
The Association between Grazing and Food Addiction: The Italian Version of the Repetitive Eating Questionnaire (Rep(Eat)-Q) and Its Relationships with Food Addiction Criteria
 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Translation and Cultural Adaptation
2.2. Sample Size Determination
2.3. Procedure
2.4. Participants
2.5. Measures
2.5.1. The Repetitive Eating Questionnaire (Rep(Eat)-Q)
2.5.2. The Modified Yale Food Addiction Scale 2.0 (mYFAS 2.0)
2.5.3. The Binge Eating Scale (BES)
2.5.4. The Measure of Eating Compulsivity (MEC10)
2.5.5. The Three-Factor Eating Questionnaire Revised—18 (TFEQ-R-18)
2.6. Statistical Analysis
3. Results
3.1. Part I: Psychometric Properties of the Italian Rep(Eat)-Q
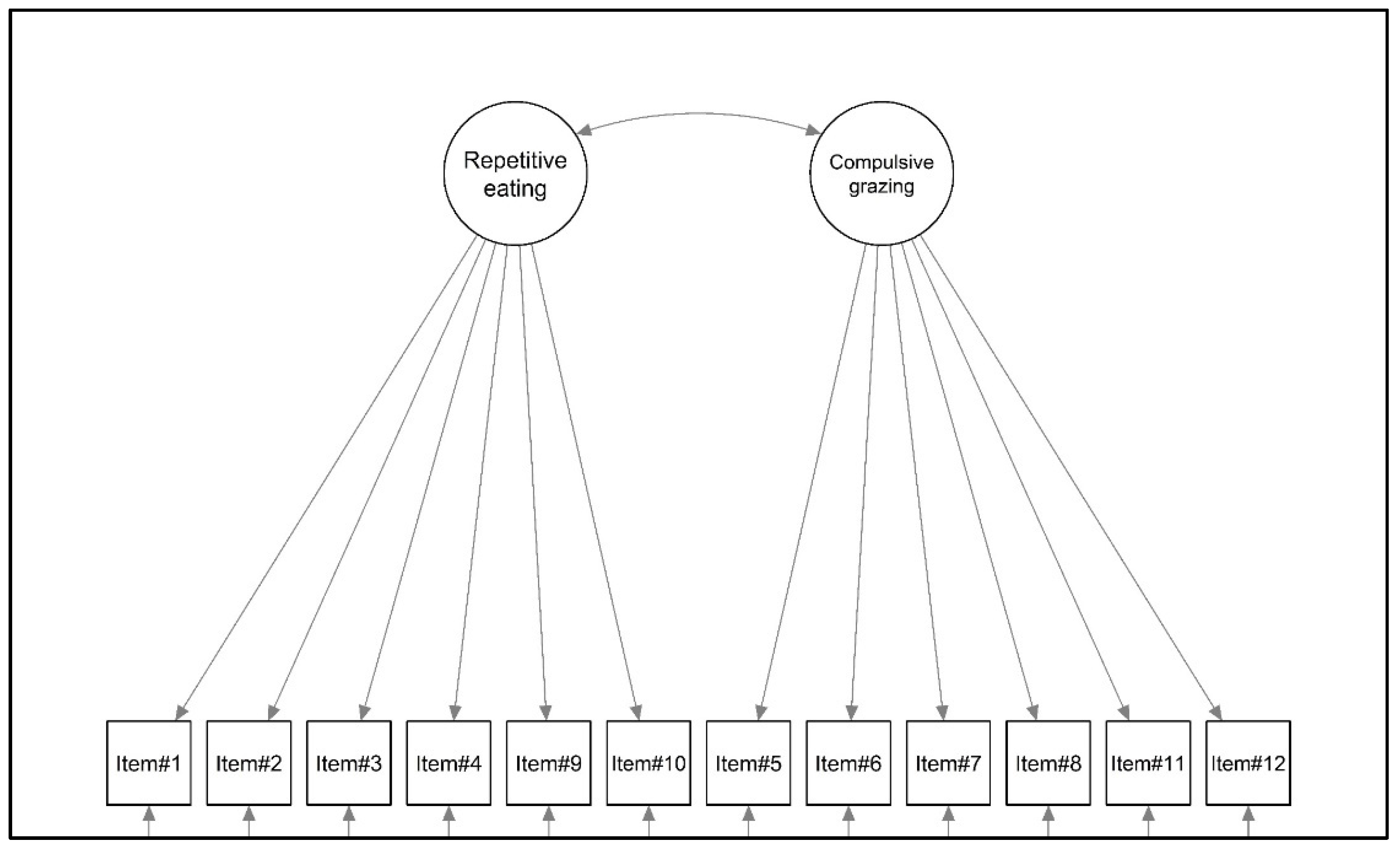
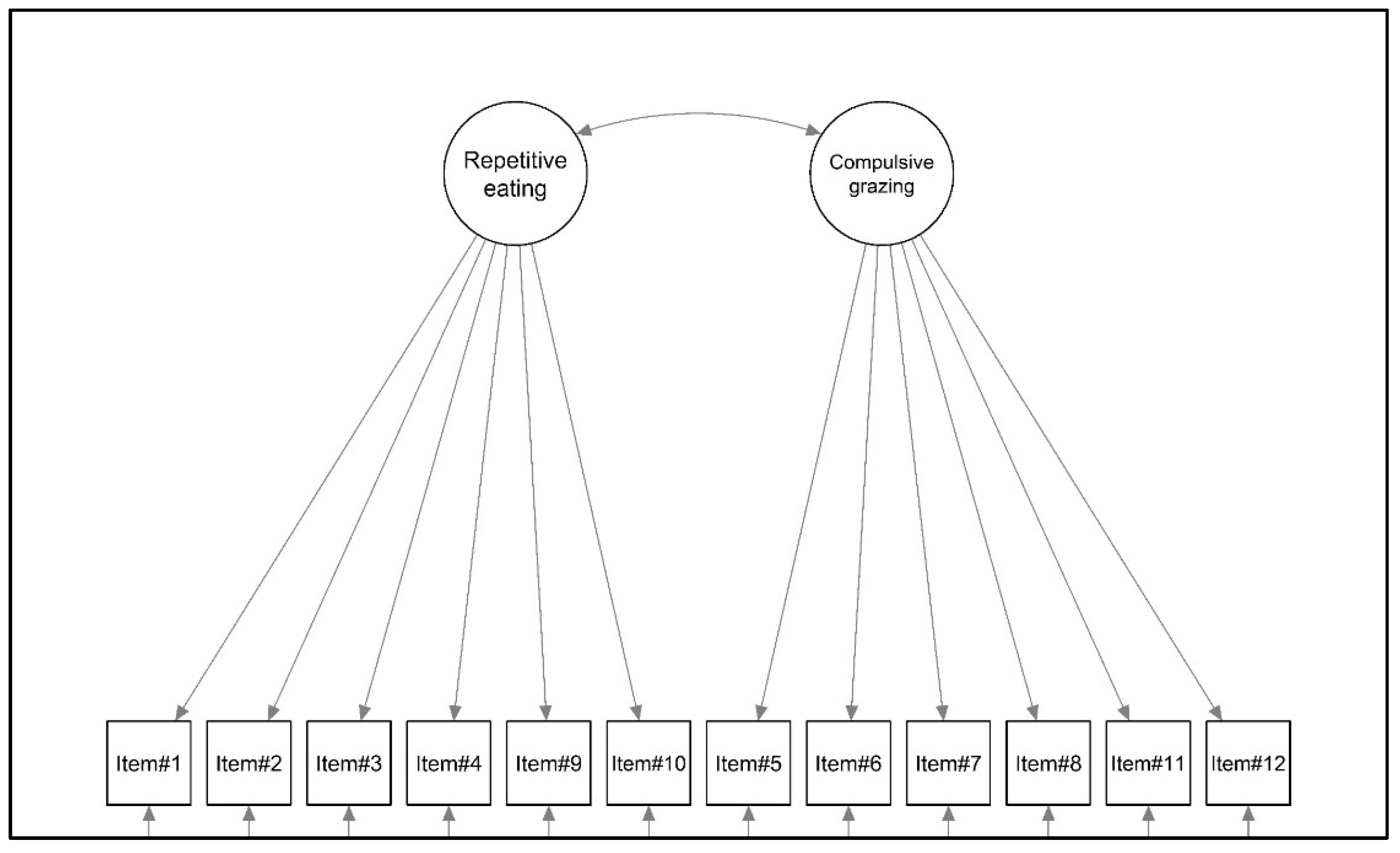
3.1.1. Structural Validity
3.1.2. Internal Consistency
3.1.3. Convergent Validity
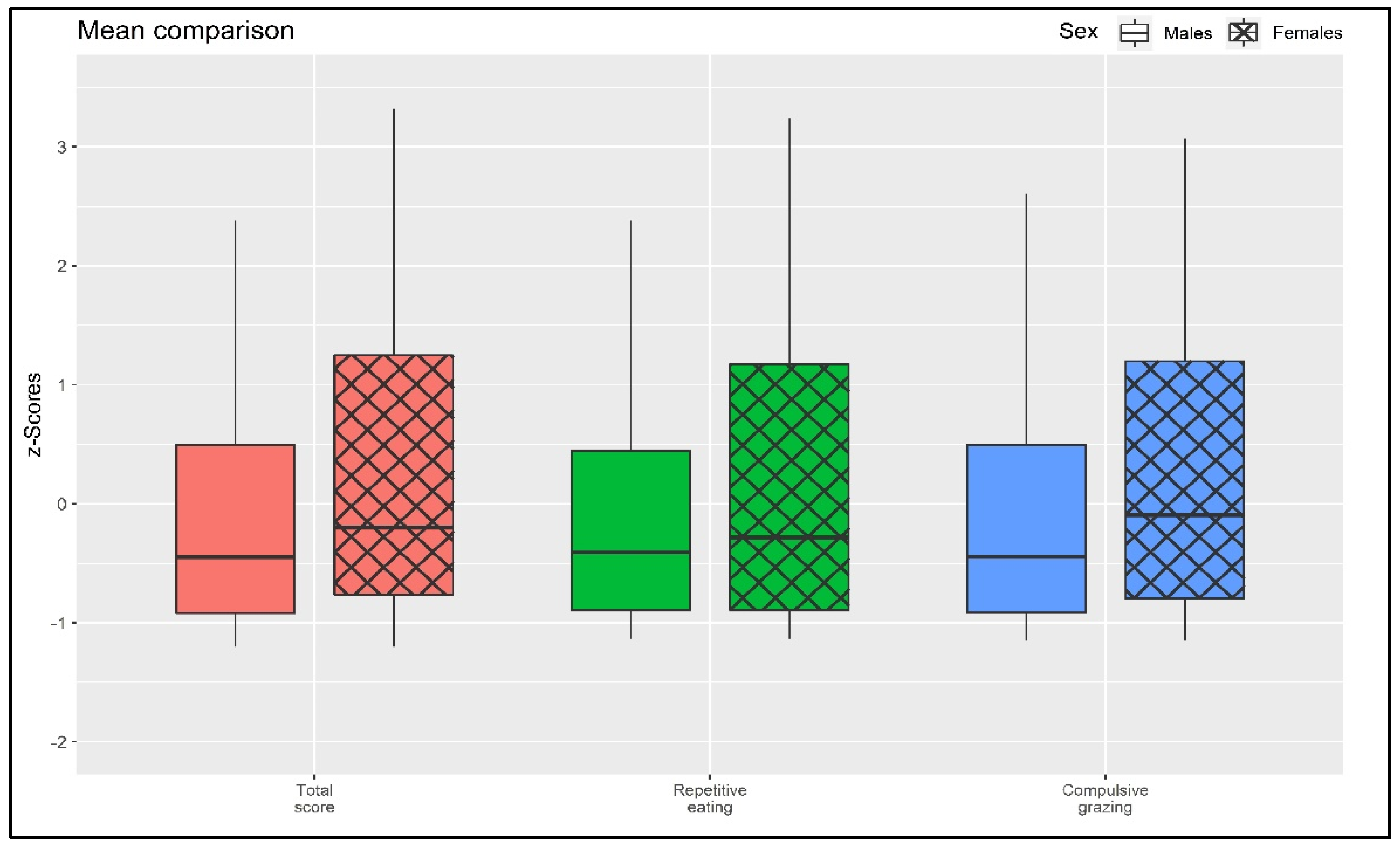
3.1.4. Differences between Males and Females
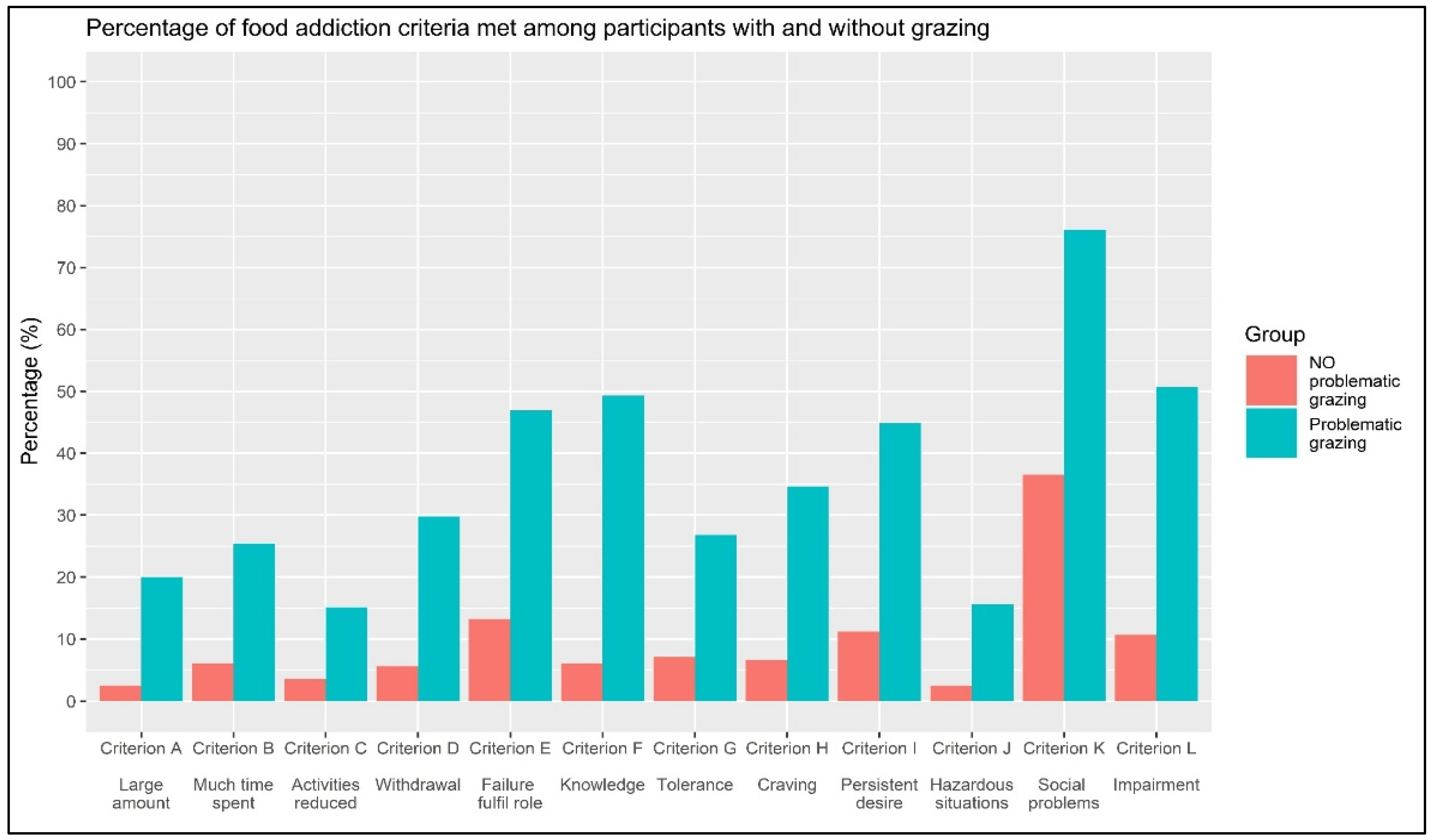
3.2. Part II: Association between Grazing and Food Addiction Criteria
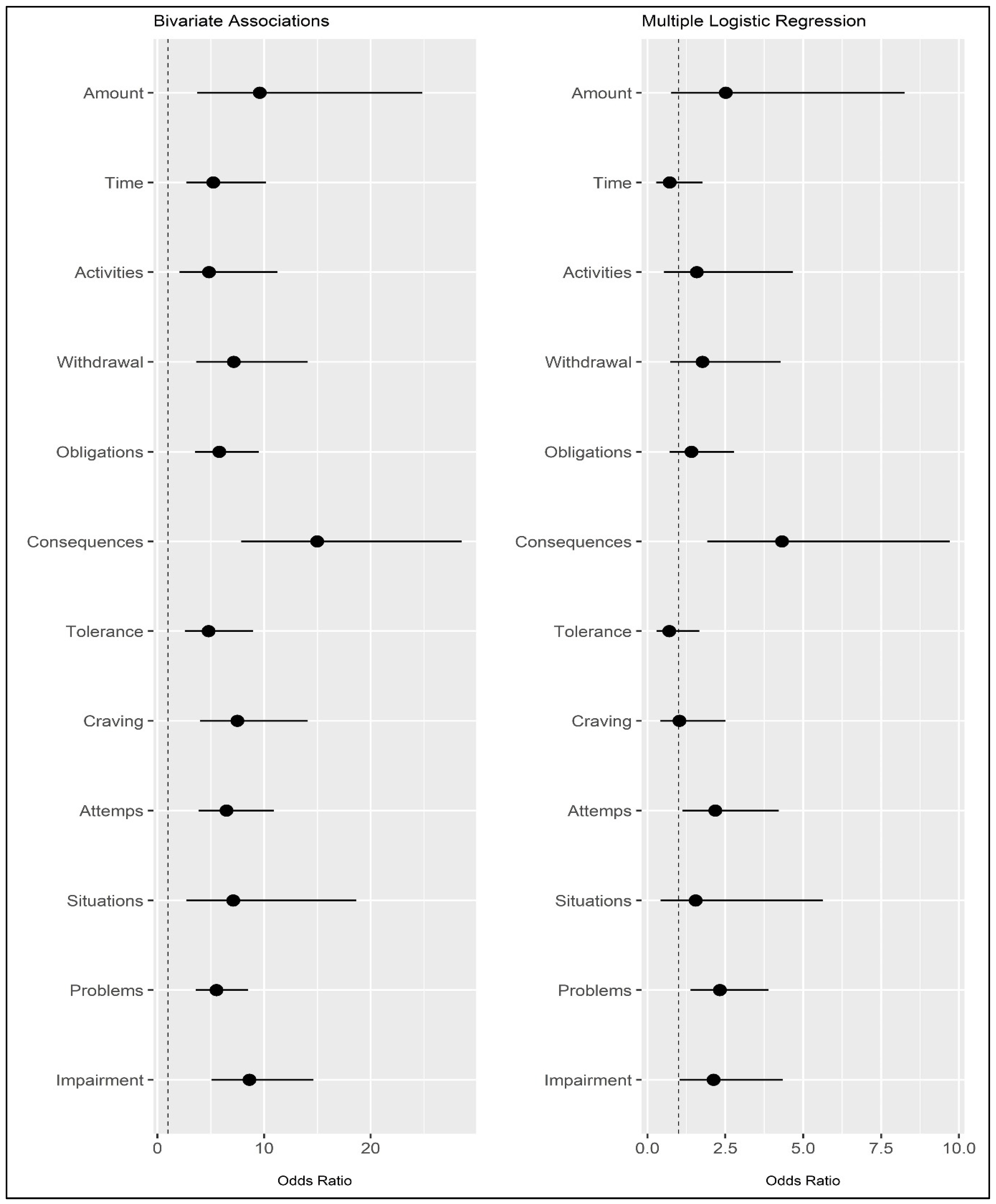
3.2.1. Bivariate Associations
3.2.2. Logistic Regression Analysis
4. Discussion
4.1. Limitations and Strengths
4.2. Clinical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Corsica, J.A.; Perri, M.G. Obesity. In Handbook of Psychology: Health Psychology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2003; Volume 9, pp. 121–145. ISBN 978-0-471-38514-1. [Google Scholar]
- Liu, Y.; Song, Y.; Hao, Q.; Wu, J. Global Prevalence of Osteosarcopenic Obesity amongst Middle Aged and Older Adults: A Systematic Review and Meta-Analysis. Arch. Osteoporos. 2023, 18, 60. [Google Scholar] [CrossRef]
- Heeren, F.A.N.; Darcey, V.L.; Deemer, S.E.; Menon, S.; Tobias, D.; Cardel, M.I. Breaking down Silos: The Multifaceted Nature of Obesity and the Future of Weight Management. Philos. Trans. R. Soc. B Biol. Sci. 2023, 378, 20220215. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Serdula, M.K.; Dietz, W.H.; Bowman, B.A.; Marks, J.S.; Koplan, J.P. The Continuing Epidemic of Obesity in the United States. JAMA 2000, 284, 1650–1651. [Google Scholar] [CrossRef]
- Haslam, D.W.; James, W.P.T. Obesity. Lancet 2005, 366, 1197–1209. [Google Scholar] [CrossRef]
- Wang, Y.; Beydoun, M.A.; Liang, L.; Caballero, B.; Kumanyika, S.K. Will All Americans Become Overweight or Obese? Estimating the Progression and Cost of the US Obesity Epidemic. Obesity 2008, 16, 2323–2330. [Google Scholar] [CrossRef]
- Sturmberg, J.P. Obesity—A Multifaceted Approach: One Problem—Different Models—Different Insights and Solutions. In Health System Redesign: How to Make Health Care Person-Centered, Equitable, and Sustainable; Sturmberg, J.P., Ed.; Springer International Publishing: Cham, Switzerland, 2018; pp. 213–232. ISBN 978-3-319-64605-3. [Google Scholar]
- Mandlik, M.; Oetzel, J.G.; Kadirov, D. Obesity and Health Care Interventions: Substantiating a Multi-Modal Challenge through the Lens of Grounded Theory. Health Promot. J. Austr. 2021, 32, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Schultes, B.; Ernst, B.; Hallschmid, M.; Bueter, M.; Meyhöfer, S.M. The ‘Behavioral Balance Model’: A New Perspective on the Aetiology and Therapy of Obesity. Diabetes Obes. Metab. 2023, 25, 3444–3452. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.M.H.; Fay, A.; Saules, K.K. Foods and Nutritional Characteristics Associated with Addictive-Like Eating. Psychol. Rep. 2022, 125, 1937–1956. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; DiFeliceantonio, A.G. The Risks of Misclassifying Addictive Food Substances as Non-Addictive. Addiction 2023, 118, 605–606. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; DiFeliceantonio, A.G. Highly Processed Foods Can Be Considered Addictive Substances Based on Established Scientific Criteria. Addiction 2023, 118, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Hebebrand, J. The Concept of “Food Addiction” Helps Inform the Understanding of Overeating and Obesity: Debate Consensus. Am. J. Clin. Nutr. 2021, 113, 274–276. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; White, M.A.; Masheb, R.M.; Morgan, P.T.; Crosby, R.D.; Grilo, C.M. An Examination of the Food Addiction Construct in Obese Patients with Binge Eating Disorder. Int. J. Eat. Disord. 2012, 45, 657–663. [Google Scholar] [CrossRef]
- Schulte, E.M.; Joyner, M.A.; Potenza, M.N.; Grilo, C.M.; Gearhardt, A.N. Current Considerations Regarding Food Addiction. Curr. Psychiatry Rep. 2015, 17, 563. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Gearhardt, A.N. Food Addiction in the Light of DSM-5. Nutrients 2014, 6, 3653–3671. [Google Scholar] [CrossRef]
- Meule, A.; Hermann, T.; Kübler, A. Food Addiction in Overweight and Obese Adolescents Seeking Weight-Loss Treatment. Eur. Eat. Disord. Rev. 2015, 23, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Davis, C. Compulsive Overeating as an Addictive Behavior: Overlap Between Food Addiction and Binge Eating Disorder. Curr. Obes. Rep. 2013, 2, 171–178. [Google Scholar] [CrossRef]
- Meule, A.; Gearhardt, A.N. Five Years of the Yale Food Addiction Scale: Taking Stock and Moving Forward. Curr. Addict. Rep. 2014, 1, 193–205. [Google Scholar] [CrossRef]
- Schulte, E.M.; Wadden, T.A.; Allison, K.C. An Evaluation of Food Addiction as a Distinct Psychiatric Disorder. Int. J. Eat. Disord. 2020, 53, 1610–1622. [Google Scholar] [CrossRef]
- Gordon, E.L.; Ariel-Donges, A.H.; Bauman, V.; Merlo, L.J. What Is the Evidence for “Food Addiction?” A Systematic Review. Nutrients 2018, 10, 477. [Google Scholar] [CrossRef]
- Hebebrand, J.; Albayrak, Ö.; Adan, R.; Antel, J.; Dieguez, C.; de Jong, J.; Leng, G.; Menzies, J.; Mercer, J.G.; Murphy, M.; et al. “Eating Addiction”, Rather than “Food Addiction”, Better Captures Addictive-like Eating Behavior. Neurosci. Biobehav. Rev. 2014, 47, 295–306. [Google Scholar] [CrossRef]
- Albayrak, Ö.; Wölfle, S.M.; Hebebrand, J. Does Food Addiction Exist? A Phenomenological Discussion Based on the Psychiatric Classification of Substance-Related Disorders and Addiction. Obes. Facts 2012, 5, 165–179. [Google Scholar] [CrossRef] [PubMed]
- Manzoni, G.M.; Rossi, A.; Pietrabissa, G.; Mannarini, S.; Fabbricatore, M.; Imperatori, C.; Innamorati, M.; Gearhardt, A.N.; Castelnuovo, G. Structural Validity, Measurement Invariance, Reliability and Diagnostic Accuracy of the Italian Version of the Yale Food Addiction Scale 2.0 in Patients with Severe Obesity and the General Population. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2021, 26, 345–366. [Google Scholar] [CrossRef]
- Abiri, B.; Valizadeh, M.; Nasreddine, L.; Hosseinpanah, F. Dietary Determinants of Healthy/Unhealthy Metabolic Phenotype in Individuals with Normal Weight or Overweight/Obesity: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2023, 63, 5856–5873. [Google Scholar] [CrossRef] [PubMed]
- Al-Jawaldeh, A.; Abbass, M.M.S. Unhealthy Dietary Habits and Obesity: The Major Risk Factors Beyond Non-Communicable Diseases in the Eastern Mediterranean Region. Front. Nutr. 2022, 9, 817808. [Google Scholar] [CrossRef] [PubMed]
- Seifu, C.N.; Fahey, P.P.; Hailemariam, T.G.; Frost, S.A.; Atlantis, E. Dietary Patterns Associated with Obesity Outcomes in Adults: An Umbrella Review of Systematic Reviews. Public Health Nutr. 2021, 24, 6390–6414. [Google Scholar] [CrossRef] [PubMed]
- Brytek-Matera, A.; Obeid, S.; Akel, M.; Hallit, S. How Does Food Addiction Relate to Obesity? Patterns of Psychological Distress, Eating Behaviors and Physical Activity in a Sample of Lebanese Adults: The MATEO Study. Int. J. Environ. Res. Public. Health 2021, 18, 10979. [Google Scholar] [CrossRef] [PubMed]
- Romero-Blanco, C.; Hernández-Martínez, A.; Parra-Fernández, M.L.; Onieva-Zafra, M.D.; Prado-Laguna, M.d.C.; Rodríguez-Almagro, J. Food Addiction and Lifestyle Habits among University Students. Nutrients 2021, 13, 1352. [Google Scholar] [CrossRef]
- Pachucki, M.A. Food Pattern Analysis over Time: Unhealthful Eating Trajectories Predict Obesity. Int. J. Obes. 2012, 36, 686–694. [Google Scholar] [CrossRef]
- Schulte, E.M.; Avena, N.M.; Gearhardt, A.N. Which Foods May Be Addictive? The Roles of Processing, Fat Content, and Glycemic Load. PLoS ONE 2015, 10, e0117959. [Google Scholar] [CrossRef]
- Schulte, E.M.; Smeal, J.K.; Lewis, J.; Gearhardt, A.N. Development of the Highly Processed Food withdrawal Scale. Appetite 2018, 131, 148–154. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA Food Classification and the Trouble with Ultra-Processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef]
- García-García, I.; Horstmann, A.; Jurado, M.A.; Garolera, M.; Chaudhry, S.J.; Margulies, D.S.; Villringer, A.; Neumann, J. Reward Processing in Obesity, Substance Addiction and Non-Substance Addiction. Obes. Rev. 2014, 15, 853–869. [Google Scholar] [CrossRef]
- Rogers, P.J. Food and Drug Addictions: Similarities and Differences. Pharmacol. Biochem. Behav. 2017, 153, 182–190. [Google Scholar] [CrossRef]
- Onaolapo, A.Y.; Onaolapo, O.J. Food Additives, Food and the Concept of ‘Food Addiction’: Is Stimulation of the Brain Reward Circuit by Food Sufficient to Trigger Addiction? Pathophysiology 2018, 25, 263–276. [Google Scholar] [CrossRef]
- Volkow, N.D.; Wise, R.A.; Baler, R. The Dopamine Motive System: Implications for Drug and Food Addiction. Nat. Rev. Neurosci. 2017, 18, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Loxton, N.J.; Levitan, R.D.; Kaplan, A.S.; Carter, J.C.; Kennedy, J.L. ‘Food Addiction’ and Its Association with a Dopaminergic Multilocus Genetic Profile. Physiol. Behav. 2013, 118, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Parnarouskis, L.; Leventhal, A.M.; Ferguson, S.G.; Gearhardt, A.N. withdrawal: A Key Consideration in Evaluating Whether Highly Processed Foods Are Addictive. Obes. Rev. 2022, 23, e13507. [Google Scholar] [CrossRef] [PubMed]
- Parnarouskis, L.; Gearhardt, A.N. Preliminary Evidence That Tolerance and withdrawal Occur in Response to Ultra-Processed Foods. Curr. Addict. Rep. 2022, 9, 282–289. [Google Scholar] [CrossRef]
- Gilbert, D.G.; Gilbert, B.O.; Schultz, V.L. withdrawal Symptoms: Individual Differences and Similarities across Addictive Behaviors. Pers. Individ. Differ. 1998, 24, 351–356. [Google Scholar] [CrossRef]
- Dingemans, A.; Danner, U.; Parks, M. Emotion Regulation in Binge Eating Disorder: A Review. Nutrients 2017, 9, 1274. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Richard, A.; Schnepper, R.; Reichenberger, J.; Georgii, C.; Naab, S.; Voderholzer, U.; Blechert, J. Emotion Regulation and Emotional Eating in Anorexia Nervosa and Bulimia Nervosa. Eat. Disord. 2021, 29, 175–191. [Google Scholar] [CrossRef]
- Reichenberger, J.; Schnepper, R.; Arend, A.-K.; Blechert, J. Emotional Eating in Healthy Individuals and Patients with an Eating Disorder: Evidence from Psychometric, Experimental and Naturalistic Studies. Proc. Nutr. Soc. 2020, 79, 290–299. [Google Scholar] [CrossRef]
- Konttinen, H. Emotional Eating and Obesity in Adults: The Role of Depression, Sleep and Genes. Proc. Nutr. Soc. 2020, 79, 283–289. [Google Scholar] [CrossRef]
- Brewerton, T.D. Food Addiction as a Proxy for Eating Disorder and Obesity Severity, Trauma History, PTSD Symptoms, and Comorbidity. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2017, 22, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Development of the Yale Food Addiction Scale Version 2.0. Psychol. Addict. Behav. 2016, 30, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Gearhardt, A.N.; Castelnuovo, G.; Mannarini, S. Different Methods of Assessment, Food Addiction, Emotional Eating, and Binge Eating Behaviors: Comparing the Total Model Effects of Sequential Mediation Analysis. CEUR Workshop Proc. 2020, 2730. [Google Scholar]
- Colles, S.L.; Dixon, J.B.; O’Brien, P.E. Grazing and Loss of Control Related to Eating: Two High-Risk Factors Following Bariatric Surgery. Obesity 2008, 16, 615–622. [Google Scholar] [CrossRef]
- Moore, C.F.; Sabino, V.; Koob, G.F.; Cottone, P. Pathological Overeating: Emerging Evidence for a Compulsivity Construct. Neuropsychopharmacology 2017, 42, 1375–1389. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.F.; Sabino, V.; Koob, G.F.; Cottone, P. Chapter 3—Dissecting Compulsive Eating Behavior into Three Elements. In Compulsive Eating Behavior and Food Addiction; Cottone, P., Sabino, V., Moore, C.F., Koob, G.F., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 41–81. ISBN 978-0-12-816207-1. [Google Scholar]
- Moore, C.F.; Sabino, V.; Koob, G.F.; Cottone, P. Chapter 4—Habitual Overeating. In Compulsive Eating Behavior and Food Addiction; Cottone, P., Sabino, V., Moore, C.F., Koob, G.F., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 83–95. ISBN 978-0-12-816207-1. [Google Scholar]
- Rossi, A.A.; Mannarini, S.; Castelnuovo, G.; Pietrabissa, G. Disordered Eating Behaviors Related to Food Addiction/Eating Addiction in Inpatients with Obesity and the General Population: The Italian Version of the Addiction-like Eating Behaviors Scale (AEBS-IT). Nutrients 2023, 15, 104. [Google Scholar] [CrossRef]
- Rossi, A.A.; Pietrabissa, G.; Gearhardt, A.N.; Musetti, A.; Castelnuovo, G.; Mannarini, S. Eating Compulsivity in Inpatients with Severe Obesity and the General Population: The Italian Version of the Measure of Eating Compulsivity (MEC10-IT). Nutrients 2023, 15, 1378. [Google Scholar] [CrossRef]
- Conceição, E.M.; Mitchell, J.E.; Machado, P.P.P.; Vaz, A.R.; Pinto-Bastos, A.; Ramalho, S.; Brandão, I.; Simões, J.B.; de Lourdes, M.; Freitas, A.C. Repetitive Eating Questionnaire [Rep(Eat)-Q]: Enlightening the Concept of Grazing and Psychometric Properties in a Portuguese Sample. Appetite 2017, 117, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Bonder, R.; Davis, C.; Kuk, J.L.; Loxton, N.J. Compulsive “Grazing” and Addictive Tendencies towards Food. Eur. Eat. Disord. Rev. 2018, 26, 569–573. [Google Scholar] [CrossRef]
- Heriseanu, A.I.; Hay, P.; Touyz, S. The Short Inventory of Grazing (SIG): Development and Validation of a New Brief Measure of a Common Eating Behaviour with a Compulsive Dimension. J. Eat. Disord. 2019, 7, 4. [Google Scholar] [CrossRef]
- Conceição, E.M.; Mitchell, J.E.; Engel, S.G.; Machado, P.P.P.; Lancaster, K.; Wonderlich, S.A. What Is “Grazing”? Reviewing Its Definition, Frequency, Clinical Characteristics, and Impact on Bariatric Surgery Outcomes, and Proposing a Standardized Definition. Surg. Obes. Relat. Dis. 2014, 10, 973–982. [Google Scholar] [CrossRef]
- Heriseanu, A.I.; Hay, P.; Touyz, S. Grazing Behaviour and Associations with Obesity, Eating Disorders, and Health-Related Quality of Life in the Australian Population. Appetite 2019, 143, 104396. [Google Scholar] [CrossRef]
- Conceição, E.M.; Utzinger, L.M.; Pisetsky, E.M. Eating Disorders and Problematic Eating Behaviours Before and After Bariatric Surgery: Characterization, Assessment and Association with Treatment Outcomes. Eur. Eat. Disord. Rev. 2015, 23, 417–425. [Google Scholar] [CrossRef]
- Poole, N.A.; Atar, A.A.; Kuhanendran, D.; Bidlake, L.; Fiennes, A.; McCluskey, S.; Nussey, S.; Bano, G.; Morgan, J.F. Compliance with Surgical After-Care Following Bariatric Surgery for Morbid Obesity: A Retrospective Study. Obes. Surg. 2005, 15, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Timothy Garvey, W.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures—2019 Update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society for Metabolic and Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Obesity 2020, 28, O1–O58. [Google Scholar] [CrossRef] [PubMed]
- Conceição, E.; Mitchell, J.E.; Vaz, A.R.; Bastos, A.P.; Ramalho, S.; Silva, C.; Cao, L.; Brandão, I.; Machado, P.P.P. The Presence of Maladaptive Eating Behaviors after Bariatric Surgery in a Cross Sectional Study: Importance of Picking or Nibbling on Weight Regain. Eat. Behav. 2014, 15, 558–562. [Google Scholar] [CrossRef]
- Conceição, E.M.; Mitchell, J.E.; Pinto-Bastos, A.; Arrojado, F.; Brandão, I.; Machado, P.P.P. Stability of Problematic Eating Behaviors and Weight Loss Trajectories after Bariatric Surgery: A Longitudinal Observational Study. Surg. Obes. Relat. Dis. 2017, 13, 1063–1070. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2023. [Google Scholar]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research, 2nd ed.; The Guilford Press: New York, NY, USA, 2015; p. xvii+462. ISBN 978-1-4625-1779-4. [Google Scholar]
- Consoli, S.; Rossi, A.; Thompson, L.Y.; Volpi, C.; Mannarini, S.; Castelnuovo, G.; Molinari, E. Assessing Psychometric Properties of the Italian Version of the Heartland Forgiveness Scale. Front. Psychol. 2020, 11, 596501. [Google Scholar] [CrossRef]
- Rossi, A.A.; Manzoni, G.M.; Pietrabissa, G.; Di Pauli, D.; Mannarini, S.; Castelnuovo, G. Weight Stigma in Patients with Overweight and Obesity: Validation of the Italian Weight Self-Stigma Questionnaire (WSSQ). Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2022, 27, 2459–2472. [Google Scholar] [CrossRef]
- Conceição, E.M.; de Lourdes, M.; Neufeld, C.B. Assessment of Grazing. In Assessment of Eating Behavior; Psychological assessment—Science and practice; Hogrefe: Göttingen, Germany, 2023; pp. 82–96. ISBN 978-0-88937-616-8. [Google Scholar]
- Schulte, E.M.; Gearhardt, A.N. Development of the Modified Yale Food Addiction Scale Version 2.0. Eur. Eat. Disord. Rev. 2017, 25, 302–308. [Google Scholar] [CrossRef]
- Imperatori, C.; Fabbricatore, M.; Lester, D.; Manzoni, G.M.; Castelnuovo, G.; Raimondi, G.; Innamorati, M. Psychometric Properties of the Modified Yale Food Addiction Scale Version 2.0 in an Italian Non-Clinical Sample. Eat. Weight Disord. 2019, 24, 37–45. [Google Scholar] [CrossRef]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The Assessment of Binge Eating Severity among Obese Persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Ricca, V.; Mannucci, E.; Moretti, S.; Di Bernardo, M.; Zucchi, T.; Cabras, P.L.; Rotella, C.M. Screening for Binge Eating Disorder in Obese Outpatients. Compr. Psychiatry 2000, 41, 111–115. [Google Scholar] [CrossRef]
- Imperatori, C.; Innamorati, M.; Lamis, D.A.; Contardi, A.; Continisio, M.; Castelnuovo, G.; Manzoni, G.M.; Fabbricatore, M. Factor Structure of the Binge Eating Scale in a Large Sample of Obese and Overweight Patients Attending Low Energy Diet Therapy. Eur. Eat. Disord. Rev. 2016, 24, 174–178. [Google Scholar] [CrossRef] [PubMed]
- Marcus, M.D.; Wing, R.R.; Hopkins, J. Obese Binge Eaters: Affect, Cognitions, and Response to Behavioral Weight Control. J. Consult. Clin. Psychol. 1988, 56, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Duarte, C.; Pinto-Gouveia, J.; Ferreira, C. Expanding Binge Eating Assessment: Validity and Screening Value of the Binge Eating Scale in Women from the General Population. Eat. Behav. 2015, 18, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Hood, M.M.; Grupski, A.E.; Hall, B.J.; Ivan, I.; Corsica, J. Factor Structure and Predictive Utility of the Binge Eating Scale in Bariatric Surgery Candidates. Surg. Obes. Relat. Dis. 2013, 9, 942–948. [Google Scholar] [CrossRef]
- Schroder, R.; Sellman, J.D.; Adamson, S. Development and Validation of a Brief Measure of Eating Compulsivity (MEC). Subst. Use Misuse 2017, 52, 1918–1924. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, J.; Persson, L.-O.; Sjöström, L.; Sullivan, M. Psychometric Properties and Factor Structure of the Three-Factor Eating Questionnaire (TFEQ) in Obese Men and Women. Results from the Swedish Obese Subjects (SOS) Study. Int. J. Obes. 2000, 24, 1715–1725. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.A.; Pietrabissa, G.; Castelnuovo, G.; Mannarini, S. Cognitive Restraint, Uncontrolled Eating, and Emotional Eating. The Italian Version of the Three Factor Eating Questionnaire-Revised 18 (TFEQ-R-18): A Three-step Validation Study. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2024, 29, 16. [Google Scholar] [CrossRef]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer International Publishing: New York, NY, USA, 2016. [Google Scholar]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using Lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Revelle, W. Psych: Procedures for Personality and Psychological Research; Elsevier B.V.: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Revelle, W. PsychTools: Tools to Accompany the “Psych” Package for Psychological Research; Elsevier B.V.: Amsterdam, The Netherlands, 2023. [Google Scholar]
- Epskamp, S. semPlot: Unified Visualizations of Structural Equation Models. Struct. Equ. Model. Multidiscip. J. 2015, 22, 474–483. [Google Scholar] [CrossRef]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Yu, C.-Y. Evaluating Cutoff Criteria of Model Fit Indices for Latent Variable Models with Binary and Continuous Outcomes. Ph.D. Thesis, University of California, Los Angeles, CA, USA, 2002. [Google Scholar]
- McDonald, R.P. Test Theory: A Unified Treatment; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1999; p. xi+485. ISBN 978-0-8058-3075-0. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: Harlow, UK, 2014. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Pietrabissa, G.; Castelnuovo, G.; Semonella, M.; Mannarini, S.; Rossi, A.A. Measuring Motivations to Eat Palatable Foods: Adaptation and Psychometric Properties of the Italian Version of the Palatable Eating Motives Scale (PEMS-IT). Healthcare 2024, 12, 574. [Google Scholar] [CrossRef]
- Meany, G.; Conceição, E.; Mitchell, J.E. Binge Eating, Binge Eating Disorder and Loss of Control Eating: Effects on Weight Outcomes after Bariatric Surgery. Eur. Eat. Disord. Rev. 2014, 22, 87–91. [Google Scholar] [CrossRef]
- Niego, S.H.; Kofman, M.D.; Weiss, J.J.; Geliebter, A. Binge Eating in the Bariatric Surgery Population: A Review of the Literature. Int. J. Eat. Disord. 2007, 40, 349–359. [Google Scholar] [CrossRef]
- Smith, K.E.; Orcutt, M.; Steffen, K.J.; Crosby, R.D.; Cao, L.; Garcia, L.; Mitchell, J.E. Loss of Control Eating and Binge Eating in the 7 Years Following Bariatric Surgery. Obes. Surg. 2019, 29, 1773–1780. [Google Scholar] [CrossRef]
- Nasirzadeh, Y.; Kantarovich, K.; Wnuk, S.; Okrainec, A.; Cassin, S.E.; Hawa, R.; Sockalingam, S. Binge Eating, Loss of Control over Eating, Emotional Eating, and Night Eating After Bariatric Surgery: Results from the Toronto Bari-PSYCH Cohort Study. Obes. Surg. 2018, 28, 2032–2039. [Google Scholar] [CrossRef] [PubMed]
- Cassin, S.; Leung, S.; Hawa, R.; Wnuk, S.; Jackson, T.; Sockalingam, S. Food Addiction Is Associated with Binge Eating and Psychiatric Distress among Post-Operative Bariatric Surgery Patients and May Improve in Response to Cognitive Behavioural Therapy. Nutrients 2020, 12, 2905. [Google Scholar] [CrossRef] [PubMed]
- Ben-Porat, T.; Weiss, R.; Sherf-Dagan, S.; Rottenstreich, A.; Kaluti, D.; Khalaileh, A.; Abu Gazala, M.; Zaken Ben-Anat, T.; Mintz, Y.; Sakran, N.; et al. Food Addiction and Binge Eating During One Year Following Sleeve Gastrectomy: Prevalence and Implications for Postoperative Outcomes. Obes. Surg. 2021, 31, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Panzeri, A.; DeVita, M.; Di Rosa, E.; Bottesi, G.; Brundisini, V.; Guarrera, C.; Ravelli, A.; Ponza, I.; Cattelan, A.; Volpe, B.; et al. Trauma Shaping the Psychopathological Correlates of Patients with Long-COVID: A 6-Months Longitudinal Study with Repeated Measures Mixed Models. Psychiatry Res. 2023, 330, 115609. [Google Scholar] [CrossRef] [PubMed]
- Panzeri, A.; Castelnuovo, G.; Spoto, A. Assessing Discriminant Validity through Structural Equation Modeling: The Case of Eating Compulsivity. Nutrients 2024, 16, 550. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive | Factor | Properties | Confirmatory Factor Analysis | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | SK | K | r(it-tot) | λ | R2 | ||
| Item#1 | 1.06 | 1.59 | 1.54 | 1.41 | RE | 0.667 | 0.689 | 0.475 |
| Item#2 | 1.70 | 1.75 | 0.82 | −0.41 | RE | 0.840 | 0.857 | 0.735 |
| Item#3 | 1.82 | 1.90 | 0.81 | −0.58 | RE | 0.819 | 0.841 | 0.708 |
| Item#4 | 1.54 | 1.80 | 1.04 | −0.07 | RE | 0.868 | 0.886 | 0.785 |
| Item#9 | 1.87 | 1.86 | 0.66 | −0.81 | RE | 0.776 | 0.836 | 0.700 |
| Item#10 | 1.82 | 1.84 | 0.74 | −0.65 | RE | 0.855 | 0.899 | 0.808 |
| Item#5 | 1.39 | 1.75 | 1.12 | 0.04 | CG | 0.767 | 0.799 | 0.638 |
| Item#6 | 1.73 | 1.79 | 0.82 | −0.51 | CG | 0.818 | 0.874 | 0.764 |
| Item#7 | 1.91 | 1.87 | 0.65 | −0.82 | CG | 0.840 | 0.892 | 0.796 |
| Item#8 | 1.70 | 1.85 | 0.93 | −0.08 | CG | 0.795 | 0.821 | 0.674 |
| Item#11 | 1.72 | 1.98 | 0.90 | −0.48 | CG | 0.701 | 0.718 | 0.515 |
| Item#12 | 2.28 | 2.05 | 0.46 | −1.08 | CG | 0.803 | 0.834 | 0.695 |
| Descriptive | Correlations | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | ||
| 1 | Rep(Eat)-Q | 1.71 | 1.53 | - | ||||||||
| 2 | Rep(Eat)-Q—RE | 1.64 | 1.56 | 0.965 ** | - | |||||||
| 3 | Rep(Eat)-Q—CG | 1.79 | 1.61 | 0.967 ** | 0.867 ** | - | ||||||
| 4 | mYFAS2.0 | 2.43 | 2.67 | 0.694 ** | 0.639 ** | 0.701 ** | - | |||||
| 5 | BES | 11.42 | 8.93 | 0.694 ** | 0.633 ** | 0.706 ** | 0.696 ** | - | ||||
| 6 | MEC10 | 14.74 | 10.34 | 0.705 ** | 0.623 ** | 0.737 ** | 0.688 ** | 0.773 ** | - | |||
| 7 | TFEQ-R-18—CR | 13.64 | 3.48 | −0.079 | −0.099 | −0.056 | −0.076 | −0.143 | −0.129 | - | ||
| 8 | TFEQ-R-18—UE | 17.61 | 6.66 | 0.753 ** | 0.690 ** | 0.762 ** | 0.667 ** | 0.728 ** | 0.823 ** | −0.079 | - | |
| 9 | TFEQ-R-18—EE | 7.07 | 3.05 | 0.643 ** | 0.553 ** | 0.684 ** | 0.573 ** | 0.585 ** | 0.648 ** | −0.003 | 0.670 ** | - |
| 10 | BMI | 42.28 | 6.48 | −0.011 | −0.011 | −0.010 | 0.061 | 0.026 | 0.037 | −0.156 * | 0.000 | −0.048 |
| Grazing | χ2 | Phi | OR | ||||
|---|---|---|---|---|---|---|---|
| No | Yes | (ϕ) | |||||
| Criterion A | Larger amount and for a longer period than intended | No | 192 | 5 | 30.229 | 0.274 | 9.600 |
| Yes | 164 | 41 | |||||
| Criterion B | Much time/activity to obtain, use, recover | No | 185 | 12 | 27.881 | 0.263 | 5.239 |
| Yes | 153 | 52 | |||||
| Criterion C | Social […] activities given up or reduced | No | 190 | 7 | 15.708 | 0.198 | 4.836 |
| Yes | 174 | 31 | |||||
| Criterion D | Characteristic withdrawal symptoms | No | 186 | 11 | 39.924 | 0.315 | 7.163 |
| Yes | 144 | 61 | |||||
| Criterion E | Failure to fulfill major role obligation | No | 171 | 26 | 53.755 | 0.366 | 5.792 |
| Yes | 109 | 96 | |||||
| Criterion F | […] Despite knowledge of adverse consequences | No | 185 | 12 | 92.677 | 0.480 | 14.972 |
| Yes | 104 | 101 | |||||
| Criterion G | Tolerance | No | 183 | 14 | 27.484 | 0.261 | 4.793 |
| Yes | 150 | 55 | |||||
| Criterion H | Craving | No | 184 | 13 | 47.769 | 0.345 | 7.499 |
| Yes | 134 | 71 | |||||
| Criterion I | Persistent desire or unsuccessful attempts to quit | No | 175 | 22 | 56.193 | 0.374 | 6.476 |
| Yes | 113 | 92 | |||||
| Criterion J | Use in physically hazardous situations | No | 192 | 5 | 20.541 | 0.226 | 7.103 |
| Yes | 173 | 32 | |||||
| Criterion K | Social or interpersonal problems | No | 125 | 72 | 64.009 | 0.399 | 5.527 |
| Yes | 49 | 156 | |||||
| Criterion L | Clinically significant impairment or distress | No | 176 | 21 | 75.289 | 0.433 | 8.630 |
| Yes | 101 | 104 | |||||
| Criterion | Symptom | β (se) | z-Value | p-Value | OR | OR 95% [L; U] |
|---|---|---|---|---|---|---|
| Criterion A | Amount | 0.922 (0.606) | 1.522 | 0.128 | 2.515 | [0.767; 8.253] |
| Criterion B | Time | −0.332 (0.463) | −0.718 | 0.473 | 0.717 | [0.290; 1.776] |
| Criterion C | Activities | 0.461 (0.552) | 0.836 | 0.403 | 1.586 | [0.538; 4.677] |
| Criterion D | Withdrawal | 0.571 (0.450) | 1.270 | 0.204 | 1.771 | [0.733; 4.278] |
| Criterion E | Obligations | 0.348 (0.344) | 1.010 | 0.312 | 1.416 | [0.721; 2.780] |
| Criterion F | Consequences | 1.463 (0.413) | 3.541 | <0.001 *** | 4.319 | [1.922; 9.707] |
| Criterion G | Tolerance | −0.356 (0.442) | −0.805 | 0.421 | 0.700 | [0.294; 1.667] |
| Criterion H | Craving | 0.031 (0.455) | 0.067 | 0.946 | 1.031 | [0.423; 2.513] |
| Criterion I | Attempts | 0.779 (0.337) | 2.312 | 0.021 * | 2.180 | [1.126; 4.221] |
| Criterion J | Situations | 0.436 (0.659) | 0.662 | 0.508 | 1.546 | [0.425; 5.629] |
| Criterion K | Problems | 0.844 (0.263) | 3.211 | 0.001 ** | 2.325 | [1.389; 3.892] |
| Criterion L | Impairment | 0.755 (0.365) | 2.068 | 0.039 * | 2.127 | [1.040; 4.348] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, A.A.; Mannarini, S.; Semonella, M.; Castelnuovo, G.; Pietrabissa, G. The Association between Grazing and Food Addiction: The Italian Version of the Repetitive Eating Questionnaire (Rep(Eat)-Q) and Its Relationships with Food Addiction Criteria. Nutrients 2024, 16, 949. https://doi.org/10.3390/nu16070949
Rossi AA, Mannarini S, Semonella M, Castelnuovo G, Pietrabissa G. The Association between Grazing and Food Addiction: The Italian Version of the Repetitive Eating Questionnaire (Rep(Eat)-Q) and Its Relationships with Food Addiction Criteria. Nutrients. 2024; 16(7):949. https://doi.org/10.3390/nu16070949
Chicago/Turabian StyleRossi, Alessandro Alberto, Stefania Mannarini, Michelle Semonella, Gianluca Castelnuovo, and Giada Pietrabissa. 2024. "The Association between Grazing and Food Addiction: The Italian Version of the Repetitive Eating Questionnaire (Rep(Eat)-Q) and Its Relationships with Food Addiction Criteria" Nutrients 16, no. 7: 949. https://doi.org/10.3390/nu16070949
APA StyleRossi, A. A., Mannarini, S., Semonella, M., Castelnuovo, G., & Pietrabissa, G. (2024). The Association between Grazing and Food Addiction: The Italian Version of the Repetitive Eating Questionnaire (Rep(Eat)-Q) and Its Relationships with Food Addiction Criteria. Nutrients, 16(7), 949. https://doi.org/10.3390/nu16070949