
Mediterranean Diet, Vitamin D, and Hypercaloric, Hyperproteic Oral Supplements for Treating Sarcopenia in Patients with Heart Failure—A Randomized Clinical Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
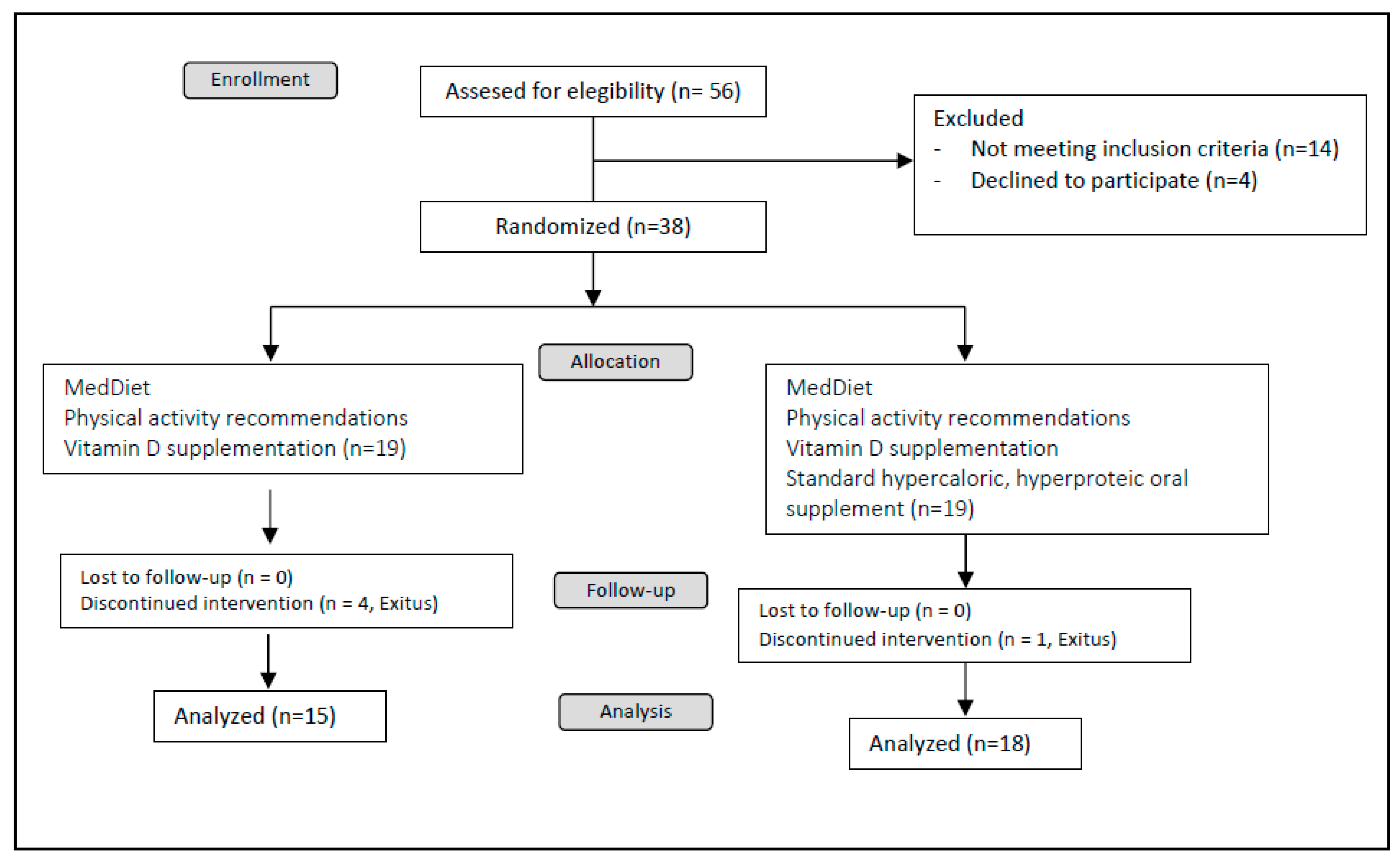
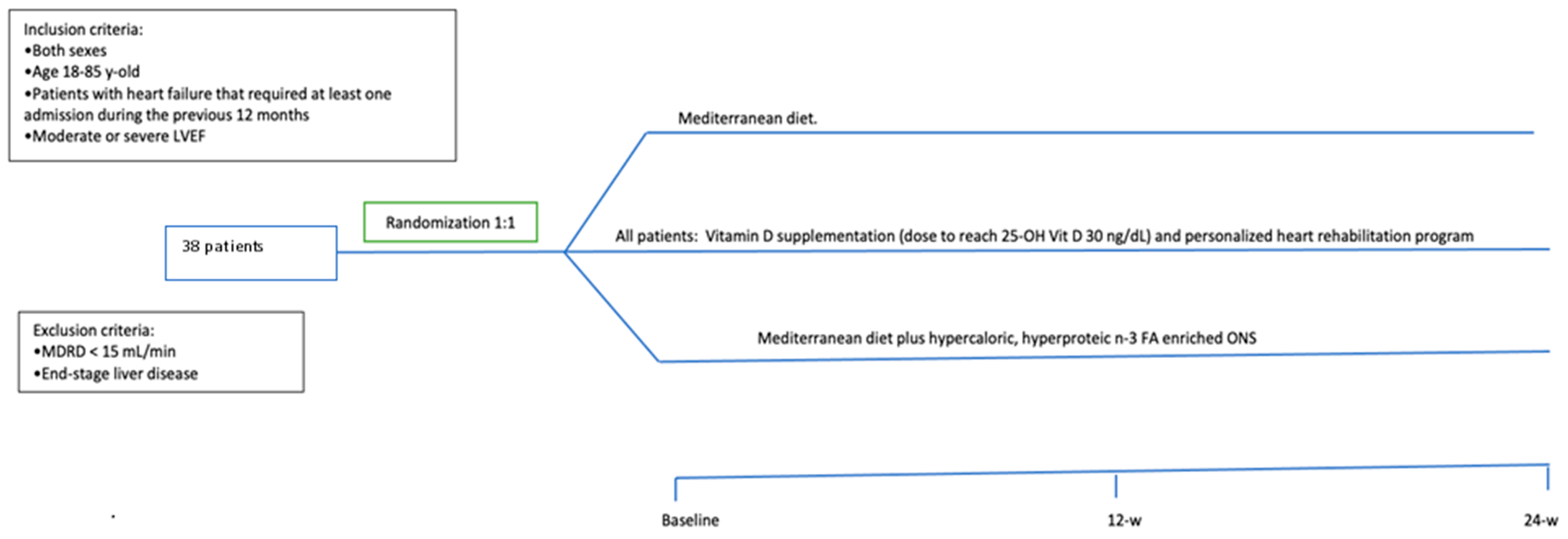
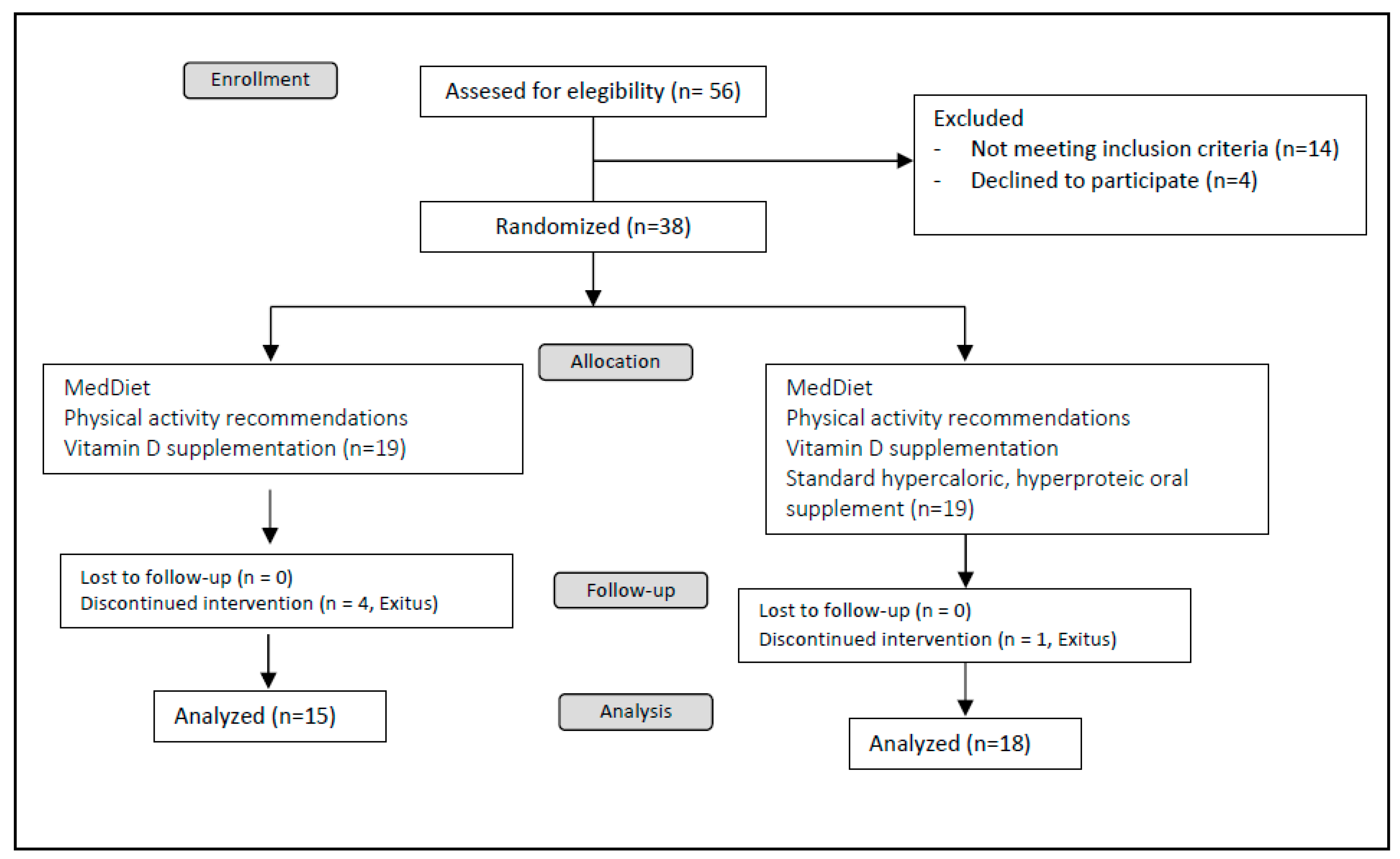
2.2. Study Design
2.3. Outcomes
2.4. Statistical Analysis
3. Results
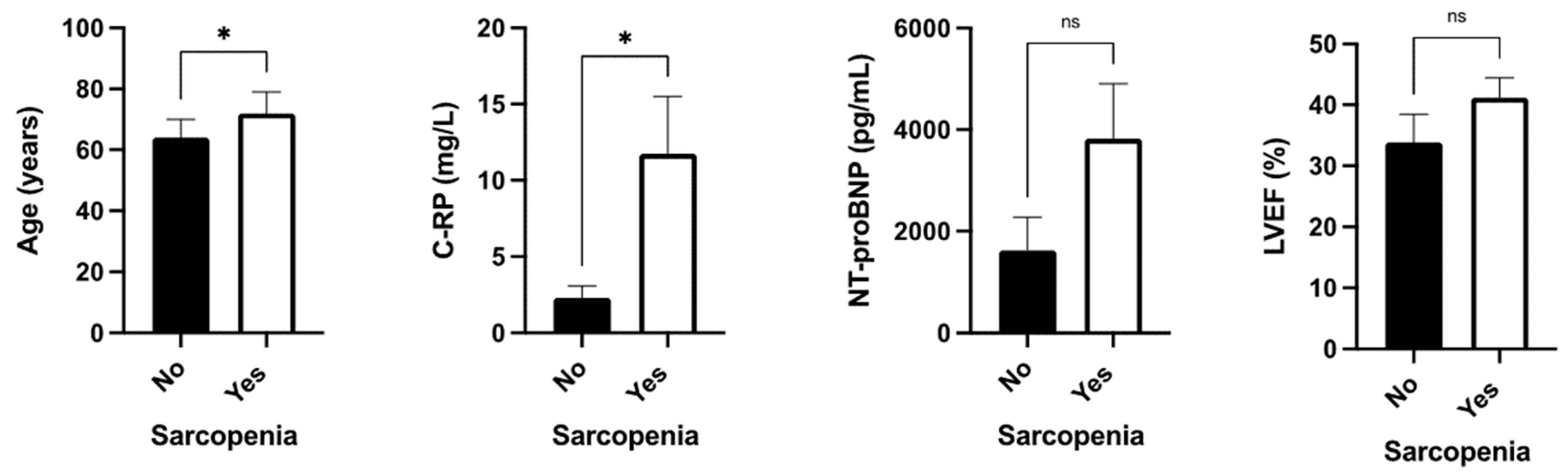
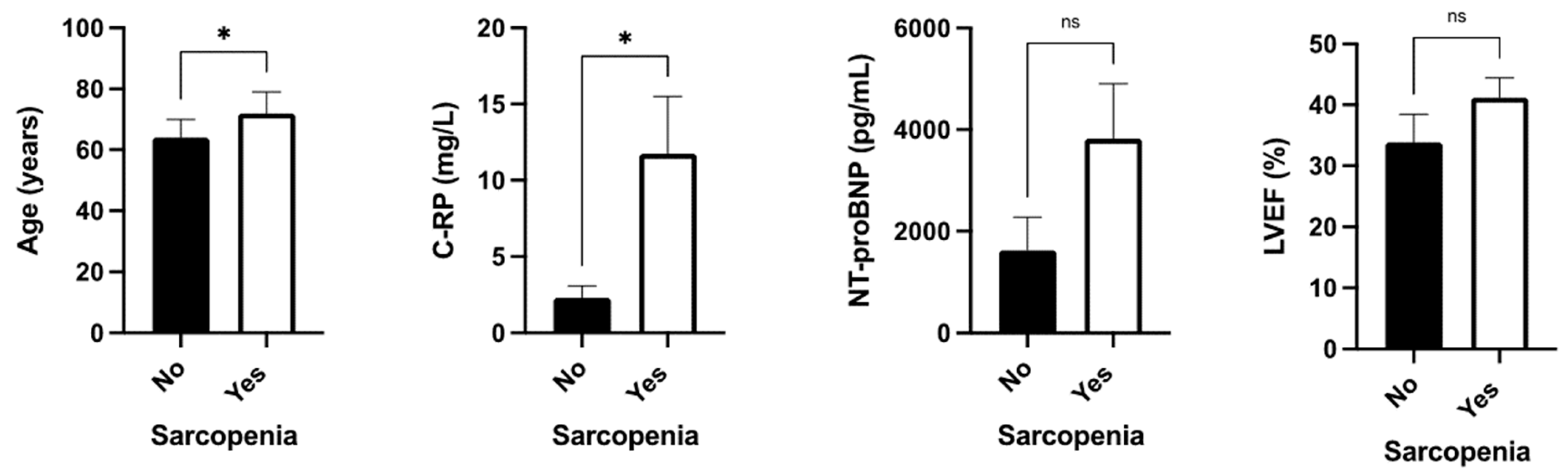
3.1. Baseline Characteristics of the Groups
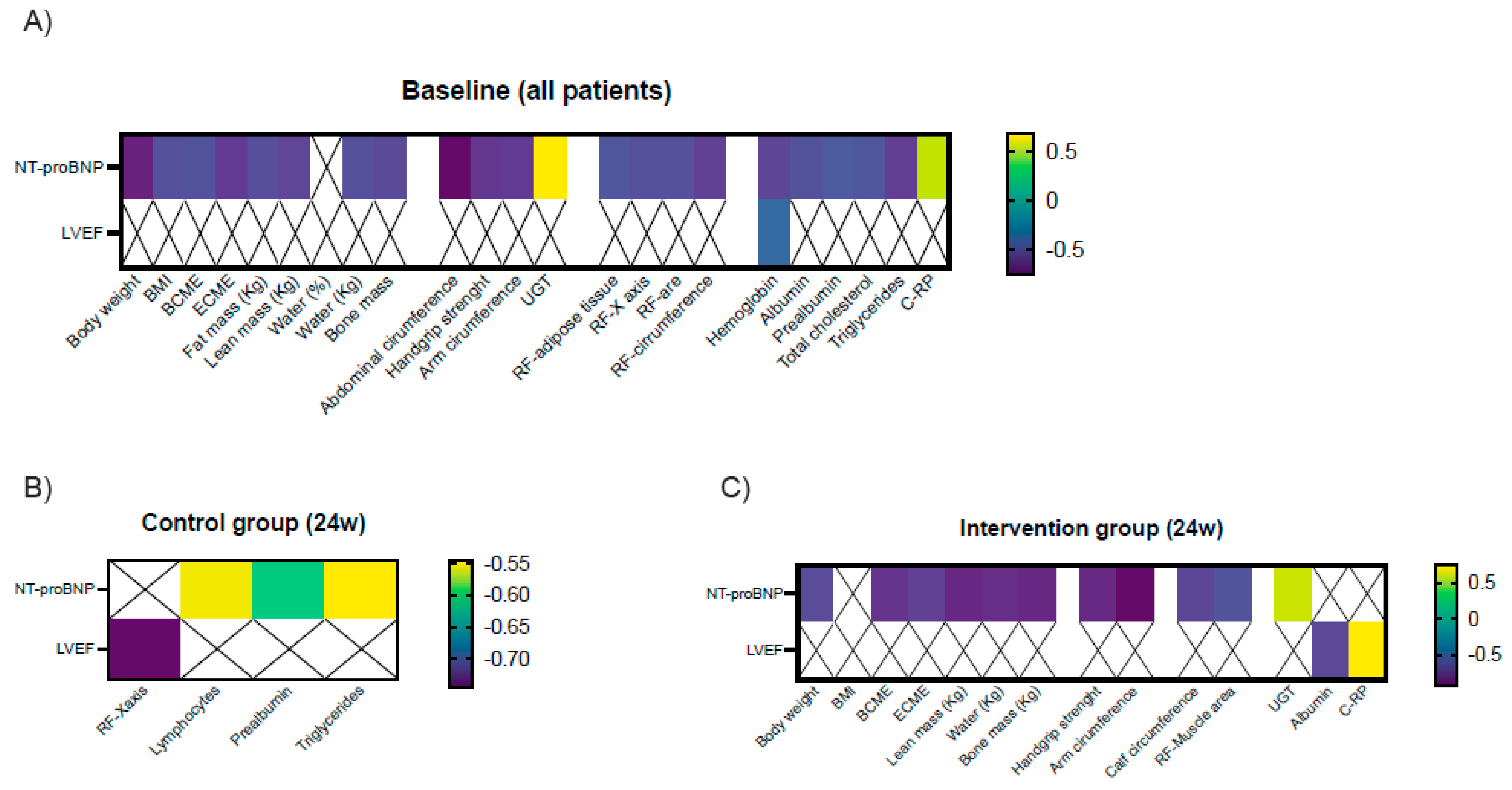
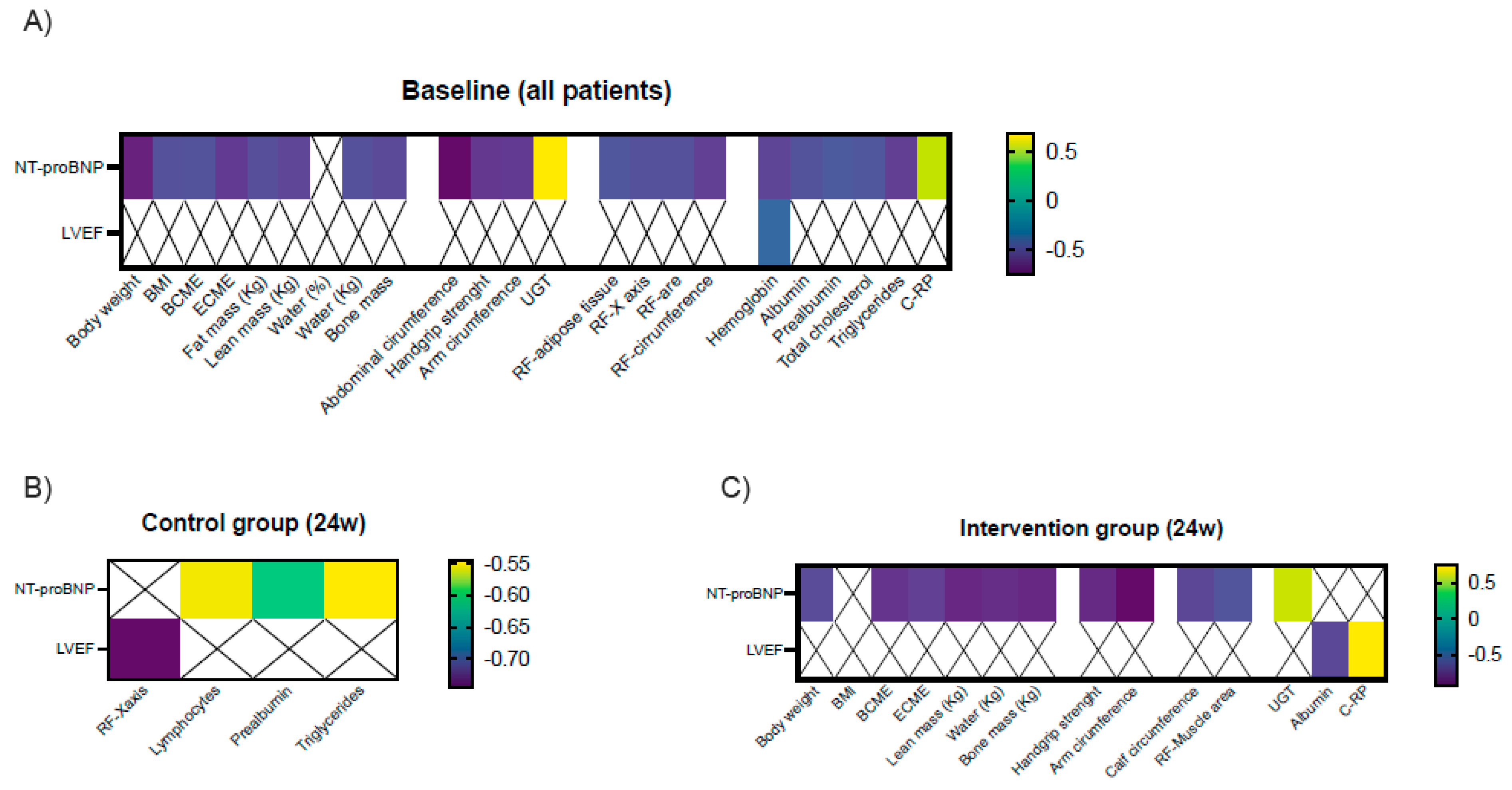
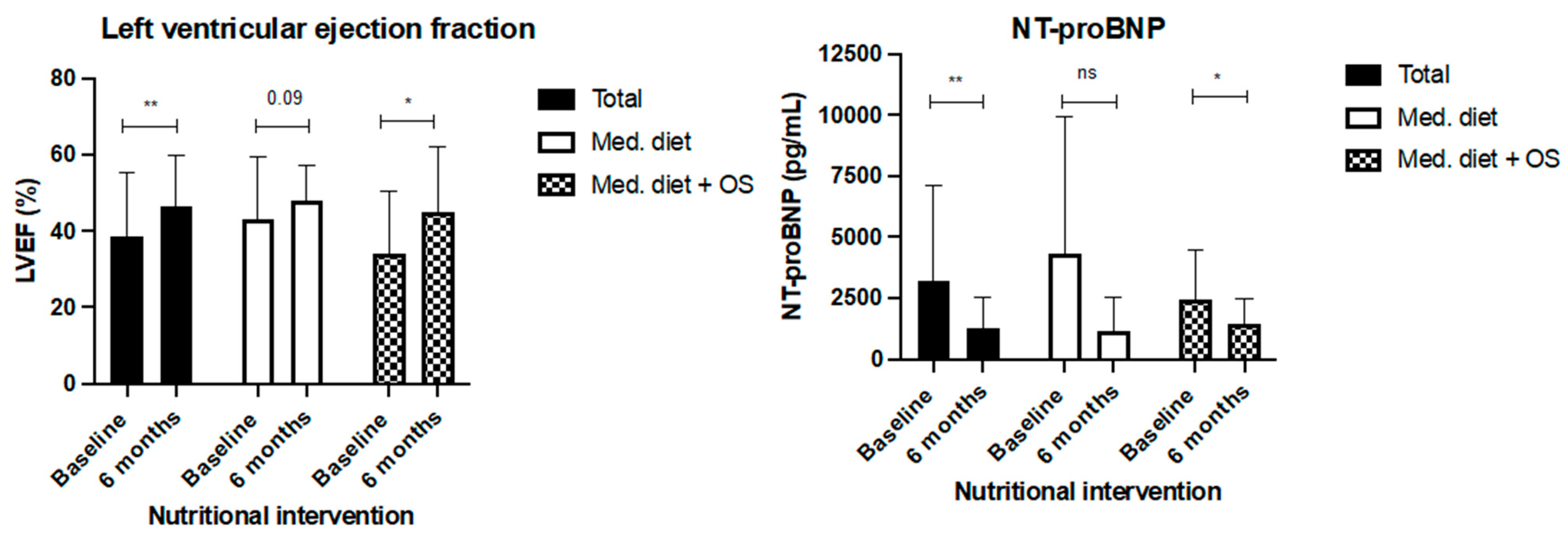
3.2. Primary and Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrera-Martínez, A.D.; León Idougourram, S.; Muñoz Jiménez, C.; Rodríguez-Alonso, R.; Alonso Echague, R.; Chica Palomino, S.; Sanz Sanz, A.; Manzano García, G.; Gálvez Moreno, M.Á.; Calañas Continente, A.; et al. Standard Hypercaloric, Hyperproteic vs. Leucine-Enriched Oral Supplements in Patients with Cancer-Induced Sarcopenia, a Randomized Clinical Trial. Nutrients 2023, 15, 2726. [Google Scholar] [CrossRef] [PubMed]
- Seferovic, P.M. Introduction to the special issue entitled ‘Heart failure management of the elderly patient: Focus on frailty, sarcopenia, cachexia, and dementia’. Eur. Heart J. Suppl. 2019, 21 (Suppl. L), L1–L3. [Google Scholar] [CrossRef] [PubMed]
- Urbich, M.; Globe, G.; Pantiri, K.; Heisen, M.; Bennison, C.; Wirtz, H.S.; Di Tanna, G.L. A Systematic Review of Medical Costs Associated with Heart Failure in the USA (2014–2020). Pharmacoeconomics 2020, 38, 1219–1236. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [PubMed]
- Mei, K.L.; Batsis, J.A.; Mills, J.B.; Holubar, S.D. Sarcopenia and sarcopenic obesity: Do they predict inferior oncologic outcomes after gastrointestinal cancer surgery? Perioper. Med. 2016, 5, 30. [Google Scholar] [CrossRef]
- Zhang, X.M.; Chen, D.; Xie, X.H.; Zhang, J.E.; Zeng, Y.; Cheng, A.S. Sarcopenia as a predictor of mortality among the critically ill in an intensive care unit: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 339. [Google Scholar] [CrossRef]
- Fonseca, G.; Dos Santos, M.R.; de Souza, F.R.; Takayama, L.; Rodrigues Pereira, R.M.; Negrao, C.E.; Alves, M.d.N.N. Discriminating sarcopenia in overweight/obese male patients with heart failure: The influence of body mass index. ESC Heart Fail. 2020, 7, 84–91. [Google Scholar] [CrossRef]
- Bekfani, T.; Pellicori, P.; Morris, D.A.; Ebner, N.; Valentova, M.; Steinbeck, L.; Wachter, R.; Elsner, S.; Sliziuk, V.; Schefold, J.C.; et al. Sarcopenia in patients with heart failure with preserved ejection fraction: Impact on muscle strength, exercise capacity and quality of life. Int. J. Cardiol. 2016, 222, 41–46. [Google Scholar] [CrossRef]
- Canteri, A.L.; Gusmon, L.B.; Zanini, A.C.; Nagano, F.E.; Rabito, E.I.; Petterle, R.R.; Jonasson, T.H.; Boguszewski, C.L.; Borba, V.Z.C. Sarcopenia in heart failure with reduced ejection fraction. Am. J. Cardiovasc. Dis. 2019, 9, 116–126. [Google Scholar]
- Curcio, F.; Testa, G.; Liguori, I.; Papillo, M.; Flocco, V.; Panicara, V.; Galizia, G.; Della-Morte, D.; Gargiulo, G.; Cacciatore, F.; et al. Sarcopenia and Heart Failure. Nutrients 2020, 12, 211. [Google Scholar] [CrossRef]
- Fernandez-Pombo, A.; Rodriguez-Carnero, G.; Castro, A.I.; Canton-Blanco, A.; Seoane, L.M.; Casanueva, F.F.; Crujeiras, A.B.; Martínez-Olmos, M.A. Relevance of nutritional assessment and treatment to counteract cardiac cachexia and sarcopenia in chronic heart failure. Clin. Nutr. 2021, 40, 5141–5155. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Ruiz-Gutierrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Arós, F.; et al. Effects of a Mediterranean-style diet on cardiovascular risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61 (Suppl. S6), 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvado, J.; Covas, M.I.; Corella, D.; Aros, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef]
- von Haehling, S.; Ebner, N.; Dos Santos, M.R.; Springer, J.; Anker, S.D. Muscle wasting and cachexia in heart failure: Mechanisms and therapies. Nat. Rev. Cardiol. 2017, 14, 323–341. [Google Scholar] [CrossRef]
- Bonilla-Palomas, J.L.; Gamez-Lopez, A.L.; Castillo-Dominguez, J.C.; Moreno-Conde, M.; Lopez Ibanez, M.C.; Alhambra Exposito, R.; Ortega, E.R.; Anguita-Sánchez, M.P.; Villar-Ráez, A. Nutritional Intervention in Malnourished Hospitalized Patients with Heart Failure. Arch. Med. Res. 2016, 47, 535–540. [Google Scholar] [CrossRef]
- Garcia Almeida, J.M.; Garcia Garcia, C.; Vegas Aguilar, I.M.; Bellido Castaneda, V.; Bellido Guerrero, D. Morphofunctional assessment of patient s nutritional status: A global approach. Nutr. Hosp. 2021, 38, 592–600. [Google Scholar]
- León-Idougourram, S.; Pérez-Gómez, J.M.; Muñoz Jiménez, C.; L-López, F.; Manzano García, G.; Molina Puertas, M.J.; Herman-Sánchez, N.; Alonso-Echague, R.; Calañas Continente, A.; Gálvez Moreno, M.Á.; et al. Morphofunctional and Molecular Assessment of Nutritional Status in Head and Neck Cancer Patients Undergoing Systemic Treatment: Role of Inflammasome in Clinical Nutrition. Cancers 2022, 14, 494. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar]
- Vest, A.R.; Chan, M.; Deswal, A.; Givertz, M.M.; Lekavich, C.; Lennie, T.; Litwin, S.E.; Parsly, L.; Rodgers, J.E.; Rich, M.W.; et al. Nutrition, Obesity, and Cachexia in Patients With Heart Failure: A Consensus Statement from the Heart Failure Society of America Scientific Statements Committee. J. Card. Fail. 2019, 25, 380–400. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Jafry, S.; Jeejeebhoy, K.; Nagpal, A.D.; Pisani, B.; Agarwala, R. Malnutrition and Cachexia in Heart Failure. JPEN J. Parenter. Enteral Nutr. 2016, 40, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Bonilla Palomas, J.L.; Gamez Lopez, A.L.; Moreno Conde, M.; Lopez Ibanez, M.C.; Castellano Garcia, P.; Raez Ruiz, C.J.; Ruíz Quirós, R.; Ramiro Ortega, E. Impact of malnutrition on long-term mortality in outpatients with chronic heart failure. Nutr. Hosp. 2017, 34, 1382–1389. [Google Scholar]
- García-Almeida, J.M.; García-García, C.; Vegas-Aguilar, I.M.; Ballesteros Pomar, M.D.; Cornejo-Pareja, I.M.; Fernández Medina, B.; de Luis Román, D.A.; Guerrero, D.B.; Lesmes, I.B.; Madueño, F.J. Nutritional ultrasound®: Conceptualisation, technical considerations and standardisation. Endocrinol. Diabetes Nutr. 2023, 70 (Suppl. S1), 74–84. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, J.; Ni, W.; Yuan, X.; Zhang, H.; Li, P.; Xu, J.; Zhao, Z. Sarcopenia in heart failure: A systematic review and meta-analysis. ESC Heart Fail. 2021, 8, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Delp, M.D.; Duan, C.; Mattson, J.P.; Musch, T.I. Changes in skeletal muscle biochemistry and histology relative to fiber type in rats with heart failure. J. Appl. Physiol. 1997, 83, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.; Matheson, E.M.; Matarese, L.E.; Luo, M.; Baggs, G.E.; Nelson, J.L.; Hegazi, R.A.; Tappenden, K.A.; Ziegler, T.R.; NOURISH Study Group; et al. Readmission and mortality in malnourished, older, hospitalized adults treated with a specialized oral nutritional supplement: A randomized clinical trial. Clin. Nutr. 2016, 35, 18–26. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Colvin, M.M., Jr.; Drazner, M.H.; Filippatos, G.; Fonarow, G.C.; Givertz, M.M.; et al. 2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure: An Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll. Cardiol. 2016, 68, 1476–1488. [Google Scholar]
- Sciatti, E.; Lombardi, C.; Ravera, A.; Vizzardi, E.; Bonadei, I.; Carubelli, V.; Gorga, E.; Metra, M. Nutritional Deficiency in Patients with Heart Failure. Nutrients 2016, 8, 442. [Google Scholar] [CrossRef]
- Adamo, L.; Rocha-Resende, C.; Prabhu, S.D.; Mann, D.L. Reappraising the role of inflammation in heart failure. Nat. Rev. Cardiol. 2020, 17, 269–285. [Google Scholar] [CrossRef]
- Vinoy, S.; Laville, M.; Feskens, E.J. Slow-release carbohydrates: Growing evidence on metabolic responses and public health interest. Summary of the symposium held at the 12th European Nutrition Conference (FENS 2015). Food Nutr. Res. 2016, 60, 31662. [Google Scholar] [CrossRef] [PubMed]
- Standl, E.; Schnell, O.; Ceriello, A. Postprandial hyperglycemia and glycemic variability: Should we care? Diabetes Care 2011, 34 (Suppl. S2), S120–S127. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Martinez, A.D.; Herrero-Aguayo, V.; Perez-Gomez, J.M.; Gahete, M.D.; Luque, R.M. Inflammasomes: Cause or consequence of obesity-associated comorbidities in humans. Obesity 2022, 30, 2351–2362. [Google Scholar] [CrossRef] [PubMed]
- Ocon Breton, M.J.; Tapia Guerrero, M.J.; Ramirez Rodriguez, J.M.; Peteiro Miranda, C.; Ballesteros Pomar, M.D.; Botella Romero, F.; Olmos, M.M.; Pérez, L.M.L.; Minchot, E.C.; Malpartida, K.G.; et al. Multidisciplinary consensus on nutritional and metabolic therapy in enhanced recovery after abdominal surgery programs: NutRICA Project. Endocrinol. Diabetes Nutr. 2022, 69, 98–111. [Google Scholar] [CrossRef] [PubMed]
- Barajas-Galindo, D.E.; Vidal-Casariego, A.; Pintor-de la Maza, B.; Fernandez-Martinez, P.; Ramos-Martinez, T.; Garcia-Arias, S.; Hernández-Moreno, A.; Urioste-Fondo, A.; Cano-Rodríguez, I.; Ballesteros-Pomar, M.D.; et al. Postoperative enteral immunonutrition in head and neck cancer patients: Impact on clinical outcomes. Endocrinol. Diabetes Nutr. 2020, 67, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Dalal, H.M.; Zwisler, A.D. Cardiac rehabilitation for heart failure: ‘Cinderella’ or evidence-based pillar of care? Eur. Heart J. 2023, 44, 1511–1518. [Google Scholar] [CrossRef]
- Prado, C.M.; Purcell, S.A.; Laviano, A. Nutrition interventions to treat low muscle mass in cancer. J. Cachexia Sarcopenia Muscle 2020, 11, 366–380. [Google Scholar] [CrossRef]
- Busa, V.; Dardeir, A.; Marudhai, S.; Patel, M.; Valaiyaduppu Subas, S.; Ghani, M.R.; Cancarevic, I. Role of Vitamin D Supplementation in Heart Failure Patients With Vitamin D Deficiency and Its Effects on Clinical Outcomes: A Literature Review. Cureus 2020, 12, e10840. [Google Scholar] [CrossRef]
- Leon, S.A.L.M.; Molina Puerta, M.J.; Galvez Moreno, M.A.; Herrera-Martinez, A.D. 25-OH-vitamina D y reversión de comorbilidades metabólicas asociadas a la obesidad tras la cirugía bariátrica. Rev. Osteoporos. Metab. Miner. 2022, 14, 42–47. [Google Scholar] [CrossRef]
- Herrera-Martínez, A.D.; Castillo-Peinado, L.L.S.; Molina-Puerta, M.J.; Calañas-Continente, A.; Membrives, A.; Castilla, J.; Cardenosa, M.C.; Casado-Díaz, A.; Gálvez-Moreno, M.A.; Gahete, M.D.; et al. Bariatric surgery and calcifediol treatment, Gordian knot of severe-obesity-related comorbidities treatment. Front. Endocrinol. 2023, 14, 1243906. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 38) | Mediterranean Diet (n = 19) | Mediterranean Diet and OS (n = 19) | p |
|---|---|---|---|---|
| Sex (♂/♀) | 71.1%/28.9% (11/27) | 31.6/68.4 (6/13) | 73.7/26.3 (14/5) | 0.50 |
| Age (years) | 67.5 (61–78) | 72 (64.5–80) | 65 (56–72) | 0.06 |
| Tobacco exposure (%) | 0.01 | |||
| No | 57.9 (22/38) | 42.1 (8/19) | 73.7 (14/19) | |
| Active | 18.4 (7/38) | 15.8 (3/19) | 21.1 (4/19) | |
| Previous exposure | 23.7 (9/38) | 42.1 (8/19) | 5.3 (1/19) | |
| Type 2 Diabetes | 42.1 (16/38) | 36.8 (7/19) | 47.4 (9/19) | 0.38 |
| Previous ischaemic cardiomyopathy | 34.2 (13/38) | 36.8 (7/19) | 31.6 (6/19) | 0.50 |
| Ejection fraction (%) | 33 (25–49.5) | 40 (32.5–54) | 38 (23–35) | 0.46 |
| NT-proBNP (pg/mL) | 4225 (2001–7289) | 3678 (1966–7203) | 4412 (2177–7255) | 0.59 |
| Current weight (kg) | 78 ± (70.3–89.5) | 81 (75–90) | 76 (70–85) | 0.17 |
| Symptoms (%) | ||||
| Weight loss (3 months) | 55.3 (21/38) | 47.4 (9/19) | 63.2 (12/19) | 0.26 |
| Weight loss kg (3 months) | 2 (0–4.75) | 0 (0–3.5) | 2 (0–5) | 0.56 |
| Weight loss (6 months) | 28.9 | 31.6 (6/19) | 26.3 (5/19) | 0.50 |
| Weight loss kg (6 months) | 0.5 (0–3) | 0.1 (0–3) | 0 (0–1.5) | 0.80 |
| Uncomplete denture | 63.2 (24/38) | 47.4 (9/19) | 78.9 (15/19) | 0.05 |
| Food intake (%) | ||||
| Soft | 7.9 (3/38) | 5.3 (1/19) | 10.5 /2/19) | 0.50 |
| Normal | 92.1 (35/38) | 94.7 (18/19) | 89.5 (17/19) | 0.50 |
| Gastrointestinal symptoms (%) | 15.8 (6/38) | 15.8 (3/19) | 15.8 (3/19) | 0.70 |
| Abdominal pain | 10.5 (4/38) | 21.1 (4/19) | 0 | 0.05 |
| Nauseas/vomits | 5.3 (2/38) | 0 | 10.5 (2/19) | 0.24 |
| Diarrhea | 5.3 (2/38) | 0 | 10.5 (2/19) | 0.24 |
| Body lesions | 0 | 0 | 0 | - |
| Dyspnea | 78.9 (30/38) | 94.7 (18/19) | 63.2 (12/19) | 0.09 |
| Malnutrition (%) | 23.7 (9/38) | 26.3 (5/19) | 21.1 (4/19) | 0.50 |
| Sarcopenia (%) | 65.8 (25/38) | 78.9 (15/19) | 52.6 (10/19) | 0.09 |
| Physical activity (%) | ||||
| Intense | 0 | 0 | 0 | - |
| Moderate | 18.4 (7/38) | 10.5 (2/19) | 26.3 (5/19) | 0.20 |
| Resting time (hours/day) | 7 (5–10) | 10 (6–11) | 6 (4–8.5) | 0.09 |
| Quality of life | ||||
| Self-rated health score | 72.5 (50–85) | 65 (40–78) | 80 (70–90) | 0.04 |
| Overweight/obesity (%) | 73.7 (28/38) | 57.1 (16/19) | 42.9 (12/19) | 0.14 |
| Characteristics | Total (n = 32) | Mediterranean Diet (n = 15) | Mediterranean Diet and OS (n = 18) | p |
|---|---|---|---|---|
| Heart failure hospitalizations (%) | 29 (9/31) | 33.3 (5/15) | 22.2 (4/18) | 0.37 |
| Number of hospitalizations | 0.5 | 0.5 | 0.5 | 0.71 |
| Weight loss (%) | 21.2 (7/32) | 20 (3/15) | 22.2 (4/18) | 0.58 |
| Gastrointestinal symptoms (%) | 15.2 (5/32) | 20 (3/15) | 11.1 (2/18) | 0.44 |
| Abdominal pain | 6.3 (2/32) | 13.3 (2/15) | 0 | 0.21 |
| Nauseas/vomits | 3.1 (1/32) | 0 | 5.5 (1/18) | 0.53 |
| Diarrhea | 7.9 (3/32) | 6.7 (1/15) | 11.8 (2/18) | 0.55 |
| Body lesions | 0 | 6.7 (1/15) | 0 | - |
| Dyspnea | 75 (26/32) | 93.7 (14/15) | 58.8 (10/18) | 0.09 |
| Physical activity (%) | ||||
| Intense | 0 | 0 | 0 | - |
| Moderate | 34.4 (11/32) | 26.7 (4/15) | 41.2 (7/17) | 0.31 |
| Resting time (hours) | 6 (4–10) | 8 (6–10) | 4.5 (4–7.3 ) | 0.08 |
| Quality of life | 80 (80–90) | 75 (67–80) | 85 (75–95) | 0.03 |
| Mortality (%) | 13.2 (5/38) | 21.1 (4/19) | 5.3 (1/19) | 0.17 |
| Total | Mediterranean Diet | Mediterranean Diet and OS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Baseline (n = 38) | Six Months (n = 33) | p1 | Baseline (n = 19) | Six Months (n = 15) | p2 | Baseline (n = 19) | Six Months (n = 18) | p3 |
| Body weight | 79 (69–85) | 81 (68–88) | 0.02 | 82.5 (73.9–90.1) | 88.1 (81.3–92.7) | 0.18 | 78.6 (65.1–81.9) | 69.8 (65–84) | 0.06 |
| Bioimpedance analysis | |||||||||
| BMI (kg/m2) | 28.5 (25–30) | 28.5 (25.6–32.5) | 0.02 | 29.6 (27–34.3) | 30.6 (28.2–36.1) | 0.21 | 27.4 (23.5–28.9) | 27.4 (24– 28.6) | 0.05 |
| BCME (kg) | 37.2 (33.3–43) | 37 (33–42.1) | 0.67 | 38.1 (33.8–43.8) | 36.9 (33.3–42) | 0.08 | 35.5 (33.4–41.2) | 38.2 (33.3–42.2) | 0.03 |
| ECMe (kg) | 20.7 (19.8–22.8) | 21.7 (19.3–22.9) | 0.24 | 21.5 (20–22.9) | 22.5 (20.1–23.9) | 0.42 | 20.4 (18.9–22.3) | 21.2 (18.1–22.7) | 0.36 |
| Fat mass (%) | 25.1 (21.7–31.5) | 25 (23.3–31.4) | 0.19 | 27.8 (23.2–33.3) | 30.9 (27.5–30.1) | 0.16 | 23.4 (20.6–23.3) | 23.5 (28.8–24.9) | 0.82 |
| Fat mass (kg) | 20.2 (14.6–25.8) | 25 (23.3–31.4) | 0.07 | 23.2 (17.4–27.6) | 26.7 (22.1–30.1) | 0.05 | 17.5 (13–22.4) | 15.4 (12.5–19.7) | 0.48 |
| Lean mass (%) | 71.2 (65.1–74.2) | 71.3 (65.2–72.9) | 0.35 | 68.6 (63.5–73) | 65.7 (61.7–68.9) | 0.20 | 72.8 (70.1–75.4) | 72.7 (70.1–75.4) | 0.82 |
| Lean mass (kg) | 52.6 (50.2–61.3) | 55.6 (50.1–62.3) | 0.30 | 56.6 (50.5–62) | 55.7 (50.1–62.5) | 0.30 | 52.5 (49.8–60.9) | 55.3 (50.1–61.1) | 0.03 |
| Water (%) | 52.6 (48.2–55.5) | 52.8 (48.5–54.4) | 0.43 | 51 (47.3–53.7) | 48.6 (44.9–51.6) | 0.22 | 54.7 (51.6–57) | 54.1 (52.9–56.9) | 0.83 |
| Water (kg) | 40.1 (36.8–45.5) | 42.4 (35.9–45.8) | 0.40 | 40.7 (37.3–46.1) | 42.5 (35.9–46.1) | 0.38 | 39.2 (36.5–44.9) | 42.3 (37–45.5) | 0.12 |
| Bone Mass (kg) | 2.8 (2.7–3.2) | 2.9 (2.7–3.2) | 0.52 | 3 (2.7–3.3) | 2.9 (2.7–3.3) | 0.14 | 2.6 (2.6–3.2) | 2.9 (2.7–3.2) | 0.03 |
| Phase angle | 4.7 (3.7–6) | 4.5 (3.6–5.9) | 0.80 | 3.7 (3.1–5.5) | 4.5 (3.3–4.9) | 0.53 | 4.9 (4.5–6.2) | 4.8 (4.3–6.5) | 0.46 |
| Anthropometric evaluation | |||||||||
| Abdominal circumference | 106 (98–110) | 106 (93–113) | 0.90 | 110 (102.5–114) | 112 (107–121) | 0.59 | 101 (93–108) | 104 (92–106) | 0.62 |
| Arm circumference | 32 (28–33) | 31 (28–33) | 0.49 | 32 (28–33) | 32 (30–35) | 0.14 | 31 (28–33) | 30 (28–32) | 0.62 |
| Calf circumference | 37 (34–39) | 37 (35–39) | 0.53 | 37 (35–39) | 38 (36–41) | 0.58 | 37 (34–40) | 37 (35–38) | 0.72 |
| RF Muscle Ultrasound | |||||||||
| Adipose tissue (cm) | 0.67 (0.5–0.8) | 0.61 (0.5–1) | 0.53 | 0.69 (0.5–0.8) | 0.8 (0.6–1.2) | 0.53 | 0.69 (0.5–0.8) | 0.5 (0.5–0.7) | 0.08 |
| Area (cm2) | 3.75 (2.2–4.6) | 3.1 (2.6–3.7) | 0.19 | 3.1 (2.1–4.6) | 3.3 (2.7–3.7) | 0.97 | 3.5 (2.7–4.4) | 3.0 (2.6–3.5) | 0.06 |
| Circumference (cm) | 8.7 (7.5–10.1) | 8.2 (7.8–9.2) | 0.42 | 8.3 (6.8–9.9) | 9.0 (7.8–9.5) | 0.46 | 9.5 (7.9–10.1) | 8.1 (7.8–9.2) | 0.05 |
| AP axis (cm) | 1.2 (1–1.4) | 1.1 (0.9–1.2) | 0.20 | 1.3 (0.9–4.6) | 1.2 (1.0–1.3) | 0.90 | 1.2 (1.0–1.5) | 1.0 (0.9–1.2) | 0.09 |
| Transversal axis (cm) | 3.8 (3.3–4.4) | 3.3 (3.6–4) | 0.42 | 3.8 (3.1–4.5) | 3.6 (3.3–4.2) | 0.78 | 3.7 (3.4–4.2) | 3.7 (3.4–4.2) | 0.30 |
| Abdominal Ultrasound | |||||||||
| Total adipose tissue (cm) | 2.2 (1.5–3) | 2.3 (1.6–3.1) | 0.87 | 2.4 (3.4–4.2) | 2.3 (1.6–3.8) | 0.78 | 1.7 (1.5–3.0) | 2.2 (1.6–3.0) | 0.87 |
| Subcutaneous adipose tissue (cm) | 1.6 (1–1.3) | 1.6 (1–2) | 0.53 | 1.6 (0.9–2.1) | 1.6 (1.0–2.1) | 0.20 | 1.6 (1.1–2.5) | 1.6 (1.0–1.9) | 0.92 |
| Preperitoneal fat (cm) | 0.5 (0.4–0.7) | 0.6 (0.4–0.7) | 0.37 | 0.5 (0.4–0.7) | 0.5 (0.4–0.7) | 0.71 | 0.5 (0.4–0.8) | 0.6 (0.5–0.7) | 0.39 |
| Functional evaluation | |||||||||
| Handgrip strenght (dominant arm, kg) | 30 (20.3–39.8) | 31.7 (18–40.8) | 0.71 | 23 (19–24) | 24 (13–36) | 0.36 | 34 (29–40) | 38 (25–44) | 0.44 |
| Up-and-go test (seconds) | 20 (16–25) | 11 (9.5–13.7) | <0.001 | 20 (18–25) | 11 (10–16) | <0.001 | 18 (14–21) | 10 (9–12) | <0.001 |
| Total | Mediterranean Diet | Mediterranean Diet and OS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Baseline (n = 38) | Six Months (n = 33) | p1 | Baseline (n = 19) | Six Months (n = 15) | p2 | Baseline (n = 19) | Six Months (n = 18) | p3 |
| Biochemical parameters | |||||||||
| Hemoglobin (g/dL) | 13.8 (12.9–15.3) | 14.2 (13–15.6) | 0.03 | 13.5 (12.7–15) | 14 (13–14.8) | 0.22 | 13.9 (13.1–15.5) | 14.9 (13.2–15.7) | 0.03 |
| Lymphocytes (x mm3) | 1730 (1320–2360) | 1655 (1324–1912) | 0.13 | 1730 (1470–2150) | 1860 (1390–2060) | 0.41 | 1665 (1267–2420) | 1550 (1070–1810) | 0.18 |
| Albumin (g/dL) | 4.5 (4.3–4.9) | 4.5 (4.2–4.7) | 0.30 | 4.5 (4.4–4.9) | 4.6 (4.3–4.8) | 0.81 | 4.5 (4.3–4.9) | 4.4 (4.2–4.6) | 0.28 |
| Prealbumin (mg/dL) | 26 (21–28) | 25 (22–28) | 0.55 | 25 (20–28) | 24 (21–28) | 0.76 | 27 (23–29) | 25 (22–28) | 0.23 |
| Ferritin (mg/dL) | 106 (35–176) | 73 (32–111) | 0.003 | 74 (32–171) | 80 (37–113) | 0.46 | 130 (104–169) | 80 (37–113) | <0.01 |
| Transferrin (mg/dL) | 245 (218–262) | 239 (227–286) | 0.12 | 252 (233–308) | 240 (232–299) | 0.71 | 240 (214–253) | 234 (223–285) | 0.04 |
| Total cholesterol (mg/dL) | 158 (126–196) | 161 (133–192) | 0.72 | 159 (126–187) | 166 (131–195) | 0.44 | 157 (126–195) | 157 (141–190) | 0.11 |
| HDL cholesterol (mg/dL) | 46 (41–53) | 45 (38–51) | 0.17 | 44 (39–50) | 44 (32–50) | 0.11 | 48 (45–54) | 47 (38–56) | 0.85 |
| LDL cholesterol (mg/dL) | 86 (65–115) | 93 (61–123) | 0.12 | 80 (55–103) | 99 (58–120) | 0.78 | 86 (70–122) | 90 (61–123) | 0.04 |
| Triglycerides (mg/dL) | 136 (101–174) | 112 (91–147) | <0.001 | 144 (92–209) | 117 (102–152) | 0.01 | 132 (105–164) | 90 (61–123) | 0.17 |
| C-RP (mg/L) | 2.1 (0.5–6.9) | 1.0 (0.5–2.6) | 0.02 | 2.2 (0.5–15) | 2.1 (0.5–5.6) | 0.79 | 1.4 (0.7–5.8) | 0.7 (0.5–1.5) | <0.01 |
| NT-proBNP (pg/mL) | 1855 (1080–4364) | 741 (393–1992) | <0.01 | 1757 (557–6027) | 489 (178–1676) | 0.17 | 1952 (1179–3307) | 1303 (741–2111) | 0.02 |
| Vitamin D (ng/dL) | 18 (11–26) | 22 (16–31) | 0.08 | 15 (11–21) | 17 (9–29) | 0.51 | 17 (9–29) | 25 (19–38) | 0.08 |
| Variable | OR | CI | p | |
|---|---|---|---|---|
| Mortality | Nutritional support | 0.24 | 0.02–2.62 | 0.24 |
| Baseline LVEF | 0.98 | 0.92–1.05 | 0.64 | |
| Baseline NT-proBNP | 1.00 | 1.00–1.00 | 0.67 | |
| Baseline BMI | 0.94 | 0.75–1.18 | 0.61 | |
| Baseline BCME | 0.99 | 0.90–1.10 | 0.88 | |
| Baseline Phase angle | 0.51 | 0.19–1.37 | 0.18 | |
| Baseline Handgrip strength | 0.92 | 0.81–1.05 | 0.22 | |
| Baseline up-and-go test | 1.09 | 0.98–1.23 | 0.11 | |
| Baseline Preperitoneal fat | 0.36 | 0.00–15.48 | 0.60 | |
| Baseline C-RP | 0.99 | 0.94–1.06 | 0.98 | |
| New hospital admissions | Nutritional support | 0.65 | 0.12–3.57 | 0.62 |
| Baseline LVEF | 1.00 | 0.95–1.05 | 0.94 | |
| Baseline NT-proBNP | 1.00 | 1.00–1.00 | 0.09 | |
| Baseline BMI | 1.06 | 0.89–1.26 | 0.48 | |
| Baseline BCME | 1.00 | 0.97–1.03 | 0.98 | |
| Baseline Phase angle | 0.92 | 0.63–1.32 | 0.63 | |
| Baseline Handgrip strength | 1.02 | 0.93–1.13 | 0.62 | |
| Baseline up-and-go test | 1.05 | 0.94–1.17 | 0.38 | |
| Baseline Preperitoneal fat | 0.25 | 0.01–4.38 | 0.34 | |
| Baseline C-RP | 1.01 | 0.97–1.06 | 0.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera-Martínez, A.D.; Muñoz Jiménez, C.; López Aguilera, J.; Crespin, M.C.; Manzano García, G.; Gálvez Moreno, M.Á.; Calañas Continente, A.; Molina Puerta, M.J. Mediterranean Diet, Vitamin D, and Hypercaloric, Hyperproteic Oral Supplements for Treating Sarcopenia in Patients with Heart Failure—A Randomized Clinical Trial. Nutrients 2024, 16, 110. https://doi.org/10.3390/nu16010110
Herrera-Martínez AD, Muñoz Jiménez C, López Aguilera J, Crespin MC, Manzano García G, Gálvez Moreno MÁ, Calañas Continente A, Molina Puerta MJ. Mediterranean Diet, Vitamin D, and Hypercaloric, Hyperproteic Oral Supplements for Treating Sarcopenia in Patients with Heart Failure—A Randomized Clinical Trial. Nutrients. 2024; 16(1):110. https://doi.org/10.3390/nu16010110
Chicago/Turabian StyleHerrera-Martínez, Aura D., Concepción Muñoz Jiménez, José López Aguilera, Manuel Crespin Crespin, Gregorio Manzano García, María Ángeles Gálvez Moreno, Alfonso Calañas Continente, and María José Molina Puerta. 2024. "Mediterranean Diet, Vitamin D, and Hypercaloric, Hyperproteic Oral Supplements for Treating Sarcopenia in Patients with Heart Failure—A Randomized Clinical Trial" Nutrients 16, no. 1: 110. https://doi.org/10.3390/nu16010110
APA StyleHerrera-Martínez, A. D., Muñoz Jiménez, C., López Aguilera, J., Crespin, M. C., Manzano García, G., Gálvez Moreno, M. Á., Calañas Continente, A., & Molina Puerta, M. J. (2024). Mediterranean Diet, Vitamin D, and Hypercaloric, Hyperproteic Oral Supplements for Treating Sarcopenia in Patients with Heart Failure—A Randomized Clinical Trial. Nutrients, 16(1), 110. https://doi.org/10.3390/nu16010110