
Food, Dietary Patterns, or Is Eating Behavior to Blame? Analyzing the Nutritional Aspects of Functional Dyspepsia

 ,
,  ,
,  and
and 
Abstract
1. Introduction
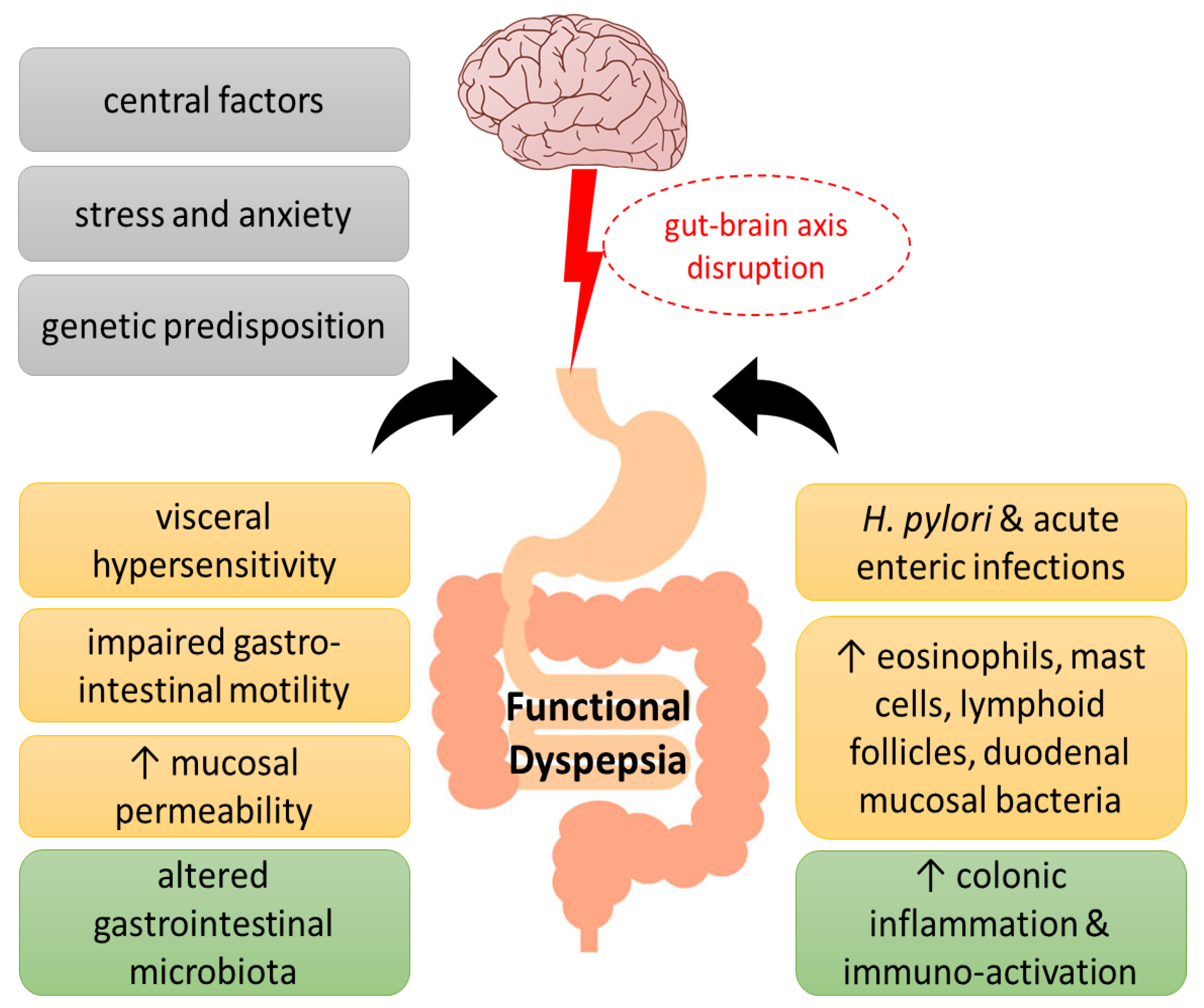
1.1. Pathophysiology
1.2. Clinical Manifestations
1.3. Medicines
1.4. Herbal Remedies
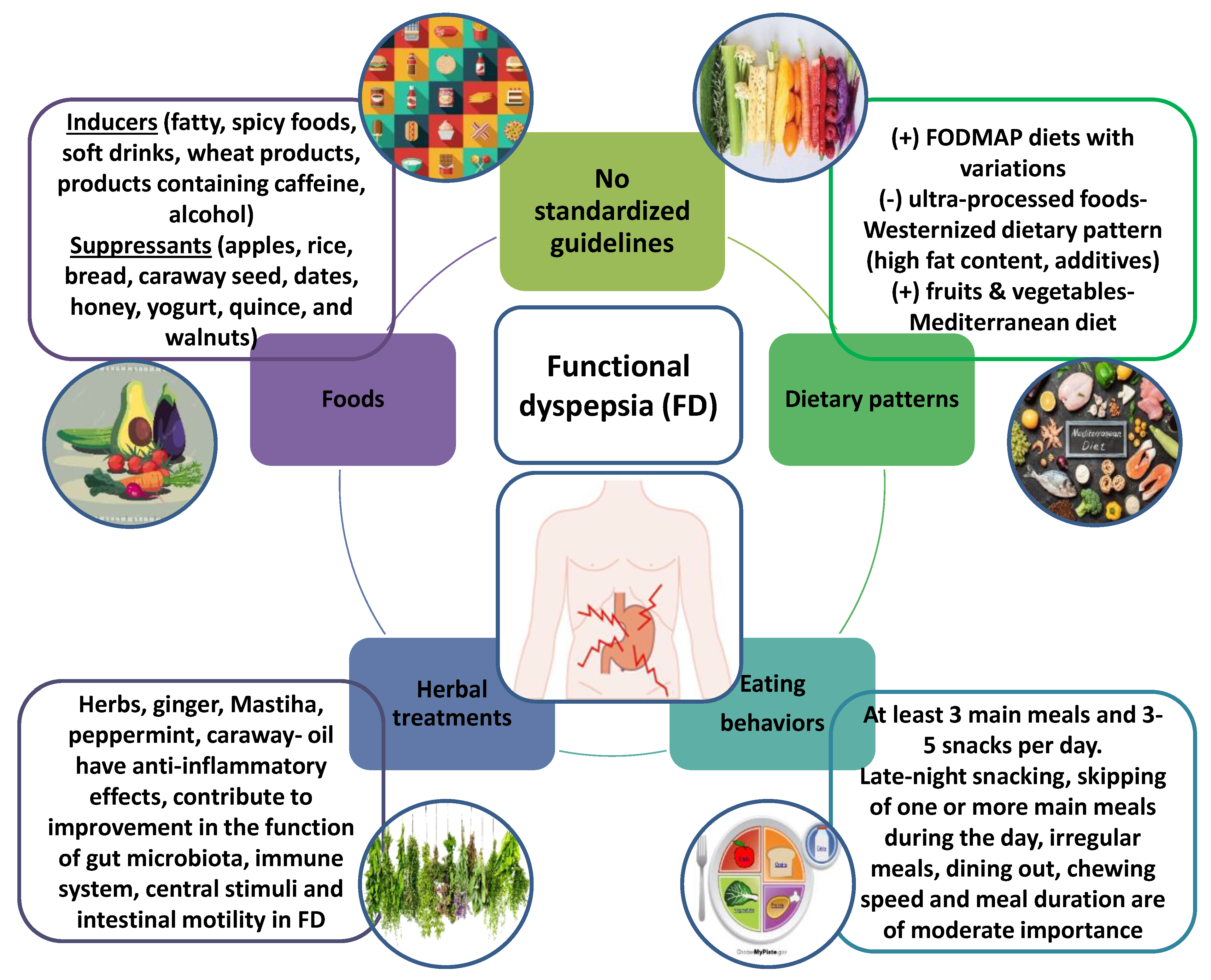
2. Certain Foods as Inducers or Suppressants of Functional Dyspepsia Symptoms
3. Dietary Patterns and Eating Behaviors; Proportions, Variety, Frequency, and Cooking Habits
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wauters, L.; Dickman, R.; Drug, V.; Mulak, A.; Serra, J.; Enck, P.; Tack, J.; Accarino, A.; Barbara, G.; Bor, S.; et al. United European Gastroenterology (UEG) and European Society for Neurogastroenterology and Motility (ESNM) consensus on functional dyspepsia. United Eur. Gastroenterol. J. 2021, 9, 307–331. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Meroni, G.; Pistone, D.; Pasquale, L.; Milazzo, G.; Monica, F.; Aragona, S.; Ficano, L.; Vassallo, R. Evaluation of main functional dyspepsia symptoms after probiotic administration in patients receiving conventional pharmacological therapies. J. Int. Med. Res. 2021, 49, 0300060520982657. [Google Scholar] [CrossRef]
- Wauters, L.; Talley, N.J.; Walker, M.M.; Tack, J.; Vanuytsel, T. Novel concepts in the pathophysiology and treatment of functional dyspepsia. Gut 2019, 69, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Holtmann, G.; Shah, A.; Morrison, M. Pathophysiology of Functional Gastrointestinal Disorders: A Holistic Overview. Dig. Dis. 2017, 35 (Suppl. S1), 5–13. [Google Scholar] [CrossRef]
- Wauters, L.; Li, H.; Talley, N.J. Editorial: Disruption of the Microbiota-Gut-Brain Axis in Functional Dyspepsia and Gastroparesis: Mechanisms and Clinical Implications. Front. Neurosci. 2022, 16, 941810. [Google Scholar] [CrossRef] [PubMed]
- Komori, K.; Ihara, E.; Minoda, Y.; Ogino, H.; Sasaki, T.; Fujiwara, M.; Oda, Y.; Ogawa, Y. The Altered Mucosal Barrier Function in the Duodenum Plays a Role in the Pathogenesis of Functional Dyspepsia. Dig. Dis. Sci. 2019, 64, 3228–3239. [Google Scholar] [CrossRef]
- Wauters, L.; Burns, G.; Ceulemans, M.; Walker, M.M.; Vanuytsel, T.; Keely, S.; Talley, N.J. Duodenal inflammation: An emerging target for functional dyspepsia? Expert Opin. Ther. Targets 2020, 24, 511–523. [Google Scholar] [CrossRef]
- Stanghellini, V.; Chan, F.K.L.; Hasler, W.L.; Malagelada, J.R.; Suzuki, H.; Tack, J.; Talley, N.J. Gastroduodenal Disorders. Gastroenterology 2016, 150, 1380–1392. [Google Scholar] [CrossRef]
- Duboc, H.; Latrache, S.; Nebunu, N.; Coffin, B. The Role of Diet in Functional Dyspepsia Management. Front. Psychiatry 2020, 11, 23. [Google Scholar] [CrossRef]
- Moayyedi, P.M.; Lacy, B.E.; Andrews, C.N.; Enns, R.A.; Howden, C.W.; Vakil, N. ACG and CAG Clinical Guideline: Management of Dyspepsia. Am. J. Gastroenterol. 2017, 112, 988–1013. [Google Scholar] [CrossRef]
- Tack, J.; Janssen, P.; Masaoka, T.; Farré, R.; Van Oudenhove, L. Efficacy of Buspirone, a Fundus-Relaxing Drug, in Patients With Functional Dyspepsia. Clin. Gastroenterol. Hepatol. 2012, 10, 1239–1245. [Google Scholar] [CrossRef]
- Pittayanon, R.; Yuan, Y.; Bollegala, N.P.; Khanna, R.; Lacy, B.E.; Andrews, C.N.; Leontiadis, G.I.; Moayyedi, P. Prokinetics for Functional Dyspepsia. Am. J. Gastroenterol. 2019, 114, 233–243. [Google Scholar] [CrossRef]
- Talley, N.J.; Locke, G.R.; Saito, Y.A.; Almazar, A.E.; Bouras, E.P.; Howden, C.W.; Lacy, B.E.; DiBaise, J.K.; Prather, C.M.; Abraham, B.P.; et al. Effect of Amitriptyline and Escitalopram on Functional Dyspepsia: A Multicenter, Randomized Controlled Study. Gastroenterology 2015, 149, 340–349.e2. [Google Scholar] [CrossRef]
- Meyrat, P.; Safroneeva, E.; Schoepfer, A.M. Rifaximin treatment for the irritable bowel syndrome with a positive lactulose hydrogen breath test improves symptoms for at least 3 months. Aliment. Pharmacol.Ther. 2012, 36, 1084–1093. [Google Scholar] [CrossRef]
- Bordbar, G.; Miri, M.B.; Omidi, M.; Shoja, S.; Akhavan, M. Comparison of a Novel Herbal Medicine and Omeprazole in the Treatment of Functional Dyspepsia: A Randomized Double-Blinded Clinical Trial. Gastroenterol. Res. Pract. 2020, 2020, 5152736. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Kim, J.-W.; Ha, N.-Y.; Kim, J.; Ryu, H.S. Herbal Therapies in Functional Gastrointestinal Disorders: A Narrative Review and Clinical Implication. Front. Psychiatry 2020, 11, 601. [Google Scholar] [CrossRef] [PubMed]
- Heiran, A.; Bagheri Lankarani, K.; Bradley, R.; Simab, A.; Pasalar, M. Efficacy of herbal treatments for functional dyspepsia: A systematic review and meta-analysis of randomized clinical trials. Phytother. Res. 2021, 36, 686–704. [Google Scholar] [CrossRef]
- Ho, L.; Zhong, C.C.W.; Wong, C.H.L.; Wu, J.C.Y.; Chan, K.K.H.; Wu, I.X.Y.; Leung, T.H.; Chung, V.C.H. Chinese herbal medicine for functional dyspepsia: A network meta-analysis of prokinetic-controlled randomised trials. Chin. Med. 2021, 16, 140. [Google Scholar] [CrossRef]
- Yoon, J.Y.; Ko, S.-J.; Park, J.-W.; Cha, J.M. Complementary and alternative medicine for functional dyspepsia: An Asian perspective. Medicine 2022, 101, e30077. [Google Scholar] [CrossRef]
- Ko, S.; Park, J.; Kim, M.; Kim, J.; Park, J. Effects of the herbal medicine Rikkunshito, for functional dyspepsia: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2021, 36, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Di Pierro, F.; Giovannone, M.; Saponara, M.; Ivaldi, L. Effectiveness of a nutraceutical supplement containing highly standardized perilla and ginger extracts in patients with functional dyspepsia. Minerva Gastroenterol. Dietol. 2020, 66, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Giacosa, A.; Guido, D.; Grassi, M.; Riva, A.; Morazzoni, P.; Bombardelli, E.; Perna, S.; Faliva, M.A.; Rondanelli, M. The Effect of Ginger (Zingiber officinalis) and Artichoke (Cynara cardunculus) Extract Supplementation on Functional Dyspepsia: A Randomised, Double-Blind, and Placebo-Controlled Clinical Trial. Evid.-Based Complement. Altern. Med. 2015, 2015, 915087. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.-L. Effect of ginger on gastric motility and symptoms of functional dyspepsia. World J. Gastroenterol. 2011, 17, 105. [Google Scholar] [CrossRef]
- Li, J.; Lv, L.; Zhang, J.; Xu, L.; Zeng, E.; Zhang, Z.; Wang, F.; Tang, X. A Combination of Peppermint Oil and Caraway Oil for the Treatment of Functional Dyspepsia: A Systematic Review and Meta-Analysis. Evid. -Based Complement. Altern. Med. 2019, 2019, 7654947. [Google Scholar] [CrossRef]
- Dabos, K.J.; Sfika, E.; Vlatta, L.J.; Frantzi, D.; Amygdalos, G.I.; Giannikopoulos, G. Is Chios mastic gum effective in the treatment of functional dyspepsia? A prospective randomised double-blind placebo controlled trial. J. Ethnopharmacol. 2010, 127, 205–209. [Google Scholar] [CrossRef]
- Akhondi-Meybodi, M.; Aghaei, M.A.; Hashemian, Z. The role of diet in the management of non-ulcer dyspepsia. Middle East J. Dig. Dis. 2015, 7, 19–24. [Google Scholar]
- Führer, M.; Vogelsang, H.; Hammer, J. A Placebo Controlled Trial of an Oral Capsaicin Load in Patients With Functional Dyspepsia. Gastroenterology 2011, 23, 918-e397. [Google Scholar] [CrossRef]
- Hammer, J.; Führer, M.; Pipal, L.; Matiasek, J. Hypersensitivity for capsaicin in patients with functional dyspepsia. Neurogastroenterol. Motil. 2008, 20, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Tahara, T.; Shibata, T.; Nakamura, M.; Yamashita, H.; Yoshioka, D.; Hirata, I.; Arisawa, T. Homozygous TRPV1 315C Influences the Susceptibility to Functional Dyspepsia. J. Clin. Gastroenterol. 2010, 44, e1–e7. [Google Scholar] [CrossRef]
- Lee, S.Y.; Masaoka, T.; Han, H.S.; Matsuzaki, J.; Hong, M.J.; Fukuhara, S.; Choi, H.S.; Suzuki, H. A prospective study on symptom generation according to spicy food intake and TRPV1 genotypes in functional dyspepsia patients. Neurogastroenterol. Motil. 2016, 28, 1401–1408. [Google Scholar] [CrossRef]
- Göktaş, Z.; Köklü, S.; Dikmen, D.; Öztürk, Ö.; Yılmaz, B.; Asıl, M.; Korkmaz, H.; Tuna, Y.; Kekilli, M.; Karamanoğlu Aksoy, E.; et al. Nutritional habits in functional dyspepsia and its subgroups: A comparative study. Scand. J. Gastroenterol. 2016, 51, 903–907. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.-p.; Wang, K.; Duan, Y.-h.; Yang, G. Correlation between lifestyle and social factors in functional dyspepsia among college freshmen. J. Int. Med. Res. 2020, 48, 1–8. [Google Scholar] [CrossRef]
- Chirila, I.; Morariu, I.D.; Barboi, O.B.; Drug, V.L. The role of diet in the overlap between gastroesophageal reflux disease and functional dyspepsia. Turk. J. Gastroenterol. 2016, 27, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Potter, M.D.E.; Walker, M.M.; Jones, M.P.; Koloski, N.A.; Keely, S.; Talley, N.J. Wheat Intolerance and Chronic Gastrointestinal Symptoms in an Australian Population-based Study: Association Between Wheat Sensitivity, Celiac Disease and Functional Gastrointestinal Disorders. Am. J. Gastroenterol. 2018, 113, 1036–1044. [Google Scholar] [CrossRef]
- Shahbazkhani, B.; Fanaeian, M.M.; Farahvash, M.J.; Aletaha, N.; Alborzi, F.; Elli, L.; Shahbazkhani, A.; Zebardast, J.; Rostami-Nejad, M. Prevalence of Non-Celiac Gluten Sensitivity in Patients with Refractory Functional Dyspepsia: A Randomized Double-blind Placebo Controlled Trial. Sci. Rep. 2020, 10, 2401. [Google Scholar] [CrossRef] [PubMed]
- Colak, H.; Gunes, F.E.; Ozen Alahdab, Y.; Karakoyun, B. Investigation of Eating Habits in Patients with Functional Dyspepsia. Turk. J. Gastroenterol. 2022, 5, 11. [Google Scholar] [CrossRef]
- Azadbakht, L.; Khodarahm, M. Dietary fat intake and functional dyspepsia. Adv. Biomed. Res. 2016, 5, 76. [Google Scholar] [CrossRef]
- Carvalho, R.V.B.; Lorena, S.L.S.; de Souza Almeida, J.R.; Mesquita, M.A. Food Intolerance, Diet Composition, and Eating Patterns in Functional Dyspepsia Patients. Dig. Dis. Sci. 2009, 55, 60–65. [Google Scholar] [CrossRef]
- Mawe, G.M.; Hoffman, J.M. Serotonin signalling in the gut—Functions, dysfunctions and therapeutic targets. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 473–486. [Google Scholar] [CrossRef]
- Lee, I.-S.; Kullmann, S.; Scheffler, K.; Preissl, H.; Enck, P. Fat label compared with fat content: Gastrointestinal symptoms and brain activity in functional dyspepsia patients and healthy controls. Am. J. Clin. Nutr. 2018, 108, 127–135. [Google Scholar] [CrossRef]
- Ianiro, G.; Pizzoferrato, M.; Franceschi, F.; Tarullo, A.; Luisi, T.; Gasbarrini, G. Effect of an extra-virgin olive oil enriched with probiotics or antioxidants on functional dyspepsia: A pilot study. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 2085–2090. [Google Scholar] [PubMed]
- Mehta, R.S.; Song, M.; Staller, K.; Chan, A.T. Association Between Beverage Intake and Incidence of Gastroesophageal Reflux Symptoms. Clin. Gastroenterol. Hepatol. 2020, 18, 2226–2233.e4. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.-Z.; Yi, P.; Wang, G.-S.; Tan, S.-Y.; Huang, G.-M.; Qi, L.-Z.; Jia, Y.; Wang, F. Lifestyle intervention for gastroesophageal reflux disease: A national multicenter survey of lifestyle factor effects on gastroesophageal reflux disease in China. Ther. Adv. Gastroenterol. 2019, 12, 1–12. [Google Scholar] [CrossRef]
- Wang, C.-C.; Wei, T.-Y.; Hsueh, P.-H.; Wen, S.-H.; Chen, C.-L. The role of tea and coffee in the development of gastroesophageal reflux disease. Tzu Chi Med. J. 2019, 31, 169. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.-H.; Lai, Y.; Zhuang, L.-P.; Huang, C.-Z.; Li, C.-Q.; Chen, Q.-K.; Yu, T. Certain Dietary Habits Contribute to the Functional Dyspepsia in South China Rural Area. Med. Sci. Monit. 2017, 23, 3942–3951. [Google Scholar] [CrossRef]
- Correia, H.; Peneiras, S.; Levchook, N.; Peneiras, E.; Levchook, T.; Nayyar, J. Effects of a non-caffeinated coffee substitute on functional dyspepsia. Clin. Nutr. ESPEN 2020, 41, 412–416. [Google Scholar] [CrossRef]
- Staudacher, H.M.; Nevin, A.N.; Duff, C.; Kendall, B.J.; Holtmann, G.J. Epigastric symptom response to low FODMAP dietary advice compared with standard dietetic advice in individuals with functional dyspepsia. Neurogastroenterol. Motil. 2021, 33, e14148. [Google Scholar] [CrossRef]
- Goyal, O.; Nohria, S.; Batta, S.; Dhaliwal, A.; Goyal, P.; Sood, A. Low FODMAP diet versus traditional dietary advice for functional dyspepsia: A randomized controlled trial. J. Gastroenterol. Hepatol. 2021, 37, 301–309. [Google Scholar] [CrossRef]
- Schnabel, L.; Kesse-Guyot, E.; Allès, B.; Touvier, M.; Srour, B.; Hercberg, S.; Buscail, C.; Julia, C. Association Between Ultraprocessed Food Consumption and Risk of Mortality Among Middle-aged Adults in France. JAMA Intern. Med. 2019, 179, 490. [Google Scholar] [CrossRef]
- Shau, J.P.; Chen, P.H.; Chan, C.F.; Hsu, Y.C.; Wu, T.C.; James, F.E.; Pan, W.H. Fast foods--are they a risk factor for functional gastrointestinal disorders? Asia Pac J Clin Nutr. 2016, 25, 393–401. [Google Scholar] [CrossRef]
- Feinle-Bisset, C.; Azpiroz, F. Dietary Lipids and Functional Gastrointestinal Disorders. Am. J. Gastroenterol. 2013, 108, 737–747. [Google Scholar] [CrossRef]
- Poti, J.M.; Mendez, M.A.; Ng, S.W.; Popkin, B.M. Is the degree of food processing and convenience linked with the nutritional quality of foods purchased by US households? Am. J. Clin. Nutr. 2015, 101, 1251–1262. [Google Scholar] [CrossRef]
- Csáki, K.F. Synthetic surfactant food additives can cause intestinal barrier dysfunction. Med. Hypotheses 2011, 76, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Tessier, F.J.; Birlouez-Aragon, I. Health effects of dietary Maillard reaction products: The results of ICARE and other studies. Amino Acids 2010, 42, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Yap, P.; Mahadeva, S.; Goh, K.-L. The Influence of Cultural Habits on the Changing Pattern of Functional Dyspepsia. Dig. Dis. 2014, 32, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Tabibian, S.; Hajhashemy, Z.; Shaabani, P.; Saneei, P.; Keshteli, A.H.; Esmaillzadeh, A.; Adibi, P. The relationship between fruit and vegetable intake with functional dyspepsia in adults. Neurogastroenterol. Motil. 2021, 33, e14129. [Google Scholar] [CrossRef]
- Zito, F.P.; Polese, B.; Vozzella, L.; Gala, A.; Genovese, D.; Verlezza, V.; Medugno, F.; Santini, A.; Barrea, L.; Cargiolli, M.; et al. Good adherence to mediterranean diet can prevent gastrointestinal symptoms: A survey from Southern Italy. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 564. [Google Scholar] [CrossRef]
- Hassanzadeh, S.; Saneei, P.; Keshteli, A.H.; Daghaghzadeh, H.; Esmaillzadeh, A.; Adibi, P. Meal frequency in relation to prevalence of functional dyspepsia among Iranian adults. Nutrition 2016, 32, 242–248. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Furukawa, S.; Watanabe, J.; Kato, A.; Kusumoto, K.; Miyake, T.; Takeshita, E.; Ikeda, Y.; Yamamoto, N.; Kohara, K.; et al. Association Between Eating Behavior, Frequency of Meals, and Functional Dyspepsia in Young Japanese Population. J. Neurogastroenterol. Motil. 2022, 28, 418–423. [Google Scholar] [CrossRef]
- Sinn, D.H.; Shin, D.H.; Lim, S.W.; Kim, K.-M.; Son, H.J.; Kim, J.J.; Rhee, J.C.; Rhee, P.-L. The Speed of Eating and Functional Dyspepsia in Young Women. Gut Liver 2010, 4, 173–178. [Google Scholar] [CrossRef][Green Version]



{kind=link}
{kind=link}
| a/a | Ref. No | Foods/Nutrients Investigated | Design | Results | FD Symptoms |
|---|---|---|---|---|---|
| 1 | [26] | Commonly consumed foods |
|
| ↑ |
| ↓ | ||||
| 2 | [27] | Capsaicin containing capsule |
|
| |
| ↑ | ||||
| |||||
| 3 | [28] | Capsaicin containing capsule |
|
| |
| ↑ | ||||
| |||||
| 4 | [29] | Capsaicin |
|
| ↑ |
| |||||
| 5 | [30] | Spicy foods |
|
| ↑ |
| 6 | [31] | Commonly consumed foods |
|
| ↑ |
| |||||
| ↑ | ||||
| 7 | [32] | Commonly consumed foods |
|
| |
| ↑ | ||||
| |||||
| 8 | [33] | Commonly consumed foods |
|
| ↑ |
| 9 | [34] | Wheat |
|
| ↑ |
| 10 | [35] | Gluten |
|
| |
| |||||
| ↔ | ||||
| |||||
| ↔ | ||||
| 11 | [36] | List of foods that may stimulate FD |
|
| ↓ |
| ↓ | ||||
| ↓ | ||||
| 12 | [38] | Commonly consumed foods |
|
| |
| ↑ | ||||
| ↑ | ||||
| ↑ | ||||
| ↑ | ||||
| ↑ | ||||
| 13 | [40] | Four different yogurts differentiated in fat composition label |
|
| |
| ↑ | ||||
| ↑ | ||||
| ↑ | ||||
| ↑ | ||||
| ↓ | ||||
| ↑ | ||||
| |||||
| |||||
| |||||
| 14 | [41] | Extra virgin olive oil enriched with antioxidants or probiotics |
|
| |
| ↓ | ||||
| ↓ | ||||
| |||||
| ↓ | ||||
| ↓ | ||||
| |||||
| 15 | [45] | Commonly consumed foods |
|
| |
| ↑ | ||||
| 16 | [46] | Non-caffeinated coffee substitute |
|
| |
| ↓ | ||||
| ↓ |
| a/a | Ref. No | Dietary Pattern/Eating Behavior | Design | Results | FD Symptoms |
|---|---|---|---|---|---|
| 1 | [47] | Low FODMAP |
|
| |
| ↓ | ||||
| ↓ | ||||
| 2 | [49] | Ultra-processed food rich diet |
|
| |
| ↑ | ||||
| 3 | [50] | Fast food diets |
|
| |
| ↑ | ||||
| ↑ | ||||
| 4 | [56] | Fruit and vegetable intake |
|
| |
| ↓ | ||||
| ↔ | ||||
| |||||
| 5 | [57] | Mediterranean diet |
|
| |
| ↑ | ||||
| 6 | [31] | Eating behavior |
|
| |
| ↔ | ||||
| ↔ | ||||
| ↑ | ||||
| 7 | [36] | Eating behavior |
|
| |
| ↔ | ||||
| ↑ | ||||
| 8 | [45] | Eating behavior |
|
| |
| ↑ | ||||
| 9 | [58] | Meal frequency |
|
| |
| ↓ | ||||
| ↓ | ||||
| 10 | [59] | Eating behavior |
|
| |
| ↑ | ||||
| ↔ | ||||
| ↓ | ||||
| 11 | [38] | Eating behavior |
|
| |
| ↑ | ||||
| ↓ | ||||
| ↔ | ||||
| 12 | [60] | Eating behavior |
|
| |
| ↑ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amerikanou, C.; Kleftaki, S.-A.; Valsamidou, E.; Chroni, E.; Biagki, T.; Sigala, D.; Koutoulogenis, K.; Anapliotis, P.; Gioxari, A.; Kaliora, A.C. Food, Dietary Patterns, or Is Eating Behavior to Blame? Analyzing the Nutritional Aspects of Functional Dyspepsia. Nutrients 2023, 15, 1544. https://doi.org/10.3390/nu15061544
Amerikanou C, Kleftaki S-A, Valsamidou E, Chroni E, Biagki T, Sigala D, Koutoulogenis K, Anapliotis P, Gioxari A, Kaliora AC. Food, Dietary Patterns, or Is Eating Behavior to Blame? Analyzing the Nutritional Aspects of Functional Dyspepsia. Nutrients. 2023; 15(6):1544. https://doi.org/10.3390/nu15061544
Chicago/Turabian StyleAmerikanou, Charalampia, Stamatia-Angeliki Kleftaki, Evdokia Valsamidou, Eirini Chroni, Theodora Biagki, Demetra Sigala, Konstantinos Koutoulogenis, Panagiotis Anapliotis, Aristea Gioxari, and Andriana C. Kaliora. 2023. "Food, Dietary Patterns, or Is Eating Behavior to Blame? Analyzing the Nutritional Aspects of Functional Dyspepsia" Nutrients 15, no. 6: 1544. https://doi.org/10.3390/nu15061544
APA StyleAmerikanou, C., Kleftaki, S.-A., Valsamidou, E., Chroni, E., Biagki, T., Sigala, D., Koutoulogenis, K., Anapliotis, P., Gioxari, A., & Kaliora, A. C. (2023). Food, Dietary Patterns, or Is Eating Behavior to Blame? Analyzing the Nutritional Aspects of Functional Dyspepsia. Nutrients, 15(6), 1544. https://doi.org/10.3390/nu15061544