable prognosis in acute myelogenous leukemia with a normal karyotype. Blood 2005, 106, 3733–3739. [Google Scholar] [CrossRef] [PubMed]
- Whitman, S.P.; Maharry, K.; Radmacher, M.D.; Becker, H.; Mrózek, K.; Margeson, D.; Holland, K.B.; Wu, Y.Z.; Schwind, S.; Metzeler, K.H.; et al. FLT3 internal tandem duplication associates with adverse outcome and gene- and microRNA-expression signatures in patients 60 years of age or older with primary cytogenetically normal acute myeloid leukemia: A cancer and leukemia group B study. Blood 2010, 116, 3622–3626. [Google Scholar] [CrossRef]
- Straube, J.; Ling, V.Y.; Hill, G.R.; Lane, S.W. The impact of age, NPM1 mut, and FLT3 ITD allelic ratio in patients with acute myeloid leukemia. Blood 2018, 131, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Gabert, J.; Beillard, E.; van der Velden, V.H.J.; Bi, W.; Grimwade, D.; Pallisgaard, N.; Barbany, G.; Cazzaniga, G.; Cayuela, J.M.; Cave, H.; et al. Standardization and quality control studies of ‘real-time’ quantitative reverse transcriptase polymerase chain reaction of fusion gene transcripts for residual disease detection in leukemia—A Europe Against Cancer program. Leukemia 2003, 17, 2318–2357. [Google Scholar] [CrossRef]
- Foran, J.M.; Sun, Z.; Paietta, E.; Racevskis, J.; Claxton, D.F.; Lazarus, H.M.; Arber, D.A.; Rowe, J.M.; Godwin, J.; Zhang, Y.; et al. FLT3-ITD Mutations Are Prevalent and Significantly Impact Outcome after Intensive Therapy in Elderly Adults with Acute Myeloid Leukemia (AML): Analysis of the North American Intergroup E2906 Phase III Trial in Patients Age ≥60 Years. Blood 2018, 132, 3995. [Google Scholar] [CrossRef]
- Cappelli, L.V.; Meggendorfer, M.; Dicker, F.; Jeromin, S.; Hutter, S.; Kern, W.; Haferlach, T.; Haferlach, C.; Höllein, A. DNMT3A mutations are over-represented in young adults with NPM1 mutated AML and prompt a distinct co-mutational pattern. Leukemia 2019, 33, 2741–2746. [Google Scholar] [CrossRef] [PubMed]
- Ley, T.J.; Ding, L.; Walter, M.J.; McLellan, M.D.; Lamprecht, T.; Larson, D.E.; Kandoth, C.; Payton, J.E.; Baty, J.; Welch, J.; et al. DNMT3A mutations in acute myeloid leukemia. N. Engl. J. Med. 2010, 363, 2424–2433. [Google Scholar] [CrossRef]
- Hájková, H.; Marková, J.; Haškovec, C.; Šárová, I.; Fuchs, O.; Kostečka, A.; Cetkovský, P.; Michalová, K.; Schwarz, J. Decreased DNA methylation in acute myeloid leukemia patients with DNMT3A mutations and prognostic implications of DNA methylation. Leuk. Res. 2012, 36, 1128–1133. [Google Scholar] [CrossRef]
- Emperle, M.; Adam, S.; Kunert, S.; Dukatz, M.; Baude, A.; Plass, C.; Rathert, P.; Bashtrykov, P.; Jeltsch, A. Mutations of R882 change flanking sequence preferences of the DNA methyltransferase DNMT3A and cellular methylation patterns. Nucleic Acids Res. 2019, 47, 11355–11367. [Google Scholar] [CrossRef]
- Russler-Germain, D.A.; Spencer, D.H.; Young, M.A.; Lamprecht, T.L.; Miller, C.A.; Fulton, R.; Meyer, M.R.; Erdmann-Gilmore, P.; Townsend, R.R.; Wilson, R.K.; et al. The R882H DNMT3A Mutation Associated with AML Dominantly Inhibits Wild-Type DNMT3A by Blocking Its Ability to Form Active Tetramers. Cancer Cell 2014, 25, 442–454. [Google Scholar] [CrossRef]
- Guryanova, O.A.; Shank, K.; Spitzer, B.; Luciani, L.; Koche, R.P.; Garrett-Bakelman, F.E.; Ganzel, C.; Durham, B.H.; Mohanty, A.; Hoermann, G.; et al. DNMT3A mutations promote anthracycline resistance in acute myeloid leukemia via impaired nucleosome remodeling. Nat. Med. 2016, 22, 1488–1495. [Google Scholar] [CrossRef]
- Hubmann, M.; Köhnke, T.; Hoster, E.; Schneider, S.; Dufour, A.; Zellmeier, E.; Fiegl, M.; Braess, J.; Bohlander, S.K.; Subklewe, M.; et al. Molecular response assessment by quantitative real-time polymerase chain reaction after induction therapy in NPM1-mutated patients identifies those at high risk of relapse. Haematologica 2014, 99, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Schnittger, S.; Kern, W.; Tschulik, C.; Weiss, T.; Dicker, F.; Falini, B.; Haferlach, C.; Haferlach, T. Minimal residual disease levels assessed by NPM1 mutation-specific RQ-PCR provide important prognostic information in AML. Blood 2009, 114, 2220–2231. [Google Scholar] [CrossRef]
- Shayegi, N.; Kramer, M.; Bornhäuser, M.; Schaich, M.; Schetelig, J.; Platzbecker, U.; Röllig, C.; Heiderich, C.; Landt, O.; Ehninger, G.; et al. The level of residual disease based on mutant NPM1 is an independent prognostic factor for relapse and survival in AML. Blood 2013, 122, 83–92. [Google Scholar] [CrossRef]
- Ivey, A.; Hills, R.K.; Simpson, M.A.; Jovanovic, J.V.; Gilkes, A.; Grech, A.; Patel, Y.; Bhudia, N.; Farah, H.; Mason, J.; et al. Assessment of minimal residual disease in standard-risk AML. N. Engl. J. Med. 2016, 374, 422–433. [Google Scholar] [CrossRef]
- Kristensen, T.; Møller, M.B.; Friis, L.; Bergmann, O.J.; Preiss, B. NPM1 mutation is a stable marker for minimal residual disease monitoring in acute myeloid leukaemia patients with increased sensitivity compared to WT1 expression. Eur. J. Haematol. 2011, 87, 400–408. [Google Scholar] [CrossRef]
- Ommen, H.B.; Schnittger, S.; Jovanovic, J.V.; Ommen, I.B.; Hasle, H.; Østergaard, M.; Grimwade, D.; Hokland, P. Strikingly different molecular relapse kinetics in NPM1c, PML-RARA, RUNX1-RUNX1T1, and CBFB-MYH11 acute myeloid leukemias. Blood 2010, 115, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, M.F.; Lima, A.S.; Piqué-Borràs, M.R.; Silveira, D.R.; Coelho-Silva, J.L.; Pereira-Martins, D.A.; Weinhäuser, I.; Franca-Neto, P.L.; Quek, L.; Corby, A.; et al. Co-occurrence of DNMT3A, NPM1, FLT3 mutations identifies a subset of acute myeloid leukemia with adverse prognosis. Blood 2020, 135, 870–875. [Google Scholar] [CrossRef] [PubMed]
- Perl, A.E.; Martinelli, G.; Cortes, J.E.; Neubauer, A.; Berman, E.; Paolini, S.; Montesinos, P.; Baer, M.R.; Larson, R.A.; Ustun, C.; et al. Gilteritinib or chemotherapy for relapsed or refractory FLT3-mutated AML. N. Engl. J. Med. 2019, 381, 1728–1740. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Cohort (N = 138) | DNMT3Amut (N = 52) | DNMT3Awt (N = 42) |
|---|---|---|---|
| Age, years, median (range) | 66.1 (60–78.2) | 65.9 (60.1–76.1) | 66.3 (60–76.3) |
| 60–64 yo | - | 27/46 (58.7%) | 19/46 (41.3%) |
| 65–69 yo | - | 14/29 (48.2%) | 15/29 (51.8%) |
| 70+ yo | - | 11/19 (57.9%) | 8/19 (42.1%) |
| Secondary AML, n(%) | 10/138 (7.3%) | - | - |
| Karyotype | |||
| Normal, n(%) | 113/138 (81.8%) | 44/52 (84.6%) | 34/42 (81.0%) |
| Abnormal intermediate, n(%) | 15/138 (10.9%) | 5/52 (9.6%) | 4/42 (9.5%) |
| Unfavorable, n(%) | 4/138 (2.9%) | 3/52 (5.8%) | 1/42 (2.4%) |
| Missing, n(%) | 6/138 (4.4%) | 0/52 | 3/42 (7.1%) |
| NPM1 type of mutation | |||
| Type A, n(%) | 105/138 (76.1%) | - | - |
| Type B, n(%) | 11/138 (8.0%) | ||
| Type D, n(%) | 10/138 (7.3%) | ||
| Others, n(%) | 12/138 (8.6%) | ||
| FLT3-ITD status | |||
| Positive, n(%) | 52/138 (37.6%) | 25/52 (48.1%) | 9/42 (21.4%) |
| Ratio, median (range) | 0.53 (0.05–3) | 0.59 (0.07–4.3) | 0.56 (0.14–0.7) |
| DNMT3A type of mutation | |||
| Positive, n(%) | 52/94 (55.3%) | - | - |
| R882, n(%) | 27/52 (51.9%) | ||
| Missing, n(%) | 40/138 (28.9%) | ||
| VAF, median, % (range) | 42% (1.8–50) | ||
| NPM1 MRD1 response (evaluable in 126/138 patients) | |||
| ≥4log reduction, n(%) | 50/126 (38.9%) | 16/49 (32.6%) | 15/35 (42.8%) |
| <4 log reduction, n(%) | 77/126 (61.1%) | 33/49 (67.4%) | 20/35 (57.2%) |
| HSCT in CR1, n(%) | 19/138 (13.7%) | 6/52 (11.5%) | 11/42 (26.2%) |
| Median follow-up, months (range) | 20.0 (0.07–128.4) | - | - |
| Variables | Overall Survival HR (IC 95%) | p-Value | Leukemia Free Survival HR (IC 95%) | p-Value |
|---|---|---|---|---|
| ELN classification (Favorable vs. other) | 1.75 (0.97–3.15) | 0.062 | 1.34 (0.77–2.33) | 0.30 |
| FLT3-ITD (wt vs. mut) | 1.48 (0.81–2.58) | 0.21 | 1.56 (0.92–2.66) | 0.097 |
| DNMT3A (wt vs. mut) | 2.08 (1.06–4.1) | 0.034 | 2.41 (1.33–4.36) | 0.004 |
| DNMT3A (wt vs. unknown) | 2.07 (1.04–4.15) | 0.038 | 2.02 (1.09–3.73) | 0.024 |
| MRD1 ≥ 4log reduction (yes vs. no) | 2.72 (1.54–4.80) | 0.001 | 2.56 (1.56–4.17) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heiblig, M.; Duployez, N.; Marceau, A.; Lebon, D.; Goursaud, L.; Plantier, I.; Stalnikiewich, L.; Cambier, N.; Balsat, M.; Fossard, G.; et al. The Impact of DNMT3A Status on NPM1 MRD Predictive Value and Survival in Elderly AML Patients Treated Intensively. Cancers 2021, 13, 2156. https://doi.org/10.3390/cancers13092156
Heiblig M, Duployez N, Marceau A, Lebon D, Goursaud L, Plantier I, Stalnikiewich L, Cambier N, Balsat M, Fossard G, et al. The Impact of DNMT3A Status on NPM1 MRD Predictive Value and Survival in Elderly AML Patients Treated Intensively. Cancers. 2021; 13(9):2156. https://doi.org/10.3390/cancers13092156
Chicago/Turabian StyleHeiblig, Maël, Nicolas Duployez, Alice Marceau, Delphine Lebon, Laure Goursaud, Isabelle Plantier, Laure Stalnikiewich, Nathalie Cambier, Marie Balsat, Gaëlle Fossard, and et al. 2021. "The Impact of DNMT3A Status on NPM1 MRD Predictive Value and Survival in Elderly AML Patients Treated Intensively" Cancers 13, no. 9: 2156. https://doi.org/10.3390/cancers13092156
APA StyleHeiblig, M., Duployez, N., Marceau, A., Lebon, D., Goursaud, L., Plantier, I., Stalnikiewich, L., Cambier, N., Balsat, M., Fossard, G., Labussière-Wallet, H., Barraco, F., Ducastelle-Lepretre, S., Sujobert, P., Huet, S., Hayette, S., Ghesquières, H., Thomas, X., & Preudhomme, C. (2021). The Impact of DNMT3A Status on NPM1 MRD Predictive Value and Survival in Elderly AML Patients Treated Intensively. Cancers, 13(9), 2156. https://doi.org/10.3390/cancers13092156