Abstract
OnabotulinumtoxinA (BT-A) is one of the few drugs approved for the preventive treatment of chronic migraine (CM). Despite this, some aspects of its mechanism of action are still a matter of debate, and the precise magnitude of BT-A effects needs to be completely elucidated. BT-A acts primarily upon trigeminal and cervical nerve endings, by inhibiting the release of inflammatory mediators such as calcitonin gene-related peptide, as well as reducing the insertion of ionotropic and metabotropic receptors into the neuronal membrane. These actions increase the depolarization threshold of trigeminal and cervical nerve fibers, thus reducing their activation. The central actions of BT-A are still a matter of debate: a retrograde axonal transport has been postulated, but not clearly assessed in humans. Clinically, the efficacy of BT-A in CM has been assessed by large, randomized placebo-controlled trials, such as the Phase 3 REsearch Evaluating Migraine Prophylaxis Therapy (PREEMPT) trials. Those results were also confirmed in a wide range of open-label studies, even for long-term periods. Recently, novel findings have led to a better understanding of its pharmacological actions and clinical usefulness in migraine prevention. This narrative review summarizes, updates and critically revises the available data on BT-A and its possible implementation in chronic migraine. Moreover, the current role of BT-A in CM treatment has been discussed.
Key Contribution:
Summarizing and critically analyzing the pre-clinical and clinical evidence of the action of OnabotulinumtoxinA in the preventive treatment of chronic migraine.
1. Introduction
Chronic migraine (CM) is diagnosed when a patient experiences migraine attacks for ≥15 days per month, at least for 3 months [1]. CM affects around 1–2% of the worldwide population and is considered one of the main neurological disabilities, as it tremendously affects patients’ quality of life [2]. Moreover, patients with CM usually take large amounts of painkillers, which may paradoxically worsen CM itself, leading to a secondary headache called medication overuse headache (MOH) [3]. The burden of CM is further aggravated by the shortage of effective preventive treatments, which are often associated with poor efficacy and tolerability as early as the first months of treatment [4]. Moreover, the frequent association with MOH usually lowers the effectiveness of the preventive treatments, thus requiring painkiller withdrawal [5] before a preventive treatment could be started. Today, only topiramate, onabotulinumtoxinA (BT-A) and monoclonal antibodies targeting the calcitonin gene-related peptide (CGRP) or its receptor are specifically approved for the preventive treatment of CM [6]. Many randomized clinical trials (RCT), as well as real-life studies, pointed out the effectiveness of BT-A in CM treatment; however, some issues remain unresolved. Indeed, it is not clear where its pharmacological effect takes place and its exact magnitude. Moreover, BT-A indications should also be reconsidered, stating the availability of anti-CGRP drugs in the therapeutic armamentarium against CM. The aim of the present review is to discuss and critically reconsider the current pre-clinical and clinical data available on BT-A in CM.
2. Materials and Methods
A data search via Embase, MEDLINE, Web of Sciences, Google Scholar, and Clinical Trials.gov (30 September 2022) was performed, as suggested in previous work by Bramer et al. [7]. In particular, the following was conducted using the following non-MESH terms: “onabotulinumtoxinA” AND “chronic migraine”. Only articles published up to 30 September 2022 were considered. Originally, 507 articles were found. For each one, the full text was analyzed in order to decide its inclusion in the article. Additionally, reference lists of relevant original research and/or reviews were also reviewed to identify any clinical and/or preclinical investigations related to the purposes of this article. In particular, pre-clinical studies were considered only if referred to a trigeminal pain model. Only clinical studies adopting the Phase 3 REsearch Evaluating Migraine Prophylaxis Therapy (PREEMPT) injection paradigm (155 or 195 IUs in 31–38 pericranial sites) [8] on adult patients were included in this review. Real-life studies with fewer than 50 patients were not considered, in order to increase the reliability of the results [9]. Only English-written articles were considered. Abstracts and book chapters were excluded.
3. Current Understanding of Migraine Pathophysiology with Relevance for BT-A Treatment
3.1. Anatomy
The trigeminal nerve conveys pain signals from the anterior two-thirds of the scalp [10], whilst the posterior third is innervated by the second and third cervical nerves [11]. First-order trigeminal neurons are pseudo-unipolar and are located in the trigeminal ganglion (TG) [10]. The peripheral branches of their axons project peripherally to the meninges and cranial dermatomes, whereas the central projections synapse with second-order trigeminal neurons located in the brainstem into the trigeminal nucleus caudalis (TNC) [10,11]. In particular, the peripheral branches of first-order trigeminal neurons are unmyelinated C-fibers or poor myelinated Aδ-fibers which reach the meninges mainly with the ophthalmic branch of the V cranial nerve and, to a lesser extent, with the maxillary and mandibular ones. These fibers terminate freely in the dura mater, surrounding meningeal arteries or terminating, to a lesser extent, around veins, capillaries, or in poorly vascularized zones [12]. These fibers send two more branches, one reaching the pia mater [12] and the other one crossing the skull through cranial sutures to reach the periosteum of the skull, pericranial muscles and the skin [11]. The extensive discussion of the meningeal distribution of the trigeminal fibers is beyond the scope of this article, but it is summarized in a review by Levy and co-workers [12]. In a similar way, the occipital and supraclavicular nerves are formed by the peripheral branches of the axons of the pseudounipolar neurons located in the second and third cervical ganglion. These axons are C-fibers or Aδ-fibers that terminate peripherally in the skin, periosteum, and pericranial muscles located in the posterior third area of the scalp, sending collateral branches that cross the cranial sutures, bone canals and foramen magnum to reach the TNC, thus contributing to the trigeminal pain [13]. Therefore, the skull appears to be englobed by a wide network of intracranial and extracranial nociceptive fibers, originating from the V cervical nerve as well as from the second and third cervical nerves [14]. The pain signals conveyed by the trigeminal and the cervical fibers are integrated into the TNC, which can be considered as the “hub” of peripheral stimuli in migraine [15]. The axons of second-order neurons in the TNC decussate and reach the ventral posteromedial nucleus (VPMN) of the contralateral thalamus through the trigeminothalamic tract. The VPMN of the thalamus contains the third-order neurons that project to the primary and secondary somatosensory cortexes [10].
The abovementioned anatomic considerations are necessary to understand:
- The injection protocol used for CM;
- The ability of BT-A to inhibit cranial nociceptor activation toward both intracranial and extracranial stimuli.
3.2. Spotlights of Mechanisms in CM Justifying BT-A Use
3.2.1. Stimuli Potentially Activating Cranial Nociceptive Fibers
Pain in CM arises from the activation of the nociceptive fibers innervating the meninges and the cranial dermatomes. These fibers may be activated by a wide range of stimuli (mechanical, thermal, chemical) because of the presence on their membranes of different kinds of receptors, such as the transient receptor potential vanilloid type 1 receptor (TRPV1); transient receptor potential ankyrin 1 receptor (TRPA1); and transient receptor potential membrane protein 8 (TRPM8) [16]. Moreover, the fact that both trigeminal and cervical fibers cross the skull gives the reason for their activation by intracranial as well as extracranial stimuli [17]. Among the first, cortical spreading depression (CSD) may activate nociceptive fibers [18]. Specifically, CSD is a cortical wave of neuronal and glial depolarization propagating at a speed of 2–6 mm per minute and followed by a long hyperpolarization (20–30 min). CSD activates meningeal nociceptors through the diffusion of small molecules such as nitric oxide (NO), potassium ions (K+), adenosine triphosphate (ATP) or hydrogen ions (H+) in the superficial cortical layer and their subsequent diffusion through the pia mater, arachnoid and dura mater [18]. The small molecules released by the abovementioned events act upon receptors such as the TRPV1, the TRPA1 and the TRPM8 [19]. Notably, as CSD is the physiological correlate of migraine with aura, this finding may justify the connection between aura symptoms and pain [20]. Extracranial stimuli activating nociceptive fibers may be physical, such as the mechanical deformation of the skin that can trigger the release of adenosine triphosphate (ATP) from keratinocytes and the activation of purinergic receptor P2X ligand-gated ion channel 3 (P2X3) expressed on the membrane of sensory nerve terminals [21]. Thermal stimuli may activate trigeminal nerve fibers as well, through the activation of TRMP8 channels [21]. Chemical stimuli, such as capsaicin, may activate TRPV1 channels [21]. The abovementioned receptors are ionotropic, and their exposure to a specific stimulus induces conformational changes and an increase in membrane conductivity towards cations, thus determining the depolarization of the cranial nociceptive fibers.
3.2.2. Consequences of the Generation of an Action Potential in the Cranial Nociceptors
Regardless of the stimulus, if the depolarization of the neuronal membrane is supra-threshold, an action potential is generated and propagates both orthodromically and antidromically [22]. The antidromic conduction of the action potential increases the exocytosis of large dense-core vesicles from the termination of both C- and Aδ-fibers [23], whereas the orthodromic conduction determines the same phenomena at the level of the nerve bundles, which are not surrounded by Schwann’s cells. It ought to be taken into consideration that the abovementioned phenomena usually happen at a quantile level even in the basal conditions, but, if driven by an action potential, are more important. As a whole, the action potential causes the opening of the voltage-gated calcium channels, thus inducing the flow of Ca2+ inside the neurons [15] and the subsequent activation of the soluble N-ethymalemide-sensitive factor attachment protein receptor (SNARE) complex. The activation of the last complex is critical for the exocytosis processes. The exocytosis of large dense core vesicles has two main implications for migraine pathogenesis: the exocytosis of neurotransmitters and neuromodulators [24] as well as the insertion of receptors in the plasma membrane of cranial nociceptive fibers [25]. In particular, trigeminal nerve fibers contain large dense core vesicles containing CGRP, substance P, pituitary adenylyl cyclase-activating polypeptide 38 (PACAP-38) and receptors such as TRPV1, TRPA1 and P2X3 [21]. The exocytosis of neuromodulators determines the induction of a state of sterile neurogenic inflammation at the meningeal level, for which the most well-known actor is the CGRP [24]. For this reason, the discussion will take over on CGRP. The exocytosis of the CGRP determines three main phenomena. The first one is vasodilation at the meningeal level, as unequivocally demonstrated by an experiment with CGRP-blocking antibodies in rats [26]. Furthermore, the action of CGRP on pericytes at the endothelial levels determines an increase in the permeability of meningeal arteries [27]. Furthermore, the degranulation of meningeal mast cells has been linked to trigeminal nerve fiber activation [28]. It should be noticed that meningeal immune cells and CGRP are a growing field of research, but their relationship has not been completely unveiled yet. Despite this, readers may find an exhaustive review on this topic [28]. Moreover, CGRP also binds upon its receptors located on the Aδ-fibers, thus activating the PKA pathway and, consequently, trigeminal fiber sensitization [29]. On the other hand, the increase in the receptor expression upon the membrane of the cranial nerve fibers determines a reduction in the activation threshold of these fibers and, consequently, a higher probability of action potentials being generated [30].
3.2.3. Central Transmission of the Pain Signals
After that, an action potential is transmitted towards the pyrenophore of the trigeminal and/or cervical neurons and through the centripetal branch of their axon, thus synapsing with the second-order neurons located in the TNC [10,22]. It should also be considered that the pain signal transmission at a cranial level is much more complex than described with the possibility of different neurons influencing the activity of the neighboring neurons, both at the level of the axon [31] and the pyrenophore [32]. At the central terminals, glutamate, serotonin and NO activate excitatory receptors on second-order neurons in the TNC in a frequency-dependent manner, which in turn displays an enhanced response following repeated stimuli [33]. Given these issues, in CM, trigeminal first-order neurons are sensitized at two levels: at the axon and at the pyrenophore [34]. Indeed, CM is often accompanied by an enhanced sensitivity to a light touch applied to the skin (tactile allodynia), reflecting the somatic convergence upon the same pool of second-order neurons receiving meningeal inputs [35]. Hence, CM may be considered as a referred pain mechanism, reflecting the convergence of sensory afferents originating from intracranial and extracranial structures to the second-order neurons in the TNC [35,36]. The distinction between intracranial and extracranial stimuli activating cranial nociceptors is clinically translated by the feature of an “imploding headache” as well as an “exploding headache”, respectively [37]. As BT-A is more effective in the relief of the imploding headache, it is more effective in inhibiting the activation of cranial nociceptors towards extracranial stimuli. Obviously, the present dissertation on migraine pathophysiology only considers the mechanism which can have relevance for BT-A treatment. Despite a growing amount of evidence pointing out the involvement of central mechanisms in CM pathophysiology, they will be only partially discussed.
4. Putative Mechanisms of BT-A in Migraine
The abovementioned mechanisms are fundamental to understanding the rationale behind the action of the BT-A in CM and, primarily, the rationale sustaining the internationally accepted injection protocol [8]. According to the PREEMPT protocol, the injections of the BT-A are given in 31 different points localized in muscles: frontalis, corrugator, procerus, temporalis, occipitalis, trapezius and cervical paraspinal muscle group. Additionally, up to 40 IU of BT-A may be administered using a “follow the pain” strategy into the temporalis, occipitalis or trapezius muscles [8]. Those areas correspond to the main nerves containing the peripheral branches of the axons of the trigeminal and cervical primary neurons (supraorbital, supratrochlear, zygomaticotemporal and auriculotemporal nerves) and in the second and third cervical ganglions (greater, lesser and accessory occipital nerves, supraclavicular nerves). These points are graphically summarized in Figure 1.
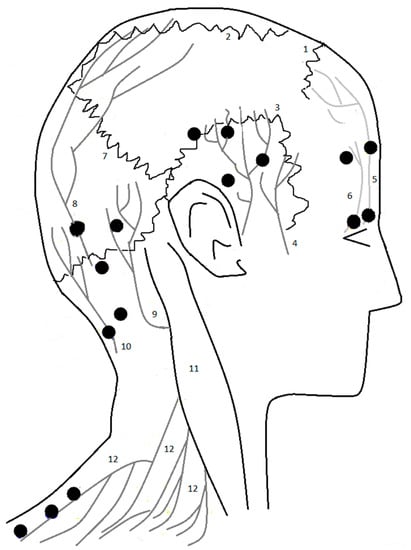
Figure 1.
The points of the injections of BT-A and the nearby nerves from the PREEMPT 1 and 2 studies. Legend: 1: coronal suture; 2: sagittal suture; 3: squamosal suture; 4: auriculotemporal nerve; 5: supratrochlear nerve; 6: supraorbital nerve; 7: lambdoid suture; 8: greater occipital nerve; 9: lesser occipital nerve; 10: Third occipital nerve; 11: sternocleidomastoid muscle; 12: supraclavicular nerve.
The possibility for extracranial-injected BT-A to influence the activity of intracranial neurons derives from the presence of intracranial nociceptive fibers that send collaterals crossing the skull through the sutures and emissary vein channels in mice, rats and humans [38,39,40]. Notably, a new version of the injection protocol specifically targets the sutures, i.e., the points in which the cranial nociceptive fibers enter the skull [41]. BT-A is a 900 kDa complex consisting of a 150 kDa botulinum neurotoxin associated with non-toxic proteins (neurotoxic-associated proteins—NAPs). The NAPs play a role in the pharmacological stability of the neurotoxin, determining its stability and protecting it from proteolysis. After the injection in the dermis, the NAPs rapidly dissociate from BT-A itself at a neutral pH, due to conformational changes, thus allowing BT-A to diffuse through extracellular space and reach the external projection of the trigeminal as well as the cervical neurons, which pass through the skull and reach the cranial dermatomes [42]. Probably, a still-unquantified, small amount of BT-A does not bind to the nerve fibers, and it is probably washed out from the lymphatic circulation [43]. The 150 kDa BT-A neurotoxin is composed of a light chain of 50 kDa (which contains the catalytic domain) and a heavy chain of 100 KDa. The last one is important for stability and transit, and the cellular penetration of the light chain is linked with it via a disulfide bond. The C-terminus of the heavy chain binds to the glycoproteins of the neuronal membrane surface, mainly trisialoganglioside GT1b and ganglioside GD1a [44]. The binding between GT1b and GD1a induces an initial, low-affinity binding to the neuronal membrane. After that, the interaction with the synaptic vesicle protein 2 (SV2) [45] or with the fibroblast growth factor receptor 3 (FGFR3) [46] induces clathrin-mediated endocytosis [47]. Interestingly, some evidence pointed out a role even for TRPV1 in this process [48]. Moreover, the N-terminus of the heavy chain (HN) may also be involved in the specific neuronal binding via interaction with phosphatidyl inositol phosphates at the presynaptic plasma membrane [49]. Once endocytosed, the BT-A mainly enters into the acidic vesicles, whereas the smaller fraction that enters non-acidic vesicular compartments may be sorted into the microtubule-dependent retrograde axonal transport pathways. The BT-A that enters the non-acidic compartment is sorted into the microtubule-dependent retrograde axonal transport towards the Gasser’s ganglion [49]. The entrance of the BT-A in the acidic vacuole determines its degradation into two parts: the 100 kDa remains in the acidic vacuole, whereas the 50 kDa domain is released into the cytoplasm and enters the cytosol through the reduction of the dysulfidrile bond that links the two parts [50]. The 50 kDa subunit concentrates near the inner layer of the plasma membrane thanks to its interactions with septins and the recruiting of specialized enzymes that inhibit ubiquitination [51,52]. This may explain the long-term persistence of BT-A action in nerve terminals, which is up to 1 year in cultured neurons and about 5 months in vivo [51]. The BT-A light chain is a Zn2+ dependent metalloprotease that cleaves the synaptosomal-associated protein of 25 kDa (SNAP-25), thus forming SNAP-25 (1–197), which is inactive and forms heterotrimers with other SNARE proteins to create inactive complexes [53]. The cleavage of SNAP-25 inhibits the exocytosis processes, thus limiting neuropeptides’ and neurotransmitters’ exocytosis and reducing the presentation of receptors on the plasma membrane [54]. Many pre-clinical papers have unveiled the mechanisms of action of BT-A in CM. Firstly, BT-A is able to inhibit the firing of meningeal nociceptors activated by cortical spreading depression in female rats, thus demonstrating the capability of BT-A to inhibit the activation of the meningeal nociceptor towards intracranial stimuli [55]. Among extracranial stimuli, BT-A has also been proven to inhibit the mechanical stimulation of the meningeal nociceptors, and, notably, BT-A inhibited only C-fibers and was also more effective in inhibiting the branch of peripheral nociceptors, but not the dural axon [56]. Moreover, a reduction in the response mediated by the TRPV1 and TRPA1 has also been detected in the peripheral branches of the cranial nociceptive neurons [57,58]. Interestingly, a decrease in the expression of TRPV1 was detected even at the level of the TG [25]. Furthermore, a decrease in the release of CGRP from the trigeminal neurons has been demonstrated, at the levels of both the peripheral branch of the axon [58] and the pyrenophore inside the TG [59]. Notably, a reduction in peripheral inflammation and peripheral sensitization has been found in human models of trigeminal sensitization [60,61]. It ought to be taken into consideration that cranial C-fibers contain the largest amount of CGRP, whereas Aδ-fibers have the highest expression of the CGRP receptor. Therefore, BT-A inhibits mainly C-fibers rather than Aδ ones [56]. Additionally, BT-A has been shown to undergo retroactive transport to influence the trigeminal neurons’ activity even at the level of TNC [62,63], as this effect is blocked by colchicine [64,65]. Despite this, not enough evidence is present to prove that BT-A may have central effects [66].
5. Clinical Use of BT-A in the Treatment of Chronic Migraine
5.1. Clinical Trials
5.1.1. PREEMPT-1 and PREEMPT-2 Protocols
The first trials exploring the efficacy and safety of BT-A for the preventive treatment of CM were the PREEMPT ones. In particular, two randomized placebo-controlled trials were conducted. In the PREEMPT-1 trial, no significant differences were found between the BT-A and the placebo groups regarding the reduction in the number of headache episodes (−5.2 vs. −5.3; p = 0.344). Moreover, in the treated group, there was a significantly higher reduction in the number of headache days (p = 0.006), the number of migraine days (p = 0.002) and the number of triptans taken (p = 0.023) [67]. In the second PREEMPT-2 trial, 347 patients were randomly assigned to BT-A and 358 to placebo. In this trial, a significantly higher change from the baseline in the frequency of headache days (p < 0.001), in the frequency of migraine days (p < 0.001), in the frequency of moderate/severe headache days (p < 0.001) and in the HIT-6 score (p < 0.001) was found [68].
5.1.2. Pooled Results of the PREEMPT-1 and PREEMPT-2 Protocols
A pooled analysis of the PREEMPT-1 and PREEMPT-2 results showed that BT-A (n = 688) determined a significant reduction in the number of headache days per month, the number of migraine days per month and the number of moderate/severe headache days per month after 24 weeks of treatment following the PREEMPT protocol [69]. A sub-group analysis by Lipton and coworkers performed on the pooled analysis unveiled that patients treated with BT-A experienced a significant amelioration in their quality of life, as witnessed by the 6-items headache impact test (HIT-6) and the Migraine-Specific Quality of Life Questionnaire v2.1 (MSQ) after 24 weeks of treatment [70]. Moreover, patients treated with BT-A also displayed bigger ameliorations of the HIT-6 score and of the MSQ score already after 12 weeks of treatment [70]. Furthermore, Silberstein and collaborators compared the effects of BT-A vs. placebo for the preventive treatment of CM in patients who displayed medication overuse at the baseline [71]. Interestingly, BT-A was superior to the placebo in the 24th week in terms of headache reduction and in the amelioration of the quality of life [71]. Among the painkillers, a significant decrease was seen for triptan and ergots, suggesting that BT-A is more effective on migraine-specific attacks rather than the ones with a tensive component [71].
5.1.3. Pooled Results of the Open-Label Phase of the PREEMPT-1 and PREEMPT-2 Protocols
The PREEMPT trials foresaw a first double-blind 24-week-long phase, followed by a 32-week, open-label, single-treatment phase. Aurora’s group was the first to publish the results of even the open-label phase, still highlighting some significant differences between the patients taking BT-A or a placebo at the end of the observational period [72]. In particular, a significant reduction compared to the placebo was detected in terms of the frequency of headache and/or migraine days and in the number of moderate/severe headache days at 36 and 48 weeks. After the end of the open-label phase, the abovementioned parameters remained significant over the course of 1 year [72]. The ameliorations in the quality of life were even maintained after the open-label phase of the PREEMPT trial. Indeed, as Lipton and coworkers demonstrated, the HIT-6 and MSQ ameliorations observed in patients who received BT-A in the first 24-week-long phase were maintained even in the open-label phase of the trial, but not until the 56th week [73].
5.1.4. Speed of Action of the BT-A from the PREEMPT-1 and PREEMPT-2 Protocols Pooled Analysis
The ameliorations in the quality of life found by Lipton and co-workers may also be attributed to a drastic reduction in the days with severe headache attacks, which was higher for the group treated with BT-A in the PREEMPT trial, whereas in the open-label phase, these differences were null [74]. In particular, the benefits of BT-A spread rapidly, as also witnessed by the percentage of patients experiencing a ≥50% response, which was about half of the patients after 12 weeks [75]. Despite the effectiveness that BT-A has demonstrated vs. placebo in treating MOH, BT-A did not afford any additional benefit over acute withdrawal alone in a recent trial conducted in patients with CM and MOH, neither on headache frequency nor on quality of life, disability or other outcome measures [76]. Despite this, another article highlighted how the effects of BT-A spread even after 1 week, thus suggesting a rapid onset of BT-A activity [77].
5.1.5. BT-A vs. Topiramate
Additionally, BT-A was also explored in some RCTs against the only other drug specifically approved for the preventive treatment of CM, i.e., topiramate. The comparison between BT-A and topiramate was explored in the FORWARD study, demonstrating that the proportion of ≥50% responders was significantly higher in the group treated with BT-A [78,79]. RCTs regarding BT-A in CM are summarized in Table 1.

Table 1.
Clinical trials of BT-A in migraine.
5.2. Real-Life Studies
Several real-world studies have been published, with findings consistent with PREEMPT studies in CM patients with and without MOH [80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127]. Real-world studies primarily exploring the effectiveness and safety of BT-A compared to the baseline are summarized in Table 2. One of the largest real-life studies was aimed at measuring healthcare resource utilization, and patient-reported outcomes observed in clinical practice (REPOSE study) [103,107]. In 633 patients with CM who received at least one dose of BT-A during a 2-year clinical routine, the CM frequency significantly diminished at all post-baseline visits, with improvements reported also in quality of life [103]. The results are congruent with a different group of 725 patients with CM, with the chances of a good outcome increased by starting treatment in the first 12 months after CM diagnosis [98]. Another big study was conducted by Khalil et al. on 254 adults with CM [80]. After one month of a single BT-A injection following the PREEMPT paradigm, there was a reduction in the number of headache and migraine days compared with the baseline, as well as an overall reduction in the number of days spent using analgesics and triptans [80]. Interestingly, the authors discovered that a longer CM duration and a higher disability as well as a higher consumption of painkillers at the baseline were negatively associated with a good response to BT-A after 1 year of treatment [80]. These results were substantially confirmed by Aicua-Rapun et al. [88]. B-TA has been demonstrated to be an effective and safe treatment even for long-time use. Indeed, different groups have unveiled that the BT-A effectiveness even lasts for 2 years of treatment [83,85,86]. Notably, some research groups have discovered that BT-A is effective even at longer time points, such as 3 years [95,99] and 4 years [108]. Apart from the prolonged effectiveness, it has been unveiled that the BT-A action spread fast, thus confirming the results of the PREEMPT study [76]. Indeed, many patients respond even at the first cycle [103,106]. Recently, a European collaboration has published different papers on a sample of 2879 patients in order to answer some still-open questions about the clinical use of the BT-A. Firstly, this group determined that two BT-A cycles are usually enough to establish if a patient is a responder or a non-responder to the BT-A. Indeed, patients who do not respond to the first two cycles of BT-A are unlikely to respond to the third cycle [125]. This indicates that, as BT-A effects spread rapidly, the first 6 months of treatment should be enough to establish if BT-A should be continued or not. Moreover, due to its relative expensiveness and the arrival of new anti-CGRP mAbs, it should also be important to identify patients who may benefit more from BT-A injections. In particular, the predictors of response towards BT-A are a higher CM duration, a higher disability and a higher VAS score at the baseline [98]. In the study by Dominguez and collaborators, no influence on MOH was detected. Despite this, Caronna et al. demonstrated the effectiveness of BT-A even in the treatment of CM complicated with MOH [102]. Negro et al. described the sustained effectiveness of the toxin for up to two years, even in patients complicated by MOH [85]. Specifically, BT-A reduced the number of migraine days and medication intake, also ameliorating HIT-6 scores [85]. Similar findings were described by Guerzoni and co-workers in a severely impaired population [86] and also for a longer time, up to 3 years [87]. Moreover, Ahmed et al. explored the effects of BT-A in 343 patients with CM, either overusing or not overusing medications [82]. Moreover, these data have been explored even up to 4 years, demonstrating stable effectiveness through time [88]. An improvement in the quality of life associated with a reduction in the HIT-6 score was also described [115,116,117,118]. Such findings were in accordance with another study conducted by Stark et al. [109]. In 211 patients with CM, around 74% of the treated patients achieved a relevant reduction in monthly headache days after only two treatment cycles, with concomitant lower use of acute headache medications [109]. BT-A’s efficacy has also been assessed on allodynia [110,111], which is frequent among chronic migraineurs and complicates their management. Young and co-workers clearly demonstrated that patients with and without allodynia similarly respond to BT-A [111]. Besides its effectiveness in difficult-to-treat patients, such as MOH sufferers and ones displaying allodynia, BT-A treatment response is also sustained in time. Indeed, about two-thirds of patients with CM achieving 50% or more response to BT-A within the third cycle of treatment maintain this positive response over time [110]. As CM is frequently associated with psychiatric comorbidities [2], different studies investigate the effects of BT-A on depressive symptoms [84,90,100]. Demiryurek et al. explored the activity of the toxin on depression and anxiety with the Beck Depression Inventory and the Beck Anxiety Inventory. After the third treatment cycle, only a slight improvement in the Beck Depression Inventory was achieved [90]. Similar results were obtained by Maasumi et al. using the nine-item Patient Health Questionnaire. In the latter study, a slight improvement in 359 patients was observed only at the third cycle [84]. A more recent study by Blumenfeld et al. demonstrated that the nine-item Patient Health Questionnaire and the seven-item generalized anxiety disorder score results were significantly lower compared to the baseline at all time-points until the ninth injection cycle [100]. By week 108, around 80% of the patients obtained a meaningful improvement in their depressive and anxiety symptoms [100]. Additionally, Aydinlar and collaborators found a significant reduction in the Migraine Disability Assessment (MIDAS) questionnaire score after the fifth BT-A injection compared to the baseline, but no improvements in the patients’ sleep quality [92]. Taken together, all this evidence points out also a favorable BT-A effect on the psychiatric comorbidities of CM, which may be an obstacle to its successful treatment, which is why it should be diagnosed early in CM. Gender does not influence patients’ response to BT-A [124]. Additionally, BT-A may also be a safe and valuable tool to treat CM in the elderly, when many treatments are not indicated [126].
Table 2.
Real-life studies.
5.3. Tolerability and Interactions
Adverse events (AEs) associated with BT-A are mainly local and transitory [80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127]. Muscular weakness, especially in the trapezius muscle, is one of the most common [116]. Other AEs include local itch, pain, inflammation, edema and swelling, mainly due to the mechanical stress related to the injection procedure. A flu-like syndrome and general malaise are rare but described. Both are possibly related to the systemic effects of BT-A. Post-injection headaches have also been reported; thus, BT-A injections should not be performed during migraine attacks. Such adverse events have been described for dosages of 155 U per treatment cycle, but also higher dosages have shown a similar safety profile [92]. Notably, BT-A safety is comparable to the placebo and maintained even after long-term therapies [87,96]. As a consequence, most patients were satisfied or extremely satisfied with BT-A treatment [88]. The overall incidence of adverse events and the most common individual events decreased with repeated BT-A administration [116]. In particular, the local AEs may be avoided by careful injection techniques, such as avoiding touching the periosteum or deep injections. Furthermore, as the extracranial prolongation of the trigeminal and cervical nerves cross the skull towards sutures and emissary canals, another way to reduce the potential of the BT-A inducing adverse events could be to practice injections only at the sutures [41]. Notably, some research groups have been focused on how ultrasound-guided injections improve the safety of BT-A injections. In particular, Kara et al. have described a new protocol for eco-guided injections of BT-A along the sutures, which improved the safety and effectiveness of the BT-A [128,129,130,131]. No interactions between BT-A and other drugs have been described so far.
5.4. Current Role of BT-A in the Treatment of Chronic Migraine
BT-A has the merit of being the first treatment specifically approved for the prevention of CM. The advent of BT-A shed light on a previously neglected disorder for which there were few available treatments with severe AEs and poor efficacy, which dramatically reduced patients’ compliance [4]. Beyond its effectiveness, the scheduling of the injections 3 months from each other increases patients’ compliance. Furthermore, BT-A has been demonstrated to have a more favorable cost-effectiveness profile than oral preventive anti-migraine drugs, especially in terms of a significantly lower likelihood of head-ache-related emergency department visits and hospitalizations [118]. Moreover, Rothrock and co-workers assessed that patients affected by CM experienced a significant cost offset during only the first 6 months of treatment [119]. The advent of BT-A also encouraged an interesting field of research in the pathophysiology of migraines, improving the understanding of the peripheral circuitry of migraine pain [43]. BT-A might also have central actions that are, however, yet to be defined on a mechanistic basis [62]. A large body of evidence from randomized and open-label studies summarized in this review supports the use of BT-A for the treatment of CM [67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127]. However, there are several open issues in the management of BT-A in clinical practice. For instance, it is unclear whether detoxication can enhance the preventive efficacy of BT-A in patients with medication overuse. BT-A is a proven treatment for medication overuse, in both randomized [71] and real-life [111] settings. However, a randomized trial emphasized the low value of detoxification treatments [76]. Moreover, good real-life data on the added value of combining detoxication and BT-A are lacking. Identifying predictors of response to BT-A could help avoid unnecessary treatments; however, the literature data in the field are inconclusive [99,132]. In the absence of clear selection criteria, a trial of BT-A can be offered to all patients with CM unless contraindicated. A further clinical issue is when declaring the failure of BT-A, as evidence suggests that patients not responding to the initial doses might respond later, even after one year [111], but, despite this, patients who do not respond to the first two cycles rarely found benefit from the third one [124]. A further clinical issue is whether treatment should be stopped in patients who present a sustained response to BT-A, as CM might undergo a rebound. An alternative approach to treatment stopping in those patients could be to increase the injection-free period from 3 to 4 or more months; however, the advantages of delayed injections have to be balanced with the potential wear-off of BT-A [105,121,122]. Moreover, some evidence suggests that BT-A suspension is associated with up to 6 months of well-being before CM relapses, at least in responders [106], but a recent article showed that the delay of BT-A due to the spread of the SARS-CoV-2 pandemic determines an overall worsening of migraines in patients previously affected by CM and MOH [123]. All these aspects of clinical practice are worth assessing in real-life studies. Moreover, BT-A could provide additional value when bruxism and/or temporomandibular joint disorder is present as a comorbidity to the CM [133]. Injecting additional BT-A into the masseter and temporalis muscles may not only ameliorate the bruxism but also improve the efficacy of PREEMPT. BT-A is now not the only specific preventive treatment for CM, as new treatments specifically targeting the calcitonin gene-related peptide (CGRP) or its receptor also represent a valid option [130]. In patients with CM that are resistant or have contraindications to several oral preventatives, it is uncertain whether BT-A or anti-CGRP mAbs should be used first. The choice between a monoclonal antibody against the CGRP or its receptor and BT-A should be targeted according to the patient’s headache history, comorbidities, and preferences. BT-A is particularly indicated in those patients who have an unfavorable cardiovascular risk profile or in older patients with polytherapy who might not tolerate treatments with a systemic action [127]. On the other hand, monoclonal antibodies might be preferred before BT-A in younger patients with a more favorable vascular risk profile. Notably, both BT-A and anti-CGRP mAbs act on the peripheral mechanisms of migraine pain. However, the peripheral action of BT-A is different from that of monoclonal Abs, paving the way for a possible combination of those two treatments in the future [134]. Indeed, the association between BT-A and anti-CGRP mAbs could be particularly indicated to reduce the wearing-off effect of BT-A, which is responsible for the reduction in the BT-A effect in the final part of the 3-month period between different toxin injections [107].
6. Conclusions
BT-A has been extensively studied in the preventive treatment of CM. Evidence that BT-A leads to a reduction in monthly headache and migraine days and improves quality of life originated from a series of clinical trials and real-world studies. Additionally, BT-A proved to be a safe medication, and patients are more comfortable than with traditional preventatives [85]. BT-A is also associated with lower health service utilization, especially for emergency departments [118]. In patients with CM and MOH, more work is necessary to clarify the usefulness of BT-A. Concerning its mechanism of action, there is still uncertainty about the true anti-nociceptive mechanism in CM, regarding in particular its hypothesized central effects.
Author Contributions
C.B., F.L.C., R.O., S.S., L.P. and S.G. have equally contributed to the conceptualization, the data collection and the writing of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
C.B. and S.G. received travel grants and honoraria from Eli Lilly, Novartis, Teva and Allergan. L.P. is the Chief Scientific Officer of EDRA-LSWR Publishing Company and of Inpeco SA Total Lab Automation Company. In the last year, he has been a scientific consultant to AbbVie, USA; BCG, Switzerland; Boehringer-Ingelheim, Germany; Compass Pathways, UK; Johnson & Johnson, USA; Takeda, USA; VeraSci, USA; Vifor, Switzerland. R.O. reports speaker fees from Novartis and Eli Lilly, travel grants from Teva, and support for publication from Novartis and Allergan. S.S. reports personal fees from Allergan-AbbVie, AstraZeneca, Abbott, Teva, Novartis, Novo Nordisk, Medscape, Neurodiem and Eli Lilly. F.L.C. declares no conflict of interest.
References
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd Edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine: Epidemiology, burden and comorbidity. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Holle, D.; Solbach, K.; Gaul, C. Medication-overuse headache: Risk factors, pathophysiology and management. Nat. Rev. Neurol. 2016, 12, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Hepp, Z.; Dodick, D.W.; Varon, S.F.; Chia, J.; Matthew, N.; Gillard, P.; Hansen, R.N.; Devine, E.B. Persistence and switching patterns of oral migraine prophylactic medications among patients with chronic migraine: A retrospective claims analysis. Cephalalgia 2017, 37, 470–485. [Google Scholar] [CrossRef]
- Carlsen, L.N.; Munksgaard, S.B.; Jensen, R.H.; Bendsten, L. Complete detoxification is the most effective treatment of medication-overuse headache: A randomized controlled open-label trial. Cephalalgia 2018, 38, 225–236. [Google Scholar] [CrossRef]
- Agostoni, E.C.; Barbanti, P.; Calabresi, P.; Colombo, B.; Cortelli, P.; Frediani, F.; Geppetti, P.; Grazzi, L.; Leone, M.; Martel-Letti, P.; et al. Italian chronic migraine group. Current and emerging evidence-based treatment options in chronic migraine: A narrative review. J. Headache Pain 2019, 20, 92. [Google Scholar] [CrossRef]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combination for literature searches in systematic review: A prospective exploratory study. Syst. Rev. 2017, 6, 245. [Google Scholar] [CrossRef]
- Blumefeld, A.; Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; Binder, W.J. Method of injection of OnabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache 2010, 50, 1406–1418. [Google Scholar] [CrossRef]
- Hobart, J.C.; Cano, S.J.; Warner, T.T.; Thompson, A.J. What sample sizes for reliability and validity studies in neurology? J. Neurol. 2012, 259, 2681–2694. [Google Scholar] [CrossRef]
- Edvinsson, J.C.A.; Viganò, A.; Alekseeva, A.; Alieva, E.; Arruda, R.; De Luca, C.; D’Ettore, N.; Frattale, I.; Kurnukhina, M.; Macerola, N.; et al. European Headache Federation School of Advanced Studies (EHF-SAS). The fifth cranial nerve in headaches. J. Headache Pain 2020, 21, 65. [Google Scholar] [CrossRef]
- Noseda, R.; Melo-Carrillo, A.; Nir, R.R.; Strassman, M.; Burstein, R. Non-trigeminal nociceptive innervation of the posterior dura: Implication to occipital headache. J. Neurosci. 2019, 39, 1867–1880. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Labastida-Ramirez, A.; MaassenVanDenBrink, A. Current understanding of meningeal and cerebral vascular function underlying migraine headache. Cephalalgia 2019, 39, 1606–1622. [Google Scholar] [CrossRef] [PubMed]
- Schueler, M.; Messlinger, K.; Dux, M.; Neuhuber, W.L.; De Col, R. Extracranial projections of meningeal afferents and their impact on meningeal nociception and headache. Pain 2013, 154, 1622–1631. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Blake, P.; Schain, A.; Perry, C. Extracranial origin of headache. Curr. Opin. Neurol. 2017, 30, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Busch, V.; Jakob, W.; Juergens, T.; Schulte-Mattler, W.; Kaube, H.; May, A. Functional connectivity between trigeminal and occipital nerve blockade and nociceptive blink reflexes. Cephalalgia 2006, 26, 50–55. [Google Scholar] [CrossRef]
- Terrier, L.M.; Hadjikhani, N.; Destrieux, C. The trigeminal pathways. J. Neurol. 2022, 269, 3443–3460. [Google Scholar] [CrossRef]
- Matak, I.; Bolcskej, K.; Bach-Rojecky, L.; Helyes, Z. Mechanisms of botulinum toxin type A action on pain. Toxins 2019, 11, 459. [Google Scholar] [CrossRef]
- Zhang, X.; Levy, D.; Noseda, R.; Kainz, V.; Jakubowski, M.; Burstein, R. Activation of meningeal nociceptors by cortical spreading depression: Implication for migraine with aura. J. Neurosci. 2010, 30, 8807–8814. [Google Scholar] [CrossRef]
- Zhao, J.; Levy, D. Modulation of intracranial meningeal nocicpetor activity by cortical spreading depression: A reassessment. J. Neurophysiol. 2015, 113, 2778–2785. [Google Scholar] [CrossRef]
- Close, L.N.; Eftekhari, S.; Wang, M.; Charles, A.C.; Russo, A.F. Cortical spreading depression as a site of origin for migraine: Role of CGRP. Cephalalgia 2019, 39, 428–434. [Google Scholar] [CrossRef]
- Viana, F. Chemosensory properties of the trigeminal system. ACS Chem. Neurosci. 2011, 2, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Gafurov, O.; Koroleva, K.; Gianitullin, R. Antidromic spike propagation and dissimilar expression of P2X, 5-HT, and TRPV1 channels in peripheral vs. central sensory axons in meninges. Front. Cell Neurosci. 2021, 14, 6231134. [Google Scholar] [CrossRef]
- Ferrandiz-Huertas, C.; Mathivanan, S.; Wolf, C.J.; Devesa, I.; Ferrer-Montiel, A. Trafficking of thermoTRP channels. Membranes 2014, 4, 525–564. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, R. Neurogenic inflammation and its role in migraine. Semin Immunopathol. 2018, 40, 301–314. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Shibata, M.; Toriumi, H.; Iwashita, T.; Funakubo, M.; Sato, H.; Kuroi, T.; Ebine, T.; Koizumi, K.; Suzuki, N. Reduction of TRPV1 expression in the trigeminal system by botulinum neurotoxin type-A. Neurobiol. Dis. 2012, 48, 367–378. [Google Scholar] [CrossRef]
- Dux, M.; Vogler, B.; Kuhn, A.; Mackenzie, K.D.; Stratton, J.; Messlinger, K. The anti-CGRP antibody fremanezumab lowers CGRP release from rat dura mater and meningeal blood flow. Cells 2022, 11, 1768. [Google Scholar] [CrossRef]
- Schain, A.J.; Melo-Carrillo, A.; Stratton, J.; Strassman, A.M.; Burstein, R. CSD-induced arterial dilatation and plasma protein extravasation are unaffected by fremanezumab: Implications for CGRP’s role in migraine with aura. J. Neurosci. 2019, 39, 6001–6011. [Google Scholar] [CrossRef]
- Balcziak, L.K.; Russo, A.F. Dural immune cells, CGRP, and migraine. Front. Neurol. 2022, 13, 874193. [Google Scholar] [CrossRef]
- Levy, D.; Burstein, R.; Kainz, V.; Jakubovsky, M.; Strassman, A.M. Mast cells degranulation activates a pain pathway underlying migraine headache. Pain 2007, 130, 166–176. [Google Scholar] [CrossRef]
- Meng, J.; Ovsepian, S.V.; Wang, J.; Pickeringg, M.; Sasse, A.; Aoki, K.R.; Lawrence, G.W.; Dolly, J.O. Activation of TRPV1 mediates calcitonin gene-related peptide release, which excites trigeminal sensory neurons and is attenuated by a retargeted botulinum toxin with anti-nociceptive potential. J. Neurosci. 2009, 29, 4981–4992. [Google Scholar] [CrossRef]
- Edvinsson, J.C.A.; Warfringe, K.; Krause, D.N.; Blixt, F.W.; Sheykhzade, M.; Edvinsson, L.; Haanes, K.A. C-fibers may modulate adjacent Aδ-fibers through axon-axon CGRP signaling at nodes of Ranvier in the trigeminal system. J. Headache Pain 2019, 20, 105. [Google Scholar] [CrossRef]
- Messlinger, K.; Balcziak, L.K.; Russo, A.F. Cross-talking signaling in the trigeminal ganglion: Role of neuropeptides and other mediators. J. Neural Transm. 2020, 127, 431–444. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Yamamura, H.; Malick, A.; Strassman, A.M. Chemical stimulation of the intracranial dural induces enhanced responses to facial stimulation in brain stem trigeminal neurons. J. Neurophysiol. 1998, 79, 964–982. [Google Scholar] [CrossRef] [PubMed]
- Strassman, A.M.; Mineta, Y.; Vos, B.P. Distribution of fos-like immunoreactivity in the medullary and upper cervical dorsal horn produced by stimulation of dural blood vessels in the rat. J. Neurosci. 1994, 14, 3725–3735. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Cutrer, M.Y.; Yarnitsky, D. The development of cutaneous allodynia during a migraine attack: Clinical evidence for the sequential recruitment of spinal and supraspinal nociceptive neurons in migraine. Brain 2000, 123, 1703–1709. [Google Scholar] [CrossRef]
- Noseda, R.; Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, CSD, sensitization and modulation of pain. Pain 2013, 154, 1. [Google Scholar] [CrossRef]
- Jakubowski, M.; McAllister, P.J.; Bajwa, Z.H.; Ward, T.N.; Smith, P.; Burstein, R. Exploding vs. imploding headache in migraine prophylaxis with Botulinum Toxin A. Pain 2006, 125, 286–295. [Google Scholar] [CrossRef]
- Kosaras, B.; Jakubowski, M.; Kainz, V.; Burstein, R. Sensory innervation of the calvarial bones of the mouse. J. Compar. Neurol. 2009, 515, 331–348. [Google Scholar] [CrossRef]
- Schueler, M.; Neuhuber, W.L.; De Col, R.; Messlinger, K. Innervation of rat and human dura mater and pericranial tissues in the parieto-temporal region by meningeal afferents. Headache 2014, 54, 996–1009. [Google Scholar] [CrossRef]
- Messlinger, K.; Russo, A.F. Current understanding of trigeminal ganglion structure and function in headache. Cephalalgia 2019, 39, 1661–1674. [Google Scholar] [CrossRef]
- Stovner, L.J.; Hagen, K.; Tronvik, E.; Gravdahl, G.B.; Burstein, R.; Dodick, D.W. FollowTheSutures: Piloting a new way to administer onabotulinumtoxinA for chronic migraine. Cephalalgia 2022, 42, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Blumenfeld, A.M.; Silberstein, S.D.; Manack, A.A.; Brin, M.F. Mechanism of action of OnabtoulinumtoxinA in chronic migraine: A narrative review. Headache 2020, 60, 1259–1272. [Google Scholar] [CrossRef] [PubMed]
- Louveau, A.; Harz, J.; Nordheim Alme, M.; Salvador, A.F.; Dong, M.Q.; Viar, K.E.; Herod, G.; Knopp, J.; Setliff, J.; Lupi, A.L.; et al. CNS lymphatic drainage and neuroinflammation are regulated by meningeal lymphatic vasculature. Nat. Neurosci. 2018, 21, 1380–1391. [Google Scholar] [CrossRef]
- Hamark, C.; Berntsson, R.P.; Masuyer, G.; Gustafsson, R.; Stenmark, P.; Widmalm, G. Glycans confer specificity to the recognition of ganglioside receptors by botulinum neurotoxin. J. Am. Chem. Soc. 2017, 139, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Yeh, F.; Tepp, W.H.; Dean, C.; Johnson, E.A.; Janz, R.; Chapman, E.R. SV2 is the protein receptor for botulinum neurotoxin A. Science 2006, 312, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Jacky, B.P.S.; Garaay, P.E.; Dupuy, J.; Nelson, J.B.; Cai, B.; Molina, Y.; Wang, J.; Steward, L.E.; Broide, R.S.; Francis, J.; et al. Identification of fibroblast growth factor receptor 3 (FGFR3) as a protein receptor for botulinum neurotoxin serotype A (BoNT/A). PLoS Pathog. 2013, 9, e1003369. [Google Scholar] [CrossRef]
- Meng, J.; Wang, J.; Lawrence, G.W.; Dolly, O.J. Molecular components required for resting and stimulated endocytosis of botulinum eurotoxins by glutamatergic and peptidergic neurons. FASEB J. 2013, 27, 3167–3180. [Google Scholar] [CrossRef]
- Li, X.; Coffield, J.A. Structural and functional interactions between transient receptor potential vanilloid subfamily 1 and botulinum neurotoxin serotype A. PLoS ONE 2016, 11, e0143024. [Google Scholar] [CrossRef] [PubMed]
- Muraro, L.; Tosatto, S.; Motterlini, L.; Rossetto, O.; Montecucco, C. The N-terminal half of the receptor domain of botulinum neurotoxin A binds to microdomains of the plasma membrane. Biochem. Biophys. Res. Commun. 2009, 380, 76–80. [Google Scholar] [CrossRef]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum Neurotoxins: Biology, pharmacology, and toxicology. Pharmacaol. Rev. 2017, 69, 200–235. [Google Scholar] [CrossRef]
- Shoemaker, C.B.; Oyler, G.A. Persistence of botulinum neurotoxin inactivation of nerve function. Curr. Top Microbiol. Immunol. 2013, 364, 179–196. [Google Scholar] [PubMed]
- Whitemarsh, R.C.M.; Tepp, W.H.; Johnson, E.A.; Pellett, S. Persistence of botulinum neurotoxin a subtypes 1-5 in primary rat spinal cord cells. PLoS ONE 2014, 9, e90252. [Google Scholar] [CrossRef] [PubMed]
- Belinskaia, M.; Zurawski, T.; Kumar Kaza, S.; Antoniazzi, C.; Dolly, O.J.; Lawrence, G.W. NGF enhances CGRP release evoked by capsaicin from rat trigeminal neurons: Differential inhibitionn by SNAP-25-cleaving proteases. Int. J. Mol. Sci. 2022, 23, 892. [Google Scholar] [CrossRef]
- Neale, E.A.; Bowers, L.M.; Jia, M.; Bateman, K.E.; Williamson, L.C. Botulinum neurotoxin A blocks synaptic vesicle exocytosis but not endocytosis at the nerve terminal. J. Cell Biol. 1999, 147, 1249–1260. [Google Scholar] [CrossRef]
- Melo-Carrillo, A.; Strassman, A.M.; Schain, A.J.; Noseda, R.; Ashina, S.; Adams, A.; Brin, M.F.; Burstein, R. Exploring the effects of extracranial injections of botulinum toxin type A on prolonged intracranial meningeal nociceptors responses to cortical spreading depression in female rats. Cephalalgia 2019, 39, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Zhang, X.C.; Levy, D.; Aoki, K.R.; Brin, M.F. Selective inhibition of meningeal nociceptors by botulinum neurotoxin type A: Therapeutic implications for migraine and other pains. Cephalalgia 2014, 34, 853–869. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.C.; Strassman, A.M.; Novack, V.; Brin, M.F.; Burstein, R. Extracranial injections of botulinum neurotoxin type A inhibit intracranial meningeal nociceptors’ responses to stimulation of TRPV1 and TRPA1 channels: Are we getting closer to solve this puzzle? Cephalalgia 2016, 36, 875–886. [Google Scholar]
- Durham, P.L.; Cady, R.; Cady, R. Regulation of calcitonin gene-related peptide secretion from trigeminal nerve cells by botulinum toxin type A: Implications for migraine therapy. Headache 2004, 44, 35–43. [Google Scholar] [CrossRef]
- Kitamura, Y.; Matsuka, Y.; Spigelman Im Ishihara, Y.; Yamamoto, Y.; Sonoyama, W.; Kamioka, H.; Yamashiro, T.; Ku-boki, T.; Oguma, K. Botulinum toxin type a (150 kDa) decreases exaggerated neurotransmitter release from trigeminal ganglion neurons and relieves neuropathy behaviours induced by infraorbital nerve constriction. Neuroscience 2009, 159, 1422–1429. [Google Scholar] [CrossRef]
- Gazerani, P.; Staahl, C.; Drewes, A.M.; Arendt-Nielsen, L. The effects of Botulinum Toxin type A on capsaicin-evoked pain, flare, and secondary hyperalgesia in an experimental human model of trigeminal sensitization. Pain 2006, 122, 315–325. [Google Scholar] [CrossRef]
- Gazerani, P.; Pedersen, N.S.; Staahl, C.; Drewes, A.M.; Arendt-Nielsen, L. Subcutaneous Botulinum toxin type A reduces capsaicin-induced trigeminal pain and vasomotor reactions in human skin. Pain 2009, 141, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Matak, I.; Bach-Rojecky, L.; Filipović, B.; Lacković, Z. Behavioral and immunohistochemical evidence for central antinociceptive activity of botulinum toxin A. Neuroscience 2011, 186, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Filipovic, B.; Matak, I.; BachRojecky, L.; Lackovic, Z. Central action of peripherally applied botulinum toxin type A on pain and dural protein extravasation in rat model of trigeminal neuropathy. PLoS ONE 2012, 7, e29803. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Xie, N.; Lian, Y.; Xu, H.; Chen, C.; Zheng, Y.; Chen, Y.; Zhang, H. Central antinoniceptive activity of peripherally applied botulinum toxin type A in lab rat model of trigeminal neuralgia. SpringerPlus 2016, 5, 431. [Google Scholar] [CrossRef]
- Restani, L.; Novelli, E.; Bottari, D.; Leone, P.; Barone, I.; Galli-Resta, L.; Strettoi En Caleo, M. Botulinum neurotoxin A impairs neurotransmission following retrograde transynaptic transport. Traffic 2012, 13, 1083–1089. [Google Scholar] [CrossRef]
- Lackovic, Z.; Filipovic, B.; Matak, I.; Helyes, Z. Activity of botulinum toxin type A in cranial dura: Implications from treatment of migraine and other headaches. Br. J. Pharmacol. 2016, 173, 279–291. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; DeGryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F.; PREEMPT 2 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef]
- Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. Onabotuli-numtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef]
- Lipton, R.B.; Varon, S.F.; Grosberg, B.; McAllister, P.J.; Freitag, F.; Aurora, S.K.; Dodick, D.W.; Silberstein, S.D.; Diener, H.C.; DeGryse, R.E.; et al. OnabotulinumtoxinA improves quality of life and reduces impact of chronic migraine. Neurology 2011, 77, 1465–1472. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Blumemfeld, A.M.; Cady, R.K.; Turner, I.M.; Lipton, R.B.; Diener, H.C.; Aurora, S.K.; Sirimanne, M.; DeGryse, R.E.; Turkel, C.C.; et al. OnabotulinumtoxinA for treatment of chronic migraine: PREEMPT 24-week pooled subgroup analysis of patients who had acute headache medication overuse at baseline. J. Neurol. Sci. 2013, 133, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Winner, P.; Freeman, M.C.; Spierings, E.L.; Heiring, J.O.; DeGryse, R.E.; VanDenburgh, A.M.; Nolan, M.E.; Turkel, C.C. OnabotulinumtoxinA for treatment of chronic migraine: Pooled analyses of the 56-week PREEMPT clinical program. Headache 2011, 51, 1358–1373. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Rosen, N.L.; Ailani, J.; DeGryse, R.E.; Gillad, P.J.; Varon, S.F. OnabotulinumtoxinA improves quality of life and reduces impact of chronic migraine over one year of treatment: Pooled results from the PREEMPT random-ized clinical trial program. Cephalalgia 2016, 36, 899–908. [Google Scholar] [CrossRef]
- Matharu, M.; Halker, R.; Pozo-Rosich, P.; Manack, A.A.; Aurora, S.K. The impact of onabotulinumtoxinA on severe headache days: PREEMPT 56-week pooled analysis. J. Headache Pain 2017, 18, 78. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Diener, H.C.; DeGryse, R.E.; Lipton, R.B.; Turkel, C.C. Per cent of patients with chronic migraine who responded per onabotulinumtoxinA treatment cycle: PREEMPT. J. Neurol. Neurosurg. Psychiatry 2015, 86, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Pijpers, J.A.; Kies, D.A.; Louter, M.A.; van Zwet, E.W.; Ferrari, M.D.; Terwindt, G.M. Acute withdrawal and botulinum toxin A in chronic migraine with medication overuse: A double-blind randomized controlled trial. Brain 2019, 142, 1203–1214. [Google Scholar] [CrossRef]
- Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; DeGreyse, R.E.; Adams, A.M.; Diener, H.C. Early onset of effect of OnabotulinumtoxinA for chronic migraine treatment: Analysis of PREEMPT data. Cephalalgia 2019, 39, 945–956. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Diener, H.C.; DeGryse, R.E.; Turkerl, C.C.; Lipton, R.B.; Silberstein, S.D. OnabotulinumtoxinA for chronic migraine: Efficacy, safety, and tolerability in patients who received all five treatment cycles in the PREEMPT clinical program. Acta Neurol. Scand. 2014, 129, 61–70. [Google Scholar] [CrossRef]
- Rothrock, J.F.; Adams, A.M.; Lipton, R.B.; Silberstein, S.D.; JoE; Zhao, X.; Blumenfeld, A.M. FORWARD Study Investigative Group. FORWARD Study: Evaluating the comparative effectiveness of OnabotulinumtoxinA and topiramate for headache prevention in adults with chronic migraine. Headache 2019, 59, 1700–1713. [Google Scholar]
- Blumenfeld, A.M.; Patel, A.T.; Turner, I.M.; Mullin, K.B.; Adams, A.M.; Rothrock, J.F. Patient-reported outcomes from a 1-year, real-world, head-to-head comparison of OnabotulinumtoxinA and topiramate for headache prevention in adults with chronic migraine. J. Prim. Care Community Health 2020, 11, 2150132720959936. [Google Scholar] [CrossRef]
- Khalil, M.; Zafar, H.W.; Quarshie, V.; Ahmed, F. Prospective analysis of the use of OnabotulinumtoxinA (BOTOX) in the treatment of chronic migraine; real-life data in 254 patients from Hull, UK. J. Headache Pain 2014, 15, 54. [Google Scholar] [CrossRef] [PubMed]
- Pedraza, M.I.; de la Cruz, C.; Ruiz, M.; Lopez-Mesonero, L.; Martinez, E.; de Lera, M.; Guerrero, A.L. OnobatulinumtoxinA treatment of chronic migraine: Experience in 52 patients treated with the PREEMPT paradigm. SpringerPlus 2015, 4, 176. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Zafar, H.W.; Buture, A.; Khalil, M. Does analgesic overuse matter? Response to OnabotulinumtoxinA in patients with chronic migraine with or without medication overuse. SpringerPlus 2015, 4, 589. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cernuda-Morollon, E.; Ramon, C.; Larrosa, D.; Alvarez, R.; Riesco, N.; Pascual, J. Long-term experience with onabotulinumtoxinA in the treatment of chronic migraine: What happens after one year? Cephalalgia 2015, 35, 864–868. [Google Scholar] [CrossRef] [PubMed]
- Maasumi, K.; Thompson, N.R.; Kriegler, J.S.; Tepper, S.J. Effect of onabotulinumtoxinA injection on depression in chronic migraine. Headache 2015, 55, 1218–1224. [Google Scholar] [CrossRef] [PubMed]
- Negro, A.; Curto, M.; Lionetto, L.; Crialesi, D.; Martelletti, P. OnabotulinumtoxinA 155 U in medication overuse headache: A two years prospective study. SpringerPlus 2015, 4, 826. [Google Scholar] [CrossRef] [PubMed]
- Guerzoni, S.; Pellesi, L.; Baraldi, C.; Pini, L.A. Increased efficacy of regularly repeated cycles with OnabotulinumtoxinA in MOH patients beyond the first year of treatment. J. Headache Pain 2016, 17, 48. [Google Scholar] [CrossRef]
- Vikelis, M.; Argyruou, A.A.; Dermitzakis, E.V.; Spingos, K.C.; Mitsikostas, D.D. Onabotulinumtoxin-A treatment in Greek patients with chronic migraine. J. Headache Pain 2016, 17, 84. [Google Scholar] [CrossRef]
- Aicua-Rapun, I.; Martìnez-Velasco, E.; Rojo, A.; Hernando, A.; Ruiz, M.; Carreres, A.; Porqueres Em Herrero, S.; Iglesias, F.; Guerrero, A.L. Real-life data in 115 chronic migraine patients treated with OnabotulinumtoxinA during more than one year. J. Headache Pain 2016, 17, 112. [Google Scholar] [CrossRef]
- Russo, M.; Manzoni, G.C.; Taga, A.; Genovese, A.; Veronesi, L.; Paquarella, C.; Sansebastiano, G.E.; Torelli, P. The use of onabotulinum toxin A (Botox®) in the treatment of chronic migraine at the Parma Headache Centre: A prospective observational study. Neurol. Sci. 2016, 37, 1127–1131. [Google Scholar] [CrossRef]
- Demiryurek, B.E.; Ertem, D.H.; Tekin, A.; Ceylan, M.; Aras, Y.G.; Gungen, B.D. Effects of onabotulinumtoxinA treatment on efficacy, depression, anxiety, and disability in Turkish patients with chronic migraine. Neurol. Sci. 2016, 37, 1779–1784. [Google Scholar] [CrossRef] [PubMed]
- Negro, A.; Curto, M.; Lionetto, L.; Martelletti, P. A two years open-label prospective study of OnabotulinumtoxinA 195 U in medication overuse headache: A real-world experience. J. Headache Pain 2015, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Aydinlar, E.I.; Dikmen, P.Y.; Kosak, S.; Kocaman, A.S. OnabotulinumtoxinA effectiveness on chronic migraine, negative emotional states and sleep quality: A single-center prospective cohort study. J. Headache Pain 2017, 18, 23. [Google Scholar] [CrossRef] [PubMed]
- Matharu, M.; Pascual, J.; Nilsson Remahl, I.; Straube, A.; Lum, A.; Davar, G.; Odom, D.; Bennett, L.; Proctor, C.; Gutierrez, L.; et al. Utilization and safety of onabotulinumtoxinA for the prophylactic treatment of chronic migraine from an observational study in Europe. Cephalalgia 2017, 37, 1384–1397. [Google Scholar] [CrossRef]
- Byun, J.I.; Sim, J.Y.; Kim, M. Prolonged effect of OnabotulinumtoxinA on chronic migraine in 87 koreans. J. Clin. Neurol. 2017, 13, 98–100. [Google Scholar] [CrossRef]
- Guerzoni, S.; Pellesi, L.; Baraldi, C.; Cainazzo, M.M.; Negro, A.; Martelletti, P.; Pini, L.A. Long-term treatment benefits and prolonged efficacy of OnabotulinumtoxinA in patients affected by chronic migraine and medication overuse headache over 3 years of therapy. Front. Neurol. 2017, 8, 586. [Google Scholar] [CrossRef]
- Dikmen, P.Y.; Kosak, S.; Aydinlar, E.I.; Kocaman, A.S. A single-center retrospective study of onabotulinumtoxinA for treatment of 245 chronic migraine patients: Survey results of a real-world experience. Acta Neur. Belg. 2018, 118, 475–484. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.; Stark, R.J.; Freeman, M.C.; Orejudos, A.; Manack, A.A. Long-term study of the efficacy and safety of OnabotulinumtoxinA for the prevention of chronic migraine: COMPEL study. J. Headache Pain 2018, 19, 13. [Google Scholar] [CrossRef]
- Domínguez, C.; Pozo-Rosich, P.; Torres-Ferrús, M.; Hernández-Beltrán, N.; Jurado-Cobo, C.; González-Oria, C.; Santos, S.; Monzón, M.J.; Latorre, G.; Álvaro, L.C.; et al. OnabotulinumtoxinA in chronic migraine: Predictors of response. A prospective multicentre descriptive study. Eur. J. Neurol. 2018, 25, 411–416. [Google Scholar] [CrossRef]
- Vikelis, M.; Argryriou, A.A.; Dermitzakis, E.V.; Spingos, K.C.; Makris, N.; Kararizou, E. Sustained onabotulinumtoxinA therapeutic benefits in patients with chronic migraine over 3 years of treatment. J. Headache Pain 2018, 19, 87. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.; Tepper, S.J.; Robbins, L.D.; Manack, A.A.; Buse, D.C.; Orejudos, A.; Silberstein, S. Effects of onabotulinumtoxinA treatment for chronic migraine on common comorbidities including depression and anxiety. J. Neurol. Neurosurg. Psychiatry 2019, 90, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Andreou, A.P.; Trimboli, M.; Al-Kaisy, A.; Murphy, M.; Palmisani, S.; Fenech, C.; Smith, T.; Lambru, G. Prospective real-world analysis of OnabotulinumtoxinA in chronic migraine post-National Institute for Health and Care Excellence UK technology appraisal. Eur. J. Neurol. 2018, 25, 1069–1083. [Google Scholar] [CrossRef]
- Caronna, E.; Gallardo, V.J.; Hernandez-Beltran, N.; Torres-Ferrus, M.; Pozo-Rosich, P. OnabotulinumtoxinA: An effective tool in the therapeutic arsenal for chronic migraine with medication overuse. Front. Neurol. 2018, 9, 808. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Gaul, C.; García-Moncó, J.C.; Sommer, K.; Martelletti, P. REPOSE Principal Investigators. An open-label prospective study of the real-life use of onabotulinumtoxinA for the treatment of chronic migraine: The REPOSE study. J. Headache Pain 2019, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Quintas, S.; Garcia-Azorin, D.; Heredia, P.; Talavera, B.; Gago-Viega, A.B.; Guerrero, A.L. Wearing off response to OnabotulinumtoxinA in chronic migraine: Analysis in a series of 193 patients. Pain Med. 2019, 20, 1815–1821. [Google Scholar] [CrossRef] [PubMed]
- Ching, J.; Tinsley, A.; Rothrock, J. Prognosis following discontinuation of OnabotulinumA therapy in “super-responding” chronic migraine patients. Headache 2018, 59, 1279–1285. [Google Scholar] [CrossRef]
- Alpuente, A.; Gallardo, V.J.; Torres-Ferrus, M.; Alvarez-Sabin, J.; Pozo-Rosich, P. Early efficacy and late gain in chronic and high frequency episodic migraine with onabotulinumtoxinA. Eur. J. Neurol. 2019, 26, 1464–1470. [Google Scholar] [CrossRef]
- Davies, B.; Gaul, C.; Martelletti, P.; Garcia-Moncò, J.C.; Brown, S. Real-life use of onabotulinumtoxinA for symptom relief in patients with chronic migraine: REPOSE study methodology and baseline data. J. Headache Pain 2017, 18, 93. [Google Scholar] [CrossRef][Green Version]
- Santoro, A.; Copetti, M.; Miscio, A.M.; Leone, M.A.; Fontana, A. Chronic migraine long-term regular treatment with onabotulinumtoxinA: A retrospective real-life observational study up to 4 years of therapy. Neurol. Sci. 2020, 41, 1809–1820. [Google Scholar] [CrossRef]
- Stark, C.; Stark, R.; Limber, N.; Rodrigues, J.; Cordato, D.; Schwartz, R.; Jukic, R. Real-world effectiveness of onabotulinumtoxinA treatment for the prevention of headaches in adults with chronic migraine in Australia: A retrospective study. J. Headache Pain 2019, 20, 81. [Google Scholar] [CrossRef]
- De Tommaso, M.; Brighina, F.; Delussi, M. Effect of Botulinum Toxin A on allodynia in chronic migraine: An observational open-label two-years study. Eur. Neurol. 2019, 81, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Young, W.B.; Lopez, J.I.; Rothrock, J.F.; Orejundos, A.; Manack, A.A.; Lipton, R.B.; Blumenfeld, A.M. Effects of onabotulinumtoxinA treatment in patients with and without allodynia: Results of the COMPEL study. J. Headache Pain 2019, 20, 10. [Google Scholar] [CrossRef] [PubMed]
- Ornello, R.; Guerzoni, S.; Baraldi, C.; Evangelista, L.; Frattale, I.; Marini, C.; Tiseo, C.; Pistoia, F.; Sacco, S. Sustained response to onabotulinumtoxin A in patients with chronic migraine: Real-life data. J. Headache Pain 2020, 21, 40. [Google Scholar] [CrossRef] [PubMed]
- Young, W.B.; Lopez, J.I.; Rothrock, J.F.; Orejudos, A.; Manack, A.A.; Lipton, R.B.; Blumenfeld, A.M. Effects of onabotulinumtoxinA treatment in chronic migraine patients with and without daily headache at baseline: Results from the COMPEL Study. J. Headache Pain 2019, 20, 12. [Google Scholar] [CrossRef]
- Barad, M.; Sturgeon, J.A.; Fish, S.; Dexter, F.; Mackey, S.; Flood, P.D. Response to BotulinumtoxinA in a migraine cohort with multiple comorbidities and widespread pain. Reg. Anesth. Pain Med. 2019, 44, 660–668. [Google Scholar] [CrossRef]
- Diener, H.C.; Dodick, D.W.; Turkel, C.C.; Demos, G.; Degryse, R.E.; Earl, N.L.; Brin, M.F. Pooled analysis of the safety and tolerability of onabotulinumtoxinA in the treatment of chronic migraine. Eur. J. Neurol. 2014, 21, 851–859. [Google Scholar] [CrossRef]
- Winner, P.K.; Blumenfeld, A.M.; Eross, E.J.; Orejudos, A.C.; Mirjah, D.L.; Manack, A.A.; Brin, M.F. Long-term safety and tolerability of OnabotulinumtoxinA treatment in patients with chronic migraine: Results of the COMPEL study. Drug Saf. 2019, 42, 1013–1024. [Google Scholar] [CrossRef]
- Hepp, Z.; Rosen, N.L.; Gillard, P.G.; Varon, S.F.; Mathew, N.; Dodick, D.W. Comparative effectiveness of onabotulinumtoxinA versus oral migraine prophylactic medications on headache-related resource utilization in the management of chronic migraine: Retrospective analysis of a US-based insurance claims database. Cephalalgia 2016, 36, 862–874. [Google Scholar] [CrossRef]
- Rothrock, J.F.; Bloudek, L.M.; Houle, T.T.; Rothrpck, D.A.; Varon, S.F. Real-world economic impact of OnabotulinumtoxinA in patients with chronic migraine. Headache 2014, 54, 1565–1573. [Google Scholar] [CrossRef]
- Vernieri, F.; Paolucci, M.; Altamura, C.; Pasqualetti, P.; Mastrangelo, V.; Pierangeli, G.; Cevoli, S.; D’Amico, D.; Grazzi, L. Onabotulinumtoxin-A in chronic migraine: Should timing and definition of non-responder status be revised? Suggestions from a real-life Italian multicenter experience. Headache 2019, 59, 1300–1309. [Google Scholar] [CrossRef]
- Masters-Israilov, A.; Robbins, M.S. OnabotulinumtoxinA wear-off phenomenon in the treatment of chronic migraine. Headache 2019, 59, 1753–1761. [Google Scholar] [CrossRef]
- Ruscheweyh, R.; Athwal, B.; Gryglas-Dworak, A.; Frattale, I.; Latysheva, N.; Ornello, R.; Pozo-Rosich, P.; Sacco, S.; Torres-Ferrus, M.; Stark, C.D. Wear-off of OnabotulinumtoxinA effect over the treatment interval in chronic migraine: A retrospective chart review with analysis of headache diaries. Headache 2020, 60, 1673–1682. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, C.; Ornello, R.; Favoni, V.; Sacco, S.; Cponnetto, V.; Pierangeli, G.; Cevoli, S.; Guerzoni, S. Chroni migraine and medication overuse headache worsening after OnabotulinumtoxinA withdrawn due to the severe acute respiratory syndrome-coronavirus-2 pandemic. Front. Neurol. 2021, 12, 647995. [Google Scholar] [CrossRef] [PubMed]
- Ornello, R.; Ahmed, F.; BNegro, A.; Miscio, A.M.; Santoro, A.; Alpuente, A.; Russo, A.; Silvestro, M.; Cevoli, S.; Brunelli, N.; et al. Early management of OnabotulinumtoxinA treatment in chronic migraine: Insights from a real-life European multicenter study. Pain Ther. 2021, 10, 637–650. [Google Scholar] [CrossRef]
- Ornello, R.; Ahmed, F.; BNegro, A.; Miscio, A.M.; Santoro, A.; Alpuente, A.; Russo, A.; Silvestro, M.; Cevoli, S.; Brunelli, N.; et al. Is there a gender difference in the response to onabotulinumtoxinA ion chronic migraine? Insights from a real-life European multicenter study on 2879 patients. Pain Ther. 2021, 10, 1605–1618. [Google Scholar] [CrossRef] [PubMed]
- Ornello, R.; Baraldi, C.; Ahmed, F.; Negro, A.; Miscio, A.M.; Santoro, A.; Alpuente, A.; Russo, A.; Silvestro, M.; Cevoli, S.; et al. Excellent response to OnabotulinumtoxinA: Different definitions, different predictors. Int. J. Environ. Res. Public Health 2022, 19, 10975. [Google Scholar] [CrossRef]
- Altamura, C.; Ornello, R.; Ahmed, F.; Negro, A.; Miscio, A.M.; Santoro, A.; Alpuente, A.; Russo, A.; Silvestro, M.; Cevoli, S.; et al. OnabotulinumtoxinA in elderly patients with chronic migraine: Insights from a real-life European multicenter study. J. Neurol. 2022. [Google Scholar] [CrossRef]
- Kara, M.; Sekizkardes, M.; Gürçay, E.; Akinci, A.; Özçakar, L. Ultrasound-guided perisutural botulinum toxin injection for chronic migraine headache. Initial report with technical description. Am. J. Phys. Med. Rehab. 2019, 98, e98–e100. [Google Scholar] [CrossRef]
- Kara, M.; Erdam, Y.S.; Doğan, Y.; Erdal, O.D.; D’Amico, V.; Özçakar, L. The chronicle of headache treatment throught human history from trepanation to perisutural botulinum toxin injections. Int. J. Neurosci. 2022, 1–4. [Google Scholar] [CrossRef]
- Murat, K.; Gürcay, E.; Gülümser, A.; Kaymak, B.; Sekizkardes, M.; Akinci, A.; Uludüz, D.; Özçakar, L. Botulinum toxin injections to cranial sutures for chronic migraine revwinding the technique using ultrasound imaging. Toxicon 2019, 172, 19–22. [Google Scholar]
- Kara, M.; Sekizkardes, K.M.; Özçakar, L. The effects/injections of botulinum toxin in chronic migraine headache. Acta Neurol. Scand. 2018, 138, 99. [Google Scholar] [CrossRef] [PubMed]
- De Matteis, E.; Guglielmetti, M.; Ornello, R.; Spuntarelli, V.; Martelletti, P.; Sacco, S. Targeting CGRP for migraine treatment: Mechanisms, antibodies, small molecules, perspectives. Expert. Rev. Neurother. 2020, 20, 627–641. [Google Scholar] [CrossRef]
- Ondo, W.G.; Simmons, J.H.; Shahid, M.H.; Hashem, V.; Hunter, C.; Jankovic, J. Onabotulinum toxin-A injections for sleep bruxism: A double-blind, placebo-controlled study. Neurology 2018, 90, e559–e564. [Google Scholar] [CrossRef] [PubMed]
- Guerzoni, S.; Baraldi, C.; Pani, L. The association between onabotulinumtoxinA and anti-CGRP monoclonal antibodies: A reliable option for the optimal treatment of chronic migraine. Neurol. Sci. 2022, 43, 5687–5695. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).