

The Impact of the ENDORSE Digital Weight Management Program on the Metabolic Profile of Children and Adolescents with Overweight and Obesity and on Food Parenting Practices

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Setting
Inclusion/Exclusion Criteria
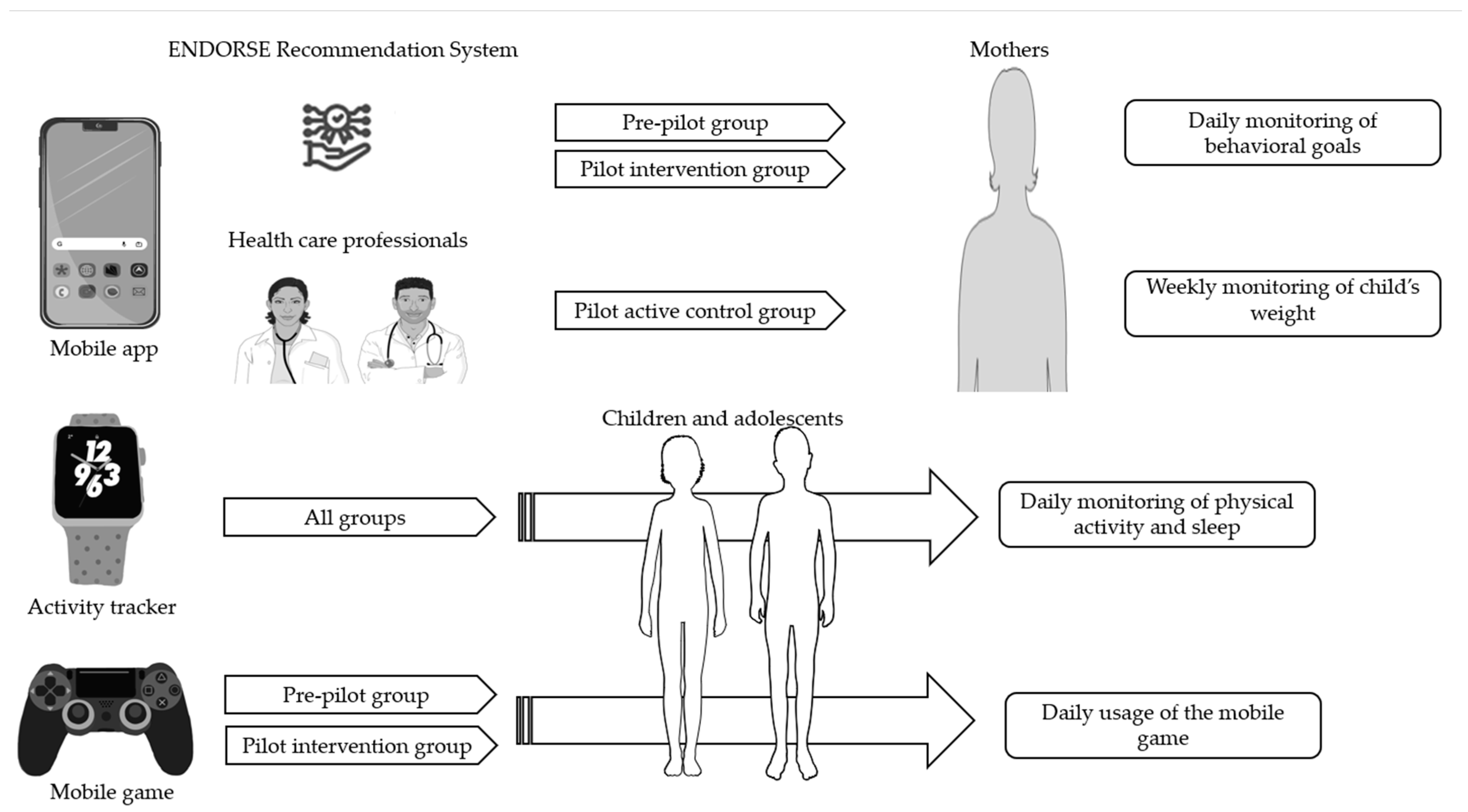
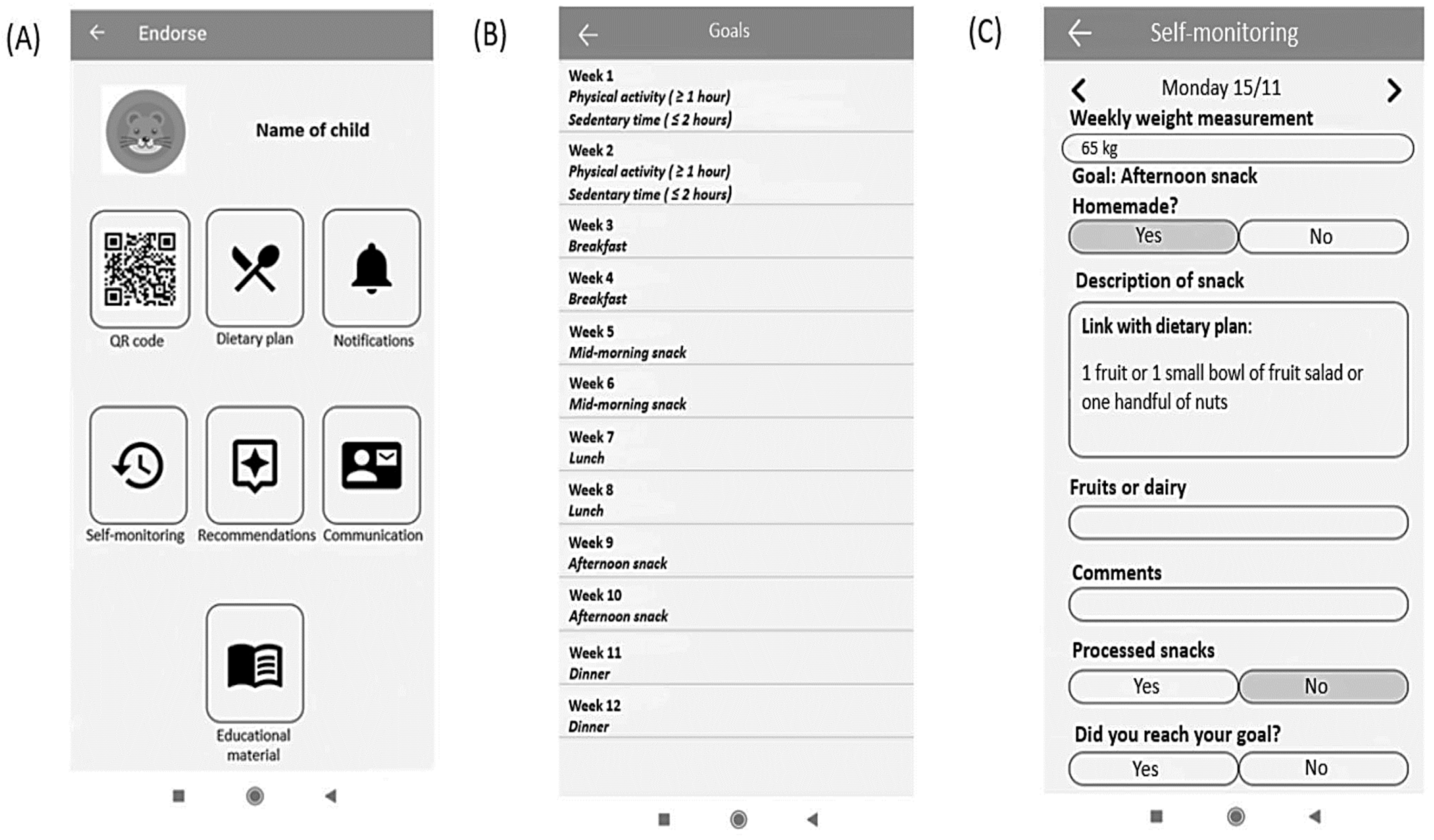
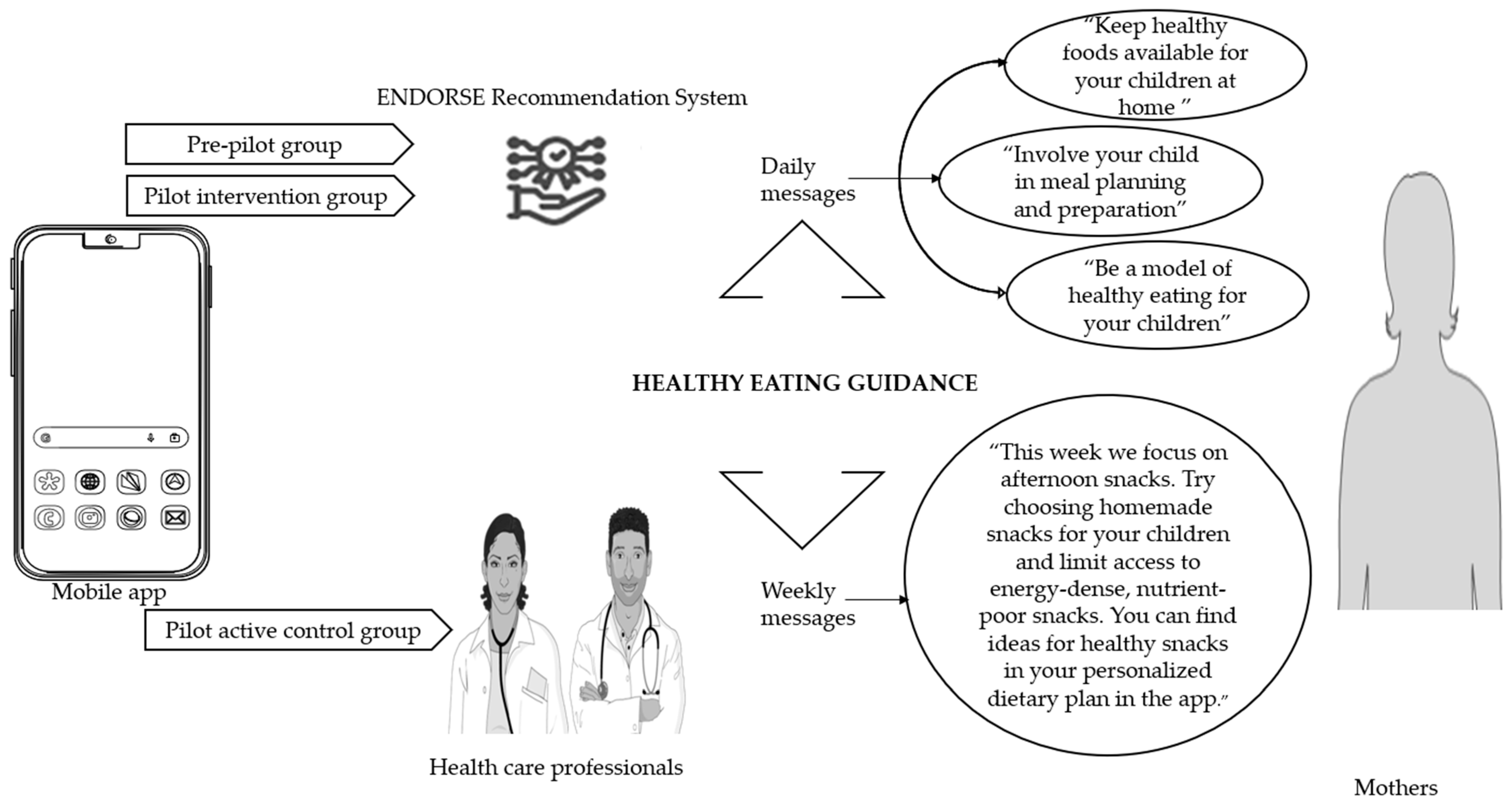
2.2. Study Implementation
2.3. Measures
2.3.1. Clinical Assessment
2.3.2. Laboratory Assessment
2.3.3. Nutritional Assessment
2.3.4. Assessment of Food Parenting Practices
2.3.5. Psychological Assessment
2.3.6. Sociodemographic Assessment of Mothers
2.4. Statistical Analysis
3. Results
3.1. Participant’s Characteristics
3.2. Changes in Cardiometabolic Factors According to BMI z-Score Change
3.3. Linear Regression Analysis between Change in BMI z-Score and Change in Metabolic Parameters of Children Participating in the ENDORSE Program
3.4. Food Parenting Practices and BMI z-Score Change
3.5. Linear Regression Analysis for Healthy Eating Guidance and BMI z-Score
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bomberg, E.M.; Ryder, J.R.; Brundage, R.C.; Straka, R.J.; Fox, C.K.; Gross, A.C.; Oberle, M.M.; Bramante, C.T.; Sibley, S.D.; Kelly, A.S. Precision Medicine in Adult and Pediatric Obesity: A Clinical Perspective. Ther. Adv. Endocrinol. Metab. 2019, 10, 2042018819863022. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.S.; Marcus, M.D.; Yanovski, J.A.; Yanovski, S.Z.; Osganian, S.K. Working toward Precision Medicine Approaches to Treat Severe Obesity in Adolescents: Report of an NIH Workshop. Int. J. Obes. 2018, 42, 1834–1844. [Google Scholar] [CrossRef]
- Ryder, J.R.; Kaizer, A.M.; Jenkins, T.M.; Kelly, A.S.; Inge, T.H.; Shaibi, G.Q. Heterogeneity in Response to Treatment of Adolescents with Severe Obesity: The Need for Precision Obesity Medicine. Obesity 2019, 27, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended International (IOTF) Body Mass Index Cut-Offs for Thinness, Overweight and Obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Skinner, A.C.; Perrin, E.M.; Moss, L.A.; Skelton, J.A. Cardiometabolic Risks and Severity of Obesity in Children and Young Adults. N. Engl. J. Med. 2015, 373, 1307–1317. [Google Scholar] [CrossRef]
- Spinelli, A.; Buoncristiano, M.; Kovacs, V.A.; Yngve, A.; Spiroski, I.; Obreja, G.; Starc, G.; Pérez, N.; Rito, A.I.; Kunešová, M.; et al. Prevalence of Severe Obesity among Primary School Children in 21 European Countries. Obes. Facts 2019, 12, 244–258. [Google Scholar] [CrossRef]
- Cena, H.; Fiechtner, L.; Vincenti, A.; Magenes, V.C.; De Giuseppe, R.; Manuelli, M.; Zuccotti, G.V.; Calcaterra, V. COVID-19 Pandemic as Risk Factors for Excessive Weight Gain in Pediatrics: The Role of Changes in Nutrition Behavior. A Narrative Review. Nutrients 2021, 13, 4255. [Google Scholar] [CrossRef]
- Androutsos, O.; Perperidi, M.; Georgiou, C.; Chouliaras, G. Lifestyle Changes and Determinants of Children’s and Adolescents’ Body Weight Increase during the First COVID-19 Lockdown in Greece: The COV-EAT Study. Nutrients 2021, 13, 930. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, E.A.; Evans, C.V.; Burda, B.U.; Walsh, E.S.; Eder, M.; Lozano, P. Screening for Obesity and Intervention for Weight Management in Children and Adolescents: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2017, 317, 2427–2444. [Google Scholar] [CrossRef]
- Reinehr, T.; Lass, N.; Toschke, C.; Rothermel, J.; Lanzinger, S.; Holl, R.W. Which Amount of BMI-SDS Reduction Is Necessary to Improve Cardiovascular Risk Factors in Overweight Children? J. Clin. Endocrinol. Metab. 2016, 101, 3171–3179. [Google Scholar] [CrossRef] [PubMed]
- El-Medany, A.Y.M.; Birch, L.; Hunt, L.P.; Matson, R.I.B.; Chong, A.H.W.; Beynon, R.; Hamilton-Shield, J.; Perry, R. What Change in Body Mass Index Is Required to Improve Cardiovascular Outcomes in Childhood and Adolescent Obesity through Lifestyle Interventions: A Meta-Regression. Child. Obes. 2020, 16, 449–478. [Google Scholar] [CrossRef] [PubMed]
- Clinical Practice Guideline for the Treatment of Obesity and Overweight in Children and Adolescents. Available online: https://www.apa.org/obesity-guideline (accessed on 29 December 2022).
- Barlow, S.E.; Expert Committee. Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report. Pediatrics 2007, 120 (Suppl. 4), S164–S192. [Google Scholar] [CrossRef]
- Wilfley, D.E.; Hayes, J.F.; Balantekin, K.N.; Van Buren, D.J.; Epstein, L.H. Behavioral Interventions for Obesity in Children and Adults: Evidence Base, Novel Approaches, and Translation into Practice. Am. Psychol. 2018, 73, 981–993. [Google Scholar] [CrossRef] [PubMed]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef]
- Di Pasquale, R.; Rivolta, A. A Conceptual Analysis of Food Parenting Practices in the Light of Self-Determination Theory: Relatedness-Enhancing, Competence-Enhancing and Autonomy-Enhancing Food Parenting Practices. Front. Psychol. 2018, 9, 2373. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.R.; Goodman, L.; Roberts, L.; Marx, J.; Taylor, M.; Hoffmann, D. An Examination of Food Parenting Practices: Structure, Control and Autonomy Promotion. Public Health Nutr. 2019, 22, 814–826. [Google Scholar] [CrossRef]
- Vaughn, A.E.; Ward, D.S.; Fisher, J.O.; Faith, M.S.; Hughes, S.O.; Kremers, S.P.J.; Musher-Eizenman, D.R.; O’Connor, T.M.; Patrick, H.; Power, T.G. Fundamental Constructs in Food Parenting Practices: A Content Map to Guide Future Research. Nutr. Rev. 2016, 74, 98–117. [Google Scholar] [CrossRef]
- Yee, A.Z.H.; Lwin, M.O.; Ho, S.S. The Influence of Parental Practices on Child Promotive and Preventive Food Consumption Behaviors: A Systematic Review and Meta-Analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 47. [Google Scholar] [CrossRef]
- Shloim, N.; Edelson, L.R.; Martin, N.; Hetherington, M.M. Parenting Styles, Feeding Styles, Feeding Practices, and Weight Status in 4–12 Year-Old Children: A Systematic Review of the Literature. Front. Psychol. 2015, 6, 1849. [Google Scholar] [CrossRef]
- Selzam, S.; McAdams, T.A.; Coleman, J.R.I.; Carnell, S.; O’Reilly, P.F.; Plomin, R.; Llewellyn, C.H. Evidence for Gene-Environment Correlation in Child Feeding: Links between Common Genetic Variation for BMI in Children and Parental Feeding Practices. PLoS Genet. 2018, 14, e1007757. [Google Scholar] [CrossRef] [PubMed]
- Langer, S.L.; Seburg, E.; JaKa, M.M.; Sherwood, N.E.; Levy, R.L. Predicting Dietary Intake among Children Classified as Overweight or at Risk for Overweight: Independent and Interactive Effects of Parenting Practices and Styles. Appetite 2017, 110, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Beckers, D.; Karssen, L.T.; Vink, J.M.; Burk, W.J.; Larsen, J.K. Food Parenting Practices and Children’s Weight Outcomes: A Systematic Review of Prospective Studies. Appetite 2021, 158, 105010. [Google Scholar] [CrossRef] [PubMed]
- Holland, J.C.; Kolko, R.P.; Stein, R.I.; Welch, R.R.; Perri, M.G.; Schechtman, K.B.; Saelens, B.E.; Epstein, L.H.; Wilfley, D.E. Modifications in Parent Feeding Practices and Child Diet during Family-Based Behavioral Treatment Improve Child ZBMI. Obesity 2014, 22, E119–E126. [Google Scholar] [CrossRef]
- Fowler, L.A.; Grammer, A.C.; Staiano, A.E.; Fitzsimmons-Craft, E.E.; Chen, L.; Yaeger, L.H.; Wilfley, D.E. Harnessing Technological Solutions for Childhood Obesity Prevention and Treatment: A Systematic Review and Meta-Analysis of Current Applications. Int. J. Obes. 2021, 45, 957–981. [Google Scholar] [CrossRef] [PubMed]
- Hammersley, M.L.; Jones, R.A.; Okely, A.D. Parent-Focused Childhood and Adolescent Overweight and Obesity EHealth Interventions: A Systematic Review and Meta-Analysis. J. Med. Internet Res. 2016, 18, e203. [Google Scholar] [CrossRef]
- Kouvari, M.; Karipidou, M.; Tsiampalis, T.; Mamalaki, E.; Poulimeneas, D.; Bathrellou, E.; Panagiotakos, D.; Yannakoulia, M. Digital Health Interventions for Weight Management in Children and Adolescents: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2022, 24, e30675. [Google Scholar] [CrossRef]
- Park, J.; Park, M.-J.; Seo, Y.-G. Effectiveness of Information and Communication Technology on Obesity in Childhood and Adolescence: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2021, 23, e29003. [Google Scholar] [CrossRef]
- Tully, L.; Burls, A.; Sorensen, J.; El-Moslemany, R.; O’Malley, G. Mobile Health for Pediatric Weight Management: Systematic Scoping Review. JMIR MHealth UHealth 2020, 8, e16214. [Google Scholar] [CrossRef]
- Calcaterra, V.; Verduci, E.; Vandoni, M.; Rossi, V.; Di Profio, E.; Carnevale Pellino, V.; Tranfaglia, V.; Pascuzzi, M.C.; Borsani, B.; Bosetti, A.; et al. Telehealth: A Useful Tool for the Management of Nutrition and Exercise Programs in Pediatric Obesity in the COVID-19 Era. Nutrients 2021, 13, 3689. [Google Scholar] [CrossRef]
- Garza, C.; Martinez, D.A.; Yoon, J.; Nickerson, B.S.; Park, K.-S. Effects of Telephone Aftercare Intervention for Obese Hispanic Children on Body Fat Percentage, Physical Fitness, and Blood Lipid Profiles. Int. J. Environ. Res. Public Health 2019, 16, 5133. [Google Scholar] [CrossRef]
- Baranowski, T.; Baranowski, J.; Chen, T.-A.; Buday, R.; Beltran, A.; Dadabhoy, H.; Ryan, C.; Lu, A.S. Videogames That Encourage Healthy Behavior Did Not Alter Fasting Insulin or Other Diabetes Risks in Children: Randomized Clinical Trial. Games Health J. 2019, 8, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Stephens, T.N.; Joerin, A.; Rauws, M.; Werk, L.N. Feasibility of Pediatric Obesity and Prediabetes Treatment Support through Tess, the AI Behavioral Coaching Chatbot. Transl. Behav. Med. 2019, 9, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Bonvicini, L.; Pingani, I.; Venturelli, F.; Patrignani, N.; Bassi, M.C.; Broccoli, S.; Ferrari, F.; Gallelli, T.; Panza, C.; Vicentini, M.; et al. Effectiveness of Mobile Health Interventions Targeting Parents to Prevent and Treat Childhood Obesity: Systematic Review. Prev. Med. Rep. 2022, 29, 101940. [Google Scholar] [CrossRef]
- Zarkogianni, K.; Chatzidaki, E.; Polychronaki, N.; Kalafatis, E.; Nicolaides, N.C.; Voutetakis, A.; Chioti, V.; Kitani, R.-A.; Mitsis, K.; Perakis, Κ.; et al. The ENDORSE Feasibility Study: Exploring the Use of M-Health, Artificial Intelligence and Serious Games for the Management of Childhood Obesity. Nutrients 2023, 15, 1451. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory and the Facilitation of Intrinsic Motivation, Social Development, and Well-Being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a Standard Definition for Child Overweight and Obesity Worldwide: International Survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef]
- Michou, M.; Panagiotakos, D.B.; Mamalaki, E.; Yannakoulia, M.; Costarelli, V. Development and Validation of the Greek Version of the Comprehensive Parental Feeding Questionnaire. Mediterr. J. Nutr. Metab. 2019, 12, 211–221. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.; Holub, S. Comprehensive Feeding Practices Questionnaire: Validation of a New Measure of Parental Feeding Practices. J. Pediatr. Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef]
- Tanner, J.M.; Whitehouse, R.H. Clinical Longitudinal Standards for Height, Weight, Height Velocity, Weight Velocity, and Stages of Puberty. Arch. Dis. Child. 1976, 51, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and Development. Vital Health Stat. 11 2002, 246, 1–190. [Google Scholar]
- Freedman, D.S.; Berenson, G.S. Tracking of BMI z Scores for Severe Obesity. Pediatrics 2017, 140, e20171072. [Google Scholar] [CrossRef]
- Browning, L.M.; Hsieh, S.D.; Ashwell, M. A Systematic Review of Waist-to-Height Ratio as a Screening Tool for the Prediction of Cardiovascular Disease and Diabetes: 0·5 Could Be a Suitable Global Boundary Value. Nutr. Res. Rev. 2010, 23, 247–269. [Google Scholar] [CrossRef]
- Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report. Pediatrics 2011, 128 (Suppl. 5), S213–S256. [Google Scholar] [CrossRef]
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2014, 37 (Suppl. 1), S81–S90. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- van der Aa, M.P.; Knibbe, C.A.J.; de Boer, A.; van der Vorst, M.M.J. Definition of Insulin Resistance Affects Prevalence Rate in Pediatric Patients: A Systematic Review and Call for Consensus. J. Pediatr. Endocrinol. Metab. 2017, 30, 123–131. [Google Scholar] [CrossRef]
- Schwimmer, J.B.; Dunn, W.; Norman, G.J.; Pardee, P.E.; Middleton, M.S.; Kerkar, N.; Sirlin, C.B. SAFETY Study: Alanine Aminotransferase Cutoff Values Are Set Too High for Reliable Detection of Pediatric Chronic Liver Disease. Gastroenterology 2010, 138, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Kastorini, C.-M.; Critselis, E.; Zota, D.; Coritsidis, A.L.; Nagarajan, M.K.; Papadimitriou, E.; Belogianni, K.; Benetou, V.; Linos, A.; Greek National Dietary Guidelines Scientific Team. National Dietary Guidelines of Greece for Children and Adolescents: A Tool for Promoting Healthy Eating Habits. Public Health Nutr. 2019, 22, 2688–2699. [Google Scholar] [CrossRef]
- Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academies Press: Washington, DC, USA, 2005; ISBN 978-0-309-08525-0.
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Patient Health Questionnaire (PHQ) Screeners. Available online: https://www.hrsa.gov/behavioral-health/patient-health-questionnaire-phq-screeners (accessed on 6 February 2023).
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric Features and Clinical Correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef]
- Simos, G. Investigation of Psychogenic Eating Disorders and Prevention Possibilities; Aristotle University of Thessaloniki: Thessaloniki, Greece, 1996. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Bibou-Nakou, I.; Kiosseoglou, G.; Stogiannidou, A. Strengths and Difficulties of School-Aged Children in the Family and School Context. Psychol. J. Hell. Psychol. Soc. 2001, 8, 506–525. [Google Scholar]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 6 February 2023).
- Bondyra-Wiśniewska, B.; Myszkowska-Ryciak, J.; Harton, A. Impact of Lifestyle Intervention Programs for Children and Adolescents with Overweight or Obesity on Body Weight and Selected Cardiometabolic Factors-A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 2061. [Google Scholar] [CrossRef]
- Ford, A.L.; Hunt, L.P.; Cooper, A.; Shield, J.P.H. What Reduction in BMI SDS Is Required in Obese Adolescents to Improve Body Composition and Cardiometabolic Health? Arch. Dis. Child. 2010, 95, 256–261. [Google Scholar] [CrossRef]
- Zhu, L.; Liu, J.; Yu, Y.; Tian, Z. Effect of High-Intensity Interval Training on Cardiometabolic Risk Factors in Childhood Obesity: A Meta-Analysis. J. Sports Med. Phys. Fit. 2021, 61, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Savoye, M.; Shaw, M.; Dziura, J.; Tamborlane, W.V.; Rose, P.; Guandalini, C.; Goldberg-Gell, R.; Burgert, T.S.; Cali, A.M.G.; Weiss, R.; et al. Effects of a Weight Management Program on Body Composition and Metabolic Parameters in Overweight Children: A Randomized Controlled Trial. JAMA 2007, 297, 2697–2704. [Google Scholar] [CrossRef] [PubMed]
- Kolsgaard, M.L.P.; Joner, G.; Brunborg, C.; Anderssen, S.A.; Tonstad, S.; Andersen, L.F. Reduction in BMI Z-Score and Improvement in Cardiometabolic Risk Factors in Obese Children and Adolescents. The Oslo Adiposity Intervention Study—A Hospital/Public Health Nurse Combined Treatment. BMC Pediatr. 2011, 11, 47. [Google Scholar] [CrossRef]
- Cordellat, A.; Padilla, B.; Grattarola, P.; García-Lucerga, C.; Crehuá-Gaudiza, E.; Núñez, F.; Martínez-Costa, C.; Blasco-Lafarga, C. Multicomponent Exercise Training Combined with Nutritional Counselling Improves Physical Function, Biochemical and Anthropometric Profiles in Obese Children: A Pilot Study. Nutrients 2020, 12, 2723. [Google Scholar] [CrossRef] [PubMed]
- Soltero, E.G.; Olson, M.L.; Williams, A.N.; Konopken, Y.P.; Castro, F.G.; Arcoleo, K.J.; Keller, C.S.; Patrick, D.L.; Ayers, S.L.; Barraza, E.; et al. Effects of a Community-Based Diabetes Prevention Program for Latino Youth with Obesity: A Randomized Controlled Trial. Obesity 2018, 26, 1856–1865. [Google Scholar] [CrossRef]
- Vos, M.B.; Abrams, S.H.; Barlow, S.E.; Caprio, S.; Daniels, S.R.; Kohli, R.; Mouzaki, M.; Sathya, P.; Schwimmer, J.B.; Sundaram, S.S.; et al. NASPGHAN Clinical Practice Guideline for the Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children: Recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN). J. Pediatr. Gastroenterol. Nutr. 2017, 64, 319–334. [Google Scholar] [CrossRef]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; O’Dea, K.; Desmond, P.V.; Johnson, N.A.; Wilson, A.M. The Mediterranean Diet Improves Hepatic Steatosis and Insulin Sensitivity in Individuals with Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef]
- Yanovski, J.A.; Yanovski, S.Z.; Gold, P.W.; Chrousos, G.P. Differences in Corticotropin-Releasing Hormone-Stimulated Adrenocorticotropin and Cortisol before and after Weight Loss. J. Clin. Endocrinol. Metab. 1997, 82, 1874–1878. [Google Scholar] [CrossRef]
- Reinehr, T.; Kulle, A.; Wolters, B.; Lass, N.; Welzel, M.; Riepe, F.; Holterhus, P.-M. Steroid Hormone Profiles in Prepubertal Obese Children before and after Weight Loss. J. Clin. Endocrinol. Metab. 2013, 98, E1022–E1030. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; Andler, W. Cortisol and Its Relation to Insulin Resistance before and after Weight Loss in Obese Children. Horm. Res. 2004, 62, 107–112. [Google Scholar] [CrossRef]
- Stasinaki, A.; Büchter, D.; Shih, C.-H.I.; Heldt, K.; Güsewell, S.; Brogle, B.; Farpour-Lambert, N.; Kowatsch, T.; l’Allemand, D. Effects of a Novel Mobile Health Intervention Compared to a Multi-Component Behaviour Changing Program on Body Mass Index, Physical Capacities and Stress Parameters in Adolescents with Obesity: A Randomized Controlled Trial. BMC Pediatr. 2021, 21, 308. [Google Scholar] [CrossRef]
- Gomes, A.I.; Pereira, A.I.; Roberto, M.S.; Boraska, K.; Barros, L. Changing Parental Feeding Practices through Web-Based Interventions: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0250231. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.O.; Power, T.G.; Orlet Fisher, J.; Mueller, S.; Nicklas, T.A. Revisiting a Neglected Construct: Parenting Styles in a Child-Feeding Context. Appetite 2005, 44, 83–92. [Google Scholar] [CrossRef]
- Hughes, S.O.; Power, T.G.; Papaioannou, M.A.; Cross, M.B.; Nicklas, T.A.; Hall, S.K.; Shewchuk, R.M. Emotional Climate, Feeding Practices, and Feeding Styles: An Observational Analysis of the Dinner Meal in Head Start Families. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 60. [Google Scholar] [CrossRef] [PubMed]
- Lopez, B.A.; Nicholson, J.S.; Garcia, R.N.; Johnson, H.R.; Power, T.G.; Hughes, S.O. Review and Meta-Analysis for the Caregiver’s Feeding Styles Questionnaire Administered to Low-Income Families. Eat. Behav. 2022, 46, 101659. [Google Scholar] [CrossRef]
- Herle, M.; Fildes, A.; Steinsbekk, S.; Rijsdijk, F.; Llewellyn, C.H. Emotional Over- and under-Eating in Early Childhood Are Learned Not Inherited. Sci. Rep. 2017, 7, 9092. [Google Scholar] [CrossRef]
- Steinsbekk, S.; Barker, E.D.; Llewellyn, C.; Fildes, A.; Wichstrøm, L. Emotional Feeding and Emotional Eating: Reciprocal Processes and the Influence of Negative Affectivity. Child Dev. 2018, 89, 1234–1246. [Google Scholar] [CrossRef] [PubMed]
- Carnell, S.; Haworth, C.M.A.; Plomin, R.; Wardle, J. Genetic Influence on Appetite in Children. Int. J. Obes. 2008, 32, 1468–1473. [Google Scholar] [CrossRef]
- Fildes, A.; van Jaarsveld, C.H.; Cooke, L.; Wardle, J.; Llewellyn, C.H. Common Genetic Architecture Underlying Young Children’s Food Fussiness and Liking for Vegetables and Fruit123. Am. J. Clin. Nutr. 2016, 103, 1099–1104. [Google Scholar] [CrossRef]
- Hampl, S.E.; Hassink, S.G.; Skinner, A.C.; Armstrong, S.C.; Barlow, S.E.; Bolling, C.F.; Avila Edwards, K.C.; Eneli, I.; Hamre, R.; Joseph, M.M.; et al. Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents with Obesity. Pediatrics 2023, 151, e2022060640. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.C.; Blissett, J.M.; Brunstrom, J.M.; Carnell, S.; Faith, M.S.; Fisher, J.O.; Hayman, L.L.; Khalsa, A.S.; Hughes, S.O.; Miller, A.L.; et al. Caregiver Influences on Eating Behaviors in Young Children: A Scientific Statement From the American Heart Association. J. Am. Heart Assoc. 2020, 9, e014520. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 45) | Group 1 Decrease in BMI z-Score ≥0.2 (n = 21) | Group 2 Decrease in BMI z-Score ≥0.0 <−0.2 (n = 16) | Group 3 Increase in BMI z-Score >0.00–0.25 (n = 8) | * p Value for Differences between Groups |
|---|---|---|---|---|---|
| Mean Follow-up Duration (Baseline to the last visit, months) | 4.71 (1.05) | 4.53 (0.91) | 4.52 (1.09) | 5.52 (1.02) | 0.050 |
| Age (years) | 10.42 (2.04) | 10.27 (2.17) | 10.64 (1.64) | 10.41 (2.61) | 0.867 |
| Sex | 0.349 | ||||
| Female | 24 (53.3) | 11 (52.4) | 7 (43.8) | 6 (75.0) | |
| Male | 21 (46.7) | 10 (47.6) | 9 (56.3) | 2 (25.0) | |
| Pubertal Stage | 0.840 | ||||
| Prepubertal | 19 (42.2) | 9 (42.9) | 6 (37.5) | 4 (50.0) | |
| Pubertal | 26 (57.8) | 12 (57.1) | 10 (62.5) | 4 (50.0) | |
| Weight (kg) | 69.42 (23.48) | 72.39 (26.25) | 66.41 (21.54) | 67.65 (21.28) | 0.734 |
| Height (m) | 1.49 (0.14) | 1.49 (0.14) | 1.49 (0.12) | 1.48 (0.17) | 0.993 |
| BMI (kg/m2) | 30.52 (6.46) | 31.59 (6.85) | 29.32 (6.62) | 30.08 (5.21) | 0.568 |
| BMI z-score | 2.83 (2.22, 3.97) | 3.18 (2.67, 4.32) | 2.47 (2.00, 3.03) | 2.36 (1.95, 4.97) | 0.109 |
| Weight Status (IOTF) [4] | 0.457 | ||||
| Overweight | 4 (8.9) | 2 (9.5) | 1 (6.3) | 1 (12.5) | |
| Simple Obesity | 23 (51.1) | 8 (38.1) | 11 (68.8) | 4 (50.0) | |
| Severe Obesity | 18 (40.0) | 11 (52.4) | 4 (25.0) | 3 (37.5) | |
| Waist-to-Height Ratio | 0.63 (0.08) | 0.64 (0.09) | 0.60 (0.06) | 0.64 (0.07) | 0.176 |
| Systolic BP (mmHg) | 115.0 (108.0, 120.0) | 115.0 (109.5, 120.0) | 115.0 (104.5, 120.8) | 115.0 (109.3, 116.5) | 0.902 |
| Diastolic BP (mmHg) | 73.84 (8.40) | 73.95 (9.72) | 73.06 (6.82) | 75.13 (8.41) | 0.855 |
| Characteristics | Total (n = 45) | Group 1 Decrease in BMI z-Score ≥0.2 (n = 21) | Group 2 Decrease in BMI z-Score ≥0.0 <−0.2 (n = 16) | Group 3 Increase in BMI z-Score >0.00–0.25 (n = 8) | * p Value for Differences between Groups |
|---|---|---|---|---|---|
| Glucose (mg/dL) | 90.02 (7.71) | 92.76 (9.02) | 86.69 (5.39) | 89.43 (5.13) | 0.055 |
| Insulin (μUI/mL) | 23.90 (17.80, 35.40) | 30.55 (18.88, 39.33) | 23.40 (17.80, 28.80) | 22.15 (12.73, 32.68) | 0.302 |
| HOMA IR | 5.60 (4.05, 7.68) | 7.04 (4.28, 9.80) | 4.62 (3.96, 6.07) | 4.48 (2.19, 6.18) | 0.110 |
| HbA1c (%) | 5.44 (0.28) | 5.39 (0.30) | 5.46 (0.27) | 5.51 (0.26) | 0.566 |
| Cholesterol (mg/dL) | 158.31 (25.72) | 165.28 (26.19) | 156.00 (22.67) | 145.50 (27.65) | 0.168 |
| LDL Cholesterol (mg/dL) | 88.77 (21.65) | 94.35 (22.04) | 85.25 (17.92) | 81.88 (26.45) | 0.284 |
| HDL Cholesterol (mg/dL) | 49.60 (11.10) | 48.53 (11.13) | 52.88 (11.89) | 45.75 (8.55) | 0.287 |
| Triglycerides (mg/dL) | 85.00 (60.25, 133.25) | 104.00 (64.25, 162.25) | 80.00 (53.00, 94.25) | 84.00 (60.25, 120.50) | 0.512 |
| SGPT (U/L) | 22.00 (15.50, 31.00) | 25.00 (14.50, 35.50) | 25.00 (17.25, 35.25) | 16.00 (11.75, 19.00) | 0.071 |
| SGOT (U/L) | 23.00 (17.00, 26.50) | 22.00 (17.00, 26.00) | 24.50 (17.25, 29.25) | 23.00 (16.00, 24.75) | 0.627 |
| Cortisol (μg/dL) | 13.54 (5.12) | 15.10 (5.60) | 12.43 (3.72) | 11.45 (5.55) | 0.156 |
| ACTH (pg/mL) | 23.15 (15.35, 23.95) | 24.10 (12.80, 40.15) | 20.80 (16.10, 25.00) | 31.10 (14.90, 39.20) | 0.713 |
| Characteristics | Total (n = 45) | Group 1 Decrease in BMI z-Score ≥0.2 (n = 21) | Group 2 Decrease in BMI z-Score ≥0.0 <−0.2 (n = 16) | Group 3 Increase in BMI z-Score >0.00–0.25 (n = 8) | * p Value for Differences between Groups |
|---|---|---|---|---|---|
| Maternal age (years) | 43.89 (5.40) | 44.19 (5.47) | 43.75 (3.32) | 43.38 (8.55) | 0.931 |
| Maternal BMI (kg/m2) | 30.18 (6.15) | 30.74 (6.15) | 30.60 (6.40) | 27.85 (5.84) | 0.509 |
| Mothers of Greek origin | 43 (95.6) | 20 (95.2) | 16 (100.0) | 7 (87.5) | 0.373 |
| Married mothers | 35 (77.8) | 18 (85.7) | 11 (68.8) | 6 (75.0) | 0.459 |
| Maternal education | 0.881 | ||||
| Primary | 4 (8.9) | 2 (9.5) | 1 (6.3) | 1 (12.5) | |
| Secondary | 23 (51.3) | 12 (57.1) | 8 (50.0) | 3 (37.5) | |
| Tertiary | 18 (40.0) | 7 (33.3) | 7 (43.8) | 4 (50.0) | |
| Annual income | 0.823 | ||||
| Less than 10,000 euros/year | 11 (24.4) | 7 (33.3) | 3 (18.8) | 1 (12.5) | |
| 10,000–20,000 euros/year | 10 (22.2) | 5 (23.8) | 3 (18.8) | 2 (25) | |
| More than 20,000 euros/year | 4 (8.9) | 2 (9.5) | 1 (6.3) | 1 (12.5) | |
| Omission | 20 (44.4) | 7 (33.3) | 9 (56.3) | 4 (50) | |
| Satisfaction from income | 0.490 | ||||
| (5-point Likert scale) | |||||
| Very dissatisfied | 11 (24.4) | 6 (28.6) | 4 (25) | 1 (12.5) | |
| Dissatisfied | 6 (13.3) | 3 (14.3) | 1 (6.3) | 2 (25) | |
| Neither satisfied nor dissatisfied | 21 (46.7) | 10 (47.6) | 8 (50) | 3 (37.5) | |
| Satisfied | 6 (13.3) | 2 (9.5) | 3 (18.8) | 1 (12.5) | |
| Very satisfied | 1 (2.2) | 0 | 0 | 1 (12.5) | |
| Employed Mothers | 35 (77.8) | 16 (76.2) | 13 (81.3) | 6 (75.0) | 0.915 |
| Depressive Symptomatology | |||||
| PHQ-9 score ≥ 10 | 9 (20.0) | 5 (23.8) | 4 (25.0) | - | 0.295 |
| Eating disorders symptomatology | |||||
| EAT-26 score ≥ 20 | 7 (15.6) | 3 (14.3) | 2 (12.5) | 2 (25.0) | 0.711 |
| Feeding practices (CFPQ) | |||||
| (5-point Likert scale) | |||||
| Monitoring | 4.11 (0.77) | 4.15 (0.84) | 4.09 (0.71)) | 4.00 (0.79) | 0.762 |
| Child Control | 2.91 (0.67) | 2.81 (0.79) | 3.10 (0.54) | 2.78 (0.55) | 0.413 |
| Emotional Regulation/Food as Reward | 2.05 (0.73) | 2.02 (0.73) | 2.01 (0.72) | 2.21 (0.84) | 0.852 |
| Healthy Eating Guidance | 4.27 (0.49) | 4.25 (0.45) | 4.15 (0.58) | 4.54 (0.35) | 0.216 |
| Restriction | 3.65 (0.69) | 3.63 (0.73) | 3.60 (0.74) | 3.80 (0.55) | 0.817 |
| Pressure to eat | 1.35 (0.50) | 1.29 (0.41) | 1.42 (0.45) | 1.37 (0.80) | 0.497 |
| SDQ total score group | 0.385 | ||||
| (parental version) | |||||
| Clinical | 4 (8.9) | 2 (9.5) | 1 (6.3) | 1 (12.5) | |
| Borderline | 7 (15.6) | 2 (9.5) | 2 (12.5) | 3 (37.5) | |
| Normal | 34 (75.6) | 17 (81.0) | 13 (81.3) | 4 (50.0) |
| Total | Group 1 Decrease in BMI z-Score ≥0.2 | Group 2 Decrease in BMI z-Score ≥0.0 <−0.2 | Group 3 Increase in BMI z-Score >0.00–0.25 | * p-Value for Differences between Groups | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | n | n | n | ||||||
| BMI z-score | 45 | −0.21 (0.26) | 21 | −0.43 (0.20) | 16 | −0.08 (0.06) | 8 | 0.12 (0.09) | <0.001 |
| Waist-to-height ratio | 44 | −0.001 (0.04) | 20 | −0.02 (0.03) | 16 | 0.01 (0.04) | 8 | 0.02 (0.02) | 0.003 |
| Systolic BP (mmHg) | 44 | −1.05 (12.25) | 20 | 0.45 (13.10) | 16 | −4.44 (13.38) | 8 | 2.00 (5.37) | 0.373 |
| Diastolic BP (mmHg) | 44 | −0.50 (6.67) | 20 | −1.65 (9.02) | 16 | −0.25 (7.07) | 8 | 1.88 (4.79) | 0.550 |
| Glucose (mg/dL) | 44 | −0.80 (7.73) | 21 | −2.76 (8.61) | 16 | 4.44 (6.51) | 7 | 0.0001 (6.9) | 0.256 |
| Insulin (μUI/mL) | 43 | −2.04 (10.99) | 20 | −4.86 (13.05) | 15 | −1.21 (8.55) | 8 | 3.46 (7.63) | 0.162 |
| HOMA-IR | 42 | −0.50 (2.83) | 20 | −1.27 (3.46) | 15 | −0.13 (2.03) | 7 | 0.94 (1.53) | 0.133 |
| HbA1c (%) | 42 | −0.10 (0.24) 1 | 20 | −0.05 (0.22) | 14 | −0.24 (0.27) 1 | 8 | 0.001 (0.16) | 0.026 |
| Total cholesterol (mg/dL) | 44 | 0.38 (15.29) | 20 | −4.43 (12.10) | 16 | −0.63 (12.07) | 8 | 14.38 (19.32) | 0.009 |
| LDL cholesterol (mg/dL) | 43 | 0.44 (12.01) | 19 | −4.63 (10.71) | 16 | 0.81 (8.58) | 8 | 11.75 (14.04) 1 | 0.003 |
| HDL chole−−sterol (mg/dL) | 44 | 0.55 (7.39) | 20 | 2.02 (6.85) | 16 | −3.06 (7.58) | 8 | 4.13 (5.89) | 0.073 |
| Triglycerides (mg/dL) | 44 | −5.84 (42.33) | 20 | −17.75 (41.81) | 16 | 8.69 (48.96) | 8 | −5.13 (15.39) | 0.257 |
| SGOT (U/L) | 45 | −1.84 (5.12) 1 | 21 | −0.95 (5.91) | 16 | −2.88 (3.16) | 8 | −2.13 (6.22) | 0.493 |
| SGPT (U/L) | 45 | −2.95 (9.07) 1 | 21 | −4.85 (8.89) | 16 | −4.25 (6.72) | 8 | 4.63 (10.72) | 0.104 |
| Cortisol (μg/dL) | 42 | −1.54 (5.86) | 20 | −3.87 (6.34) 1 | 15 | 0.06 (5.10) | 7 | 1.66 (3.25) | 0.037 |
| ACTH (pg/mL) | 38 | −1.37 (32.25) | 17 | −11.23 (21.87) 1 | 14 | 11.04 (44.61) | 7 | −2.23 (13.85) | 0.317 |
| Independent Variables | Dependent Variable: HOMA-IR Change (μUI/mL) (n = 42) | ||||
|---|---|---|---|---|---|
| Beta-Coefficient | Standard Error | 95% Confidence Interval | * p-Value | ||
| BMI z-score change | 3.60 | 1.74 | 0.07 | 7.14 | 0.046 |
| Baseline pubertal stage | 0.50 | 1.27 | −2.08 | 3.08 | 0.697 |
| Sex | −1.82 | 1.13 | −4.12 | 0.47 | 0.116 |
| Baseline BMI z-score | −0.16 | 0.32 | −0.81 | 0.48 | 0.610 |
| Baseline age (years) | −0.24 | 0.37 | −0.99 | 0.50 | 0.512 |
| Independent Variables | Dependent Variable: SGPT Change (U/L) (n = 45) | ||||
|---|---|---|---|---|---|
| Beta-Coefficient | Standard Error | 95% Confidence Interval | * p-Value | ||
| BMI z-score change | 11.90 | 5.52 | 0.74 | 23.06 | 0.037 |
| Baseline pubertal stage | −0.46 | 3.91 | −8.37 | 7.46 | 0.907 |
| Sex | 2.93 | 3.36 | −3.87 | 9.74 | 0.388 |
| Baseline BMI z-score | 0.91 | 1.02 | −1.15 | 2.98 | 0.375 |
| Age at baseline (years) | 0.58 | 1.06 | −1.56 | 2.72 | 0.587 |
| Independent Variables | Dependent Variable: Cortisol Change (μg/dL) (n = 42) | ||||
|---|---|---|---|---|---|
| Beta-Coefficient | Standard Error | 95% Confidence Interval | * p-Value | ||
| BMI z-score change | 9.96 | 3.58 | 2.71 | 17.22 | 0.008 |
| Baseline pubertal stage | −4.35 | 2.63 | −9.68 | 0.98 | 0.106 |
| Sex | 1.33 | 2.15 | −3.04 | 5.70 | 0.542 |
| Baseline BMI z-score | −0.32 | 0.64 | −1.61 | 0.97 | 0.622 |
| Age at baseline (years) | 0.59 | 0.69 | −0.82 | 1.99 | 0.402 |
| Total | Group 1 Decrease in BMI z-Score ≥0.2 | Group 2 Decrease in BMI z-Score ≥0.0 <−0.2 | Group 3 Increase in BMI z-Score >0.00–0.25 | * p-Value for Differences between Groups | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | n | n | n | ||||||
| Healthy eating guidance | 42 | 0.11 (0.38) 1 | 19 | 0.23 (0.41) | 15 | 0.14 (0.30) | 8 | −0.21 (0.29) | 0.013 |
| Monitoring | 42 | 0.14 (0.69) | 19 | 0.18 (0.36) | 15 | 0.13 (0.72) | 8 | 0.06 (0.56) | 0.845 |
| Child control | 42 | −0.12 (0.59) | 19 | −0.21 (0.58) | 15 | −0.24 (0.62) | 8 | 0.33 (0.37) | 0.037 |
| Emotional feeding/Food as reward | 42 | −0.21 (0.48) 2 | 19 | −0.35 (0.48) | 15 | −0.10 (0.46) | 8 | −0.10 (0.53) | 0.257 |
| Restriction | 42 | −0.13 (0.55) | 19 | −0.34 (0.65) | 15 | 0.01 (0.31) | 8 | −0.40 (0.61) | 0.169 |
| Pressure to eat | 42 | 0.16 (0.74) | 19 | 0.19 (0.87) | 15 | 0.20 (0.75) | 8 | 0.04 (0.33) | 0.953 |
| Independent Variables | Dependent Variable: BMI z-Score Change (n = 42) | ||||
|---|---|---|---|---|---|
| Beta-Coefficient | Standard Error | 95% Confidence Interval | * p-Value | ||
| Healthy eating guidance change | −0.29 | 0.10 | −0.49 | −0.08 | 0.007 |
| Maternal education | 0.05 | 0.06 | −0.08 | 0.18 | 0.40 |
| Maternal marital status | −0.07 | 0.09 | −0.26 | 0.12 | 0.489 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pervanidou, P.; Chatzidaki, E.; Nicolaides, N.C.; Voutetakis, A.; Polychronaki, N.; Chioti, V.; Kitani, R.-A.; Kyrkopoulou, E.; Zarkogianni, K.; Kalafatis, E.; et al. The Impact of the ENDORSE Digital Weight Management Program on the Metabolic Profile of Children and Adolescents with Overweight and Obesity and on Food Parenting Practices. Nutrients 2023, 15, 1777. https://doi.org/10.3390/nu15071777
Pervanidou P, Chatzidaki E, Nicolaides NC, Voutetakis A, Polychronaki N, Chioti V, Kitani R-A, Kyrkopoulou E, Zarkogianni K, Kalafatis E, et al. The Impact of the ENDORSE Digital Weight Management Program on the Metabolic Profile of Children and Adolescents with Overweight and Obesity and on Food Parenting Practices. Nutrients. 2023; 15(7):1777. https://doi.org/10.3390/nu15071777
Chicago/Turabian StylePervanidou, Panagiota, Evi Chatzidaki, Nicolas C. Nicolaides, Antonis Voutetakis, Nektaria Polychronaki, Vassiliki Chioti, Rosa-Anna Kitani, Eleni Kyrkopoulou, Konstantia Zarkogianni, Eleftherios Kalafatis, and et al. 2023. "The Impact of the ENDORSE Digital Weight Management Program on the Metabolic Profile of Children and Adolescents with Overweight and Obesity and on Food Parenting Practices" Nutrients 15, no. 7: 1777. https://doi.org/10.3390/nu15071777
APA StylePervanidou, P., Chatzidaki, E., Nicolaides, N. C., Voutetakis, A., Polychronaki, N., Chioti, V., Kitani, R.-A., Kyrkopoulou, E., Zarkogianni, K., Kalafatis, E., Mitsis, K., Perakis, Κ., Nikita, K., & Kanaka-Gantenbein, C. (2023). The Impact of the ENDORSE Digital Weight Management Program on the Metabolic Profile of Children and Adolescents with Overweight and Obesity and on Food Parenting Practices. Nutrients, 15(7), 1777. https://doi.org/10.3390/nu15071777