
The Profiles of Diet- or Exercise-Related Self-Efficacy and Social Support Associated with Insufficient Fruit/Vegetable Intake and Exercise in Women with Abdominal Obesity

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Data Collection
2.5. Measurement
2.6. Statistical Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics
3.2. Daily Fruit/Vegetable Intake and Exercise Behaviors
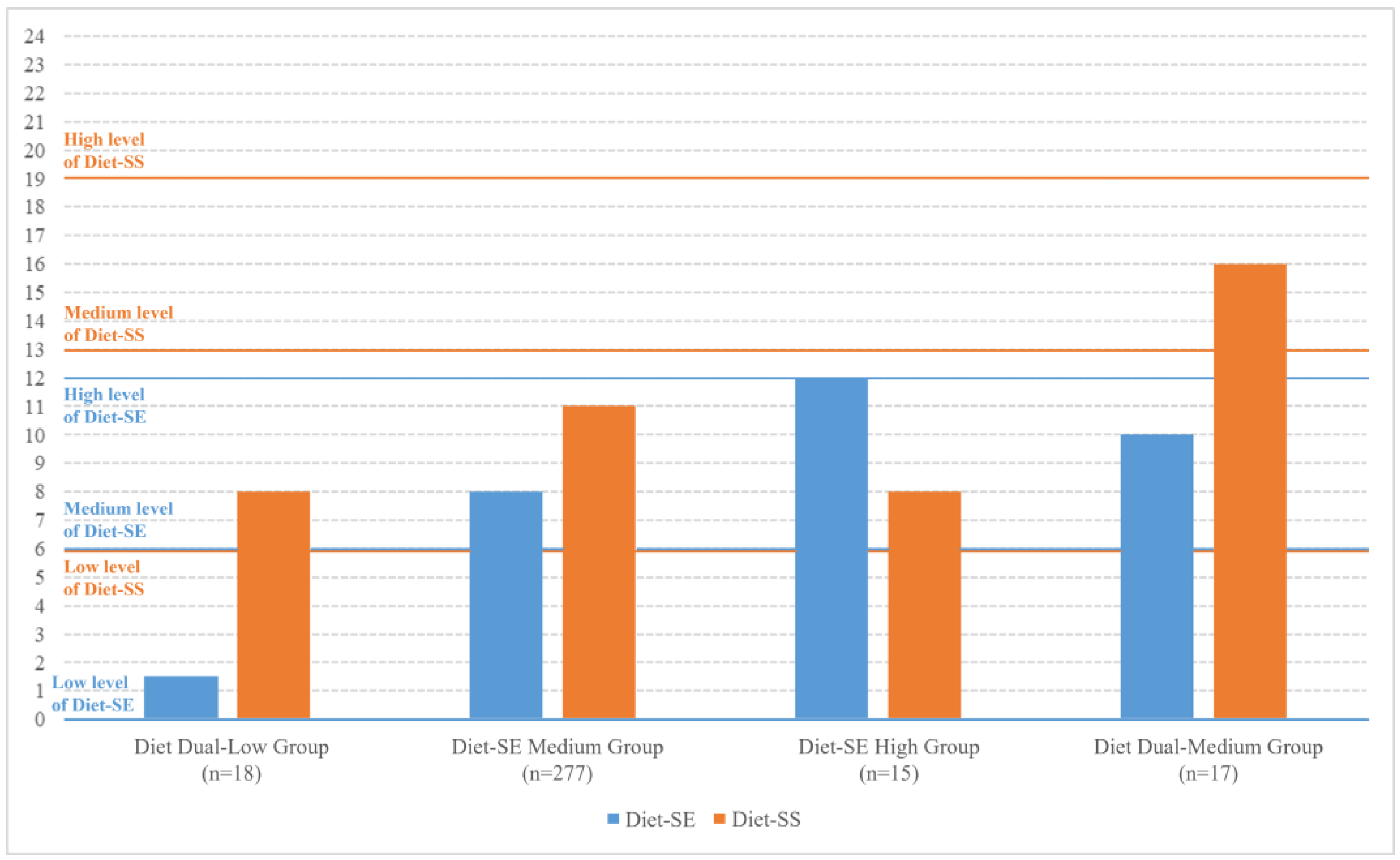
3.3. Latent Profile Analysis of Diet-Related Self-Efficacy (Diet-SE) and Social Support (Diet-SS)
3.4. Diet Dual-Low Group Associated with Less than Five Servings of Daily Fruit/Vegetable Intake
3.5. Associating Factors of the Diet Dual-Low Group
3.6. Latent Profile Analysis of Exercise-Related Self-Efficacy (Exercise-SE) and Social Support (Exercise-SS)
3.7. Exercise Dual-Low Group and Exercise-SS Medium–Low Group Associated with Less than 30 Min of Daily Exercise
3.8. Associating Factors of the Exercise Dual-Low Group and the Exercise-SS Medium–Low Group
4. Discussion
4.1. Implication for Research and Practice
4.2. Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Obesity Federation. World Obesity Atlas 2023. 2023. Available online: https://s3-eu-west-1.amazonaws.com/wof-files/World_Obesity_Atlas_2023_Report.pdf (accessed on 13 July 2024).
- World Health Organization. World Health Statistics 2023: Monitoring Health for the SDGs, Sustainable Development Goals. 2023. Available online: https://www.who.int/publications/i/item/9789240074323 (accessed on 13 June 2024).
- Carr, D.B.; Utzschneider, K.M.; Hull, R.L.; Kodama, K.; Retzlaff, B.M.; Brunzell, J.D.; Shofer, J.B.; Fish, B.E.; Knopp, R.H.; Kahn, S.E. Intra-abdominal fat is a major determinant of the National Cholesterol Education Program Adult Treatment Panel III criteria for the metabolic syndrome. Diabetes 2004, 53, 2087–2094. [Google Scholar] [CrossRef]
- Xue, Y.; Liu, C.; Pang, S.B.; Mao, Z.X.; Zhang, D.D.; Gao, J.J.; Lin, J.S.; Wang, C.J.; Li, X.; Li, W.J. The association between the dietary pattern in abdominal obesity based on visceral fat index and dyslipidaemia in the Henan Rural Cohort Study. Br. J. Nutr. 2022, 128, 762–769. [Google Scholar] [CrossRef]
- Sadeghi, T.; Soltani, N.; Jamali, Z.; Ayoobi, F.; Khalili, P.; Shamsizadeh, A.; Nasirzadeh, M.; Esmaeili-Nadimi, A.; Vecchia, C.L.; Jalali, Z. The prevalence and associated factors of overweight/obesity and abdominal obesity in South-eastern of Iran: A cross-sectional study based on Rafsanjan cohort study. BMC Public Health 2023, 23, 861. [Google Scholar] [CrossRef]
- World Health Organization; Food and Agriculture Organization of the United Nations. What Are Healthy Diets? Joint Statement by the Food and Agriculture Organization of the United Nations and the World Health Organization. 2024. Available online: https://www.who.int/publications/i/item/9789240101876 (accessed on 27 November 2024).
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: At a Glance. 2020. Available online: https://www.who.int/publications/i/item/9789240014886 (accessed on 27 November 2024).
- Guo, Q.; Fang, H.; Zhao, L.; Ju, L.; Xu, X.; Yu, D. Level of Fruit and Vegetable Intake and Its Relationship with Risk for Malnutrition in China’s Adult Labor Force: China Nutrition and Health Surveillance, 2015–2017. Nutrients 2023, 15, 1431. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. 2018. Available online: https://www.who.int/publications/i/item/9789241514187 (accessed on 11 December 2024).
- Yarcheski, A.; Mahon, N.E.; Yarcheski, T.J.; Cannella, B.L. A meta-analysis of predictors of positive health practices. J. Nurs. Scholarsh. 2004, 36, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Pinski, R.B.; Grossman, R.M.; Patterson, T.L.; Nader, P.R. The development of self-efficacy scales for healthrelated diet and exercise behaviors. Health Educ. Res. 1988, 3, 283–292. [Google Scholar] [CrossRef]
- Sallis, J.F.; Grossman, R.M.; Pinski, R.B.; Patterson, T.L.; Nader, P.R. The development of scales to measure social support for diet and exercise behaviors. Prev. Med. 1987, 16, 825–836. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Carraça, E.V.; Marques, M.M.; Rutter, H.; Oppert, J.M.; De Bourdeaudhuij, I.; Lakerveld, J.; Brug, J. Successful behavior change in obesity interventions in adults: A systematic review of self-regulation mediators. BMC Med. 2015, 13, 84. [Google Scholar] [CrossRef] [PubMed]
- Wolfenden, L.; Barnes, C.; Lane, C.; McCrabb, S.; Brown, H.M.; Gerritsen, S.; Barquera, S.; Véjar, L.S.; Munguia, A.; Yoong, S.L. Consolidating evidence on the effectiveness of interventions promoting fruit and vegetable consumption: An umbrella review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 11. [Google Scholar] [CrossRef]
- van der Wardt, V.; di Lorito, C.; Viniol, A. Promoting physical activity in primary care: A systematic review and meta-analysis. Br. J. Gen. Pract. 2021, 71, e399–e405. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Gan, Y.; Hamilton, K.; Schwarzer, R. The Role of Social Support and Self-efficacy for Planning Fruit and Vegetable Intake. J. Nutr. Educ. Behav. 2017, 49, 100–106.e1. [Google Scholar] [CrossRef]
- Lin, H.; Chen, H.; Liu, Q.; Xu, J.; Li, S. A meta-analysis of the relationship between social support and physical activity in adolescents: The mediating role of self-efficacy. Front. Psychol. 2023, 14, 1305425. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Shudo, Y.; Yamaura, K.; Yasuda, J.; Sato, A.; Ebi, K. Dietary self-efficacy and social support interactions in junior athletes’ acquisition of life skills. Front. Sports Act Living 2022, 4, 673633. [Google Scholar] [CrossRef]
- Li, N.; Zhao, S.; Liu, C.; Dai, K.; Huang, W. Exploring the relationship between perceived social support and college students’ autonomous fitness behavior: Chain mediating effect test. Front. Psychol. 2022, 13, 1036383. [Google Scholar] [CrossRef] [PubMed]
- Laursen, B.P.; Hoff, E. Person-Centered and Variable-Centered Approaches to Longitudinal Data. Merrill-Palmer Q. 2006, 52, 377–389. [Google Scholar] [CrossRef]
- Liang, W.; Duan, Y.; Wang, Y.; Lippke, S.; Shang, B.; Lin, Z.; Wulff, H.; Baker, J.S. Psychosocial Mediators of Web-Based Interventions for Promoting a Healthy Lifestyle Among Chinese College Students: Secondary Analysis of a Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, e37563. [Google Scholar] [CrossRef]
- Berlin, K.S.; Williams, N.A.; Parra, G.R. An introduction to latent variable mixture modeling (part 1): Overview and cross-sectional latent class and latent profile analyses. J. Pediatr. Psychol. 2014, 39, 174–187. [Google Scholar] [CrossRef]
- World Health Organization. STEPwise Approach to NCD Risk Factor Surveillance (STEPS): Part 3. Data Collection—Section 5: Physical Measurements. 2017. Available online: https://cdn.who.int/media/docs/default-source/ncds/ncd-surveillance/steps/part3-section5.pdf?sfvrsn=a46653c7_2 (accessed on 27 July 2025).
- Mao, X.; Zeng, X.; Zhong, Q.; Guo, J. Translation and psychometric testing of the simplified version of the health-related diet and exercise self-efficacy scale in China. Health Qual Life Outcomes 2022, 20, 127. [Google Scholar] [CrossRef]
- Mao, X.; Mao, X.; Yu, Y.; Guo, J. Chinese Translation and Psychometric Testing of the Simplified Version of Social Support Scale for Physical Activity. Psychol. Res. Behav. Manag. 2022, 15, 2691–2700. [Google Scholar] [CrossRef]
- Guo, J.; Shi, Z.; Chen, J.L.; Dixon, J.K.; Wiley, J.; Parry, M. Translation and validation of the Canadian diabetes risk assessment questionnaire in China. Public Health Nurs. 2018, 35, 18–28. [Google Scholar] [CrossRef]
- Barr, N.; Corral Rodríguez, A. Latent profile analysis of veterans’ psychological risk and protective factors: Associations with nonroutine military discharge. Psychol. Trauma 2023, 15, 1355–1366. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, M.; Zhang, X.; Zhao, Z.; Li, C.; Yu, M.; Xue, T.; Tan, F.; Wang, L. Trends in Fruit and Vegetable Intake Among the Labor Force Population—China, 2010–2018. China CDC Wkly. 2024, 6, 401–407. [Google Scholar] [CrossRef]
- Lee, S.H.; Moore, L.V.; Park, S.; Harris, D.M.; Blanck, H.M. Adults Meeting Fruit and Vegetable Intake Recommendations—United States, 2019. Morb. Mortal. Wkly. Rep. 2022, 71, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jardim, T.V.; Mozaffarian, D.; Abrahams-Gessel, S.; Sy, S.; Lee, Y.; Liu, J.; Huang, Y.; Rehm, C.; Wilde, P.; Micha, R.; et al. Cardiometabolic disease costs associated with suboptimal diet in the United States: A cost analysis based on a microsimulation model. PLoS Med. 2019, 16, e1002981. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 19 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Zang, J.; Ng, S.W. Age, period and cohort effects on adult physical activity levels from 1991 to 2011 in China. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 40. [Google Scholar] [CrossRef]
- Kaiser, B.L.; Brown, R.L.; Baumann, L.C. Perceived influences on physical activity and diet in low-income adults from two rural counties. Nurs. Res. 2010, 59, 67–75. [Google Scholar] [CrossRef]
- Vaughan, C.A.; Ghosh-Dastidar, M.; Dubowitz, T. Attitudes and Barriers to Healthy Diet and Physical Activity: A Latent Profile Analysis. Health Educ. Behav. 2018, 45, 381–393. [Google Scholar] [CrossRef] [PubMed]
- Prestwich, A.; Kellar, I.; Parker, R.; MacRae, S.; Learmonth, M.; Sykes, B.; Taylor, N.; Castle, H. How can self-efficacy be increased? Meta-analysis of dietary interventions. Health Psychol. Rev. 2014, 8, 270–285. [Google Scholar] [CrossRef] [PubMed]
- Tay, L.; Tan, K.; Diener, E.; Gonzalez, E. Social relations, health behaviors, and health outcomes: A survey and synthesis. Appl. Psychol. Health Well Being 2013, 5, 28–78. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Reed, J.L.; Martinello, N.; Adamo, K.B.; Fodor, J.G.; Hiremath, S.; Kristjansson, E.A.; Mullen, K.A.; Nerenberg, K.A.; Tulloch, H.E.; et al. Why are adult women physically active? A systematic review of prospective cohort studies to identify intrapersonal, social environmental and physical environmental determinants. Obes. Rev. 2016, 17, 919–944. [Google Scholar] [CrossRef] [PubMed]
- Mogre, V.; Johnson, N.A.; Tzelepis, F.; Shaw, J.E.; Paul, C. A systematic review of adherence to diabetes self-care behaviours: Evidence from low- and middle-income countries. J. Adv. Nurs. 2019, 75, 3374–3389. [Google Scholar] [CrossRef]
- Deslippe, A.L.; Soanes, A.; Bouchaud, C.C.; Beckenstein, H.; Slim, M.; Plourde, H.; Cohen, T.R. Barriers and facilitators to diet, physical activity and lifestyle behavior intervention adherence: A qualitative systematic review of the literature. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 14. [Google Scholar] [CrossRef]
- Vettore, M.V.; Stea, T.H.; Zahl-Olsen, R.; Faerstein, E. Longitudinal evidence of the influence of early life circumstances, family characteristics, social ties and psychological distress on healthy behaviours of Brazilian adults: The Pro-Saude cohort study. PLoS ONE 2024, 19, e0306565. [Google Scholar] [CrossRef]
- Li, W.; Wan, Z.; XianYu, Y. Factors influencing nurses self-efficacy two years after the COVID-19 outbreak: A cross-sectional study in Wuhan, China. Medicine 2023, 102, e35059. [Google Scholar] [CrossRef]
- Salinero-Fort, M.Á.; del Otero-Sanz, L.; Martín-Madrazo, C.; de Burgos-Lunar, C.; Chico-Moraleja, R.M.; Rodés-Soldevila, B.; Jiménez-García, R.; Gómez-Campelo, P.; HEALTH & MIGRATION Group. The relationship between social support and self-reported health status in immigrants: An adjusted analysis in the Madrid Cross Sectional Study. BMC Fam. Pract. 2011, 12, 46. [Google Scholar] [CrossRef]
- Jürgensen, I.N.; Koch, P.; Otto, R.; Nock, A.M.; Petersen-Ewert, C. Subjective Health Status, Health-Related Behavior, and Health Literacy of Health Professional Students: Results from a Cross-Sectional Study. Healthcare 2024, 12, 277. [Google Scholar] [CrossRef]
- De Cocker, K.; De Bourdeaudhuij, I.; Cardon, G.; Vandelanotte, C. What are the working mechanisms of a web-based workplace sitting intervention targeting psychosocial factors and action planning? BMC Public Health 2017, 17, 382. [Google Scholar] [CrossRef] [PubMed]
- Fluit, M.; Bortolotti, T.; Broekhuis, M.; van Teerns, M. Segmenting citizens according to their self-sufficiency: A tool for local government. Soc. Sci. Med. 2023, 335, 116246. [Google Scholar] [CrossRef]
- Caperchoine, C.; Mummery, W.K.; Joyner, K. Addressing the challenges, barriers, and enablers to physical activity participation in priority women’s groups. J. Phys. Act. Health 2009, 6, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Peng, F.; Yan, H.; Sharma, M.; Liu, Y.; Lu, Y.; Zhu, S.; Li, P.; Ren, N.; Li, T.; Zhao, Y. Exploring factors influencing whether residents participate in square dancing using social cognitive theory: A cross-sectional survey in Chongqing, China. Medicine 2020, 99, e18685. [Google Scholar] [CrossRef]
- Wang, H.; Dai, X.; Wu, J.; Wu, X.; Nie, X. Influence of urban green open space on residents’ physical activity in China. BMC Public Health 2019, 19, 1093. [Google Scholar] [CrossRef] [PubMed]
- Owolabi, E.O.; Ajayi, A.I. Adherence to medication, dietary and physical activity recommendations: Findings from a multicenter cross-sectional study among adults with diabetes in rural South Africa. J. Eval. Clin. Pract. 2024, 30, 1261–1271. [Google Scholar] [CrossRef]
- League of American Bicyclists. National: Demographics of Biking & Walking. Available online: https://data.bikeleague.org/data/national-demographics-of-active-transportation/ (accessed on 17 July 2025).
- Beltrán-Sánchez, H.; Pebley, A.; Goldman, N. Links between Primary Occupation and Functional Limitations among Older Adults in Mexico. SSM Popul. Health 2017, 3, 382–392. [Google Scholar] [CrossRef]
- Cui, Q.; Xia, Y.; Wu, Q.; Chang, Q.; Niu, K.; Zhao, Y. Validity of the food frequency questionnaire for adults in nutritional epidemiological studies: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2023, 63, 1670–1688. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | n (%) | M (IQR a) |
|---|---|---|
| Age, years | 36.00 (33.00, 40.00) | |
| Residence | ||
| Urban | 240 (73.4) | |
| Rural | 87 (26.6) | |
| Ethnicity | ||
| Han Chinese | 300 (91.7) | |
| Minority | 27 (8.3) | |
| Marital status | ||
| Married | 322 (98.5) | |
| Single | 5 (1.5) | |
| Education | ||
| 9 years or less | 86 (26.3) | |
| 10 years or more | 241 (73.7) | |
| Occupation | ||
| Part-time job or no job | 219 (67.0) | |
| Full-time job | 108 (33.0) | |
| Monthly income | ||
| ≤1500 RMB (233 dollars) | 81 (24.8) | |
| >1500 RMB (233 dollars) | 246 (75.2) | |
| Number of pregnancies | 2.00 (2.00, 3.00) | |
| Age of the youngest child | ||
| 1–5 years | 123 (37.6) | |
| 6–12 years | 204 (62.4) | |
| WC b, cm | 86.00 (82.00, 93.00) | |
| BMI c | ||
| <24.0 | 140 (42.8) | |
| 24.0–27.9 | 125 (38.2) | |
| ≥28.0 | 62 (19.0) | |
| With any chronic disease | ||
| No | 165 (50.5) | |
| Yes | 162 (49.5) | |
| Family history of diabetes | ||
| No | 267 (81.7) | |
| Yes | 60 (18.3) | |
| Family history of CVD d | ||
| No | 275 (84.1) | |
| Yes | 52 (15.9) | |
| Family history of hypertension | ||
| No | 192 (58.7) | |
| Yes | 135 (41.3) |
| Variables | Profiles | AIC a | BIC b | aBIC c | LMR d | BLRT e | Entropy | Category Probability | Case Number |
|---|---|---|---|---|---|---|---|---|---|
| Diet-related self-efficacy and social support | 1 | 3255.622 | 3270.782 | 3258.094 | — — | — — | — — | 1 | 327 |
| 2 | 3238.975 | 3265.505 | 3243.301 | p < 0.01 | p < 0.01 | 0.916 | 0.963/0.037 | 315/12 | |
| 3 | 3234.859 | 3272.759 | 3241.039 | p = 0.257 | p = 0.05 | 0.780 | 0.107/0.841/0.052 | 35/275/17 | |
| 4 | 3229.831 | 3279.101 | 3237.865 | p < 0.05 | p < 0.05 | 0.821 | 0.046/0.055/0.847/0.052 | 15/18/277/17 | |
| 5 | 3230.968 | 3291.607 | 3240.856 | p = 0.612 | p = 0.375 | 0.722 | 0.768/0.055/0.07/0.067/0.040 | 251/18/23/22/13 | |
| Exercise-related self-efficacy and social support | 1 | 3740.222 | 3755.382 | 3742.694 | — — | — — | — — | 1 | 327 |
| 2 | 3666.209 | 3692.738 | 3670.535 | p < 0.01 | p < 0.01 | 0.561 | 0.529/0.471 | 173/154 | |
| 3 | 3649.924 | 3687.824 | 3656.104 | p = 0.251 | p < 0.01 | 0.671 | 0.572/0.080/0.349 | 187/26/114 | |
| 4 | 3645.926 | 3695.195 | 3653.960 | p = 0.729 | p = 0.146 | 0.779 | 0.125/0.119/0.443/0.312 | 41/39/145/102 | |
| 5 | 3579.451 | 3640.090 | 3589.339 | p < 0.01 | p < 0.01 | 0.918 | 0.122/0.281/0.364/0.180/0.052 | 40/92/119/59/17 |
| Variables | p | OR | 95% CI |
|---|---|---|---|
| Profiles of diet-SE and diet-SS | |||
| Diet Dual-Low Group | 0.015 | 0.129 | (0.025, 0.672) |
| Diet-SE Medium Group | 0.490 | 0.693 | (0.244, 1.964) |
| Diet-SE High Group | 0.712 | 1.340 | (0.284, 6.319) |
| (Ref. Diet Dual-Medium Group) | |||
| Age | 0.248 | 1.028 | (0.981, 1.078) |
| Residence | |||
| Urban | 0.527 | 1.213 | (0.667, 2.206) |
| (Ref. Rural) | |||
| Ethnicity | |||
| Han Chinese | 0.823 | 1.104 | (0.463, 2.632) |
| (Ref. Minority) | |||
| Marital status | |||
| Married | 0.864 | 0.841 | (0.115, 6.145) |
| (Ref. Single) | |||
| Education | |||
| 9 years or less | 0.082 | 0.546 | (0.276, 1.080) |
| (Ref. 10 years or more) | |||
| Occupation | |||
| Part-time job or no job | 0.262 | 1.383 | (0.785, 2.438) |
| (Ref. Full-time job) | |||
| Monthly income | |||
| ≤233 dollars | 0.256 | 1.441 | (0.767, 2.706) |
| (Ref. > 233 dollars) | |||
| Number of pregnancies | 0.187 | 0.863 | (0.693, 1.074) |
| Age of the youngest child | |||
| 1–5 years | 0.484 | 0.825 | (0.482, 1.413) |
| (Ref. 6–12 years) | |||
| WC a | 0.921 | 1.002 | (0.968, 1.036) |
| BMI b | |||
| <24.0 | 0.972 | 0.987 | (0.461, 2.112) |
| 24.0–27.9 | 0.131 | 0.573 | (0.278, 1.179) |
| (Ref. ≥ 28.0) | |||
| With any chronic disease | |||
| No | 0.013 | 1.852 | (1.140, 3.008) |
| (Ref. Yes) | |||
| Family history of diabetes | |||
| No | 0.301 | 0.723 | (0.392, 1.336) |
| (Ref. Yes) | |||
| Family history of CVD c | |||
| No | 0.836 | 0.932 | (0.481, 1.808) |
| (Ref. Yes) | |||
| Family history of hypertension | |||
| No | 0.509 | 1.182 | (0.719, 1.943) |
| (Ref. Yes) |
| Outcome * | Variables | p | OR | 95% CI |
|---|---|---|---|---|
| Profiles of Diet-SE and Diet-SS | Ethnicity | |||
| Han Chinese | 0.058 | 0.278 | (0.074, 1.042) | |
| (Ref. Minority) | ||||
| Marital status | ||||
| Married | 0.011 | 0.061 | (0.007, 0.525) | |
| (Ref. Divorced/widowed) | ||||
| Monthly income | ||||
| ≤233 dollars | 0.003 | 4.735 | (1.702, 13.171) | |
| (Ref. > 233 dollars) | ||||
| Profiles of Exercise-SE and Exercise-SS | Occupation | |||
| Part-time job or no job | 0.047 | 0.602 | (0.364, 0.994) | |
| (Ref. Full-time job) | ||||
| Monthly income | ||||
| ≤233 dollars | 0.037 | 0.541 | (0.304, 0.964) | |
| (Ref. > 233 dollars) | ||||
| With any chronic disease | ||||
| No | 0.004 | 0.506 | (0.316, 0.809) | |
| (Ref. Yes) |
| Variables | p | OR | 95% CI |
|---|---|---|---|
| Profiles of Exercise-SE and Exercise-SS | |||
| Exercise Dual-Low Group | <0.001 | 0.046 | (0.010, 0.213) |
| Exercise-SS Medium–Low Group | 0.002 | 0.136 | (0.037, 0.495) |
| Exercise Dual-Medium–Low Group | 0.097 | 0.347 | (0.099, 1.213) |
| Exercise Dual-Medium–High Group | 0.642 | 1.388 | (0.349, 5.527) |
| (Ref. Exercise-SE High Group) | |||
| Age | 0.025 | 1.060 | (1.007, 1.115) |
| Residence | |||
| Urban | 0.484 | 0.787 | (0.403, 1.539) |
| (Ref. Rural) | |||
| Ethnicity | |||
| Han Chinese | 0.155 | 0.523 | (0.214, 1.279) |
| (Ref. Minority) | |||
| Marital status | |||
| Married | 0.920 | 1.114 | (0.136, 9.131) |
| (Ref. Single) | |||
| Education | |||
| 9 years or less | 0.150 | 0.566 | (0.261, 1.229) |
| (Ref. 10 years or more) | |||
| Occupation | |||
| Part-time job or no job | 0.123 | 1.632 | (0.876, 3.038) |
| (Ref. Full-time job) | |||
| Monthly income | |||
| ≤233 dollars | 0.112 | 1.770 | (0.875, 3.581) |
| (Ref. > 233 dollars) | |||
| Number of pregnancies | 0.166 | 0.842 | (0.660, 1.074) |
| Age of the youngest child | |||
| 1–5 years | 0.229 | 1.444 | (0.794, 2.629) |
| (Ref. 6–12 years) | |||
| WC a | 0.915 | 1.002 | (0.966, 1.040) |
| BMI b | |||
| <24.0 | 0.568 | 1.281 | (0.548, 2.993) |
| 24.0–27.9 | 0.664 | 1.193 | (0.538, 2.647) |
| (Ref. ≥ 28.0) | |||
| With any chronic disease | |||
| No | 0.057 | 1.689 | (0.984, 2.899) |
| (Ref. Yes) | |||
| Family history of diabetes | |||
| No | 0.458 | 0.773 | (0.392, 1.524) |
| (Ref. Yes) | |||
| Family history of CVD c | |||
| No | 0.798 | 0.908 | (0.434, 1.900) |
| (Ref. Yes) | |||
| Family history of hypertension | |||
| No | 0.711 | 0.902 | (0.522, 1.559) |
| (Ref. Yes) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeng, Y.; Long, Q.; Jiang, Y.; Li, J.; Rao, Z.; Zhong, J.; Guo, J. The Profiles of Diet- or Exercise-Related Self-Efficacy and Social Support Associated with Insufficient Fruit/Vegetable Intake and Exercise in Women with Abdominal Obesity. Nutrients 2025, 17, 2478. https://doi.org/10.3390/nu17152478
Zeng Y, Long Q, Jiang Y, Li J, Rao Z, Zhong J, Guo J. The Profiles of Diet- or Exercise-Related Self-Efficacy and Social Support Associated with Insufficient Fruit/Vegetable Intake and Exercise in Women with Abdominal Obesity. Nutrients. 2025; 17(15):2478. https://doi.org/10.3390/nu17152478
Chicago/Turabian StyleZeng, Yanjing, Qing Long, Yan Jiang, Jieqian Li, Zhenzhen Rao, Jie Zhong, and Jia Guo. 2025. "The Profiles of Diet- or Exercise-Related Self-Efficacy and Social Support Associated with Insufficient Fruit/Vegetable Intake and Exercise in Women with Abdominal Obesity" Nutrients 17, no. 15: 2478. https://doi.org/10.3390/nu17152478
APA StyleZeng, Y., Long, Q., Jiang, Y., Li, J., Rao, Z., Zhong, J., & Guo, J. (2025). The Profiles of Diet- or Exercise-Related Self-Efficacy and Social Support Associated with Insufficient Fruit/Vegetable Intake and Exercise in Women with Abdominal Obesity. Nutrients, 17(15), 2478. https://doi.org/10.3390/nu17152478