
Effect of Time-Restricted Eating versus Daily Calorie Restriction on Mood and Quality of Life in Adults with Obesity
 , , ,
, , ,  , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Participant Selection and Randomization
2.2. Time-Restricted Eating Protocol
2.3. Calorie Restriction Protocol
2.4. Control Group Protocol
2.5. Assessment of Body Weight and Body Composition
2.6. Diet Adherence and Physical Activity
2.7. Assessment of Mood
2.8. Assessment of Quality of Life
2.9. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Body Weight and Body Composition
3.3. Diet Adherence and Physical Activity
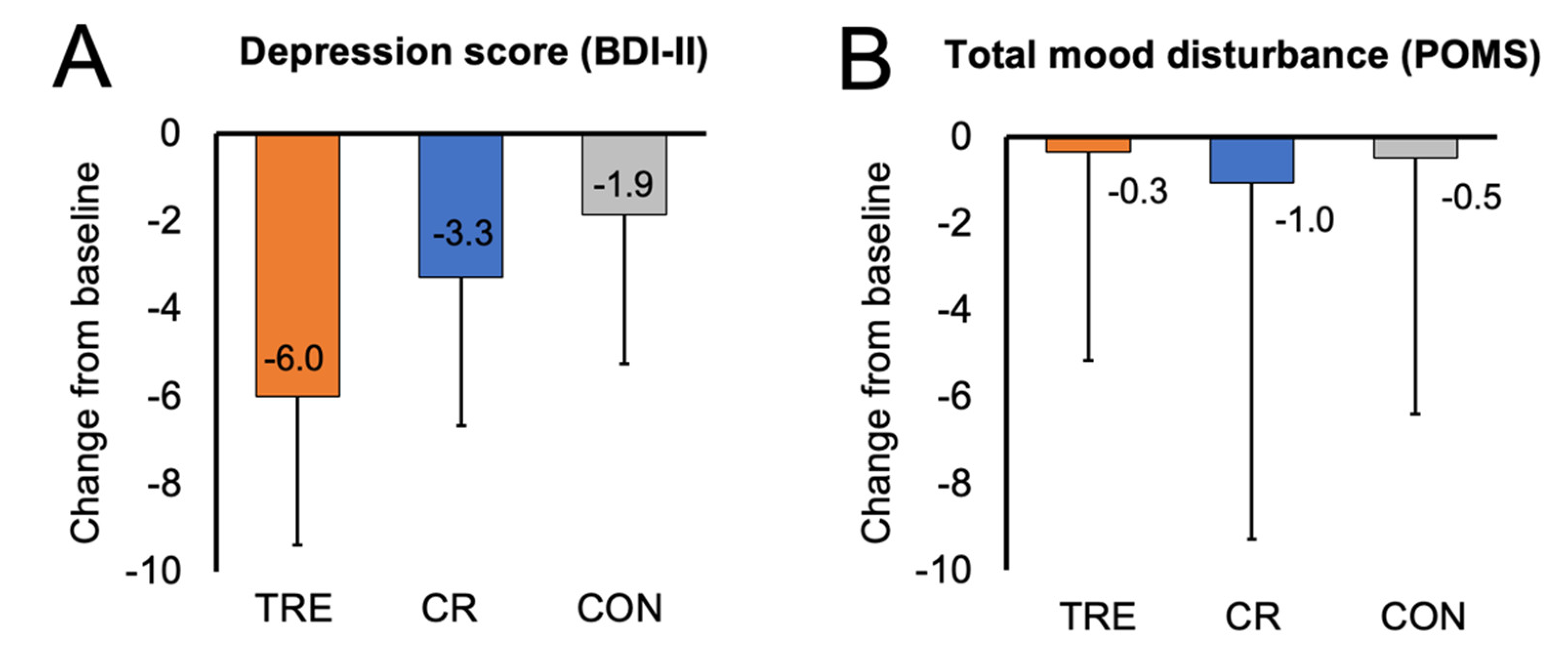
3.4. Mood
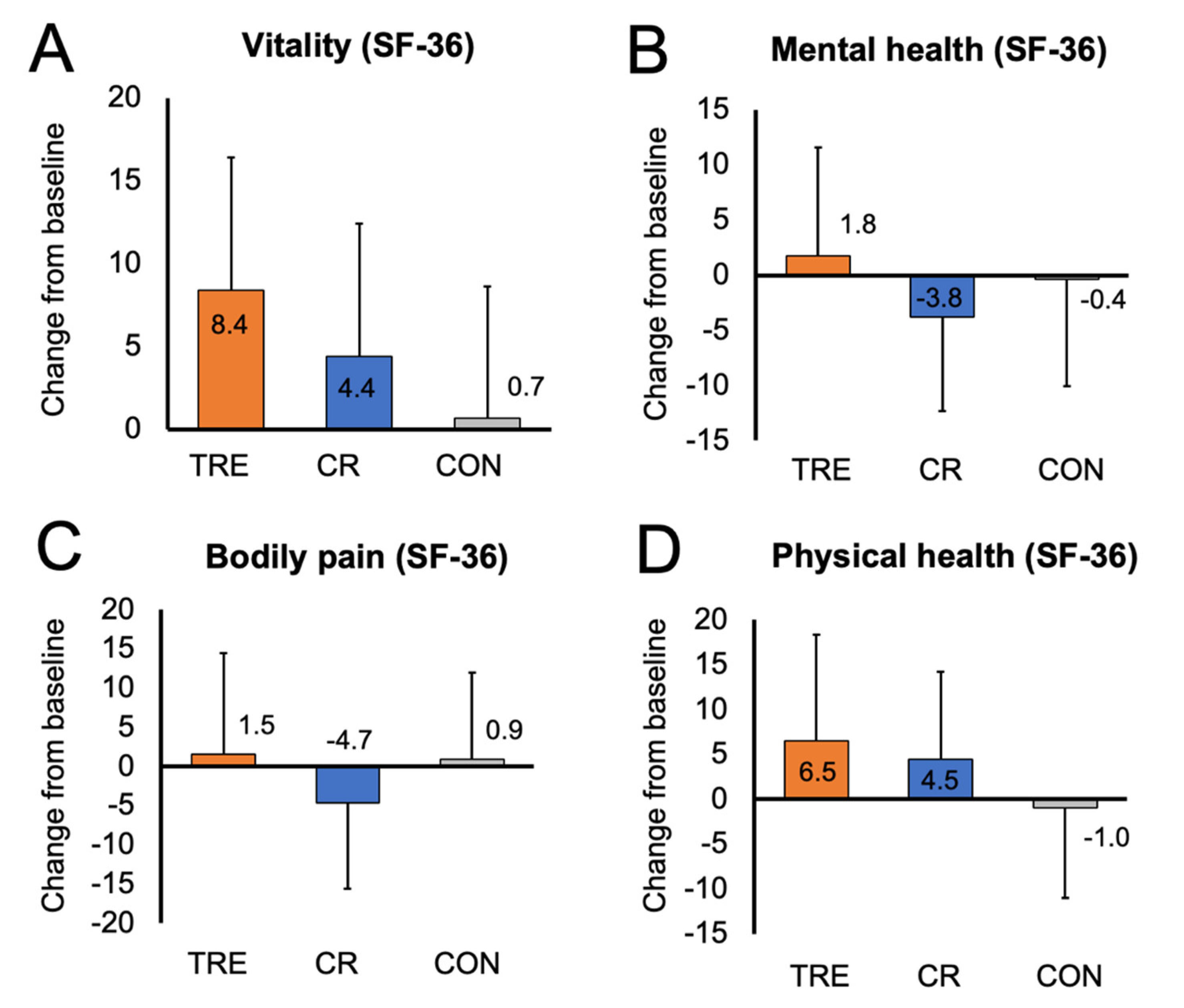
3.5. Quality of Life
3.6. Relationships between Changes in Body Weight, Physical Activity, Mood, and Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Trial Registration
References
- Mather, A.A.; Cox, B.J.; Enns, M.W.; Sareen, J. Associations of obesity with psychiatric disorders and suicidal behaviors in a nationally representative sample. J. Psychosom. Res. 2009, 66, 277–285. Available online: https://www.clinicalkey.es/playcontent/1-s2.0-S0022399908004297 (accessed on 1 August 2023). [CrossRef]
- Simon, G.E.; Von Korff, M.; Saunders, K.; Miglioretti, D.L.; Crane, P.K.; van Belle, G.; Kessler, R.C. Association between obesity and psychiatric disorders in the US adult population. Arch. Gen. Psychiatry 2006, 63, 824–830. [Google Scholar] [CrossRef]
- Petry, N.M.; Barry, D.; Pietrzak, R.H.; Wagner, J.A. Overweight and obesity are associated with psychiatric disorders: Results from the national epidemiologic survey on alcohol and related conditions. Psychosom. Med. 2008, 70, 288–297. Available online: https://www.ncbi.nlm.nih.gov/pubmed/18378873 (accessed on 1 August 2023). [CrossRef]
- Murphy, J.M.; Horton, N.J.; Burke, J.D.; Monson, R.R.; Laird, N.M.; Lesage, A.; Sobol, A.M. Obesity and weight gain in relation to depression: Findings from the stirling county study. Int. J. Obes. 2009, 33, 335–341. Available online: https://agris.fao.org/agris-search/search.do?recordID=US201301612652 (accessed on 1 August 2023). [CrossRef][Green Version]
- Anderson, S.E.; Cohen, P.; Naumova, E.N.; Must, A. Association of depression and anxiety disorders with weight change in a prospective community-based study of children followed up into adulthood. Arch. Pediatr. Adolesc. Med. 2006, 160, 285–291. [Google Scholar] [CrossRef]
- Roberts, R.E.; Deleger, S.; Strawbridge, W.J.; Kaplan, G.A. Prospective association between obesity and depression: Evidence from the alameda county study. Int. J. Obes. 2003, 27, 514–521. Available online: https://agris.fao.org/agris-search/search.do?recordID=US201500073875 (accessed on 1 August 2023). [CrossRef]
- Herva, A.; Laitinen, J.; Miettunen, J.; Veijola, J.; Karvonen, J.T.; Läksy, K.; Joukamaa, M. Obesity and depression: Results from the longitudinal northern finland 1966 birth cohort study. Int. J. Obes. 2006, 30, 520–527. [Google Scholar] [CrossRef]
- Barry, D.; Pietrzak, R.H.; Petry, N.M. Gender differences in associations between body mass index and DSM-IV mood and anxiety disorders: Results from the national epidemiologic survey on alcohol and related conditions. Ann. Epidemiol. 2008, 18, 458–466. Available online: https://www.clinicalkey.es/playcontent/1-s2.0-S1047279708000100 (accessed on 1 August 2023). [CrossRef]
- Heo, M.; Pietrobelli, A.; Fontaine, K.R.; Sirey, J.A.; Faith, M.S. Depressive mood and obesity in US adults: Comparison and moderation by sex, age, and race. Int. J. Obes. 2006, 30, 513–519. [Google Scholar] [CrossRef]
- Kolotkin, R.L.; Andersen, J.R. A systematic review of reviews: Exploring the relationship between obesity, weight loss and health-related quality of life. Clin. Obes. 2017, 7, 273–289. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/cob.12203 (accessed on 1 August 2023). [CrossRef]
- Ul-Haq, Z.; Mackay, D.F.; Fenwick, E.; Pell, J.P. Meta-analysis of the association between body mass index and health-related quality of life among adults, assessed by the SF-36. Obesity 2013, 21, E322–E327. [Google Scholar] [CrossRef]
- De Zwaan, M.; Petersen, I.; Kaerber, M.; Burgmer, R.; Nolting, B.; Legenbauer, T.; Benecke, A.; Herpertz, S. Obesity and quality of life: A controlled study of normal-weight and obese individuals. Psychosomatics (Wash. DC) 2009, 50, 474–482. Available online: https://www.clinicalkey.es/playcontent/1-s2.0-S0033318209708400 (accessed on 1 August 2023). [CrossRef]
- Kushner, R.F.; Foster, G.D. Obesity and quality of life. Nutrition 2000, 16, 947. [Google Scholar] [CrossRef]
- Larsson, U.; Karlsson, J.; Sullivan, M. Impact of overweight and obesity on health-related quality of life—A Swedish population study. Int. J. Obes. 2002, 26, 417–424. Available online: https://www.ncbi.nlm.nih.gov/pubmed/11896499 (accessed on 1 August 2023). [CrossRef]
- Saraç, F.; Parýldar, S.; Duman, E.; Saygýlý, F.; Tüzün, M.; Yýlmaz, C. Quality of life for obese women and men in turkey. Prev. Chronic Dis. 2007, 4, A50. Available online: https://www.ncbi.nlm.nih.gov/pubmed/17572954 (accessed on 1 August 2023).
- Fabricatore, A.N.; Wadden, T.A.; Higginbotham, A.J.; Faulconbridge, L.F.; Nguyen, A.M.; Heymsfield, S.B.; Faith, M.S. Intentional weight loss and changes in symptoms of depression: A systematic review and meta-analysis. Int. J. Obes. 2011, 35, 1363–1376. Available online: https://agris.fao.org/agris-search/search.do?recordID=US201500073606 (accessed on 1 August 2023). [CrossRef]
- Warkentin, L.M.; Das, D.; Majumdar, S.R.; Johnson, J.A.; Padwal, R.S. Effect of weight loss on health-related quality of life: Systematic review and meta-analysis of randomized trials. Obes. Rev. 2014, 15, 169–182. Available online: https://agris.fao.org/agris-search/search.do?recordID=US201500079926 (accessed on 1 August 2023). [CrossRef]
- Martin, C.K.; Bhapkar, M.; Pittas, A.G.; Pieper, C.F.; Das, S.K.; Williamson, D.A.; Scott, T.; Redman, L.M.; Stein, R.; Gilhooly, C.H.; et al. Effect of calorie restriction on mood, quality of life, sleep, and sexual function in healthy nonobese adults: The CALERIE 2 randomized clinical trial. JAMA Intern. Med. 2016, 176, 743–752. [Google Scholar] [CrossRef]
- Prehn, K.; von Schwartzenberg, R.J.; Mai, K.; Zeitz, U.; Witte, A.V.; Hampel, D.; Szela, A.-M.; Fabian, S.; Grittner, U.; Spranger, J.; et al. Caloric restriction in older Adults—Differential effects of weight loss and reduced weight on brain structure and function. Cereb. Cortex 2017, 27, 1765–1778. Available online: https://www.ncbi.nlm.nih.gov/pubmed/26838769 (accessed on 1 August 2023). [CrossRef]
- Varady, K.A.; Cienfuegos, S.; Ezpeleta, M.; Gabel, K. Clinical application of intermittent fasting for weight loss: Progress and future directions. Nat. Rev. Endocrinol. 2022, 18, 309–321. Available online: https://www.ncbi.nlm.nih.gov/pubmed/35194176 (accessed on 1 August 2023). [CrossRef]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutr. Healthy Aging 2018, 4, 345–353. Available online: https://www.ncbi.nlm.nih.gov/pubmed/29951594 (accessed on 1 August 2023). [CrossRef]
- Cienfuegos, S.; Gabel, K.; Kalam, F.; Ezpeleta, M.; Wiseman, E.; Pavlou, V.; Lin, S.; Oliveira, M.L.; Varady, K.A. Effects of 4- and 6-h time-restricted feeding on weight and cardiometabolic health: A randomized controlled trial in adults with obesity. Cell Metab. 2020, 32, 366–378.e3. [Google Scholar] [CrossRef]
- Jamshed, H.; Beyl, R.A.; Della Manna, D.L.; Yang, E.S.; Ravussin, E.; Peterson, C.M. Early time-restricted feeding improves 24-hour glucose levels and affects markers of the circadian clock, aging, and autophagy in humans. Nutrients 2019, 11, 1234. Available online: https://www.ncbi.nlm.nih.gov/pubmed/31151228 (accessed on 1 August 2023). [CrossRef]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metab. 2020, 31, 92–104.e5. [Google Scholar] [CrossRef]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q.F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. J. Transl. Med. 2016, 14, 290. Available online: https://www.ncbi.nlm.nih.gov/pubmed/27737674 (accessed on 1 August 2023). [CrossRef]
- Varady, K.A.; Cienfuegos, S.; Ezpeleta, M.; Gabel, K. Cardiometabolic benefits of intermittent fasting. Annu. Rev. Nutr. 2021, 41, 333–361. [Google Scholar] [CrossRef]
- Chow, L.S.; Manoogian, E.N.C.; Alvear, A.; Fleischer, J.G.; Thor, H.; Dietsche, K.; Wang, Q.; Hodges, J.S.; Esch, N.; Malaeb, S.; et al. Time-Restricted eating effects on body composition and metabolic measures in humans who are overweight: A feasibility study. Obesity 2020, 28, 860. [Google Scholar] [CrossRef]
- Lin, S.; Cienfuegos, S.; Ezpeleta, M.; Gabel, K.; Pavlou, V.; Mulas, A.; Chakos, K.; McStay, M.; Wu, J.; Tussing-Humphreys, L.; et al. Time-restricted eating without calorie counting for weight loss in a racially diverse population: A randomized controlled trial. Ann. Intern. Med. 2023. Available online: https://www.ncbi.nlm.nih.gov/pubmed/37364268 (accessed on 1 August 2023). [CrossRef]
- Diabetes Management Guidelines. American Diabetes Association. Available online: http://www.ndei.org/ADA-diabetes-management-guidelines-diagnosis-A1C-testing.aspx.html (accessed on 1 August 2023).
- Mifflin, M.; St Jeor, S.; Hill, L.; Scott, B.; Daugherty, S.; Koh, Y. A new predictive equation for resting energy expenditure in healthy individuals. Am. J. Clin. Nutr. 1990, 51, 241–247. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US department of agriculture automated multiple-pass method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef]
- Wang, Y.; Gorenstein, C. Psychometric properties of the beck depression inventory-II: A comprehensive review. Rev. Bras. Psiquiatr. 2013, 35, 416–431. Available online: https://www.ncbi.nlm.nih.gov/pubmed/24402217 (accessed on 1 August 2023). [CrossRef]
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Profile of Mood States: Technical Update; Multi-Health Systems: North Tonawanda, NY, USA, 2003. [Google Scholar]
- Ware, J.E., Jr. SF-36 Health Survey: Manual and Interpretation Guide; Health Assessment Lab: New York, NY, USA, 1993. [Google Scholar]
- Blasco, B.V.; García-Jiménez, J.; Bodoano, I.; Gutiérrez-Rojas, L. Obesity and depression: Its prevalence and influence as a prognostic factor: A systematic review. Psychiatry Investig. 2020, 17, 715–724. Available online: https://search.proquest.com/docview/2432858016 (accessed on 1 August 2023). [CrossRef] [PubMed]
- Lasikiewicz, N.; Myrissa, K.; Hoyland, A.; Lawton, C.L. Psychological benefits of weight loss following behavioural and/or dietary weight loss interventions. A systematic research review. Appetite 2014, 72, 123–137. [Google Scholar] [CrossRef] [PubMed]
- Steger, F.L.; Jamshed, H.; Bryan, D.R.; Richman, J.S.; Warriner, A.H.; Hanick, C.J.; Martin, C.K.; Salvy, S.; Peterson, C.M. Early time-restricted eating affects weight, metabolic health, mood, and sleep in adherent completers: A secondary analysis. Obesity 2023, 31 (Suppl. 1), 96–107. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/oby.23614 (accessed on 1 August 2023). [CrossRef] [PubMed]
- Patsalos, O.; Keeler, J.; Schmidt, U.; Penninx, B.W.J.H.; Young, A.H.; Himmerich, H. Diet, obesity, and depression: A systematic review. J. Pers. Med. 2021, 11, 176. Available online: https://www.narcis.nl/publication/RecordID/oai:pure.atira.dk:publications%2F45d937b1-bffc-42ea-81da-967a81b8a777 (accessed on 1 August 2023). [CrossRef]
- Fagundes, G.B.P.; Tibães, J.R.B.; Silva, M.L.; Braga, M.M.; Silveira, A.L.M.; Teixeira, A.L.; Ferreira, A.V.M. Metabolic and behavioral effects of time-restricted eating in women with overweight or obesity: Preliminary findings from a randomized study. Nutrition 2023, 107, 111909. [Google Scholar] [CrossRef]
- Bowie, R.; Komp, M.; Thomas, A.; Boudrey, S.; Taylor, H.; Martin, B.; Martin, G.; Baum, J.I. The effect of protein supplementation during time restricted feeding in overweight and obese adults. FASEB J. 2022, 36 (Suppl. 1). Available online: https://onlinelibrary.wiley.com/doi/abs/10.1096/fasebj.2022.36.S1.R5724 (accessed on 1 August 2023). [CrossRef]
- Manchishi, S.M.; Cui, R.J.; Zou, X.H.; Cheng, Z.Q.; Li, B.J. Effect of caloric restriction on depression. J. Cell Mol. Med. 2018, 22, 2528. [Google Scholar] [CrossRef]
- Igwe, O.; Sone, M.; Matveychuk, D.; Baker, G.B.; Dursun, S.M. A review of effects of calorie restriction and fasting with potential relevance to depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 111, 110206. [Google Scholar] [CrossRef]
- Araya, A.V.; Orellana, X.; Espinoza, J. Evaluation of the effect of caloric restriction on serum BDNF in overweight and obese subjects: Preliminary evidences. Endocrine 2008, 33, 300–304. Available online: https://link.springer.com/article/10.1007/s12020-008-9090-x (accessed on 1 August 2023). [CrossRef]
- Mayra, S.T.; Kravat, N.; Chondropoulos, K.; De Leon, A.; Johnston, C.S. Early time-restricted eating may favorably impact cognitive acuity in university students: A randomized pilot study. Nutr. Res. 2022, 108, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Irani, H.; Abiri, B.; Khodami, B.; Yari, Z.; Ghazi, M.L.; Hosseinzadeh, N.; Saidpour, A. Effect of time restricted feeding on anthropometric measures, eating behavior, stress, serum levels of BDNF and LBP in overweight/obese women with food addiction: A randomized clinical trial. Nutr. Neurosci. 2023, 1–13. Available online: https://www.tandfonline.com/doi/abs/10.1080/1028415X.2023.2234704 (accessed on 1 August 2023). [CrossRef] [PubMed]
- Kishi, T.; Hirooka, Y.; Nagayama, T.; Isegawa, K.; Katsuki, M.; Takesue, K.; Sunagawa, K. Calorie restriction improves cognitive decline via up-regulation of brain-derived neurotrophic factor: Tropomyosin-related kinase B in hippocampus of obesity-induced hypertensive rats. Int. Heart J. 2015, 56, 110. Available online: https://www.ncbi.nlm.nih.gov/pubmed/25503654 (accessed on 1 August 2023).
- Stephenson, J.; Smith, C.M.; Kearns, B.; Haywood, A.; Bissell, P. The association between obesity and quality of life: A retrospective analysis of a large-scale population-based cohort study. BMC Public Health 2021, 21, 1990. Available online: https://www.ncbi.nlm.nih.gov/pubmed/34732156 (accessed on 1 August 2023). [CrossRef]
- Friedman, K.E.; Reichmann, S.K.; Costanzo, P.R.; Zelli, A.; Ashmore, J.A.; Musante, G.J. Weight stigmatization and ideological beliefs: Relation to psychological functioning in obese adults. Obesity 2005, 13, 907–916. Available online: https://agris.fao.org/agris-search/search.do?recordID=US201301001411 (accessed on 1 August 2023). [CrossRef] [PubMed]
- Forhan, M.; Gill, S.V. Obesity, functional mobility and quality of life. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 129–137. Available online: https://www.clinicalkey.es/playcontent/1-s2.0-S1521690X13000171 (accessed on 1 August 2023). [CrossRef] [PubMed]
- Carson, T.L.; Hidalgo, B.; Ard, J.D.; Affuso, O. Dietary interventions and quality of life: A systematic review of the literature. J. Nutr. Educ. Behav. 2014, 46, 90–101. Available online: https://www.clinicalkey.es/playcontent/1-s2.0-S1499404613006295 (accessed on 1 August 2023). [CrossRef] [PubMed]
- Kesztyüs, D.; Fuchs, M.; Cermak, P.; Kesztyüs, T. Associations of time-restricted eating with health-related quality of life and sleep in adults: A secondary analysis of two pre-post pilot studies. BMC Nutr. 2020, 6, 76. Available online: https://www.ncbi.nlm.nih.gov/pubmed/33327959 (accessed on 1 August 2023). [CrossRef]
- Schroder, J.D.; Falqueto, H.; Mânica, A.; Zanini, D.; de Oliveira, T.; de Sá, C.A.; Cardoso, A.M.; Manfredi, L.H. Effects of time-restricted feeding in weight loss, metabolic syndrome and cardiovascular risk in obese women. J. Transl. Med. 2021, 19, 3. Available online: https://www.ncbi.nlm.nih.gov/pubmed/33407612 (accessed on 1 August 2023). [CrossRef]
- Anton, S.D.; Lee, S.A.; Donahoo, W.T.; McLaren, C.; Manini, T.; Leeuwenburgh, C.; Pahor, M. The effects of time restricted feeding on overweight, older adults: A pilot study. Nutrients 2019, 11, 1500. Available online: https://www.ncbi.nlm.nih.gov/pubmed/31262054 (accessed on 1 August 2023). [CrossRef]
- Crose, A.; Alvear, A.; Singroy, S.; Wang, Q.; Manoogian, E.; Panda, S.; Mashek, D.G.; Chow, L.S. Time-restricted eating improves quality of life measures in overweight humans. Nutrients 2021, 13, 1430. Available online: https://www.ncbi.nlm.nih.gov/pubmed/33922683 (accessed on 1 August 2023). [CrossRef]
- Parr, E.B.; Devlin, B.L.; Radford, B.E.; Hawley, J.A. A delayed morning and earlier evening time-restricted feeding protocol for improving glycemic control and dietary adherence in men with overweight/obesity: A randomized controlled trial. Nutrients 2020, 12, 505. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32079327 (accessed on 1 August 2023). [CrossRef]



{kind=link}
{kind=link}
| TRE | CR | Control | |
|---|---|---|---|
| n | 30 | 30 | 30 |
| Age (year) | 44 ± 12 | 44 ± 9 | 44 ± 13 |
| Sex, no. (%) | |||
| Female | 25 (83%) | 24 (80%) | 25 (83%) |
| Male | 5 (17%) | 6 (20%) | 5 (17%) |
| Race or ethnic group, no. (%) | |||
| Black | 11 (37%) | 9 (30%) | 10 (33%) |
| Asian | 3 (10%) | 3 (10%) | 0 (0%) |
| Hispanic | 13 (43%) | 11 (37%) | 17 (57%) |
| White | 3 (10%) | 7 (23%) | 3 (10%) |
| Body weight and composition | |||
| Body weight (kg) | 100 ± 17 | 102 ± 18 | 102 ± 17 |
| Fat mass (kg) | 46 ± 11 | 47 ± 11 | 47 ± 10 |
| Lean mass (kg) | 50 ± 10 | 50 ± 9 | 51 ± 8 |
| Visceral fat mass (kg) | 1.6 ± 0.6 | 1.6 ± 0.8 | 1.7 ± 0.8 |
| Waist circumference (cm) | 109 ± 13 | 110 ± 14 | 110 ± 13 |
| Height (cm) | 164 ± 9 | 166 ± 9 | 165 ± 7 |
| BMI (kg/m2) | 37 ± 6 | 37 ± 5 | 38 ± 5 |
| Physical activity (steps/day) | 6465 ± 2653 | 6627 ± 2842 | 6424 ± 2302 |
| Mood | |||
| BDI-II, depression score | 15 ± 8 | 12 ± 12 | 10 ± 8 |
| POMS, tension | 3 ± 3 | 2 ± 3 | 4 ± 5 |
| POMS, depression | 1 ± 2 | 2 ± 5 | 1 ± 2 |
| POMS, anger | 1 ± 2 | 2 ± 4 | 1 ± 2 |
| POMS, fatigue | 3 ± 3 | 3 ± 5 | 3 ± 4 |
| POMS, vigor (good mood) | 7 ± 4 | 8 ± 4 | 9 ± 5 |
| POMS, confusion | 2 ± 3 | 2 ± 3 | 2 ± 2 |
| POMS, total mood disturbance score | −14 ± 3 | −10 ± 24 | −18 ± 14 |
| Quality of Life | |||
| SF-36, vitality | 54 ± 19 | 60 ± 21 | 64 ± 19 |
| SF-36, mental health | 74 ± 16 | 77 ± 19 | 80 ± 14 |
| SF-36, bodily pain | 72 ± 24 | 81 ± 17 | 82 ± 24 |
| SF-36, general physical health | 62 ± 18 | 62 ± 23 | 66 ± 18 |
| Variables | Change from Baseline to Month 12 (95% CI) | Difference between Groups by Month 12 (95% CI) | ||||
|---|---|---|---|---|---|---|
| TRE | CR | CON | TRE vs. CR | TRE vs. CON | CR vs. CON | |
| Body weight and composition | ||||||
| Body weight (kg) | −3.49 (−5.65, −1.32) | −4.30 (−7.63, −0.96) | 1.12 (−0.69, 2.94) | 0.81 (−3.07, 4.69) | −4.61 (−7.37, −1.85) | −5.42 (−9.13, −1.71) |
| Body weight (%) | −3.76 (−5.89, −1.64) | −4.20 (−7.59, −0.80) | 1.11 (−0.72, 2.94) | 0.43 (−3.48, 4.34) | −4.87 (−7.61, −2.13) | −5.30 (−9.06, −1.54) |
| Fat mass (kg) | −2.20 (−3.88, −0.52) | −2.61 (−5.97, 0.74) | 0.57 (−1.14, 2.27) | 0.42 (−3.24, 4.07) | −2.77 (−5.10, −0.43) | −3.18 (−6.85, 0.49) |
| Lean mass (kg) | −0.41 (−0.91, 0.08) | −0.74 (−1.44, −0.03) | 0.39 (−0.51, 1.29) | 0.32 (−0.52, 1.16) | −0.81 (−1.81, 0.20) | −1.13 (−2.24, −0.01) |
| Visceral fat mass (kg) | −0.14 (−0.23, −0.04) | −0.12 (−0.29, 0.06) | −0.03 (−0.16, 0.10) | −0.02 (−0.22, 0.17) | −0.11 (−0.27, 0.06) | −0.08 (−0.30, 0.13) |
| Waist circumference (cm) | −6.44 (−8.65, −4.24) | −3.77 (−7.46, −0.08) | −1.46 (−3.77, 0.84) | −2.67 (−6.86, 1.52) | −4.98 (−8.09, −1.87) | −2.30 (−6.55, 1.94) |
| Mood | ||||||
| BDI-II, depression score | −5.99 (−9.37, −2.60) | −3.27 (−6.55, 0.01) | −1.85 (−5.26, 1.55) | −2.72 (−7.32, 1.88) | −4.13 (−8.82, 0.56) | −1.41 (−6.03, 3.20) |
| POMS, tension | 0.02 (−1.31, 1.35) | −0.35 (−2.19, 1.49) | 0.19 (−1.12, 1.50) | 0.37 (−1.85, 2.59) | −0.16 (−1.99, 1.66) | −0.53 (−2.74, 1.67) |
| POMS, depression | 0.84 (−0.05, 1.72) | 0.53 (−1.09, 2.16) | 0.12 (−0.82, 1.06) | 0.31 (−1.50, 2.11) | 0.72 (−0.54, 1.98) | 0.41 (−1.42, 2.25) |
| POMS, anger | 0.39 (−0.47, 1.24) | 0.56 (−1.29, 2.41) | −0.38 (−1.37, 0.60) | −0.17 (−2.16, 1.82) | 0.77 (−0.50, 2.05) | 0.94 (−1.10, 2.99) |
| POMS, fatigue | 0.68 (−0.58, 1.95) | −0.28 (−1.61, 1.04) | 0.41 (−0.91, 1.73) | 0.97 (−0.82, 2.75) | 0.27 (−1.51, 2.06) | −0.69 (−2.52, 1.13) |
| POMS, vigor (good mood) | 0.86 (−0.98, 2.69) | 1.19 (−0.52, 2.90) | 0.26 (−1.29, 1.81) | −0.33 (−2.79, 2.12) | 0.60 (−1.75, 2.94) | 0.93 (−1.32, 3.18) |
| POMS, confusion | −0.22 (−1.30, 0.87) | −0.48 (−1.75, 0.78) | −0.20 (−1.35, 0.95) | 0.27 (−1.36, 1.89) | −0.02 (−1.56, 1.52) | −0.29 (−1.95, 1.38) |
| POMS, total mood disturbance score | −0.33 (−5.15, 4.49) | −1.05 (−9.29, 7.19) | −0.47 (−6.40, 5.46) | 0.72 (−8.59, 10.03) | 0.14 (−7.32, 7.60) | −0.58 (−10.49, 9.32) |
| Quality of Life | ||||||
| SF-36, vitality | 8.42 (2.86, 13.98) | 4.42 (−2.63, 11.47) | 0.65 (−4.82, 6.12) | 4.00 (−4.76, 12.76) | 7.77 (0.15, 15.39), p = 0.05 | 3.77 (−4.93, 12.47) |
| SF-36, mental health | 1.77 (−4.41, 7.95) | −3.79 (−11.65, 4.07) | −0.36 (−6.46, 5.75) | 5.56 (−4.20, 15.32) | 2.13 (−6.36, 10.61) | −3.43 (−13.14, 6.28) |
| SF-36, bodily pain | 1.52 (−7.72, 10.75) | −4.68 (−14.20, 4.84) | 0.90 (−5.45, 7.25) | 6.20 (−6.75, 19.14) | 0.61 (−10.33, 11.55) | −5.58 (−16.75, 5.58) |
| SF-36, general physical health | 6.53 (−1.80, 14.86) | 4.46 (−4.25, 13.17) | −0.96 (−6.60, 4.68) | 2.07 (−9.68, 13.83) | 7.49 (−2.32, 17.30) | 5.42 (−4.71, 15.55) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.; Cienfuegos, S.; Ezpeleta, M.; Pavlou, V.; Chakos, K.; McStay, M.; Runchey, M.-C.; Alexandria, S.J.; Varady, K.A. Effect of Time-Restricted Eating versus Daily Calorie Restriction on Mood and Quality of Life in Adults with Obesity. Nutrients 2023, 15, 4313. https://doi.org/10.3390/nu15204313
Lin S, Cienfuegos S, Ezpeleta M, Pavlou V, Chakos K, McStay M, Runchey M-C, Alexandria SJ, Varady KA. Effect of Time-Restricted Eating versus Daily Calorie Restriction on Mood and Quality of Life in Adults with Obesity. Nutrients. 2023; 15(20):4313. https://doi.org/10.3390/nu15204313
Chicago/Turabian StyleLin, Shuhao, Sofia Cienfuegos, Mark Ezpeleta, Vasiliki Pavlou, Kaitlin Chakos, Mara McStay, Mary-Claire Runchey, Shaina J. Alexandria, and Krista A. Varady. 2023. "Effect of Time-Restricted Eating versus Daily Calorie Restriction on Mood and Quality of Life in Adults with Obesity" Nutrients 15, no. 20: 4313. https://doi.org/10.3390/nu15204313
APA StyleLin, S., Cienfuegos, S., Ezpeleta, M., Pavlou, V., Chakos, K., McStay, M., Runchey, M.-C., Alexandria, S. J., & Varady, K. A. (2023). Effect of Time-Restricted Eating versus Daily Calorie Restriction on Mood and Quality of Life in Adults with Obesity. Nutrients, 15(20), 4313. https://doi.org/10.3390/nu15204313