

Association of Nutritional Status and Diet Diversity with Skeletal Muscle Strength and Quality of Life among Older Arab Adults: A Cross-Sectional Study
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
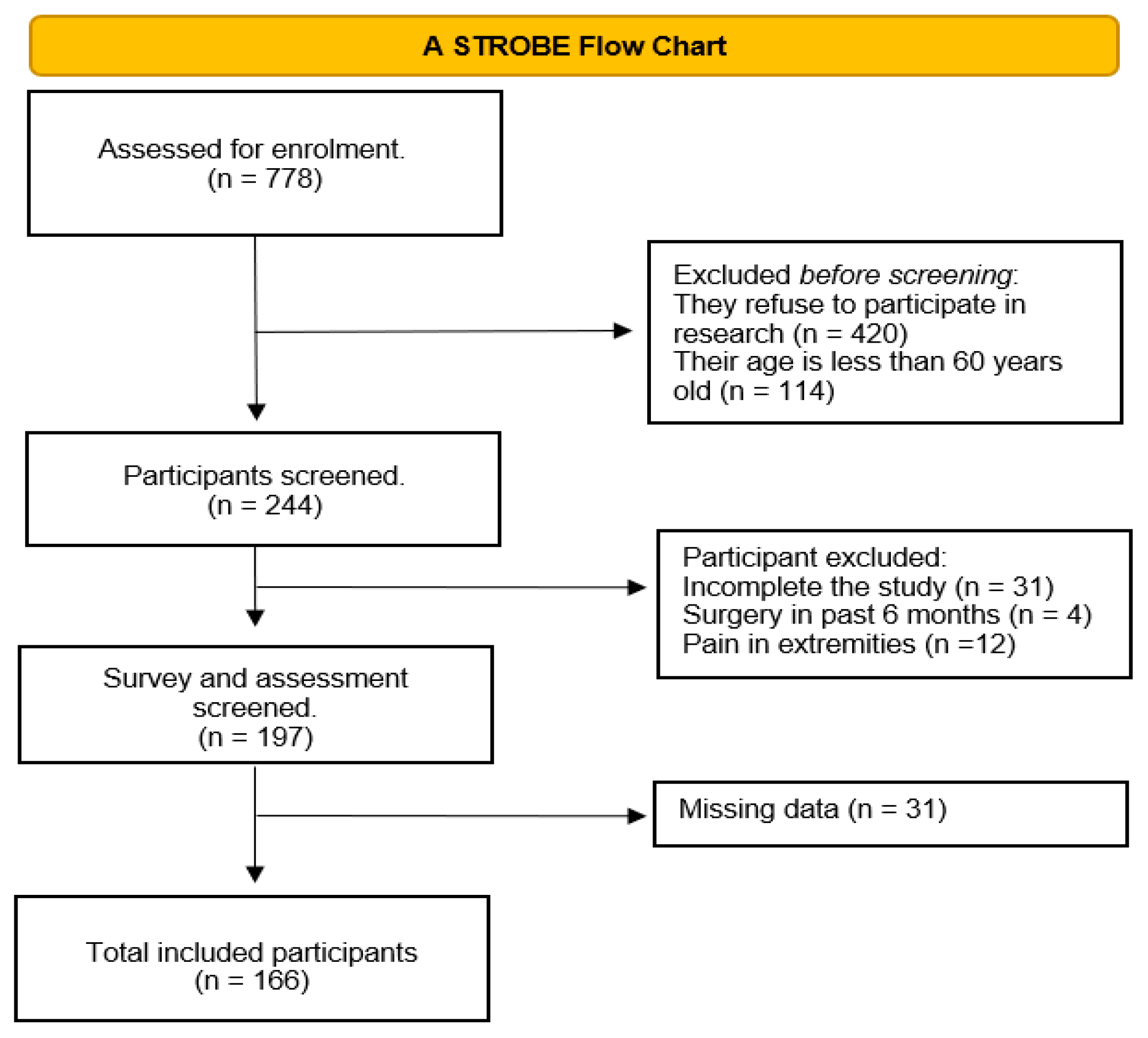
2.1. Study Design and Sample Selection
2.2. Sociodemographic Data and Anthropometric Measurements
2.3. Skeletal Muscle Strength
2.3.1. Handgrip Strength (HGS)
2.3.2. Knee Extension Strength (KES)
2.4. Nutritional Screening and Assessment
2.4.1. Mini Nutritional Assessment Short-Form (MNA-SF)
2.4.2. Dietary Variety Score (DVS)
2.5. Health-Related Quality of Life (HR-QoL)
2.6. Statistical Analysis
3. Results
3.1. General Characteristics and Nutritional Status of Older Adults
3.2. Muscle Strength, Calf Circumference, and Body Mass Index
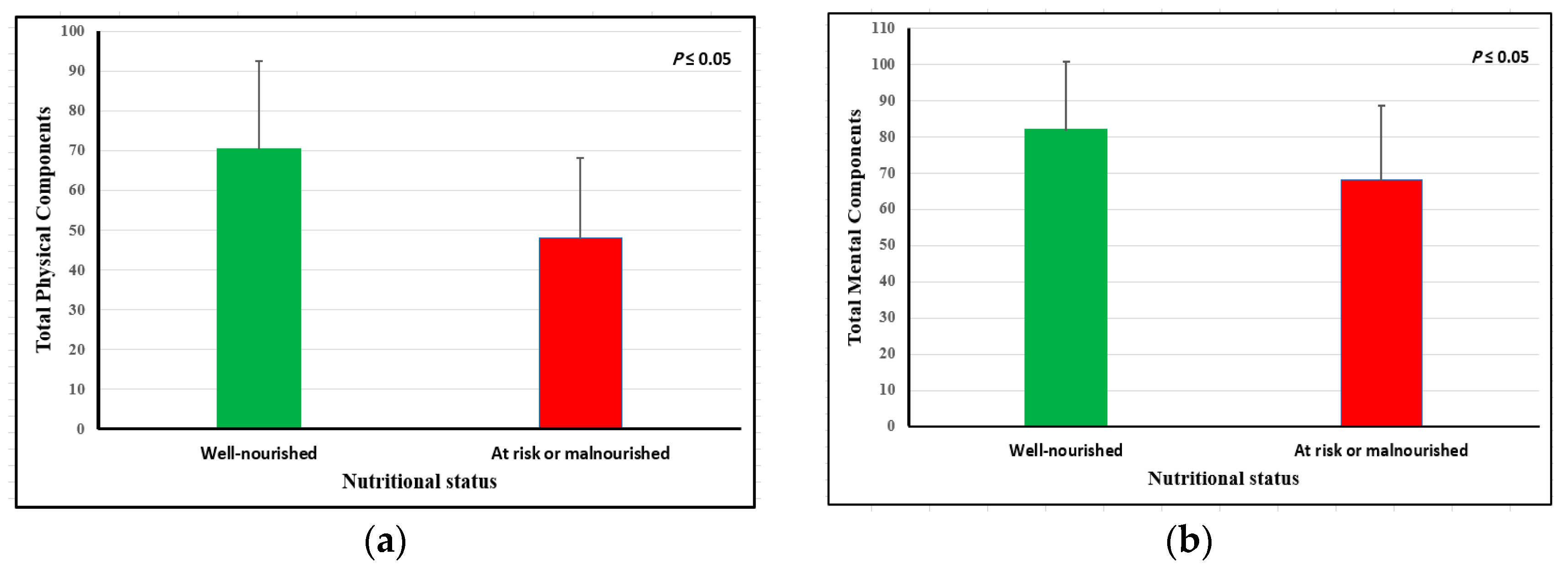
3.3. Health-Related Quality of Life and Nutritional Status
3.4. Diet Variety Score (DVS)
3.5. Binary Logistic Regression According to Nutritional Status of the Study Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Ageing and Health. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 11 March 2023).
- UNFPA. Arabstates. 2020. Available online: https://arabstates.unfpa.org/sites/default/files/pub-pdf/country_profile_-_saudia_27-10-2021.pdf (accessed on 20 April 2023).
- Bachmann, M.C.; Bellalta, S.; Basoalto, R.; Gómez-Valenzuela, F.; Jalil, Y.; Lépez, M.; Matamoros, A.; von Bernhardi, R. The Challenge by Multiple Environmental and Biological Factors Induce Inflammation in Aging: Their Role in the Promotion of Chronic Disease. Front. Immunol. 2020, 11, 570083. [Google Scholar] [CrossRef]
- Bindawas, S.M.; Vennu, V. The National and Regional Prevalence Rates of Disability, Type, of Disability and Severity in Saudi Arabia—Analysis of Demographic Survey Data. Int. J. Environ. Res. 2018, 15, 419. [Google Scholar]
- Dent, E.; Hoogendijk, E.O.; Visvanathan, R.; Wright, O.R.L. Malnutrition Screening and Assessment in Hospitalised Older People: A Review. J. Nutr. Heal. Aging 2019, 23, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Kiesswetter, E.; Colombo, M.G.; Meisinger, C.; Peters, A.; Thorand, B.; Holle, R.; Ladwig, K.H.; Schulz, H.; Grill, E.; Diekmann, R.; et al. Malnutrition and Related Risk Factors in Older Adults from Different Health-Care Settings. Public Health Nutr. 2020, 23, 446–456. [Google Scholar] [CrossRef]
- Walters, S.J.; Munro, J.F.; Brazier, J.E. Using the SF-36 with Older Adults: A Cross-Sectional Community-Based Survey. Age Ageing 2001, 30, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, S.I.; Ornelas, M.; Blanco, H.; Jurado-García, P.J.; Benavides, E.V.; Rodríguez-Villalobos, J.M.; Jiménez-Lira, C.; Blanco, J.R. Quality of Life in Mexican Older Adults: Factor Structure of the SF-36 Questionnaire. Healthcare 2022, 10, 200. [Google Scholar] [CrossRef] [PubMed]
- Halaweh, H. Correlation between Health-Related Quality of Life and Hand Grip Strength among Older Adults. Exp. Aging Res. 2020, 46, 178–191. [Google Scholar] [CrossRef]
- MNA Forms. Nestle. 2020. Available online: https://www.mna-elderly.com/development-and-validation (accessed on 8 March 2023).
- Kwon, J.; Suzuki, T.; Kumagai, S.; Shinkai, S.; Yukawa, H. Risk Factors for Dietary Variety Decline among Japanese Elderly in a Rural Community: A 8-Year Follow-up Study. Eur. J. Clin. Nutr. 2006, 60, 305–311. [Google Scholar] [CrossRef]
- Soysal, P.; Isik, A.T.; Arik, F.; Kalan, U.; Eyvaz, A.; Veronese, N. Validity of the Mini-Nutritional Assessment Scale for Evaluating Frailty Status in Older Adults. J. Am. Med. Dir. Assoc. 2019, 20, 183–187. [Google Scholar] [CrossRef]
- Zhang, X.; Pang, L.; Sharma, S.V.; Li, R.; Nyitray, A.G.; Edwards, B.J. The Validity of Three Malnutrition Screening Markers among Older Patients with Cancer. BMJ Support. Palliat. Care 2020, 10, 363–368. [Google Scholar] [CrossRef]
- Torheim, L.E.; Barikmo, I.; Parr, C.L.; Hatløy, A.; Ouattara, F.; Oshaug, A. Validation of Food Variety as an Indicator of Diet Quality Assessed with a Food Frequency Questionnaire for Western Mali. Eur. J. Clin. Nutr. 2003, 57, 1283–1291. [Google Scholar] [CrossRef]
- Papadopoulou, S.K. Sarcopenia: A Contemporary Health Problem among Older Adult Populations. Nutrients 2020, 12, 1293. [Google Scholar] [CrossRef]
- Benton, M.J.; Spicher, J.M.; Silva-Smith, A.L. Validity and Reliability of Handgrip Dynamometry in Older Adults: A Comparison of Two Widely Used Dynamometers. PLoS ONE 2022, 17, e0270132. [Google Scholar] [CrossRef]
- Yeung, S.Y.; Reijnierse, E.M.; Trappenburg, M.C.; Blauw, G.J.; Meskers, C.M.; Maier, A.B. Knee Extension Strength Measurements Should Be Considered as Part of the Comprehensive Geriatric Assessment. BMC Geriatr. 2018, 10, 130. [Google Scholar] [CrossRef]
- Sheikh, K.A.; Yagoub, U.; Elsatouhy, M.; Al Sanosi, R.; Mohamud, S.A. Reliability and Validity of the Arabic Version of the SF-36 Health Survey Questionnaire in Population of Khat Chewers—Jazan Region-Kingdom of Saudi Arabia. Appl. Res. Qual. Life 2019, 10, 1–13. [Google Scholar] [CrossRef]
- Godbole, V.Y.; Shah, M.R.; Mehta, K.G.; Shah, D.N. Assessment of Nutritional and Functional Status of Patients Attending the Geriatric Clinic of a Tertiary Care Hospital in Gujarat, India. Singapore Med. J. 2020, 61, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Olson, S.L.; Protas, E.J. Test-Retest Strength Reliability: Hand-Held Dynamometry in Community-Dwelling Elderly Fallers. Arch. Phys. Med. Rehabil. 2002, 83, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Ottenbacher, K.J.; Branch, L.G.; Ray, L.; Gonzales, V.A.; Peek, M.K.; Hinman, M.R. The Reliability of Upper- and Lower-Extremity Strength Testing in a Community Survey of Older Adults. Arch. Phys. Med. Rehabil. 2002, 83, 1423–1427. [Google Scholar] [CrossRef]
- Alfaro-Acha, A.; Snih, S.A.; Raji, M.A.; Kuo, Y.F.; Markides, K.S.; Ottenbacher, K.J. Handgrip Strength and Cognitive Decline in Older Mexican. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 61, 859–865. [Google Scholar] [CrossRef]
- Kim, Y.A.; Cho, Y.J.; Lee, G.H. Association of Handgrip Strength in Various Disabilities in Korean Adults over 50 Years Old: A Nationwide Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 9745. [Google Scholar] [CrossRef]
- Scott, D.; Shore-Lorenti, C.; McMillan, L.B.; Mesinovic, J.; Clark, R.A.; Hayes, A.; Sanders, K.M.; Duque, G.; Ebeling, P.R. Calf Muscle Density Is Independently Associated with Physical Function in Overweight and Obese Older Adults. J. Musculoskelet. Neuronal Interact. 2018, 18, 9–17. [Google Scholar]
- Vellas, B.; Villars, H.; Abellan, G.; Soto, M.E.; Rolland, Y.; Guigoz, Y.; Morley, J.E.; Chumlea, W.; Salva, A.; Rubenstein, L.Z.; et al. Overview of the MNA®-Its History and Challenges. J. Nutr. Heal. Aging 2006, 10, 456–463. [Google Scholar]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for Undernutrition in Geriatric Practice: Developing the Short-Form Mini-Nutritional Assessment (MNA-SF). J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2001, 56, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Guigoz, Y. The Mini Nutritional Assessment (MNA) Review of The Literature–What Does It Tell Us? Y. J. Nutr. Health Aging 2006, 10, 1–15. [Google Scholar]
- Kimura, M.; Moriyasu, A.; Kumagai, S.; Furuna, T.; Akita, S.; Kimura, S.; Suzuki, T. Community-Based Intervention to Improve Dietary Habits and Promote Physical Activity among Older Adults: A Cluster Randomized Trial. BMC Geriatr. 2013, 13, 8. [Google Scholar] [CrossRef]
- Tsuji, T.; Yamamoto, K.; Yamasaki, K.; Hayashi, F.; Momoki, C.; Yasui, Y.; Ohfuji, S.; Fukushima, W.; Habu, D. Lower Dietary Variety Is a Relevant Factor for Malnutrition in Older Japanese Home-Care Recipients: A Cross-Sectional Study. BMC Geriatr. 2019, 19, 197. [Google Scholar] [CrossRef]
- Alkhalaf, M.M.; Edwards, C.A.; Combet, E. Validation of a Food Frequency Questionnaire Specific for Salt Intake in Saudi Arabian Adults Using Urinary Biomarker and Repeated Multiple Pass 24-Hour Dietary Recall. Proc. Nutr. Soc. 2015, 74, 1–49. [Google Scholar] [CrossRef]
- 36-Item Short Form Survey. RAND Medical Outcomes Study. 2020. Available online: https://www.rand.org/health-care/surveys_tools/mos/36-item-short-form.html (accessed on 8 April 2022).
- El Osta, N.; Kanso, F.; Saad, R.; Khabbaz, L.R.; Fakhouri, J.; El Osta, L. Validation Du SF-36, Questionnaire Générique de La Qualité de Vie Liée à La Santé Chez Les Personnes Âgées Au Liban. East. Mediterr. Health J. 2019, 25, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Akoglu, H. User’s Guide to Correlation Coefficients. Turkish J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Acar Tek, N.; Karaçil-Ermumcu, M. Determinants of Health Related Quality of Life in Home Dwelling Elderly Population: Appetite and Nutritional Status. J. Nutr. Health Aging 2018, 22, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Cai, W.; Wang, G.; Shen, X. Prevalence and Contributing Factors of Osteoporosis in the Elderly over 70 Years Old: An Epidemiological Study of Several Community Health Centers in Shanghai. Ann. Cardiothorac. Surg. 2020, 9, 231–238. [Google Scholar] [CrossRef]
- Hua, N.; Zhang, Y.; Tan, X.; Liu, L.; Mo, Y.; Yao, X.; Wang, X.; Wiley, J.; Wang, X. Nutritional Status and Sarcopenia in Nursing Home Residents: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 17013. [Google Scholar] [CrossRef]
- Salminen, K.S.; Suominen, M.H.; Soini, H.; Kautiainen, H.; Savikko, N.; Saarela, R.K.; Muurinen, S.; Pitkala, K.H. Associations Between Nutritional Status and Health-Related Quality of Life Among Long-Term Care Residents in Helsinki. J. Nutr. Health Aging 2019, 23, 474–478. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional Status in Older Persons According to Healthcare Setting: A Systematic Review and Meta-Analysis of Prevalence Data Using MNA®. Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef]
- Alzahrani, S.H.; Abdelmoneim, I.; Sayed, E.; Alshamrani, S.M. Prevalence and Factors Associated with Geriatric Malnutrition in an Outpatient Clinic of a Teaching Hospital in Jeddah, Saudi Arabia. Ann. Saudi Med. 2016, 16, 346–351. [Google Scholar] [CrossRef]
- Seesen, M.; Sirikul, W.; Ruangsuriya, J.; Griffiths, J.; Siviroj, P. Cognitive Frailty in Thai Community-Dwelling Elderly: Prevalence and Its Association with Malnutrition. Nutrients 2021, 11, 4239. [Google Scholar] [CrossRef] [PubMed]
- Khatami, F.; Shafiee, G.; Kamali, K.; Ebrahimi, M.; Sharifi, F.; Tanjani, P.T. Correlation between Malnutrition and Health-Related Quality of Life (HRQOL) in Elderly Iranian Adults. J. Int. Med. Res. 2020, 48. [Google Scholar] [CrossRef]
- Debia, N.; Oliveira, A.C.; Rego, S. Prediction of Nutritional Risk in Elderly Using MNA-SF and Its Association with Anthropometric Measures. IOSR J. Nurs. Health Sci. 2021, 10, 1–5. [Google Scholar]
- Akbar and Setiati. Hand Grip Strength and Nutritional Status in Hospitalized Oncological Patients. Rev. Nutr. 2018, 31, 489–499. [Google Scholar] [CrossRef]
- Bahat, G.; Tufan, F.; Saka, B.; Akin, S.; Ozkaya, H.; Yucel, N.; Erten, N.; Karan, M.A. Which Body Mass Index (BMI) Is Better in the Elderly for Functional Status? Arch. Gerontol. Geriatr. 2012, 54, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Javed, A.A.; Aljied, R.; Allison, D.J.; Anderson, L.N.; Ma, J.; Raina, P. Body Mass Index and All-Cause Mortality in Older Adults: A Scoping Review of Observational Studies. Obes. Rev. 2020, 21, e13035. [Google Scholar] [CrossRef] [PubMed]
- Burman, M.; Hörnsten, C.; Gustafson, Y.; Olofsson, B.; Nordström, P. Obesity May Increase Survival, Regardless of Nutritional Status: A Swedish Cohort Study in Nursing Homes. BMC Geriatr. 2022, 22, 655. [Google Scholar] [CrossRef] [PubMed]
- Roberts-Clarke, D.; Fornusek, C.; Singh, M.F.; Burns, J.; Hackett, D.A. Examining Hand Dominance Using Dynamometric Grip Strength Testing as Evidence for Overwork Weakness in Charcot-Marie-Tooth Disease: A Systematic Review and Meta-Analysis. Int. J. Rehabil. Res. 2016, 39, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Wichelhaus, A.; Harms, C.; Neumann, J.; Ziegler, S.; Kundt, G.; Prommersberger, K.J.; Mittlmeier, T.; Mühldorfer-Fodor, M. Parameters Influencing Hand Grip Strength Measured with the Manugraphy System. BMC Musculoskelet. Disord. 2018, 19, 54. [Google Scholar] [CrossRef]
- Willems, S.M.; Wright, D.J.; Day, F.R. Large-Scale GWAS Identifies Multiple Loci for Hand Grip Strength Providing Biological Insights into Muscular Fitness. Nat. Commun. 2017, 8, 2–10. [Google Scholar] [CrossRef]
- Lin, M.H.; Chang, C.Y.; Wu, D.M.; Lu, C.H.; Kuo, C.C.; Chu, N.F. Relationship of Multimorbidity, Obesity Status, and Grip Strength among Older Adults in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 7540. [Google Scholar] [CrossRef]
- Nuzzo, J.L. Narrative Review of Sex Differences in Muscle Strength, Endurance, Activation, Size, Fiber Type, and Strength Training Participation Rates, Preferences, Motivations, Injuries, and Neuromuscular Adaptations. J. Strength Cond. Res. 2023, 37, 494–536. [Google Scholar] [CrossRef]
- Moghadam, M.R.S.F.; Jazinaki, M.S.; Rashidipour, M.; Rezvani, R.; Pezeshki, P.; Mobarhan, M.G.; Hosseini, Z. Mini Nutrition Assessment-Short Form score is associated with sarcopenia even among nourished people—A result of a feasibility study of a registry. Aging Med. 2023, 6, 264–271. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Dawson Hughes, B.; Scott, D.; Sanders, K.M.; Rizzoli, R. Nutritional Strategies for Maintaining Muscle Mass and Strength from Middle Age to Later Life: A Narrative Review. Maturitas 2020, 132, 57–64. [Google Scholar] [CrossRef]
- Kojima, N.; Kim, M.; Saito, K.; Yoshida, H.; Yoshida, Y.; Hirano, H.; Obuchi, S.; Shimada, H.; Suzuki, T.; Kim, H. Lifestyle-Related Factors Contributing to Decline in Knee Extension Strength among Elderly Women: A Cross-Sectional and Longitudinal Cohort Study. PLoS ONE 2015, 10, e0132523. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Nishi, M.; Murayama, H.; Amano, H.; Taniguchi, Y.; Nofuji, Y.; Narita, M.; Matsuo, E.; Seino, S.; Kawano, Y.; et al. Dietary Variety and Decline in Lean Mass and Physical Performance in Community-Dwelling Older Japanese: A 4-Year Follow-up Study. J. Nutr. Health Aging 2017, 21, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Tasigchana, R.F.; León-Muñoz, L.M.; López-García, E.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Mediterranean Diet and Health-Related Quality of Life in Two Cohorts of Community-Dwelling Older Adults. PLoS ONE 2016, 11, e0151596. [Google Scholar]
- Gopinath, B.; Russell, J.; Flood, V.M.; Burlutsky, G.; Mitchell, P. Adherence to Dietary Guidelines Positively Affects Quality of Life and Functional Status of Older Adults. J. Acad. Nutr. Diet. 2014, 114, 220–229. [Google Scholar] [CrossRef]
- Salminen, K.S.; Suominen, M.H.; Kautiainen, H.; Pitkälä, K.H. Associations Between Nutritional Status, Frailty and Health-Related Quality of Life Among Older Long-Term Care Residents in Helsinki. J. Nutr. Health Aging 2020, 24, 319–324. [Google Scholar] [CrossRef]
- Rasheed, S.; Woods, R.T. Malnutrition and Quality of Life in Older People: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2013, 12, 561–566. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| MNA-SF | ||||
|---|---|---|---|---|
| Variable | All n = 166 | Well-Nourished n = 138 | At Risk of Malnutrition or Malnourished n = 28 | p-Value |
| Age | 66 (8) | 66 (8) | 67 (9) | 0.416 |
| Gender | 0.440 | |||
| Male | 70 (42.2%) | 63 (45.7%) | 7 (25%) | |
| Female | 96 (57.8%) | 75 (54.3%) | 21(75%) | |
| Academic level | 0.010 | |||
| Illiterate | 63 (38.0%) | 48 (34.8%) | 15 (53.6%) | |
| School | 53 (31.9%) | 41 (29.7%) | 12 (42.9%) | |
| Diploma or bachelor | 46 (27.7%) | 45 (32.6%) | 1 (3.6%) | |
| Postgraduate | 4 (2.4%) | 4 (2.9%) | 0 (0.0%) | |
| Marital status | 0.328 | |||
| Single | 3 (1.8%) | 2 (1.4%) | 1 (3.6%) | |
| Married | 113 (68.1%) | 98 (71.0%) | 15 (53.6%) | |
| Divorced | 13 (7.8%) | 10 (7.2%) | 3 (10.7%) | |
| Widowed | 37 (22.3%) | 28 (20.3%) | 9 (32.1%) | |
| Monthly income | 0.220 | |||
| <3000 SR | 63 (38.0%) | 51 (37.0%) | 12 (42.9%) | |
| 3000–5999 SR | 37 (22.3%) | 26 (18.8%) | 11(39.3%) | |
| 6000–10,000 SR | 21 (12.7%) | 18 (13.0%) | 3 (10.7%) | |
| >10,000 SR | 45 (27.1%) | 43 (31.2%) | 2 (7.1%) | |
| Older adults have a disease | 161 (97.0%) | 133 (96.4%) | 28 (100%) | 0.590 |
| Older adults on medication | 159 (95.8%) | 132 (95.7%) | 27 (96.4%) | 1.000 |
| Comorbidities | ||||
| Hypercholesterolemia | 43 (25.9%) | 34 (24.6%) | 9 (32.1%) | 0.409 |
| CVD | 17 (10.2%) | 12 (8.7%) | 5 (17.9%) | 0.170 |
| HTN | 115 (69.3%) | 93 (67.4%) | 22 (78.6%) | 0.242 |
| Osteoporosis | 43 (25.9%) | 29 (21%) | 14 (50%) | 0.001 |
| DM | 119 (71.7%) | 98 (71%) | 21 (75%) | 0.670 |
| Other | 75 (45.2%) | 59 (42.8%) | 16 (57.1%) | 0.163 |
| Number of comorbidities | 0.071 | |||
| None | 4 (2.4%) | 4 (2.9%) | 0 (0.0%) | |
| One | 36 (21.7%) | 34 (24.6%) | 2 (7.1%) | |
| Two | 47 (28.3%) | 40 (29%) | 7 (25%) | |
| Three | 41 (24.7%) | 34 (24.6%) | 7 (25%) | |
| Four | 31 (18.7%) | 21(15.2%) | 10 (35.7%) | |
| Five or more | 7 (4.2%) | 5 (3.6%) | 2 (7.1%) | |
| MNA-SF | ||||
|---|---|---|---|---|
| Variable | All n = 166 | Well-Nourished n = 138 | At Risk of Malnutrition or Malnourished n = 28 | p-Value |
| HGS (kg) | 20 (14) | 21 (12.25) | 17.5 (9.75) | 0.001 |
| KES (kg) | 10.85 (3.7) | 11 (3.70) | 10.1 (4.03) | 0.048 |
| CC (cm) | 36 (5.8) | 36 (5.13) | 36.5 (11.75) | 0.943 |
| BMI (kg/m2) | 29.3 (7.74) | 29.6 (7.35) | 28.38 (13.94) | 0.380 |
| Variable | HGS (Kg) | KES (Kg) | BMI (kg/m2) | CC (CM) |
|---|---|---|---|---|
| All | ||||
| MNA-SF scores | 0.30 ** | 0.23 ** | 0.080 | 0.09 |
| HGS (Kg) | - | 0.54 ** | −0.10 | −0.02 |
| KES (Kg) | - | - | −0.06 | −0.12 |
| BMI (kg/m2) | - | - | - | 0.70 ** |
| MNA-SF Score | ||
|---|---|---|
| Variable | r | p Value |
| Total physical components | 0.35 | 0.001 |
| Total mental components | 0.33 | 0.001 |
| Total HR-QoL score | 0.40 | 0.001 |
| DVS | ||||
|---|---|---|---|---|
| Variable | All n = 166 | Well-Nourished n = 138 | At Risk of Malnutrition or Malnourished n = 28 | p-Value |
| Daily intake of food groups | ||||
| Daily intake of dairy products | 69 (41.6%) | 59 (42.8%) | 10 (35.7%) | 0.491 |
| Daily intake of fruits | 136 (81.9%) | 116 (84.1%) | 20 (71.4%) | 0.113 |
| Daily intake of vegetables | 96 (57.8%) | 76 (55.1%) | 20 (71.4%) | 0.110 |
| Daily intake of meats and eggs | 95 (57.2%) | 79 (57.2%) | 16 (57.1%) | 0.992 |
| Daily intake of carbohydrates | 136 (81.9%) | 113 (81.9%) | 23 (82.1%) | 0.974 |
| Daily intake of all food groups | 23 (13.9%) | 21 (15.2%) | 2 (7.1%) | 0.373 |
| Dairy products | 0.223 | |||
| Rarely | 16 (9.6%) | 11 (8.0%) | 5 (17.9%) | |
| 1–2 times/week | 34 (20.5%) | 29 (21%) | 5 (17.9%) | |
| 3–4 times/week | 30 (18.1%) | 23(16.7%) | 7 (25.0%) | |
| 5–7 times/week | 86 (51.8%) | 75 (54.3%) | 11 (39.3%) | |
| Fruits | 0.247 | |||
| Rarely | 1 (0.6%) | 1 (0.7%) | 0 (0.0%) | |
| 1–2 times/week | 5 (3.0%) | 3 (2.2%) | 2 (7.1%) | |
| 3–4 times/week | 9 (5.4%) | 6 (4.3%) | 3 (10.7%) | |
| 5–7 times/week | 151 (91.0%) | 128 (92.8%) | 23 (82.1%) | |
| Vegetables | 0.343 | |||
| Rarely | 3 (1.8%) | 2 (1.4%) | 1 (3.6%) | |
| 1–2 times/week | 23 (13.9%) | 18 (13.0%) | 5 (17.9%) | |
| 3–4 times/week | 30 (18.1%) | 28 (20.3%) | 2 (7.1%) | |
| 5–7 times/week | 110 (66.3%) | 90 (65.2%) | 20 (71.4%) | |
| Meats and eggs | 0.562 | |||
| Rarely | 1 (0.6%) | 1 (0.7%) | 0 (0.0%) | |
| 1–2 times/week | 19 (11.4%) | 14 (10.1%) | 5 (17.9%) | |
| 3–4 times/week | 27 (16.3%) | 24 (17.4%) | 3 (10.7%) | |
| 5–7 times/week | 119 (71.7%) | 99 (71.7%) | 20 (71.4%) | |
| Breads/grains/cereals | 0.712 | |||
| Rarely | 2 (1.2%) | 2 (1.4%) | 0 (0.0%) | |
| 1–2 times/week | 8 (4.8%) | 7 (5.1%) | 1 (3.6%) | |
| 3–4 times/week | 11 (6.6%) | 8 (5.8%) | 3 (10.7%) | |
| 5–7 times/week | 145 (87.3%) | 121(87.7%) | 24 (85.7%) | |
| DVS categories | 0.037 | |||
| Low | 60 (36.1%) | 44 (31.9%) | 16 (57.1%) | |
| Moderate | 64 (38.6%) | 56 (40.6%) | 8 (28.6%) | |
| High | 42 (25.3%) | 38 (27.5%) | 4 (14.3%) | |
| DVS | ||
|---|---|---|
| Variable | r | p-Value |
| Total physical components | 0.19 * | 0.016 |
| Total mental components | 0.09 | 0.253 |
| Total HR-QoL score | 0.16 * | 0.039 |
| Variable | Model 1 OR (95% CI) | Model 2 OR (95% CI) | Model 3 OR (95% CI) |
|---|---|---|---|
| Total MNA-SF score | 1.33 (1.08–1.64) * | 1.32 (1.07–1.63) * | 1.30 (1.01–1.72) * |
| Total DVS | 1.07 (0.91–1.26) | 1.11 (0.88–1.41) | 1.13 (0.83–1.53) |
| Variable | Model 1 OR (95% CI) | Model 2 OR (95% CI) | Model 3 OR (95% CI) |
|---|---|---|---|
| Total MNA-SF score | 1.19 (1.10–1.44) * | 1.18 (0.96–1.45) | 1.09 (0.86–1.38) |
| Total DVS | 1.12(0.95–1.32) | 1.04 (0.82–1.32) | 1.02 (0.77–1.33) |
| Variable | Model 1 OR (95% CI) | Model 2 OR (95% CI) | Model 3 OR (95% CI) |
|---|---|---|---|
| Total MNA-SF score | 1.62 (1.30–2.03) * | 1.64 (1.30–2.07) * | 1.64 (1.23–2.18) * |
| Total DVS | 1.24 (1.05–1.47) * | 1.12 (0.87–1.44) | 1.25 (0.91–1.71) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alotaibi, R.; Aladel, A.; Alshammari, S.A.; Abulmeaty, M.M.A.; Alhamdan, A.A. Association of Nutritional Status and Diet Diversity with Skeletal Muscle Strength and Quality of Life among Older Arab Adults: A Cross-Sectional Study. Nutrients 2023, 15, 4382. https://doi.org/10.3390/nu15204382
Alotaibi R, Aladel A, Alshammari SA, Abulmeaty MMA, Alhamdan AA. Association of Nutritional Status and Diet Diversity with Skeletal Muscle Strength and Quality of Life among Older Arab Adults: A Cross-Sectional Study. Nutrients. 2023; 15(20):4382. https://doi.org/10.3390/nu15204382
Chicago/Turabian StyleAlotaibi, Rahaf, Alanoud Aladel, Sulaiman A. Alshammari, Mahmoud M. A. Abulmeaty, and Adel A. Alhamdan. 2023. "Association of Nutritional Status and Diet Diversity with Skeletal Muscle Strength and Quality of Life among Older Arab Adults: A Cross-Sectional Study" Nutrients 15, no. 20: 4382. https://doi.org/10.3390/nu15204382
APA StyleAlotaibi, R., Aladel, A., Alshammari, S. A., Abulmeaty, M. M. A., & Alhamdan, A. A. (2023). Association of Nutritional Status and Diet Diversity with Skeletal Muscle Strength and Quality of Life among Older Arab Adults: A Cross-Sectional Study. Nutrients, 15(20), 4382. https://doi.org/10.3390/nu15204382