
Optimal Vegetable Intake for Metabolic-Dysfunction-Associated Steatotic Liver Disease (MASLD) Prevention: Insights from a South Italian Cohort

 , , , , and
, , , , and 
Abstract
1. Introduction
2. Materials and Methods
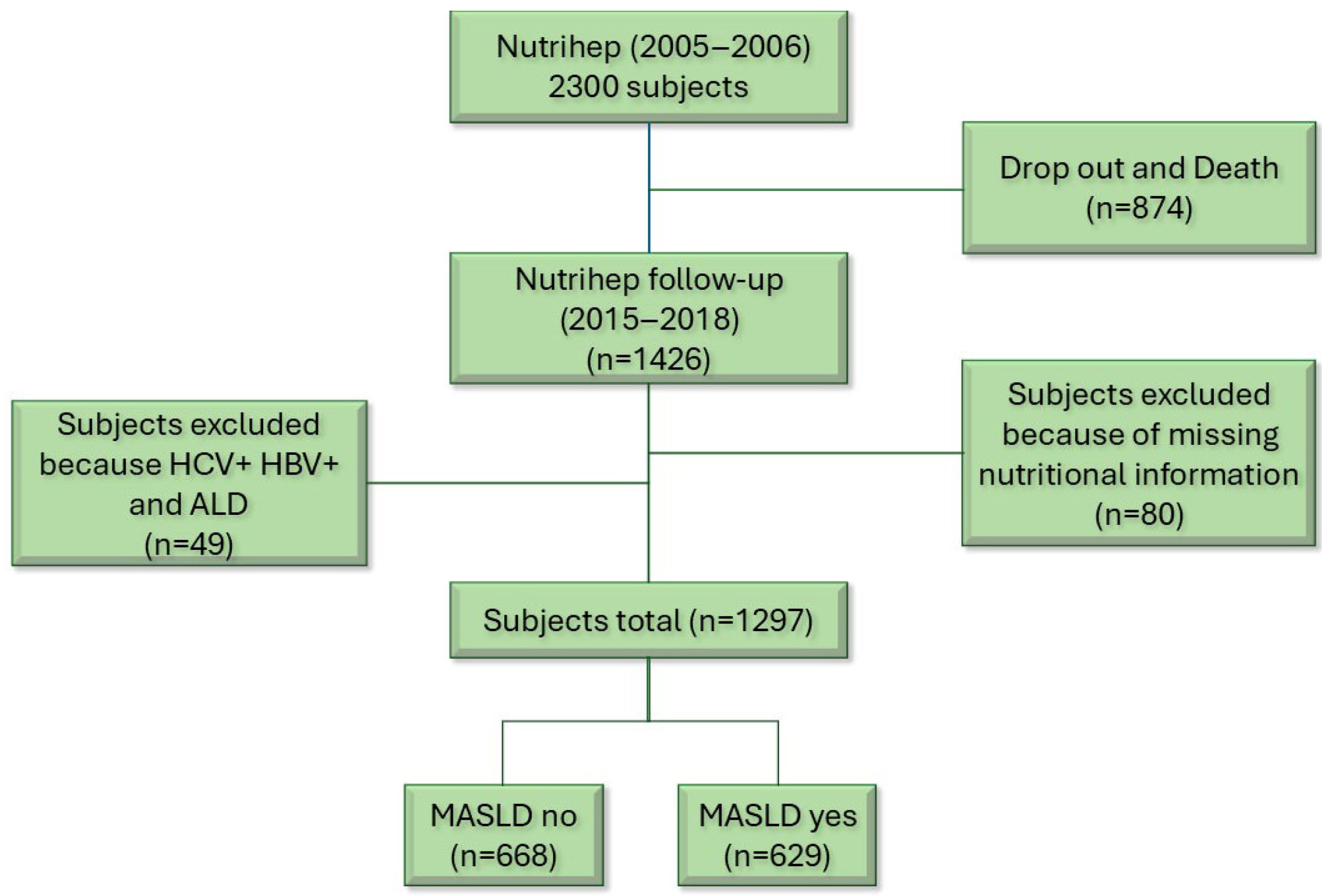
2.1. Study Population
2.2. Data Collection
2.3. Outcome Assessment
2.4. Exposure Variable
2.5. Confounding Variables
2.6. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
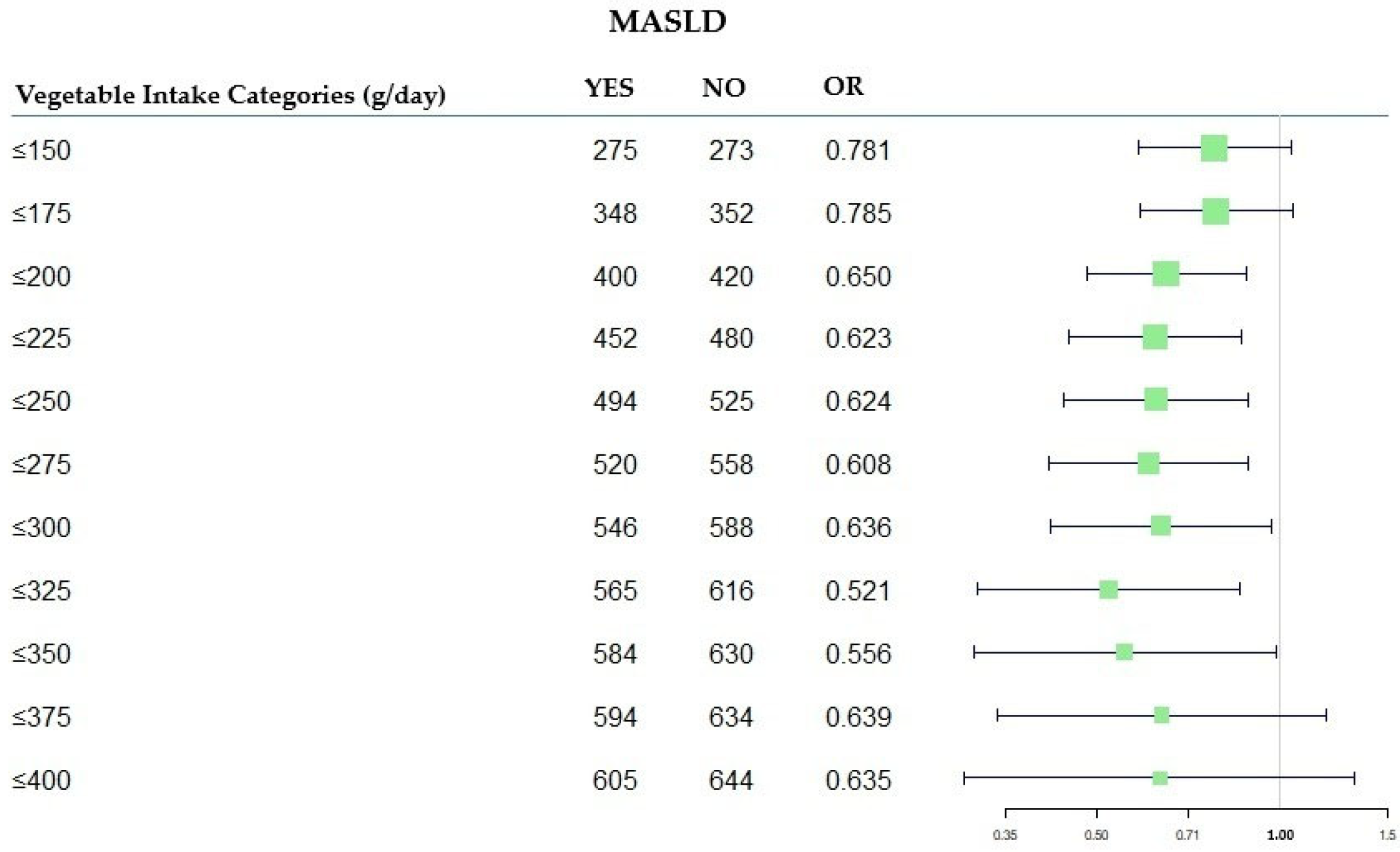
3.2. The Associations Between Different Kinds of Vegetable Intake and the Occurrence of MASLD
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NUTRIHEP | Nutrition and Hepatology |
| MASLD | Metabolic-Dysfunction-Associated Steatotic Liver Disease |
| OR | Odds Ratio |
References
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A Multisociety Delphi Consensus Statement on New Fatty Liver Disease Nomenclature. J. Hepatol. 2023, 79, 1542–1556. [Google Scholar] [CrossRef]
- Proceedings of the 73 Rd Session of the WHO Regional Committee for Europe, Astana, Kazakhstan, 24–26 October 2023.
- Byrne, C.D.; Armandi, A.; Pellegrinelli, V.; Vidal-Puig, A.; Bugianesi, E. Μetabolic Dysfunction-Associated Steatotic Liver Disease: A Condition of Heterogeneous Metabolic Risk Factors, Mechanisms and Comorbidities Requiring Holistic Treatment. Nat. Rev. Gastroenterol. Hepatol. 2025, 22, 314–328. [Google Scholar] [CrossRef]
- Mejía-Guzmán, J.E.; Belmont-Hernández, R.A.; Chávez-Tapia, N.C.; Uribe, M.; Nuño-Lámbarri, N. Metabolic-Dysfunction-Associated Steatotic Liver Disease: Molecular Mechanisms, Clinical Implications, and Emerging Therapeutic Strategies. Int. J. Mol. Sci. 2025, 26, 2959. [Google Scholar] [CrossRef] [PubMed]
- Tacke, F.; Horn, P.; Wong, V.W.S.; Ratziu, V.; Bugianesi, E.; Francque, S.; Zelber-Sagi, S.; Valenti, L.; Roden, M.; Schick, F.; et al. EASL-EASD-EASO Clinical Practice Guidelines on the Management of Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD). Obes. Facts 2024, 17, 374–444. [Google Scholar] [CrossRef]
- Huang, D.Q.; Wong, V.W.S.; Rinella, M.E.; Boursier, J.; Lazarus, J.V.; Yki-Järvinen, H.; Loomba, R. Metabolic Dysfunction-Associated Steatotic Liver Disease in Adults. Nat. Rev. Dis. Primers 2025, 11, 14. [Google Scholar] [CrossRef]
- Donghia, R.; Di Nicola, E.; Tatoli, R.; Forte, G.; Lepore Signorile, M.; Bonfiglio, C.; Latrofa, M.; De Marco, K.; Manghisi, A.; Disciglio, V.; et al. The Protective Effect of FOXO3 Rs2802292 G-Allele on Food Intake in a Southern Italian Cohort Affected by MASLD. Nutrients 2025, 17, 1315. [Google Scholar] [CrossRef]
- Meroni, M.; Longo, M.; Tria, G.; Dongiovanni, P. Genetics Is of the Essence to Face Nafld. Biomedicines 2021, 9, 1359. [Google Scholar] [CrossRef] [PubMed]
- Baratta, F.; Pastori, D.; Polimeni, L.; Bucci, T.; Ceci, F.; Calabrese, C.; Ernesti, I.; Pannitteri, G.; Violi, F.; Angelico, F.; et al. Adherence to Mediterranean Diet and Non-Alcoholic Fatty Liver Disease: Effect on Insulin Resistance. Am. J. Gastroenterol. 2017, 112, 1832–1839. [Google Scholar] [CrossRef] [PubMed]
- Sangouni, A.A.; Hosseinzadeh, M.; Parastouei, K. The Effect of Dietary Approaches to Stop Hypertension (DASH) Diet on Fatty Liver and Cardiovascular Risk Factors in Subjects with Metabolic Syndrome: A Randomized Controlled Trial. BMC Endocr. Disord. 2024, 24, 126. [Google Scholar] [CrossRef]
- Huang, X.; Gan, D.; Fan, Y.; Fu, Q.; He, C.; Liu, W.; Li, F.; Ma, L.; Wang, M.; Zhang, W. The Associations between Healthy Eating Patterns and Risk of Metabolic Dysfunction-Associated Steatotic Liver Disease: A Case-Control Study. Nutrients 2024, 16, 1956. [Google Scholar] [CrossRef]
- Cunha, G.M.; Guzman, G.; Correa De Mello, L.L.; Trein, B.; Spina, L.; Bussade, I.; Marques Prata, J.; Sajoux, I.; Countinho, W. Efficacy of a 2-Month Very Low-Calorie Ketogenic Diet (VLCKD) Compared to a Standard Low-Calorie Diet in Reducing Visceral and Liver Fat Accumulation in Patients with Obesity. Front. Endocrinol. 2020, 11, 607. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Ivancovsky-Wajcman, D.; Fliss Isakov, N.; Webb, M.; Orenstein, D.; Shibolet, O.; Kariv, R. High Red and Processed Meat Consumption Is Associated with Non-Alcoholic Fatty Liver Disease and Insulin Resistance. J. Hepatol. 2018, 68, 1239–1246. [Google Scholar] [CrossRef]
- García, S.; Monserrat-Mesquida, M.; Ugarriza, L.; Casares, M.; Gómez, C.; Mateos, D.; Angullo-Martínez, E.; Tur, J.A.; Bouzas, C. Ultra-Processed Food Consumption and Metabolic-Dysfunction-Associated Steatotic Liver Disease (MASLD): A Longitudinal and Sustainable Analysis. Nutrients 2025, 17, 472. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.A.; Shin, S. Fruit and Vegetable Consumption and Non-Alcoholic Fatty Liver Disease Among Korean Adults: A Prospective Cohort Study. J. Epidemiol. Community Health 2020, 74, 1035–1042. [Google Scholar] [CrossRef] [PubMed]
- Donghia, R.; Campanella, A.; Bonfiglio, C.; Cuccaro, F.; Tatoli, R.; Giannelli, G. Protective Role of Lycopene in Subjects with Liver Disease: NUTRIHEP Study. Nutrients 2024, 16, 562. [Google Scholar] [CrossRef] [PubMed]
- Bonfiglio, C.; Tatoli, R.; Donghia, R.; Guido, D.; Giannelli, G. Exploratory Role of Flavonoids on Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in a South Italian Cohort. Antioxidants 2024, 13, 1286. [Google Scholar] [CrossRef]
- Li, H.; Wang, X.; Ye, M.; Zhang, S.; Zhang, Q.; Meng, G.; Liu, L.; Wu, H.; Gu, Y.; Wang, Y.; et al. Does a High Intake of Green Leafy Vegetables Protect from NAFLD? Evidence from a Large Population Study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1691–1701. [Google Scholar] [CrossRef]
- Sasada, T.; Iino, C.; Sato, S.; Tateda, T.; Igarashi, G.; Yoshida, K.; Sawada, K.; Mikami, T.; Nakaji, S.; Sakuraba, H.; et al. The Impact of Japanese Dietary Patterns on Metabolic Dysfunction-Associated Steatotic Liver Disease and Liver Fibrosis. Nutrients 2024, 16, 2877. [Google Scholar] [CrossRef]
- Liu, C.; Liu, Y.; Liu, J.; Liu, J.; Lu, T.; Yu, J.; Zhang, G.; Xu, K. Associations between Intake of Different Types of Vegetables and Metabolic Dysfunction-Associated Fatty Liver Disease: A Population-Based Study. BMC Public Health 2025, 25, 315. [Google Scholar] [CrossRef]
- Taniguchi, H.; Ueda, M.; Kobayashi, Y.; Shima, T. BMI Gain and Dietary Characteristics Are Risk Factors of MASLD in Non-Obese Individuals. Sci. Rep. 2025, 15, 2606. [Google Scholar] [CrossRef]
- Cozzolongo, R.; Osella, A.R.; Elba, S.; Petruzzi, J.; Buongiorno, G.; Giannuzzi, V.; Leone, G.; Bonfiglio, C.; Lanzilotta, E.; Manghisi, O.G.; et al. Epidemiology of HCV Infection in the General Population: A Survey in a Southern Italian Town. Off. J. Am. Coll. Gastroenterol. ACG 2009, 104, 2740–2746. [Google Scholar] [CrossRef]
- International Standard Classification of Education (ISCED); The United Nations Educational, Scientific and Cultural Organization: Paris, France, 1997.
- International Standard Classification of Occupations (ISCO-08); International Labour Office: Geneva, Switzerland, 2012.
- Sever, P. New Hypertension Guidelines from the National Institute for Health Clinical Excellence the British Hypertension Society. J. Renin-Angiotensin-Aldosterone Syst. 2006, 7, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Riboli, E.; Hunt, K.J.; Slimani, N.; Ferrari, P.; Norat, T.; Fahey, M.; Charrondière, U.R.; Hémon, B.; Casagrande, C.; Vignat, J.; et al. European Prospective Investigation into Cancer and Nutrition (EPIC): Study Populations and Data Collection. Public Health Nutr. 2002, 5, 1113–1124. [Google Scholar] [CrossRef]
- Riboli, E.; Kaaks, R. The EPIC Project: Rationale and Study Design. European Prospective Investigation into Cancer and Nutrition. Int. J. Epidemiol. 1997, 26, S6. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Chiloiro, M.; Caruso, M.G.; Cisternino, A.M.; Inguaggiato, R.; Reddavide, R.; Bonfiglio, C.; Guerra, V.; Notarnicola, M.; De Michele, G.; Correale, M.; et al. Ultrasound Evaluation and Correlates of Fatty Liver Disease: A Population Study in a Mediterranean Area. Metab. Syndr. Relat. Disord. 2013, 11, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Pisani, P. Relative Validity and Reproducibility of a Food Frequency Dietary Questionnaire for Use in the Italian EPIC Centres. Int. J. Epidemiol. 1997, 26, S152–S160. [Google Scholar] [CrossRef] [PubMed]
- Dulai, P.S.; Singh, S.; Patel, J.; Soni, M.; Prokop, L.J.; Younossi, Z.; Sebastiani, G.; Ekstedt, M.; Hagstrom, H.; Nasr, P.; et al. Increased Risk of Mortality by Fibrosis Stage in Nonalcoholic Fatty Liver Disease: Systematic Review and Meta-analysis. Hepatology 2017, 65, 1557–1565. [Google Scholar] [CrossRef]
- Simon, S.D. Understanding the Odds Ratio and the Relative Risk. J. Androl. 2001, 22, 533–536. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Society Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Belsley, D.A.; Kuh, E.; Welsch, R.E. Regression Diagnostics; Wiley: Hoboken, NJ, USA, 1980; ISBN 9780471058564. [Google Scholar]
- Adinolfi, F.; Carcea, M.; De Gara, L. Linee Guida Definitive—CREA. 2019. Available online: https://sapermangiare.mobi/files/download/linee-guida/linee-guida-completo.pdf (accessed on 26 July 2025).
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean Diet Pyramid Today. Science and Cultural Updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef]
- Sato, S.; Iino, C.; Sasada, T.; Soma, G.; Furusawa, K.; Yoshida, K.; Sawada, K.; Mikami, T.; Nakaji, S.; Sakuraba, H.; et al. Epidemiological Study on the Interaction between the PNPLA3 (Rs738409) and Gut Microbiota in Metabolic Dysfunction-Associated Steatotic Liver Disease. Genes 2024, 15, 1172. [Google Scholar] [CrossRef]
- Us Altay, D.; Kaya, Y.; Mataraci Değirmenci, D.; Kocyiğit, E.; Üner, A.; Noyan, T. Non-Alcoholic Fatty Liver Disease: The Importance of Physical Activity and Nutrition Education—A Randomized Controlled Study. J. Gastroenterol. Hepatol. 2024, 39, 2723–2734. [Google Scholar] [CrossRef]
- Pintó, X.; Fanlo-Maresma, M.; Corbella, E.; Corbella, X.; Mitjavila, M.T.; Moreno, J.J.; Casas, R.; Estruch, R.; Corella, D.; Bulló, M.; et al. A Mediterranean Diet Rich in Extra-Virgin Olive Oil Is Associated with a Reduced Prevalence of Nonalcoholic Fatty Liver Disease in Older Individuals at High Cardiovascular Risk. J. Nutr. 2019, 149, 1920–1929. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Yan, R.; Jiao, J.; Li, F.; Zhang, H.; Chang, Z.; Wei, H.; Yan, S.; Li, J. Fruit and Vegetable Intake and the Risk of Non-Alcoholic Fatty Liver Disease: A Meta-Analysis of Observational Studies. Front. Nutr. 2024, 11, 1398184. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, L.; Jia, L.; Liu, J. Association between Carotenoid Intake and Metabolic Dysfunction-Associated Fatty Liver Disease among US Adults: A Cross-Sectional Study. Medicine 2023, 102, E36658. [Google Scholar] [CrossRef]
- Gao, X.; Zhao, X.; Liu, M.; Zhao, H.; Sun, Y. Lycopene Prevents Non-Alcoholic Fatty Liver Disease through Regulating Hepatic NF-ΚB/NLRP3 Inflammasome Pathway and Intestinal Microbiota in Mice Fed with High-Fat and High-Fructose Diet. Front. Nutr. 2023, 10, 1120254. [Google Scholar] [CrossRef]
- Ni, Y.; Zhuge, F.; Nagashimada, M.; Nagata, N.; Xu, L.; Yamamoto, S.; Fuke, N.; Ushida, Y.; Suganuma, H.; Kaneko, S.; et al. Lycopene Prevents the Progression of Lipotoxicity-Induced Nonalcoholic Steatohepatitis by Decreasing Oxidative Stress in Mice. Free Radic. Biol. Med. 2020, 152, 571–582. [Google Scholar] [CrossRef]
- Donghia, R.; Tatoli, R.; Campanella, A.; Cuccaro, F.; Bonfiglio, C.; Giannelli, G. Adding a Leafy Vegetable Fraction to Diets Decreases the Risk of Red Meat Mortality in MASLD Subjects: Results from the MICOL Cohort. Nutrients 2024, 16, 1207. [Google Scholar] [CrossRef]
- De Nucci, S.; Rinaldi, R.; Di Chito, M.; Donghia, R.; Giannuzzi, V.; Shahini, E.; Cozzolongo, R.; Pesole, P.L.; Coletta, S.; De Pergola, G.; et al. The Replacement of Only One Portion of Starchy Carbohydrates with Green Leafy Vegetables Regresses Mid and Advanced Stages of NAFLD: Results from a Prospective Pilot Study. Nutrients 2023, 15, 2289. [Google Scholar] [CrossRef]
- Chee, N.M.Z.; Sinnanaidu, R.P.; Chan, W.K. Vitamin E Improves Serum Markers and Histology in Adults with Metabolic Dysfunction-Associated Steatotic Liver Disease: Systematic Review and Meta-Analysis. J. Gastroenterol. Hepatol. 2024, 39, 2545–2554. [Google Scholar] [CrossRef]
- Wu, S.; Chen, R.; Chen, J.; Yang, N.; Li, K.; Zhang, Z.; Zhang, R. Study of the Anti-Inflammatory Mechanism of β-Carotene Based on Network Pharmacology. Molecules 2023, 28, 7540. [Google Scholar] [CrossRef] [PubMed]
- Abera, M.; Suresh, S.B.; Malireddi, A.; Boddeti, S.; Noor, K.; Ansar, M.; Malasevskaia, I. Vitamin E and Non-Alcoholic Fatty Liver Disease: Investigating the Evidence Through a Systematic Review. Cureus 2024, 16, e72596. [Google Scholar] [CrossRef]
- Mirmiran, P.; Teymoori, F.; Farhadnejad, H.; Mokhtari, E.; Salehi-Sahlabadi, A. Nitrate Containing Vegetables and Dietary Nitrate and Nonalcoholic Fatty Liver Disease: A Case Control Study. Nutr. J. 2023, 22, 3. [Google Scholar] [CrossRef]
- Cordero-Herrera, I.; Kozyra, M.; Zhuge, Z.; Haworth, S.M.C.; Moretti, C.; Peleli, M.; Caldeira-Dias, M.; Jahandideh, A.; Huirong, H.; de Campos Cruz, J.; et al. AMP-Activated Protein Kinase Activation and NADPH Oxidase Inhibition by Inorganic Nitrate and Nitrite Prevent Liver Steatosis. Proc. Natl. Acad. Sci. USA 2019, 116, 217–226. [Google Scholar] [CrossRef]
- Xu, Y.; Huang, X.; Huangfu, B.; Hu, Y.; Xu, J.; Gao, R.; Huang, K.; He, X. Sulforaphane Ameliorates Nonalcoholic Fatty Liver Disease Induced by High-Fat and High-Fructose Diet via LPS/TLR4 in the Gut–Liver Axis. Nutrients 2023, 15, 743. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Lei, Y.; Zhao, F.; Che, J.; Wu, Y.; Lei, P.; Kang, Y.E.; Shan, Y. Improving Insulin Resistance by Sulforaphane via Activating the Bacteroides and Lactobacillus SCFAs–GPR–GLP1 Signal Axis. Food Funct. 2024, 15, 8644–8660. [Google Scholar] [CrossRef] [PubMed]
- Kianian, F.; Marefati, N.; Boskabady, M.; Ghasemi, S.Z.; Boskabady, M.H. Pharmacological Properties of Allium Cepa, Preclinical and Clinical Evidences: A Review. Iran. J. Pharm. Res. 2021, 20, 107–134. [Google Scholar] [CrossRef]
- Emamat, H.; Foroughi, F.; Eini–Zinab, H.; Taghizadeh, M.; Rismanchi, M.; Hekmatdoost, A. The Effects of Onion Consumption on Treatment of Metabolic, Histologic, and Inflammatory Features of Nonalcoholic Fatty Liver Disease. J. Diabetes Metab. Disord. 2015, 15, 25. [Google Scholar] [CrossRef] [PubMed]
- Emamat, H.; Foroughi, F.; Eini-Zinab, H.; Hekmatdoost, A. The Effects of Onion Consumption on Prevention of Nonalcoholic Fatty Liver Disease. Indian J. Clin. Biochem. 2018, 33, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, A.; Tormo, E.; Barat, J.M.; Fernández-Segovia, I. Importance of the Origin, Organic Production and Other Extrinsic Parameters in Fruit and Vegetable Choices. Food Sci. Technol. Int. 2023, 31, 275–286. [Google Scholar] [CrossRef]
- Nutrition Research Must Go Local. Nat. Med. 2025, 31, 1371. [CrossRef]
- Miglio, C.; Chiavaro, E.; Visconti, A.; Fogliano, V.; Pellegrini, N. Effects of Different Cooking Methods on Nutritional and Physicochemical Characteristics of Selected Vegetables. J. Agric. Food Chem. 2008, 56, 139–147. [Google Scholar] [CrossRef]
- Schmiedeskamp, A.; Schreiner, M.; Baldermann, S. Impact of Cultivar Selection and Thermal Processing by Air Drying, Air Frying, and Deep Frying on the Carotenoid Content and Stability and Antioxidant Capacity in Carrots (Daucus Carota L.). J. Agric. Food Chem. 2022, 70, 1629–1639. [Google Scholar] [CrossRef]
- Taylor, M.K.; Sullivan, D.K.; Ellerbeck, E.F.; Gajewski, B.J.; Gibbs, H.D. Nutrition Literacy Predicts Adherence to Healthy/Unhealthy Diet Patterns in Adults with a Nutrition-Related Chronic Condition. Public Health Nutr. 2019, 22, 2157–2169. [Google Scholar] [CrossRef]
- Donghia, R.; Bonfiglio, C.; Giannelli, G.; Tatoli, R. Impact of Education on Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A Southern Italy Cohort-Based Study. J. Clin. Med. 2025, 14, 1950. [Google Scholar] [CrossRef]
- Cueto-Galán, R.; Fontalba-Navas, A.; Gutiérrez-Bedmar, M.; Ruiz-Canela, M.; Martínez-González, M.A.; Alves, L.; Babio, N.; Fitó, M.; Ros, E.; Fiol, M.; et al. Adherence to the Mediterranean Diet to Prevent or Delay Hepatic Steatosis: A Longitudinal Analysis within the PREDIMED Study. Front. Nutr. 2025, 12, 1518082. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Kalligeros, M.; Henry, L. Epidemiology of Metabolic Dysfunction-Associated Steatotic Liver Disease. Clin. Mol. Hepatol. 2025, 31, S32–S50. [Google Scholar] [CrossRef] [PubMed]
- Bagnato, C.B.; Bianco, A.; Bonfiglio, C.; Franco, I.; Verrelli, N.; Carella, N.; Shahini, E.; Zappimbulso, M.; Giannuzzi, V.; Pesole, P.L.; et al. Healthy Lifestyle Changes Improve Cortisol Levels and Liver Steatosis in MASLD Patients: Results from a Randomized Clinical Trial. Nutrients 2024, 16, 4225. [Google Scholar] [CrossRef] [PubMed]
- Fewell, Z.; Davey Smith, G.; Sterne, J.A.C. The Impact of Residual and Unmeasured Confounding in Epidemiologic Studies: A Simulation Study. Am. J. Epidemiol. 2007, 166, 646–655. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Color group |
| Green vegetables: cruciferous (cabbage, broccoli, Brussel sprouts, turnips, kale, cauliflower), leafy greens (spinach, Swiss chard, chicory), leafy salads, lettuce, artichokes, green beans, zucchini |
| Red/orange vegetables: tomatoes, carrots, red beets |
| White and other color vegetables: eggplant, mushrooms, onions, leeks, fennel, celery, peppers, soy sprouts |
| Variables a | MASLD | |||
|---|---|---|---|---|
| Whole Sample b | No | Yes | p-value c | |
| N (%) | 1297 | 668 (51.50) | 629 (48.50) | |
| Exposure variables | ||||
| Total vegetables (g/day) | 183.17 (102.90) | 185.85 (101.67) | 180.33 (104.20) | 0.33 |
| Green vegetables (g/day) | 53.85 (39.69) | 54.31 (40.29) | 53.38 (39.07) | 0.67 |
| Red and orange vegetables (g/day) | 61.65 (52.69) | 61.27 (52.82) | 62.05 (52.59) | 0.79 |
| White and other color vegetables (g/day) | 46.53 (29.93) | 47.55 (29.16) | 45.45 (30.72) | 0.21 |
| Demographic and lifestyle characteristics | ||||
| Age (years) | 54.33 (14.34) | 49.24 (13.80) | 59.74 (12.86) | <0.001 |
| Gender (%) | ||||
| Female | 744 (57.4) | 417 (56.0) | 327 (44.0%) | <0.001 |
| Male | 553 (42.6) | 251 (45.4) | 302 (54.6%) | |
| Fruits (g/day) | 409.17 (238.15) | 395.87 (228.02) | 423.29 (247.86) | 0.038 |
| Legumes (g/day) | 33.89 (29.06) | 33.20 (29.07) | 34.63 (29.05) | 0.37 |
| Cereals (g/day) | 219.22 (119.29) | 223.85 (117.30) | 214.31 (121.26) | 0.15 |
| Fish (g/day) | 39.09 (26.04) | 40.06 (25.44) | 38.05 (26.64) | 0.16 |
| Olive oil (g/day) | 18.17 (10.85) | 18.26 (10.97) | 18.08 (10.72) | 0.76 |
| Total meat (g/day) | 93.54 (53.79) | 95.36 (54.56) | 91.60 (52.94) | 0.21 |
| rMED | 8.04 (2.55) | 7.91 (2.54) | 8.18 (2.56) | 0.05 |
| rMED score (%) | ||||
| Low | 365 (28.1%) | 196 (53.7%) | 169 (46.3%) | 0.46 |
| Moderate | 705 (54.4%) | 362 (51.3%) | 343 (48.7%) | |
| High | 227 (17.5%) | 110 (48.5%) | 117 (51.5%) | |
| Alcohol intake (g/day) | 10.58 (12.72) | 10.74 (13.41) | 10.42 (11.96) | 0.66 |
| Wine intake (ml/day) | 67.18 (174.36) | 56.88 (214.44) | 78.13 (116.89) | 0.028 |
| Kcal (day) | 2056.26 (750.22) | 2100.33 (724.88) | 2009.46 (774.05) | 0.029 |
| Smoker (%) | ||||
| Never/former | 1137 (87.7) | 587 (51.6) | 550 (48.4) | 0.87 |
| Current | 159 (12.3) | 81 (50.9) | 78 (49.1) | |
| Marital Status (%) | ||||
| Single | 181 (14.0) | 115 (63.5) | 66 (36.5) | <0.001 |
| Married or living together | 1034 (79.7) | 519 (50.2) | 515 (49.8) | |
| Separated or divorced | 28 (2.2) | 20 (71.4) | 8 (28.6) | |
| Widow/er | 54 (4.2) | 14 (25.9) | 40 (74.1) | |
| Education (%) | ||||
| Primary school | 282 (21.8) | 71 (25.2) | 211 (74.8) | <0.001 |
| Secondary school | 383 (29.5) | 171 (44.6) | 212 (55.5) | |
| High School | 460 (35.5) | 307 (66.7) | 153 (33.3) | |
| Graduate | 172 (13.3) | 119 (69.2) | 53 (30.8) | |
| Work (%) | ||||
| Managers and professionals | 102 (7.9) | 57 (55.9) | 45 (44.1) | <0.001 |
| Craft, agricultural, and sales workers | 469 (36.2) | 285 (60.8) | 184 (39.2) | |
| Elementary occupations | 185 (14.1) | 93 (50.3) | 92 (49.7) | |
| Housewife | 141 (10.9) | 74 (52.5) | 67 (47.5) | |
| Pensioner | 325 (25.1) | 110 (33.8) | 215 (66.2) | |
| Unemployed | 75 (5.8) | 49 (65.3) | 26 (34.7) | |
| Family income assessment (%) | ||||
| Insufficient | 27 (2.1) | 10 (37.0) | 17 (63.0) | 0.025 |
| Just sufficient | 167 (12.9) | 81 (48.5) | 86 (51.5) | |
| Sufficient | 1019 (78.6) | 521 (51.1) | 498 (48.9) | |
| More than sufficient | 64 (4.9) | 44 (68.8) | 20 (31.2) | |
| Good | 20 (1.5) | 12 (60.0) | 8 (40.0) | |
| Anthropometric and clinical parameters | ||||
| BMI (kg/m2) | 27.58 (5.05) | 25.04 (3.59) | 30.28 (4.97) | <0.001 |
| Weight (kg) | 72.93 (14.87) | 66.66 (12.02) | 79.58 (14.73) | <0.001 |
| Waist (cm) | 90.45 (13.46) | 83.04 (10.38) | 98.32 (11.79) | <0.001 |
| SBP (mmHg) | 120.93 (15.81) | 115.64 (15.35) | 126.52 (14.30) | <0.001 |
| DBP (mmHg) | 77.68 (8.00) | 75.69 (7.88) | 79.78 (7.58) | <0.001 |
| Hypertension (%) | ||||
| No | 847 (68.8) | 517 (61.0) | 330 (39.0) | <0.001 |
| Yes | 385 (31.2) | 115 (29.9) | 270 (70.1) | |
| Dyslipidemia (%) | ||||
| No | 1047 (85.1) | 561 (53.6) | 486 (46.4) | <0.001 |
| Yes | 184 (14.9) | 71 (38.6) | 113 (61.4) | |
| Diabetes (%) | ||||
| No | 1148 (93.2) | 620 (54.0) | 528 (46.0) | <0.001 |
| Yes | 84 (6.8) | 12 (14.3) | 72 (85.7) | |
| Blood Test | ||||
| HbA1c (mmol/mol) | 38.07 (6.87) | 36.59 (5.05) | 39.64 (8.09) | <0.001 |
| HOMA | 1.89 (1.88) | 1.33 (0.90) | 2.43 (2.38) | <0.001 |
| ALT (U/L) | 22.20 (16.21) | 19.70 (8.27) | 24.86 (21.37) | <0.001 |
| ɣGT (U/L) | 17.58 (13.46) | 14,80 (7,67) | 20,54 (17,16) | <0.001 |
| AST (U/L) | 21.74 (10.87) | 20,70 (5,94) | 22,85 (14,29) | <0.001 |
| TG (mg/dL) | 98.41 (69.23) | 80.73 (58.55) | 117.22 (74.60) | <0.001 |
| C-reactive protein (mg/dL) | 0.26 (0.55) | 0.21 (0.52) | 0.31 (0.58) | <0.001 |
| TC (mg/dL) | 191.35 (35.36) | 188.90 (33.06) | 193.96 (37.50) | 0.010 |
| HDL (mg/dL) | 50.79 (12.59) | 53.18 (12.80) | 48.24 (11.85) | <0.001 |
| Glucose (mg/dL) | 95.34 (17.34) | 90.13 (10.54) | 100.89 (21.06) | <0.001 |
| ALP (U/L) | 52.98 (16.10) | 50.10 (15.56) | 56.04 (16.11) | <0.001 |
| Variables | MASLD | |||
|---|---|---|---|---|
| Whole Sample | No | Yes | p-value a | |
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| Green vegetables (g/day) | ||||
| Artichokes | 3.31 (4.19) | 3.32 (4.14) | 3.30 (4.25) | 0.94 |
| Cruciferous b | 7.87 (7.96) | 7.60 (7.41) | 8.16 (8.50) | 0.21 |
| Green leafy vegetables c | 12.42 (15.49) | 12.79 (15.76) | 12.03 (15.19) | 0.38 |
| Lettuce | 16.24 (19.96) | 16.18 (22.23) | 16.31 (17.24) | 0.90 |
| Zucchini | 9.30 (10.39) | 9.77 (10.49) | 8.79 (10.27) | 0.090 |
| Green beans | 4.71 (6.08) | 4.65 (5.91) | 4.78 (6.26) | 0.70 |
| Red/orange vegetables (g/day): | ||||
| Tomatoes | 46.33 (47.02) | 45.60 (48.32) | 47.10 (45.63) | 0.57 |
| Carrots | 13.87 (15.61) | 14.14 (14.50) | 13.59 (16.71) | 0.53 |
| Red beets | 1.45 (2.46) | 1.52 (2.26) | 1.36 (2.65) | 0.23 |
| White and other color vegetables (g/day) | ||||
| Peppers | 2.52 (3.51) | 2.53 (3.42) | 2.52 (3.62) | 0.97 |
| Mushrooms | 4.32 (5.67) | 4.54 (6.78) | 4.09 (4.17) | 0.15 |
| Onions | 11.74 (14.02) | 11.02 (14.06) | 12.51 (13.95) | 0.050 |
| Fennel | 15.45 (13.79) | 15.87 (13.24) | 15.00 (14.36) | 0.26 |
| Eggplant | 6.10 (6.86) | 6.35 (6.80) | 5.83 (6.92) | 0.17 |
| Soy sprouts | 0.16 (0.82) | 0.17 (0.85) | 0.14 (0.79) | 0.52 |
| Celery | 8.85 (9.86) | 9.01 (9.85) | 8.68 (9.88) | 0.55 |
| OR a | p-Value | 95% CI | |
|---|---|---|---|
| Total Vegetables (g/day) | |||
| Categories: | |||
| >150 vs. ≤150 | 0.781 | 0.096 | 0.584; 1.045 |
| >175 vs. ≤175 | 0.785 | 0.101 | 0.588; 1.048 |
| >200 vs. ≤200 | 0.650 | 0.005 | 0.480; 0.881 |
| >225 vs. ≤225 | 0.623 | 0.004 | 0.450; 0.863 |
| >250 vs. ≤250 | 0.624 | 0.008 | 0.440; 0.886 |
| >275 vs. ≤275 | 0.608 | 0.010 | 0.416; 0.888 |
| >300 vs. ≤300 | 0.636 | 0.035 | 0.418; 0.968 |
| >325 vs. ≤325 | 0.521 | 0.010 | 0.317; 0.858 |
| >350 vs. ≤350 | 0.556 | 0.046 | 0.313; 0.989 |
| >375 vs. ≤375 | 0.639 | 0.161 | 0.342; 1.194 |
| >400 vs. ≤400 | 0.635 | 0.228 | 0.303; 1.329 |
| Total intake | 1.002 | 0.014 | 1.000; 1.003 |
| OR a | p-Value | 95% CI | |
|---|---|---|---|
| Green vegetables (g/day) | |||
| Categories: | |||
| >30 vs. ≤30 | 0.670 | 0.019 | 0.480; 0.935 |
| >35 vs. ≤35 | 0.616 | 0.003 | 0.446; 0.851 |
| >40 vs. ≤40 | 0.656 | 0.009 | 0.478; 0.900 |
| >45 vs. ≤45 | 0.704 | 0.029 | 0.514; 0.964 |
| >50 vs. ≤50 | 0.734 | 0.056 | 0.534; 1.008 |
| >55 vs. ≤55 | 0.813 | 0.212 | 0.588; 1.125 |
| Total intake | 1.005 | 0.009 | 1.001; 1.009 |
| Red and orange vegetables (g/day) | |||
| Categories | |||
| >70 vs. ≤70 | 0.818 | 0.209 | 0.598; 1.119 |
| >80 vs. ≤80 | 0.612 | 0.004 | 0.440; 0.851 |
| >90 vs. ≤90 | 0.511 | 0.000 | 0.356; 0.733 |
| >100 vs. ≤100 | 0.511 | 0.000 | 0.356; 0.733 |
| >110 vs. ≤110 | 0.514 | 0.002 | 0.337; 0.784 |
| >120 vs. ≤120 | 0.477 | 0.002 | 0.298; 0.762 |
| >130 vs. ≤130 | 0.457 | 0.003 | 0.274; 0.762 |
| >140 vs. ≤140 | 0.481 | 0.008 | 0.280; 0.829 |
| >150 vs. ≤150 | 0.504 | 0.023 | 0.280; 0.910 |
| >160 vs. ≤160 | 0.532 | 0.060 | 0.275; 1.027 |
| >170 vs. ≤170 | 0.633 | 0.214 | 0.307; 1.303 |
| Total intake | 1.004 | 0.004 | 1.001; 1.007 |
| White and other color vegetables (g/day) | |||
| Total intake | 0.995 | 0.047 | 0.989; 0.999 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pastore, M.N.; Bonfiglio, C.; Tatoli, R.; Donghia, R.; Pesole, P.L.; Giannelli, G. Optimal Vegetable Intake for Metabolic-Dysfunction-Associated Steatotic Liver Disease (MASLD) Prevention: Insights from a South Italian Cohort. Nutrients 2025, 17, 2477. https://doi.org/10.3390/nu17152477
Pastore MN, Bonfiglio C, Tatoli R, Donghia R, Pesole PL, Giannelli G. Optimal Vegetable Intake for Metabolic-Dysfunction-Associated Steatotic Liver Disease (MASLD) Prevention: Insights from a South Italian Cohort. Nutrients. 2025; 17(15):2477. https://doi.org/10.3390/nu17152477
Chicago/Turabian StylePastore, Maria Noemy, Caterina Bonfiglio, Rossella Tatoli, Rossella Donghia, Pasqua Letizia Pesole, and Gianluigi Giannelli. 2025. "Optimal Vegetable Intake for Metabolic-Dysfunction-Associated Steatotic Liver Disease (MASLD) Prevention: Insights from a South Italian Cohort" Nutrients 17, no. 15: 2477. https://doi.org/10.3390/nu17152477
APA StylePastore, M. N., Bonfiglio, C., Tatoli, R., Donghia, R., Pesole, P. L., & Giannelli, G. (2025). Optimal Vegetable Intake for Metabolic-Dysfunction-Associated Steatotic Liver Disease (MASLD) Prevention: Insights from a South Italian Cohort. Nutrients, 17(15), 2477. https://doi.org/10.3390/nu17152477