Soy Protein-Based Infant Formulas with Supplemental Fructooligosaccharides: Gastrointestinal Tolerance and Hydration Status in Newborn Infants

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Subjects
2.2. Study Formulas

{kind=link}
{kind=link}
| Nutrients | CF | EF1 | EF2 |
|---|---|---|---|
| Supplemental scFOS, g/L | 0 | 2.5 | 2.5 |
| Carbohydrate blend, % | 20% sucrose | 20% sucrose | 0% sucrose |
| 80% corn syrup solids | 80% corn syrup solids | 100% corn syrup solids | |
| Supplemental Mixed Carotenoids (MC) * | None | Yes | Yes |
2.3. Study Procedures
2.4. Statistical Methods
3. Results
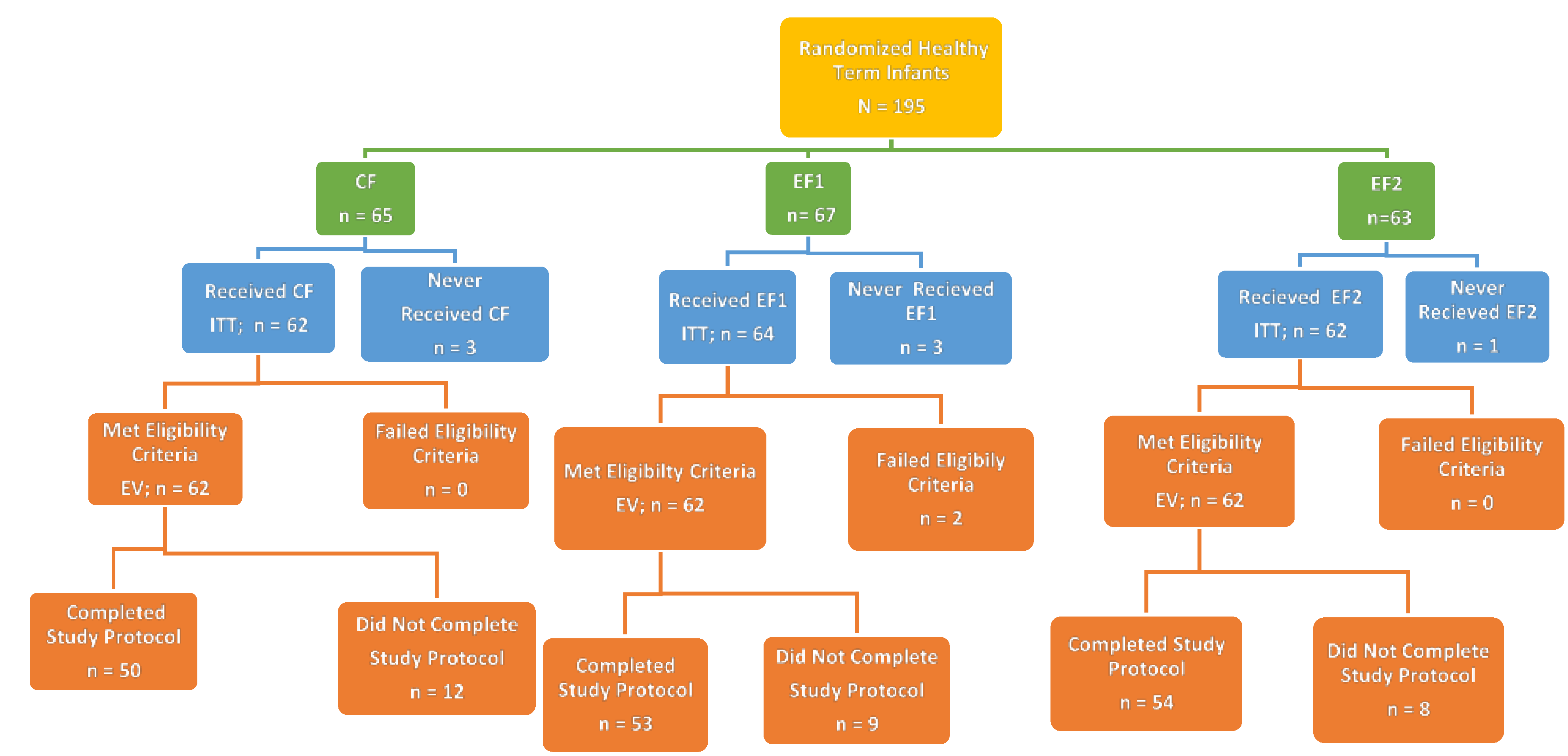
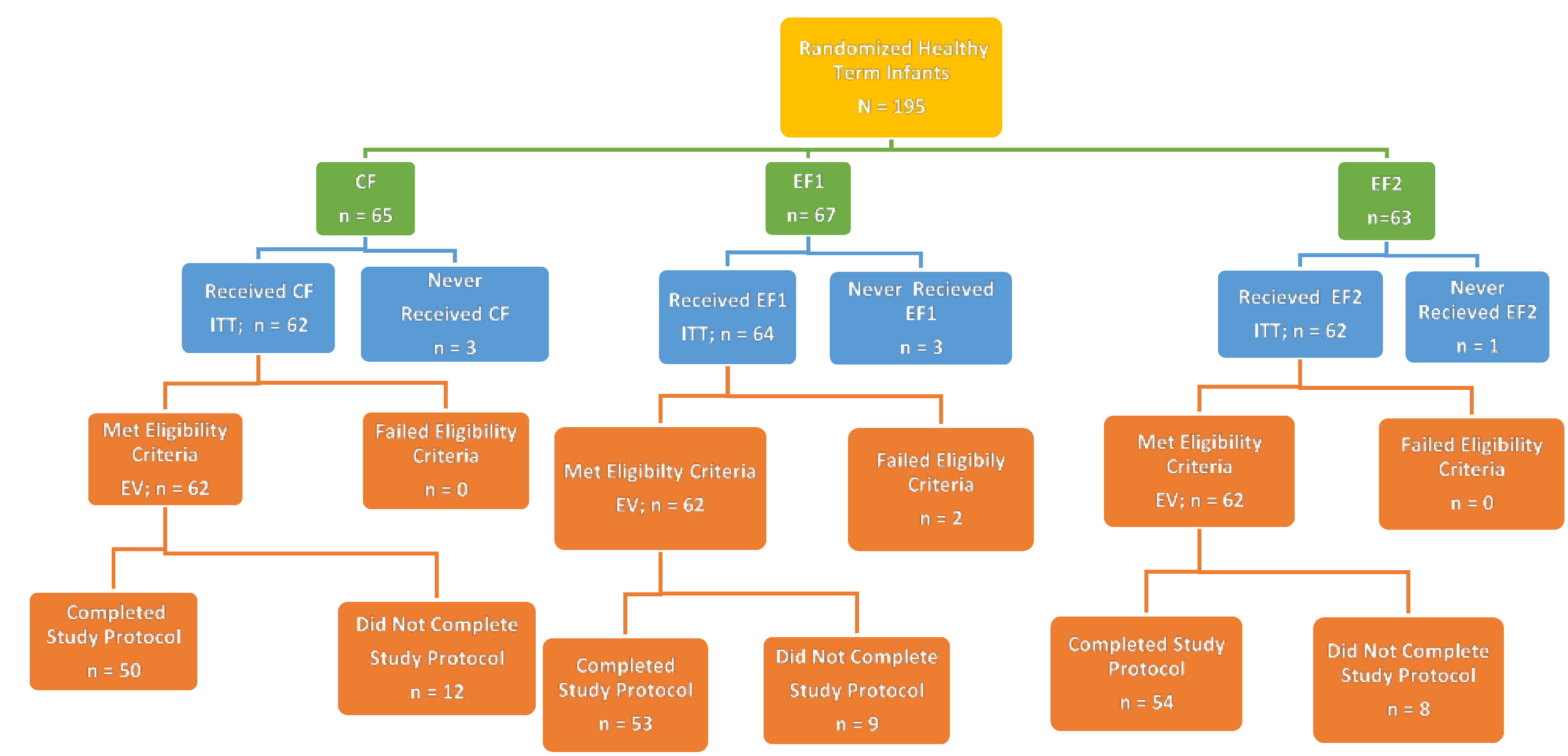
3.1. Disposition, Demographic and Anthropometry Measures among Study Subjects
| Variables | Treatment Groups | ||
|---|---|---|---|
| CF | EF1 | EF2 | |
| Gender | |||
| Male/Female, n (%) | 33/32 (51/49) | 32/35 (48/52) | 30/33 (48/52) |
| Race, n (%) | |||
| White | 42 (65) | 45 (67) | 37 (59) |
| Black | 15 (23) | 12 (18) | 23 (37) |
| Asian | 0 (0) | 1 (1) | 0 (0) |
| Pacific Islander | 0 (0) | 1 (1) | 0 (0) |
| White/Hispanic | 0 (0) | 1 (1) | 0 (0) |
| White/Black | 7 (11) | 6 (9) | 3 (5) |
| White/Asian | 0 (0) | 1 (1) | 0 (0) |
| Black/Asian | 1 (2) | 0 (0) | 0 (0) |
| Gestational Age, weeks * | 39.1 ± 0.1 (65) | 38.9 ± 0.1 (67) | 38.9 ± 0.1 (62) |
| Mode of Delivery ** | |||
| Vaginal/C-Section, n (%) | 42/20 (68/32) | 54/10 (84/16) | 40/22 (65/35) |
| Age at Enrollment, days | 5.3 ± 0.2 (65) | 4.7 ± 0.2 (67) | 5.3 ± 0.2 (63) |
| Birth Weight, g | 3382 ± 57 (65) | 3345 ± 52 (67) | 3211 ± 51 (63) |
| Birth Length, cm ‡ | 50.3 ± 0.3 (65) | 50.5 ± 0.3 (67) | 49.8 ± 0.2 (63) |
| Birth Head Circumference, cm | 33.8 ± 0.4 (35) | 34.0 ± 0.3 (48) | 33.9 ± 0.2 (39) |
| Study Variables | Treatment Groups | ||
|---|---|---|---|
| CF | EF1 | EF2 | |
| Weight | |||
| Day 1, g | 3297 ± 58 (62) | 3318 ± 49 (62) | 3150 ± 48 (62) |
| Day 1, percentile | 32.4 ± 3.0 (62) | 33.4 ± 2.8 (62) | 24.3 ± 2.4 (62) |
| Day 35, g | 4307 ± 73 (37) | 4302 ± 72 (39) | 4190 ± 70 (44) |
| Day 35, percentile | 43.3 ± 3.4 (37) | 44.7 ± 3.6 (39) | 36.2 ± 3.5 (44) |
| Weight gain, g/day | |||
| Days 1–35 | 35.8 ± 1.9 (37) | 34.0 ± 1.7 (39) | 35.3 ± 1.6 (44) |
| Length gain, cm/day | |||
| Days 1–35 | 0.14 ± 0.01 (37) | 0.14 ± 0.01 (39) | 0.14 ± 0.01 (44) |
| Head circumference gain, cm/day | |||
| Days 1–35 | 0.09 ± 0.00 (37) | 0.10 ± 0.01 (39) | 0.09 ± 0.00 (44) |
| Intent-to-Treat (ITT) Group | |||
| Weight | |||
| Day 1, g | 3297 ± 58 (62) | 3311 ± 50 (64) | 3150 ± 48 (62) |
| Day 1, percentile | 32.4 ± 3.0 (62) | 33.2 ± 2.8 (64) | 24.3 ± 2.4 (62) |
| Day 35, g | 4339 ± 68 (50) | 4373 ± 66 (54) | 4213 ± 60 (54) |
| Day 35, percentile | 44.1 ± 3.3 (50) | 46.6 ± 3.3 (54) | 37.5 ± 3.1 (54) |
| Weight gain, g/day | |||
| Days 1–35 | 35.1 ± 1.6 (50) | 34.7 ± 1.4 (54) | 35.6 ± 1.4 (54) |
| Length gain, cm/day | |||
| Days 1–35 | 0.13 ± 0.01 (49) | 0.15 ± 0.01 (54) | 0.14 ± 0.01 (54) |
| Head circumference gain, cm/day | |||
| Days 1–35 | 0.09 ± 0.00 (50) | 0.10 ± 0.01 (54) | 0.10 ± 0.00 (54) |
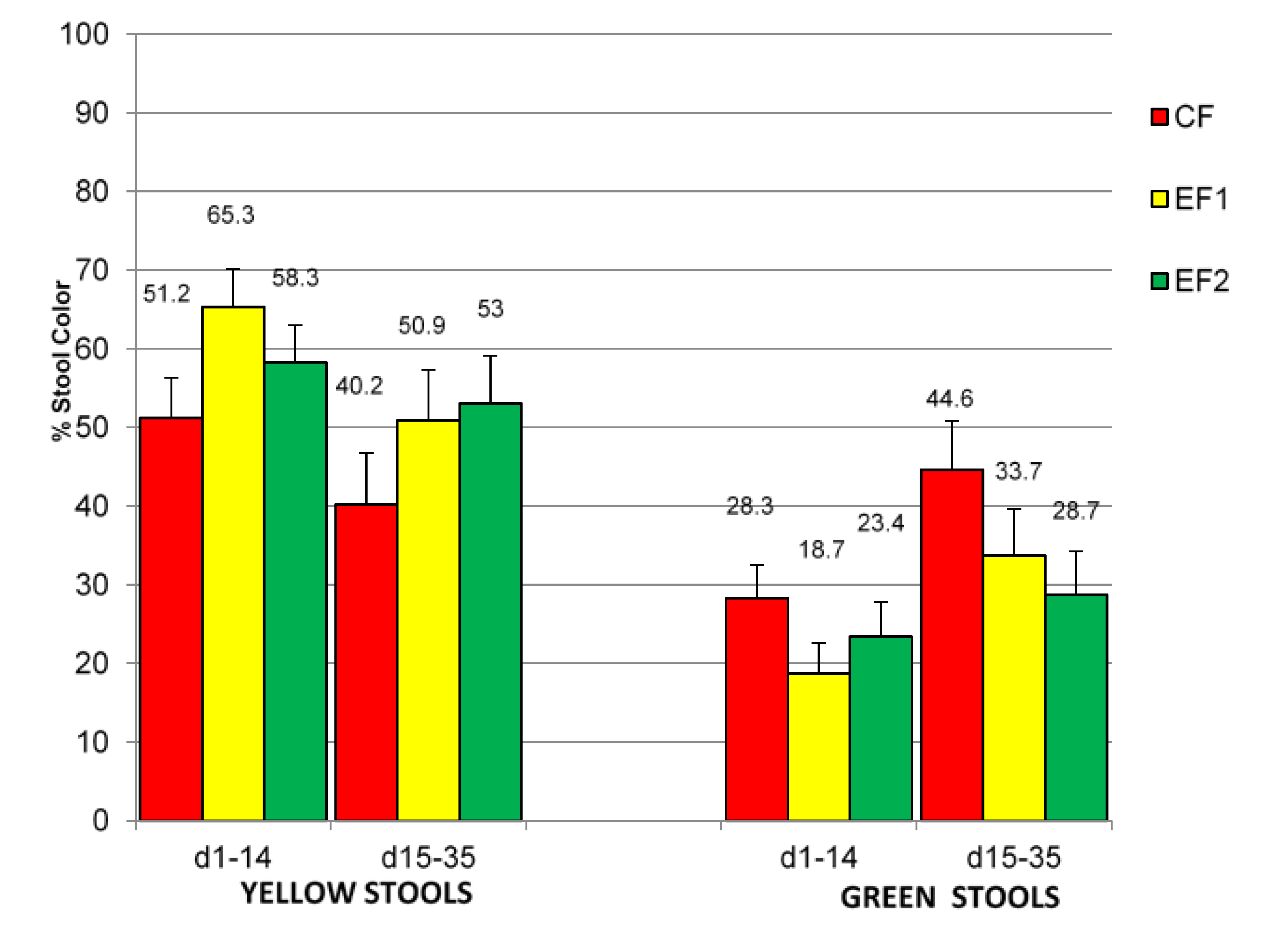
3.2. Stool and Gastrointestinal Tolerance and Formula Acceptability
| Study Variables | Treatment Groups | ||
|---|---|---|---|
| CF | EF1 | EF2 | |
| Mean Rank Stool Consistency Score ** (Primary Study Variable) | |||
| Days 1–14 | 2.5 ± 0.1 (51) | 2.6 ± 0.1 (57) | 2.5 ± 0.1 (57) |
| Days 15–35 | 2.6 ± 0.1 (40) | 2.7 ± 0.1 (41) | 2.5 ± 0.1 (46) |
| Stool Frequency, # stools/day | |||
| Days 1–14 | 2.9 ± 0.3 (48) | 3.3 ± 0.3 (55) | 3.1 ± 0.3 (56) |
| Days 15–35 | 2.1 ± 0.2 (40) | 2.7 ± 0.3 (41) | 2.7 ± 0.3 (46) |
| Percent Watery Stools, % | |||
| Days 1–14 | 11.3 ± 2.6 (51) | 16.3 ± 3.4 (57) | 12.7 ± 2.8 (57) |
| Days 15–35 | 8.9 ± 2.0 (40) | 11.4 ± 3.4 (41) | 13.3 ± 3.4 (46) |
| Percent Loose/Mushy Stools, % | |||
| Days 1–14 | 47.7 ± 4.7 (51) | 32.9 ± 3.9 (57) | 39.5 ± 3.7 (57) |
| Days 15–35 | 40.4 ± 5.5 (40) | 31.7 ± 4.5 (41) | 41.0 ± 4.7 (46) |
| Percent Soft Stools, % | |||
| Days 1–14 | 26.7 ± 3.7 (51) | 34.8 ± 3.9 (57) | 37.5 ± 4.1 (57) |
| Days 15–35 | 35.3 ± 5.1 (40) | 40.1 ± 4.3 (41) | 30.3 ± 4.6 (46) |
| Percent Formed Stools, % | |||
| Days 1–14 | 10.8 ± 3.0 (51) | 10.4 ± 1.9 (57) | 9.0 ± 2.3 (57) |
| Days 15–35 | 11.4 ± 2.8 (40) | 15.5 ± 2.9 (41) | 12.6 ± 2.9 (46) |
| Percent Hard Stools, % ‡ | |||
| Days 1–14 | 3.5 ± 1.7 (51) | 5.6 ± 2.5 (57) | 1.3 ± 0.9 (57) |
| Days 15–35 | 4.0 ± 2.2 (40) | 1.4 ± 0.6 (41) | 2.8 ± 1.4 (46) |

| Study Variables | Treatment Groups | ||
|---|---|---|---|
| CF | EF1 | EF2 | |
| Average Numbers of Feedings, #/day ** | |||
| Days 1–14 | 7.6 ± 0.2 (47) | 7.1 ± 0.2 (56) | 7.9 ± 0.2 (56) |
| Days 15–35 | 7.1 ± 0.2 (40) | 7.1 ± 0.2 (40) | 7.5 ± 0.3 (47) |
| Average Formula Intake, mL/day | |||
| Days 1–14 | 555 ± 17 (47) | 559 ± 20 (56) | 570 ± 20 (56) |
| Days 15–35 | 673 ± 22 (40) | 739 ± 26 (40) | 726 ± 35 (47) |
| Spit-up/Vomit, % of feedings | |||
| Days 1–14 | 22.4 ± 4.0 (52) | 23.5 ± 3.8 (58) | 23.2 ± 3.9 (59) |
| Days 15–35 | 17.4 ± 4.1 (40) | 17.8 ± 4.1 (40) | 17.5 ± 3.6 (47) |
3.3. Safety Measures
| Treatment Groups | |||
|---|---|---|---|
| CF | EF1 | EF2 | |
| Day 14 | |||
| 1.0041 ± 0.0005 (40) | 1.0038 ± 0.0004 (42) | 1.0044 ± 0.0009 (47) |
| None | None | 1 (2) |
| Day 35 | |||
| 1.0043 ± 0.0004 (35) | 1.0034 ± 0.0003 (38) | 1.0039 ± 0.0004 (43) |
| None | None | None |
| Serious Adverse Events (SAEs) | |||
| Total Number of Subjects | (N = 62) | (N = 64) | (N = 62) |
| Subjects with SAEs, n (%) | 2 (3.2) | 2 (3.1) | 2 (3.2) |
| SAE Complaint/Diagnosis | Respiratory syncytial virus Bronchiolitis Pyrexia | Streptococcal sepsis Urinary tract infection | Meningitis enterovirus Vomiting |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Academy of Pediatrics Committee on Nutrition. Formula feeding of term infants. In Pediatric Nutrition, 7th ed.; Kleinman, R.E., Greer, F.R., Eds.; American Academy of Pediatrics: Elk Grove Village, IL, USA, 2014; pp. 61–81. [Google Scholar]
- Vandenplas, Y.; Castrellon, P.; Rivas, R.; Gutiérrez, C.; Garcia, L.; Jimenez, J.; Anzo, A.; Hegar, B.; Alarcon, P. Safety of soya-based infant formulas in children. Br. J. Nutr. 2014, 111, 1340–1360. [Google Scholar] [CrossRef] [PubMed]
- Lasekan, J.; Ostrom, K.; Jacobs, J.; Blatter, M.; Ndife, L.; Gooch, W., 3rd; Cho, S. Growth of newborn, term infants fed soy formulas for one year. Clin. Pediatr. 1999, 38, 563–571. [Google Scholar] [CrossRef]
- Hyams, J.S.; Treem, W.R.; Etienne, N.L.; Weinerman, H.; MacGilpin, D.; Hine, P.; Choy, K.; Burke, G. Effect of infant formula on stool characteristics of young infants. Pediatrics 1995, 95, 50–54. [Google Scholar] [PubMed]
- Berseth, C.L.; Johnston, W.H.; Stolz, S.I.; Harris, C.L.; Mitmesser, S.H. Clinical response to 2 commonly used switch formulas occurs within 1 day. Clin. Pediatr. 2009, 48, 58–65. [Google Scholar] [CrossRef]
- Vanderhoof, J.A.; Murray, N.D.; Paule, C.L.; Ostrom, K.M. Use of soy fiber in acute diarrhea in infants and toddlers. Clin. Pediatr. 1997, 36, 135–139. [Google Scholar] [CrossRef]
- Roberfroid, M. Prebiotics: The concept revisited. J. Nutr. 2007, 137, 830S–837S. [Google Scholar] [PubMed]
- Moore, N.; Chao, C.; Yang, L.; Storm, H.; Oliva-Hemker, M.; Saavedra, J.M. Effects of fructo-oligosaccharide-supplemented infant cereal: A double-blind, randomized trial. Br. J. Nutr. 2003, 90, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Euler, A.; Mitchell, D.; Kline, R.; Pickering, L. Prebiotic effect of fructo-oligosaccharide supplemented term infant formula at two concentrations compared with unsupplemented formula and human milk. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Moro, G.; Minoli, I.; Mosca, M.; Fanaro, S.; Jelinek, J.; Stahl, B.; Boehm, G. Dosage-related bifidogenic effects of galacto- and fructooligosaccharides in formula-fed term infants. J. Pediatr. Gastroenterol. Nutr. 2002, 34, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Boehm, G.; Lidestri, M.; Casetta, P.; Jelinek, J.; Negretti, F.; Stahl, B.; Marini, A. Supplementation of a bovine milk formula with an oligosaccharide mixture increases counts of faecal bifidobacteria in preterm infants. Arch. Dis. Child Fetal Neonatal Ed. 2002, 86, F178–F181. [Google Scholar] [CrossRef] [PubMed]
- Ben, X.; Zhou, X.; Zhao, W.; Yu, W.; Pan, W.; Zhang, W.; Wu, S.; Van Beusekom, C.; Schaafsma, A. Supplementation of milk formula with galacto-oligosaccharides improves intestinal micro-flora and fermentation in term infants. Chin. Med. J. 2004, 117, 927–931. [Google Scholar] [PubMed]
- Fanaro, S.; Boehm, G.; Garssen, J.; Knol, J.; Mosca, F.; Stahl, B.; Vigi, V. Galacto-oligosaccharides and long-chain fructo-oligosaccharides as prebiotics in infant formulas: A review. Acta Paediatr. Suppl. 2005, 94, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Paineau, D.; Respondek, F.; Menet, V.; Sauvage, R.; Bornet, F.; Wagner, A. Effects of short-chain fructooligosaccharides on faecal bifidobacteria and specific immune response in formula-fed term infants: A randomized, double-blind, placebo-controlled trial. J. Nutr. Sci. Vitaminol. 2014, 60, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Litov, R.; Moore, N.; Sun, S. Evaluation of prebiotic tolerance in pre-weaning infants. J. Pediatr. Gastroenterol. Nutr. 2006, 43, E64, (Abstract). [Google Scholar] [CrossRef]
- European Food Safety Authority, EFSA. Opinion of the scientific panel on dietetic products, nutrition and allergies on a request from the commission relating to the safety and suitability for the particular nutritional use by infants of fructooligosaccharides in infant formulae and follow-on formulae. EFSA J. 2004, 31, 1–11. [Google Scholar]
- Barr, R.G.; Young, S.N.; Wright, J.H.; Gravel, R.; Alkawaf, R. Differential calming responses to sucrose taste in crying infants with and without colic. Pediatrics 1999, 103, e68. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.; Beggs, S.; Stevens, B. Sucrose for procedural pain management in infants. Pediatrics 2012, 130, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Mares-Perlman, J.; Millen, A.; Ficek, T.; Hankinson, S. The body of evidence to support a protective role for lutein and zeaxanthin in delaying chronic disease: Overview. J. Nutr. 2002, 132, 518–524. [Google Scholar]
- Chew, B.; Park, J. Carotenoid action on the immune response. J. Nutr. 2004, 134, 257S–261S. [Google Scholar] [PubMed]
- Canfield, L.; Clandinin, M.; Davies, D.; Fernandez, M.; Jackson, J.; Hawkes, J.; Goldman, W.; Pramuk, K.; Reyes, H.; Sablan, B.; et al. Multinational study of major breast milk carotenoids of healthy mothers. Eur. J. Nutr. 2003, 42, 133–141. [Google Scholar] [PubMed]
- Sommerburg, O.; Meissner, K.; Nelle, M.; Lenhartz, H.; Leichsenring, M. Carotenoid supply in breast-fed and formula-fed neonates. Eur. J. Pediatr. 2000, 159, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Mackey, A.D.; Albrecht, D.; Oliver, J.; Williams, T.; Long, A.C.; Price, P. Plasma carotenoids concentrations of infants are increased by feeding a milk-based infant formula supplemented with carotenoids. J. Sci. Food Agric. 2013, 93, 1945–1952. [Google Scholar] [CrossRef] [PubMed]
- Capeding, R.; Gepanayao, C.P.; Calimon, N.; Lebumfacil, J.; Davis, A.M.; Stouffer, N.; Harris, B. Lutein-fortified infant formula fed to healthy term infants: Evaluation of growth effects and safety. Nutr. J. 2010, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Rules and regulations: Nutrient requirements for infant formulas (21 CFR part 107). Fed. Regist. 1985, 50, 45106–45108. [Google Scholar]
- Gordon, C.C.; Chumlea, W.C.; Roche, A.F. Stature, recumbent length and weight. In Anthropometric Standardization Reference Manual; Lohman, T.G., Roche, A.F., Martorell, R., Eds.; Human Kinetics Books: Champaign, IL, USA, 1988; pp. 3–8. [Google Scholar]
- Callaway, C.W.; Chumlea, W.C.; Bouchard, C.; Himes, J.H.; Lohman, T.G.; Martin, A.D.; Mitchell, C.D.; Mueller, W.H.; Roche, A.F.; Seefeldt, V.D. Circumference. In Anthropometric Standardization Reference Manual; Lohman, T.G., Roche, A.F., Martorell, R., Eds.; Human Kinetics Books: Champaign, IL, USA, 1988; pp. 39–54. [Google Scholar]
- Friedman, J.N.; Goldman, R.D.; Srivastava, R.; Parkin, P.C. Development of a clinical dehydration scale for use in children between 1 and 36 months of age. J. Pediatr. 2004, 145, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.R.; Ostrom, K.M.; Fligner, M.A.; Verducci, J.S. Validation of pediatric tolerance questionnaires. FASEB J. 2002, 16, A659–A660. [Google Scholar]
- Lasekan, J.B.; Linke, H.K.; Oliver, J.S.; Carver, J.D.; Blatter, M.M.; Kuchan, M.J.; Cramer, J.M.; Pollack, P.F. Milk protein-based infant formula containing rice starch and low lactose reduces common regurgitation in healthy term infants: A randomized, blinded and prospective Trial. J. Am. Coll. Nutr. 2014, 33, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Leite, M.E.D.Q.; Lasekan, J.; Baggs, G.; Ribeiro, T.; Menezes-Filho, J.; Pontes, M.; Druzian, J.; Barreto, D.L.; de Souza, C.O.; Mattos, Â.; et al. Calcium and fat metabolic balance, and gastrointestinal tolerance in term infants fed milk-based formulas with and without palm olein and palm kernel oils: A randomized blinded crossover study. BMC Pediatr. 2013, 13, 215. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control (CDC). Growth Charts for the United States: Methods and Development; Series Report 11; CDC: Hyattsville, MD, USA, 2000; No. 246. [Google Scholar]
- Lloyd, B.; Halter, R.J.; Kuchan, M.J.; Baggs, G.; Ryan, A.; Masor, M. Formula tolerance in post-breastfed and exclusively formula-fed infants. Pediatrics 1999, 103, e7. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.C.; de Klerk, N.; Holt, P.; Lehmann, D.; Richmond, P. Hospitalization for bronchiolitis in infants is more common after elective caesarean delivery. Arch. Dis. Child. 2012, 97, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Bager, P.; Wohlfahrt, J.; Westergaard, T. Caesarean delivery and risk of atopic and allergic disease: Meta-analyses. Clin. Exp. Allergy 2008, 38, 634–642. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lasekan, J.; Baggs, G.; Acosta, S.; Mackey, A. Soy Protein-Based Infant Formulas with Supplemental Fructooligosaccharides: Gastrointestinal Tolerance and Hydration Status in Newborn Infants. Nutrients 2015, 7, 3022-3037. https://doi.org/10.3390/nu7043022
Lasekan J, Baggs G, Acosta S, Mackey A. Soy Protein-Based Infant Formulas with Supplemental Fructooligosaccharides: Gastrointestinal Tolerance and Hydration Status in Newborn Infants. Nutrients. 2015; 7(4):3022-3037. https://doi.org/10.3390/nu7043022
Chicago/Turabian StyleLasekan, John, Geraldine Baggs, Sonja Acosta, and Amy Mackey. 2015. "Soy Protein-Based Infant Formulas with Supplemental Fructooligosaccharides: Gastrointestinal Tolerance and Hydration Status in Newborn Infants" Nutrients 7, no. 4: 3022-3037. https://doi.org/10.3390/nu7043022
APA StyleLasekan, J., Baggs, G., Acosta, S., & Mackey, A. (2015). Soy Protein-Based Infant Formulas with Supplemental Fructooligosaccharides: Gastrointestinal Tolerance and Hydration Status in Newborn Infants. Nutrients, 7(4), 3022-3037. https://doi.org/10.3390/nu7043022