

Systematic Review on Protocols of Coenzyme Q10 Supplementation in Non-Surgical Periodontitis Therapy

Abstract
1. Introduction
2. Materials and Methods
2.1. Focused Question and Selection Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
3. Results
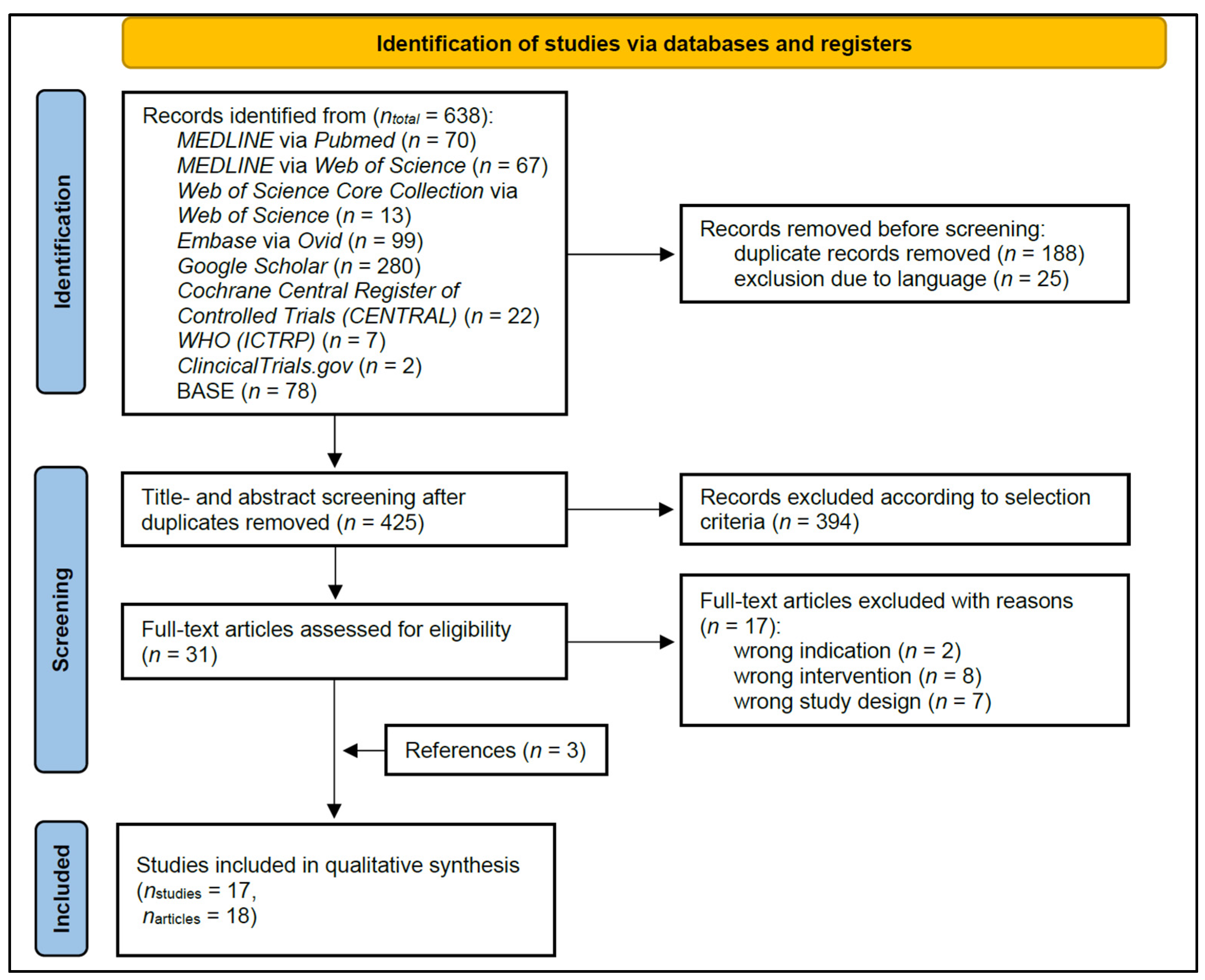
3.1. Study Selection (Figure 1)

3.2. Characteristics of the Included Studies (Table 1)

{kind=link}
{kind=link}
| Type of CoQ10 Administration Local/ Systemic) | Study | Country of Investigation | Observation Period Total (Time-Points) | Design SM/ FM | Participants n Total; Age Range (Mean ± SD); Sex f/m; nt/s: Teeth/sites | Periodontal Disease Periodontal Inclusion Criteria | Systemic Conditions Smoking Status; Systemic Diseases | Study Groups (np: Participants, ns: Sites) | Outcome Measures with Interest of the Review |
|---|---|---|---|---|---|---|---|---|---|
| Local | Attia et al., 2016 [42] | Egypt | 30 D | FM | n = 28; 29–46 (38 ± 6); 18 f, 10 m | CP, mild to moderate; PPD ≤ 6 mm, CAL ≤ 4 mm | Non-smokers; free from any systemic diseases (modified Cornell medical index) | Test group (np = 14): SRP + CoQ10 Control group (np = 14): SRP | PPD, CAL; LS; SL |
| Barakat et al., 2019 [47] | Saudi Arabia | 30 D | SM | n = 20; 25–60 (40 ± 4.33); 0 f, 20 m | CP, moderate | Systemically healthy (Cornell medical index) | Test group (np = 20): SRP + CoQ10 Control group (np = 20): SRP | PPD, CAL; BI; PI | |
| Chaudhry et al., 2014 [43] | India | 30 D (15 D) | n.r. | 20–50; both sexes; ns = 24 | CP, generalized; PPD = 4–8 mm | No smokers; no systemic diseases, not pregnant, not lactating | Test group (ns = 12): SRP + CoQ10 Control group (ns = 12): SRP | PPD, RAL; LS; TGG | |
| Hans et al., 2012 [38] | India | 6 W (3 W) | SM | n = 12; 22–55; both sexes; ≥4 sites per quadrant | CP, generalized; PPD = 4–8 mm; diagnosed clinically and radiographically | No smokers; no systemic diseases | Test group (np = 12, ns ≥ 4): SRP + CoQ10 Control group (np = 12, ns ≥ 4): SRP Additional group I (np = 12, ns ≥ 4): CoQ10 topical Additional group II (np = 12, ns ≥ 4): CoQ10 intrasulcular | PPD, CAL; LS, GBI; SL | |
| Jha et al., 2018 [46] | India | 3 M (4 W) | FM/SM | n = 30; 22–55; both sexes | CP; PPD = 4–8 mm | No smokers; systemically healthy | Test group (np = 15): SRP + CoQ10 Control group (np = 15): SRP Additional group (np = 15, SM with CoQ10): Lycopene | PPD, RAL; mSBIa | |
| Pranam et al., 2020 [48] | India | 3 M (1 M) | SM | n = 16; 30–50 (42); 7 f, 9 m; ns = 64 (4 per participant) | CP, mild to moderate; PPD = 5–7 mm (in four non-adjacent interproximal sites) | No history of tobacco usage; no relevant medical history, not pregnant, not lactating | Test group (ns = 32): SRP + CoQ10 Control group (ns = 32): SRP + placebo | PPD, CAL; LS; TGG | |
| Raut et al., 2019 [44] | India | 3 M (4 W) | FM | n = 40; 20–60 (37.4 ± 9.76) | CP, moderate to severe; PPD ≥ 5 mm, CAL ≥ 4 mm; diagnosed clinically and radiographically | Only current smokers with 10 cigarettes per day for min. 5 years; systemically healthy | Test group (np = 20): SRP + CoQ10 Control group (np = 20): SRP | PPD, CAL; mSBI; SL | |
| Raut et al., 2016 [49] | India | 1 M | SM | n = 15; 20–60 (37.4 ± 9.76); 9 f, 6 m; ≥3 sites per participant | CP, moderate to severe, untreated; PPD > 5 mm, CAL > 4 mm; diagnosed clinically and radiographically | No smoking > 10 cigarettes per day; no systemic disease that affects the periodontium | Test group (np = 15, ns = 15): SRP + CoQ10 Control group (np = 15, ns = 15): SRP + placebo (methyl cellulose gel) Additional group (np = 15, ns = 15): SRP + Tea-tree oil | PPD, CAL; SBI; SL | |
| Sale et al., 2014 [50] | India | 4 W (2 W) | SM | n = 18; 20–55 (33.8); both sexes; min. 6 teeth per quadrant | CP; PPD ≥ 5 mm (in different quadrants); diagnosed clinically and radiographically | No smokers; no systemic diseases | Test group I (np = 18): SRP + intrasulcular CoQ10 Test group II (np = 18): SRP + topical CoQ10 Control group (np = 18): SRP | PPD; LS, UBI; SL | |
| Salih et al., 2016 [51] | Iraq | 6 W (3 W) | SM | n = 15; 33–55; min. 20 teeth | CP; PPD = 5–8 mm at min. 4 sites per quadrant CAL ≥ 1–2 mm | No smokers; systemically healthy | Test group (np = 15, ns = 106): SRP + CoQ10 Control group (np = 15, ns = 106): SRP Additional group (np = 15, ns = 111): CoQ10 | PPD, RAL; LS, UP; SL | |
| Shaheen et al., 2020 [52] | Egypt | 7 W | SM | n = 15; 33–55; min. 20 teeth | Moderate periodontitis; PPD = 3–5 mm, CAL = 3–4 mm; diagnosed clinically and radiographically | No smokers; no systemic diseases | Test group (np = 15): SRP + CoQ10 Control group (np = 15): SRP | PPD, CAL; LS, PBI; SL | |
| Sharma et al., 2016 [53] | India | 6 W (1 W, 2 W) | SM | n = 24; 25–55 | CP, generalized; PPD ≥ 5 mm, BOP+ | No systemic diseases | Test group (np = 24, ns = 40): SRP + CoQ10 Control group (np = 24, ns = 40): SRP Additional group (np = 24, ns = 40): SRP + Hyaluronic acid | PPD, CAL; EIBI, GCCI; SL | |
| Systemic | Darweesh et al., 2015 [36] | Egypt | 3 M (1 M) | FM | n = 40; 37–55 (46.9 ± 5.7); 14 f, 26 m | CP, generalized moderate to severe; CAL > 3 mm | No smoking; no acute or chronic systemic disorders such as diabetes, hemorrhagic disorders cardio-vascular diseases, and conditions possibly affecting wound healing or interfering with the treatment or affecting patient’s compliance | Test group (np = 10): SRP + CoQ10 Control group (np = 10): SRP Additional group I (np = 10): SRP + Doxycycline Additional group II (np = 10): SRP + CoQ10 + Doxycycline | PPD, CAL; GI, BI; PI |
| Mani et al., 2013 [39] | India | 4 M (2 M) | FM | n = 100; 18–55 | CP, generalized | No smokers, no tobacco in any form; no diabetes, arthritis, heart diseases, obesity, neurological disorders, or diseases with possible effects on the immune system | Test group I (np = 25): SRP + CoQ10 (with chlorine dioxide toothpaste and mouthwash), Test group II (np = 25): SRP + CoQ10 (with conventional toothpaste and mouthwash) Control group I (np = 25): SRP (with chlorine dioxide toothpaste and mouthwash Control group II (np = 25): SRP (with conventional toothpaste and mouthwash) | PPD, CAL; LS; TGG | |
| Pandav et al., 2021 [35] | India | 3 M (6 W) | FM | n = 60; 30–60 | CP; PPD = 3–5 mm, BOP+ | No smokers; systemically healthy | Test group (np = 20): SRP + CoQ10 Control group (np = 20): SRP Additional group (np = 20): CoQ10 | PPD, RAL; LS | |
| Saini et al., 2014 [37] | India | 4 M (2 M) | FM | n = 50; 18–55; 21 f, 29 m | CP, generalized | No smokers, no tobacco in any form; No diabetes, arthritis, heart diseases, obesity, neurological disorders, or diseases with possible effects on the immune system | Test group (np = 25): SRP + CoQ10 Control group (np = 25): SRP | PPD, CAL; GIa; PI | |
| Shoukheba et al., 2019 [45] | Egypt | 6 M (4 W, 3 M) | FM | n = 30; 30–50; 18 f, 12 m | CP, generalized moderate; CAL = 4–5 mm | No smokers, no tobacco in any form; diabetes mellitus type II (HbA1c: 6–8%) and no further systemic diseases | Test group (np = 15): SRP + CoQ10 Control group (np = 15): SRP + Placebo | PPD, CAL; LS, MS |
3.2.1. Study Samples (Table 1)
3.2.2. Treatment Modalities (Table 2)
| Type of CoQ10 Administration (Local/Systemic) | Study (Name, Year) | CoQ10 Supplement Product; Dose; Amount as Reported | Placebo-Controlled (Yes, No) | CoQ10 Administration (Application Method; Timepoints, Duration of Application; Instructions after Application) | Procedures (Pre-Treatment; SRP Protocol; Oral Hygiene Instructions) |
|---|---|---|---|---|---|
| Local | Attia et al., 2016 [42] | Perio Q gel, PerioQ INC, Manchester, USA; gel; 1:9 | No | Intrasulcular, isolation (cotton rolls), drying (paper points) + blunted needle tip; at day 0–day 7–day 15; restriction for eating, spitting, drinking for one hour, brushing, and flossing for four hours after application | SRP (in 3 visits); instructions for plaque control regimen and oral hygiene provided at each appointment, no use of mouthwashes (exclusion criteria) |
| Barakat et al., 2019 [47] | Perio QTM gel, Hamilton, USA; gel; 0.2 ml | No | Intrasulcular, one time, directly after SRP, periodontal dressing for 1 week | SRP (in 2 visits) using ultrasonic scaler and Gracey curettes | |
| Chaudhry et al., 2014 [43] | Perio QTM gel, Hamilton, USA; 0.2 ml | No | Intrasulcular, syringe; one time, directly after SRP | SRP using ultrasonic scaler | |
| Hans et al., 2012 [38] | PerioQ gel, PerioQ INC, Manchester, USA; gel; 1:9 | No | Intrasulcular, drying (paper points), syringe with irrigation needle (Max-i-probe, Dentsply, USA); one time, one day after SRP | SRP (one day after recording of clinical parameter) with ultrasonic scaler and hand instruments | |
| Jha et a. 2018 [46] | Gel; 2%; 0.1 ml | No | Intrasulcular; syringe + blunt cannula; one time, directly after SRP; refrain from chewing hard or sticky foods, brushing near the treated areas or using any interdental aids for 1 week | SRP performed until the root surface was considered smooth and clean by the operator | |
| Pranam et al., 2020 [48] | Perio Q10, Perio Inc, United States | Yes | Intrasulcular, drying (paper points), 2 mL syringe with intrasulcular applicator tip, withdrawn extruding till the superior portion of the pocket, one time, directly after SRP; avoidance of dental floss or interdental aids or mouth rinses | SRP at baseline; oral hygiene instructions: modified bass brushing technique, no dental floss or interdental aids, no use of mouth rinses (exclusion criteria) | |
| Raut et al., 2019 [44] | Perio Q gel, PerioQ Inc., Manchester, USA; gel; 1:9 | No | Intrasulcular, special needles, periodontal pack for 7 days; one time, directly after SRP | SRP at baseline | |
| Raut et al., 2016 [49] | Perio Q® gel, PerioQ Inc., Manchester, USA; gel; 1:9 | Yes (methyl-cellulose gel) | Intrasulcular, special needles, periodontal pack for 7 days; one time, directly after SRP; | SRP at baseline | |
| Sale et al., 2014 [50] | Perio QTM gel; gel; 1:9 | No | Intrasulcular: special needles; topical: tip of the applicator completely soaked in gel; every alternate day for one week; restriction for eating, spitting, and drinking for 1 h after application | SRP at baseline | |
| Salih et al., 2016 [51] | Perio Q gel; gel; 1:9; total 1 mL, each pocket 0.1–0.3 ml | No | Intrasulcular, isolation (cotton rolls), drying (air, paper points), syringe + blunted needle, removing gel excessing from pocket; one time one hour after SRP if bleeding the next day; instruction to avoid spitting, washing, eating, and drinking for 2 h after application, pause of toothbrush and interdental aids the day after the gel application | Supragingival scaling; motivation and instruction in initial visit | |
| Shaheen et al., 2020 [52] | NMQ10 (self-produced; thermo-reversible carrier system); gel; 5%; 0.1 mL per study side | No | Intrasulcular; syringe + atraumatic needle; each alternate day for one week; restriction for rinsing, drinking for 1 h after application | Full-mouth SRP; oral hygiene instructions | |
| Sharma et al., 2016 [53] | Perio Q10 gel, PerioQ Inc., Manchester, USA; gel; 1:9 | No | Intrasulcular, wide-gauge needle, gel slightly overflowing, periodontal pack; three times: after SRP, 1 week–2 weeks; | - | |
| Systemic | Darweesh et al., 2015 [36] | CoQ10, BioMérieux, France; capsules; 30 mg | No | Systemic; twice a day, 3 months | SRP using hand and ultrasonic instruments (Hu-Friedy EMS Piezon®, Chicago, IL, US), hand instruments |
| Mani et al., 2013 [39] | Oxyfresh CoQ10 Complex; dietary supplement | No | Systemic; three times a day, 4 months | SRP using EMS ultrasonic scaler; tooth brushing: twice daily 5 min with modified bass method technique (technique demonstrated to each subject) with the provided similar medium-bristle toothbrushes, toothpaste: Oxyfresh Power Paste (with chlorine dioxide)/Pepsodent (conventional), mouth rinse: twice daily (5 mL in quantity for 1 min), Oxyfresh Power Rinse (with chlorine dioxide)/Listerine (conventional) | |
| Pandav et al., 2021 [35] | Recharje Forte, Troikaa Pharmaceuticals Ltd. Uttarakhand, India; capsules; 30 mg | No | Systemic; twice a day, 6 weeks | No use of mouth rinse was permitted | |
| Saini et al., 2014 [37] | Nutritional supplement of CoQ10, Oxyfresh® Company; nutritional supplement | No | Systemic; three times a day, 4 months | SRP at baseline, using Electro Medical Systems ultrasonic scaler; tooth brushing: twice daily for 5 min with modified bass method technique (technique demonstrated to each subject) with the provided similar medium-bristle toothbrushes, conventional toothpaste, conventional mouth wash | |
| Shoukheba et al., 2019 [45] | CoQ10, MEPACO-MEDIFOOD, Enshas El Raml-Sharke-ia-Eygpt; capsules; 30 mg | Yes (oral placebo capsule) | Systemic; twice a day, 3 months | Full-mouth SRP in two sessions at an interval of 1 week, polishing, no SRP at recall visits; twice daily brushing technique with interproximal plaque control, no mouthwash |
3.2.3. Outcomes (Table 3)
| Type of CoQ10 Administration (Local/ Systemic) | Study | Groups | Primary Outcomes | Secondary Outcomes | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PPD | BOP | CAL | Gingival Index | Plaque Index | |||||||
| Baseline (mm) | ∆ PPD (mm) * | Intergroup Significance* | Baseline (mm) | ∆ CAL (mm)* | Intergroup Significance * | Intergroup Significance * | Intergroup Significance * | ||||
| Local | Attia et al., 2016 [42] | Test | 4.22 ± 0.36 | 0.90 | NSSD p = 0.103 | N/A | 2.35 ± 0.96 | 0.65 | NSSD p = 0.312 | NSSD p = 0.601 | NSSD p = 0.635 |
| Control | 4.27 ± 0.44 | 0.72 | 2.33 ± 0.47 | 0.50 | |||||||
| Barakat et al., 2019 [47] | Test | 3.76 ± 0.49 | 0.59 | SSD f.t. p < 0.001 | N/A | 2.76 ± 0.47 | 0.46 | SSD f.t. p = 0.006 | SSD f.t. p = 0 | SSD f.t. p = 0 | |
| Control | 3.83 ± 0.55 | 0.33 | 2.83 ± 0.49 | 0.32 | |||||||
| Chaudhry et al., 2014 [43] | Test | 5.50 ± 5.52 | 2.00 | SSD f.t. p = 0.018 | N/A | 9.50 ± 1.087 | 2.08 | SSD f.t. p = 0.031 | SSD f.t. p = 0.000 | NSSD p = 0.557 | |
| Control | 5.58 ± 0.52 | 1.33 | 9.42 ± 0.900 | 1.54 | |||||||
| Hans et al., 2012 [38] | Test | 4.97 ± 0.23 | 1.14 | NSSD p = 0.90 | N/A | 2.25 ± 0.48 | 0.33 | NSSD p = 0.78 | LS: NSSD p = 0.62 GBI: SSD f.t. p < 0.05 | NSSD p = 0.22 | |
| Control | 4.75 ± 0.34 | 1.02 | 2.08 ± 0.32 | 0.38 | |||||||
| Jha et al., 2018 [46] | Test | 5.39 ± 0.31 | 2.26 | n.r. | N/A | 6.55 ± 0.26 | 2.42 | n.r. | n.r. | N/A | |
| Control | 6.39 ± 0.48 | 2.20 | 6.21 ± 0.43 | 1.81 | |||||||
| Pranam et al., 2020 [48] | Test | 5.47 ± 0.56 | 1.16 | NSSD p = 0.321 | N/A | 6.13 ± 0.61 | 1.25 | NSSD p = 0.448 | NSSD p = 0.210 | NSSD p = 0.110 | |
| Control | 5.13 ± 0.42 | 1.09 | 6.16 ± 0.62 | 1.19 | |||||||
| Raut et al., 2019 [44] | Test | 6.42 ± 0.60 | 2.83 | SSD f.t. p < 0.001 | N/A | 5.59 ± 0.63 | 2.52 | SSD f.t. p < 0.001 | SSD f.t. p = 0.0004 | NSSD p = 0.329 | |
| Control | 6.33 ± 0.66 | 1.95 | 5.46 ± 0.60 | 1.75 | |||||||
| Raut et al., 2016 [49] | Test | 5.69 ± 0.83 | 2.95 | n.r. | N/A | 5.94 ± 0.80 | 2.33 | n.r. | NSSD | NSSD | |
| Control | 5.10 ± 0.68 | 0.50 | 5.22 ± 0.64 | 0.45 | |||||||
| Sale et al., 2014 [50] | Test I | 6.33 ± 1.09 | 2.61 | NSSD p = 0.965 | N/A | N/A | N/A | N/A | LS: NSSD p = 0.518, UBI: SSD f.c. p = 0.031 | SSD f.t. p < 0.0001 | |
| Test II | 5.72 ± 0.57 | 2.00 | |||||||||
| Control | 5.00 ± 0.84 c | 1.34 | |||||||||
| Salih et al., 2016 [51] | Test | 6.20 ± 0.62 | 1.01 | SSD f.t. | N/Aa | 7.20 ± 0.62 | 1.45 | SSD f.t. | n.r. | n.r. | |
| Control | 6.40 ± 0.66 | 0.65 | 7.50 ± 0.66 | 0.75 | |||||||
| Shaheen et al., 2020 [52] | Test | 2.66 ± 0.42 | 1.09 | SSD f.t. p < 0.05 | N/Ab | 2.47 ± 0.36 | 1.04 | SSD f.t. p < 0.005 | LS: SSD f.t. p < 0.005, PBI: SSD f.t. p < 0.005 | SSD f.t. p < 0.05 | |
| Control | 2.51 ± 0.42 | 0.66 | 2.38 ± 2.04 | 0.55 | |||||||
| Sharma et al., 2016 [53] | Test | 5.53 ± 0.59 | 2.33 | NSSD | N/A | 4.53 ± 1.26 | 1.66 | NSSD | EIBI: NSSD, GCCI: NSSD | NSSD | |
| Control | 5.60 ± 0.87 | 2.23 | 4.50 ± 1.01 | 1.75 | |||||||
| Systemic | Darweesh et al., 2015 [36] | Test | 4.57 ± 0.44 | 1.17 | NSSD | N/A | 4.79 ± 0.52 | 1.40 | NSSD | GI: SSD f.t. p = 0.0001, BI: SSD f.t. p = 0.0003 | SSD f.t. p = 0.0001 |
| Control | 4.78 ± 0.41 | 1.17 | 4.90 ± 0.50 | 1.25 | |||||||
| Mani et al., 2013 [39] | Test I | n.r. | n.r. | n.r. | N/A | 4.08 ± 1.19 | 1.20 | n.r. | n.r. | n.r. | |
| Control I | n.r. | n.r. | 4.37 ± 1.17 | 0.41 | |||||||
| Test II | n.r. | n.r. | n.r. | 5.64 ± 0.72 | 1.12 | n.r. | n.r. | n.r. | |||
| Control II | n.r. | n.r. | 5.64 ± 0.60 | 0.24 | |||||||
| Pandav et al., 2021 [35] | Test | 3.6 ± 0.68 | 1.35 | SSD f.t. p = 0.018 | N/A | 6.70 ± 0.96 | 1.22 | NSSD p = 0.153 | NSSD p = 0.489 | N/A | |
| Control | 3.5 ± 0.36 | 1.05 | 6.72 ± 0.92 | 0.87 | |||||||
| Saini et al., 2014 [37] | Test | 5.28 ± 1.16 | 0.20 | SSD f.c. p < 0.01 | N/A | 5.64 ± 0.72 | 1.12 | SSD f.t. p < 0.01 | SSD f.c. p < 0.01 | SSD f.c. p < 0.01 | |
| Control | 6.74 ± 0.79 | 0.66 | 5.64 ± 0.60 | 0.24 | |||||||
| Shoukheba et al., 2019 [45] | Test | 5.66 ± 0.72 | 1.20 | SSD f.t. p = 0.008 | N/A | 4.33 ± 0.48 | 0.40 | SSD f.t. p = 0.002 | LS: SSD f.t. p = 0, MS: SSD f.t. p = 0 | N/A | |
| Control | 5.46 ± 0.74 | 0.40 | 4.53 ± 0.51 | −0.13 | |||||||
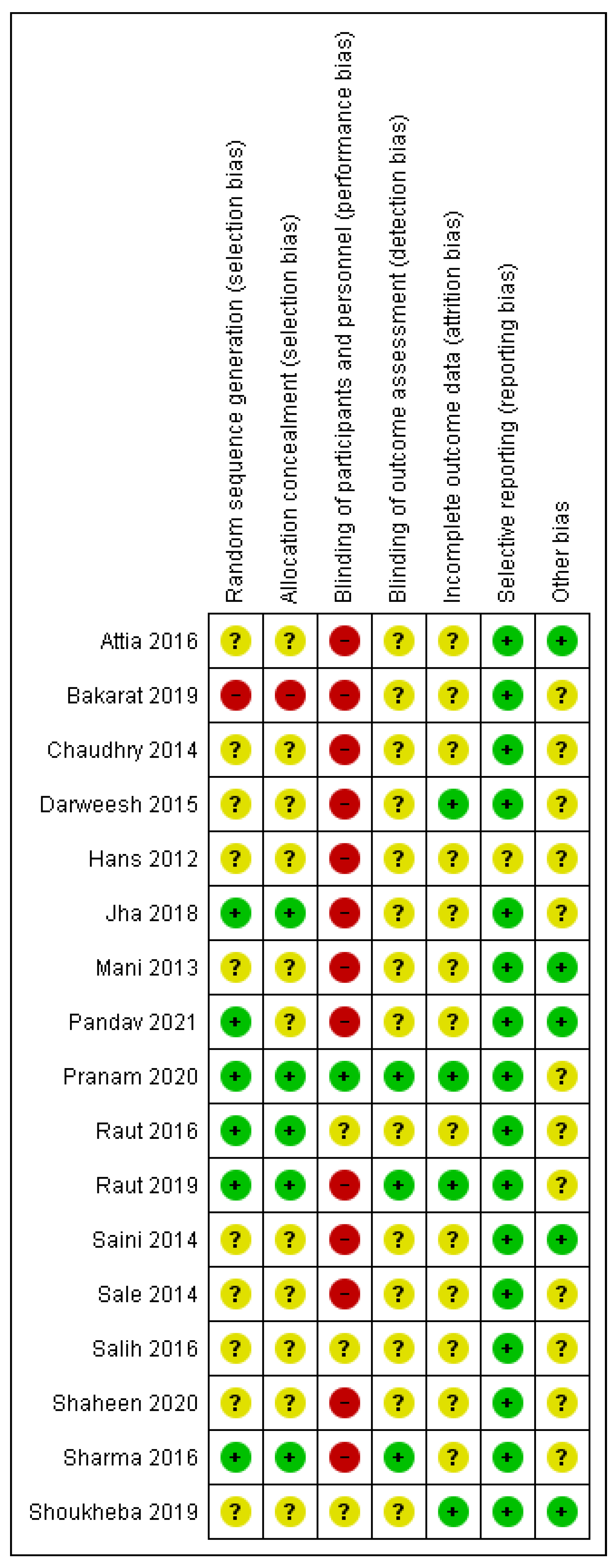
3.3. Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flemmig, T.F. Periodontitis. Ann. Periodontol. 1999, 4, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Page, R.C.; Kornman, K.S. The pathogenesis of human periodontitis: An introduction. Periodontol. 2000 1997, 14, 9–11. [Google Scholar] [CrossRef] [PubMed]
- van Dyke, T.E. Pro-resolving mediators in the regulation of periodontal disease. Mol. Aspects Med. 2017, 58, 21–36. [Google Scholar] [CrossRef]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef]
- Petersilka, G.J.; Ehmke, B.; Flemmig, T.F. Antimicrobial effects of mechanical debridement. Periodontol. 2000 2002, 28, 56–71. [Google Scholar] [CrossRef]
- van der Weijden, G.A.; Timmerman, M.F. A systematic review on the clinical efficacy of subgingival debridement in the treatment of chronic periodontitis. J. Clin. Periodontol. 2002, 29 (Suppl. S3), 55–71. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.; Abusleme, L.; Bravo, D.; Dutzan, N.; Garcia-Sesnich, J.; Vernal, R.; Hernández, M.; Gamonal, J. Host response mechanisms in periodontal diseases. J. Appl. Oral Sci. 2015, 23, 329–355. [Google Scholar] [CrossRef] [PubMed]
- Papantonopoulos, G.; Delatola, C.; Takahashi, K.; Laine, M.L.; Loos, B.G. Hidden noise in immunologic parameters might explain rapid progression in early-onset periodontitis. PLoS ONE 2019, 14, e0224615. [Google Scholar] [CrossRef]
- Matesanz-Pérez, P.; García-Gargallo, M.; Figuero, E.; Bascones-Martínez, A.; Sanz, M.; Herrera, D. A systematic review on the effects of local antimicrobials as adjuncts to subgingival debridement, compared with subgingival debridement alone, in the treatment of chronic periodontitis. J. Clin. Periodontol. 2013, 40, 227–241. [Google Scholar] [CrossRef] [PubMed]
- Sgolastra, F.; Petrucci, A.; Ciarrocchi, I.; Masci, C.; Spadaro, A. Adjunctive systemic antimicrobials in the treatment of chronic periodontitis: A systematic review and network meta-analysis. J. Periodontal Res. 2021, 56, 236–248. [Google Scholar] [CrossRef]
- Zandbergen, D.; Slot, D.E.; Niederman, R.; der Weijden, A.V. The concomitant administration of systemic amoxicillin and metronidazole compared to scaling and root planing alone in treating periodontitis: =A systematic review=. BMC Oral Health 2016, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Matesanz, P.; Martín, C.; Oud, V.; Feres, M.; Teughels, W. Adjunctive effect of locally delivered antimicrobials in periodontitis therapy: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 239–256. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Hu, J.; Zhao, L. Adjunctive subgingival application of Chlorhexidine gel in nonsurgical periodontal treatment for chronic periodontitis: A systematic review and meta-analysis. BMC Oral Health 2020, 20, 34. [Google Scholar] [CrossRef]
- Rosa, C.D.D.R.D.; de Luna Gomes, J.M.; Moraes, S.L.D.d.; Lemos, C.A.A.; da Fonte, T.P.; Limirio, J.P.J.d.O.; Pellizzer, E.P. Use of chlorhexidine chip after scaling and root planning on periodontal disease: A systematic review and meta-analysis. Saudi Dent. J. 2021, 33, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Teughels, W.; Feres, M.; Oud, V.; Martín, C.; Matesanz, P.; Herrera, D. Adjunctive effect of systemic antimicrobials in periodontitis therapy: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 257–281. [Google Scholar] [CrossRef]
- Gruner, D.; Paris, S.; Schwendicke, F. Probiotics for managing caries and periodontitis: Systematic review and meta-analysis. J. Dent. 2016, 48, 16–25. [Google Scholar] [CrossRef]
- Hu, D.; Zhong, T.; Dai, Q. Clinical efficacy of probiotics as an adjunctive therapy to scaling and root planning in the management of periodontitis: A Systematic Review and Meta-Analysis of randomized controlled trails. J. Evid. Based Dent. Pract. 2021, 21, 101547. [Google Scholar] [CrossRef] [PubMed]
- Rasoolzadeh, E.A.; Shidfar, F.; Rasoolzadeh, R.A.; Hezaveh, Z.S. The Effect of Coenzyme Q10 on periodontitis: A Systematic Review and Meta-analysis of Clinical Trials: In-press. J. Evid. Based Dent. Pract. 2022, 22, 101710. [Google Scholar] [CrossRef]
- Garrido-Maraver, J.; Cordero, M.D.; Oropesa-Ávila, M.; Fernández Vega, A.; La Mata, M.d.; Delgado Pavón, A.; de Miguel, M.; Pérez Calero, C.; Villanueva Paz, M.; Cotán, D.; et al. Coenzyme q10 therapy. Mol. Syndromol. 2014, 5, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Soni, S.; Agrawal, P.; Sharma, N.; Chander, S. Coenzyme Q10 and periodontal health: A review. J. Oral Maxillofac. Pathol. 2012, 3, 21–26. [Google Scholar]
- Prakash, S.; Sunitha, J.; Hans, M. Role of coenzyme Q(10) as an antioxidant and bioenergizer in periodontal diseases. Indian J. Pharmacol. 2010, 42, 334–337. [Google Scholar] [CrossRef]
- Schmelzer, C.; Lindner, I.; Vock, C.; Fujii, K.; Döring, F. Functional connections and pathways of coenzyme Q10-inducible genes: An in-silico study. IUBMB Life 2007, 59, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Schmelzer, C.; Lorenz, G.; Rimbach, G.; Döring, F. In Vitro Effects of the Reduced Form of Coenzyme Q10 on Secretion Levels of TNF-alpha and Chemokines in Response to LPS in the Human Monocytic Cell Line THP-1. J. Clin. Biochem. Nutr. 2009, 44, 62–66. [Google Scholar] [CrossRef]
- Littarru, G.P.; Nakamura, R.; Ho, L.; Folkers, K.; Kuzell, W.C. Deficiency of coenzyme Q 10 in gingival tissue from patients with periodontal disease. Proc. Natl. Acad. Sci. USA 1971, 68, 2332–2335. [Google Scholar] [CrossRef] [PubMed]
- Hansen, I.L.; Iwamoto, Y.; Kishi, T.; Folkers, K.; Thompson, L.E. Bioenergetics in clinical medicine. IX. Gingival and leucocytic deficiencies of coenzyme Q10 in patients with periodontal disease. Res. Commun. Chem. Pathol. Pharmacol. 1976, 14, 729–738. [Google Scholar] [PubMed]
- Nakamura, R.; Littarru, G.P.; Folkers, K.; Wilkinson, E.G. Study of CoQ10-enzymes in gingiva from patients with periodontal disease and evidence for a deficiency of coenzyme Q10. Proc. Natl. Acad. Sci. USA 1974, 71, 1456–1460. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, E.G.; Arnold, R.M.; Folkers, K.; Hansen, I.; Kishi, H. Bioenergetics in clinical medicine. II. Adjunctive treatment with coenzyme Q in periodontal therapy. Res. Commun. Chem. Pathol. Pharmacol. 1975, 12, 111–123. [Google Scholar] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2. Available online: https://training.cochrane.org/handbook. (accessed on 5 April 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Centre for Reviews and Dissemination University of York. PROSPERO: International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/ (accessed on 20 February 2021).
- Armitage, G.C. Periodontal diagnoses and classification of periodontal diseases. Periodontol. 2000 2004, 34, 9–21. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S173–S182. [Google Scholar] [CrossRef] [PubMed]
- Ramfjord, S.P. The Periodontal Disease Index (PDI). J. Periodontol. 1967, 38, 602–610. [Google Scholar] [CrossRef]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- Pandav, G.; Oandav, S.; Jain, S.; Saxena, D.; Aggarwal, R.; Gulati, P. Evaluation of the Efficacy of Coenzyme Q10 in the Management of Chronic Periodontitis: A Clinical Study. Eur. J. Dent. 2021, 9, 138–146. [Google Scholar]
- Darweesh, M. Doxycycline and Coenzyme Q10 Treatment Modalities for Chronic Periodontitis: A Preliminary Study. Int. J. Oral Dent. Health 2015, 1, 014. [Google Scholar] [CrossRef]
- Saini, R. A clinical and microbiological study to evaluate the effect of dietary supplement of coenzyme Q10 in nonsurgical treatment outcome of chronic periodontitis patients after phase 1 periodontal therapy. Eur. J. Gen. Dent. 2014, 3, 194. [Google Scholar] [CrossRef]
- Hans, M.; Prakash, S.; Gupta, S. Clinical evaluation of topical application of perio-Q gel (Coenzyme Q10) in chronic periodontitis patients. J. Indian Soc. Periodontol. 2012, 16, 193–199. [Google Scholar] [CrossRef]
- Mani, S.; Mani, A.; Saini, R. Clinical and Microbiological Evaluation of Chlorine Dioxide Based Mouthwash and Toothpaste in Periodontitis Patients along with Combination of Nutritional Dietary Supplement of CoQ10. Int. J. Exp. Dent. Sci. 2013, 2, 98–103. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Training. Review Manager (RevMan); Cochrane Training: Cochrane, Singapore, 2022. [Google Scholar]
- Attia, A.M.; Edrees, M.F.; Alghriany, A. Clinical and immunological evaluation of Coenzyme Q10 as an adjunct to nonsurgical periodontal therapy in chronic periodontitis patients. J. Periodontal Med. Clin. Prac. 2016, 3, 128–140. [Google Scholar]
- Chaudhry, S.; Vaish, S.; Dodwad, V.; Arora, A. Natural antioxidant: Coenzyme Q10 (PERIO Q)TM in management of chronic periodontitis: A clinical study. Int. J. Dent. Health Sci. 2014, 1, 475–484. [Google Scholar]
- Raut, C.P.; Sethi, K.S.; Kohale, B.; Mamajiwala, A.; Warang, A. Subgingivally delivered coenzyme Q10 in the treatment of chronic periodontitis among smokers: A randomized, controlled clinical study. J. Oral Biol. Craniofac. Res. 2019, 9, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Shoukheba, M.; El-Kholy, S. Coenzyme Q10 Food Supplement on the Treatment of Chronic Periodontitis in Patients with Type II Diabetes Mellitus: A Randomized Control Study. Egypt. Dent. J. 2019, 65, 253–261. [Google Scholar] [CrossRef]
- Jha, P.; Shukla, P.; Shukla, P.; Malhotra, G.; Dahiya, V. Comparative Evaluation of Locally Delivered Lycopene Gel and Coenzyme Q10 Gel as an Adjunct in the Treatment of Chronic Periodontitis: A Clinico-Biochemical Study. Int. J. Prev. Clin. Dent. Res. 2018, 5, 80–87. [Google Scholar]
- Barakat, A. Clinical Evaluation of Co-enzyme Q10 in Management of Chronic Periodontitis Patients: Mouth Split Study. Int. J. Health Sci. Res. 2019, 9, 69–75. [Google Scholar]
- Pranam, S.; Palwankar, P.; Pandey, R.; Goyal, A. Evaluation of Efficacy of Coenzyme Q10 as an Adjunct to Nonsurgical Periodontal Therapy and Its Effect on Crevicular Superoxide Dismutase in Patients with Chronic Periodontitis. Eur. J. Dent. 2020, 14, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Raut, C.P.; Sethi, K.S. Comparative evaluation of co-enzyme Q10 and Melaleuca alternifolia as antioxidant gels in treatment of chronic periodontitis: A clinical study. Contemp. Clin. Dent. 2016, 7, 377–381. [Google Scholar] [CrossRef]
- Sale, S.T.; Parvez, H.; Yeltiwar, R.K.R.; Vivekanandan, G.; Pundir, A.J.; Jain, P. A comparative evaluation of topical and intrasulcular application of coenzyme Q10 (Perio Q™) gel in chronic periodontitis patients: A clinical study. J. Indian Soc. Periodontol. 2014, 18, 461–465. [Google Scholar] [CrossRef]
- Salih, T.M. An Evaluation of the Effectiveness of Coenzyme Q10 Gel in Management of Patients with Chronic Periodontitis (II Inter Group Comparison). JBCD 2016, 28, 127–132. [Google Scholar] [CrossRef]
- Shaheen, M.A.; Elmeadawy, S.H.; Bazeed, F.B.; Anees, M.M.; Saleh, N.M. Innovative coenzyme Q10-loaded nanoformulation as an adjunct approach for the management of moderate periodontitis: Preparation, evaluation, and clinical study. Drug Deliv. Transl. Res. 2020, 10, 548–564. [Google Scholar] [CrossRef]
- Sharma, V.; Gupta, R.; Dahiya, P.; Kumar, M. Comparative evaluation of coenzyme Q(10)-based gel and 0.8% hyaluronic acid gel in treatment of chronic periodontitis. J. Indian Soc. Periodontol. 2016, 20, 374–380. [Google Scholar] [CrossRef]
- Loe, H.; Silness, J. Periodontal Disease in Pregnancy I. Prevalence and Severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Silness, J.; Loe, H. Periodontal Disease in Pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Abrams, K.; Caton, J.; Polson, A. Histologic comparisons of interproximal gingival tissues related to the presence or absence of bleeding. J. Periodontol. 1984, 55, 629–632. [Google Scholar] [CrossRef]
- Gupta, R.; Pandit, N.; Makkar, A. Role of professionally applied 0.8% hyaluronic acid gel in managing inflammation in periodontal disease. Baba Farid Univ. Dent. J. 2011, 2, 117–120. [Google Scholar]
- Mühlemann, H.R.; Son, S. Gingival sulcus bleeding—a leading symptom in initial gingivitis. Helv. Odontol. Acta 1971, 15, 107–113. [Google Scholar] [PubMed]
- Mombelli, A.; van Oosten, M.A.; Schurch, E.; Land, N.P. The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Saxer, U.P.; Mühlemann, H.R. Motivation und Aufklärung. SSO. Schweiz. Mon. Zahnheilkd 1975, 85, 905–919. [Google Scholar]
- Turesky, S.; Gilmore, N.D.; Glickman, I. Reduced plaque formation by the chloromethyl analogue of vitamine C. J. Periodontol. 1970, 41, 41–43. [Google Scholar] [CrossRef]
- Alimohammadi, M.; Rahimi, A.; Faramarzi, F.; Golpour, M.; Jafari-Shakib, R.; Alizadeh-Navaei, R.; Rafiei, A. Effects of coenzyme Q10 supplementation on inflammation, angiogenesis, and oxidative stress in breast cancer patients: A systematic review and meta-analysis of randomized controlled- trials. Inflammopharmacology 2021, 29, 579–593. [Google Scholar] [CrossRef]
- Jorat, M.V.; Tabrizi, R.; Kolahdooz, F.; Akbari, M.; Salami, M.; Heydari, S.T.; Asemi, Z. The effects of coenzyme Q10 supplementation on biomarkers of inflammation and oxidative stress in among coronary artery disease: A systematic review and meta-analysis of randomized controlled trials. Inflammopharmacology 2019, 27, 233–248. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Mealey, B.L.; van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S74–S84. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Castro Dos Santos, N.C.; Furukawa, M.V.; Oliveira-Cardoso, I.; Cortelli, J.R.; Feres, M.; van Dyke, T.; Rovai, E.S. Does the use of omega-3 fatty acids as an adjunct to non-surgical periodontal therapy provide additional benefits in the treatment of periodontitis? A systematic review and meta-analysis. J. Periodontal Res. 2022, 57, 435–447. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- Qiu, F.; Liang, C.-L.; Liu, H.; Zeng, Y.-Q.; Hou, S.; Huang, S.; Lai, X.; Dai, Z. Impacts of cigarette smoking on immune responsiveness: Up and down or upside down? Oncotarget 2017, 8, 268–284. [Google Scholar] [CrossRef] [PubMed]
- Shiels, M.S.; Katki, H.A.; Freedman, N.D.; Purdue, M.P.; Wentzensen, N.; Trabert, B.; Kitahara, C.M.; Furr, M.; Li, Y.; Kemp, T.J.; et al. Cigarette smoking and variations in systemic immune and inflammation markers. J. Natl. Cancer Inst. 2014, 106, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Daryabor, G.; Atashzar, M.R.; Kabelitz, D.; Meri, S.; Kalantar, K. The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System. Front. Immunol. 2020, 11, 1582. [Google Scholar] [CrossRef]
- Anwaristi, A.Y. Effect of coenzyme-q10 in the post-curettage against probing depth, relative attachment loss, and bleeding on probing. J. Syiah Kuala Dent. Soc. 2022, 5, 66–69. [Google Scholar] [CrossRef]
- Bhalla, A.; Jithendra, K.D.; Shailendra, S. Co-Enzyme Q10:-Another Armour For Novel Periodontal Therapy. 2019. Available online: https://web.s.ebscohost.com/abstract?direct=true&profile=ehost&scope=site&authtype=crawler&jrnl=09762248&AN=136410177&h=f4JoktM3lV6%2bOuVxrvdSxQFt4WhBLdCcL8PZu35rF3ZPWCKiIsMicGQW4iHybQSqx5IaE2p5X1Nh%2fcmTLAsZvA%3d%3d&crl=c&resultNs=AdminWebAuth&resultLocal=ErrCrlNotAuth&crlhashurl=login.aspx%3fdirect%3dtrue%26profile%3dehost%26scope%3dsite%26authtype%3dcrawler%26jrnl%3d09762248%26AN%3d136410177 (accessed on 20 February 2021).
- Chug, A.; Shukla, S. Placement of Sticky Bone™ in patients with generalized periodontitis previously treated with coenzyme Q10. J. Contemp. Dent. Pract. 2020, 21, 156–160. [Google Scholar] [CrossRef]
- Folkers, K.; Watanabe, T. Bioenergetics in clinical medicine-X. Survey of the adjunctive use of coenzyme Q with oral therapy in treating periodontal disease. J. Med. 1977, 8, 333–348. [Google Scholar]
- Hanioka, T.; Tanaka, M.; Ojima, M.; Shizukuishi, S.; Folkers, K. Effect of topical application of Coenzyme Q10 on adult periodontitis. Mol. Asp. Med. 1994, 15, s241–s248. [Google Scholar] [CrossRef] [PubMed]
- Lister, R.E. Coenzyme Q10 and periodontal disease. Br. Dent. J. 1995, 179, 200. [Google Scholar] [CrossRef]
- Manthena, S.; Rao, M.V.R.; Penubolu, L.P.; Putcha, M.; Harsha, A.V.N.S. Effectiveness of CoQ10 Oral Supplements as an Adjunct to Scaling and Root Planing in Improving Periodontal Health. J. Clin. Diagn. Res. JCDR 2015, 9, ZC26-8. [Google Scholar] [CrossRef] [PubMed]
- Matthews-Brzozowska, T.; Kurhañska-Flisykowska, A.; Wyganowska-Swiatkowska, M.; Stopa, J. Healing of periodontal tissue assisted by coenzyme Q10 with vitamin E—Clinical and laboratory evaluation. Pharm. Rep. 2007, 59 (Suppl. S1), 257–260. [Google Scholar]
- Matsumura, T.; Saji, S.; Nakamura, R.; Folkers, K. Evidence for enhanced treatment of periodontal disease by therapy with coenzyme Q. Int. J. Vitam. Nutr. Res. 1973, 43, 537–548. [Google Scholar] [PubMed]
- Nakamura, R.; Littaru, G.; Folkers, K.; Wilkinson, E.G. Deficiency of Coenzyme Q in Gingiva of Patients with Periodontal Disease. J. Int. Vitaminol. Nutr. 1973, 43, 84–92. [Google Scholar]
- Pitale, U.; Khetarpal, S.; Peter, K.; Pal, V.; Verma, E.; Gupta, P. Evaluation of efficacy of coenzyme Q 10 in management of gingivitis & slight periodontitis - a clinical study. Int. J. Curr. Pharm. Res. 2012, 4, 33–38. [Google Scholar]
- Rasperini, G.; Pellegrini, G.; Sugai, J.; Mauro, C.; Fiocchi, S.; Mora, P.C.; Dellavia, C. Effects of food supplements on periodontal status and local and systemic inflammation after nonoperative periodontal treatment. J. Oral Sci. 2019, 61, 213–220. [Google Scholar] [CrossRef]
- Roopa, D.A.; Gupta, R.; Gupta, I.; Chauhan, S.; Pandey, A.; Sharma, N.K. Clinical evaluation of topical application of CNBC gel (Coenzyme Q10) in chronic periodontitis patients. J. Dent. Res. Updates 2014, 1, 13–17. [Google Scholar]
- Saini, R. Coenzyme Q10: The essential nutrient. J. Pharm. Bioallied Sci. 2011, 3, 466–467. [Google Scholar] [CrossRef]
- Wilkinson, E.G.; Arnold, R.M.; Folkers, K. Bioenergetics in clinical medicine. VI. Adjunctive treatment of periodontal disease with coenzyme Q10. Res. Commun. Chem. Pathol. Pharmacol. 1976, 14, 715–719. [Google Scholar] [PubMed]
- Zaki, N.M. Site-specific delivery of the Nutraceutical COQ10 for periodontal therapy. Int. J. Pharm. Pharm. Sci. 2012, 4, 717–723. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merle, C.L.; Lenzen, C.; Schmalz, G.; Ziebolz, D. Systematic Review on Protocols of Coenzyme Q10 Supplementation in Non-Surgical Periodontitis Therapy. Nutrients 2023, 15, 1585. https://doi.org/10.3390/nu15071585
Merle CL, Lenzen C, Schmalz G, Ziebolz D. Systematic Review on Protocols of Coenzyme Q10 Supplementation in Non-Surgical Periodontitis Therapy. Nutrients. 2023; 15(7):1585. https://doi.org/10.3390/nu15071585
Chicago/Turabian StyleMerle, Cordula Leonie, Carina Lenzen, Gerhard Schmalz, and Dirk Ziebolz. 2023. "Systematic Review on Protocols of Coenzyme Q10 Supplementation in Non-Surgical Periodontitis Therapy" Nutrients 15, no. 7: 1585. https://doi.org/10.3390/nu15071585
APA StyleMerle, C. L., Lenzen, C., Schmalz, G., & Ziebolz, D. (2023). Systematic Review on Protocols of Coenzyme Q10 Supplementation in Non-Surgical Periodontitis Therapy. Nutrients, 15(7), 1585. https://doi.org/10.3390/nu15071585