
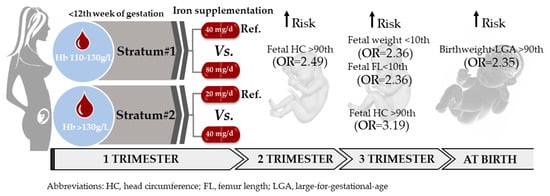
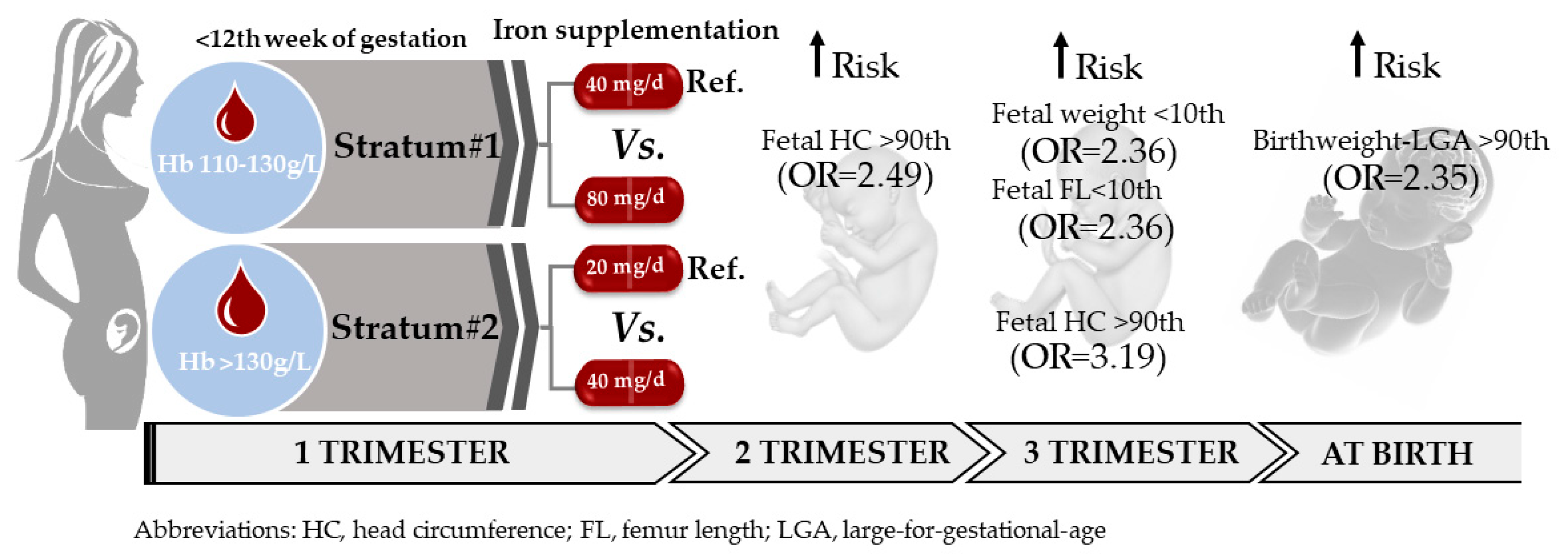
Effect of Prenatal Iron Supplementation Adapted to Hemoglobin Levels in Early Pregnancy on Fetal and Neonatal Growth—ECLIPSES Study




Abstract
1. Introduction
2. Materials and Methods
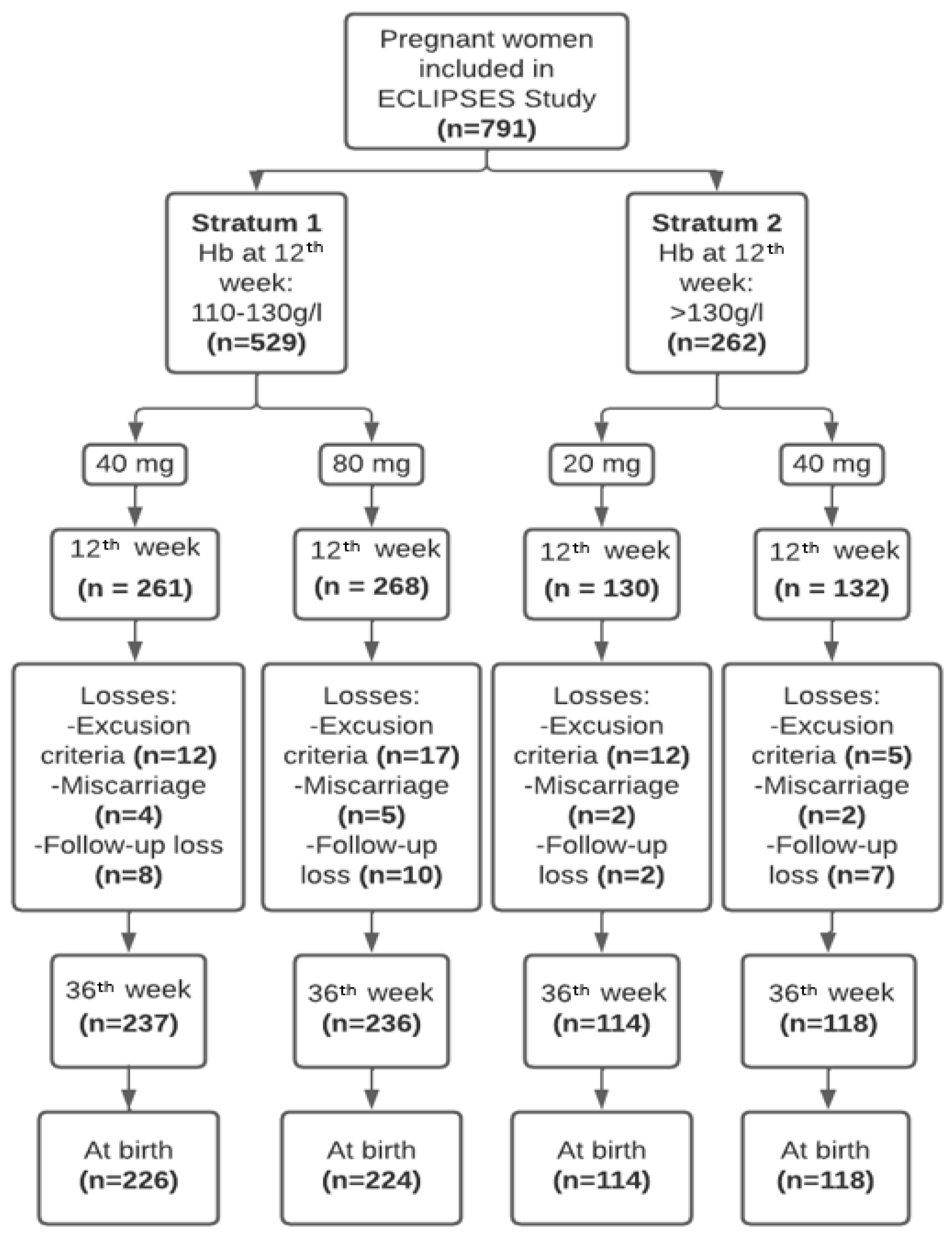
2.1. Study Design and Participants
2.2. Outcomes Measurements
2.3. Assessment of Covariates
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
3.2. Effect of Iron Supplementation, Adjusted to the Pregnant Women’s Initial Individual Iron Status, on Mean Growth Values of the Fetus and at Birth
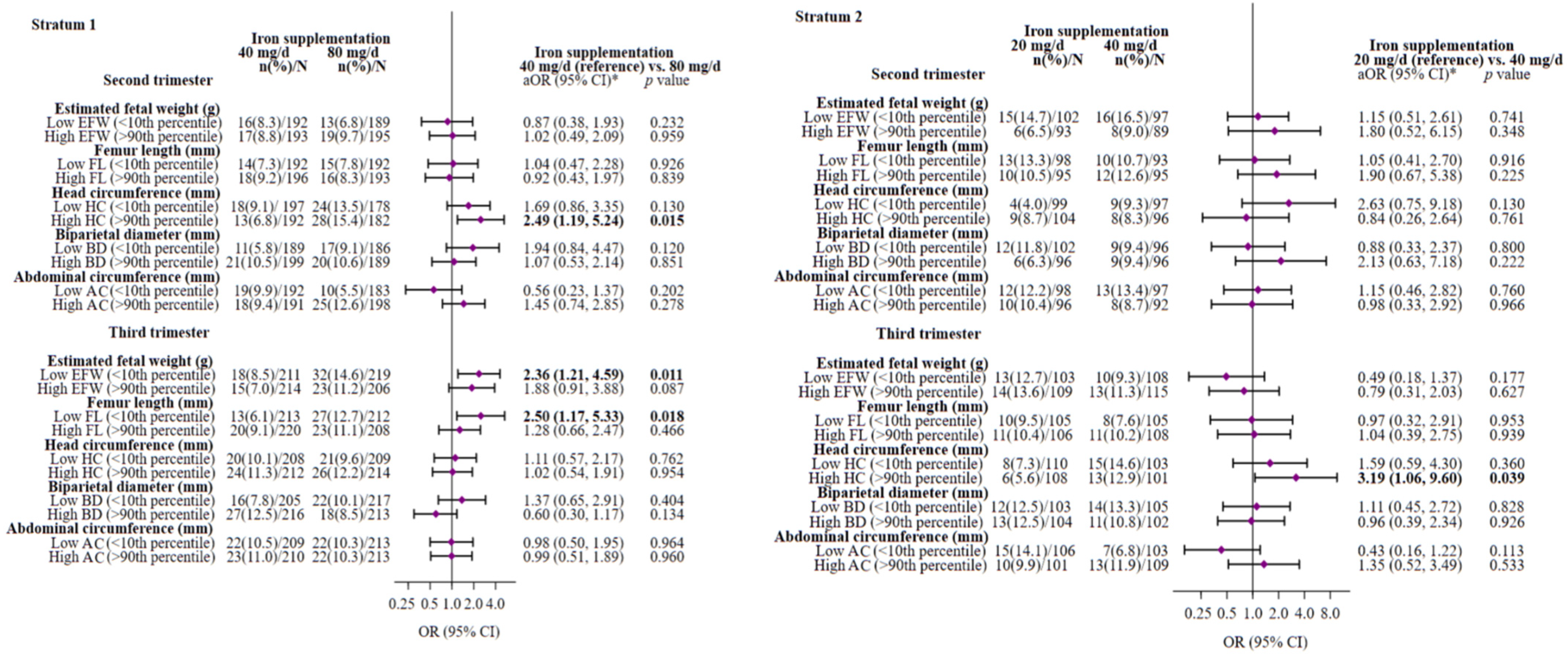
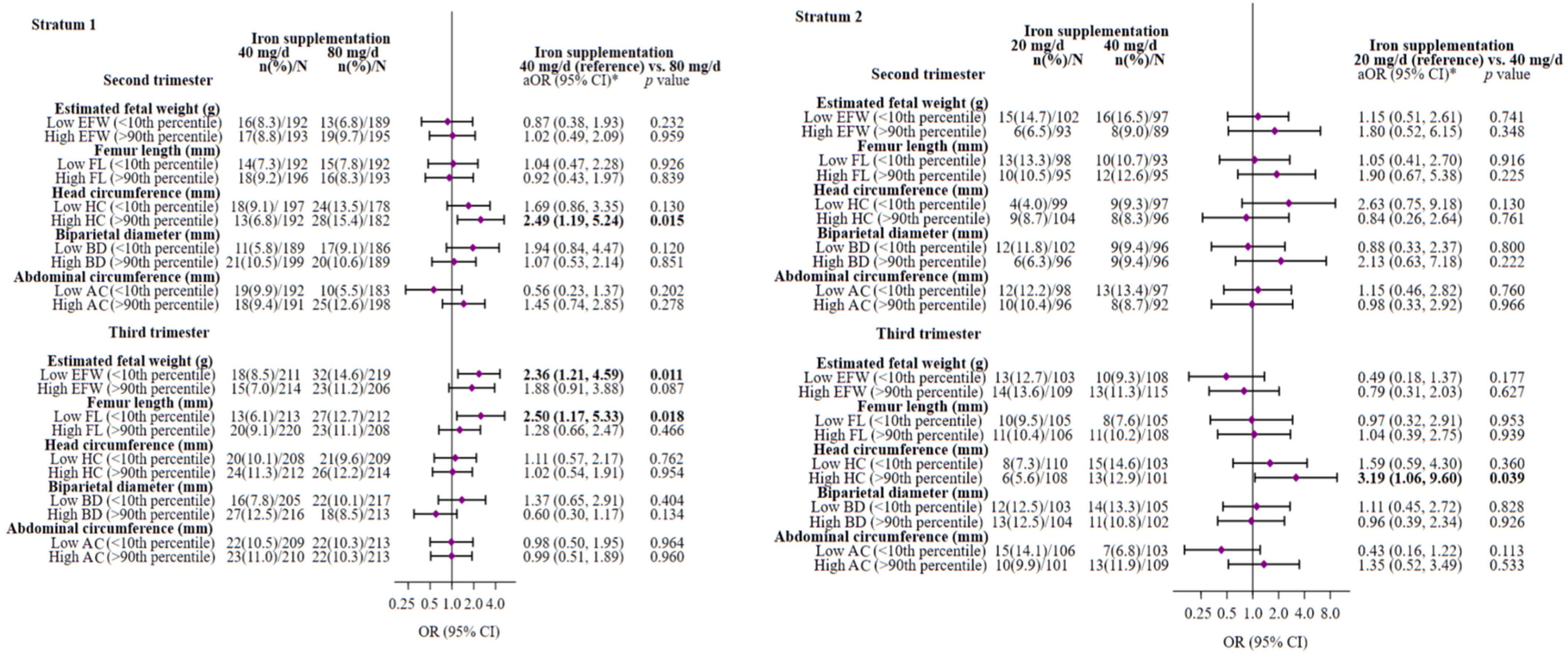
3.3. Effect of Iron Supplementation, Adjusted to the Pregnant Women’s Initial Individual Iron Status, on Optimal Fetal Growth (between the 10th and 90th Percentile)
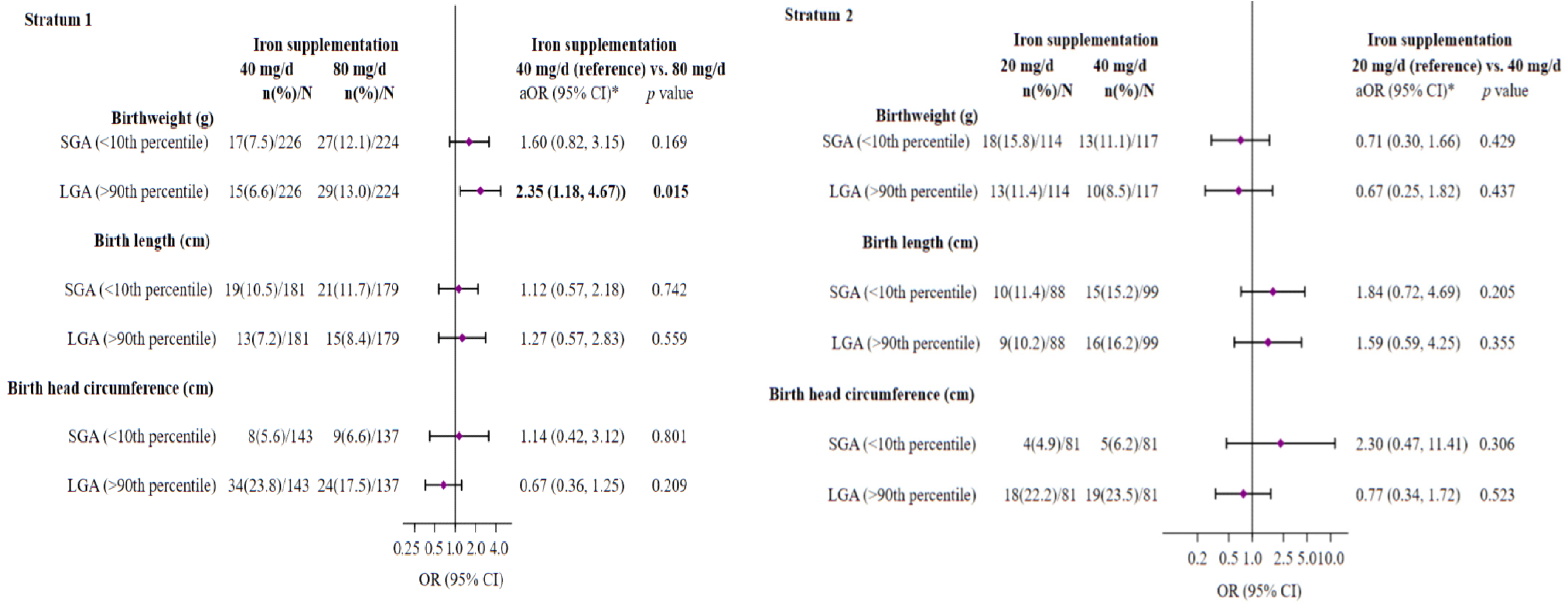
3.4. Effect of Iron Supplementation, Adjusted to the Pregnant Women’s Initial Individual Iron Status, on the Risk of SGA or LGA at Birth
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garzon, S.; Cacciato, P.M.; Certelli, C.; Salvaggio, C.; Magliarditi, M.; Rizzo, G. Iron Deficiency Anemia in Pregnancy: Novel Approaches for an Old Problem. Oman Med. J. 2020, 35, e166. [Google Scholar] [CrossRef]
- WHO. Anaemia in Women and Children Geneva: World Health Organization; 2021 Edition; WHO Global Anaemia Estimates: Geneva, Switzerland, 2022; Available online: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children#:~:text=In%202019%2C%20global%20anaemia%20prevalence,39.1%25)%20in%20pregnant%20women (accessed on 21 October 2023).
- Stevens, G.A.; Paciorek, C.J.; Flores-Urrutia, M.C.; Borghi, E.; Namaste, S.; Wirth, J.P.; Suchdev, P.S.; Ezzati, M.; Rohner, F.; Flaxman, S.R.; et al. National, regional, and global estimates of anaemia by severity in women and children for 2000-19: A pooled analysis of population-representative data. Lancet Glob. Health 2022, 10, e627–e639. [Google Scholar] [CrossRef]
- Sangkhae, V.; Fisher, A.L.; Ganz, T.; Nemeth, E. Iron Homeostasis During Pregnancy: Maternal, Placental, and Fetal Regulatory Mechanisms. Annu. Rev. Nutr. 2023, 43, 279–300. [Google Scholar] [CrossRef]
- Bothwell, T.H. Iron requirements in pregnancy and strategies to meet them. Am. J. Clin. Nutr. 2000, 72 (Suppl. S1), 257S–264S. [Google Scholar] [CrossRef]
- Iglesias Vázquez, L.; Arija, V.; Aranda, N.; Aparicio, E.; Serrat, N.; Fargas, F.; Ruiz, F.; Pallejà, M.; Coronel, P.; Gimeno, M.; et al. The Effectiveness of Different Doses of Iron Supplementation and the Prenatal Determinants of Maternal Iron Status in Pregnant Spanish Women: ECLIPSES Study. Nutrients 2019, 11, 2418. [Google Scholar]
- Georgieff, M.K.; Krebs, N.F.; Cusick, S.E. The Benefits and Risks of Iron Supplementation in Pregnancy and Childhood. Annu. Rev. Nutr. 2019, 39, 121–146. [Google Scholar] [CrossRef] [PubMed]
- Petry, C.J. Iron Supplementation in Pregnancy and Risk of Gestational Diabetes: A Narrative Review. Nutrients 2022, 14, 4791. [Google Scholar] [CrossRef] [PubMed]
- WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK409108/ (accessed on 11 October 2023).
- Peña-Rosas, J.P.; De-Regil, L.M.; Dowswell, T.; Viteri, F.E. Daily oral iron supplementation during pregnancy. Cochrane Database Syst. Rev. 2012, 12, CD004736. [Google Scholar] [PubMed]
- Peña-Rosas, J.P.; De-Regil, L.M.; Garcia-Casal, M.N.; Dowswell, T. Daily oral iron supplementation during pregnancy. Cochrane Database Syst. Rev. 2015, 2015, CD004736. [Google Scholar] [CrossRef] [PubMed]
- Hansen, R.; Sejer, E.P.F.; Holm, C.; Schroll, J.B. Iron supplements in pregnant women with normal iron status: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2023, 102, 1147–1158. [Google Scholar] [CrossRef] [PubMed]
- Tura, S.; Carenza, L.; Baccarani, M.; Bagnara, M.; Bocci, A.; Bottone, P.; Bresadola, M.; Bruzzese, G.; Cassano, F.; Coccia, M.E. Therapy and iron supplements with ferritin iron during pregnancy. Randomized prospective study of 458 cases. Recenti Prog. Med. 1989, 80, 607–614. [Google Scholar]
- Tholin, K.; Sandström, B.; Palm, R.; Hallmans, G. Changes in blood manganese levels during pregnancy in iron supplemented and non supplemented women. J. Trace Elem. Med. Biol. 1995, 9, 13–17. [Google Scholar] [CrossRef]
- Puolakka, J.; Jänne, O.; Pakarinen, A.; Järvinen, P.A.; Vihko, R. Serum ferritin as a measure of iron stores during and after normal pregnancy with and without iron supplements. Acta Obstet. Gynecol. Scand. Suppl. 1980, 95, 43–51. [Google Scholar] [CrossRef]
- Falahi, E.; Akbari, S.; Ebrahimzade, F.; Gargari, B.P. Impact of prophylactic iron supplementation in healthy pregnant women on maternal iron status and birth outcome. Food Nutr. Bull. 2011, 32, 213–217. [Google Scholar] [CrossRef]
- Alizadeh, L.; Salehi, L. Is Routine Iron Supplementation Necessary in Pregnant Women with High Hemoglobin? Iran. Red Crescent Med. J. 2016, 18, 22761. [Google Scholar] [CrossRef] [PubMed]
- Ziaei, S.; Janghorban, R.; Shariatdoust, S.; Faghihzadeh, S. The effects of iron supplementation on serum copper and zinc levels in pregnant women with high-normal hemoglobin. Int. J. Gynaecol. Obstet. 2008, 100, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Ziaei, S.; Mehrnia, M.; Faghihzadeh, S. Iron status markers in nonanemic pregnant women with and without iron supplementation. Int. J. Gynaecol. Obstet. 2008, 100, 130–132. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, M.E.; Parvanta, I.; Ickes, L.; Yip, R.; Brittenham, G.M. Iron supplementation during pregnancy, anemia, and birth weight: A randomized controlled trial. Am. J. Clin. Nutr. 2003, 78, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Xu, G.; Zhou, M.; Jiang, Y.; Richards, B.; Clark, K.M.; Kaciroti, N.; Georgieff, M.K.; Zhang, Z.; Tardif, T.; et al. Prenatal Iron Supplementation Reduces Maternal Anemia, Iron Deficiency, and Iron Deficiency Anemia in a Randomized Clinical Trial in Rural China, but Iron Deficiency Remains Widespread in Mothers and Neonates. J. Nutr. 2015, 145, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Oaks, B.M. U-shaped curve for risk associated with maternal hemoglobin, iron status, or iron supplementation. Am. J. Clin. Nutr. 2017, 106 (Suppl. S6), 1694S. [Google Scholar] [CrossRef] [PubMed]
- Ziaei, S.; Norrozi, M.; Faghihzadeh, S.; Jafarbegloo, E. A randomised placebo-controlled trial to determine the effect of iron supplementation on pregnancy outcome in pregnant women with haemoglobin ≥13.2 g/dl. BJOG 2007, 114, 684–688. [Google Scholar] [CrossRef]
- Shastri, L.; Mishra, P.E.; Dwarkanath, P.; Thomas, T.; Duggan, C.; Bosch, R.; McDonald, C.M.; Thomas, A.; Kurpad, A.V. Association of oral iron supplementation with birth outcomes in non-anaemic South Indian pregnant women. Eur. J. Clin. Nutr. 2015, 69, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Petry, C.J.; Ong, K.K.; Hughes, I.A.; Dunger, D.B. Associations between maternal iron supplementation in pregnancy and changes in offspring size at birth reflect those of multiple micronutrient supplementation. Nutrients 2021, 13, 2480. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.Y.; Lee, J.Y.; Kim, K.N.; Kim, H.; Ha, E.H.; Park, H.; Ha, M.; Kim, Y.; Hong, Y.C.; Chang, N. Maternal iron intake at mid-pregnancy is associated with reduced fetal growth: Results from Mothers and Children’s Environmental Health (MOCEH) study. Nutr. J. 2013, 12, 38. [Google Scholar] [CrossRef]
- Aranda, N.; Ribot, B.; Garcia, E.; Viteri, F.E.; Arija, V. Pre-pregnancy iron reserves, iron supplementation during pregnancy, and birth weight. Early Hum. Dev. 2011, 87, 791–797. [Google Scholar] [CrossRef]
- Milman, N.; Bergholt, T.; Byg, K.E.; Eriksen, L.; Graudal, N. Iron status and iron balance during pregnancy. A critical reappraisal of iron supplementation. Acta Obstet. Gynecol. Scand. 1999, 78, 749–757. [Google Scholar] [CrossRef]
- Casanueva, E.; Pfeffer, F.; Drijanski, A.; Fernández-Gaxiola, A.C.; Gutiérrez-Valenzuela, V.; Rothenberg, S.J. Iron and folate status before pregnancy and anemia during pregnancy. Ann. Nutr. Metab. 2003, 47, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Cheikh Ismail, L.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International Fetal and Newborn Growth Consortium for the 21st Century (INTERGROWTH-21st). International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar]
- Black, M.H.; Sacks, D.A.; Xiang, A.H.; Lawrence, J.M. The relative contribution of prepregnancy overweight and obesity, gestational weight gain, and IADPSG-defined gestational diabetes mellitus to fetal overgrowth. Diabetes Care 2013, 36, 56–62. [Google Scholar] [CrossRef]
- Aarnoudse-Moens, C.S.H.; Weisglas-Kuperus, N.; Van Goudoever, J.B.; Oosterlaan, J. Meta-analysis of neurobehavioral outcomes in very preterm and/or very low birth weight children. Pediatrics 2009, 124, 717–728. [Google Scholar] [CrossRef]
- McCarthy, E.A.; Walker, S.P. International fetal growth standards: One size fits all. Lancet 2014, 384, 835–836. [Google Scholar] [CrossRef]
- Arija, V.; Fargas, F.; March, G.; Abajo, S.; Basora, J.; Canals, J.; Ribot, B.; Aparicio, E.; Serrat, N.; Hernández-Martínez, C.; et al. Adapting iron dose supplementation in pregnancy for greater effectiveness on mother and child health: Protocol of the ECLIPSES randomized clinical trial. BMC Pregnancy Childbirth 2014, 14, 33. [Google Scholar] [CrossRef]
- Hadlock, F.P.; Harrist, R.B.; Sharman, R.S.; Deter, R.L.; Park, S.K. Estimation of fetal weight with the use of head, body, and femur measurements-A prospective study. Am. J. Obstet. Gynecol. 1985, 151, 333–337. [Google Scholar] [CrossRef]
- Willet, W. Nutritional Epidemiology. Monographs in Epidemiology and Biostatstics; Oxford University Press: Oxford, UK, 2012; pp. 50–67. Available online: https://books.google.com/books/about/Nutritional_Epidemiology.html?id=UKs3VaEtNukC (accessed on 13 April 2023).
- Zhang, J.; Merialdi, M.; Platt, L.D.; Kramer, M.S. Defining normal and abnormal fetal growth: Promises and challenges. Am. J. Obstet. Gynecol. 2010, 202, 522–528. [Google Scholar] [CrossRef]
- Institut d’Estadística de Catalunya. Catalan Classification of Occupations; Institut d’Estadística de Catalunya: Catalonia, Spain, 2011; Available online: https://www.idescat.cat/serveis/biblioteca/docs/cat/cco2011.pdf (accessed on 2 April 2023).
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerström, K.O. The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Favier, J.C.; Ireland-Ripert, J.; Toque, C.; Feinberg, M. Répertoire Général Des Aliments: Tables De Composition; Technique & Documentation; INRA: Paris, France, 1995; XXVII; 897p. [Google Scholar]
- Mataix, J.; García-Diz, L.; Mañas, M.; Martínez, E.; Llopis, J. Food Composition Tables, 5th ed.; Publisher University of Granada: Granada, Spain, 2009. [Google Scholar]
- World Health Organization (WHO). Global Dabatase on Body Mass Index; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Gómez, F.; Simó, J.M.; Camps, J.; Clivillé, X.; Bertran, N.; Ferré, N.; Bofill, C.; Joven, J. Evaluation of a particle-enhanced turbidimetric immunoassay for the measurement of ferritin: Application to patients participating in an autologous blood transfusion program. Clin. Biochem. 2000, 33, 191–196. [Google Scholar] [CrossRef]
- Haider, B.A.; Olofin, I.; Wang, M.; Spiegelman, D.; Ezzati, M.; Fawzi, W.W. Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: Systematic review and meta-analysis. BMJ 2013, 346, f3443. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Fan, H.B.; Yang, W.W.; Mao, X.D.; Xu, S.H.; Ma, X.P.; Wan, G.P.; Yao, X.M.; Chen, K. Correlation between plasma ferritin level and gestational diabetes mellitus and its impact on fetal macrosomia. J. Diabetes Investig. 2018, 9, 1354–1359. [Google Scholar] [CrossRef] [PubMed]
- Hua, X.G.; Jiang, W.; Hu, R.; Hu, C.Y.; Huang, K.; Li, F.L.; Zhang, X.J. Large for gestational age and macrosomia in pregnancies without gestational diabetes mellitus. J. Matern. Fetal Neonatal Med. 2020, 33, 3549–3558. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Dibley, M.J.; Cheng, Y.; Dang, S.; Chang, S.; Kong, L.; Yan, H. Impact of micronutrient supplementation during pregnancy on birth weight, duration of gestation, and perinatal mortality in rural western China: Double blind cluster randomised controlled trial. BMJ 2008, 337, 1211–1215. [Google Scholar] [CrossRef] [PubMed]
- Milman, N. Iron and pregnancy--a delicate balance. Ann. Hematol. 2006, 85, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Kell, D.B. Iron behaving badly: Inappropriate iron chelation as a major contributor to the aetiology of vascular and other progressive inflammatory and degenerative diseases. BMC Med. Genom. 2009, 2, 2. [Google Scholar]
- Aranda, N.; Fernandez-Cao, J.C.; Tous, M.; Arija, V. Increased iron levels and lipid peroxidation in a Mediterranean population of Spain. Eur. J. Clin. Investig. 2016, 46, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, S.; Bobby, Z.; Habeebullah, S.; Elizabeth Jacob, S. Differences in the response to iron supplementation on oxidative stress, inflammation, and hematological parameters in nonanemic and anemic pregnant women. J. Matern. Fetal Neonatal Med. 2022, 35, 465–471. [Google Scholar] [CrossRef]
- Sultana, Z.; Qiao, Y.; Maiti, K.; Smith, R. Involvement of oxidative stress in placental dysfunction, the pathophysiology of fetal death and pregnancy disorders. Reproduction 2023, 166, R25–R38. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. Oxidative stress. Best Pract. Res. Clin. Obstet. Gynaecol. 2011, 25, 287–299. [Google Scholar] [CrossRef]
- Menon, R. Oxidative Stress Damage as a Detrimental Factor in Preterm Birth Pathology. Front. Immunol. 2014, 5, 567. [Google Scholar] [CrossRef]
- Ganz, T. Systemic iron homeostasis. Physiol. Rev. 2013, 93, 1721–1741. [Google Scholar] [CrossRef]
- Erlandsson, L.; Masoumi, Z.; Hansson, L.R.; Hansson, S.R. The roles of free iron, heme, haemoglobin, and the scavenger proteins haemopexin and alpha-1-microglobulin in preeclampsia and fetal growth restriction. J. Intern. Med. 2021, 290, 952–968. [Google Scholar] [CrossRef]
- Shaji, G.N.; Bobby, Z.; Dorairajan, G.; Jacob, S.E. Increased hepcidin levels in preeclampsia: A protective mechanism against iron overload mediated oxidative stress? J. Matern. Fetal Neonatal Med. 2022, 35, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Zein, S.; Sitti, F.; Osman, M.; Arnaud, J.; Batandier, C.; Gauchez, A.S.; Rachidi, S.; Couturier, K.; Hininger-Favier, I. Middle Iron-Enriched Fructose Diet on Gestational Diabetes Risk and on Oxidative Stress in Offspring Rats. Biol. Trace Elem. Res. 2017, 175, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Olmos, P.R.; Borzone, G.R.; Olmos, R.I.; Valencia, C.N.; Bravo, F.A.; Hodgson, M.I.; Belmar, C.G.; Poblete, J.A.; Escalona, M.O.; Gómez, B. Gestational diabetes and pre-pregnancy overweight: Possible factors involved in newborn macrosomia. J. Obstet. Gynaecol. Res. 2012, 38, 208–214. [Google Scholar] [CrossRef] [PubMed]
- King, J.C. Zinc: An essential but elusive nutrient. Am. J. Clin. Nutr. 2011, 94, 679S–684S. [Google Scholar] [CrossRef] [PubMed]
- Hentze, M.W.; Muckenthaler, M.U.; Galy, B.; Camaschella, C. Two to Tango: Regulation of Mammalian Iron Metabolism. Cell 2010, 142, 24–38. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Wessling-Resnick, M. Iron and mechanisms of emotional behavior. J. Nutr. Biochem. 2014, 25, 1101–1107. [Google Scholar] [CrossRef]
- Drakesmith, H.; Prentice, A.M. Hepcidin and the iron-infection axis. Science 2012, 338, 768–772. [Google Scholar] [CrossRef]
- Milman, N.; Paszkowski, T.; Cetin, I.; Castelo-Branco, C. Supplementation during pregnancy: Beliefs and science. Gynecol. Endocrinol. 2016, 32, 509–516. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Iron Supplementation Group | ||||||
|---|---|---|---|---|---|---|
| Stratum 1 | Stratum 2 | |||||
| 40 mg/d | 80 mg/d | p Value | 20 mg/d | 40 mg/d | p Value | |
| Characteristics | N = 261 | N = 268 | N = 130 | N = 132 | ||
| Age (years), mean ± SD | 30.7 ± 4.3 | 30.1 ± 5.3 | 0.217 | 30.2 ± 4.9 | 30.1 ± 5.6 | 0.812 |
| BMI (kg/m2), mean ± SD | 24.6 ± 4.1 | 24.7 ± 4.1 | 0.757 | 25.7 ± 5.3 | 25.8 ± 4.8 | 0.856 |
| BMI categories, n (%) | ||||||
| 18.5–24.9 (normal weight) | 198 (64) | 162 (60) | 74 (57) | 67 (51) | ||
| 25.0–29.9 (overweight) | 61 (24) | 74 (28) | 0.530 | 31 (24) | 42 (32) | 0.355 |
| ≥30 (obese) | 32 (12) | 32 (12) | 25 (19) | 23 (17) | ||
| GWG (kg), mean ± SD | 10.5 ± 3.5 | 10.3 ± 3.7 | 0.448 | 10.0 ± 3.9 | 10.5 ± 3.9 | 0.322 |
| Educational level, n (%) | ||||||
| Low (primary or less) | 88 (34) | 87 (32) | 46 (35) | 40 (30) | ||
| medium (secondary) | 103 (39) | 104 (39) | 0.882 | 47 (36) | 49 (37) | 0.639 |
| High (university or more) | 70 (27) | 77 (29) | 37 (29) | 43 (33) | ||
| Family SES, n (%) | ||||||
| Low | 39 (15) | 47 (18) | 24 (18) | 18 (14) | ||
| Medium | 174 (67) | 180 (67) | 0.521 | 87 (67) | 89 (67) | 0.431 |
| High | 48 (18) | 41 (15) | 19 (15) | 25 (19) | ||
| Cigarette smoking, n (%) | ||||||
| No | 222 (85) | 219 (82) | 0.302 | 104 (80) | 105 (80) | 0.927 |
| Yes | 39 (15) | 49 (18) | 26 (20) | 27 (20) | ||
| Alcohol consumption, n (%) | ||||||
| No | 213 (87) | 211 (87) | 0.934 | 106 (86) | 107 (89) | 0.479 |
| Yes | 32 (13) | 31 (13) | 17 (14) | 13 (11) | ||
| Physical activity (METs—min/week), n (%) | ||||||
| Sedentary/low (<600) | 49 (19) | 54 (20) | 28 (22) | 39 (30) | ||
| Moderate (≥600–1200) | 41 (16) | 39 (15) | 0.884 | 20 (15) | 14 (11) | 0.234 |
| High (≥1200) | 171 (66) | 175 (65) | 82 (63) | 79 (60) | ||
| Energy intake (kcal), mean ± SD | 2095 ± 460 | 2123 ± 477 | 0.510 | 2121 ± 544 | 2165 ± 528 | 0.522 |
| Dietary iron intake (mg), mean ± SD | 7.8 ± 2.7 | 7.7 ± 2.4 | 0.628 | 7.7 ± 2.8 | 7.6 ± 2.2 | 0.752 |
| Dietary vitamin C intake (mg), mean ± SD | 76.5 ± 33.8 | 78.3 ± 35.6 | 0.582 | 77.5 ± 38.5 | 75.4 ± 37.2 | 0.658 |
| Fiber intake (g), mean ± SD | 12.5 ± 4.6 | 12.7 ± 4.3 | 0.623 | 12.5 ± 5.1 | 12.2 ± 4.1 | 0.648 |
| Parity, n (%) | ||||||
| Primiparous | 94 (36) | 105 (39) | 0.473 | 57 (44) | 59 (45) | 0.890 |
| Multiparous | 166 (64) | 163 (61) | 73 (56) | 73 (55) | ||
| Iron status characteristics | ||||||
| Hb (g/L), mean ± SD | 123.4 ± 4.7 | 123.3 ± 5.3 | 0.690 | 136.6 ± 4.4 | 135.7 ± 4.6 | 0.101 |
| SF (µg/L), mean ± SD * | 32.1 ± 2.0 | 32.8 ± 2.1 | 0.740 | 34.8 ± 1.9 | 34.8 ± 1.9 | 0.965 |
| Iron deficiency, n (%) ** | 37 (14) | 38 (14) | 0.999 | 16 (12) | 19 (14) | 0.620 |
| Carrier of HFE gene mutation, n (%) | 62 (30) | 74 (36) | 0.164 | 32 (30) | 40 (38) | 0.192 |
| H63D mutation, n (%) | 51 (24) | 63 (31) | 0.150 | 29 (27) | 34 (32) | 0.377 |
| S65C/C282Y mutation, n (%) | 13 (6) | 14 (7) | 0.802 | 3 (3) | 8 (8) | 0.110 |
| Cortisol (µg/dl), mean ± SD | 17.6 ± 4.7 | 18.4 ± 4.6 | 0.064 | 18.6 ± 5.5 | 18.3 ± 5.2 | 0.693 |
| Fetal Growth Parameters | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Period of Fetal Growth Measurement and Iron Supplementation | Estimated Fetal Weight (g) | Femur Length (mm) | Head Circumference (mm) | Biparietal Diameter (mm) | Abdominal Circumference (mm) | |||||
| β (95% CI) | p Value | β (95% CI) | p Value | β (95% CI) | p Value | β (95% CI) | p Value | β (95% CI) | p Value | |
| Second trimester | ||||||||||
| Stratum 1 | ||||||||||
| Iron supplementation **: (40 mg/d (ref.) vs. 80 mg/d) | 1.43 (−4.40, 7.26) | 0.630 | −0.05 (−0.40, 0.30) | 0.780 | 0.26 (−1.14, 1.67) | 0.711 | −0.12 (−0.57, 0.33) | 0.588 | 1.26 (−0.03, 2.54) | 0.056 |
| Stratum 2 | ||||||||||
| Iron supplementation **: (20 mg/d (ref.) vs. 40 mg/d) | 1.54 (−7.44, 10.53) | 0.735 | 0.28 (−0.22, 0.79) | 0.267 | 0.03 (−1.52, 1.59) | 0.965 | 0.07 (−0.51, 0.65) | 0.813 | −0.58 (−2.55, 1.38) | 0.559 |
| Third trimester | ||||||||||
| Stratum 1 | ||||||||||
| Iron supplementation †: (40 mg/d (ref.) vs. 80 mg/d) | −9.77 (−41.11, 21.57) | 0.540 | −0.30 (−0.75, 0.14) | 0.183 | −0.15 (−1.76, 1.46) | 0.855 | −0.32 (−0.78, 0.51) | 0.184 | −0.30 (−2.32, 1.72) | 0.767 |
| Stratum 2 | ||||||||||
| Iron supplementation †: (20 mg/d (ref.) vs. 40 mg/d) | 13.51 (−27.41, 54.47) | 0.515 | 0.03 (−0.57, 0.62) | 0.929 | −0.05 (−2.42, 2.31) | 0.963 | 0.13 (−0.66, 0.92) | 0.744 | 2.36 (−0.47, 5.19) | 0.103 |
| Birth parameters | ||||||||||
| Birthweight (g) | Length (cm) | Head circumference (mm) | ||||||||
| At birth | β (95% CI) | p value | β (95% CI) | p value | β (95% CI) | p value | ||||
| Stratum 1 | ||||||||||
| Iron supplementation †: (40 mg/d (ref.) vs. 80 mg/d) | −14.74 (−90.37, 60.89) | 0.702 | −0.02 (−0.41, 0.38) | 0.939 | −0.21 (−0.53, 0.10) | 0.180 | ||||
| Stratum 2 | ||||||||||
| Iron supplementation †: (20 mg/d (ref.) vs. 40 mg/d) | 18.53 (−98.35, 135.52) | 0.755 | −0.24 (−0.82, 0.34) | 0.414 | −0.06 (−0.56, 0.45) | 0.823 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Torres, S.; Díaz-López, A.; Arija, V. Effect of Prenatal Iron Supplementation Adapted to Hemoglobin Levels in Early Pregnancy on Fetal and Neonatal Growth—ECLIPSES Study. Nutrients 2024, 16, 437. https://doi.org/10.3390/nu16030437
Díaz-Torres S, Díaz-López A, Arija V. Effect of Prenatal Iron Supplementation Adapted to Hemoglobin Levels in Early Pregnancy on Fetal and Neonatal Growth—ECLIPSES Study. Nutrients. 2024; 16(3):437. https://doi.org/10.3390/nu16030437
Chicago/Turabian StyleDíaz-Torres, Sandra, Andrés Díaz-López, and Victoria Arija. 2024. "Effect of Prenatal Iron Supplementation Adapted to Hemoglobin Levels in Early Pregnancy on Fetal and Neonatal Growth—ECLIPSES Study" Nutrients 16, no. 3: 437. https://doi.org/10.3390/nu16030437
APA StyleDíaz-Torres, S., Díaz-López, A., & Arija, V. (2024). Effect of Prenatal Iron Supplementation Adapted to Hemoglobin Levels in Early Pregnancy on Fetal and Neonatal Growth—ECLIPSES Study. Nutrients, 16(3), 437. https://doi.org/10.3390/nu16030437