18F-FDOPA PET/CT Combined with MRI for Gross Tumor Volume Delineation in Patients with Skull Base Paraganglioma

 and
and
Abstract
1. Introduction
2. Results
2.1. Patients
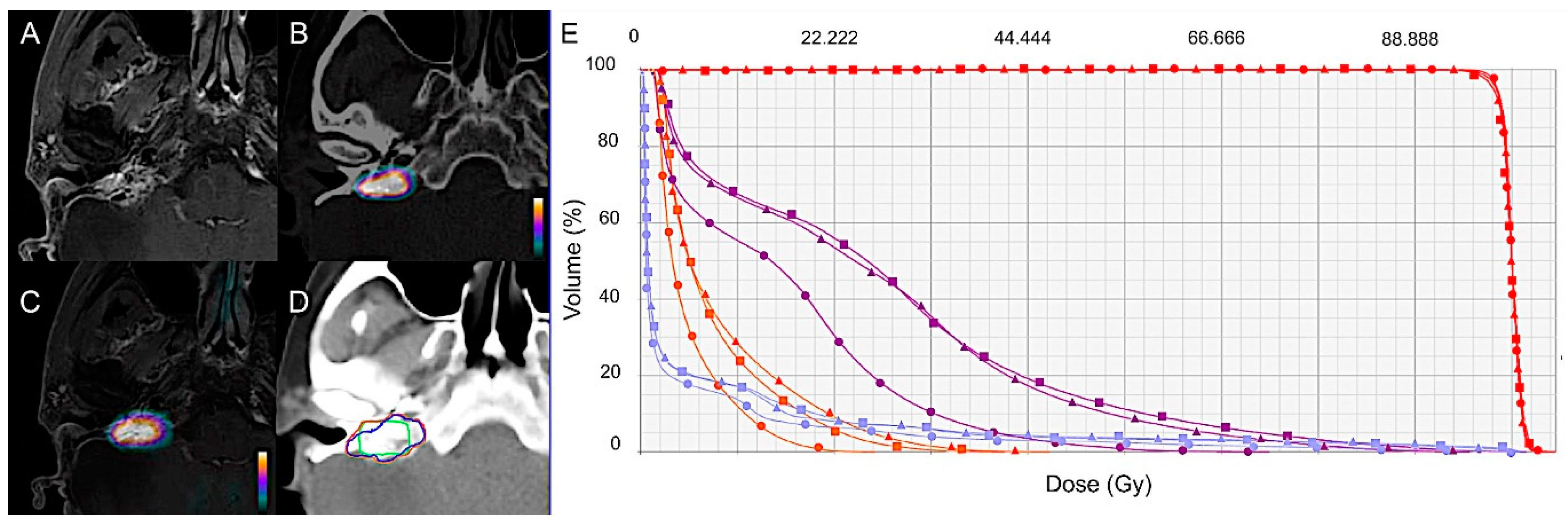
2.2. Tumor Volume Assessment
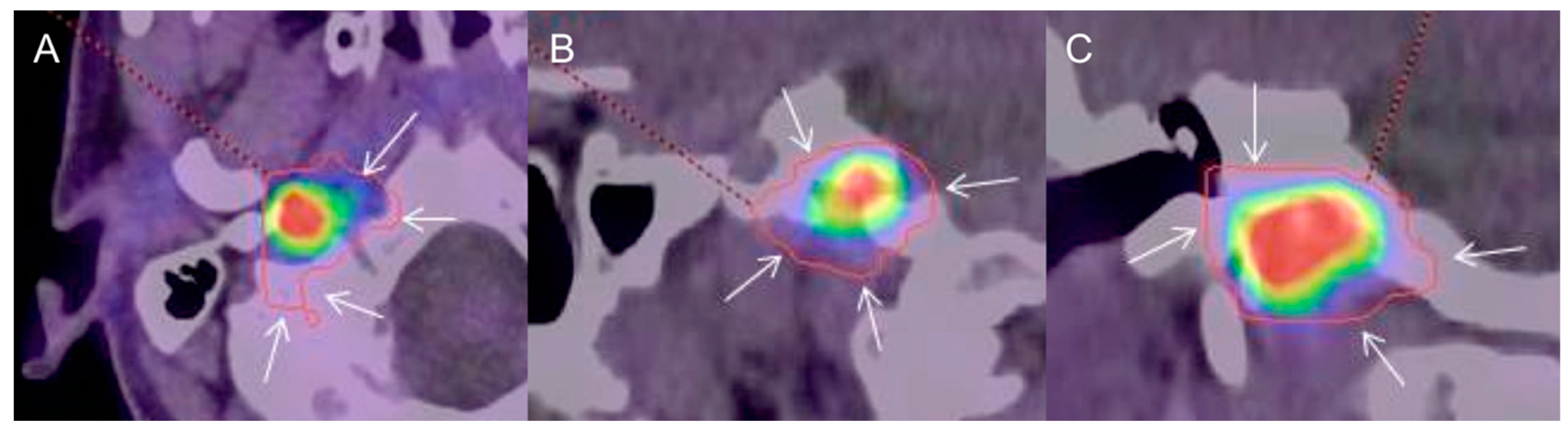
2.3. Positional GTV Assessment
2.4. Radiation Treatment Planning
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Reference Diagnostic Imaging
4.3. Tumor Volume Assessment
4.4. Radiation Treatment Planning
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kumar, V.; Abbas, A.; Fausto, N.; Aster, J. Robbins and Cotran: Pathological Basis of Disease, 8th ed.; Saunders: Philadelphia, PA, USA, 2010. [Google Scholar]
- Baysal, B.E.; Willett-Brozick, J.E.; Lawrence, E.C.; Drovdlic, C.M.; Savul, S.A.; McLeod, D.R.; Yee, H.A.; Brackmann, D.E.; Slattery, W.H.; Myers, E.N.; et al. Prevalence of SDHB, SDHC, and SDHD germline mutations in clinic patients with head and neck paragangliomas. J. Med. Genet. 2002, 39, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Lenders, J.W.M.; Duh, Q.-Y.; Eisenhofer, G.; Gimenez-Roqueplo, A.-P.; Grebe, S.K.G.; Murad, M.H.; Naruse, M.; Pacak, K.; Young, W.F.; et al. Pheochromocytoma and Paraganglioma: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2014, 99, 1915–1942. [Google Scholar] [CrossRef] [PubMed]
- Manolidis, S.; Shohet, J.A.; Jackson, C.G.; Glasscock, M.E., 3rd. Malignant glomus tumors. Laryngoscope 1999, 109, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Taïeb, D.; Timmers, H.J.; Hindié, E.; Guillet, B.A.; Neumann, H.P.; Walz, M.K.; Opocher, G.; Herder, W.W.; Boedeker, C.C.; Krijger, R.R.; et al. EANM 2012 guidelines for radionuclide imaging of phaeochromocytoma and paraganglioma. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1977–1995. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Cocciolillo, F.; De Waure, C.; Di Nardo, F.; Gualano, M.R.; Castaldi, P.; Rufini, V.; Giordano, A. Diagnostic performance of 18F-dihydroxyphenylalanine positron emission tomography in patients with paraganglioma: A meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Heimburger, C.; Veillon, F.; Taïeb, D.; Goichot, B.; Riehm, S.; Petit-Thomas, J.; Averous, G.; Cavalcanti, M.; Hubelé, F.; Chabrier, G.; et al. Head-to-head comparison between 18F-FDOPA PET/CT and MR/CT angiography in clinically recurrent head and neck paragangliomas. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Amodru, V.; Guerin, C.; Delcourt, S.; Romanet, P.; Loundou, A.; Viana, B.; Brue, T.; Castinetti, F.; Sebag, F.; Pacak, K.; et al. Quantitative 18F-DOPA PET/CT in pheochromocytoma: The relationship between tumor secretion and its biochemical phenotype. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 278–282. [Google Scholar] [CrossRef]
- Taïeb, D.; Kaliski, A.; Boedeker, C.C.; Martucci, V.; Fojo, T.; Adler, J.R.; Pacak, K. Current approaches and recent developments in the management of head and neck paragangliomas. Endocr. Rev. 2014, 35, 795–819. [Google Scholar] [CrossRef]
- Wanna, G.B.; Sweeney, A.D.; Haynes, D.S.; Carlson, M.L. Contemporary management of jugular paragangliomas. Otolaryngol. Clin. N. Am. 2015, 48, 331–341. [Google Scholar] [CrossRef]
- Moore, M.G.; Netterville, J.L.; Mendenhall, W.M.; Isaacson, B.; Nussenbaum, B. Head and Neck Paragangliomas: An Update on Evaluation and Management. Otolaryngol. Head Neck Surg. 2016, 154, 597–605. [Google Scholar] [CrossRef]
- Marchetti, M.; Pinzi, V.; Tramacere, I.; Bianchi, L.C.; Ghielmetti, F.; Fariselli, L. Radiosurgery for paragangliomas of the head and neck: Another step for the validation of a treatment paradigm. World Neurosurg. 2017, 98, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Persky, M.S. Treatment of head and neck paragangliomas. Cancer Control 2016, 23, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Huy, P.T.B. Radiotherapy for glomus jugulare paraganglioma. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2014, 131, 223–226. [Google Scholar] [CrossRef]
- Queiroz, M.A.; Hüllner, M.; Kuhn, F.; Huber, G.; Meerwein, C.; Kollias, S.; Von Schulthess, G.; Veit-Haibach, P. PET/MRI and PET/CT in follow-up of head and neck cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1066–1075. [Google Scholar] [CrossRef] [PubMed]
- Schaarschmidt, B.M.; Heusch, P.; Buchbender, C.; Ruhlmann, M.; Bergmann, C.; Ruhlmann, V.; Schlamann, M.; Antoch, G.; Forsting, M.; Wetter, A.; et al. Locoregional tumour evaluation of squamous cell carcinoma in the head and neck area: A comparison between MRI, PET/CT and integrated PET/MRI. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Pauleit, D.; Floeth, F.; Hamacher, K.; Riemenschneider, M.J.; Reifenberger, G.; Müller, H.-W.; Zilles, K.; Coenen, H.H.; Langen, K.-J. O-(2-[18F]fluoroethyl)-l-tyrosine PET combined with MRI improves the diagnostic assessment of cerebral gliomas. Brain 2005, 128, 678–687. [Google Scholar] [CrossRef] [PubMed]
- Cicone, F.; Filss, C.P.; Minniti, G.; Rossi-Espagnet, C.; Papa, A.; Scaringi, C.; Galldiks, N.; Bozzao, A.; Shah, N.J.; Scopinaro, F.; et al. Volumetric assessment of recurrent or progressive gliomas: Comparison between F-DOPA PET and perfusion-weighted MRI. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 905–915. [Google Scholar] [CrossRef]
- Carideo, L.; Minniti, G.; Mamede, M.; Scaringi, C.; Russo, I.; Scopinaro, F.; Cicone, F. 18F-DOPA uptake parameters in glioma: Effects of patients’ characteristics and prior treatment history. Br. J. Radiol. 2018, 91, 20170847. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Combs, S.E.; Leotta, K.; Afshar-Oromieh, A.; Rieken, S.; Debus, J.; Haberkorn, U.; Giesel, F.L. Intra-individual comparison of 18F-FET and 18FDOPA in PET imaging of recurrent brain tumors. Neuro Oncol. 2014, 16, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Lapa, C.; Linsenmann, T.; Monoranu, C.M.; Samnick, S.; Buck, A.; Bluemel, C.; Czernin, J.; Kessler, A.F.; Homola, G.A.; Ernestus, R.-I.; et al. Comparison of the amino acid tracers 18F-FET and 18F-DOPA in high-grade glioma patients. J. Nucl. Med. 2014, 55, 1611–1616. [Google Scholar] [CrossRef] [PubMed]
- Verma, V.; Choi, J.I.; Sawant, A.; Gullapalli, R.P.; Chen, W.; Alavi, A.; Simone, C.B. Use of PET and Other Functional Imaging to Guide Target Delineation in Radiation Oncology. Semin. Radiat. Oncol. 2018, 28, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Pafundi, D.H.; Laack, N.N.; Youland, R.S.; Parney, I.F.; Lowe, V.J.; Giannini, C.; Kemp, B.J.; Grams, M.P.; Morris, J.M.; Hoover, J.M.; et al. Biopsy validation of 18F-DOPA PET and biodistribution in gliomas for neurosurgical planning and radiotherapy target delineation: Results of a prospective pilot study. Neuro Oncol. 2013, 15, 1058–1067. [Google Scholar] [CrossRef] [PubMed]
- Pafundi, D.; Brinkmann, D.; Laack, N.; Sarkaria, J.; Yan, E.; Kemp, B.; Löwe, V. WE-G-214-02: Utility of 18F-FDOPA PET for Radiotherapy Target Delineation in Glioma Patients. Med. Phys. 2011, 38, 3830. [Google Scholar] [CrossRef]
- Kosztyla, R.; Chan, E.K.; Hsu, F.; Wilson, D.; Ma, R.; Cheung, A.; Zhang, S.; Moiseenko, V.; Bénard, F.; Nichol, A.; et al. High-grade glioma radiation therapy target volumes and patterns of failure obtained from magnetic resonance imaging and 18F-FDOPA positron emission tomography delineations from multiple observers. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Navarria, P.; Reggiori, G.; Pessina, F.; Ascolese, A.M.; Tomatis, S.; Mancosu, P.; Lobefalo, F.; Clerici, E.; Lopci, E.; Bizzi, A.; et al. Investigation on the role of integrated PET/MRI for target volume definition and radiotherapy planning in patients with high grade glioma. Radiother. Oncol. 2014, 112, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Palaniappan, N.; Cole, N.; Jayaprakasam, V.; Rackley, T.; Spezi, E.; Berthon, B.; Evans, M. Head and neck target delineation using a novel PET automatic segmentation algorithm. Radiother. Oncol. 2017, 122, 242–247. [Google Scholar] [CrossRef]
- Handel, S.F.; Miller, M.H.; Miller, L.S.; Goepfert, H.; Wallace, S. Angiographic changes of head and neck chemodectomas following radiotherapy. Arch. Otolaryngol. 1977, 103, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Mullins, B.T.; Falchook, A.D.; Lian, J.; He, K.; Shen, D.; Dance, M.; Lin, W.; Sills, T.M.; Das, S.K.; et al. Evaluation of PET/MRI for Tumor Volume Delineation for Head and Neck Cancer. Front. Oncol. 2017, 23, 7–8. [Google Scholar] [CrossRef] [PubMed]
- Ligtenberg, H.; Jager, E.A.; Caldas-Magalhaes, J.; Schakel, T.; Pameijer, F.A.; Kasperts, N.; Willems, S.M.; Terhaard, C.H.; Raaijmakers, C.P.; Philippens, M.E.; et al. Modality-specific target definition for laryngeal and hypopharyngeal cancer on FDG-PET, CT and MRI. Radiother. Oncol. 2017, 123, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Songthong, A.P.; Kannarunimit, D.; Chakkabat, C.; Lertbutsayanukul, C. A randomized phase II/III study of adverse events between sequential (SEQ) versus simultaneous integrated boost (SIB) intensity modulated radiation therapy (IMRT) in nasopharyngeal carcinoma; preliminary result on acute adverse events. Radiat. Oncol. 2015, 10, 166. [Google Scholar] [CrossRef] [PubMed]
- Truc, G.; Bernier, V.; Mirjolet, C.; Dalban, C.; Mazoyer, F.; Bonnetain, F.; Blanchard, N.; Lagneau, É.; Maingon, P.; Noël, G.; et al. A phase I dose escalation study using simultaneous integrated-boost IMRT with temozolomide in patients with unifocal glioblastoma. Cancer Radiother. 2016, 20, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Erdi, Y.E.; Mawlawi, O.; Larson, S.M.; Imbriaco, M.; Yeung, H.; Finn, R.; Humm, J.L. Segmentation of lung lesion volume by adaptive positron emission tomography image thresholding. Cancer 1997, 80, 2505–2509. [Google Scholar] [CrossRef]
- Zou, K.H.; Warfield, S.K.; Bharatha, A.; Tempany, C.M.; Kaus, M.R.; Haker, S.J.; Wells, W.M.; Jolesz, F.A.; Kikinis, R. Statistical validation of image segmentation quality based on a spatial overlap index. Acad. Radiol. 2004, 11, 178–189. [Google Scholar] [CrossRef]
- Otto, K. Volumetric modulated arc therapy: IMRT in a single gantry arc. Med. Phys. 2008, 35, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.V. Guidelines, Criteria, and Rules of Thumb for Evaluating Normed and Standardized Assessment Instruments in Psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient | Age, Sex (Man/Woman) | Symptoms | PGL Size (mm), Side (Left/Right) | Genetics | Primary Staging, Recurrence | Prior Treatment |
|---|---|---|---|---|---|---|
| 1 | 62, M | Tinnitus | 10, L | Sporadic | Primary Staging | - |
| 2 | 57, W | Tinnitus Ear discharge | 23, R | SDHC3 | Recurrence | Surgery PRRT 2 |
| 3 | 57, M | Tinnitus | 8, R | Sporadic | Recurrence | Surgery |
| 4 | 58, M | Tinnitus | 8, R | Sporadic | Recurrence | Surgery IMRT 3 |
| 5 | 43, W | Tinnitus Local pain | 40, R | Sporadic | Recurrence | Surgery |
| 6 | 84, W | Tinnitus | 31, L | Sporadic | Recurrence | Surgery Gamma Knife |
| 7 | 62, W | Asymptomatic | 22, L | SDHB1 | Recurrence | Surgery |
| 8 | 67, W | Pulsatile tinnitus | 8, L | Sporadic | Primary Staging | - |
| 9 | 66, M | Dizziness | 25, R | Sporadic | Primary Staging | - |
| 10 | 70, W | Pulsatile tinnitus | 21, L | Sporadic | Recurrence | PRRT 2 |
| 11 | 47, M | Pulsatile tinnitus | 7, L | Sporadic | Primary Staging | - |
| 12 | 48, M | Pulsatile tinnitus | 13, L | Sporadic | Recurrence | IMRT 3 |
| 13 | 59, W | Asymptomatic | 22, R | Sporadic | Recurrence | Surgery PRRT 2 |
| 14 | 54, M | Tinnitus Ear discharge | 12, L | Sporadic | Primary Staging | - |
| 15 | 58, M | Pulsatile tinnitus | 9, R | Sporadic | Primary Staging | - |
| 16 | 37, M | Dizziness Hearing loss | 30, R | Sporadic | Primary Staging | - |
| Patient | GTV a (cm3) | DSC b | |||
|---|---|---|---|---|---|
| MRI | PET/CT | PET/MRI | MRI vs. PET/CT | MRI vs. PET/MRI | |
| 1 | 0.33 | 0.63 | 0.87 | 0.51 | 0.65 |
| 2 | 4.01 | 2.23 | 5.17 | 0.59 | 0.95 |
| 3 | 1.25 | 0.28 | 1.60 | 0.30 | 0.99 |
| 4 | 1.35 | 0.49 | 1.85 | 0.39 | 0.82 |
| 5 | 5.95 | 3.66 | 9.95 | 0.53 | 0.43 |
| 6 | 4.93 | 4.73 | 6.84 | 0.76 | 0.89 |
| 7 | 8.58 | 1.40 | 10.46 | 0.21 | 0.97 |
| 8 | 0.19 | 0.29 | 0.44 | 0.58 | 0.72 |
| 9 | 6.01 | 17.10 | 18.76 | 0.52 | 0.52 |
| 10 | 1.44 | 2.06 | 3.08 | 0.53 | 0.73 |
| 11 | 1.42 | 0.83 | 3.25 | 0.06 | 0.62 |
| 12 | 1.35 | 0.84 | 2.68 | 0.14 | 0.66 |
| 13 | 4.10 | 0.92 | 4.85 | 0.33 | 0.99 |
| 14 | 0.76 | 0.83 | 1.64 | 0.33 | 0.74 |
| 15 | 0.55 | 0.62 | 1.20 | 0.39 | 0.73 |
| 16 | 4.55 | 1.13 | 5.15 | 0.38 | 1.00 |
| Median (range) | 1.4 (0.19–8.58) | 0.88 (0.28–17.1) | 3.16 (0.44–18.76) | 0.4 (0.06–0.76) | 0.7 (0.43–1.0) |
| Mean (SD c) | 2.92 (2.54) | 2.38 (4.12) | 4.86 (4.79) | 0.41 (0.18) | 0.78 (0.18) |
| Patient | PGL Size (mm) 1 | V95% 2 | D98% 3 | D2% 4 | |||
|---|---|---|---|---|---|---|---|
| MRI | PET/MRI | MRI | PET/MRI | MRI | PET/MRI | ||
| 1 | 23 | 99.8 | 99.5 | 97.1 | 96.7 | 101.9 | 102.2 |
| 2 | 8 | 99.5 | 99 | 96.9 | 96.3 | 102.5 | 103.1 |
| 3 | 40 | 99.2 | 99.1 | 96.4 | 96.3 | 102.4 | 102.5 |
| Table 1 | SBPGL Size on MRI (mm) and Side (R/L 2) | OAR 3 | Dmax 4 (Gy) | Dmean 5 (Gy) | V15Gy 6 (%) | |||
|---|---|---|---|---|---|---|---|---|
| MRI | PET/MRI | MRI | PET/MRI | MRI | PET/MRI | |||
| Pt 1 2 | 23/R | Brainstem | 42.9 | 45.8 | 11.7 | 12.3 | ||
| R Parotid | 21.2 | 18.8 | 4.1 | 3.7 | 1.5 | 1 | ||
| R IAC 7 | 44.8 | 45.6 | 44.3 | 44.3 | ||||
| Mandible | 45.6 | 45.3 | 3.1 | 3.3 | ||||
| Pt 3 | 8/R | Brainstem | 46.9 | 47.0 | 12.6 | 13.1 | ||
| R Parotid | 46.4 | 46.0 | 3.6 | 3.7 | 4.9 | 5.5 | ||
| L IAC * | 2.5 | 2.8 | 2.2 | 2.7 | ||||
| L Cochlea * | 3 | 3.3 | 2.3 | 2.5 | ||||
| Pt 5 | 40/R | Brainstem | 46.7 | 46.7 | 18.9 | 19.8 | ||
| R Parotid | 46.7 | 46.9 | 14.8 | 19.3 | 35.8 | 50.9 | ||
| R IAC | 44.8 | 44.9 | 44.4 | 44.4 | ||||
| Mandible | 45 | 45.8 | 2.6 | 3 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Helali, M.; Moreau, M.; Le Fèvre, C.; Heimburger, C.; Bund, C.; Goichot, B.; Veillon, F.; Hubelé, F.; Charpiot, A.; Noel, G.; et al. 18F-FDOPA PET/CT Combined with MRI for Gross Tumor Volume Delineation in Patients with Skull Base Paraganglioma. Cancers 2019, 11, 54. https://doi.org/10.3390/cancers11010054
Helali M, Moreau M, Le Fèvre C, Heimburger C, Bund C, Goichot B, Veillon F, Hubelé F, Charpiot A, Noel G, et al. 18F-FDOPA PET/CT Combined with MRI for Gross Tumor Volume Delineation in Patients with Skull Base Paraganglioma. Cancers. 2019; 11(1):54. https://doi.org/10.3390/cancers11010054
Chicago/Turabian StyleHelali, Mehdi, Matthieu Moreau, Clara Le Fèvre, Céline Heimburger, Caroline Bund, Bernard Goichot, Francis Veillon, Fabrice Hubelé, Anne Charpiot, Georges Noel, and et al. 2019. "18F-FDOPA PET/CT Combined with MRI for Gross Tumor Volume Delineation in Patients with Skull Base Paraganglioma" Cancers 11, no. 1: 54. https://doi.org/10.3390/cancers11010054
APA StyleHelali, M., Moreau, M., Le Fèvre, C., Heimburger, C., Bund, C., Goichot, B., Veillon, F., Hubelé, F., Charpiot, A., Noel, G., & Imperiale, A. (2019). 18F-FDOPA PET/CT Combined with MRI for Gross Tumor Volume Delineation in Patients with Skull Base Paraganglioma. Cancers, 11(1), 54. https://doi.org/10.3390/cancers11010054